Back to Journals » Patient Preference and Adherence » Volume 20
Factors Influencing Adherence to Home-Based Exercise Rehabilitation in Stroke Patients from a Temporal Perspective: An Explanatory Sequential Mixed-Methods Study
Authors Shao J ![]() , Cong S, Han Y, Xu W, Wang Q, Zhang J, Wei X, Ren R
, Cong S, Han Y, Xu W, Wang Q, Zhang J, Wei X, Ren R
Received 17 November 2025
Accepted for publication 30 January 2026
Published 13 February 2026 Volume 2026:20 582280
DOI https://doi.org/10.2147/PPA.S582280
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jianing Shao,1,2,* Sunling Cong,3,* Yuxin Han,1,2 Wenjin Xu,1 Qing Wang,4 Jiachen Zhang,3 Xiaoxiao Wei,1,2 Rui Ren1,2
1Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2School of Nursing, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 3School of Medicine, Jiangsu University, Zhenjiang, Jiangsu, People’s Republic of China; 4Department of Nursing, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qing Wang, Department of Nursing, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: This study aimed to examine the factors influencing the adherence of stroke patients to home-based exercise rehabilitation and to elucidate the potential driving mechanisms of temporal perspective on rehabilitation adherence.
Patients and Methods: This study employed a sequential, explanatory, and mixed-methods design. In the quantitative phase, a questionnaire survey was conducted among 289 stroke patients from January 2025 to May 2025 using convenience sampling. In the qualitative phase, 16 stroke patients were selected from the quantitative sample through purposive and maximum variation sampling to explain and supplement the quantitative findings using semi-structured interviews.
Results: Quantitative analysis demonstrated a significant positive correlation between temporal perspective and rehabilitation adherence, with rehabilitation intention partially mediating this relationship. Behavioral advantage exerted a negative moderating effect on the intention–adherence pathway, whereas the moderating effect of self-regulation ability did not reach statistical significance. Qualitative analysis identified four main themes: consistency belief, time-bound potency, behavioral advantage, and self-regulation ability.
Conclusion: Temporal perspective is an important driver of adherence to home-based rehabilitation among stroke patients. As rehabilitation habits develop, behavioral patterns gradually shift from being “intention-driven” to becoming “automatic habits”, thereby weakening the direct driving effect of intention. Given the potential presence of latent executive dysfunction in stroke patients, targeted assessment tools and intervention strategies should be developed to bridge the gap between intention and behavior.
Keywords: temporal perspective, intention, behavioral advantage, self-regulation ability, quantitative study, qualitative study
A Letter to the Editor has been published for this article.
Introduction
Stroke has become a major global public health problem. Approximately 80% of stroke survivors experience varying degrees of motor dysfunction, which substantially increases the caregiving burden on families and society.1 The World Stroke Organization has identified rehabilitation as one of the key practical strategies to reduce the global burden of stroke, with exercise rehabilitation playing a central role in improving limb function and promoting overall functional recovery.2,3 Due to limited rehabilitation resources, more than 50% of stroke patients return home for rehabilitation following hospitalization or outpatient treatment.4 Home-based rehabilitation is a reliable alternative to institutional rehabilitation, offering benefits such as improved physical function and quality of life; however, the realization of these benefits largely depends on patients’ long-term adherence to exercise programs.5
Although many stroke survivors clearly express a willingness to participate in rehabilitation, a substantial proportion fail to maintain home-based exercise rehabilitation over time. Survey data indicate that 63–82% of patients demonstrate good adherence during hospitalization, whereas only 17.3–65.3% adhere to home exercise programs after discharge.6,7 In China, Lin et al conducted community-based surveys on adherence to functional exercise among stroke patients in 2012 and 2021.8,9 The results showed adherence rates of 61.98% and 62.00%, respectively, suggesting that adherence among stroke patients in China has not substantially improved over the past decade. This phenomenon highlights a critical clinical issue: although most patients recognize the importance of rehabilitation and possess rehabilitation intentions, these intentions are frequently not translated into sustained adherence behavior.
Behavior change theories explain the initiation, modification, and maintenance of health behaviors from psychological and behavioral perspectives. Currently, the theory of planned behavior and the health action process approach have been widely applied to explain and predict exercise adherence among stroke patients, both emphasizing behavioral intention as the most direct predictor of future behavior.10 However, although rehabilitation intention is a prerequisite for behavior change, it is often insufficient to ensure the actual occurrence of behavior. A meta-analysis11 revealed a significant “intention–behavior” gap in exercise behavior, indicating that intention alone fails to explain approximately 47.6% of behavioral variance. This suggests that exercise intention alone is insufficient to ensure adherence to home-based rehabilitation, particularly in long-term, self-managed home rehabilitation settings.
To address the “intention–behavior” gap, temporal self-regulation theory (TST) provides a robust theoretical framework. TST posits that behavior is not driven solely by intention but is also directly influenced or moderated by behavioral advantage (ie, habit intensity) and self-regulation ability (ie, executive function).12 When behaviors become habitual, or individuals possess strong self-regulation abilities, intentions are more likely to be translated into action. Behavioral advantage reflects the degree of behavioral automatization, referring to unconscious habitual behaviors, commonly conceptualized as habit strength. When habit strength is high, the predictive power of intention on behavior may be weakened. Self-regulation ability, on the other hand, represents a key executive function that enables individuals to inhibit impulses and maintain goal-directed behavior. Individuals with stronger self-regulation abilities are better able to strengthen the intention–behavior link and facilitate the transformation of intention into action. In addition, TST emphasizes temporal perspective as a pre-determinant of intention formation, highlighting the central role of individuals’ evaluations of delayed benefits relative to immediate costs in determining whether intentions are translated into action. Following a stroke, patients often experience a sudden disruption in their life trajectory, which may alter their subjective evaluation of delayed rehabilitation benefits compared with immediate costs. From this perspective, adherence to home-based exercise rehabilitation is not only a motivational issue but also depends on how patients perceive the future and regulate their behavior over time. Therefore, integrating temporal perspective with behavioral advantage and self-regulation mechanisms may provide a novel explanatory pathway for understanding the intention–behavior gap in stroke patients. Based on this theoretical framework, this study proposed the following hypotheses: (1) home-based exercise rehabilitation intention mediates the relationship between temporal perspective and rehabilitation adherence; and (2) the mediating effect of temporal perspective on adherence through rehabilitation intention is moderated by behavioral advantage and self-regulation ability.
Although previous studies have explored the influence of temporal perspective on adherence to home-based exercise rehabilitation among stroke patients, they may not have fully elucidated the underlying mechanisms. Specifically, using quantitative or qualitative methods alone may be insufficient to thoroughly examine the internal components of temporal perspective and their impact on exercise adherence. Therefore, guided by theory-driven hypotheses, this study adopted an explanatory sequential mixed-methods design. Quantitative methods were used to examine the pathways through which temporal perspective, behavioral advantage, and self-regulation ability influence adherence to home-based exercise rehabilitation. In contrast, qualitative methods were employed to further elucidate the underlying mechanisms of key variables, with particular emphasis on clarifying the disconnection between intention and behavior.
Materials and Methods
Study Design
This study employed an explanatory sequential mixed-methods design.13 In this approach, quantitative research is first conducted to test theoretical assumptions and identify relationships among key variables. Qualitative interviews are then carried out based on the quantitative findings to explain, supplement, and deepen the interpretation of the quantitative results.
Study Setting and Recruitment
In the quantitative phase, stroke patients who were referred to the neurology clinic of a class III Grade A general hospital in Nanjing from January 2025 to May 2025 were recruited as study participants. Inclusion criteria were as follows: ① age ≥18 years, <80 years; ② diagnosis meeting the “key points for the diagnosis of major cerebrovascular diseases in China (2019)”14 confirmed by head CT and MRI; ③ stroke duration longer than 1 month; ④ stable vital signs with the ability to understand and cooperate; ⑤ history of motor dysfunction (Modified Rankin Scale ≥2); ⑥ prior experience with home-based exercise rehabilitation. Exclusion criteria were as follows: ① severe heart, liver, lung, or other organ failure, malignant tumors, or receipt of palliative treatment;② Patients with consciousness or mental disorders and severe cognitive impairment. After strict screening, 289 patients were included in this study.
