Back to Journals » Clinical Interventions in Aging » Volume 17
Factors Associated with Transfer from an Acute Geriatric Unit to a Post-Acute Care Facility among Community-Dwelling Patients: Results from the DAMAGE Cohort
Authors Deschasse G, Drumez E, Visade F, Charpentier A, Delecluse C, Loggia G ![]() , Lescure P, Attier-Żmudka J, Bloch J, Gaxatte C, Bloch F
, Lescure P, Attier-Żmudka J, Bloch J, Gaxatte C, Bloch F ![]() , Puisieux F, Beuscart JB
, Puisieux F, Beuscart JB
Received 13 April 2022
Accepted for publication 14 September 2022
Published 9 December 2022 Volume 2022:17 Pages 1821—1832
DOI https://doi.org/10.2147/CIA.S370562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Guillaume Deschasse,1,2 Elodie Drumez,2,3 Fabien Visade,2,4 Anne Charpentier,5 Céline Delecluse,4 Gilles Loggia,6,7 Pascale Lescure,7 Jadwiga Attier-Żmudka,8,9 Jennifer Bloch,5 Cédric Gaxatte,5 Frédéric Bloch,1 François Puisieux,5 Jean-Baptiste Beuscart2,5
1Department of Geriatrics, CHU Amiens-Picardie, Amiens, France; 2ULR 2694 - METRICS: Évaluation des technologies de santé et des pratiques médicales, University Lille, CHU Lille, Lille, France; 3Department of Biostatistics, CHU Lille, Lille, France; 4Geriatrics Department, Lille Catholic Hospitals, Lille, France; 5Department of Geriatrics, CHU Lille, Lille, France; 6COMETE, INSERM, Normandie Univ, UNICAEN, Caen, France; 7Department of Geriatrics, Normandie Univ, UNICAEN, CHU de Caen Normandie, Caen, France; 8Geriatric Department, General Hospital of Saint-Quentin, Saint-Quentin, France; 9CHIMERE EA 7516 Team Research, Jules Verne University, Amiens, France
Correspondence: Guillaume Deschasse, Department of Geriatrics, CHU Amiens-Picardie, Amiens, France, Tel +33-322-088-000, Fax + 33-322-455-748, Email [email protected]
Background: Acute geriatric units (AGUs) require efficient discharge planning tools. Risk factors for discharge from an AGU to post-acute care (PAC) have not previously been investigated in detail.
Methods: The objective is to identify risk factors for PAC transfer. The DAMAGE (prospective multicenter cohort) consecutively included more than 3500 subjects aged 75 or older and admitted to an AGU. The patients underwent a comprehensive geriatric assessment (CGA) during their stay in the AGU. Only community-dwelling patients admitted to the AGU from the emergency department were included in the analysis. We recorded the characteristics of the care pathway and identified risk factors for discharge to home or to a PAC facility.
Results: 1928 patients were included. Loss of functional independence (a decrease in the Katz activities of daily living (ADL) score between 1 month prior to admission and AGU admission), living alone, social isolation, a high Katz ADL score at home, a low Katz ADL on admission, and delirium on admission were risk factors for transfer to PAC. Obesity, an elevated serum albumin level, and community-acquired infection were associated with discharge to home. Neither sex nor age was a risk factor for home discharge or transfer to PAC.
Conclusion: The present results might help clinicians and discharge planning teams to identify patients at risk of transfer to PAC more reliably and promptly in AGUs.
Keywords: care transitions, health services, rehabilitation, risk factors, acute geriatric unit
Introduction
In demographically changing societies, the optimization of care pathways for older people is a major challenge. In an efficient pathway, the flow of hospitalized older patients must be aligned with the “right care, right time, right place, every time” concept.1 Some hospitals have set up planning discharge and specialized teams that manage transfers and discharges to home and optimize patient flows.2,3 One of the challenges in planning discharge is the rapidly identification of patients who will require post-acute care (PAC). An appropriate discharge plan can reduce the hospital readmission rate and the length of hospital stay and might thus improve health outcomes while decreasing costs.4,5 Studies of surgical and neurology wards have shown that older age and poor functional independence are risk factors for transfer to PAC.6–9 Specific tools7–10 have been developed to identify patients at risk of transfer to PAC and it has been shown that the use of some of these tools is associated with a shorter length of hospital stay.9,11
Acute geriatric units (AGUs) provide specific care for frail, dependent or multimorbid older adults with acute health problems. The patient pathways for older people admitted to an AGU can be complex, due to the individuals’ frailty and/or dependency. In well-documented cases, most patients are admitted from home to the emergency department and are then transferred to the AGU.12–14 The downstream transfers of older people hospitalized in AGU have not been investigated in as much detail, and risk factors for transfer from an AGU to PAC have not been extensively identified and characterized.
