Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Factors Contributing to Retention in Care and Treatment Adherence Among People Living With HIV Returning to Care in South-Eastern Tanzania: A Qualitative Study
Authors Matimbwa H ![]() , Lolo SA, Matoy LS, Ndaki R, Ngahyoma S, Mollel HA, Luoga E, Vanobberghen F, Vianney JM
, Lolo SA, Matoy LS, Ndaki R, Ngahyoma S, Mollel HA, Luoga E, Vanobberghen F, Vianney JM ![]() , Idindili B, Weisser M
, Idindili B, Weisser M
Received 10 September 2024
Accepted for publication 10 December 2024
Published 4 February 2025 Volume 2025:17 Pages 39—57
DOI https://doi.org/10.2147/HIV.S492673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Hassan Matimbwa,1– 3 Sarah Andrea Lolo,1,2,4 Leila S Matoy,1,2 Regina Ndaki,1 Suzan Ngahyoma,5,6 Henry Abraham Mollel,7 Ezekiel Luoga,1,5 Fiona Vanobberghen,8,9 John-Mary Vianney,2 Boniphance Idindili,10 Maja Weisser,1,8,11 The Kilombero and Ulanga Antiretroviral Cohort study group (KIULARCO)Kabula Aaroni1. 1, Aschola Asantiel1. 1, Farida Bani1. 1, Theonestina Byakuzana1. 1, Joyce Claud1. 1, Adolphina Chale1. 1, Elizabeth Dotto1. 1, Gideon Francis3. 310. 1011. 11, Tracy Glass4. 45. 5, Yvonne Haridas1. 1, Jerry Hella1. 1, Speciosa Hwaya3. 3, Rodney Julius1. 1, Aneth V Kalinjuma1. 16. 67. 7, Andrew Katende1. 1, Yassin Kisunga1. 1, Ezekiel Luoga1. 1, Jerome Lwali1. 18. 89. 9, Edgar Enzigard Martin1. 1, Honorati Masanja1. 1, Swalehe Masoud1. 1, Mohammed Mbaruku1. 1, George Mfanando1. 1, Josephine Mhina1. 1, Mengi Mkulila3. 3, Margareth Mkusa3. 310. 1011. 11, Fransisca Alfred Mmbando1. 1, Lina Mnunga3. 310. 1011. 11, Alpha Mninje3. 310. 1011. 11, Dorcas K Mnzava1. 1, Getrud J Mollel1. 1, Lilian Moshi1. 1, Germana Mossad3. 310. 1011. 11, Rejina Mponji3. 310. 1011. 11, Dolores Mpundunga3. 3, Athumani Mtandanguo1. 1, Ummu-kulthum Mwaliga11. 1, Selerine Myeya1. 1, Sanula Nahota1. 1, Sharifa Nakapala3. 310. 1011. 11, Regina Ndaki1. 1, Robert C. Ndege1. 1, Agatha Ngulukila1. 1, Alex John Ntamatungiro1. 16. 67. 7, Vaileth Nyaenza3. 310. 1011. 11, Emmanuel Nyenza1. 1, Amina Nyuri1. 1, James Okuma4. 45. 5, Ally Olotu1. 1, Daniel H Paris4. 45. 5, Martin Rohacek1. 14. 45. 5, Leila Samson1. 1, Elizabeth Senkoro1. 1, George Sigalla1. 1, Joseph Singo1. 1, Jamali B Siru1. 1, Jenifa Tarimo1. 1, Albart R Malabe3. 310. 1011. 11, Juerg Utzinger4. 45. 5, Fiona Vanobberghen4. 45. 5, Maja Weisser1. 14. 45. 510. 10, John Wigay1. 1, Lulu Wilson1. 1 On behalf of the KIULARCO Study Group
1Interventions and Clinical Trials Department, Ifakara Health Institute, Morogoro, Tanzania; 2School of Life Science and Bioengineering, The Nelson Mandela African Institute of Science and Technology, Tengeru, Arusha, Tanzania; 3Department of Health Services, Mzumbe University, Mbeya, Tanzania; 4Department of Secondary Education, Singida, Tanzania; 5Chronic Disease of Ifakara, St. Francis Regional Referral Hospital, Morogoro, Tanzania; 6Benjamin Mkapa Foundation, Dar Es Salaam, Tanzania; 7Department of Health Systems Management, Mzumbe University, Morogoro, Tanzania; 8Swiss Tropical and Public Health Institute, Allschwil, 4123, Switzerland; 9University of Basel, Basel, 4002, Switzerland; 10Public Health Department, The Kampala International University, Dar Es Salaam, Tanzania; 11Division of Infectious Diseases, University Hospital Basel, Basel, 4031, Switzerland; 1.Ifakara Health Institute, Ifakara, Tanzania; 2.University Hospital Basel, Basel, Switzerland; 3.Saint Francis Referral Hospital, Ifakara, Tanzania; 4.Swiss Tropical and Public Health Institute, Allschwil, Switzerland; 5.University of Basel, Basel, Switzerland; 6.Epidemiology and Biostatistics Department, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand; 7.Division of Public Health, School of Public Health and Family Medicine, University of Cape Town, South Africa; 8.Indiana University, Indianapolis, U.S.; 9.Division of Infectious Diseases and Hospital Epidemiology, University Hospital Basel, University of Basel, Switzerland; 10.Benjamin Mkapa Foundation, Dar es Salaam, Tanzania; 11.USAID Afya Yangu, Dar es Salaam, Tanzania
Correspondence: Hassan Matimbwa, Ifakara Health Institute, P.O. Box 53, Off Mlabani Passage, Ifakara, Morogoro, Tanzania, Tel +255 718 371 666, Email [email protected]
Background: People living with HIV (PLHIV) with good adherence to antiretroviral therapy (ART) achieve good health outcomes. However, treatment interruptions remain a major challenge, particularly in rural Africa. This study explored factors related to dropout, return, retention in care, and treatment adherence among PLHIV returning to care after missing clinical visits.
Methods: We conducted an exploratory study using a phenomenological approach in rural South-eastern Tanzania, from July to October 2023. In-depth interviews (IDIs) were conducted with 21 PLHIV who resumed care after missing visits for three months or more from the last scheduled appointment and who were taking ART less than 60 days within the last three months, and their 13 treatment supporters. Interviews were conducted at St. Francis Regional Referral Hospital and Kibaoni Health Center.Five focus group discussions (FGDs) were conducted with 6– 8 healthcare workers from Kibaoni, Mang’ula, Mkamba, Mgeta Health Center, and St. Francis Hospital. Data were analyzed by thematic analysis, with NVivo 12 software.
Results: The median age of the 21 PLHIV was 40 years (range 21 to 63); 10 (47.6%) were females. Reasons for dropping out of care reported included fear of disclosure, complacency with improved health, denial of HIV status, work-related absence, and religious beliefs. Reasons for returning included health deterioration, completion of work obligations causing care interruption, family support, and clinic follow up. Factors promoting retention and adherence were improved health through ART, trust in healthcare services, counseling, health education, clinic follow-up, longer drug refill periods, and family support.
Conclusion: Our study highlights persisting stigmatization contributing to dropping from care, with strong family and social support improving adherence and clinic attendance. Future interventions should focus on these factors to enhance retention of lifelong treatment adherence. Working obligations remain a challenge, that could be addressed by facilitated access to remote drug pickup.
Keywords: attrition from care, retention in HIV care, treatment adherence, people living with HIV, South-Eastern Tanzania
Introduction
Globally, 84.2 million people have been infected with HIV/AIDS since the pandemic began more than three decades ago.1 According to the UNAIDS Global Report of 2023 currently 39 million people are living with HIV (PLHIV), while more than 40 million have died from HIV-related diseases.2 Sub-Saharan Africa remains the region hit hardest with 3.4% of adults living with HIV, accounting for approximately two-thirds of all cases globally.3 In Tanzania, one person with HIV lives in 11.8% of urban and 8.7% of rural households.4 The Tanzania HIV impact survey 2022–23 reported an HIV prevalence of 4.4% with 1,548,000 adult PLHIV, higher in women (5.6%) compared to men (3.0%).5 Of 1.5 million adult PLHIV in Tanzania, 82% know their status, 98% receive treatment, and 94% are virally suppressed.5
Antiretroviral therapy (ART) is the most effective strategy for the prevention and treatment of HIV. The use of ART has resulted in a significant decrease in HIV-associated comorbidities and risk of HIV-related death.6–8 In addition, proper use of ART improves HIV patients’ well-being, suppresses viral load, and reduces HIV transmission risk, thus serving as a key prevention strategy9,10 A significant challenge is patient attrition on ART, which increases the risk of adverse health outcomes and hinders global HIV control.10,11 Retention in care is critical to ensure ART adherence, viral suppression, and prevention of HIV drug resistance.12–14 Several associated factors influence PLHIV to remain in care, including clinical, sociocultural, economic, and health systems aspects, as well as geographical and other contextual factors.15,16 Other factors contribute to poor treatment adherence and care, including fear of side effects, alcohol and substance abuse, stigma, distance from the clinic, and poverty.6,14,17–20
Experiences from the Kilombero and Ulanga Antiretroviral Cohort (KIULARCO) show the complex care cascade in a rural setting in South-eastern Tanzania21,22 with periods with poor drug adherence contributing to poor treatment outcomes.23 Efforts to improve HIV treatment adherence such as training communication skills among healthcare providers as been shown to improve treatment outcomes.22 However, attrition to care remains a major challenge15 with a high loss to follow-up (LTFU) rate of 21%-41%, whereby half of LTFU participants return to care at a later time point.24
Patients returning to care are an important group, as we can learn from them the reasons for dropping out and returning to care, as well as reasons for interrupting drug intake.25,26 Knowing these factors allows for the design of effective interventions that can improve retention in care and drug adherence27 and can be addressed by qualitative research.28 Re-engagement programs successfully led to the return of patients lost to follow-up.29,30 The role of family or treatment supporters is to support PLHIV to adhere to treatment and retention in care through emotional, social, and practical support.31,32
In this study, we explored factors associated with dropping out from and returning to care, remaining in care, and treatment adherence among PLHIV, who returned to care after missing clinical visits for more than 3 months and with an irregular ART intake since the last clinical visit in South-eastern Tanzania. In addition, we interviewed participants’ treatment supporters and healthcare workers (HCWs) involved in their care.