In the qualitative research, purposive sampling and maximum variation sampling were used to recruit interview participants from those who completed the quantitative research. To enhance sample representativeness, extreme case sampling was adopted, with particular emphasis on patients who reported high rehabilitation intention but low adherence scores during the quantitative phase. According to Bertaux,15 a minimum of 15 participants is recommended to ensure data adequacy in qualitative research. In practice, data collection was discontinued once thematic saturation was achieved, defined as the point at which no new information or themes emerged from additional interviews.16 Based on this principle, 16 patients were ultimately included in this study.
Study Instruments
Quantitative Research
Data were collected using the general characteristics scale, the consideration of future consequence scale, the exercise intention scale, the self-report habit index scale, the brief self-control scale, and the exercise adherence scale.
General Characteristics Scale
This scale was designed by researchers based on relevant literature. This scale includes general demographic information such as gender, age, educational level, marital status, and average monthly household income and information related to stroke, including stroke type, frequency of attacks, duration of onset (time since the last onset), self-care ability (activities of daily living), comorbidities, and other disease-related factors.
Consideration of Future Consequences Scale
This scale measures the extent to which stroke patients consider future outcomes in their decision-making processes, thereby reflecting their temporal perspective. It was adapted by Strathman et al17 in 1994; the scale consists of two dimensions—considering the present and the future consequences—with a total of 12 items. Each item is rated on a 7-point Likert scale (1 = completely disagree, 7 = completely agree), with higher scores indicating greater consideration of future consequences. The reported Cronbach’s α for this scale ranges from 0.71 to 0.91.
Exercise Intention Scale
The exercise intention scale was developed by Ajzen,18 and subsequently translated and revised by Fang.19 This scale was used to assess stroke patients’ behavioral intention to perform home-based exercise rehabilitation (eg, “I will consider/try/plan to exercise at home in the next month”). Each item was rated on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree”, with higher scoresindicating stronger exercise intention. The Cronbach’s α coefficient for this scale in this study was 0.938.
The Self-Report Habit Index Scale
Evaluate the intensity of home exercise habits in stroke patients.20 Each item is rated on a Likert scale from 1 (completely disagree) to 7 (completely agree). SRHI consists of a stem (behavior X is something) and includes 12 items that evaluate various aspects of habits. This study describes X behavior as exercise behavior. The Cronbach’s α coefficient of this scale is 0.961.
Brief Self-Control Scale
The BSCS was used to assess self-regulation ability during exercise rehabilitation. Revised by Morean et al21 in 2014, the scale includes two dimensions—self-discipline and self-control—and consists of seven items. Items 2, 4, 6, and 7 are reverse-scored. Each item is rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree), with higher scores indicating higher levels of self-control. The Chinese version of the scale, introduced and validated by Luo et al22 demonstrated good reliability (Cronbach’s α = 0.83).
Questionnaire of Exercise Adherence
This scale, developed by Lin et al9 in 2013, was used to assess adherence to exercise rehabilitation. The scale includes 14 items across three dimensions—physical participation in exercise, monitoring of exercise effects, and proactive seeking of exercise-related advice. Each item is scored on a 4-point Likert scale (1 = not at all, 4 = completely achieved), yielding a total score range of 14–56 points. The adherence index is calculated as the percentage of the participant’s total score relative to the highest score on the scale (56 points). Adherence indices are categorized as follows: low (<50–75%), moderate (50–75%), or high (>75%). The Cronbach’s α coefficient for this scale was 0.923.
Qualitative Research
Qualitative data were collected using a semi-structured interview guide developed based on the quantitative findings.
Semi-Structured Interview Guide
Following a systematic literature review and clarification of the research objectives, the research team designed interview questions guided by two core aims: first, explore factors influencing adherence to home-based exercise rehabilitation among stroke patients, and second, to investigate the mechanisms through which temporal perspective affects adherence. After drafting the initial draft, two rounds of optimization were conducted. First, pilot interviews were conducted with at least two participants, and questions were revised based on feedback. Subsequently, neurology experts evaluated the scientific validity of theentries from a professional perspective, resulting in a finalized interview guide (Figure 1).
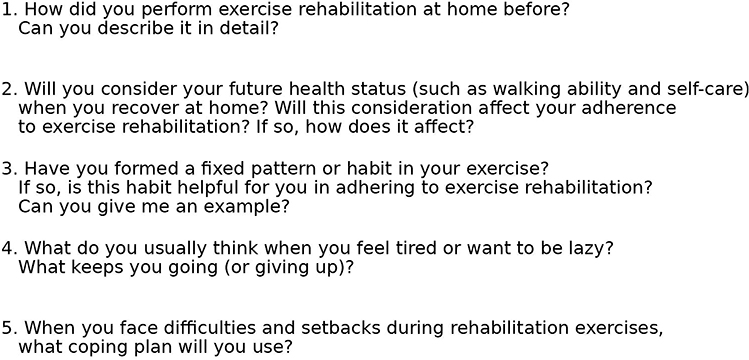 |
Figure 1 Semi-Structured Interview Outline. |
Data Collection
For the quantitative phase, all investigators received standardized training, including research objectives, inclusion and exclusion criteria, effective communication skills, and detailed explanations of research concepts. Before the survey, the investigator explained the study purpose, significance, participation precautions, and confidentiality principles to participants. Written informed consent was obtained from all participants. Paper-based questionnaires were issued face-to-face in a quiet and private outpatient room to minimize environmental noise and interference. Investigators provided clarification when participants had questions during the completion process. For older participants or those with lower education who were unable to complete the questionnaire independently, investigators read each item aloud and recorded responses based on participants’ understanding and choices. Completed questionnaires were checked on the site, and any missing or ambiguous responses were clarified immediately with the participants.
In the qualitative phase, face-to-face interviews were conducted with participants who had completed the quantitative research. Interviews were scheduled in advance and conducted in a quiet, spacious doctor–patient communication room after participants’ clinical appointments, with family members permitted to be present if desired. Prior to the interview, the interviewer explained the study’s purpose and obtained consent to record audio. During interviews, attention was paid to nonverbal cues such as body language and facial expressions, and probing questions were used to explore relevant issues in depth while avoiding leading or suggestive questioning. A researcher with qualitative research experience conducted all interviews, and interview notes were recorded throughout. Researchers consciously practiced reflexivity by “bracketing” their own opinions to minimize subjective bias.
Data Analysis
Quantitative data were analyzed using SPSS version 27.0 and PROCESS version 4.2. Harman’s single-factor test was first applied to assess common method bias. Categorical variables were described using frequencies and percentages. The distribution of continuous variables was evaluated prior to parametric testing. Given the sensitivity of the Shapiro–Wilk test to minor deviations from normality in large samples, normality was assessed by also referring to skewness and kurtosis indices.23 Variables with absolute skewness <3 and absolute kurtosis <10 were considered approximately normally distributed and eligible for parametric analysis. Normally distributed continuous variables were described as  . Pearson correlation analysis was conducted to assess associations among variables. Group differences were examined using independent-samples t tests or one-way analysis of variance, with homogeneity of variance assessed using Levene’s test. When the homogeneity hypothesis was violated, Welch’s correction or appropriate nonparametric tests were applied.
. Pearson correlation analysis was conducted to assess associations among variables. Group differences were examined using independent-samples t tests or one-way analysis of variance, with homogeneity of variance assessed using Levene’s test. When the homogeneity hypothesis was violated, Welch’s correction or appropriate nonparametric tests were applied.
The PROCESS macrowas used to test mediation and moderation effects. A mediation analysis examined the indirect effect of temporal perspective on home exercise rehabilitation adherence via rehabilitation intention. After controlling for age, disease duration, and self-care ability, Model 16 was used to test the moderating effects of behavioral advantage and self-regulation ability on the above-mentioned mediation pathway. Model 14 was additionally applied to assess the robustness of the intention–adherence pathway when necessary. If the interaction effect was significant, further simple slope analysis (±1 standard deviation) was conducted to interpret the differences in effects under different levels of the moderator variable. Bias-corrected Bootstrap sampling (5000 resamples) was used to estimate 95% confidence intervals; effects were considered significant when the confidence interval did not include zero. The significance level was set at α = 0.05.
Qualitative interviews were transcribed verbatim within 24 hours of completion and independently cross-checked by two researchers trained in qualitative research to ensure transcription accuracy. To protect participant privacy, pseudonyms (eg, P1, P2) were used. Colaizzi’s seven-step analysis method was applied to analyze the qualitative data.24 Two researchers independently read and re-read the transcripts, extracted significant statements relevant to the research objectives, coded and clustered these statements, and formed the theme. Discrepancies were resolved through discussion, with a third researcher consulted when necessary to reach consensus.
