Back to Journals » Risk Management and Healthcare Policy » Volume 18
Factors Influencing Non-Proliferative Retinopathy in Elderly Patients with T2DM: Metabolic-Behavioral Interaction Analysis
Authors Xia L, Zheng C, Zhang J, Geng G, Qian X
Received 28 May 2025
Accepted for publication 27 September 2025
Published 15 October 2025 Volume 2025:18 Pages 3329—3342
DOI https://doi.org/10.2147/RMHP.S531865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Lanting Xia,1,* Chen Zheng,1,* Jiangao Zhang,2 Guiling Geng,1,3 Xiangyun Qian4
1School of Nursing and Rehabilitation, Nantong University, Nantong, Jiangsu Province, People’s Republic of China; 2Department of Deanery, Nantong Wenci Ophthalmic Hospital, Nantong, Jiangsu Province, People’s Republic of China; 3Nursing Teaching and Research Office, Nantong Institute of Technology, Nantong, Jiangsu Province, People’s Republic of China; 4Nursing Department, Nantong Third People’s Hospital; Affiliated Nantong Hospital 3 of Nantong University, Nantong, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangyun Qian, Nursing Department, Nantong Third People’s Hospital; Affiliated Nantong Hospital 3 of Nantong University, No. 60 Qingnian Zhong Road, Chongchuan District, Nantong, Jiangsu Province, People’s Republic of China, Email [email protected] Guiling Geng, Nantong Institute of Technology, 211 Yongxing Road, Chongchuan District, Nantong, Jiangsu Province, People’s Republic of China, Email [email protected]
Purpose: To investigate the interaction between metabolic and behavioral factors in non-proliferative diabetic retinopathy (NPDR) among elderly patients with type 2 diabetes mellitus (T2DM).
Patients and Methods: A cross-sectional study was conducted from October 2023 to May 2024 using cluster random sampling to recruit elderly patients with T2DM from two tertiary hospitals in Nantong. A self-designed questionnaire was utilized to collect lifestyle and behavioral data. Non-mydriatic fundus photography was used for DR screening, and biochemical indicators were extracted from electronic medical records. Descriptive statistics were applied to analyze demographic characteristics, while univariate and multivariable logistic regression analyses were performed to identify factors influencing NPDR. Interaction models evaluated multiplicative and additive effects between metabolic indicators (low-density lipoprotein cholesterol [LDL-C], urine albumin-to-creatinine ratio [UACR]) and weekly fish consumption frequency on NPDR. Receiver operating characteristic (ROC) curves assessed the diagnostic value of elevated UACR, low fish consumption, and their interaction for NPDR.
Results: Among 978 eligible elderly patients with T2DM, 794 were included, with 306 (38.5%) diagnosed with DR, including 246 (31.0%) with NPDR. Multivariable logistic regression identified diabetes duration, LDL-C, UACR, and weekly fish consumption as independent risk factors for NPDR. Interaction analysis demonstrated significant positive multiplicative (OR=8.89, 95% CI=2.87– 9.52, P< 0.001) and additive interactions (RERI=2.77, API=0.31, SI=1.54) were observed between low fish consumption (< 2 times/week) and severe UACR (> 33.9 mg/mmol). No interactions were found with moderate UACR (3.4– 33.9 mg/mmol) or elevated LDL-C (> 1.8 mmol/L). ROC analysis demonstrated AUC values of 0.840, 0.816, and 0.893 for severe UACR, low fish consumption, and their combined effect, respectively, indicating enhanced diagnostic utility for NPDR.
Conclusion: The synergistic interaction between severe UACR and infrequent fish consumption significantly elevates NPDR risk in elderly patients with T2DM, highlighting its potential as a predictive marker for early intervention.
Keywords: type 2 diabetes mellitus, behavior, non-proliferative diabetic retinopathy, UACR, interaction
Introduction
Diabetic retinopathy (DR), one of the most prevalent microvascular complications of type 2 diabetes mellitus (T2DM), poses a formidable global public health challenge due to its substantial risk of irreversible vision loss.1,2 According to the latest data from the International Diabetes Federation (IDF),3 the global diabetic population has surpassed 589 million adults, with the highest prevalence observed among older adults aged 75–79 years (24.8% as of 2024). The accelerating trend of global population aging, coupled with the elevated prevalence of T2DM in elderly populations, has brought the health management of older adults with T2DM into sharp focus.
Non-proliferative diabetic retinopathy (NPDR), the early stage of DR, is characterized by the absence of retinal neovascularization. However, its pathological features already significantly impair visual function even at this stage and carry a heightened risk of progression to proliferative diabetic retinopathy (PDR). The NPDR stage represents a critical window for intervention to prevent vision loss, making early risk stratification and comprehensive management essential for slowing DR progression.4 Although extensive research has examined the impact of metabolic dysregulation (eg, hyperglycemia, dyslipidemia, hypertension) and adverse behavioral factors (eg, smoking, alcohol consumption, physical inactivity) on DR,5–8 most studies have focused on isolated risk factors rather than systematically analyzing metabolic-behavioral interactions. This gap is especially salient in older adults with T2DM, where age-related physiological decline (eg, polypharmacy, multimorbidity) and distinct behavioral patterns (eg, dietary habits, exercise frequency) may lead to a synergistic interplay between metabolic and behavioral factors in DR pathogenesis. For instance, elevated low-density lipoprotein cholesterol (LDL-C) exacerbates retinal microvascular endothelial damage,9 whereas dietary patterns characterized by frequent fish consumption may confer protective effects via anti-inflammatory and antioxidative pathways.10 These interactions may be amplified by age-related metabolic dysadaptation, underscoring the need to investigate metabolic-behavioral synergies in older T2DM patients. Therefore, exploring the interaction between metabolism and behavior in elderly T2DM patients is of great significance for identifying intervention factors and developing effective prevention and control strategies for NPDR in elderly T2DM patients.
Given these considerations, this cross-sectional study aims to identify independent risk and protective factors for NPDR in elderly patients with T2DM, with particular emphasis on delineating the interaction effects between metabolic parameters (eg, LDL-C, UACR) and behavioral characteristics (eg, dietary patterns). The findings are expected to inform evidence-based strategies for preventing and delaying DR progression, ultimately contributing to improved quality of life in this high-risk population.
Material and Methods
Subjects and Study Design
Conducted between October 2023 and May 2024, this study employed a cluster-randomized sampling methodology to recruit a cohort of elderly T2DM patients from diabetes outpatient clinics. Among six tertiary-level comprehensive hospitals in Nantong, two institutions were randomly selected to ensure representative sampling. The cross-sectional design enabled the evaluation of clinical and behavioral parameters within this high-risk population.