Methods
Study Design
We conducted an exploratory qualitative study using a phenomenological approach33 to study the lived perceived experiences of adult PLHIV who returned to care after missing visits for three months or more from the last scheduled appointment and who were taking ART less than 60 days within the last three months, treatment supporters’ perspectives, and healthcare workers’ (HCW) perspectives on factors contributing to drop out of ART care, return to care, retention in care, and adherence among PLHIV who returned to care after missing their visits and were on irregular ART for at least 3 months. The data collection was based on a prospective study approach using in-depth interviews (IDIs) with PLHIV, and treatment supporters, and focus group discussions (FGD) for healthcare workers.
Study Setting and Population
This study was conducted in two districts in South-eastern Tanzania including Ifakara Town Council and Mlimba District Council between July and October 2023. These districts were purposively selected as part of the KIULARCO catchment area. PLHIV who resumed ART services after missing visits for three months or more from the last scheduled appointment and without ART for 60 days or more within the last three months, along with their treatment supporters, were recruited from St. Francis Regional Referral Hospital and Kibaoni District Hospital. Healthcare workers recruited in the study included doctors, psychologists, nurses, and community health workers from Kibaoni, Mang’ula, Mkamba, Mgeta Health Centers, and St. Francis Regional Referral Hospital (Figure 1). The selected health facilities offer ART care services to a larger number of people living with HIV compared to other health care facilities in Kilombero and Ulanga districts.
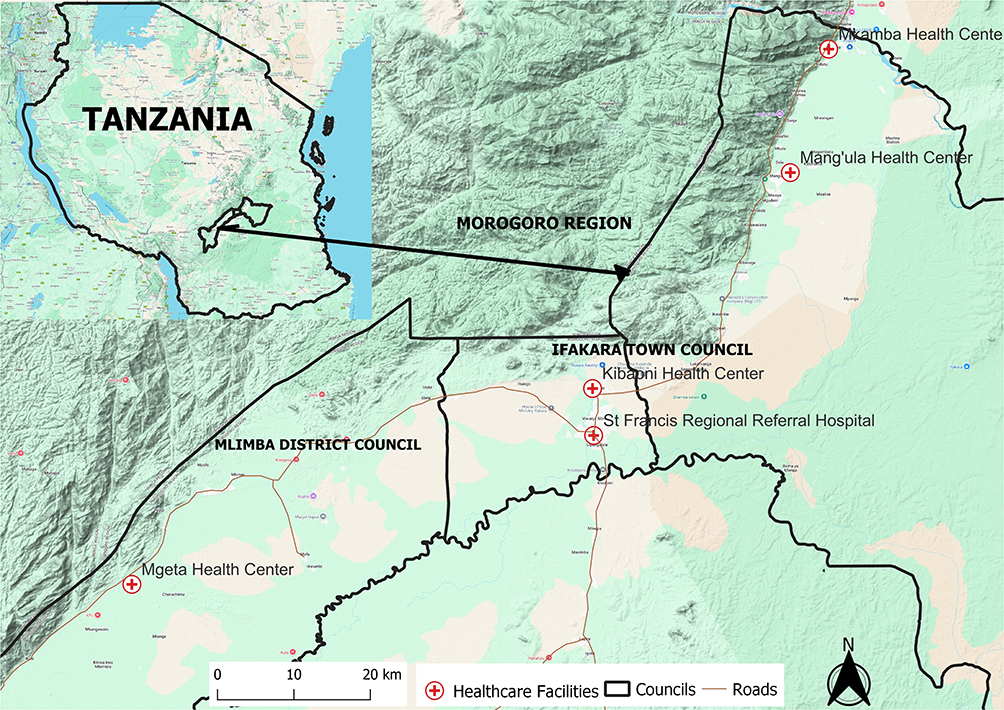 |
Figure 1 Map of the recruitment area. The map shows the recruitment area with red crosses indicating health facilities, where participants and healthcare workers were recruited for interviews. |
Sample Size, and Sampling
We used a purposive sampling method34 for in-depth interviews (IDIs). We planned IDIs for 13 PLHIV, who returned to care, and increased to 21 to reach saturation. For treatment supporters we planned to interview 9 individuals but reached saturation only at 13. Furthermore, we conducted three FDGs, one per health facility. Each FGD consisted of 6–8 healthcare workers working in HIV care and treatment centers. This brought together a total of 34 healthcare workers.
Inclusion and Exclusion Criteria
We included adult PLHIV who returned to care after missed clinical visits for at least three months from the last scheduled appointment and missing ART intake for more than 60 days within the 90 days prior to return to care. Participants were enrolled in the study on the day they returned to care. Treatment supporters - relatives and next of kin were eligible if they took care of PLHIV who had dropped out and returned to care. Healthcare workers caring for PLHIV from all five health centers were eligible if they had an experience of at least 12 months. All participants signed an informed consent for study participation. Exclusion criteria were those who could not express themselves due to illness.
Data Collection Procedures
For all IDIs, healthcare workers at the respective study sites were informed of the project and supported the identification of eligible participants.PLHIV fulfilling inclusion criteria were identified upon return to care based on documentation of the last visit and self-reported adherence together with documentation of pharmacy drug refill records. After consenting to voluntary participation, interviews were conducted in Swahili in separate rooms at the clinic to ensure confidentiality. Study participants received a unique identification number to maintain anonymity. Confidential audio records remained accessible solely to the research team with findings not revealing individual identities. For both IDIs and FGDs, topic guides were designed based on previous studies and aligned with study objectives. The guide was piloted with 5 PLHIV not included in this study.
Topics explored for both IDI and FGD with PLHIV, treatment supporters, and health care workers included i) reasons for PLHIV dropping out from care, ii) factors for returning to care, iii) reasons to remain in care, and iv) reasons for adhere to treatment. For both IDIs and FGDs, three researchers with social science skills (HM, LS, and SL) facilitated the discussions using the Swahili language. Responses were audio recorded, and field notes were taken during the sessions. All interviews ranged from 30 to 60 minutes. Saturation was reached after conducting 21 in-depth interviews (IDIs) with people living with HIV (PLHIV), 13 IDIs with treatment supporters, and 5 focus group discussions (FGDs) with 6–8 healthcare workers each,34–38 as no new themes emerged from the data.39–41 This resulted in a total of 34 health care workers being interviewed collectively across all focus groups.
Data Management and Analysis
Audio recordings of the IDIs and FGDs were transcribed verbatim in Swahili language. Field memos were incorporated into the written transcripts. Transcripts were read multiple times for familiarization and subsequently verified against the recordings for accuracy and consistency.35,40,41 Thematic analysis was conducted using NVivo 12 software. Initial codes were generated from the data, which were then grouped into themes through a collaborative process involving multiple researchers to ensure accuracy and reliability.35,40,41 All transcripts were analyzed using Nvivo 12 plus software42 in the Swahili language, and only selected quotes supporting the theme were translated into English. Deductive codes were developed from IDI and FGD guidance, while inductive codes emerged from the data.43 HM generated the initial codebook and data coding, which was then reviewed by HM, LS, SL, RN, SN, and EL, who coded independently. Discrepancies in coding were resolved through negotiation to reach a consensus, and similar codes were grouped into sub-themes.44,45 Merged themes described the factors associated with dropping out, returning to care, retention, and treatment adherence to ART among PLHIV. A thematic framework analysis was used to analyze the data.46,47
Results
The median age of the 21 people living with HIV (PLHIV) was 40 years (range 21–63); 10 (47.6%) were females and 11 (52.4%) males. A majority of participants were self-employed in subsistence farming (20; 95%); 12 (57%) had a primary education. Among 13 treatment supporters, 8(61.5%) were female and 5 (38.5%) male; the average age was 43 years (range 28–61), with the majority being self-employed (11; 84.6%) and having a primary education (7; 53.9%). Healthcare workers were 18 (54.6%) females and 15 (45.4%) males, predominantly nurses 14 (41.2%) (Tables 1 and 2).