Data Integration
This study employed a mixed-methods research with triangulation to examine home-based exercise rehabilitation behaviors among stroke patients. We assessed the coherence between qualitative subthemes and exemplar quotations, and between these and quantitative effect sizes to determine whether findings converged, diverged, or expanded upon one another.25 Convergence was identified when qualitative and quantitative findings aligned. Expansion occurred when findings were incongruent but offered complementary insights into different aspects of a construct inconsistent or contradictory. A side-by-side comparison approach was used to align qualitative topics with quantitative results. Qualitative findings were used to confirm, elaborate upon, or explain significant associations and unexpected non-significant findings from the quantitative analysis, ultimately leading to the development of integrated meta-inferences. Constructs that were not assessed in both questionnaires and interviews were not compared.
Ethical Considerations
This study has been reviewed and approved by the Medical Ethics Committee of Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School (Approval No. 2024–987-02 for the quantitative phase and 2024–758-01 for the qualitative phase). During the research process, we strictly adhere to the ethical principles of the Declaration of Helsinki, ensuring that the subjects’ privacy rights and data security are fully protected. All participants provided written informed consent after being fully informed about the study. The informed consent explicitly included permission for the publication of anonymized data and anonymized direct quotations from the interviews for research and academic dissemination purposes.
Results
Sample Characteristics
Quantitative
In the quantitative phase of this study, 289 participants were included (196 males and 93 females). Among them, 24.2% had received primary education or below. Regarding stroke incidence, 65.4% of participants had experienced a first-ever stroke. More detailed information is presented in Table 1.
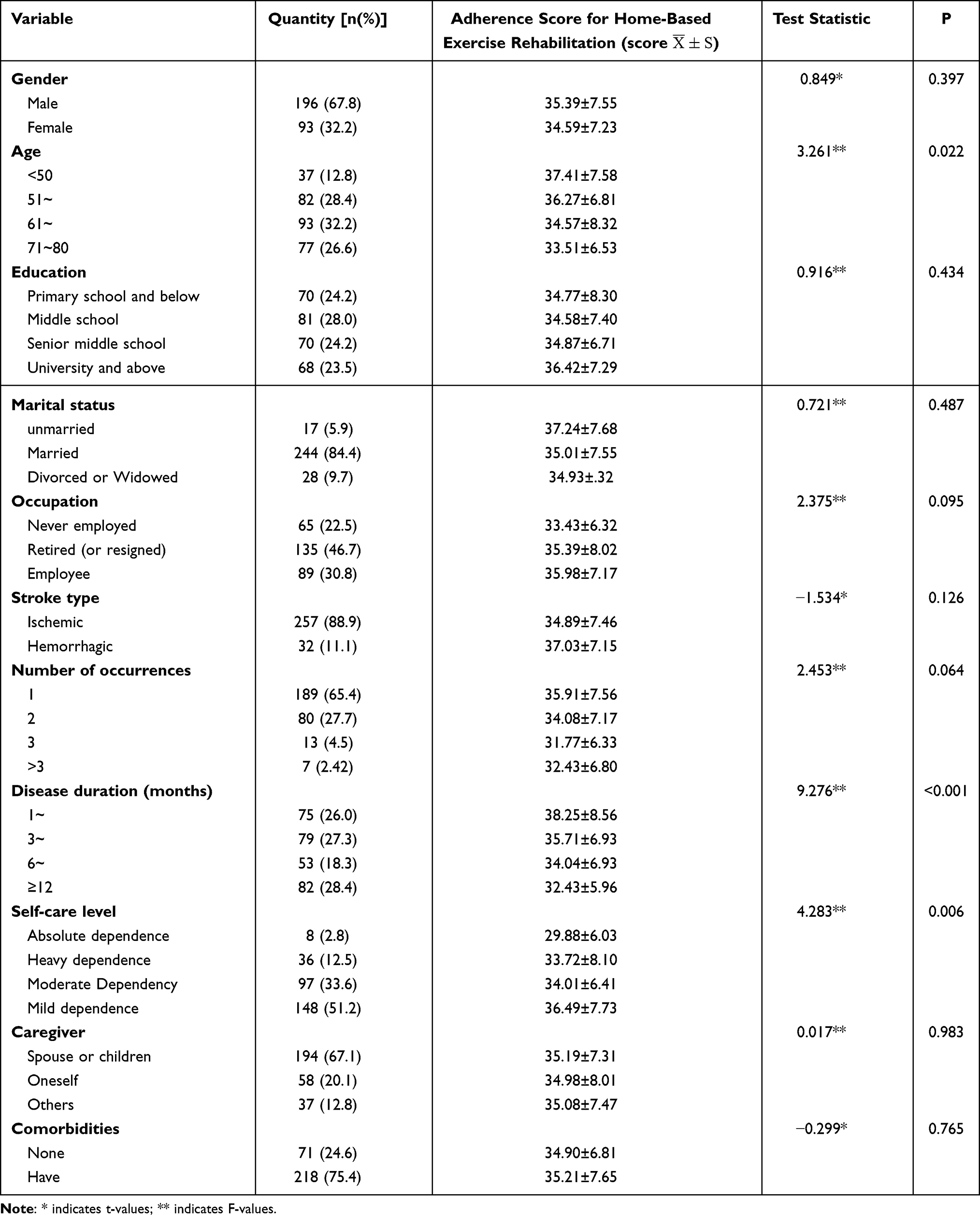 |
Table 1 Univariate Analysis of General Characteristics and Home-Based Exercise Rehabilitation Adherence of Stroke Patients (n=289) |
Qualitative
Sixteen patients were included in the qualitative study (Table 2). The mean age was 64 years (range: 55–76 years); 56.3% were male, and 87.5% were married. The interview duration ranged from 35 to 58 minutes, with a mean length of 40 minutes.
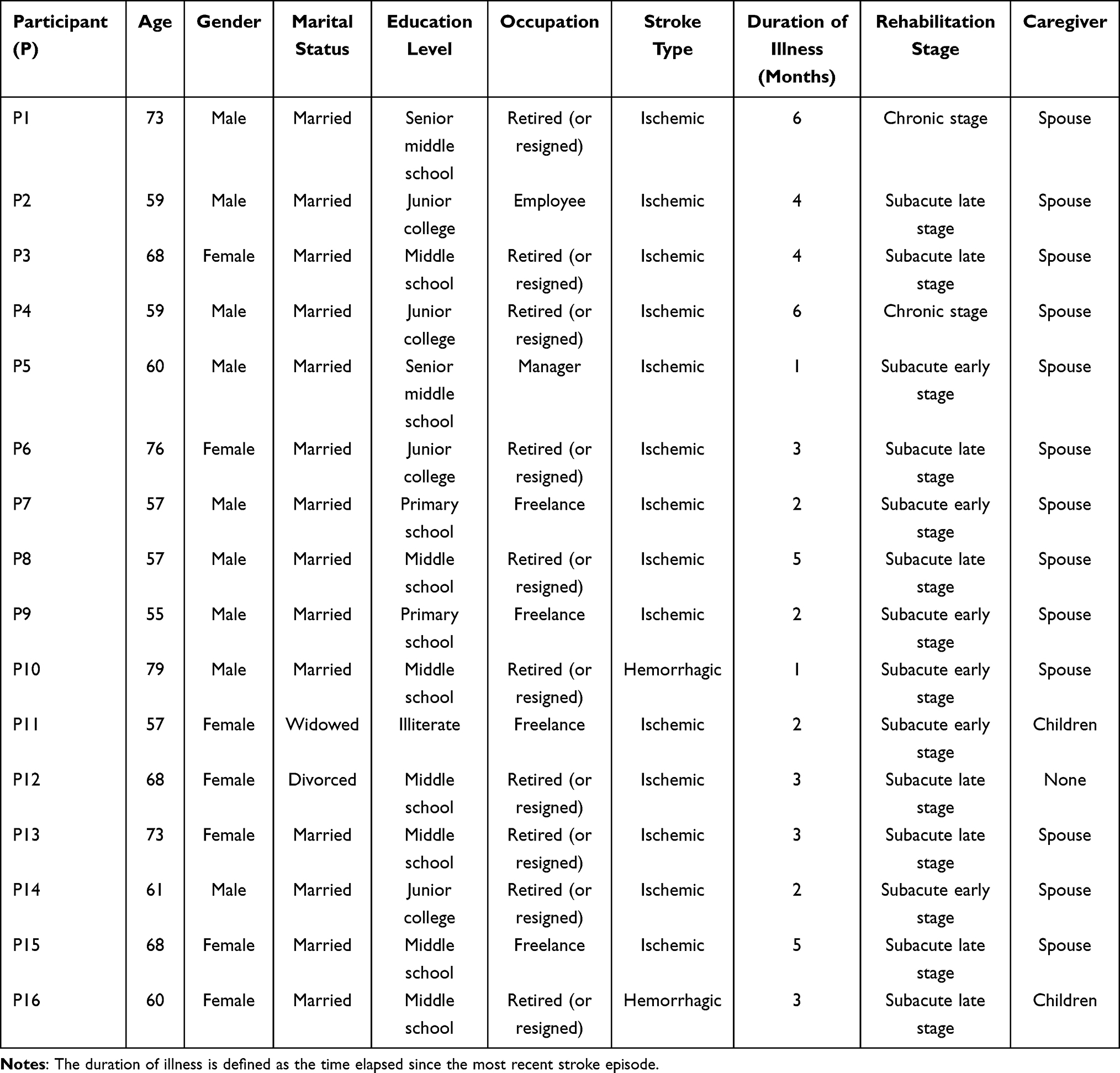 |
Table 2 Characteristics of Qualitative Study Participants (n=16) |
Quantitative Results
Common Method Bias and Normality Testing
The Harman single-factor test identified 10 common factors with eigenvalues greater than 1. The cumulative variance explained by the first factor was 21.57%, which was below the critical threshold of 40%, indicating that no serious common method bias was present in this study. Normality testing of the main continuous variables showed that skewness ranged from −0.45 to 0.53 and kurtosis ranged from −0.98 to 0.48, both within acceptable limits (|skewness<|3, |kurtosis|<10). These results indicate that the variables were approximately normally distributed. Detailed results are shown in Table 3.