Sample Size and Sampling Procedure
The sample size for this study was calculated using the formula  for cross-sectional studies. In the sample size calculation formula, π represents the population proportion. When multiple estimated values of π are available, we followed the conservative approach of selecting the value closest to 0.5 to maximize required sample size. When no prior population data exists, π = 0.5 serves as the default assumption as it yields the largest possible sample size estimate (maximum variance). With a confidence level (α) set at 0.05 (Zα/2 = 1.96), a global diabetic retinopathy (DR) prevalence rate of 22.3% (π = 22.3%) as reported in Teo et al,11 and a margin of error (δ) of 0.05, the minimum estimated sample size was 267 participants. To account for the cluster sampling design effect (DEFF = 1.5) and a projected 20% attrition rate, the final required sample size was Increased to at least 502 participants.
for cross-sectional studies. In the sample size calculation formula, π represents the population proportion. When multiple estimated values of π are available, we followed the conservative approach of selecting the value closest to 0.5 to maximize required sample size. When no prior population data exists, π = 0.5 serves as the default assumption as it yields the largest possible sample size estimate (maximum variance). With a confidence level (α) set at 0.05 (Zα/2 = 1.96), a global diabetic retinopathy (DR) prevalence rate of 22.3% (π = 22.3%) as reported in Teo et al,11 and a margin of error (δ) of 0.05, the minimum estimated sample size was 267 participants. To account for the cluster sampling design effect (DEFF = 1.5) and a projected 20% attrition rate, the final required sample size was Increased to at least 502 participants.
Inclusion and Exclusion Criteria
The study comprised individuals who met the following criteria: were diagnosed with type 2 diabetes mellitus (T2DM) and aged ≥60 years, and provided informed consent and demonstrated sufficient cooperation to complete fundus photography with a retinal camera. The exclusion criteria encompassed the following: those with ocular pathologies that could affect fundus imaging quality (eg, severe cataracts, ptosis); individuals currently participating in other clinical studies with similar research outcomes.
Survey Instruments
General Data Questionnaire
A structured questionnaire was developed based on authoritative international guidelines, expert consensus, and prior literature. It encompassed the following domains:
Demographic characteristics: Sex, age, marital status, Educational attainment, and health insurance coverage.
Clinical parameters: Height, weight, body mass index (BMI), Blood Pressure: Measured twice (1-minute interval) after 5 minutes of rest using a calibrated electronic sphygmomanometer, with the average value recorded, and Diabetes Mellitus (DM) Treatment Modalities (Categorized into four groups): No pharmacotherapy (lifestyle intervention only); oral hypoglycemic agents alone (eg, metformin, sulfonylureas); Insulin monotherapy (basal/bolus/premixed insulin); Combination therapy (oral agents + insulin).
Behavioral profiles: ① Dietary Habits: Fish consumption (≤2 times/week vs >2 times/week); alcohol intake (never/former/current); ② Smoking Status: never/former/current; ③ Physical Activity (self-reported as seldom/sometimes/regularly); ④ Screen Time: Daily electronic device usage (hours/day).
Metabolic indicators: ① Blood Tests: Venous blood collected after an 8-hour fast for measurement of Fasting blood glucose (FBG), Glycated hemoglobin (HbA1c), Total cholesterol (TC), Low-density lipoprotein cholesterol (LDL-C), High-density lipoprotein cholesterol (HDL-C), and Triglycerides (TG); ② Urinalysis: Morning urine (4 mL) collected for immunoturbidimetric assay of urinary microalbumin and creatinine, with subsequent calculation of the urinary albumin-to-creatinine ratio (UACR).
Fundus Examination
Non-mydriatic fundus imaging was performed using a TOPCON TRC-NW7SF retinal camera. Patients were classified into three groups: no DR, NPDR, and PDR, according to the Chinese Clinical Guidelines for Diabetic Retinopathy Diagnosis and Management (2022 edition).12
NPDR was subclassified as Stage I (mild, microaneurysms only), Stage II (moderate, with retinal hemorrhages, hard exudates, or cotton wool spots), or Stage III (severe, meeting ≥1 criterion: ≥20 intraretinal hemorrhages per quadrant, venous beading in ≥2 quadrants, or intraretinal microvascular abnormalities in ≥1 quadrant). Patients were assigned to the highest-grade group based on the more severely affected eye in cases of asymmetry.
Data Management and Quality Assurance
To ensure methodological rigor, the following quality assurance and control protocols were implemented: Standardized Training: All survey personnel underwent standardized training to ensure uniform administration protocols and minimize inter-rater variability; Structured Data Collection: Surveys were administered via one-on-one interviews; participants completed questionnaires independently or with investigator assistance. All responses were verified on-site for completeness and authenticity prior to submission; Immediate Image Quality Assessment: Fundus images were evaluated for diagnostic adequacy immediately following acquisition. Suboptimal images were reacquired after obtaining participant consent; Dual Independent Data Entry and Validation: Questionnaires were entered into the database using dual data entry to mitigate transcription errors. Data integrity was systematically audited, and incomplete or inconsistent records were excluded from the final analysis. The study protocol followed the principles of the Declaration of Helsinki was reviewed and approved by the Ethics Committee of Affiliated Nantong Hospital 3, Nantong University (Approval No. 2023-K045-01; 23 March 2023). All participants provided written informed consent after receiving detailed explanations about the study objectives and procedures.
Statistical Analysis
Data analysis was performed using SPSS 26.0 and R 4.4.2. Demographic characteristics were summarized as frequencies and percentages. In univariate analyses, continuous variables following a normal distribution were expressed as mean ± standard deviation (SD), while non-normally distributed variables were reported as median (interquartile range, IQR). Categorical variables were analyzed using χ²-tests and presented as proportions. Variables with P < 0.05 in univariate analyses were incorporated into a multivariable logistic regression model. Interaction effects were evaluated using R statistical software to construct additive interaction models, with the relative excess risk due to interaction (RERI), synergy index (SI), and attributable proportion of interaction (API) calculated to quantify effect modification. Receiver operating characteristic (ROC) curve analysis was employed to assess the diagnostic performance of elevated urinary albumin-to-creatinine ratio (UACR), infrequent fish consumption, and their combined predictive capacity. The AUC values ranged from 0.5 to 1.0, with values above 0.80 generally considered clinically useful. All statistical tests were two-tailed, with a significance threshold of α = 0.05. Missing data (with an overall missing rate of <5% for all variables) were addressed using the mode, mean, or median—respectively—based on the data type and distributional normality.
Results
Respondents’ General Information
A total of 978 patients with type 2 diabetes mellitus (T2DM) were initially screened for eligibility. After applying the inclusion and exclusion criteria, 794 participants were enrolled. Stratified based on fundus grading outcomes, the cohort comprised 246 cases of non-proliferative diabetic retinopathy (NPDR), 60 cases of proliferative diabetic retinopathy (PDR), and 488 cases without DR (non-DR group), as delineated in the enrollment flowchart (Figure 1). To align with the study objective of identifying NPDR-specific risk factors, the 60 PDR cases were excluded, yielding a final analytical sample of 734 participants (382 males, 52%). The median age was 66 years (range: 60–89 years).
