Back to Journals » Clinical Ophthalmology » Volume 18
Factors Influencing Endoscopic Dacryocystorhinostomy Outcomes: A Comprehensive Clinical and Histopathological Analysis and Review of the Literature
Authors Sieśkiewicz A, Piszczatowski B, Reszeć J, Sieśkiewicz M ![]() , Micun Z, Konopińska J
, Micun Z, Konopińska J ![]()
Received 9 June 2024
Accepted for publication 30 October 2024
Published 19 November 2024 Volume 2024:18 Pages 3277—3288
DOI https://doi.org/10.2147/OPTH.S482069
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andrzej Sieśkiewicz,1 Bartosz Piszczatowski,1 Joanna Reszeć,2 Michał Sieśkiewicz,3 Zuzanna Micun,3 Joanna Konopińska4
1Department of Otolaryngology, Medical University of Bialystok, Białystok, Poland; 2Department of Medical Pathomorphology, Medical University of Bialystok, Bialystok, Poland; 3Faculty of Medicine, Medical University of Białystok, Bialystok, Poland; 4Department of Ophthalmology, Medical University of Bialystok, Białystok, Poland
Correspondence: Joanna Konopińska, Department of Ophthalmology, Medical University of Bialystok, M. Sklodowska-Curie 24A Street, Białystok, 15-276, Poland, Tel/Fax +48 600471666, Email [email protected]
Purpose: The main challenge in maintaining long-term success of endoscopic dacryocystorhinostomy is preventing fibrosis and scarring at the anastomosis site. Despite numerous studies on surgical techniques, research on histological factors linked to postoperative scarring is limited. This study evaluated long-term (range, 12– 18 months) outcomes and systematically examined clinical and histopathological factors that may contribute to restenosis.
Patients and Methods: This retrospective study included 47 patients who underwent a unilateral surgery intervention for primary acquired lacrimal duct obstruction. The following clinical and histopathological variables were considered to assess the risk factors for the development of restenosis: sex, age, duration of disease, clinical manifestation of disease, clinical features of the lacrimal sac perceived intraoperatively, fibrosis, and mononuclear cell infiltrates.
Results: Statistical analysis showed that only patient sex (Pearson’s chi-squared test, p = 0.007) and severity of intraoperative adhesions in the lacrimal sac (Pearson’s chi-square test, p = 0.029) were significantly linked to restenosis. However, the skewed male-to-female ratio, few surgical failures make the conclusion that sex is a risk factor speculative. Thus, only adhesion intensity can be considered a risk factor. Additionally, fibrosis assessed using trichrome staining and T-cell lymphocytic infiltration showed potential negative prognostic value in a larger cohort.
Conclusion: Our findings indicate that patients with significant lacrimal sac adhesions, identified during endoscopic dacryocystorhinostomy, are particularly prone to postoperative restenosis. Although histological and immunohistochemical studies did not reveal a correlation between the analyzed data and restenosis, a larger patient cohort might show that fibrosis and T-cell lymphocytic infiltration could potentially have a negative prognostic value. The poorer treatment outcomes in women, seen in our study as well as in other investigations, may be due to anatomical and physiological traits of the female lacrimal drainage system that predispose them to stenosis. This hypothesis requires further study in a larger cohort.
Keywords: fibrosis, lacrimal sac, restenosis, tearing
Introduction
Tear duct obstruction is a notable challenge in ophthalmology. It is the reason for approximately 3% of visits to ophthalmic offices.1 Transnasal endoscopic dacryocystorhinostomy (EDCR) has emerged as a primary surgical modality for addressing lacrimal patency disorders by establishing a direct connection between the lacrimal sac and the nasal cavity. The current success rate of surgical endoscopic treatment for primary acquired lacrimal duct obstruction does not differ significantly from that of procedures using an external approach (ie, approximately 90% for both treatments).2 The primary challenges in maintaining the efficacy of EDCR over time are the development of fibrous tissue and scars at the site of the newly formed anastomosis.3–9 Studies exploring various surgical techniques, including the use of mucosal flaps,10 innovative devices such as lasers11,12 and angled intranasal drills,13 and the topical application of chemotherapeutic agents and drugs such as mitomycin, steroids, and 5-fluorouracil,14–16 as well as the utilization of lacrimal duct stents17 and postoperative interventions aimed at optimizing healing and mitigating fibrosis11,12 have been reported. However, research dedicated to unraveling the factors predisposing individuals to postoperative scarring and restenosis of the anastomosis is scarce. The aim of this study was to address this crucial gap by assessing the long-term treatment outcomes of patients who have undergone EDCR and to systematically investigate previously reported features that may predispose patients to restenosis of the lacrimal drainage system.
Materials and Methods
The treatment was conducted in accordance with the tenets of the Declaration of Helsinki and study received approval from the local Bioethics Committee of Medical University of Bialystok (Bialystok, Poland, decision number: R-I-002/382/2014). The recruitment period was between 1st January 2019 and 31st December 2022. All patients provided written informed consent for treatment and for data use for this study.
The study encompassed 47 patients, of whom 17 (36.2%) were men and 30 (63.8%) were women, with an age range of 18 to 94 years (mean, 62.3 years). The patients were treated at the Department of Otolaryngology at the Medical University of Bialystok (Bialystok, Poland) for primary acquired lacrimal duct obstruction. We excluded patients with a history of previous lacrimal duct surgery; suspected neoplastic and granulomatous diseases of the nose and paranasal sinuses; coexisting chronic rhinosinusitis; and high lacrimal duct obstruction, defined as obstruction of the lacrimal puncta, eyelid, and common canaliculi.
The lack of tear duct patency and the level of obstruction were confirmed during preoperative ophthalmological consultations. The severity of epiphora was subjectively assessed by the patients using a visual analog scale (VAS), where a score of 0 indicated no tearing complaints and a score of 10 indicated very profuse, persistent tearing (Figure 1).
 |
Figure 1 Visual analog scale used in this study. |
All patients underwent surgical treatment performed by the same surgeon using a standardized approach. This involved EDCR with the development of a mucoperiosteal flap, as previously described.18 All patients received identical postoperative care at the ophthalmology and ear, nose, and throat ambulatory clinics. Postoperative daily nasal rinsing with saline solution for a period of 3 months was also recommended.