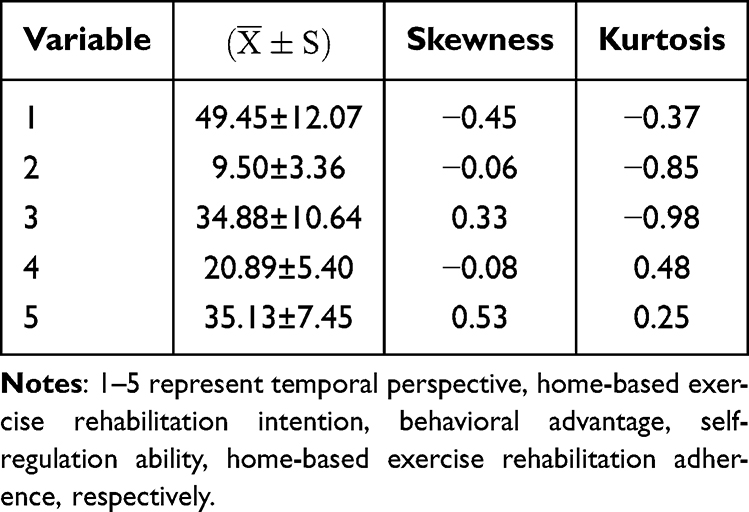 |
Table 3 Normality Test Results of Temporal Perspective, Home-Based Exercise Rehabilitation Intention, Behavioral Advantage, Self-Regulation Ability, Home-Based Exercise Rehabilitation Adherence of Stroke Patients (n=289) |
Temporal Perspective, Home-Based Exercise Rehabilitation Intention, Behavioral Advantage, Self-Regulation Ability, Home-Based Exercise Rehabilitation Adherence Score, and Correlation Analysis of Stroke Patients
The mean temporal perspective score among stroke patients was (49.45 ±12.07). The mean score for home-based exercise rehabilitation intention was (9.50 ±3.36), behavioral advantage was (34.88 ±10.64), and self-regulation ability was (20.89 ±5.40). The overall adherence score for home-based exercise rehabilitation was (35.13 ±7.45). Among adherence dimensions, physical participation in exercise had the highest score (22.16 ±5.29), with a corresponding adherence rate of (65.06 ±13.79)%. Correlation analysis showed that home-based exercise rehabilitation adherence in stroke patients was significantly and positively correlated with temporal perspective, home-based exercise rehabilitation intention, behavioral advantage, and self-regulation ability (Table 4).
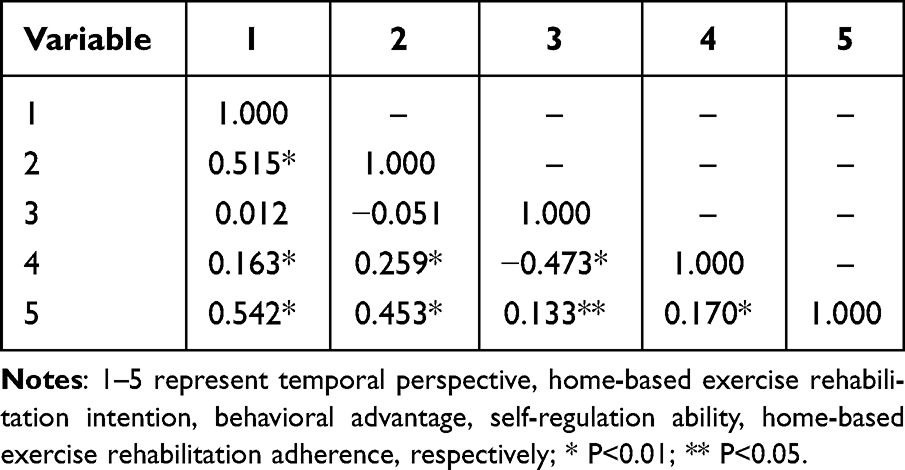 |
Table 4 Correlation Analysis Among Temporal Perspective, Home-Based Exercise Rehabilitation Intention, Behavioral Advantage, Self-Regulation Ability, Home-Based Exercise Rehabilitation Adherence of Stroke Patients (r, n=289) |
Univariate Analysis of Home-Based Exercise Rehabilitation Adherence of Stroke Patients
Significant differences in home-based exercise rehabilitation adherence were observed across patients of different ages, disease duration, and levels of self-care ability (p < 0.05), as shown in Table 1.
Mediating Effect Test of Home-Based Exercise Rehabilitation Intention of Stroke Patients Between Temporal Perspective and Adherence
Using Model 4 of PROCESS version 4.2, and after controlling for age, disease duration, and self-care ability, the mediating effect of home-based exercise rehabilitation intention was examined, with temporal perspective as the independent variable and adherence as the dependent variable. The results showed that temporal perspective significantly and positively predicted home-based exercise rehabilitation adherence (β = 0.49, t = 10.23, P < 0.001). After adding home-based exercise rehabilitation intention to the model, temporal perspective significantly and positively predicted rehabilitation intention (β = 0.50, t = 9.52, P < 0.001), and intention significantly and positively predicted adherence (β = 0.20, t = 3.78, P < 0.001). Temporal perspective remained a significant and positive predictor of adherence (β = 0.39, t = 7.25, P < 0.001). These findings indicate that home-based exercise rehabilitation intention partially mediates the relationship between time perspective and adherence. The 95% confidence interval for the mediating effect was [0.025, 0.105], with an effect size of 0.062, accounting for 20.33% of the total effect.
Moderating Effect Test of Behavioral Advantage and the Self-Regulation Ability of Stroke Patients on Mediation Model
Using Model 16 in PROCESS version 4.2 and controlling for age, disease duration, and self-care ability a moderation analysis was conducted. As shown in mediation model between the temporal perspective and home-based exercise rehabilitation adherence, the interaction between home-based exercise rehabilitation intention and behavioral advantage had a significant negative predictive effect on adherence (β = −0.03, t = −3.19, P < 0.05). In contrast, the interaction between rehabilitation intention and self-regulation ability did not significantly predict adherence (β = 0.02, t = 0.84, P > 0.05). As shown in Table 5.