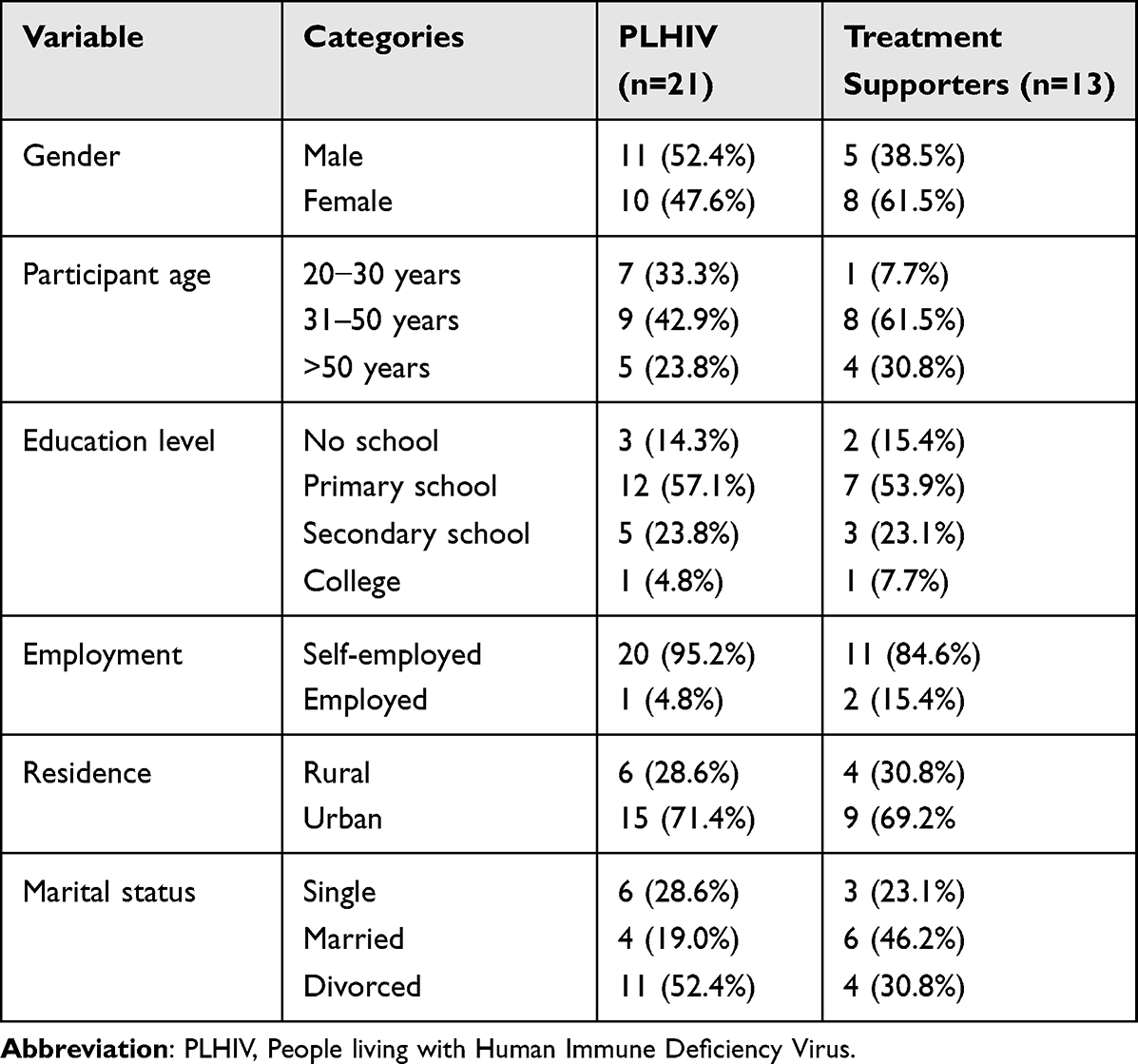 |
Table 1 Sociodemographic Characteristics of Study Participants for In-Depth Interview |
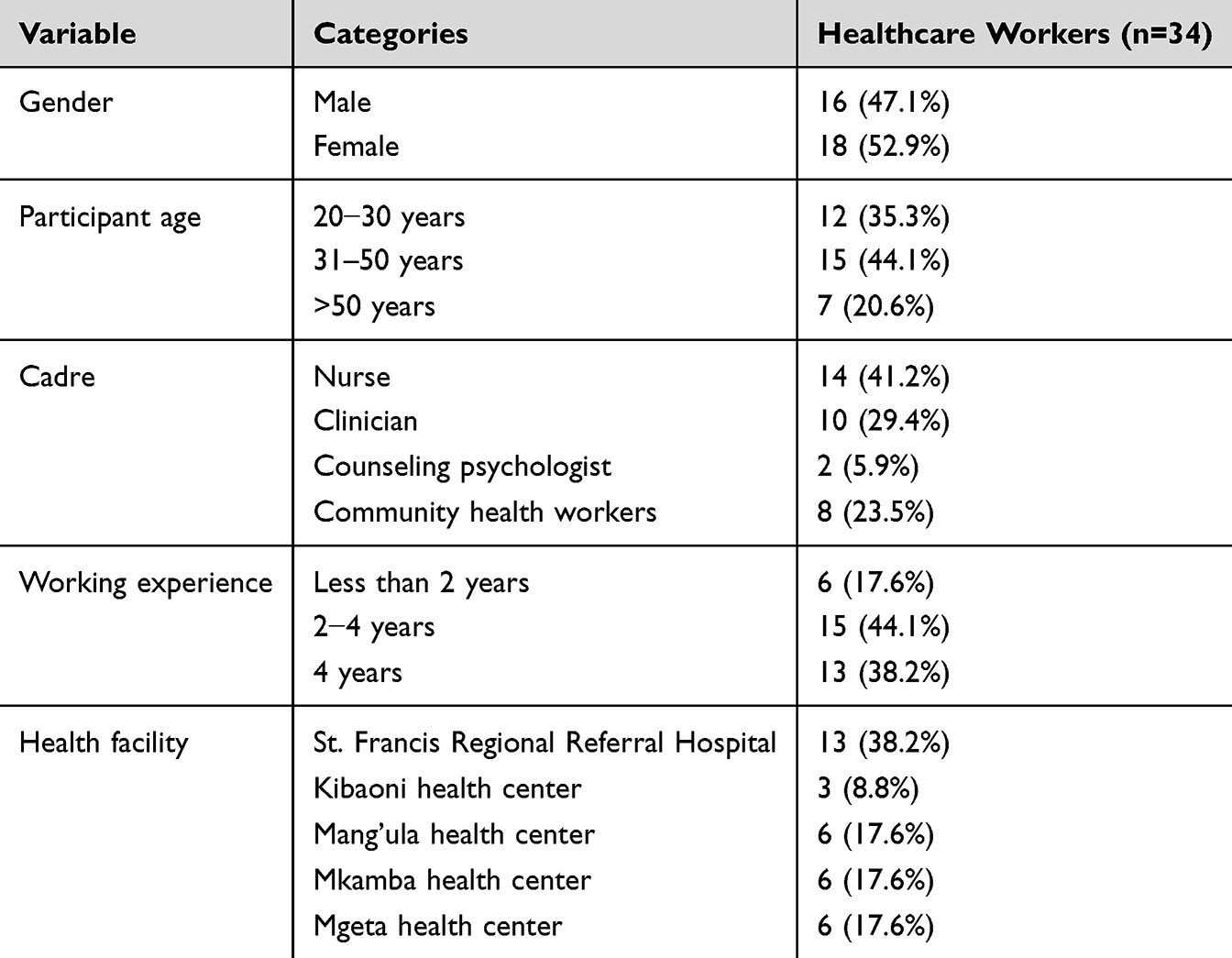 |
Table 2 Sociodemographic Characteristics of Study Participants for Focus Group Discussions |
Factors Associated With Retention in Care, Drop-Out From, Return to Care, and Treatment Adherence
Table 3 presents the factors categorized into reasons for dropping out, returning to care, retention in care, and treatment adherence. It shows the perceived experiences of PLHIV, along with the perspectives of their supporters and healthcare workers.
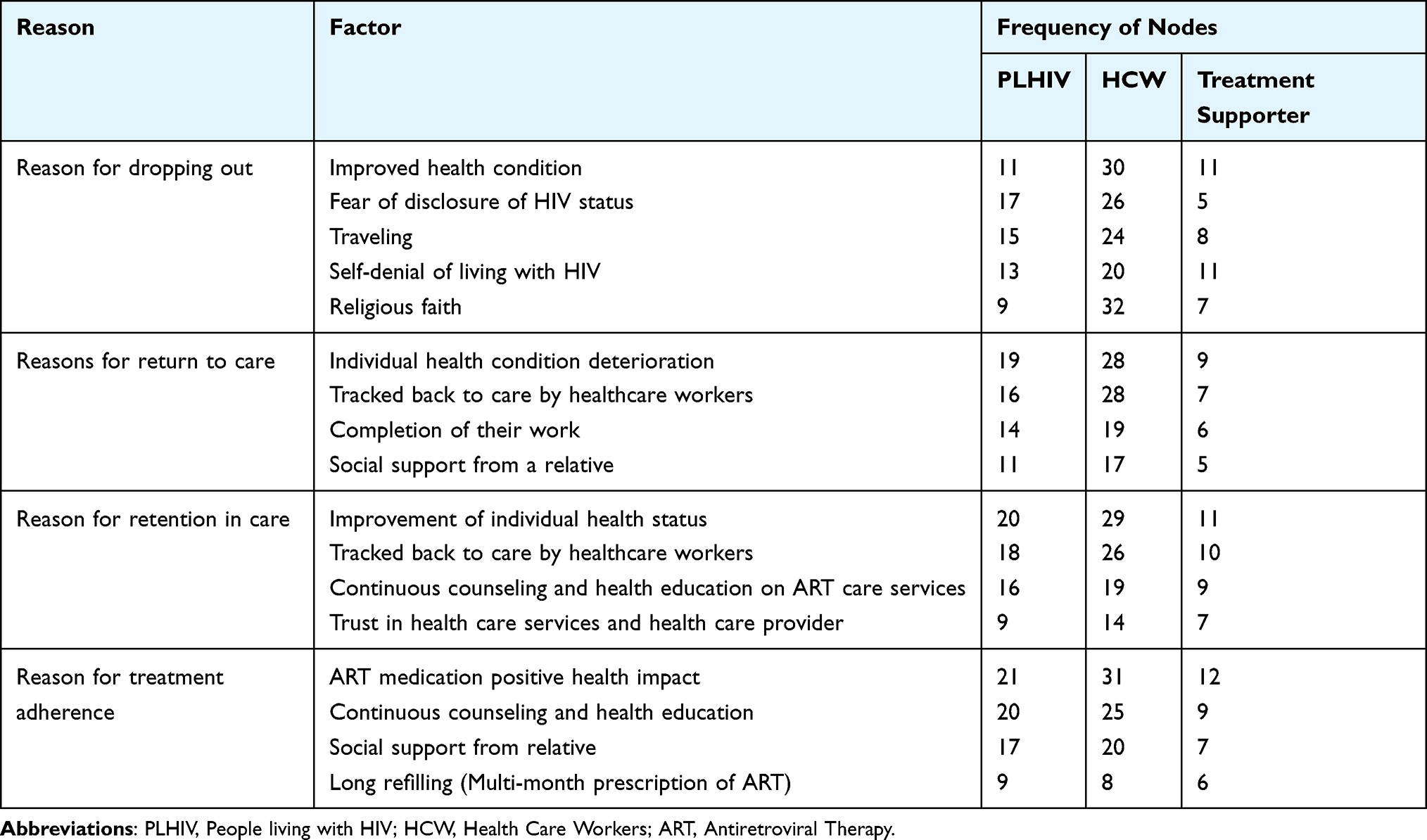 |
Table 3 Factors Contributing to Dropout, Return to Care, Retention, and Treatment Adherence: Lived Experiences of PLHIV and Perspectives of Supporters and Healthcare Workers |
Reasons Indicated for Dropping Out of ART Care Services
Improved Health Conditions
A majority of PLHIV along with their treatment supporters and healthcare providers reported that improvement in health after starting ART was the main reason for discontinuing ART intake and stopping attendance at HIV care services. Some PLHIV felt cured and thought it was unnecessary to continue adhering to their clinic appointments. A PLHIV stated.