The assessment of operative outcomes was performed after a minimum follow-up period of 1 year (range, 12–18 months; mean, 14.3 months). This assessment was based on the VAS, irrigation test, and endoscopic dye test. A cure was considered to be the complete or near-complete alleviation of complaints, indicated by a score of 0 or 1 on the subjective VAS, along with confirmed patency of the lacrimal ducts, as demonstrated by the irrigation test and the endoscopic dye test.
The saline irrigation test involved the insertion of a cannula through the lower lacrimal punctum, followed by rinsing of the lacrimal system (to test anatomical patency). A dye test combined with endoscopic observation was used to assess the functional patency of the lacrimal duct. During this test, two drops of 2% fluorescein were introduced into the conjunctival fornix, followed by endoscopic surveillance of the dye traces around the rhinostomy opening in the nasal cavity after 2–5 min.
The following clinical and histopathological variables were investigated to assess the risk factors for the development of restenosis: sex, age, duration of disease, clinical manifestation of disease (ie, epiphora and presence of dacryocystitis), clinical features of the lacrimal sac observed intraoperatively (ie, lacrimal sac size, wall thickness, and presence of adhesions inside the sac), fibrosis, and mononuclear cell infiltrates (ie, T lymphocytes, B lymphocytes, and macrophages).
Lacrimal sac size was categorized as small (ie, Grade 1) or large (ie, Grade 2), based on the vertical dimension. A small sac was defined as having a vertical dimension of less than 8 mm, as assessed using a 4-mm suction tip19 (Figure 2). The wall thickness was categorized as thin (ie, Grade 1) or thick (ie, Grade 2), based on an assessment using a 0.9-mm–thick Bowman probe. A thickness below 0.9 mm was considered thin (Figure 3). Intraoperatively observed adhesions were macroscopically assessed using a three-grade scale, as follows: Grade 1, minor adhesions were found only in the lower part of the lacrimal sac and near the nasolacrimal duct, whereas the mucous membranes of the lacrimal sacs were normal; Grade 2, moderate-severity adhesions filling 1/4 to 3/4 of the interior of the sac cavity, while swelling and redness of the sac lining were also observed; Grade 3, severe adhesions and fibrosis, with the interior of the lacrimal sac cavity filled with scars and fibrous tissue (Figure 4).
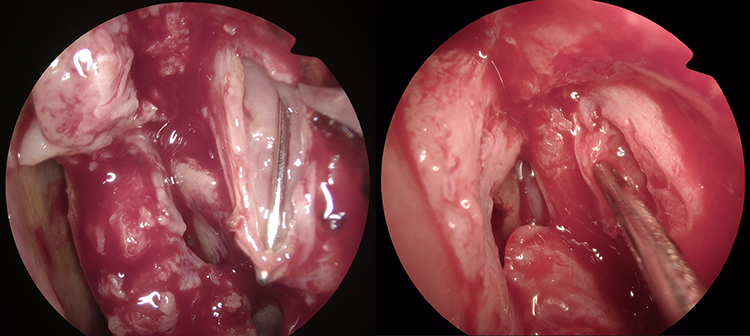 |
Figure 2 Thin-walled lacrimal sac (grade 1) with a 0.6 mm lacrimal probe. Lacrimal sac size classified as grade 1 (vertical dimension less than 8 mm, assessed using a 4 mm suction tip visible next to the incised sac). Moderate adhesions filling up to three-quarters of the sac cavity – grade 2. |
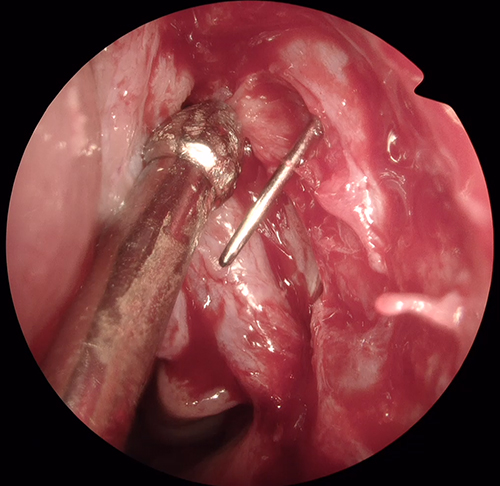 |
Figure 3 Left - Thin-walled sac (grade 1) with a 0.6 mm lacrimal probe. Lacrimal sac size classified as grade 2 (vertical dimension greater than 8 mm), with no or minimal adhesions inside the sac – grade 1. Right - Thick-walled lacrimal sac (grade 2) with a wall thicker than the diameter of a 0.9 mm lacrimal probe inserted into the nasal meatus, with the probe touching the wall of the lacrimal sac. |
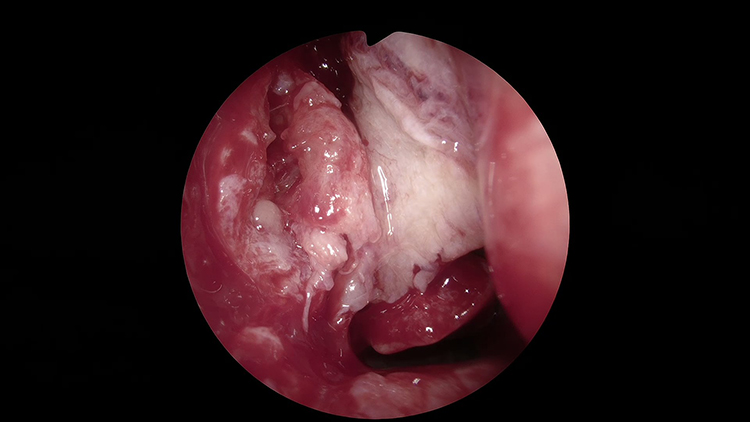 |
Figure 4 Incised lacrimal sac completely filled with inflammatory tissue and adhesions – grade 3. |
The removed fragments of the lacrimal sac wall underwent histopathological and immunohistochemical examination. Fibrosis was assessed using Masson’s trichrome staining. The evaluation was performed semi-quantitatively, based on the following grading system: Grade 0, no fibrosis (ie, no collagen deposits); Grade 1, mild fibrosis, characterized by a focal fibrous network expansion of collagen, primarily in the perivascular areas; Grade 2, moderate fibrosis showing focal dense growth of collagen bands; and Grade 3, intensive fibrosis with diffuse, strong, and dense expansion of collagen bands in the stroma (Figure 5).