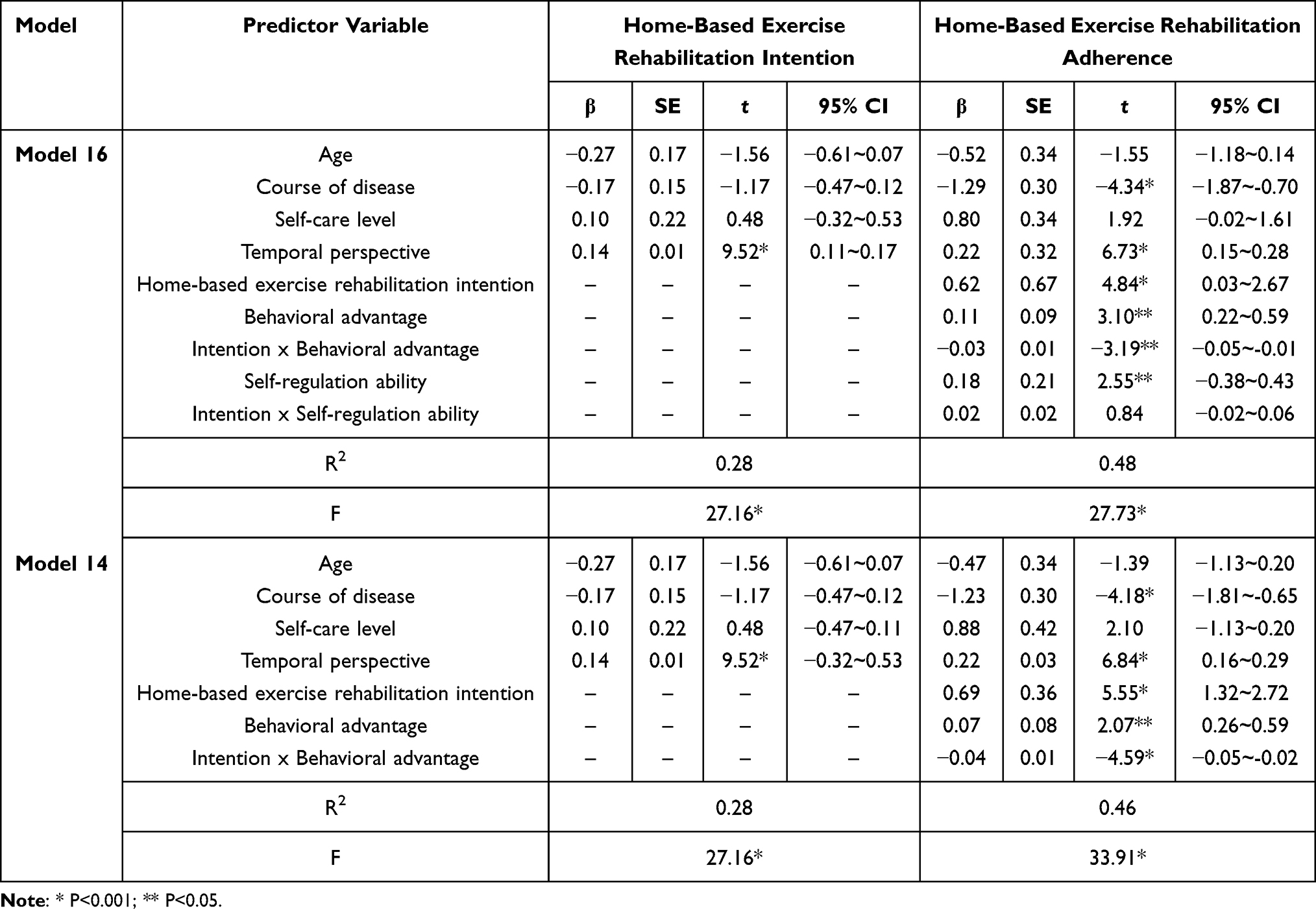 |
Table 5 Association Between Temporal Perspective and Home-Based Exercise Rehabilitation Adherence: Moderating Effects of Behavioral Advantages and Self-Regulation Ability (n=289) |
To further verify the moderating role of behavioral advantage, Model 14 was applied independently. The results showed that the interaction between rehabilitation intention and behavioral advantage remained a significant negative predictive effect of adherence (β = −0.04, t = −4.59, P < 0.05). This interaction term contributed significantly to the explanatory power of the model (Δ R2 = 0.041, f = 21.096, p < 0.001), indicating that although the moderating effect size was small, it meaningfully enhanced model explanation.
The significance test for the moderated mediation effect showed that the index of moderated mediation for behavioral advantage was −0.005, with a 95% confidence interval of [−0.008, −0.002], which did not include 0 (Table 6). These findings indicate that behavioral advantage moderates the second half of the mediating pathway involving rehabilitation intention. The path coefficients are presented in Figure 2.
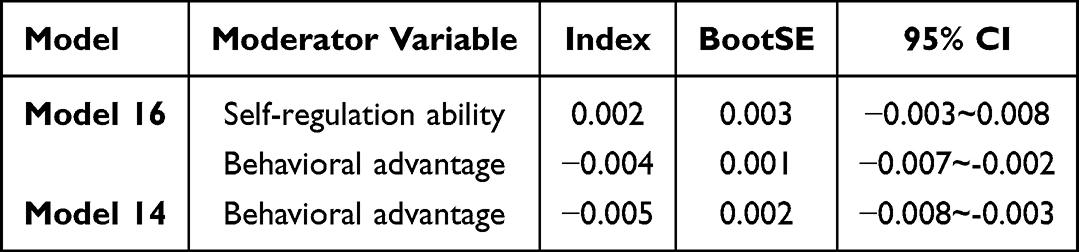 |
Table 6 Index of Moderated Mediation (Bootstrapping = 5000 Samples) |
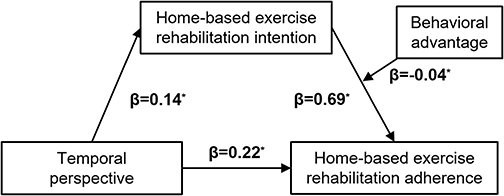 |
Figure 2 Mediation model of behavioral advantage in the association between temporal perspective and home-based exercise rehabilitation adherence. Note: * P<0.001. |
In order to clearly reveal the specific mode of the moderating effect of behavioral advantage in the second half of the path from “the temporal perspective-home exercise rehabilitation intention-home exercise rehabilitation adherence”, the mean value of behavioral advantage score plus or minus one. To further elucidate the nature of this moderating effect, simple slope analyses were conducted by categorizing behavioral advantage into high and low behavioral advantage groups. The results showed that when behavioral advantage was low, rehabilitation intention significantly and positively predicted adherence (β = 0.18, t = 6.16, P < 0.001). When behavioral advantage was high, this predictive effect was attenuated but remained significant (β = 0.12, t = 2.31, P < 0.001). These findings suggest that the influence of rehabilitation intention on adherence decreases as behavioral advantage increases (Figure 3).
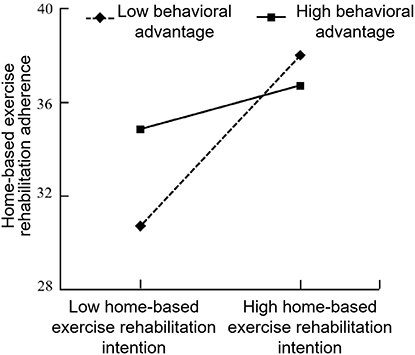 |
Figure 3 Moderating effect of behavioral advantages in the relationship between home-based exercise rehabilitation intention and adherence. |
Qualitative Results
Theme 1: Consistency Belief
Qualitative findings indicate that patients’ beliefs regarding the consistency between home-based exercise rehabilitation behaviors and expected outcomes influence their rehabilitation behaviors.
Patients who recognized the value of exercise rehabilitation demonstrated stronger behavioral intentions and were more willing to participate in and maintain rehabilitation actively.
I think it is very important to adhere to exercise rehabilitation, so although I am very tired every time I exercise, I still complete the daily training. (P9)
In contrast, patients with lower adherence believed that exercise rehabilitation would not achieve the expected results, leading to weaker rehabilitation intentions.
I tried to lift my arms, but after two attempts I was already very tired, and I could hardly see any progress. It seems my body is just like this. Practicing again feels useless. (P3)
I saw that others are recovering very quickly. I have practiced for 2 months and still need support. I feel there is little difference between sports and non sports. I cannot catch up with others anyway. (p15)
Theme 2: Time-Bound Potency
Qualitative analysis indicates that patients’ consideration of short-term costs and long-term benefits is critical to maintaining home-based rehabilitation.
Patients oriented toward future outcomes recognized the delayed benefits of home-based rehabilitation and were therefore more proactive, often creating favorable conditions to engage in rehabilitation activities.
I know recovery takes time, but when I think about being able to buy groceries and cook for myself in the future, without troubling my family, no matter how hard it is, I will persist. (P7)
I understand recovery is slow, but when I think about walking and taking my grandchildren out, I grit my teeth and keep training, no matter how difficult it is. (P11)
Conversely, due to the long-term and uncertain nature of rehabilitation, some patients exhibited poor behavioral intention, leading to low participation and adherence.