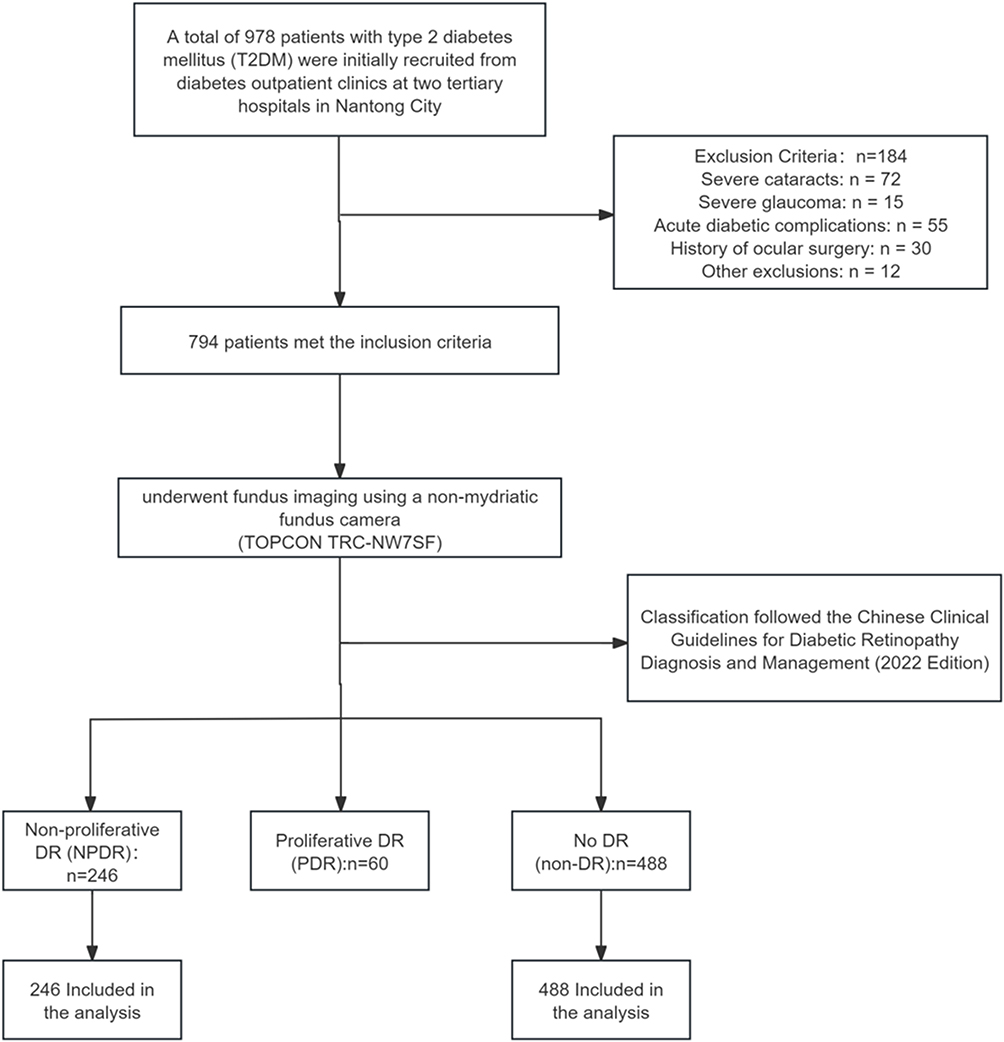 |
Figure 1 Participant Enrollment Flowchart. |
Demographic characteristics revealed that 94.8% of participants were married, 45.5% remained in active employment, and 63.8% reported a personal monthly income below 5,000 RMB. Health insurance coverage was nearly universal (99.2%), with urban resident insurance constituting the majority (61%). Notably, while 22% of T2DM patients self-reported blurred vision, only 2% underwent annual ophthalmic examinations more than twice, indicative of suboptimal adherence to routine ophthalmic surveillance in this population.
Comparative analysis between the NPDR and non-DR groups demonstrated statistically significant disparities in diabetes duration, HbA1c, fasting blood glucose (FBG), weekly fish consumption frequency, urinary albumin-to-creatinine ratio (UACR), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG) levels, and self-reported visual symptoms (all P < 0.05). Conversely, no intergroup differences were observed in age, sex, height, weight, alcohol use history, or physical activity levels (P > 0.05). The basic information of the two groups of included subjects and the variable assignment situations are detailed in Table 1 and Table 2.
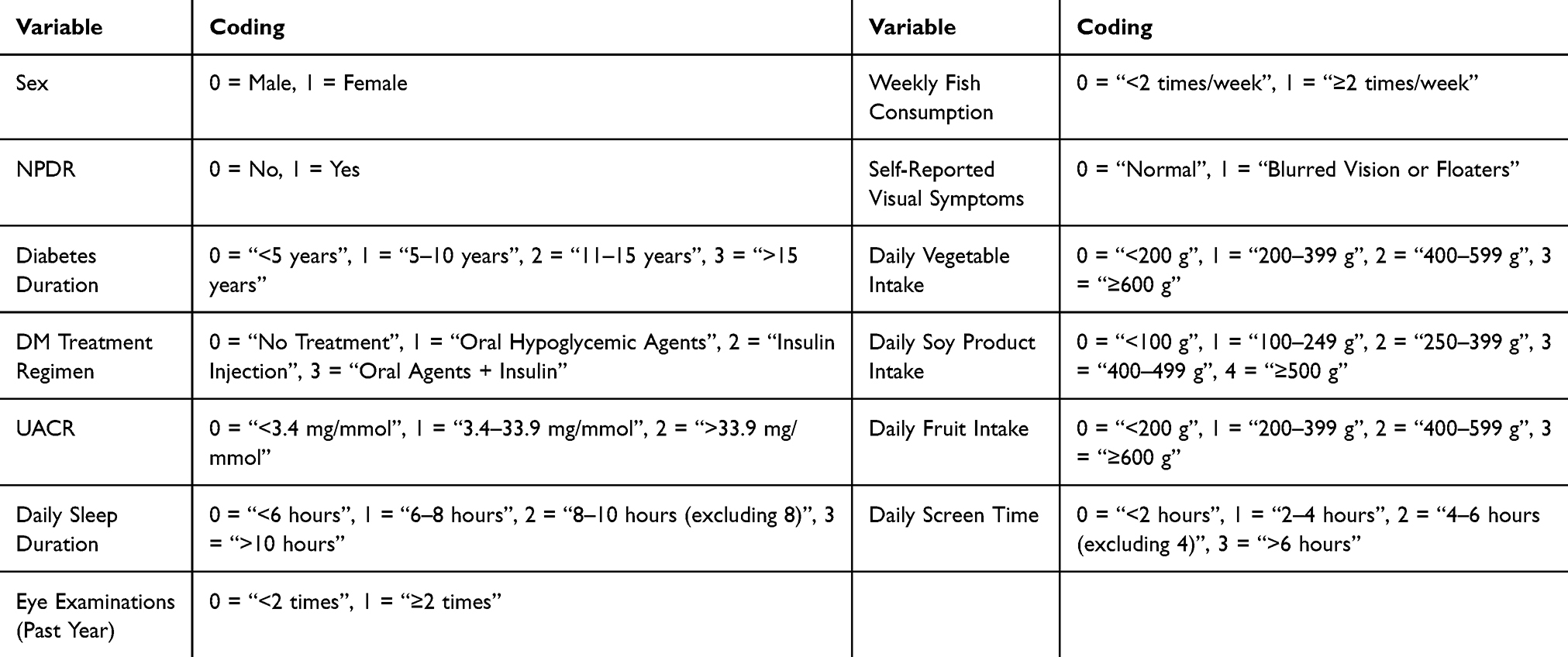 |
Table 1 Research Variables and Values |
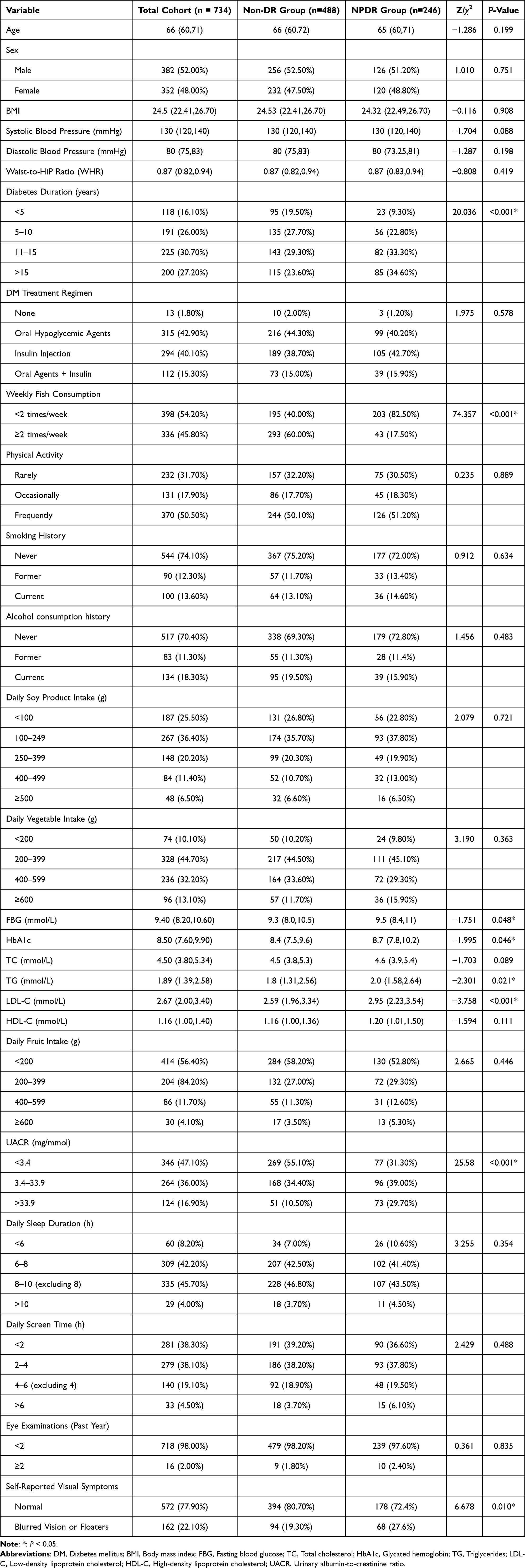 |
Table 2 General Information Survey of Two Groups of Diabetic Patients |
Multifactorial Analysis of Non-Proliferative Diabetic Retinopathy (NPDR) in Patients with Type 2 Diabetes Mellitus