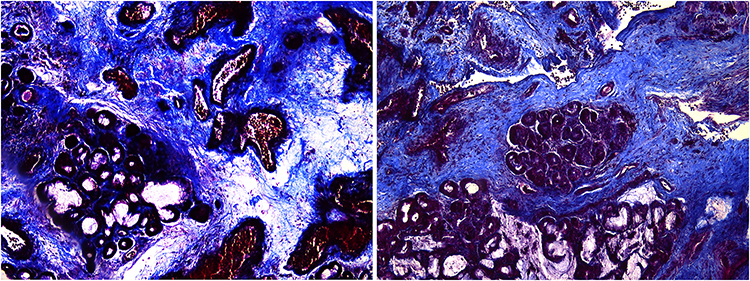 |
Figure 5 Left: Focal fibrosis - grade 1; right: strong, diffused fibrosis in all examined fields – grade 3; Masson’s trichrome staining, magn. 100x. |
Mononuclear cell subtypes were identified via immunohistochemistry using the following antibodies: anti-CD68 antibody (monoclonal mouse anti-human CD68/FITC clone KP1, DAKO Agilent, Santa Clara, CA, USA) for macrophages; anti-CD3 antibody (mouse monoclonal anti-CD3 concentrate clone F7.2.38, DAKO Omnis, Agilent) for T lymphocytes; and anti-CD20 antibody (monoclonal mouse clone L26, DAKO Omnis, Agilent) to detect B lymphocytes. The evaluation of infiltrates was based on the subsequent grading system: Grade 0, no infiltrates were observed; Grade 1, Infiltrating cells present in up to 10% of the field of view under the microscope (ie, single inflammatory cells); Grade 2, infiltrated cells present in up to 50% of the field of view (ie, focal infiltrate); and Grade 3, infiltrated cells in more than 50% of the field of view (ie, diffuse infiltrate).
The typical immunohistochemical staining images of patients from the study group are shown in Figures 6–8.
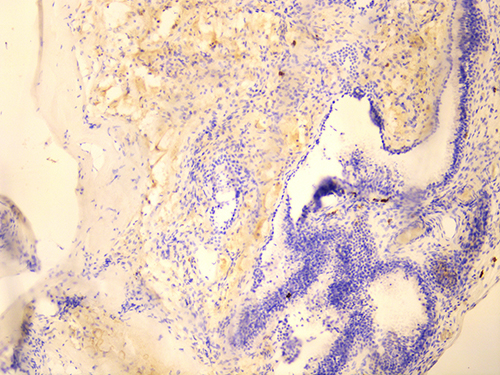 |
Figure 6 CD20 negative expression – grade 0; monoclonal mouse anti-CD20 antibody for B lymphocytes magn. 100x. |
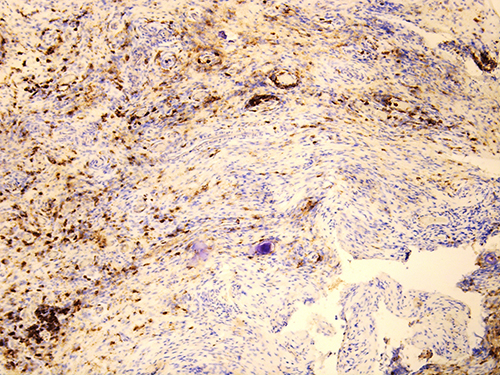 |
Figure 7 CD68 diffused expression – grade 2; monoclonal mouse anti-CD68 antibody for macrophages magn. 100x. |
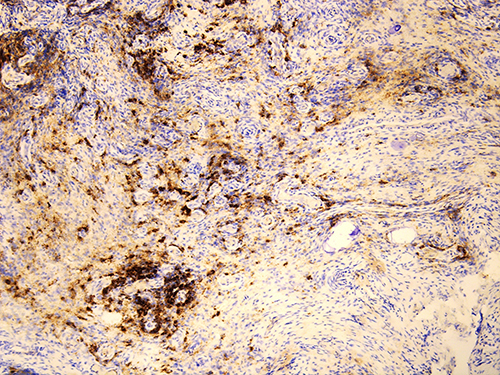 |
Figure 8 Strong diffused CD3 expression (aggregates of T lymphocytes) – grade 3; monoclonal mouse anti-CD3 antibody for T lymphocytes; magn. 100x. |
The patients were interviewed in detail regarding their medications, allergies, underlying health conditions, facial trauma, previous nasal or lacrimal surgery, or usage of a stent.
Statistical analysis was conducted using Statistica software, version 13.1 (IBM SPSS Inc., Armonk, NY, USA). The Mann–Whitney U-test was used to compare the levels of the studied traits between groups. Pearson’s chi-square test or Fisher’s exact test was used to test for between-group differences in categorical variables. The strength of the correlation between pairs of measurable parameters was determined using Spearman’s rank correlation coefficient. The significance of the correlation was evaluated using Student’s t-test. Statistical significance was set at p < 0.05.
Results
Based on the established criteria, complete recovery (ie, a score of 0 or 1 on the subjective VAS) and anatomical and functional patency (confirmed with irrigation and modified dye tests) were observed in 37 (78.7%) patients after at least 1 year of follow-up. In six (12.8%) patients, despite confirmation of patency via the irrigation test, insufficient reduction in the VAS score was achieved. In these patients, the appearance of the dye in the nose was delayed, and weakening of the dye outflow was observed. Patency was not confirmed by the irrigation test in four (8.5%) patients.
For statistical analysis, the patients were allocated into two groups: patients with complete cure [37 (78.7%) patients] and patients with partial resolution or no improvement [10 (21.3%) patients]. The results of the study are summarized in Table 1.