The doctor said rehabilitation requires long-term persistence, but I did not see obvious results. Sometimes I stop halfway and feel that the road to recovery is endless. (P12)
Theme 3: Behavioral Advantage
Qualitative findings suggest that behavioral advantage does not simply promote rehabilitation behavior but alters its underlying psychological driving mechanism.
Patients with high behavioral advantage reported that prior exercise habits and situational cues had turned rehabilitation into an “unconscioushabit”, requiring little conscious intention.
I have always had an exercise habit. I used to practice Tai Chi every day, so continuing rehabilitation daily feels natural. (P2)
After breakfast at 7 a.m., I automatically go to the living room to do lower-limb exercises. I do not even think about whether to practice. (P7)
My family prints and posts the training plan on the wall. It feels like a trigger switch—each exercise is just routine, without much thinking. (P8)
In contrast, for patients with low behavioral advantage, maintaining rehabilitation resembled an ongoing internal struggle driven by intention.
Every time I exercise, I struggle in my heart: ‘I am too tired today—should I skip it?’ ‘No, I have to keep going!’ Keep exercising just by the thoughts in my mind. (P14)
However, once stable situational cues were disrupted, the vulnerability of habitual behavior became apparent. Automation also reduced flexibility in adjusting to changing circumstances or even led to complete interruption of exercise.
Sometimes when guests come over, I forget about exercise altogether. By the time I remember, it is already too late. (P13)
Theme 4: Self-Regulation Ability
Qualitative findings indicate that stroke patients encounter multiple interfering factors during home-based rehabilitation, which weaken initiative and adherence. Differences in self-regulation ability appear to stem from individual neurobiological differences, particularly executive function.
Most patients reported difficulties with participation, maintenance, and self-monitoring during rehabilitation. Although they attempted self-adjustment, impaired self-regulation often hindered sustained engagement and negatively affected prognosis.
I cannot remember so many steps. I easily mix up the movements, and after making mistakes several times, I lose confidence and stop practicing. (P1)
After falling once, I became afraid of lower-limb exercises. I tried to overcome it, but I still felt uneasy and gradually gave up. (P12)
I often think, ‘it is okay to skip one day,’ so I stop training when friends invite me out. After that, it is hard to get back into the routine. (P16)
Mixed Research Integration Results
In this study, quantitative and qualitative findings were triangulated using a methodological integration strategy, as shown in Table 7. Through in-depth integration of mixed methods, a multi-level interpretative framework was developed to explain the factors influencing home exercise rehabilitation behavior among stroke patients.
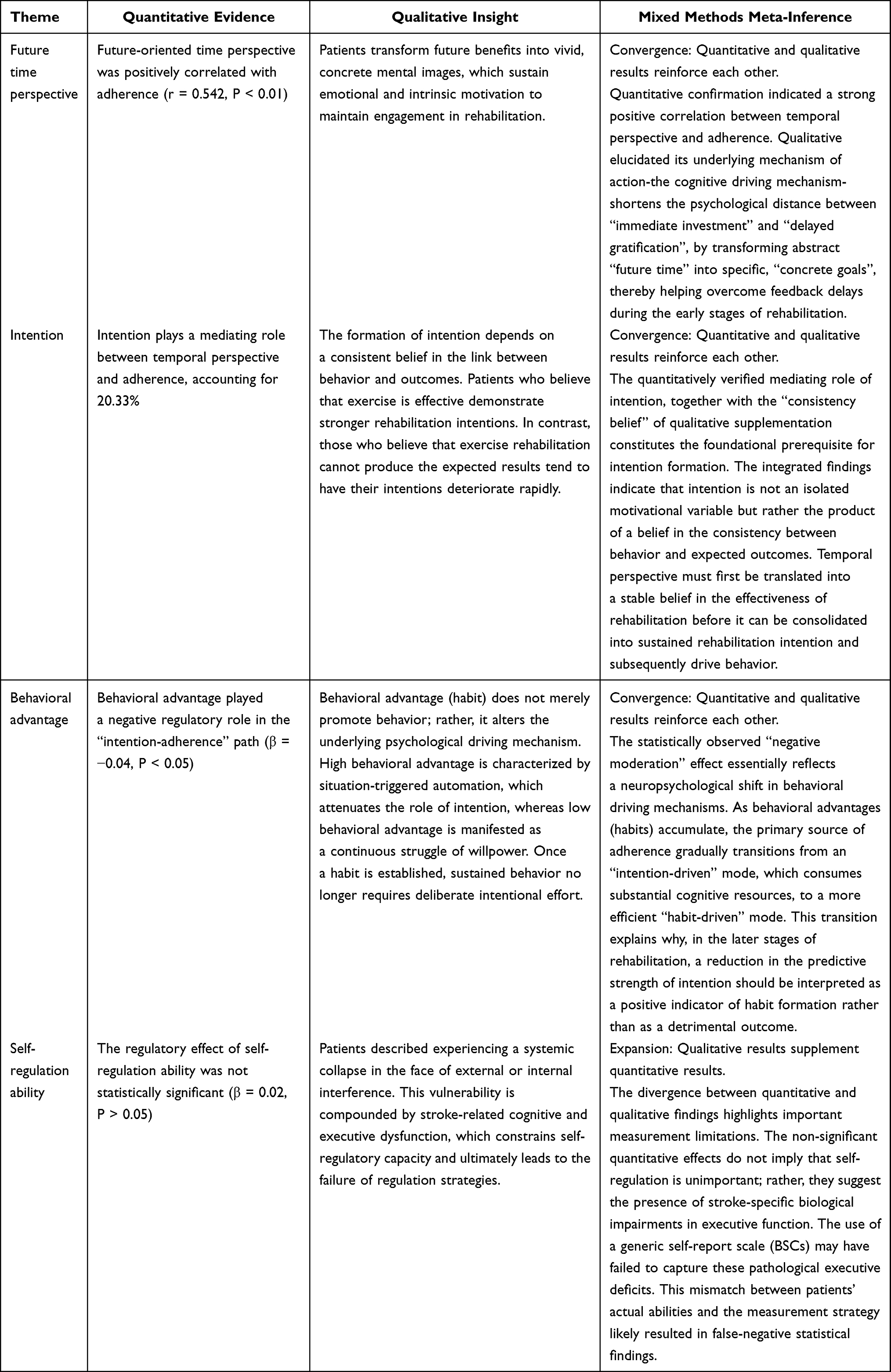 |
Table 7 Comprehensive Summary of the Qualitative and Quantitative Factors Affecting Home-Based Exercise Rehabilitation Behavior of Stroke Patients |
Discussion
This study is of considerable significance because it aims to examine the impact of a theory-driven pathway hypothesis on exercise adherence. The deep integration of quantitative and qualitative findings has enhanced our understanding of home-based exercise rehabilitation behaviors among stroke patients. The results indicate that the temporal perspective of stroke patients can promote adherence to home-based exercise rehabilitation by strengthening rehabilitation intention. At the same time, behavioral advantage plays a negative moderating role in the “intention–adherence” pathway; that is, the higher the level of behavioral advantage, the weaker the driving effect of intention on adherence. However, due to limitations in measurement tools and disease-specific characteristics, the moderating effect of self-regulation ability did not reach statistical significance.
Univariate analysis showed that age, disease duration, and degree of self-care ability were also important factors influencing adherence. The overall trends were as follows: older age and longer disease duration were associated with lower adherence, whereas better self-care ability was associated with higher adherence. These findings may be related to age-related declines in exercise endurance and executive function, as well as an increased burden of complications in older patients. When disease duration is prolonged without continuous professional feedback or dynamic goal adjustment, patients are more likely to experience motivational decline. In contrast, individuals with stronger self-care ability are more likely to integrate rehabilitation training into daily life and maintain regular exercise routines. In contrast, patients with higher levels of dependence tend to rely more heavily on caregiver supervision and support. Therefore, in clinical home rehabilitation management, priority should be given to older patients, those with longer disease duration, and those with poor self-care ability. Long-term adherence and rehabilitation outcomes can be improved by strengthening follow-up feedback and caregiver guidance.