“After using ART for some time, my health greatly improved, and I no longer needed to visit the clinic. Because I felt completely healthy and strong, I continued my farming activities without any health problems” (Female PLHIV, 62 years)
Healthcare providers also reported
“Some of our patients believe they are cured when their CD4 count improves, they gain weight, and their skin is nourished. They do not understand that ART is a lifelong treatment and that stopping it can have serious consequences” (Female HCP, 30 years)
Furthermore, treatment supporters observed that:
“For instance, my sister-in-law said: ‘I did not need these drugs. I am stronger and healthier now.’ She didn’t understand that stopping treatment would make her sick again. She felt cured”. (Female treatment supporter, 48 years)
Fear of Disclosing HIV Status
A majority of PLHIV, treatment supporters, and healthcare providers reported fear of disclosing HIV status because of the potential rejection and stigmatization. Many PLHIVs perceived stigma and discrimination from families, spouses, and workplace communities, which led some to decide to stop their ART services to hide their HIV status. PLHIV. They struggled to take ART and visit clinics discreetly. Healthcare providers and treatment supporters identified self-stigma, community stigma, and discrimination as major barriers to accessing ART care among PLHIV. A PLHIV was reported:
“I had to hide my pills in a different container and take them when no one was looking. I felt like I was living two separate lives. I was afraid they would treat me differently if they found out” (Male PLHIV, 22 years)”
Other PLHIV feared partner rejection, which caused some to stop attending clinics and taking ART.
“I had feared that my partner might reject me if he learned about my HIV status. That is why I stopped attending clinical visits and taking ART” (Female PLHIV, 38 years)
Treatment supporters also reported.
“They (PLHIV) reported to have felt lonely and ashamed. They were afraid of the consequences of disclosing their status, such as losing their loved ones and their dignity” (Female, HCW,45 years)
Moreover, healthcare providers reported:
“Some people living with HIV avoided visiting the clinic or taking their medication regularly. They believed they could avoid stigma and discrimination but were still putting themselves at risk”. (Female, treatment supporter,48 years)
Traveling
A majority of PLHIV and healthcare workers reported that traveling and engaging in other obligations were common reasons for discontinuing ART and stopping attending clinics, sometimes due to losing their CTC cards or not knowing how to transfer their care to another healthcare facility. Some PLHIV faced challenges such as losing their SIM card registered at the CTC for communication, telephone network issues, and floods during the rainy season, making it hard to access ART facilities. One PLHIV said:
“I got medicine for six months and went to Tunduma for work. But I forgot to bring my CTC card with me. My boss delayed my payment and return. That made me miss my ART care service the entire time”. (Male PLHIV, 52 years)
Also, healthcare workers stated.
“Some PLHIV drop out of ART care because they move to other areas. They face barriers such as a lack of nearby ART services, a CTC card left at home, or ignorance of how to get services elsewhere”. (Female HCW, 48 years)
Self-Denial of Living With HIV
A majority of PLHIV, treatment supporters, and healthcare workers reported that self-denial about their HIV status was a primary reason for dropping out of ART care services. Many PLHIV felt overwhelmed by embarrassment and guilt, often attributing their infection to personal failures. Some held erroneous beliefs about HIV/AIDS equating it with moral degeneracy, which exacerbated their reluctance to accept their diagnosis. This struggle led to intermittent ART engagement, neglect of medication, and ultimately dropping out of care as they sought to escape the stigma associated with HIV. Treatment supporters and healthcare workers also recognized this factor as the main reason for PLHIV’s discontinuation of care. One participant shared her struggle:
“I did not believe I had HIV. I thought it was a testing mistake. I only had sex with one person in my life. How could I get HIV? I refused to attend my treatment visit. I was in denial “. (Female PLHIV, 43 years)
Additionally, treatment supporters reported
“He (the son) was born with HIV and was taking ART medication when he was unaware of his HIV status. However, after learning his diagnosis, he denied living with HIV and stopped his treatment”. (Female treatment supporter, 40 years)
Healthcare workers acknowledged self-denial as a common factor in PLHIV dropping out of ART care as noted by a healthcare worker.
“They did not want to accept their condition or let anyone know. They avoided coming to the clinic or taking their drugs regularly. They thought they could escape the stigma and discrimination, but they were only putting themselves at risk”. (Male HCW, 61 years)
Religious Faith
A majority of PLHIV along with their treatment supporters, and healthcare workers reported that religious faith was a common reason for PLHIV to stop attending ART services. Some PLHIV believed that prayer and application of a specific oil by the religious leader could cure HIV, which led them to stop attending clinical visits and take ART. However, many returned to care when their condition worsened. One PLHIV reported:
“I stopped my HIV treatment because a radio pastor said prayer and oil could heal me. I met him in Dar es Salaam and got his blessing. Then, I stopped my clinic visits from October 2021 to June 2023”. (Male PLHIV, 55 years)
Healthcare workers report
“A couple of PLHIV discontinued their medicine and stopped attending clinical visits. They opted for prayer and a spiritual healer. They told us to leave them alone. We could not assist them any longer”. (Female HCW, 30 years)
Moreover, treatment supporters reported this factor as significant
“He used oils and prayers to cure his HIV, but he failed. He came back to his treatment when his condition worsened”. (Female treatment supporter,48 years)
Factors Associated With Return to Care
An important factor to return to ART care services was the deterioration of the health condition with symptoms or complications. But also completion of work which had led to treatment interruption was a reason. Support from the relatives and being tracked by healthcare workers convinces some participants to come to the clinic. The quotes below from the participants, including PLHIV, treatment supporters’, and healthcare providers, support these findings.
Individual Health Condition Deterioration
A majority of PLHIV, treatment supporters, and healthcare workers reported that individual health decline was a common factor for returning to ART care. Most PLHIV returned to care after experiencing opportunistic illnesses related to HIV. The fear of death and serious health complications, along with the desire to recover, motivated them to seek medical attention. Treatment supporters and healthcare workers observed similar trends, noting that many PLHIV returned to care due to these fears and experiences of HIV-related illnesses. One PLHIV who returned to care reported
”My health decline led me back”. (Female PLHIV, 62 years)
Also treatment supporters reported
“My brother underestimated his treatment and stopped taking it for several months. He decided to return to care when he experienced frequent fevers and skin rashes for several weeks”. (Male treatment supporter, 42 years)
Healthcare workers reported:
“Most of our clients came back to care when they felt sick with symptoms like frequent persistent coughing, rashes, fever, weight loss, and other HIV-related illnesses. They returned to a health facility that could treat their illness”. (Male HCW, 43 years)
Tracking Activities by Healthcare Workers
Some PLHIV, treatment supporters, and healthcare workers reported that tracking the activities of healthcare workers, including follow-up calls and home visits by healthcare workers, was crucial in facilitating PLHIV to return to care after missing appointments. Additionally health care workers reported other approaches were used such as client home-based services, phone calls, and community mobilization which facilitating PLHIV return to care. One PLHIV shared.