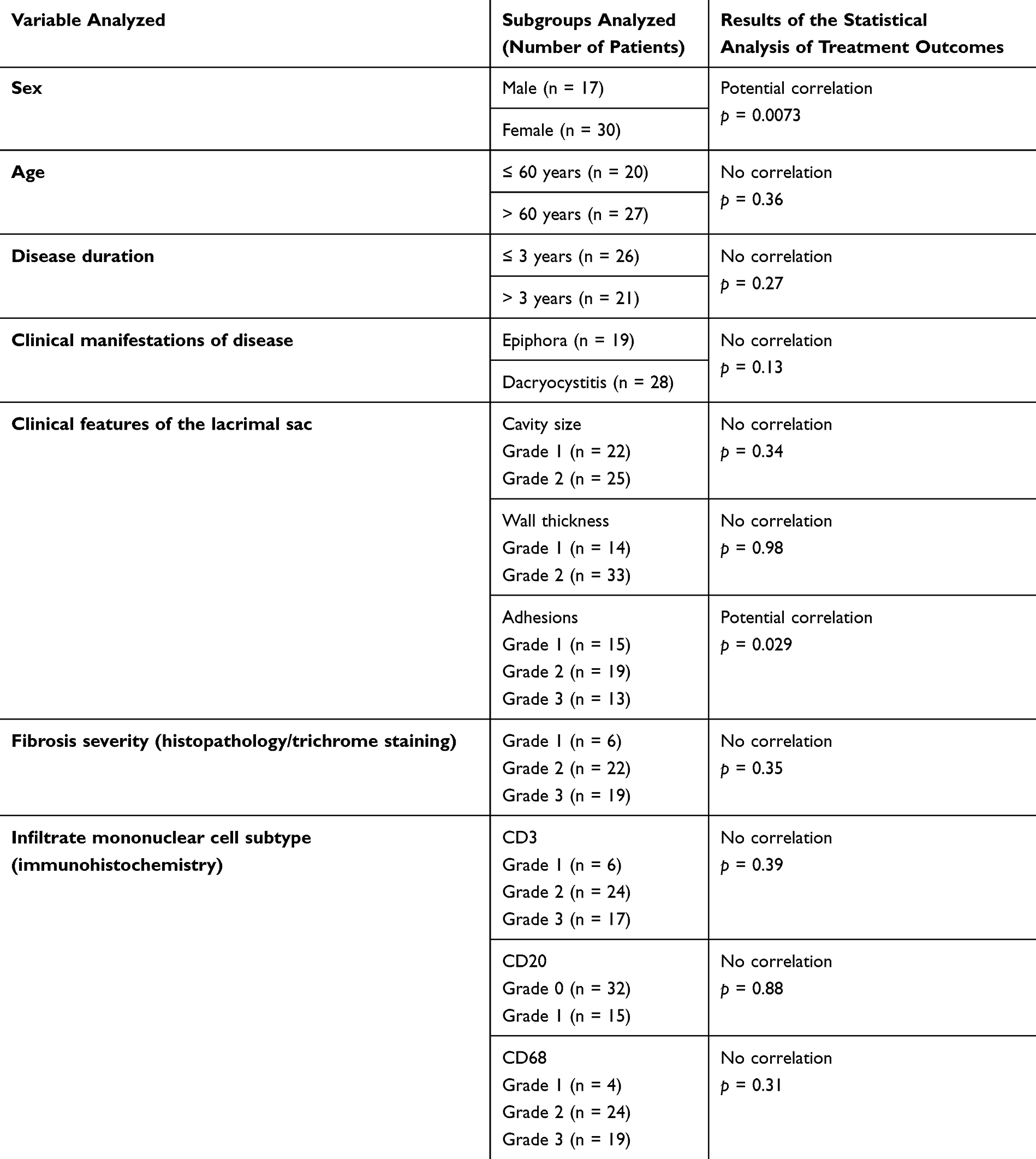 |
Table 1 Summary of Study Results |
Age of the Patients
Two groups of patients were analyzed: patients aged 60 years or younger (n = 20) and patients older than 60 years (n = 27). No significant differences existed in the treatment outcomes between the two age groups (Pearson’s chi-square test, p = 0.36).
Sex of the Patients
Analysis of the medical history data and clinical features of the groups, comprising 30 female and 17 male patients, revealed no statistically significant differences in terms of age, disease duration, type of complaints, or clinical and histopathological features of the lacrimal sac. However, in terms of treatment outcomes, all men who underwent surgery achieved a full recovery. By contrast, all treatment failures occurred in the female group (10 cases), indicating a statistically significant difference in treatment outcomes between men and women (Pearson’s chi-squared test, p = 0.007).
Duration of Disease
For analytical purposes, patients were categorized into two groups, based on the disease duration: up to 3 years (n = 26) and more than 3 years (n = 21). No statistically significant differences were found in the treatment outcomes between these groups (Pearson’s chi-square test, p = 0.27).
Clinical Manifestation of Disease (Epiphora and Presence of Dacryocystitis)
A comparative analysis of the treatment outcomes in patients with dacryocystitis (n = 28) and patients with persistent epiphora without infection (n = 19) revealed no statistically significant differences (Pearson’s chi-squared test, p = 0.13).
Lacrimal Sac Cavity Size
A comparative analysis of the treatment outcomes for patients with Grade 1 (ie, small) lacrimal sac cavities (n = 22) and patients with Grade 2 (ie, large) lacrimal sac cavities (n = 25) showed no statistically significant differences (Pearson’s chi-square test, p = 0.34).
Lacrimal Sac Wall Thickness
A comparative analysis of the treatment outcomes between patients with a Grade 1 (ie, thin) tear sac wall (n = 14) and patients with a Grade 2 (ie, thick) sac wall (n = 33) showed no statistically significant differences (Pearson’s chi-square test, p = 0.98).
Intraoperatively Observed Adhesions in the Lacrimal Sac
Analysis of the treatment outcomes among the three patient groups— patients with Grade 1 (n = 15), Grade 2 (n = 19), and Grade 3 (n = 13) adhesions observed intraoperatively—revealed a statistically significant association between adhesion severity and therapy outcomes (Pearson’s chi-square test, p = 0.029). All instances of anastomotic overgrowth occurred exclusively in the high adhesion group.
Fibrosis Assessed via Trichrome Staining
Analysis of the treatment outcomes in the three groups of patients, defined as Grade 1 (n = 6), Grade 2 (n = 22), and Grade 3 (n = 19) fibrosis severity, did not reveal a statistically significant relationship between fibrosis severity and the final therapy outcome (Pearson’s chi-square test, p = 0.35). However, improvement was observed in all patients with a single fibrotic focus (ie, Grade 1).