The findings of this study demonstrate a positive correlation between temporal perspective and adherence to home exercise rehabilitation, indicating that greater consideration of the potential long-term outcomes of current rehabilitation behaviors is associated with stronger adherence. This finding is consistent with the results reported by Chew et al26 which showed that a future time perspective is positively correlated with health-promoting behaviors. Specifically, when weighing the immediate costs of rehabilitation against future health benefits, patients with a future-oriented time perspective tend to place greater emphasis on the delayed benefits of exercise rehabilitation, such as improvements in physical function, psychological adjustment, and restoration of social roles, thereby stimulating a stronger motivation to implement rehabilitation plans.27 Further qualitative analysis revealed the underlying psychological mechanisms of this relationship. As a sudden traumatic event, a stroke often leads to “biographical disruption” in patients. During the acute phase, patients may become trapped in a “present dilemma”, characterized by an excessive focus on current functional limitations and immediate fatigue during rehabilitation training. Given that stroke rehabilitation involves “immediate investment and delayed benefit”, patients with a strong present-oriented perspective may overemphasize immediate pain and perceived costs while neglecting future functional gains and rewards. This restricted perspective makes it difficult for patients to establish a psychological link between sustained current efforts and future rehabilitation benefits, thereby weakening the maintenance of rehabilitation intention. In this study, the mean temporal perspective score among stroke patients was 49.45 ±12.07, with a percentage score of 51.90 ± 16.76, indicating a moderate level of consideration of future outcomes in decision-making for home-based exercise rehabilitation. This finding suggests that greater attention should be paid to the assessment and intervention of temporal perspective in clinical practice. Healthcare professionals can adopt time-framing strategies to break down long-term rehabilitation goals into manageable short-term tasks through goal-directed training, thereby enhancing the perception of patients and engagement with future benefits. Alternatively, episodic future thinking interventions can be used to guide patients in vividly imagining positive future outcomes, strengthening the association between “current rehabilitation behavior” and “potential long-term benefits”, and ultimately enhancing rehabilitation.28,29
A second key finding of this study was the partial mediating role of rehabilitation intention in the “temporal perspective and adherence” path, with the mediating effect accounting for 20.33% of the total effect. This indicates that a future time perspective not only directly promotes adherence but also indirectly enhances adherence by strengthening home exercise rehabilitation intention. Qualitative data further clarified that “consistency belief” serves as a critical cognitive prerequisite linking temporal perspective to rehabilitation intention. Only when patients recognize a relationship between motor behavior and long-term functional recovery can future-oriented thinking be effectively translated into active rehabilitation intention. These findings support theoretical perspectives suggesting that a future time orientation promotes long-term health behaviors by strengthening behavioral intention. Specifically, future-oriented patients are more likely to develop consistent beliefs regarding the long-term value of rehabilitation behaviors. At the same time, they tend to reinforce immediate positive feedback from rehabilitation activities, thereby effectively stimulating rehabilitation intention and facilitating its transformation into actual adherence behavior.12 Many health behavior theories emphasize intention as a direct predictor of physical activity. When patients have strong rehabilitation intentions, they are more likely to demonstrate high adherence even without external supervision. However, Zhou et al30 reported that only 38.4% of stroke patients planned to exercise after discharge, indicating generally low levels of home exercise intention. Therefore, nurses and rehabilitation professionals should fully recognize the importance of temporal perspective and the mediating role of rehabilitation intention. Individualized time-framed educational strategies should be developed based on patients’ time orientation, alongside interventions such as incentive feedback, behavior change techniques to strengthen rehabilitation intention.31
The results of this study further demonstrate that behavioral advantage plays a significant negative moderating role in the second half of the mediation pathway of “temporal perspective-rehabilitation intention-adherence”. The negative interaction term (β = –0.04) does not indicate that behavioral advantage weakens adherence; rather, it reflects a shift in behavioral control mechanisms. Specifically, as behavioral advantage (habit intensity) increases, individuals become less dependent on conscious intention to maintain adherence. Although the regression coefficient of the interaction term was relatively small, simple slope analysis revealed clear stratification effects. At lower levels of behavioral advantage, intention strongly predicted adherence, whereas at higher levels, this relationship was markedly weakened or no longer significant. These findings suggest that once rehabilitation behaviors become highly habitual, adherence is no longer primarily driven by motivational states but instead by automatic processes. Notably, correlation analysis showed no significant association between temporal perspective and behavioral advantage (r = 0.012, P > 0.05), suggesting that temporal perspective is more likely to influence adherence through motivational mechanisms, such as intention, rather than directly predicting habit formation. Home-based exercise rehabilitation is a complex behavior jointly regulated by automatic processes (habits) and goal-directed control processes (intention).32 Through repeated practice, rehabilitation behaviors may become automatically triggered by contextual cues such as fixed exercise times or environments, thereby reducing the cognitive effort required for conscious decision-making. Qualitative findings further elucidated why the predictive power of intention diminishes once habits are established. However, they also highlighted a potential vulnerability of behavioral advantage: when stable contextual cues are disrupted, automated behaviors may be easily interrupted, and excessive reliance on habitual patterns may reduce patients’ adaptability to changing circumstances. In this study, the mean behavioral advantage score among stroke patients was 34.88 ±10.64, which was higher than the score of 23.89 ±6.99 reported by Zhang et al.29 This discrepancy may be attributable to differences in sample characteristics, as Zhang et al29 focused on younger and middle-aged stroke patients who may face greater interference from work and social pressures, making habit formation more challenging. Collectively, these findings underscore the important role of behavioral advantage in regulating the intention–behavior gap. Accordingly, clinical interventions should emphasize the strategic use of behavioral advantage by establishing stable situational cues—such as fixed times and locations—to trigger rehabilitation behaviors. This approach can strengthen the “cue–behavior” association and support the development of long-term home-based rehabilitation habits.33
Finally, this study found that self-regulation ability did not moderate the intention–adherence relationship. Although self-regulation is theoretically considered a key mechanism for translating intention into behavior, quantitative analysis did not provide empirical support for this role. When interpreted alongside qualitative findings, this discrepancy may be attributed to limitations in measurement tools and disease-specific characteristics. Currently, there is a lack of assessment instruments specifically designed to measure self-regulation in stroke rehabilitation contexts, particularly for home-based exercise. Consequently, this study employed the BSCS, a widely validated general self-report measure. However, as a general instrument, the BSCS may lack sensitivity in identifying stroke-related executive dysfunction, leading assessors to underestimate the regulatory role of self-regulation in the intention–adherence pathway. Moreover, stroke patients often experience subtle impairments in executive function, and self-regulation capacity is closely tied to both self-control and executive functioning.34 Such neurobiological impairments may limit patients’ ability to mobilize self-regulatory resources to translate intention into action, thereby statistically masking their moderating effect. Therefore, despite the absence of significant quantitative findings, qualitative evidence suggests that self-regulation remains an important factor in rehabilitation adherence. Future research should prioritize the development of specific self-regulation assessment tools for stroke rehabilitation scenarios, and integrate objective neuropsychological measures to evaluate the role of self-regulation in rehabilitation behavior more accurately.
Limitation of the Study
There are several limitations in this study. First, the cross-sectional design precludes accurate inference of causal relationships among variables. Future research should carry out longitudinal studies or intervention-based experiments to further verify the causal effects of temporal perspective and future-oriented thinking. Second, questionnaire surveys and face-to-face interviews may have introduced recall and social desirability biases, as patients may tend to report better adherence to gain recognition. Third, participants were recruited via convenience sampling at a single center, which may have introduced selection bias and limited the generalizability of the findings. Future studies should adopt multi-centers and include more diverse patient populations. Fourth, key clinical factors—including lesion location, depressive symptoms, cognitive status, and executive function—were not directly assessed, which may have introduced unmeasured confounding. Future studies should incorporate relevant assessment tools to enable more comprehensive analysis and control of these factors. Fifth, other potential confounding variables such as gender, comorbidities, and social support were not included as covariates in the mediation model. Future studies employing larger sample sizes should incorporate a broader range of multidimensional covariates to further validate the robustness of the identified mediation mechanisms. Finally, as discussed above, the development and application of self-regulation and executive function assessment tools specific to stroke rehabilitation represent an important direction for advancing research in this field.