The multivariable logistic regression analysis incorporated variables identified as significant in the univariate analysis for non-proliferative diabetic retinopathy (NPDR). The model demonstrated good fit, with Nagelkerke R² = 0.313 and Cox & Snell R² = 0.205. All independent variables exhibited tolerance values >0.1 and variance inflation factors (VIF) <5, confirming the absence of multicollinearity among predictors. The analysis revealed that a weekly fish consumption frequency of ≥2 servings emerged as an independent protective factor against NPDR (OR=0.176). Conversely, diabetes mellitus (DM) duration exceeding 5 years (OR = 1.755–2.748), higher low-density lipoprotein cholesterol (LDL-C) levels (OR = 2.314) and urinary albumin-to-creatinine ratio (UACR) exceeding 3.4 mg/mmol (OR = 1.613–3.692) were independently associated with an elevated risk of NPDR development. All reported associations demonstrated statistical significance (P < 0.05), as delineated in Table 3.
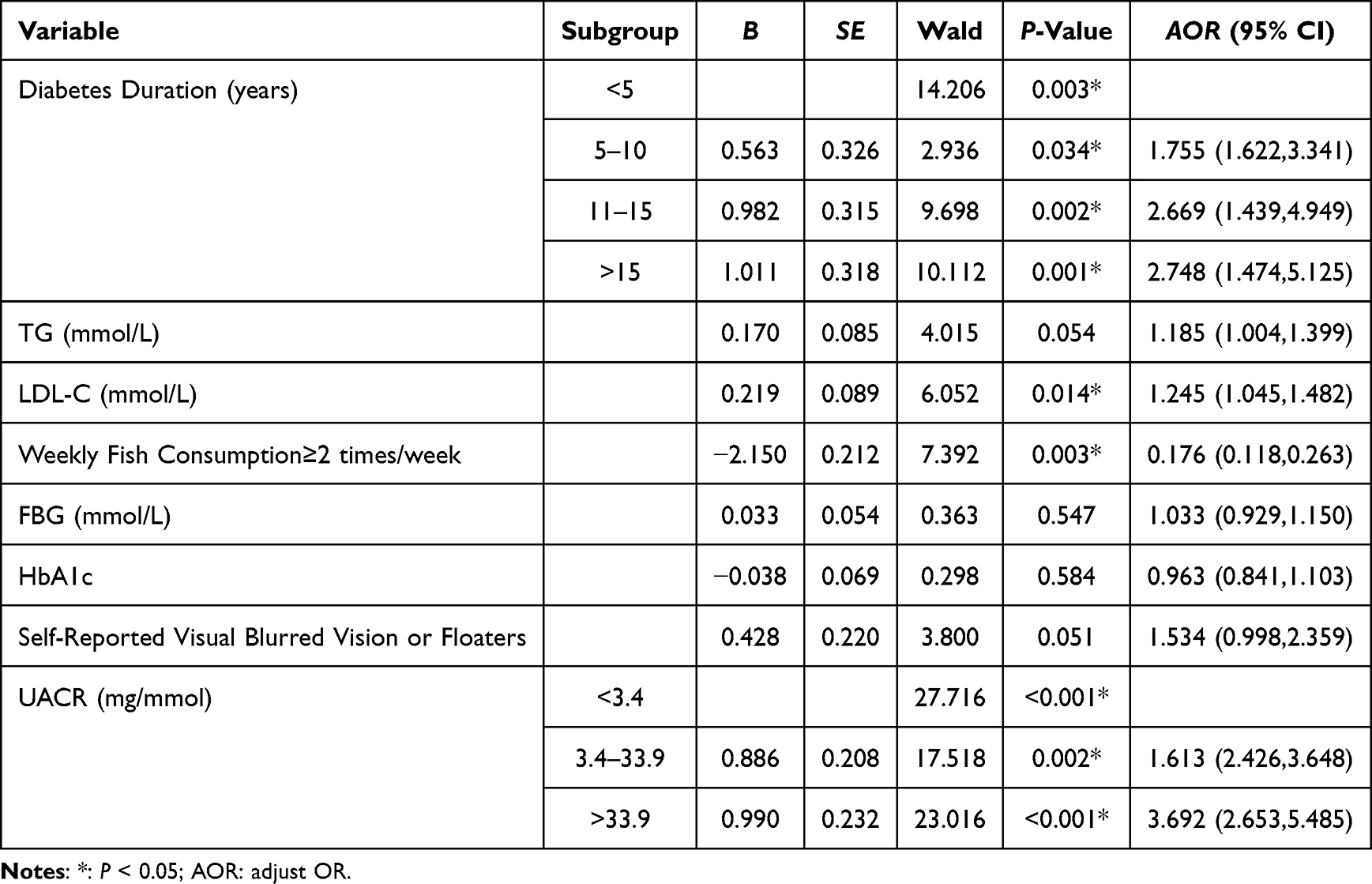 |
Table 3 Multivariable Logistic Regression Analysis of Risk Factors for NPDR |
Interaction Effects Between Low Fish Consumption and Metabolic Indicators in Non-Proliferative Diabetic Retinopathy (NPDR)
Multivariable analyses identified elevated low-density lipoprotein cholesterol (LDL-C) and urinary albumin-to-creatinine ratio (UACR) as independent risk factors for NPDR, while fish consumption of ≥2 times/week served as a protective factor. In alignment with lipid management guidelines,13 which recommend maintaining LDL-C levels below 1.8 mmol/L for patients with diabetes or cardiovascular diseases, the continuous LDL-C variable was dichotomized using 1.8 mmol/L as the threshold. Additionally, UACR was categorized into two dummy variables: UACR2 (moderate albuminuria: 3.4–33.9 mg/mmol) and UACR3 (severe albuminuria: >33.9 mg/mmol). Additive and multiplicative interaction models were