Cellular Infiltrates—T Lymphocytes
Analysis of the treatment outcomes in the three groups of patients with varying CD3 protein expression with Grade 1 (n = 6), Grade 2 (n = 24), and Grade 3 (n = 17) T-lymphocyte cell infiltration revealed no statistically significant relationship between the severity of infiltration and the treatment outcomes (Pearson’s chi-square test, p = 0.39). All patients who showed no improvement after surgical treatment had moderate (ie, Grade 2) to intense (ie, Grade 3) T-cell infiltration.
Cellular Infiltrates—B Lymphocytes
We analyzed two groups of patients with varying levels of CD20 protein expression in the samples studied: no expression (Grade 0; n = 32) and low expression (Grade 1; ≤ 10% of cells; n = 15). No significant differences were found between the groups (Pearson’s chi-square test, p = 0.88).
Cellular infiltrates—macrophages
Three groups of patients were analyzed, based on the different CD68 protein expression levels in the specimens studied: Grade 1 (n = 4), Grade 2 (n = 24), and Grade 3 (n = 19). No significant differences were observed in the final treatment effect relative to CD68 expression (Pearson’s chi-squared test, p = 0.31).
Discussion
The diversity of surgical techniques, instruments, medications, and postoperative management utilized in dacryocystorhinostomy highlights the ongoing need for an optimal approach for mitigating postoperative scarring and tear duct restenosis.
Most publications analyzing the causes of endoscopic DCR failure focus on surgical technique errors. Restenosis is attributed to factors such as an improperly sized or positioned osteotomy, excessive mucosal resection, insufficient lacrimal sac opening and postoperative sump syndrome. Additionally, uncorrected anatomical variants like septal deviations, middle turbinate abnormalities, or intervening ethmoids are cited as contributing factors (20,8,7,3,19,21). Common canalicular adhesions are also considered a negative prognostic factor (22,8, 7).
These issues lead to adhesions and scarring at the surgical site, directly causing procedure failure. Despite extensive literature exploring various surgical methods, the histopathological factors predisposing individuals to postoperative scarring and fibrosis remain poorly studied (Table 2).
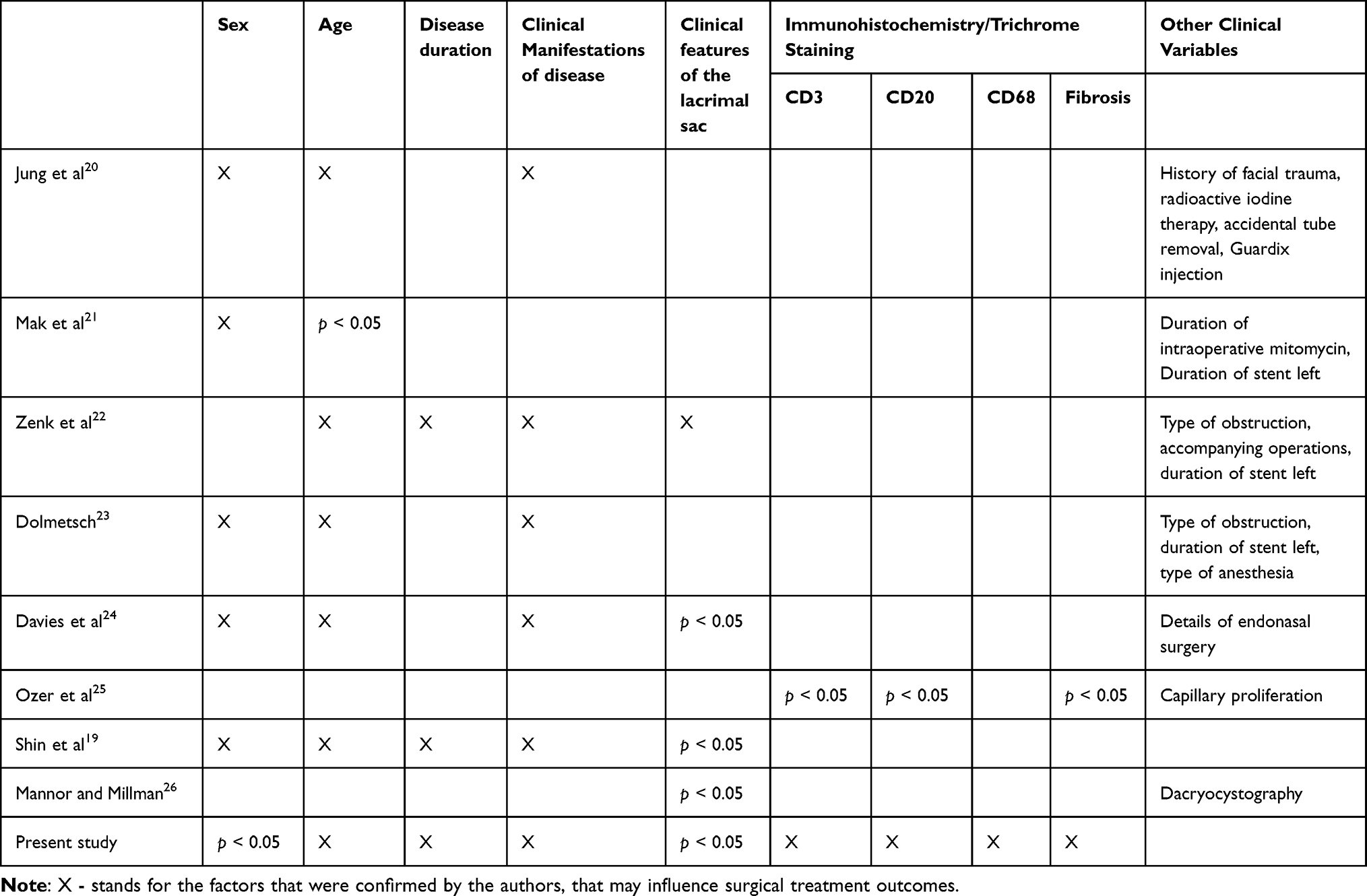 |
Table 2 Factors That May Influence Surgical Treatment Outcomes as Analyzed in Previous Studies |
In our study, the analysis of factors potentially associated with scarring revealed that only the presence of adhesions detected during surgery and patients’ sex were correlated with surgical outcomes.