Conclusion
This study adopted a mixed-methods approach to demonstrate that adherence to home-based exercise rehabilitation after stroke is not determined by a single motivational process but arises from the dynamic interaction between intention-driven and habit-driven mechanisms over time. The findings indicate that temporal perspective not only directly promotes adherence to home-based exercise rehabilitation but also indirectly enhances adherence by strengthening rehabilitation intention. Moreover, the development of behavioral advantage (habit) can effectively reduce reliance on subjective intention and facilitate the automation of rehabilitation behaviors. Nursing professionals can improve rehabilitation adherence by enhancing patients’ consideration of future outcomes, strengthening their intentions to engage in home exercise rehabilitation, and strategically using situational cues to support the maintenance of long-term exercise habits. Importantly, given the potential presence of executive dysfunction in stroke patients, generic self-regulation interventions may have limited effectiveness. Therefore, clinical nursing staff should prioritize developing and implementing stroke-specific executive function assessment tools and targeted training strategies to bridge the “intention-behavior”gap effectively.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available because some data involve personal privacy. Still, they are available from the corresponding author at a reasonable request.
Acknowledgments
Thank you to Nanjing Drum Tower Hospital for providing us with a platform for collecting data. Thank you to every patient who is willing to participate in our research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jiangsu Provincial Aging Health Research Project [grant number LKM2023024]; Natural Science Foundation Project of Nanjing University of Chinese Medicine [grant number XZR2023074].
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Prevention RoS, Group TiCW. Summary of Chinese stroke prevention report 2021. Chin J Cerebrovasc Dis. 2023;20(11):783–18. doi:10.3969/j.issn.1672-5921.2023.11.009.
2. Feigin VL, Owolabi MO. Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission. Lancet Neurol. 2023;22(12):1160–1206. doi:10.1016/s1474-4422(23)00277-6
3. Chi NF, Huang YC, Chiu HY, Chang HJ, Huang HC. Systematic review and meta-analysis of home-based rehabilitation on improving physical function among home-dwelling patients with a stroke. Arch Phys Med Rehabil. 2020;101(2):359–373. doi:10.1016/j.apmr.2019.10.181
4. Lindblom S, Tistad M, Flink M, Laska AC, von Koch L, Ytterberg C. Referral-based transition to subsequent rehabilitation at home after stroke: one-year outcomes and use of healthcare services. BMC Health Serv Res. 2022;22(1):594. doi:10.1186/s12913-022-08000-7
5. Ji L, Deng Y, Huang Q, liu G, Huang Q, Zhang L. Home based rehabilitation of stroke in developed countries and Its enlightenment to China. Chin Med Herald. 2021;18(36):165–168+182. doi:10.20047/j.issn1673-7210.2021.36.040
6. Miller KK, Porter RE, DeBaun-Sprague E, Van Puymbroeck M, Schmid AA. Exercise after stroke: patient adherence and beliefs after discharge from rehabilitation. Topic Stroke Rehabilitat. 2017;24(2):142–148. doi:10.1080/10749357.2016.1200292
7. Lin B, Xue L, An B, Zhang Z, Zhang W. An age-stratified cross-sectional study of physical activity and exercise adherence of stroke survivors in rural regions. Patient Preference Adherence. 2023;17:2013–2023. doi:10.2147/ppa.S417220
8. Lin B, Zhang Z, Mei Y, Liu L, Ping Z. The influential factors of adherence to physical activity and exercise among community-dwelling stroke survivors: a path analysis. J Clin Nurs. 2022;31(17–18):2632–2643. doi:10.1111/jocn.16091
9. Lin B, Zhang Z, Sun Y, Mei Y, Xie J, Zhang Y. Development and reliability and validity testing of a functional exercise adherence scale for community stroke patients. Chin J Rehabil Med. 2013;28(06):574–578. doi:10.3969/j.issn.1001-1242.2013.06.018
10. Yang XY. Research on Personalized Exercise Intervention Design Based on Behavior Change Theory. University of science and technology of China; 2019.
11. Feil K, Fritsch J, Rhodes RE. The intention-behaviour gap in physical activity: a systematic review and meta-analysis of the action control framework. Br J Sports Med. 2023;57(19):1265–1271. doi:10.1136/bjsports-2022-106640
12. Yu B, Bai J, Li X, Xie P. Research progress of time bound self regulation theory in the field of health behavior. Military Nurs. 2022;39(10):88–90. doi:10.3969/j.issn.2097-1826.2022.10.023
13. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage; 2017.
14. Neurology branch of Chinese Medical Association, Cerebrovascular disease group, Neurology branch of Chinese Medical Association. Diagnostic criteria of cerebrovascular diseases in China (version 2019). Chin J Neurol. 2019;52(9):710–715.
15. Bertaux D. Biography and Society: The Life History Approach in the Social Sciences. Beverly Hills, Calif: SAGE Publications; 1981.
16. Grady MP. Qualitative and Action Research: A Practitioner Handbook. Phi Delta Kappa Educational Foundation; 1998.
17. Strathman A, Gleicher F, Boninger DS, Edwards CS. The consideration of future consequences: weighing immediate and distant outcomes of behavior. J Personality Soc Psychol. 1994;66(4):742–752. doi:10.1037/0022-3514.66.4.742
18. Ajzen I. The theory of planned behavior. Org beha human decis processes. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
19. Fang M. The relation between exercise intentions and behaviour of adolescents: mediated adjustment. J Shanghai Univ Sport. 2012;36(02):45–49. doi:10.16099/j.cnki.jsus.2012.02.012
20. Verplanken B, Orbell S. Reflections on past behavior: a self-report index of habit strength. J Appl Social Psychol. 2003;33(6):1313–1330. doi:10.1111/j.1559-1816.2003.tb01951.x
21. Morean ME, DeMartini KS, Leeman RF, et al. Psychometrically improved, abbreviated versions of three classic measures of impulsivity and self-control. Psycholog Assessment. 2014;26(3):1003–1020. doi:10.1037/pas0000003
22. Luo T, Chen L, Qin L, Xiao S. Reliability and validity of chinese version of brief self-control scale. Chin J Clin Psychol. 2021;29(01):83–86. doi:10.16128/j.cnki.1005-3611.2021.01.017
23. Finney SJ, DiStefano C. Non-normal and categorical data in structural equation modeling. Struct Equation Modeling. 2006;10(6):269–314. doi:10.1108/978-1-62396-246-320251015
24. Liu M. Application of Colaizzi’s seven steps in the analysis of phenomenological research data. J Nurs. 2019;34(11):90–92. doi:10.3870/j.issn.1001-4152.2019.11.090
25. Creswell JW, Clark VLPX. Designing and Conducting Mixed Methods Research. Sage publications; 2017.
26. Chew HSJ, Sim KLD, Choi KC, Chair SY. Relationship between self-care adherence, time perspective, readiness to change and executive function in patients with heart failure. J Behav Med. 2020;43(4):1–11. doi:10.1007/s10865-019-00080-x
27. Shi H, Wang Q, Jiang Y, Zhang M, Dai Y, Ji K. Meta integration of qualitative research on exercise rehabilitation experience of stroke patients. Chin J Nurs. 2024;59(11):1397–1404. doi:10.3761/j.issn.0254-1769.2024.11.017
28. Ru Y, Ding S, Gao Y, et al. Research progress of future scenario imagination in health behavior decision making of patients with chronic diseases. Chin J Nurs. 2023;58(21):2677–2682. doi:10.3761/j.issn.0254-1769.2023.21.017
29. Zhang R, Chen Y, Huai P, Qiao C, Yang H. Effect of execution intention strategy based on time bound self-regulation theory on execution intention of rehabilitation exercise behavior of young and middle-aged stroke patients. Nurs res. 2023;37(18):3368–3373. doi:10.12102/j.issn.1009-6493.2023.18.024
30. Zhou Y, Hua B, Shi X, Du S, Yuan J, Wang Y. Exercise intention and its associated factors among persons post-stroke: a cross-sectional study. Patient Preference Adherence. 2023;17:2535–2544. doi:10.2147/ppa.S424595
31. Guan M, So J. Tailoring temporal message frames to individuals’ time orientation strengthens the relationship between risk perception and behavioral intention. J Health Commun. 2020;25(12):971–981. doi:10.1080/10810730.2021.1878310
32. Gardner B, de Bruijn GJ, Lally P. A systematic review and meta-analysis of applications of the self-report habit index to nutrition and physical activity behaviours. Annals Behav Med. 2011;42(2):174–187. doi:10.1007/s12160-011-9282-0
33. Divine A, Astill S. Reinforcing implementation intentions with imagery increases physical activity habit strength and behaviour. Brit J Health Psychol. 2025;30(2):e12795. doi:10.1111/bjhp.12795
34. Chen C, Zhai Q, Wang L, Hao J, Li X. Application progress of time bound self regulation theory in the field of health behavior. Health Educ China. 2023;39(12):1131–1135. doi:10.16168/j.cnki.issn.1002-9982.2023.12.013
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.