“I felt sad and ashamed. When healthcare workers tracked me by calling me and making a home visit, I noticed they acted differently. I realized they truly cared about my well-being”. (Female PHIV,43 years)
Moreover, healthcare workers acknowledged the track-back-to-care approach as vital in returning PLHIV to ART care. A treatment supporter reported:
Our track-back-to-care strategy involves phone calls, client follow-up using Client Home-Based Services, and regular counseling. These interventions have encouraged our clients to return to care and adhere to their treatment”. (Female HCW, 30 years)
Completion of Work
Some PLHIV, treatment supporters, and healthcare workers identified fulfilling work or personal obligations as a key factor influencing the return to ART care. People living with HIV often balance competing priorities, such as earning a living, farming, or running mobile businesses, which they perceive as necessitating temporary breaks from ART. After completing these tasks, they reassess their health and recognize the importance of returning to care. This observation was across all study groups, with PLHIV, treatment supporters, and healthcare workers acknowledged that completing work was a main influences factor for some PLHIV’s return to ART care. A PLHIV resumed care after fulfilling their obligations reported:
“I returned to my ART care service, after completing several months managing a rice farming operation as a tractor supervisor, because it was hard to leave the work behind”. (Male PLHIV, 32 years)
Also, a treatment supporters reported
“My son returned to his ART care services after finishing his farm activities where he had gone to cultivate rice”. (Male treatment supporter, 58 years)
Moreover, a healthcare worker explained.
“They returned to ART care services after completing their remoted work such as fishing and rice farming and came back to their residency area, where they had family and friends and accessible ART care to support them”. (Female HCW, 56 years)
Social Support From Relatives
A majority of PLHIV, treatment supporters, and healthcare workers reported that social support from relatives played a crucial role in helping PLHIV re-engage with ART care. Family support, including assistance with food and transportation costs, motivated PLHIV to return to care. Healthcare workers confirmed strong family networks facilitated re-engagement, with practical aid, emotional support, and financial assistance having a positive impact. Treatment supporters also emphasized that positive family relationships helped PLHIV overcome barriers and adhere to their treatment plans. One PLHIV shared:
“I committed to returning to ART care services and continuing with ART care because my children were encouraging me and they would assist me with food, transportation costs, and other expenses”. (Female PLHIV, 62 years)
One of the healthcare workers stated:
“Our clients returned to care after their relatives, which included family members and partners, had influence. Support consisting of practical aid, emotional control, and help with healthcare costs propelled them back to ART care services”. (Female HCW, 35 years)
Also, treatment supporters stated:
“I told him that we had to go to the hospital together. I am committed to supporting you in any case, but I need you to resume your ART care services for your relief and to stay healthy”. (Female treatment supporter, 49 years)
Factors Associated With Retention in ART Care Among PLHIV Returned After Missed Clinical Visits as Well as Irregular ART Intake
People living with HIV remained in their ART care services after being interrupted for more than three months because of the perceived experience of improvement of individual health condition, trust in health care services, and health care workers, in addition to the regular counseling, health education, social support, and client follow-up and tracking services they received.
Improvement of Individual Health Status
A majority of the PLHIV, along with their treatment supporters and health care workers reported that getting well from HIV-related illness since returning to ART care services, were motivated them to remain in ART care services. Because, improvements in health such as such as weight gain, skin nourishment, and no frequent fever, served as a powerful reinforcement for PLHIV, encouraging remain in ART services and treatment adherence as a PLHIV stated:
“I felt weak and hopeless when I was sick from an HIV-related illness. But after I came back to ART care, I started to feel better and stronger. I don’t want to go back to that dark place again. That’s why I remain on ART care services”. (Male, PLHIV,21 years)
Also, optimal well-being factors were acknowledged by treatment supporters, a treatment supporter stated:
“He was motivated to stay in care because of the well-being improvement he saw since returning to his ART care after discontinuing treatments”. (Male treatment supporter,42 years)
Moreover, healthcare workers highlighted that individual health improvements played a key role in sustaining ART care among PLHIV who had returned to care, as one healthcare worker noted:
“They were motivated to stay in care because of the individual health improvements they experienced since they returned to ART services”. (Male HCW,29 years)
Tracking Activities by Healthcare Workers
A majority of PLHIV reported that regular follow-up by health workers was a main contributing factor to remaining in ART care among people living with HIV who returned to care. Text messages or calls by healthcare workers helped PLHIV to attend visits and drug intake, as a PLHIV shared.
“I appreciated how they cared for me. They called me or texted me to remind me of my appointments. Sometimes, I forgot or felt too tired to go, but they encouraged me to keep up with the ART care services”. (Female PLHIV, 43 years)
Moreover, as a healthcare worker reported.
“We followed up with our clients regularly by messaging or calling them as well as using community healthcare workers to communicate with them confidentially and conveniently. We made them feel valued and respected” (Female, HCW,40 years)
Counseling and Health Education on ART Care Services
A Majority of PLHIV, Treatment supporters and healthcare workers reported that continuous counseling and health education enabling PLHIV to return to care and remaining n care. This empowerment through knowledge of their status, treatment options, and adherence importance motivated them to remain in care and adhere to ART medication, as a PLHIV reported
“I was able to get back on track with my ART care services after receiving counseling from the nurse and doctors. They helped me understand the importance of remaining in ART care services and how it can help me live a healthy life”. (Male PLHIV,59 years)
Also, one treatment supporter stated:
“Once he returned to the care and received counseling from healthcare providers, he was encouraged to adhere to his treatment”. (Male treatment supporter,58 years)
Moreover, a healthcare worker reported
“Combining health education and counseling granted patients command over their health, turning them into champions for their well-being and overcoming negative stereotypes. Working closely with patients ensured they understood the severity of HIV and the life-saving capabilities of ART, reigniting the healthcare workers’ enthusiasm for nursing”. (Male, HCW,58 years)
Trust in Healthcare Services and Healthcare Workers
A majority of PLHIV and healthcare workers mentioned that Trust in healthcare services and healthcare workers is a crucial factor in PLHIV’s continuation of ART care services, particularly among those who had previously missed clinical visits or had irregular ART. Strong trust in healthcare services and workers encourages retention in ART services, as it fosters a sense of respect, dignity, and support. A PLHIV reported:
“I trusted the health care services and workers here. They respected and dignified me. They explained my condition and medication. They supported me through challenges and difficulties. That’s why I returned to the clinic and followed their advice” (Male PLHIV,59 years)
Furthermore, A healthcare worker reported:
“Our patients trusted us, which was fundamental in retaining the ART care services. We tried to build trust with our patients by providing quality care and education. We listened to their concerns and needs and offered them psychosocial support. They were motivated to remain in their ART care service despite missing visits or experiencing irregularities”. (Female, HCW,30 years)
Social Support From Family Members
A majority of PLHIV, along with their treatment supporters, and healthcare workers reported that encouragement and support from family members played a significant role in PLHIV remaining in their care and adhering to ART medications after missing clinical visits and having irregular ART for some time. Some of the social support includes emotional and psychological support, practical support, reminders, coping strategies, logistical assistance, and financial support, which motivated PLHIV to remain in care. One of PLHIV’s reported:
“My grandmother reminded me to take my medications, and in some cases, she even went with me to the clinic. She was also helping me cope with the stigma and the side effects. she made me feel like I wasn’t alone”. (Male PLHIV,21 years)
Additionally, another PLHIV said:
“My children supported and encouraged me to remain in ART care service after I came back to the health facility” (Female PLHIV,43 years)
Also, healthcare workers reported.
““HIV patient relatives played a crucial role in ensuring that their brother/sister continued to receive ART services by providing various forms of assistance, such as through providing meals or staying close, to motivate their brother/sister to adhere to HIV treatment”. (Female, HCW,34 years)
Moreover, a treatment supporter reported that:
“I supported and encouraged him, including reminding him to take medications, providing food, and covering some expenses. I was committed to ensuring his well-being and continued managing his economic activities as usual”. (Female treatment supporter,30 years)
Factors Associated With Medication Adherence After Return to Care
The majority of participants reported that PLHIV adhered to their treatment after missing for some time because they received counseling and health education from healthcare providers and family support. They also long-refilled drugs, reduced side effects, and felt better from ART medication.
Positive Impact of ART Medication
A majority of PLHIV, treatment supporters, and healthcare workers reported that the positive impact of ART medication on health outcomes was a key motivator for PLHIV to adhere to treatment after having irregular ART.Most PLHIV who resumed ART experienced improved health outcomes such as weight gain, skin nourishment, and reduced frequency of HIV-related illnesses. This positive change motivated them to continue adherence to treatment, a PLHIV reported.
“Before restarting ART medications, my health was not enjoyable. Since I resumed ARVS, I have experienced significant positive changes, including freedom from frequent HIV-related illnesses. I followed my doctor’s ART prescription”. (Male, PLHIV,38 years)
Also, treatment supporters reported
“Ever since he resumed ART, he has felt better in his body, gained weight, and worked on income-generation activities. That motivates him to take his drugs o” time (Male treatment supporter,52 years)
Moreover, healthcare providers reported:
“Positive health condition improvements, e.g., weight gain and reduced frequent HIV-related illness, motivated clients to continue treatment after resuming antiretroviral therapy”. (Female HCW,57 years)
Counseling and Health Education
A majority of PLHIV, along with their treatment supporters and healthcare workers, reported that ongoing counseling and health education were essential in motivating PLHIV to resume care and adhere to ART medication after irregular treatment. One PLHIV reported:
“Counseling and health education were crucial in my successful return to ART care services. They not only taught me the significance of taking my medication as prescribed, but they also instilled confidence and hope in me, giving me reasons to fight for my health and well-being”. (Male PLHIV,21 years)
As well, treatment supporters reported:
“Once he returned to care and received counseling from healthcare providers, he was encouraged to adhere to his treatment “(Male treatment supporter,58 years)
Moreover, a healthcare worker reported that:
“Interacting with PLHIV and witnessing their transformation through regular counseling and health education is incredibly gratifying. Seeing them regain control over their health and becoming advocates for their well-being is a testament to the importance of our combined efforts in fighting against HIV and stigma”. (Female, HCW,33 years)
Social Support From Family Members
A majority of PLHIV reported that encouragement and practical support from family members or close relatives played a crucial role in motivating PLHIV to adhere to treatment after irregular ART. Similarly, healthcare workers acknowledged that relatives and other family members motivating treatment adherence, while a treatment supporters detailed their commitment to providing reminders, food, and financial support to ensure the well-being of their relative. A PLHIV said:
“My grandmother reminded me to take my medications, and in some cases, she even went with me to the clinic. She was also helping me cope with the stigma and the side effects. she made me feel like I wasn’t alone”. (Male PLHIV,21 years)
One of the healthcare workers reported:
“Their family members, such as partners or children, actively encouraged and motivated people living with HIV to ART medication adherence. These people living with HIV returned to care after interrupting ART medication for some time”. (Female HCW,46 years)
Moreover, a treatment supporter reported that:
“I supported and encouraged him, including reminding him to take medications, providing food, and covering some expenses. I was committed to ensuring his well-being and continued managing his economic activities as usual”. (Female, treatment supporter,30 years)
Long refilling ART Medication
Some PLHIV, and healthcare workers reported that long ART medication refills motivated adherence among PLHIV returning to care after missing ART services. The long refilling of multi-month prescriptions significantly reduced the number of clinical visits, transportation costs, and chances of being exposed as HIV-positive in the community, which led to lowered stigma and discrimination. One person living with HIV reported:
“I wanted to qualify for the long refilling group, so I followed my ART treatment faithfully. That allowed me to work on my farm without any hassle as well as reduce the number of clinical visits used to seek ARVS drugs”. (Male PLHIV,32 years)
As well, a healthcare worker stated.