DAMAGE is a prospective multicenter cohort study that comprises over 3500 consecutively included adults aged 75 and over and having been admitted to an AGU. These patients underwent a comprehensive geriatric assessment (CGA, including a description of the care pathway) during their stay in the AGU. Based on data for community-dwelling members of the DAMAGE cohort admitted to the AGU from the emergency department, we sought to determine the frequency of PAC transfer and identify risk factors for PAC transfer.
Materials and Methods
Study Design
The DAMAGE study is a multicenter, prospective cohort study of patients aged 75 or over hospitalized in an AGU in the Hauts de France and Normandie regions of France (NCT02949635). The six participating centers are Lille University Medical Center (Lille, France; two AGUs), Saint Philibert Hospital (Lille, France), Amiens-Picardie University Medical Center (Amiens, France), Caen University Medical Center (Caen, France), and Saint Quentin General Hospital (Saint Quentin, France). The inclusion period ran from September 14th, 2016, to January 29th, 2018. Each DAMAGE investigating center had a discharge planning team composed of a head nurse, a social worker, and a supervising physician. The study was funded by the French Ministry of Health. The DAMAGE study’s methodology has been described in detail elsewhere.15,16 The main goal of the DAMAGE cohort was to study outcomes after a stay in the UGA and we included 3509 patients for the primary objective analysis. This study is a post-hoc analysis.
Ethical Approval
The DAMAGE study was performed in compliance with the tenets of the Declaration of Helsinki and was approved by an institutional review board (CPP Nord-Ouest IV, Lille, France) on February 13th, 2015. An amendment was approved on January 21st, 2016 (reference: IDRCB 2014 A01670 47, CNIL. bxA15352514).
The patients and their primary family caregivers or legal representatives were given detailed verbal and written information about the study, in order to ensure that the patients fully understood the potential risks and benefits of participation. In accordance with the French legislation on observational, non-interventional studies of routine clinical care, written consent was not required. The patients were informed that they could refuse to participate in the study and that refusal would not have any impact on their treatment in the AGU. If the patient was unable to refuse to participate in the DAMAGE study (notably because of severe neurocognitive disorders), the next of kin or legal representative could refuse participation. All participants were free to withdraw from the study at any time. This withdrawal had no impact on the care received.
Inclusion and Exclusion Criteria
All patients aged 75 and over, with health insurance coverage and hospitalized in an AGU were eligible for inclusion in the study. Patients hospitalized in the AGU for less than 48 hours were not included because this short length of stay prevented the completion of a CGA. Furthermore, patients admitted for immediate palliative care were not considered for inclusion. Lastly, patients who refused to participate in the study (as notified by the patient or his/her primary family caregiver or legal representative) were not included. However, cognitive impairment was not an exclusion criterion per se.
In order to have a study care pathway that was as homogeneous as possible, we selected a dichotomous care pathway: only community-dwelling patients admitted to an AGU from the emergency department and discharge to home or PAC transfer (ie transfer to a bed in a post-acute care and rehabilitation facility; in France, post-acute care can only be performed in dedicated facilities with an mean length of stay of 35.5 for patients aged 85 and over;17,18 home-based rehabilitation is not available in France) were included in the final analysis. Patients who died in the AGU and patients who were transferred to another acute care ward (eg a surgical ward or a non-geriatric ward) and did not return to the AGU were excluded. Patients transferred to palliative care units or having received palliative care during their stay in the AGU were also excluded.
Collection of Data During the Stay in the AGU
Data were collected via a specific case report form. The social, medical and geriatric variables recorded within 72 hours of admission to the AGU are listed in Appendix 1; they included the age, sex, type of home environment, the number of medications usually taken, the number of other hospital stays in the last 6 months, the Charlson Comorbidity Index, dependency at home 1 month prior to admission and on admission (according to the Katz Index of Independence in Activities of Daily Living (Katz ADL)) and change in the Katz ADL score between 1 month prior to admission to AGU and on admission, malnutrition (weight loss >5% in the previous month or >10% in the previous 6 months, or a body mass index <21), cognitive disorders, and standard laboratory variables (if several values were available, the one recorded closest to the time of admission was selected for analysis). A daily evaluation of the patient’s clinical status enabled the AGU’s physicians to determine whether or not discharge was medically feasible but had been delayed for some reason. The quality of the collected data was audited (Appendix 1). On the patient’s last day in the AGU, the discharge destination (home or PAC) was noted.