employed to evaluate the synergistic effects between infrequent fish consumption (<2 times/week) and metabolic risk factors, including elevated LDL-C (>1.8 mmol/L), UACR2, and UACR3. The results demonstrated that while low-frequency fish consumption showed no significant additive or multiplicative interaction between infrequent fish consumption and high LDL-C or moderate UACR (P>0.05), it exhibited a significant synergistic effect with severe UACR, increasing the risk of NPDR development by 2.77 times (RERI=2.77), accounting for 31% of the total risk (API=0.31). Moreover, in patients with severe UACR who also consumed fish infrequently, the risk of developing NPDR is 1.54 times higher than the sum of the risks of the two factors acting alone (SI=1.54). Furthermore, a significant positive multiplicative interaction was observed (OR=8.89,95% CI=2.87~9.52, P<0.001). Complete interaction metrics are systematically presented in Table 4.
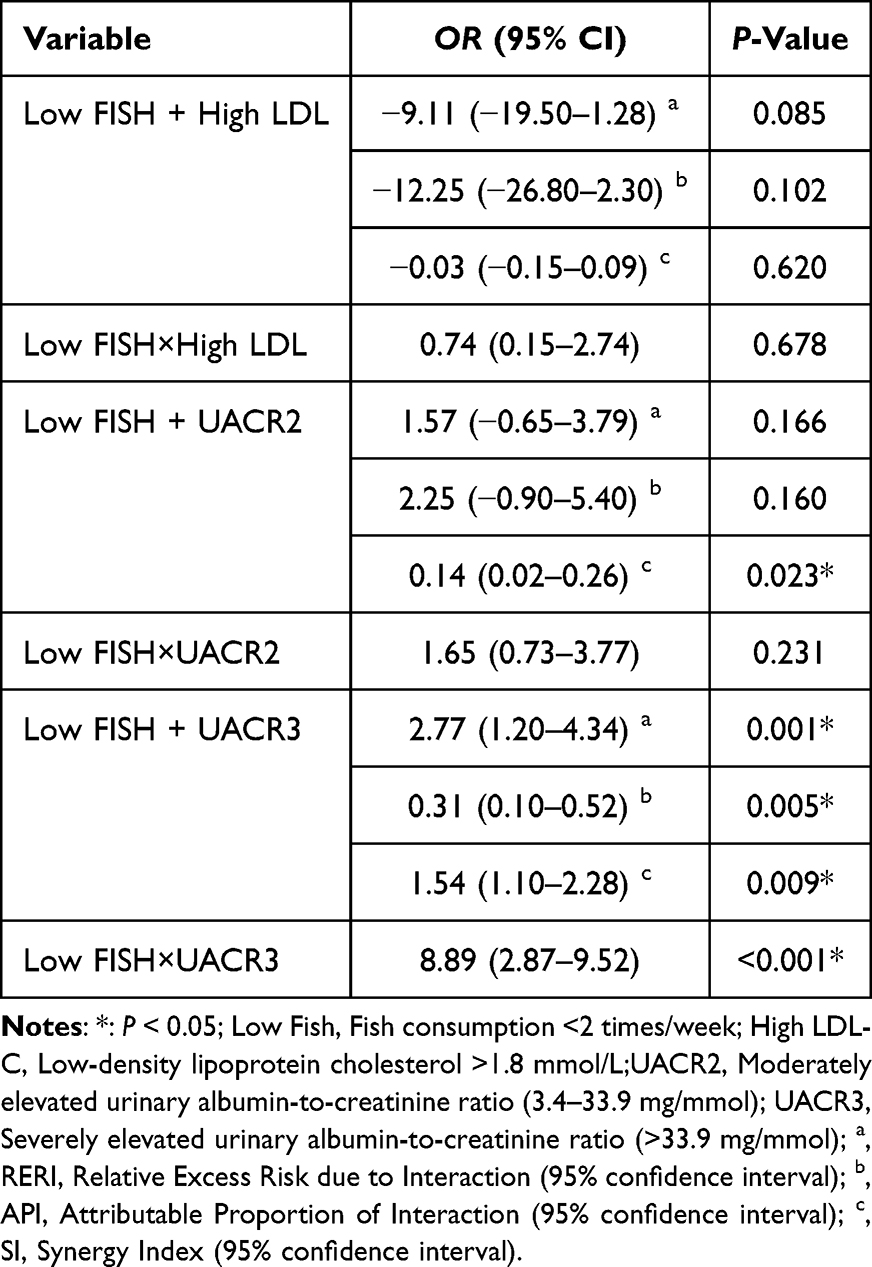 |
Table 4 Interaction Effects Between Low Fish Consumption and Metabolic Indicators on NPDR Risk |
Predictive Efficacy of UACR and Fish Consumption, Along with Their Synergistic Interaction, on NPDR Development
ROC curve analysis revealed that elevated urinary albumin-to-creatinine ratio (UACR), infrequent fish consumption, and their combined interaction demonstrated area under the curve (AUC) values of 0.840, 0.816, and 0.893, respectively, in predicting non-proliferative diabetic retinopathy (NPDR). These findings underscore the enhanced diagnostic utility of the synergistic interaction between UACR and dietary fish intake patterns compared to either factor alone. For detailed visual and tabular representations, refer to Figure 2 and Table 5.