“They were motivated to adhere to their treatment to qualify for long-term refills of medication” (Male, HCW,50 years)
Discussion
In this study, the qualitatively assessed main reasons PLHIV indicated for care interruptions after coming back to care were improved health, fear of HIV disclosure, work-related travel, self-denial of living with HIV, and religious faith influences. Factors to support linking back to care were health deterioration, being tracked by healthcare workers, completion of work obligations leading to interruption of care, and social support from a relative. Furthermore, the reasons to remain in care were the experience of improved individual health, being contacted by healthcare workers for the next visit, counseling and health education on ART care services, and trust in healthcare services and healthcare providers. Similarly, the factors that positively impacted ART adherence were included ongoing counseling and health education from healthcare providers and felt better from ART medication. Also, Social support from family members and long-refilled drugs.
Our study finding, that improved health condition was a major factor contributing to PLHIV dropping out of ART care services is consistent with previous studies that described feeling healthy or asymptomatic as a major barrier to ART retention and treatment adherence among PLHIV.48,49 This demonstrates a lack of understanding regarding the significance of lifelong HIV treatment, the risks of treatment interruptions,50 and the need for ongoing health education and counseling, regardless of the health condition.
Another reason for dropping out of ART care was the fear of disclosing HIV status, which was associated with the experience of stigma, discrimination, and rejection from relation partners, family, or friends. Previous studies described stigma, discrimination, and disclosure as causes for non-retention and poor treatment adherence.51,52 This indicates that the community still has negative perceptions of PLHIV. Psychological support and empowerment to cope with the stigma of PLHIV, as well as interventions to reduce HIV-related stigma and discrimination in the community are urgently needed.
Traveling for work made some PLHIV drop out of ART care services, as they could not access it in their new or remoted area like in farming activities. This finding is consistent with previous studies that describe migration, and mobility were barriers to HIV care and treatment among PLHIV.53–55 This finding implies that PLHIV requires more flexible and convenient HIV services to allow for mobility patterns like longer refill times and electronic referral systems. Religious faith as a reason for dropping out of ART care has been identified in previous studies.56–58 These findings indicate that respectful and culturally sensitive counseling and health education regarding their religious perspectives are vital to promoting health-seeking behavior57 in lifelong HIV treatment care.
Main reason to come back to care was a deterioration of health, which is consistent with previous studies.37,58,59 However, some previous studies found that individual health deterioration was a barrier to HIV care and treatment.60 This may reflect the different perceptions and experiences among PLHIV, who returned to care after dropping out, compared to PLHIV who never dropped out. It implies that PLHIV who discontinue ART care services require individualized interventions and methods to solve their specific challenges and needs. Another reason for returning to care was tracking by healthcare workers with encouragement to resume ART. This is consistent with previous reports61,62 and supports current practice.
The challenge of competing life activities such as farming and fishing in this study area, where rice cultivation is the major economic activity, shows the challenge of long distances to the next clinic and time-consuming clinic visits. Also, this finding is consistent with previous studies37,63 and reinforces the need for extended clinic hours, or weekend services besides long ART refilling periods. Additionally, decentralized dispensing models, like community-based distribution points or mobile clinics, enhanced access for rural PLHIV, tackling distance and work-related barriers Its benefits of this approach have been documented in improving retention and adherence among PLHIV’s distinct challenges in rural areas.64–66 Similar, to previous published studies described social support from a relative, such as a spouse, or parent, motivating and encouraging PLHIV to return to ART care after missing care for some time.67 This demonstrated that PLHIV requires family and peer support to remain in care and treatment, and we should improve these interventions.
The personal experience of improving from a serious condition was a strong motivation factor for retention in care and treatment adherence. This finding is consistent with self-regulation theory68–70 and supports the health belief model,71–73 in which people adhere to healthcare effectively when they understand their health situation, risks, benefits, and challenges. Moreover, previous studies described that individual improved health played an important role in motivating PLHIV retention in care and treatment adherence.29,74 This finding suggests that PLHIV, regardless of their health status, require ongoing counseling and education on the importance of lifelong HIV treatment.
Another finding of this study was that health education and counseling on HIV care and treatment were perceived as important support for retention and treatment adherence among PLHIV returned to care. Similarly, previous studies described that counseling and health education played an important role in increasing knowledge and could change negative attitudes toward PLHIV increasing self–efficacy and treatment adherence.75,76 This finding implies that PLHIV who returned to care after missing require counseling and education that respects their culture and needs. In addition, previous studies5–75,77,78 and our work show, that trust in healthcare services and healthcare workers play a vital role in retention in ART care services and treatment adherence among PLHIV returned to care. This finding indicates that PLHIV requires reliable and accessible healthcare services and a trustful environment.
Interestingly, our study shows that long refilling strategies - which are multi-month prescriptions and dispensing - motivate PLHIV to good treatment adherence. This strategy reduces the number of clinical visits, which leads to transportation cost savings, and reduces the chance of stigma exposures as well as health provider workload. Previous studies have shown that multi-month dispensing can influence retention in care and treatment adherence.79–81 This finding suggests that PLHIV requires convenient care services that are adaptable to their circumstance.
Healthcare workers and treatment supporters reported improved health leading to self-denial of HIV status as a cause for PLHIV discontinuing ART services. Conversely, a majority of PLHIV attribute dropout to stigma and fear of being labeled negligent. However, deteriorating health and proactive follow-up by healthcare providers are common reasons for PLHIV to re-engage in care. Also, healthcare workers view work completion as another significant motivator for return, few PLHIV report this. A majority of PLHIV, healthcare workers, and treatment supporters reported improved health status, tracked back to care, and continuous counseling and health education promoted retention and treatment adherence. A majority of PLHIV and healthcare workers indicated trust in healthcare services and providers, as well as long refilling periods, were also mentioned as factors promoting retention and adherence.
Even though the main study objective was achieved, our study has some limitations including limited generalizability and transferability to other settings. Second, the study relied on self-reported data that may introduce recall and desirability bias. Third, the study excluded PLHIV who never returned to care, which could disclose different perspectives on why they stopped and what barriers to returning to care. Fourth, our study explored the influence factors on retention and treatment adherence among PLHIV who returned to care but we did not measure retention and treatment adherence in this study. Finally, our study primarily focused on reporting the experiences and views of PLHIV from the perspectives of treatment supporters and healthcare workers, rather than directly capturing their personal views.
Conclusion
The study underscores the factors that impede patients to adhere to treatment schedules. Specifically, counseling and educational programs as well as psychological support aiming at stigma reduction are areas for interventions to improve clinic and treatment adherence. Implementing flexible care models, proactive re-engagement strategies like active tracking of those lost to follow-up, fostering partnerships with religious leaders, and involving families can significantly improve retention rates and adherence to antiretroviral therapy (ART), leading to good health well well-being of people living with HIV (PLHIV). The study also highlights the need to address persisting stigmatization, leverage strong family and social support, and focus on interventions that improve retention in lifelong treatment and treatment adherence. Additionally, facilitating access to remote drug pickup might improve their retention and adherence to lifelong treatment.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ART, Antiretroviral Therapy; CDCI, Chronic Disease Clinic Ifakara; HIV, Human Immune Deficiency Virus; IHI-IRB, Ifakara Health Institute-Institutional Review Board; NIMR, National Institute of Medical Research; PLHIV, People Living with HIV; KIULACO, Kilombero, and Ulanga Antiretroviral cohort; MMD, Multi-month prescription and dispensing.
Data Sharing Statement
The datasets used and analyzed in this study are available upon reasonable request from the corresponding author.
Ethical Consideration
Ethical approval was granted by the institutional review board of Ifakara Health Institute (Ref: IHI/IRB/No: 34-2023). This study was carried out in accordance with the ethical principles of the Declaration of Helsinki.82 Before participation, researchers informed potential study participants about the study’s purpose and procedures. Those who agreed to participate provided written informed consent, ensuring their understanding of the study’s purpose and rights. Informed consent included consent for the publication of anonymized responses and direct quotes. The researcher retained one copy of the signed consent form, and the participant received the other.