Statistical Analysis
Categorical variables were expressed as the frequency (percentage). Continuous variables were expressed as the mean ± standard deviation (SD), the median [interquartile range (IQR)], or the median (range). The normality of distribution was checked graphically and by using the Shapiro–Wilk test. Risk factors for transfer to PAC were analyzed using bivariate logistic regression models; the effect size was quantified as the odds ratio (ORs) [95% confidence interval (CI)]. For each continuous predictor, the log-linearity assumption was assessed using restricted cubic spline functions.19 When evidence of a non-log-linear relationship was found, continuous predictors were analyzed in quartiles. The absence of co-linearity between candidate predictors was assessed by calculating the variance inflation factors.20 Redundant variables were eliminated, with retention of the most relevant clinical variable. Candidate predictors with p<0.20 in a bivariate analysis were considered for inclusion in a multivariable logistic regression model. The full model was simplified using a stepwise backward selection procedure with a removal criterion of 0.05. To avoid case deletion in multivariate analyses, missing data for candidate predictors were imputed by multiple imputations using the regression-switching approach (chained equations, m=25 imputations).21 We used 25 imputations which allow to have a maximal fraction of missing information (FMI)/m<1%. The imputation procedure was performed under the missing-at-random assumption using all candidate predictors, with the predictive mean-matching method (for continuous variables) or binary, ordinal, or multinomial logistic regression models (for categorical variables). Rubin’s rules were used to combine the estimates derived from multiple imputed data sets.22 The median (range) of c-statistics (corresponding to the area under the receiver operating characteristic curve) across the 25 imputed datasets were reported.23 The threshold for statistical significance was set to p<0.05, and all tests were two-tailed. All analysis were performed with SAS software (release 9.4, SAS Institute, Cary, NC).
Results
Flow Chart
Of the 3509 DAMAGE cohort members hospitalized in an AGU, 1928 (54.9%) were living at home prior to admission through the emergency department and discharge to home (n=1317 (68.3%)) or a PAC facility (n=611 (31.7%)) (Figure 1).
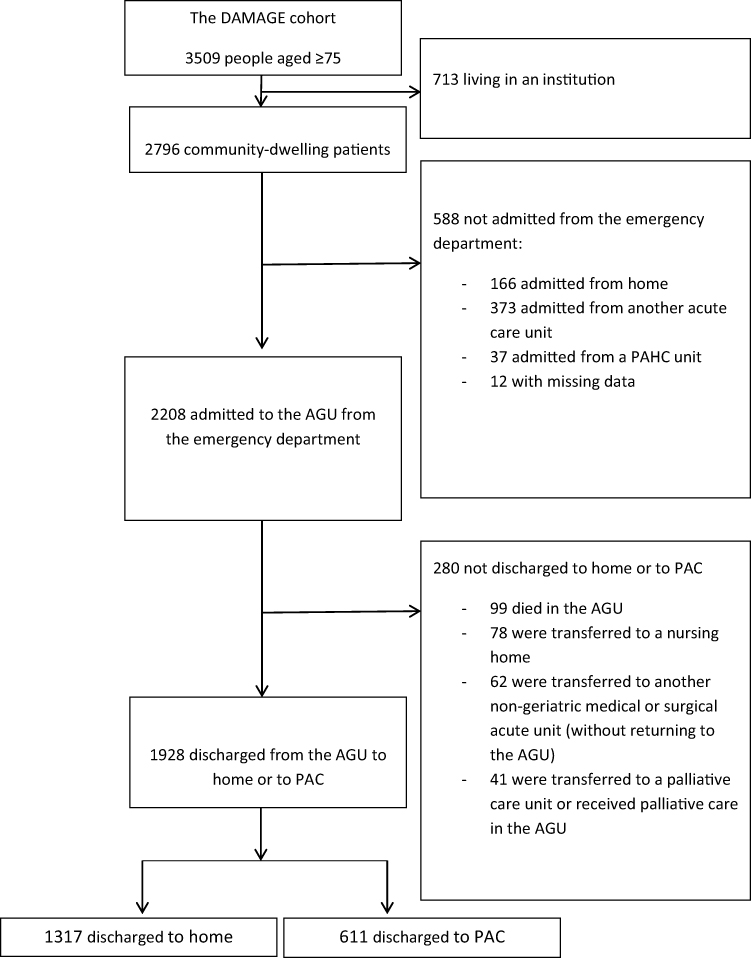 |
Figure 1 Study flow chart. |
Characteristics on Admission
The general characteristics of the study population are summarized in Table 1. The population was old (mean age: 86), with female predominance (64.5%). There were high frequencies of geriatric syndromes at home, polypharmacy (72.8% were taking more than five prescription drugs), impaired mobility (confinement to bed or a chair, or walking with assistance only) (59.3%), living alone (54,4%), a history of falls (51.4%), and cognitive disorders (50.1%). There was a high frequency of geriatric syndrome on admission, including dependency (62.5% of the patients had a Katz ADL score <5 on admission), acute loss of functional independence (an absolute decrease in the Katz ADL score of 1 point or more between home and the AGU, in 42.1% of cases), malnutrition (27.1%), obesity (18.8%), delirium (15.7%), and a low mean ± SD serum albumin level (32.1 ± 5.2). Differences between patients discharged to home and those discharged to PAC are summarized in Table 2.