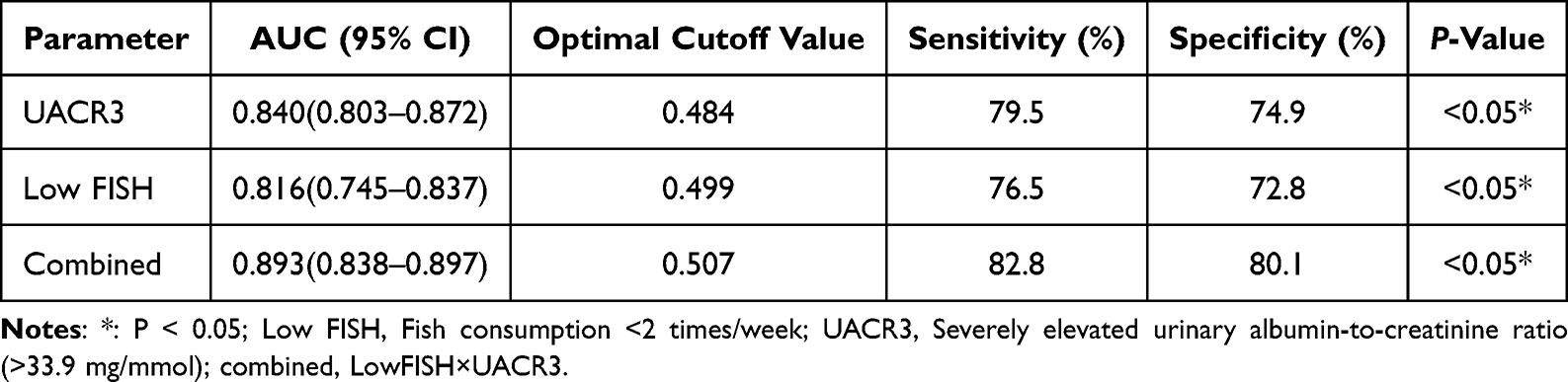 |
Table 5 Diagnostic Performance Metrics of Biomarker Parameters and Synergistic Interactions in NPDR Prediction |
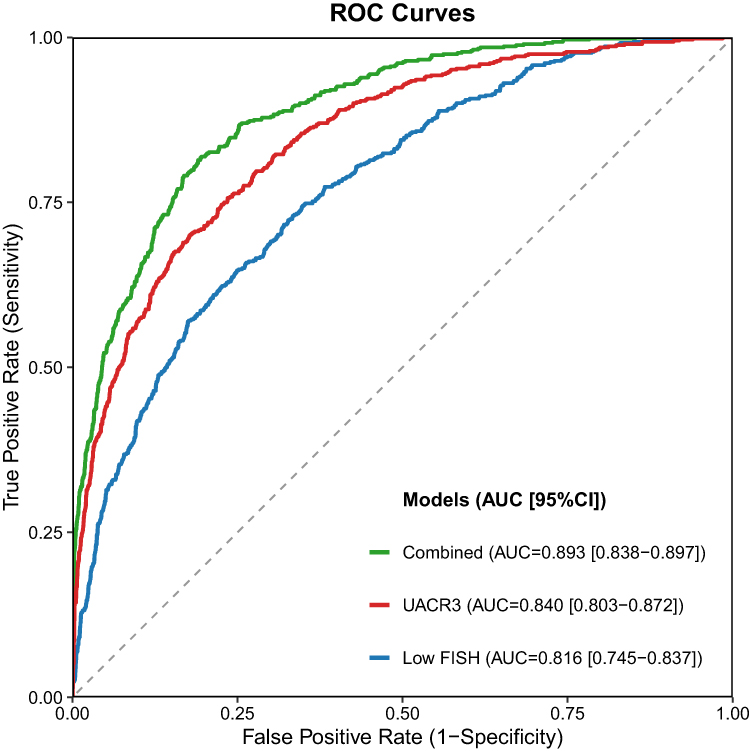 |
Figure 2 ROC Curve Analysis of Biomarker Parameters and Synergistic Interactions in NPDR Diagnosis. |
Discussion
Analysis of Current Situation and Influencing Factors of NPDR in Elderly T2DM Patients
This study enrolled 794 elderly patients with type 2 diabetes mellitus (T2DM), revealing a non-proliferative diabetic retinopathy (NPDR) prevalence of 31.0% and an overall diabetic retinopathy (DR) prevalence of 38.5%. These rates substantially exceed the 24.35% reported in Ethiopian cohorts14 yet remain marginally lower than the 41.29% observed in Dai ethnic populations from Yunnan, China.15 Discrepancies may stem from age-related metabolic decline, diminished microvascular repair capacity, and heterogeneity in screening methodologies—particularly the enhanced diagnostic sensitivity of non-mydriatic fundus cameras.16–18 Notably, while 22.1% of patients exhibited visual abnormalities, a mere 2% underwent biannual ophthalmic evaluations, highlighting critical deficits in risk perception and screening adherence. These findings underscore the imperative to intensify diabetic eye complication screening protocols.19
Multivariable regression identified diabetes duration, elevated LDL-C, and abnormal urinary albumin-to-creatinine ratio (UACR) as independent risk factors for NPDR (P < 0.05). Patients with diabetes histories exceeding 5 years demonstrated markedly increased DR risk (OR = 1.76–2.75), aligning with prior epidemiological pattern.20 Mechanistically, LDL-C dysregulation and UACR abnormalities may exacerbate DR progression by inducing retinal microvascular inflammatory cascades, oxidative stress, and blood-retinal barrier disruption.21 Conversely, frequent fish consumption (≥2 servings/week) emerged as a protective factor against NPDR (OR = 0.18, P < 0.05), likely attributable to the anti-inflammatory and endothelium-repairing properties of ω-3 polyunsaturated fatty acids abundant in marine sources.22
Metabolic and Behavioral Interactions in Elderly T2DM Patients
While existing studies predominantly investigate independent effects of metabolic indices or behavioral factors on diabetic retinopathy (DR), systematic analyses of “metabolic-behavioral synergies” remain scarce. This study provides pioneering evidence for the synergistic detrimental effects of severe urinary albumin-to-creatinine ratio (UACR >33.9 mg/mmol) and infrequent fish consumption (<2 servings/week) on non-proliferative diabetic retinopathy (NPDR), manifesting as significant additive interaction (SI=1.54, 95% CI=2.87–9.52) and multiplicative interaction (OR = 8.89, 95% CI: 2.87–9.52). This convergence likely arises from multifaceted microvascular pathophysiological mechanisms:1) UACR-Mediated Systemic Microvascular Crosstalk: As a quantitative biomarker of renal microvascular injury, elevated UACR reflects glomerular barrier dysfunction. Proinflammatory mediators released during renal damage may disseminate via systemic circulation to retinal microvasculature, exacerbating retinal ischemia and hypoxia through microvascular spasm induction.23,24 Research indicates that declining renal function is closely associated with both the onset and progression of diabetic retinopathy (DR). Patients with renal impairment not only have a significantly higher risk of developing DR but also show a strong positive correlation between retinal lesion severity and degree of renal dysfunction.25 (2) ω-3 Deficiency and Vascular Homeostasis Disruption Marine-derived ω-3 polyunsaturated fatty acids (eg, EPA/DHA) exhibit potent anti-inflammatory and antioxidant properties.Omega-3 fatty acids attenuate retinal inflammatory responses by suppressing pro-inflammatory cytokine release (eg, TNF-α, IL-6). They also enhance antioxidant enzyme activity, reducing oxidative stress-induced endothelial damage and improving microvascular function. Mechanistically, docosahexaenoic acid (DNA)—a key omega-3 derivative—exerts neuroprotective effects on retinal neurons via modulation of brain-derived neurotrophic factor (BDNF) signaling and GPR120 receptor activation, thereby delaying neurodegeneration.10,26 Cohort studies demonstrate ≥2 weekly fish servings, particularly deep-sea fish—reduce DR incidence by 60%.27,28 Insufficient intake compromises endogenous suppression of endothelial inflammatory cascades, amplifying microvascular vulnerability.29 Current evidence has established that fish consumption, particularly intake of deep-sea fish rich in omega-3 polyunsaturated fatty acids, confers cardiovascular protective effects through lipid metabolism regulation.30,31 Epidemiological studies demonstrate a significant positive correlation between fish consumption frequency and improved lipid profiles. Moderate consumption (1–2 servings/week) is associated with a 36% reduction in coronary heart disease mortality, whereas