Acknowledgments
We extend our gratitude to those who contributed to this study, including the study participants, healthcare facilities in charge, and CTC healthcare workers for their cooperation. We are also grateful to the KIULACO study group, the Ifakara Health Institute, and The Nelson Mandela African Institute of Science and Technology, for their support.
Collaborators
Author Contributions
All authors made significant contributions throughout the study process, including conception, study design, data collection, and analysis and interpretation of the results. They critically reviewed and approved the final draft for publication. The authors collaborated effectively, agreed on the journal for submission, and were accountable for the integrity of the entire work.
Funding
This study was funded by Ifakara Health Institute, training department.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Sheet F, Hiv N, Hiv N. UNAIDS, Fact sheet 2022 Global HIV Statistics. 1–6;Vol. 2022. https://www.unaids.org/en/resources/fact-sheet.
2. Global U, Update A. The Path That Ends; 2023.
3. Time F, Hm Y, Cranfield University, et al. Global Health Sector Strategies on,Respectively,HIV,Viral Hepatitis and Sexually Transmitted Infection for the Period 2022-2030. 33. 2022.
4. National Bureau of Statistics. Tanzania Hiv Impact Survey (This) 2016-2017. Vol. 2017; 2018:2016–2017
5. National Bureau of Statistics. Tanzania HIV impact survey(THIS) 2022/2023. 2023;2023:6–9.
6. Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S, Mahalingam S. Adherence to Antiretroviral Therapy Among People Living with HIV. North American Journal of Medical Sciences. 2013;5(3):220–223. doi:10.4103/1947-2714.109196
7. Hogg RS, Heath KV, Yip B, et al. Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA. 1998;279(6):450–454. doi:10.1001/jama.279.6.450
8. Mocroft A, Vella S, Benfield TL, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. Lancet. 1998;352(9142):1725–1730. doi:10.1016/S0140-6736(98)03201-2
9. Frank T, Bärnighausen T, Graspa E, Jaffer Z, Marie-Louise N. High coverage of ART associated with decline in risk of HIV acquisition in rural KwaZulu-Natal, South Africa. Science. 2013;339(6122):966–971. doi:10.1126/science.1228160
10. Rodger AJ, Cambiano V, Phillips AN, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393(10189):2428–2438. doi:10.1016/S0140-6736(19)30418-0
11. UNAIDS. Prevailing agaist pandemics by putting people at the centre. World AIDS Day Rep 2020; 2021. 42–68. https://aidstargets2025.unaids.org/assets/images/prevailing-against-pandemics_en.pdf.
12. Muwanguzi M, Lugobe HM, Ssemwanga E, et al. Retention in HIV care and associated factors among youths aged 15–24 years in rural southwestern Uganda. BMC Public Health. 2021;21(1):1–8. doi:10.1186/s12889-021-11547-5
13. Mirzaei M, Farhadian M, Poorolajal J, Kazerooni PA, Tayeri K, Mohammadi Y. Life expectancy of HIV-positive patients after diagnosis in Iran from 1986 to 2016: a retrospective cohort study at national and sub-national levels. Epidemiol Health. 2018;40:1–7.
14. Mabunda K, Ngamasana EL, Babalola JO, Zunza M, Nyasulu P. Determinants of poor adherence to antiretroviral treatment using a combined effect of age and education among human immunodeficiency virus infected young adults attending care at letaba hospital hiv clinic, Limpopo Province, South Africa. Pan Afr Med J. 2019;32:1–14. doi:10.11604/pamj.2019.32.37.17722
15. Ndege RC, Okuma J, Kalinjuma AV, et al. Failure to return pillbox is a predictor of being lost to follow-up among people living with HIV on antiretroviral therapy in rural Tanzania. HIV Med. 2022;23(6):661–672. doi:10.1111/hiv.13223
16. Shah GH, Etheredge GD, Nkuta LM, et al. Factors Associated with Retention of HIV Patients on Antiretroviral Therapy in Care: evidence from Outpatient Clinics in Two Provinces of the Democratic Republic of the Congo (DRC). Trop Med Infect Dis. 2022;7(9):1–11. doi:10.3390/tropicalmed7090229
17. Ngarina M, Popenoe R, Kilewo C, Biberfeld G, Ekstrom AM. Reasons for poor adherence to antiretroviral therapy postnatally in HIV-1 infected women treated for their own health: experiences from the Mitra Plus study in Tanzania. BMC Public Health. 2013;13:1–9.
18. Peltzer K, Preez NF, Ramlagan S, Anderson J. Antiretroviral treatment adherence among HIV patients in KwaZulu-Natal, South Africa. BMC Public Health. 2010;10(1):1. doi:10.1186/1471-2458-10-111
19. Med A. Factors Influencing Adherence to Antiretroviral Therapy among HIV Infected Patients in Nyamagana-Mwanza, Northern Tanzania: a Cross Sectional Study. Int Arch Med Microbiol. 2018;1(1):10.
20. Bukenya D, Mayanja BN, Nakamanya S, Muhumuza R, Seeley J. What causes non ‑ adherence among some individuals on long term antiretroviral therapy ? Experiences of individuals with poor viral suppression in Uganda. AIDS Res Ther. 2019;16(1):1–9. doi:10.1186/s12981-018-0214-y
21. Vanobberghen F, Letang E, Gamell A, et al. A decade of HIV care in rural Tanzania: trends in clinical outcomes and impact of clinic optimisation in an open, prospective cohort. PLoS One. 2017;12(7):1–17. doi:10.1371/journal.pone.0180983
22. Letang E, Kalinjuma AV, Glass TR, et al. Cohort profile: the Kilombero and Ulanga Antiretroviral Cohort (KIULARCO) - A prospective HIV cohort in rural Tanzania. Swiss Med Wkly. 2017;147(July):1–9. doi:10.4414/smw.2017.14485
23. Wilkinson L, Grimsrud A. The time is now: expedited HIV differentiated service delivery during the COVID-19 pandemic. J Int AIDS Soc. 2020;23(5):2019–2021. doi:10.1002/jia2.25503
24. Kalinjuma AV, Glass TR, Weisser M, et al. Prospective assessment of loss to followup: Incidence and Associated Factors in a Cohort of HIV -Postive Adults in Rural Tanzania. Journal of the International AIDS Society. 2020; 23(3):e2546o. doi:10.1002/jia2.25460
25. Fuente-Soro L, López-Varela E, Augusto O, et al. Loss to follow-up and opportunities for reengagement in HIV care in rural Mozambique: a prospective cohort study. Med (United States). 2020;99(20):236. doi:10.1097/MD.0000000000020236
26. Gill VC, Krentz HB. Patient Perspectives on Leaving, Disengaging, and Returning to HIV Care. AIDS Patient Care STDS. 2015;29(7):400–407. doi:10.1089/apc.2015.0001
27. UNAIDS Joint United Nations Programme. Fast Track Ending the AIDS Epidemics by 2030. Vol. 2014:1–40. www.unaids.org.
28. Moser A, Korstjens I. Series: practical guidance to qualitative research. part 1: introduction. Eur J Gen Pract. 2017;23(1):271–273. doi:10.1080/13814788.2017.1375093
29. Id AM, Id IE, Rrt I, et al. Interventions to reengage people living with HIV who are lost to follow-up from HIV treatment programs: a systematic review. PLoS Med. 2022;19:1–26. doi:10.1371/journal.pmed.1003940
30. Blanco N, Lavoie MCC, Koech E, et al. Re-Engagement into HIV Care: a Systematic Review. AIDS Behav. 2022;26(1):132–146. doi:10.1007/s10461-021-03365-y
31. Imani B, Zandi S, Khazaei S, Mirzaei M. The lived experience of HIV-infected patients in the face of a positive diagnosis of the disease: a phenomenological study. AIDS Res Ther. 2021;18(1):1–8. doi:10.1186/s12981-021-00421-4
32. Mohanan P, Kamath A. Family support for reducing morbidity and mortality in people with HIV/AIDS. Cochrane Database Syst Rev. 2009;3:1. doi:10.1002/14651858.CD006046.pub2
33. Huston P, Rowan M. Qualitative studies Their role in medical research. Can Fam Physician. 1998;44:2453–2458.
34. Sandelowski M. Focus on Qualitative Methods Sample Size in Qualitative. Research in Nursing & Health. 1995;18(2):179–183. doi:10.1002/nur.4770180211
35. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
36. Chirambo L, Valeta M, Banda Kamanga TM, Nyondo-Mipando AL. Factors influencing adherence to antiretroviral treatment among adults accessing care from private health facilities in Malawi. BMC Public Health. 2019;19(1382):1–11. doi:10.1186/s12889-019-7768-z
37. Beres LK, Mwamba C, Bolton-Moore C, et al. Trajectories of re-engagement: factors and mechanisms enabling patient return to HIV care in Zambia. J Int AIDS Soc. 2023;26(2):14–18. doi:10.1002/jia2.26067
38. Lakens D, Ravenzwaaij DV. Sample Size Justification. Collabra Psychol. 2022;8(1):1–28. doi:10.1525/collabra.33267
39. Mogensen AC, Caswell GR, Trick MD. Application of integrated reservoir simulation and pipeline network modeling software to the Sexsmith gas-condensate field. SPE Proc - Gas Technol Symp. 1998;1998:291–297. doi:10.2118/40002-ms
40. Moser A, Korstjens I. Series: practical guidance to qualitative research. Part 3: sampling, data collection and analysis. Eur J Gen Pract. 2018;24(1):9–18. doi:10.1080/13814788.2017.1375091