Treatment results were evaluated after a minimum of 1 year of follow-up, which is reasonable, given that the process of scarring and restenosis typically manifests within the first year postoperatively, with an average onset occurring as early as to 3–5 months postoperation.21,27,28 The significantly better surgical outcomes observed in men than in women in our study (Pearson’s chi-square test, p = 0.007) merit a separate analysis. While Pearson’s test indicated a statistically significant association between treatment outcomes and patient gender, caution is advised when interpreting gender as a potential risk factor for recurrent stenosis of nasolacrimal anastomosis. The small sample size, skewed male-to-female ratio, low number of operational failures and the lack of analysis on unfavorable anatomical variants in the surgical area in our study make such a conclusion speculative.
Nonetheless, our findings align with other studies where the majority of surgical failures occurred in women. For instance, McMurray et al29 reported an 85% rate of restenosis in female patients, Go et al30 − 76% and Dave et al8 − 66%. However, it is important to acknowledge that some studies have either not supported an association between surgical outcomes and gender or have not examined this factor.20,21,24 The disparity between men and women observed in some studies may be attributed to inherent differences in tear duct patency between the sexes. Women are predisposed to impaired tear duct patency due to hormonal and immunological changes, leading to de-epithelization, epithelial desquamation, and subsequent obstruction of the anatomically narrower lacrimal ducts.31,32 Epidemiological studies have demonstrated a higher prevalence of tear duct obstruction in women, and in the literature on the surgical treatment of lacrimal duct obstruction, women constitute the majority of patients undergoing surgery.
In addition to sex, the presence of intense adhesions and scar tissue identified during surgery were the only factors that significantly affected the final surgical outcome. Previous studies have reported fibrosis and scar tissue formation in cases of reoperated stenotic anastomoses,4–6,9 suggesting that persistent scarring and fibrosis within the lacrimal sac tissues before surgery may continue postoperatively, leading to anastomotic overgrowth. However, our study did not statistically confirm the influence of other clinical factors that, according to the literature review, could be associated with fibrosis. These factors included patient age, disease duration, complaint type, wall thickness, and sac cavity size.
Previous research has found that the amount and activity of fibroblasts decrease with age, leading to a reduction in the production of elements involved in fibrosis and its dynamics.21,33 One may consequently anticipate better surgical outcomes in older patients. Nevertheless, consistent with our findings, studies by Zenk et al22 and Dolmetsch23 failed to establish a statistically significant relationship between patient age and surgical outcomes.
Some authors34 have suggested that a prolonged inflammatory process leads to a transition from granulation to scarring, characterized by wall thickening and a reduction in the lacrimal sac cavity dimension, which is considered to be a negative prognostic factor. However, this association was not observed in this study.
Other investigators have proposed that a worse treatment outcomes in these cases are not solely attributable to the scarring process, but also to the surgical challenges associated with mobilizing mucosal flaps formed from thickened sac walls.24,35 Furthermore, histopathological studies36 using animal models have revealed that similar clinical presentations of the disease can coexist with varying stages of inflammation and with markedly different histopathological appearances.
Studies investigating whether and how particular subpopulations of inflammatory infiltrating cells affect surgical outcomes have been rare and the conclusions drawn from the analyses of existing studies are inconclusive. Some studies, such as those by Knop et al37 and Ali et al,38 have reported a clear predominance of B lymphocytes and a limited number of macrophages in inflammatory infiltrates. In contrast, other studies have suggested that different lymphocyte subpopulations are predominant in lacrimal sac samples. For instance, Ozer et al25 and Yang et al39 reported this phenomenon.
Although Ozer et al,25 Davies et al,24 and Shin et al19 proposed that lymphocytic infiltration may contribute to lacrimal sac wall thickening, which is a negative prognostic factor in dacryocystorhinostomy. A study by Knop et al,37 which evaluated lacrimal sac biopsies obtained from healthy individuals at autopsy, also demonstrated a predominance of T lymphocytes. In the current study, T lymphocytes were the predominant group of inflammatory cells, outnumbering B lymphocytes. B lymphocyte infiltration was remarkably undetectable in 68% of cases. However, despite this observation, we did not establish a statistically significant association between the T-lymphocyte infiltration severity and treatment outcomes. Nonetheless, a discernible trend appeared that warrants further investigation in larger study groups: notably, none of the patients who showed improvement after surgical treatment exhibited moderate-to-intense T-lymphocyte infiltration. The relatively intense T-lymphocyte infiltration observed in our study group can explain the higher severity of macrophage infiltration, compared with that of previous studies by Knop et al37 and Ali et al38 This finding may be attributed to the activating effect of the Th1 subpopulation on macrophage migration.39 Additionally, the high number of patients with abscesses and recurrent suppurative conditions may have contributed to the greater severity of macrophage infiltration in our study, compared with that of the cited studies. However, despite these observations, the severity of these infiltrates did not significantly influence surgical outcomes. The presence of various inflammatory cells and their subpopulations, along with the complex inflammatory cascades leading to fibrosis, pose challenges in identifying the exact causes of scarring and closure of the newly formed nasolacrimal junction. Moreover, the reversibility of many of these processes adds further complexity to the identification of underlying mechanisms.
The discovery of fibrous and scar tissue at the anastomotic site post-surgery, as highlighted in previous publications4–6,9 may stem from the surgical injury itself, as suggested by Ciftci et al40 However, only few researchers have addressed the problem of whether the severity of fibrosis in the sac wall sections affects surgical outcomes. Mannor and Millman26 suggest that fibrosis and scarring resulting from ongoing prolonged inflammation of the lacrimal sac significantly diminishes the potential success of surgery. Onerci et al35 and Lee-Wing and Ashenhurst41 similarly cited fibrosis as a cause of EDCR failure. Ozer and et al25 found severe fibrosis in 66% of the patients after unsuccessful surgeries; however, they did not confirm a statistically significant relationship in their study. Our study similarly did not establish a statistical relationship between fibrosis, as assessed with trichrome staining, and postoperative outcomes. Nevertheless, among patients with minimal fibrosis (Grade 1), the resolution of complaints was attained in all patients. In contrast, 75% of patients with postoperative failure exhibited diffuse fibrosis.
This study has a few limitations. First, it is a retrospective analysis of surgical treatment outcomes. However, the study included all eligible patients treated with DCR at our department, reducing the risk of selection bias. Second, it was a single-center study with a small cohort, especially considering the number of variables analyzed, which may limit the interpretation of our findings.