excessive intake (≥5 servings/week) may exert adverse effects due to heavy metal (eg, mercury) accumulation.32 Notably, our study failed to detect significant interaction effects between low-frequency fish consumption and elevated LDL-C levels (P>0.05). This result may be attributed to age-related metabolic decline potentially attenuating the lipid-modulating effects of fish-derived nutrients in our elderly cohort, combined with potential mixed bias from the lack of fish species classification in dietary assessments. Clinically, the combined evaluation of UACR and fish consumption frequency enhanced NPDR diagnostic accuracy, achieving an AUC of 0.893 (sensitivity: 82.8%, specificity: 80.1%)—significantly surpassing individual biomarker performance. These findings establish that the interaction between metabolic derangements (renal microvascular injury) and nutritional behaviors (ω-3 insufficiency) potentiates NPDR risk. These finding provide innovative approaches for comprehensive risk management of diabetic patients. During intervals between scheduled fundus screenings, biochemical marker monitoring (UACR) combined with nutritional assessment (fish consumption) helps identify high-risk groups. It addresses current limitations in existing screening systems by quantifying behavioral factors, while establishing a critical biomarker combination for developing a multidimensional NPDR risk prediction model based on metabolic and behavioral parameters.
Conclusion
The risk of developing diabetic retinopathy (DR) is high in elderly patients with diabetes. Previous studies have predominantly examined general risk factors for diabetic retinopathy (DR), yet few have specifically investigated non-proliferative DR (NPDR) in elderly populations with type 2 diabetes mellitus (T2DM). Crucially, existing research has neglected to account for potential interactions between metabolic dysregulation and behavioral determinants within this high-risk cohort. This study reveals the combined predictive value of the urine albumin/creatinine ratio (UACR) and dietary intake of omega-3 fatty acids for non-proliferative diabetic retinopathy (NPDR), suggesting that certain metabolic abnormalities and behavioral patterns may interact to influence disease development. It is recommended to incorporate dynamic monitoring of UACR and dietary guidance rich in ω-3 into the comprehensive prevention and control pathway for diabetic eye disease. Establishing dual interventions on both metabolism and behavior while managing independent influencing factors can not only compensate for the lag in imaging screening but also reduce medical costs through lifestyle interventions, breaking the synergistic pathogenic effect between metabolism and behavior, thereby delaying the onset and progression of DR as much as possible. This study has several limitations. First, as a cross-sectional investigation, although significant associations were identified between NPDR and factors such as fish consumption, the inherent constraints of the study design preclude causal inferences. Second, regarding the assessment of dietary fish intake, the study did not quantify specific fish types (eg, deep-sea vs freshwater fish) or preparation methods (eg, raw vs fried consumption), which may introduce variability in the accurate evaluation of protective components such as ω-3 fatty acids. Third, the single-center design and relatively homogeneous sample (limited to elderly patients with type 2 diabetes mellitus) may restrict the generalizability of the findings. Caution is warranted when extrapolating these results to diverse ethnic populations (eg, potential dietary pattern disparities between Asian and Western demographics) or other diabetes subtypes. Lastly, self-reported dietary and behavioral data are susceptible to recall bias, with diabetic patients potentially exhibiting heightened dietary awareness bias. To address these limitations, future research should prioritize multicenter prospective cohort studies to longitudinally examine the dynamic relationship between NPDR progression and dietary modifications. Furthermore, incorporating objective nutritional biomarkers and comprehensive dietary assessments would enhance the robustness of the findings.
Acknowledgments
We sincerely appreciate the contributions of all individuals involved in this research endeavor.
Funding
This is a part research accomplishment of the project “Nantong Municipal Health Commission“ (NO. MSZ2023070), the project “Special Scientific Research Fund Project of Clinical Medicine, Nantong University, 2024” (No. 2024HZ001), the project “Hospital Management Innovation Research Project of Jiangsu Provincial Hospital Association in 2024” (NO.JSYGY-3-2024-289), the project “Nantong Social livelihood science and technology plan (guidance) project“ (No. MSZ2023013).
Disclosure
The authors confirm the absence of any conflicts of interest, financial or otherwise, that could have unduly affected the objectivity of this academic work.