41. Seale C, Gobo G, Guvbrium JF. Qualitative Research Practice. 2005.
42. Allsop DB, Chelladurai JM, Kimball ER, Marks LD, Hendricks JJ. Qualitative Methods with Nvivo Software: a Practical Guide for Analyzing Qualitative Data. Psych. 2022;4(2):142–159. doi:10.3390/psych4020013
43. Hennink MHIAB. Qualitative Research Methods. 2020;4.
44. Ka K, Cheung C, Tai KWH. The use of intercoder reliability in qualitative interview data analysis in science education ABSTRACT. Res Sci Technol Educ. 2021;2021:1–21. doi:10.1080/02635143.2021.1993179
45. Connor CO, Joffe H. Intercoder Reliability in Qualitative Research: debates and Practical Guidelines. Int J Qual Methods. 2020;19:1–13. doi:10.1177/1609406919899220
46. Goldsmith LJ. Using Framework Analysis in Applied Qualitative Research. Qualitative Rep. 2021;26(6):2061–2076. doi:10.46743/2160-3715/2021.5011
47. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide. Med Teach. 2020;1–9. doi:10.1080/0142159X.2020.1755030
48. Kim MH, Zhou A, Mazenga A, et al. Why did I stop? Barriers and facilitators to uptake and adherence to ART in option B+ HIV care in Lilongwe, Malawi. PLoS One. 2016;11(2):1–16. doi:10.1371/journal.pone.0149527
49. Kuznetsova AV, Meylakhs AY, Amirkhanian YA, et al. HHS Public Access Author manuscript. AIDS Behav. 2016;20(10):2433–2443. doi:10.1007/s10461-015-1282-9
50. Miller CM, Ketlhapile M, Rybasack-Smith H, Rosen S. Why are antiretroviral treatment patients lost to follow-up? A qualitative study from South Africa. Trop Med Int Heal. 2010;15(SUPPL. 1):48–54. doi:10.1111/j.1365-3156.2010.02514.x
51. Lailulo Y, Kitenge M, Jaffer S, Aluko O, Nyasulu PS. Factors associated with antiretroviral treatment failure among people living with HIV on antiretroviral therapy in resource-poor settings: a systematic review and metaanalysis. Syst Rev. 2020;9(1):1–17. doi:10.1186/s13643-020-01524-1
52. Liao B, Zhang XW, Wang JY, et al. Analysis of factors associated with dropping-out from HIV antiretroviral therapy in Kunming City, China. BMC Infect Dis. 2019;19(1):1–8. doi:10.1186/s12879-019-4658-z
53. Ayieko J, Thorp M, Getahun M, et al. Geographic Mobility and HIV Care Engagement among People Living with HIV in Rural Kenya and Uganda. Trop Med Infect Dis. 2023;8(11). doi:10.3390/tropicalmed8110496
54. Bernardo EL, Nhampossa T, Clouse K, et al. Patterns of mobility and its impact on retention in care among people living with HIV in the Manhiça District, Mozambique. PLoS One. 2021;16(5 May):1–14. doi:10.1371/journal.pone.0250844
55. Hendricks L, Eshun-wilson I, Rohwer A. A mega-aggregation framework synthesis of the barriers and facilitators to linkage, adherence to ART and retention in care among people living with HIV. Syst Rev. 2021;10:1–28.
56. Azia IN, Nyembezi A, Carelse S, Mukumbang FC. Understanding the role of religious beliefs in adherence to antiretroviral therapy among Pentecostal Christians living with HIV in sub-Saharan Africa: a scoping review. BMC Public Health. 2023;23(1):1–12. doi:10.1186/s12889-023-16616-5
57. Hernandez M, Gibb JK. Culture, behavior and health. Evol Med Public Heal. 2020;2020(1):12–13. doi:10.1093/emph/eoz036
58. Heo M, Agins BD. NIH Public Access; 2015. Vol. 66. 419–427. doi:10.1097/QAI.0000000000000171.Factors
59. Sariah A, Rugemalila J, Protas J, et al. Why did i stop? And why did i restart? Perspectives of women lost to follow-up in option B+ HIV care in Dar es Salaam, Tanzania. BMC Public Health. 2019;19(1):1–11. doi:10.1186/s12889-019-7518-2
60. Li L, Maiga AI, Maiga A, Costagliola D, Abgrall S, Pierre I. Re-engagement in care of people living with HIV lost to follow-up after initiation of antiretroviral therapy in Mali: who returns to. PLoS One. 2020;2020:687. doi:10.1371/journal.pone.0238687
61. Africa S, Id MAB, Davies N, Monareng S, Buthelezi F. Why do patients interrupt and return to antiretroviral therapy ? Retention in HIV care from the patient’s perspective in. PLoS One. 2021;1–15. doi:10.1371/journal.pone.0256540
62. Nabaggala MS, Parkes-Ratanshi R, Kasirye R, et al. Re-engagement in HIV care following a missed visit in rural Uganda. BMC Res Notes. 2018;11(1):9–13. doi:10.1186/s13104-018-3865-9
63. Chamberlin S, Mphande M, Phiri K, Kalande P, Dovel K. How HIV Clients Find Their Way Back to the ART Clinic: a Qualitative Study of Disengagement and Re ‑ engagement with HIV Care in Malawi. AIDS Behav. 2022;26(3):674–685. doi:10.1007/s10461-021-03427-1
64. Scale-up ASGFOR. Decentralized Distribution of Antiretroviral Therapy Through the Private Sector. 2019;Vol. 7200.
65. Targets M Decentralized Drug Distribution in Mozambique: Final Report. 2021;(2020):1–10.
66. Moiane J, Panguane B, Saturnino J, Alexandre J, Joaquim I, Prieto M. Decentralized Dispensing of ART at Private Pharmacies: Follow-up of Patients Enrolled in This Model in Four Provinces of Mozambique and Health Providers’ Perceptions of the Challenges and Benefits. 2022;Vol. 2022:1.
67. Buregyeya E, Naigino R, Mukose A, et al. Facilitators and barriers to uptake and adherence to lifelong antiretroviral therapy among HIV infected pregnant women in Uganda: a qualitative study. BMC Pregnancy Children. 2017;17:1–9. doi:10.1186/s12884-017-1276-x
68. de la Fuente J, Martínez-Vicente JM, Santos FH, et al. Advances on Self-Regulation Models: a New Research Agenda Through the SR vs ER Behavior Theory in Different Psychology Contexts. Front Psychol. 2022;13(July). doi:10.3389/fpsyg.2022.861493
69. Laulié L, Briceño-Jiménez G, Henríquez-Gómez G. Exploring self-regulation theory as a mechanism of the effects of psychological contract fulfillment: the role of emotional intelligence. Front Psychol. 2023;14(March):1–9. doi:10.3389/fpsyg.2023.1090094
70. Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Process. 1991;50(2):248–287. doi:10.1016/0749-5978(91)90022-L
71. Rosenstock IM. The health belief model and personal health behavior. Health Educ Monogr. 1974;2(4):354–386. doi:10.1177/109019817400200405
72. Green EC, Murphy EM, Gryboski K. The Health Belief Model. Wiley Encycl Heal Psychol. 2020;2:211–214. doi:10.1002/9781119057840.ch68
73. Kacunko S. Immediation. Artnodes. 2018;2018(21):154–176. doi:10.7238/a.v0i21.3154
74. Palacio-vieira J, Reyes-urueña JM, Imaz A, et al. Strategies to reengage patients lost to follow up in HIV care in high income countries, a scoping review. BMC Publ Health. 2021;21:1–11.
75. Mbuagbaw L, Mertz D, Lawson DO, et al. Strategies to improve adherence to antiretroviral therapy and retention in care for people living with HIV in high- income countries: a protocol for an overview of systematic reviews. BMJ Open. 2018;8(9):e022982. doi:10.1136/bmjopen-2018-022982
76. Chinyandura C, Jiyane A, Tsalong X, Struthers HE, McIntyre JA, Rees K. Supporting retention in HIV care through a holistic, patient-centred approach: a qualitative evaluation. BMC Psychol. 2022;10(1):1–9. doi:10.1186/s40359-022-00722-x
77. Kremer H, Ironson G, Porr M, et al. Spiritual and Mind – body Beliefs as Barriers and Motivators to HIV-Treatment Decision-Making. AIDS Patient Care STDS. 2009;23(2):127–134. doi:10.1089/apc.2008.0131
78. Nozaki I, Kuriyama M, Manyepa P, Zyambo MK, Kakimoto K, Bärnighausen T. False beliefs about ART effectiveness, side effects and the consequences of non-retention and non-adherence among art patients in Livingstone, Zambia. AIDS Behav. 2013;17(1):122–126. doi:10.1007/s10461-012-0221-2
79. Report F. A rapid assessment of multi-month dispensing of antiretroviral treatment and pre-exposure prophylaxis the Asia-Pacific region. AIDS Behav. 2020;2020:1.
80. Mantell JE, Zech JM, Masvawure TB, et al. Implementing six multi-month dispensing of antiretroviral therapy in Ethiopia: perspectives of clients and healthcare workers. BMC Health Service Res. 2023;23:1–19.
81. Hubbard J, Phiri K, Moucheraud C, et al. A Qualitative Assessment of Provider and Client Experiences With 3- and 6-Month Dispensing Intervals of Antiretroviral Therapy in Malawi. Global Health, Science and Practice. 2020;8(1):18–27. doi:10.9745/GHSP-D-19-00286
82. Shrestha B, Dunn L. The Declaration of Helsinki on Medical Research involving Human Subjects: a Review of Seventh Revision. J Nepal Health Res Counc. 2020;17(4):548–552. doi:10.33314/jnhrc.v17i4.1042
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.