Nonetheless, certain trends were observed in this group of patients, despite the absence of clear statistical significance. The presence of these trends, particularly those seen in our immunohistochemical and histopathological studies, should be investigated in a larger cohort, as they may underlie the pathomechanism of restenosis development. Therefore, we believe that the conclusions of the study are valid.
Conclusion
Our study findings suggest that, among various epidemiological data, clinical features of inflammation, intraoperative macroscopic changes in the lacrimal sac, and histological and immunohistochemical evaluation of inflammatory infiltrates, only the presence of adhesions in the lacrimal sac can be considered a risk factor for restenosis following EDCR procedures. Thus, when intense lacrimal sac adhesions are identified during surgery, measures aimed at minimizing the risk of restenosis, such as the use of mitomycin, stents, modification of the surgical technique with mucosal flap edge approximation, or more vigilant postoperative care, should be considered.
Histological and immunohistochemical studies did not reveal a correlation of fibrosis, and the type and severity of cellular infiltration with treatment outcomes. However, if the patient cohort were larger, fibrosis and T-cell lymphocytic infiltration could potentially have a negative prognostic value. Nevertheless, as the direct mechanisms leading to fibrosis and scarring of the created anastomosis remain elusive, further research is warranted. Multicenter studies using the same research methods and discriminant analysis would allow for a more precise assessment of groups of risk factors that may negatively impact surgical treatment outcomes.
The poorer treatment outcomes observed in women compared to men in our study, as well as in other investigations, may be attributed to the anatomical and physiological characteristics of the female lacrimal drainage system, which predispose them to stenosis. This hypothesis warrants further investigation in a larger patient cohort.
Data Sharing Statement
All materials and information are available upon an e-mail request on corresponding author.
Disclosure
No author has a financial or proprietary interest in any material or method mentioned.
References
1. Mandal R, Banerjee AR, Biswas MC, Mondal A, Kundu PK, Sasmal NK. Clinicobacteriological study of chronic dacryocystitis in adults. J Indian Med Assoc. 2008;106(5):296–298.
2. Rajabi MT, Shahraki K, Nozare A, et al. External versus endoscopic dacryocystorhinostomy for primary acquired nasolacrimal duct obstruction. Middle East Afr J Ophthalmol. 2022;29(1):1–6. doi:10.4103/meajo.meajo_238_21
3. Welham RA, Wulc AE. Management of unsuccessful lacrimal surgery. Br J Ophthalmol. 1987;71(2):152–157. doi:10.1136/bjo.71.2.152
4. Tucker N, Chow D, Stockl F, Codère F, Burnier M. Clinically suspected primary acquired nasolacrimal duct obstruction: clinicopathologic review of 150 patients. Ophthalmology. 1997;104(11):1882–1886. doi:10.1016/S0161-6420(97)30012-8
5. Bernardini FP, Moin M, Kersten RC, Reeves D, Kulwin DR. Routine histopathologic evaluation of the lacrimal sac during dacryocystorhinostomy: how useful is it? Ophthalmology. 2002;109(7):1214–1217. doi:10.1016/S0161-6420(02)01082-5
6. Anderson NG, Wojno TH, Grossniklaus HE. Clinicopathologic findings from lacrimal sac biopsy specimens obtained during dacryocystorhinostomy. Ophthalmic Plast Reconstr Surg. 2003;19(3):173–176. doi:10.1097/01.IOP.0000066646.59045.5A
7. Narioka J, Ohashi Y. Transcanalicular-endonasal semiconductor diode laser-assisted revision surgery for failed external dacryocystorhinostomy. Am J Ophthalmol. 2008;146(1):60–68. doi:10.1016/j.ajo.2008.02.028
8. Dave TV, Mohammed FA, Ali MJ, Naik MN. Etiologic analysis of 100 anatomically failed dacryocystorhinostomies. Clin Ophthalmol. 2016;10:1419–1422. doi:10.2147/OPTH.S113733
9. Salour H, Hatami MM, Parvin M, et al. Clinicopathological study of lacrimal sac specimens obtained during DCR. Orbit. 2010;29(5):250–253. doi:10.3109/01676830.2010.485720
10. Green R, Gohil R, Ross P. Mucosal and lacrimal flaps for endonasal dacryocystorhinostomy: a systematic review. Clin Otolaryngol. 2017;42(3):514–520. doi:10.1111/coa.12754
11. Vinciguerra A, Nonis A, Giordano Resti A, Bussi M, Trimarchi M. Best treatments available for distal acquired lacrimal obstruction: a systematic review and meta-analysis. Clin Otolaryngol. 2020;45(4):545–557. doi:10.1111/coa.13551
12. Vinciguerra A, Nonis A, Resti AG, Bussi M, Trimarchi M. Impact of post-surgical therapies on endoscopic and external dacryocystorhinostomy: systematic review and meta-analysis. Am J Rhinol Allergy. 2020;34(6):846–856. doi:10.1177/1945892420945218
13. Ali MJ, Psaltis AJ, Murphy J, Wormald PJ. Powered endoscopic dacryocystorhinostomy: a decade of experience. Ophthalmic Plast Reconstr Surg. 2015;31(3):219–221. doi:10.1097/IOP.0000000000000261
14. Cheng SM, Feng YF, Xu L, Li Y, Huang JH. Efficacy of mitomycin C in endoscopic dacryocystorhinostomy: a systematic review and meta-analysis. PLoS One. 2013;8(5):e62737. doi:10.1371/journal.pone.0062737
15. Yim M, Wormald PJ, Doucet M, et al. Adjunctive techniques to dacryocystorhinostomy: an evidence-based review with recommendations. Int Forum Allergy Rhinol. 2021;11(5):885–893. doi:10.1002/alr.22699