References
1. Tan TE, Wong TY. Diabetic retinopathy: looking forward to 2030. Front Endocrinol. 2022;13:1077669. doi:10.3389/fendo.2022.1077669
2. Sun H, Saeedi P, Karuranga S, et al. Erratum to “IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045” [diabetes res. Clin. Pract. 183 (2022) 109119]. Diabet Res Clin Pract. 2023;204:110945. doi:10.1016/j.diabres.2023.110945
3. IDF diabetes atlas. Diabetes Atlas. 2025. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/.
4. Yang P, Yang B. Development and validation of predictive models for diabetic retinopathy using machine learning. PLoS One. 2025;20(2):e0318226. doi:10.1371/journal.pone.0318226
5. Aldosari DI, Malik A, Alhomida AS, Ola MS. Implications of diabetes-induced altered metabolites on retinal neurodegeneration. Front Neurosci. 2022;16:938029. doi:10.3389/fnins.2022.938029
6. Aytenew TM, Kefale D, Birhane BM, et al. Visual impairment among diabetes patients in Ethiopia: a systematic review and meta-analysis. PLoS One. 2024;19(5):e0303388. doi:10.1371/journal.pone.0303388
7. Zhu C, Zhu J, Wang L, et al. Development and validation of a risk prediction model for diabetic retinopathy in type 2 diabetic patients. Sci Rep. 2023;13(1):5034. doi:10.1038/s41598-023-31463-5
8. Wang B, Li H, Ma H, Chen Z. The association of cigarette smoking with the development and progression of diabetic retinopathy: based on cross-sectional survey and mendelian randomization. J Transl Med. 2024;22(1):1169. doi:10.1186/s12967-024-06002-z
9. Karimi MA, Vaezi A, Ansari A, et al. Lipid variability and risk of microvascular complications in patients with diabetes: a systematic review and meta-analysis. BMC Endocr Disord. 2024;24(1):4. doi:10.1186/s12902-023-01526-9
10. Zeppieri M, Gagliano C, D’Esposito F, et al. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA): a targeted antioxidant strategy to counter oxidative stress in retinopathy. Antioxid Basel Switz. 2024;14(1):6. doi:10.3390/antiox14010006
11. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
12. Ocular Fundus Disease Group, Chinese Society of Ophthalmology; Ocular Fundus Disease Group, Chinese Medical Doctor Association. Clinical guidelines for diagnosis and treatment of diabetic retinopathy in China (2022) [in Chinese]. Chin J Ocul Fundus Dis. 2023;39(2):99–124.
13. Marathe PH, Gao HX, Close KL. American diabetes association standards of medical care in diabetes 2017. J Diabetes. 2017;9(4):320–324. doi:10.1111/1753-0407.12524
14. Tg W, Ja M. Prevalence of diabetic retinopathy and its associated risk factors among adults in Ethiopia: a systematic review and meta-analysis. Sci Rep. 2024;14(1):28266. doi:10.1038/s41598-024-78596-9
15. Cun YK, Qu JL, Li BA, Yang M, Zhong H. Prevalence and risk factors of type 2 diabetic retinopathy in Dai ethnic areas of Yunnan Province [in Chinese]. J Kunming Univ Sci Technol. 2024;49(2):104–111.
16. Tang T, Tran D, Han D, Zeger SL, Crews DC, Cai CX. Place, race, and lapses in diabetic retinopathy care. JAMA Ophthalmol. 2024;142(6):581–583. doi:10.1001/jamaophthalmol.2024.0974
17. Ghanma RA, Al-Asa’d R, Mohammad A, Al Qararah M, Bani Issa A. Factors affecting the awareness of diabetic retinopathy: an observational cross-sectional study. Cureus. 2024;16(4):e59020. doi:10.7759/cureus.59020
18. Curran K, Piyasena P, Congdon N, Duke L, Malanda B, Peto T. Inclusion of diabetic retinopathy screening strategies in national level diabetes care planning in low and middle-income countries: a scoping review. Eur J Ophthalmol. 2021;31(2_SUPPL):18.
19. ElSayed NA, McCoy RG, Aleppo G, American Diabetes Association Professional Practice Committee. Diagnosis and classification of diabetes: standards of care in diabetes-2025. Diabetes Care. 2025;48(1):S27–S49. doi:10.2337/dc25-S002
20. Scanlon PH, Nevill CR, Stratton IM, et al. Prevalence and incidence of diabetic retinopathy (DR) in the UK population of gloucestershire. Acta Ophthalmol. 2022;100(2):e560–e570. doi:10.1111/aos.14927
21. Yao X, Pei X, Fan S, Yang X, Yang Y, Li Z. Relationship between renal and liver function with diabetic retinopathy in patients with type 2 diabetes mellitus: a study based on cross-sectional data. Sci Rep. 2022;12(1):9363. doi:10.1038/s41598-022-13164-7
22. Brockington M, Beale D, Gaupholm J, et al. Identifying barriers and pathways linking fish and seafood to food security in inuit nunangat: a scoping review. Int J Environ Res Public Health. 2023;20(3):2629. doi:10.3390/ijerph20032629
23. Heyman SN, Raz I, Dwyer JP, Weinberg Sibony R, Lewis JB, Abassi Z. Diabetic proteinuria revisited: updated physiologic perspectives. Cells. 2022;11(18):2917. doi:10.3390/cells11182917
24. Wang Q, Cheng H, Jiang S, et al. The relationship between diabetic retinopathy and diabetic nephropathy in type 2 diabetes. Front Endocrinol. 2024;15:1292412. doi:10.3389/fendo.2024.1292412
25. Fang J, Luo C, Zhang D, He Q, Liu L. Correlation between diabetic retinopathy and diabetic nephropathy: a two-sample mendelian randomization study. Front Endocrinol. 2023;14:1265711. doi:10.3389/fendo.2023.1265711
26. Rodríguez González-Herrero ME, Ruiz M, López Román FJ, Marín Sánchez JM, Domingo JC. Supplementation with a highly concentrated docosahexaenoic acid plus xanthophyll carotenoid multivitamin in nonproliferative diabetic retinopathy: prospective controlled study of macular function by fundus microperimetry. Clin Ophthalmol Auckl NZ. 2018;12:1011–1020. doi:10.2147/OPTH.S157635
27. Rondanelli M, Gasparri C, Riva A, et al. Diet and ideal food pyramid to prevent or support the treatment of diabetic retinopathy, age-related macular degeneration, and cataracts. Front Med. 2023;10:1168560. doi:10.3389/fmed.2023.1168560
28. Bryl A, Mrugacz M, Falkowski M, Zorena K. A Mediterranean diet may Be protective in the development of diabetic retinopathy. Int J Mol Sci. 2023;24(13):11145. doi:10.3390/ijms241311145
29. Weir NL, Guan W, Karger AB, et al. OMEGA-3 fatty acids are associated with decreased presence and severity of diabetic retinopathy: a combined analysis of Mesa and GOLDR cohorts. Retina. 2023;43(6):984–991. doi:10.1097/IAE.0000000000003745
30. Utri-Khodadady Z, Głąbska D. Effects of increasing farmed salmon intake to the recommended fish-intake amounts on lipid profile in young women: an 8-week intervention study. Nutrients. 2024;16(23):4051. doi:10.3390/nu16234051
31. Zhao H, Wang M, Peng X, et al. Fish consumption in multiple health outcomes: an umbrella review of meta-analyses of observational and clinical studies. Ann Transl Med. 2023;11(3):152. doi:10.21037/atm-22-6515
32. Mozaffarian D, Rimm EB. Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA. 2006;296(15):1885–1899. doi:10.1001/jama.296.15.1885
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.