16. Chen I, Ayalon H, Drabkin E, Cohen O, Peleg U. Introduction of steroid absorbed Spongostan in endoscopic dacryocystorhinostomy improves success rates. Ophthalmic Plast Reconstr Surg. 2022;38(5):444–447. doi:10.1097/IOP.0000000000002156
17. Orsolini MJ, Schellini SA, Souza Meneguim RLF, Catâneo AJM. Success of endoscopic dacryocystorhinostomy with or without stents: systematic review and meta-analysis. Orbit. 2020;39(4):258–265. doi:10.1080/01676830.2019.1677726
18. Tsirbas A, Wormald PJ. Endonasal dacryocystorhinostomy with mucosal flaps. Am J Ophthalmol. 2003;135(1):76–83. doi:10.1016/S0002-9394(02)01830-5
19. Shin HJ, Woo KI, Kim YD. Factors associated with rhinostomy shape after endoscopic dacryocystorhinostomy. Clin Otolaryngol. 2017;42(3):550–556. doi:10.1111/coa.12767
20. Jung SK, Kim YC, Cho WK, Paik JS, Yang SW. Surgical outcomes of endoscopic dacryocystorhinostomy: analysis of 1083 consecutive cases. Can J Ophthalmol. 2015;50(6):466–470. doi:10.1016/j.jcjo.2015.08.007
21. Mak ST, Io IY, Wong AC. Prognostic factors for outcome of endoscopic dacryocystorhinostomy in patients with primary acquired nasolacrimal duct obstruction. Graefes Arch Clin Exp Ophthalmol. 2013;251(5):1361–1367. doi:10.1007/s00417-012-2228-9
22. Zenk J, Karatzanis AD, Psychogios G, et al. Long-term results of endonasal dacryocystorhinostomy. Eur Arch Otorhinolaryngol. 2009;266(11):1733–1738. doi:10.1007/s00405-009-1000-1
23. Dolmetsch AM. Nonlaser endoscopic endonasal dacryocystorhinostomy with adjunctive mitomycin C in nasolacrimal duct obstruction in adults. Ophthalmology. 2010;117(5):1037–1040. doi:10.1016/j.ophtha.2009.09.028
24. Davies MJ, Lee S, Lemke S, Ghabrial R. Predictors of anatomical patency following primary endonasal dacryocystorhinostomy: a pilot study. Orbit. 2011;30(1):49–53. doi:10.3109/01676830.2010.516468
25. Ozer O, Eskiizmir G, Unlü H, Işisağ A, Aslan A. Chronic inflammation: a poor prognostic factor for endoscopic dacryocystorhinostomy. Eur Arch Otorhinolaryngol. 2012;269(3):839–845. doi:10.1007/s00405-011-1728-2
26. Mannor GE, Millman AL. The prognostic value of preoperative dacryocystography in endoscopic intranasal dacryocystorhinostomy. Am J Ophthalmol. 1992;113(2):134–137. doi:10.1016/S0002-9394(14)71524-7
27. McLachlan DL, Shannon GM, Flanagan JC. Results of dacryocystorhinostomy: analysis of the reoperations. Ophthalmic Surg. 1980;11(7):427–430.
28. Lee E, Yuen H, Javed Ali M. Revising a failed dacryocystorhinostomy. In: Javed Ali M, editor. Principles Pract Lacrimal Surg. New Delhi: Springer; 2015: 245–256.
29. McMurray CJ, McNab AA, Selva D. Late failure of dacryocystorhinostomy. Ophthalmic Plast Reconstr Surg. 2011;27(2):99–101. doi:10.1097/IOP.0b013e3181d35267
30. Go Y, Park J, Kim K, Lee S. Comparison of nonlaser endoscopic endonasal revision surgery and diode laser transcanalicular revision surgery for failed dacryocystorhinostomy. J Craniofac Surg. 2015;26(3):863–866. doi:10.1097/SCS.0000000000001272
31. Mills DM, Meyer DR. Acquired nasolacrimal duct obstruction. Otolaryngol Clin North Am. 2006;39(5):979–999. doi:10.1016/j.otc.2006.07.002
32. Shigeta KI, Takegoshi H, Kikuchi S. Sex and age differences in the bony nasolacrimal canal: an anatomical study. Arch Ophthalmol. 2007;125(12):1677–1681. doi:10.1001/archopht.125.12.1677
33. Sato K, Hirano M, Nakashima T. Age-related changes of collagenous fibers in the human vocal fold mucosa. Ann Otol Rhinol Laryngol. 2002;111(1):15–20. doi:10.1177/000348940211100103
34. Thakur S. An observation on pathological changes of lacrimal sac in chronic dacryocystitis. Indian J Ophthalmol. 1985;33(4):251–253.
35. Onerci M, Orhan M, Ogretmenoğlu O, Irkeç M. Long-term results and reasons for failure of intranasal endoscopic dacryocystorhinostomy. Acta Otolaryngol. 2000;120(2):319–322. doi:10.1080/000164800750001170
36. Liu R, Li H, Ai T, Hu W, Luo B, Xiang N. Pathological changes of the nasolacrimal duct in rabbit models of chronic dacryocystitis: correlation with lacrimal endoscopic findings. Graefes Arch Clin Exp Ophthalmol. 2018;256(11):2103–2112. doi:10.1007/s00417-018-4129-z
37. Knop E, Knop N. Lacrimal drainage-associated lymphoid tissue (LDALT): a part of the human mucosal immune system. Invest Ophthalmol Vis Sci. 2001;42(3):566–574.
38. Ali MJ, Mulay K, Pujari A, Naik MN. Derangements of lacrimal drainage-associated lymphoid tissue (LDALT) in human chronic dacryocystitis. Ocul Immunol Inflamm. 2013;21(6):417–423. doi:10.3109/09273948.2013.797473
39. Yang X, Wang L, Li L, Yu Z, Xiao C. The imbalance of lymphocyte subsets and cytokines: potential immunologic insights into the pathogenesis of chronic dacryocystitis. Invest Ophthalmol Vis Sci. 2018;59(5):1802–1809. doi:10.1167/iovs.17-23660
40. Ciftci F, Erşanli D, Civelek L, Baloglu H, Karadayi K, Güngör A. Histopathologic changes in the lacrimal sac of dacryocystorhinostomy patients with and without silicone intubation. Ophthalmic Plast Reconstr Surg. 2005;21(1):59–64. doi:10.1097/01.IOP.0000148408.51615.FE
41. Lee-Wing MW, Ashenhurst ME. Clinicopathologic analysis of 166 patients with primary acquired nasolacrimal duct obstruction. Ophthalmology. 2001;108(11):2038–2040. doi:10.1016/S0161-6420(01)00783-7
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.