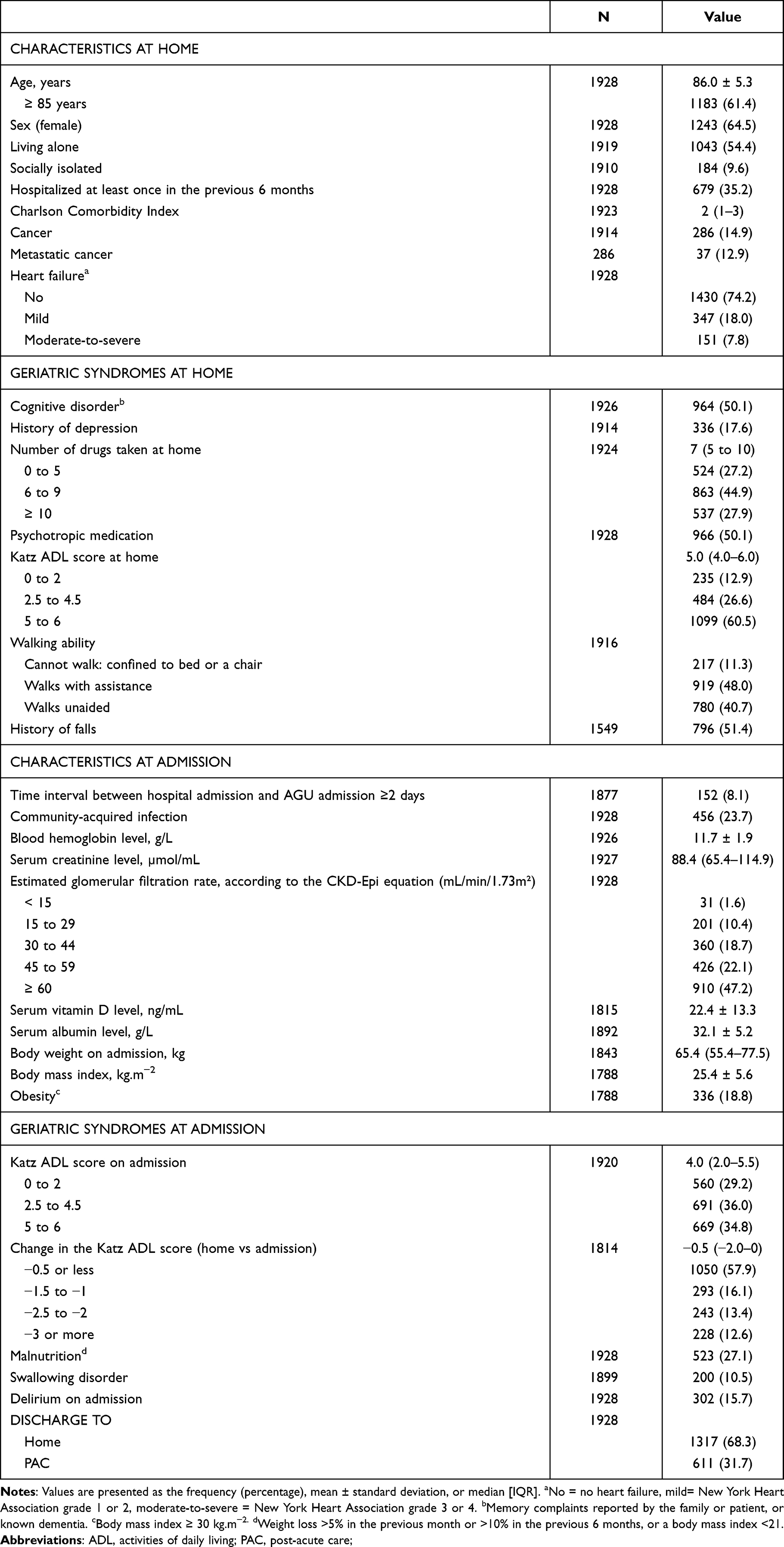 |
Table 1 Characteristics of the Overall Study Population (n=1928) |
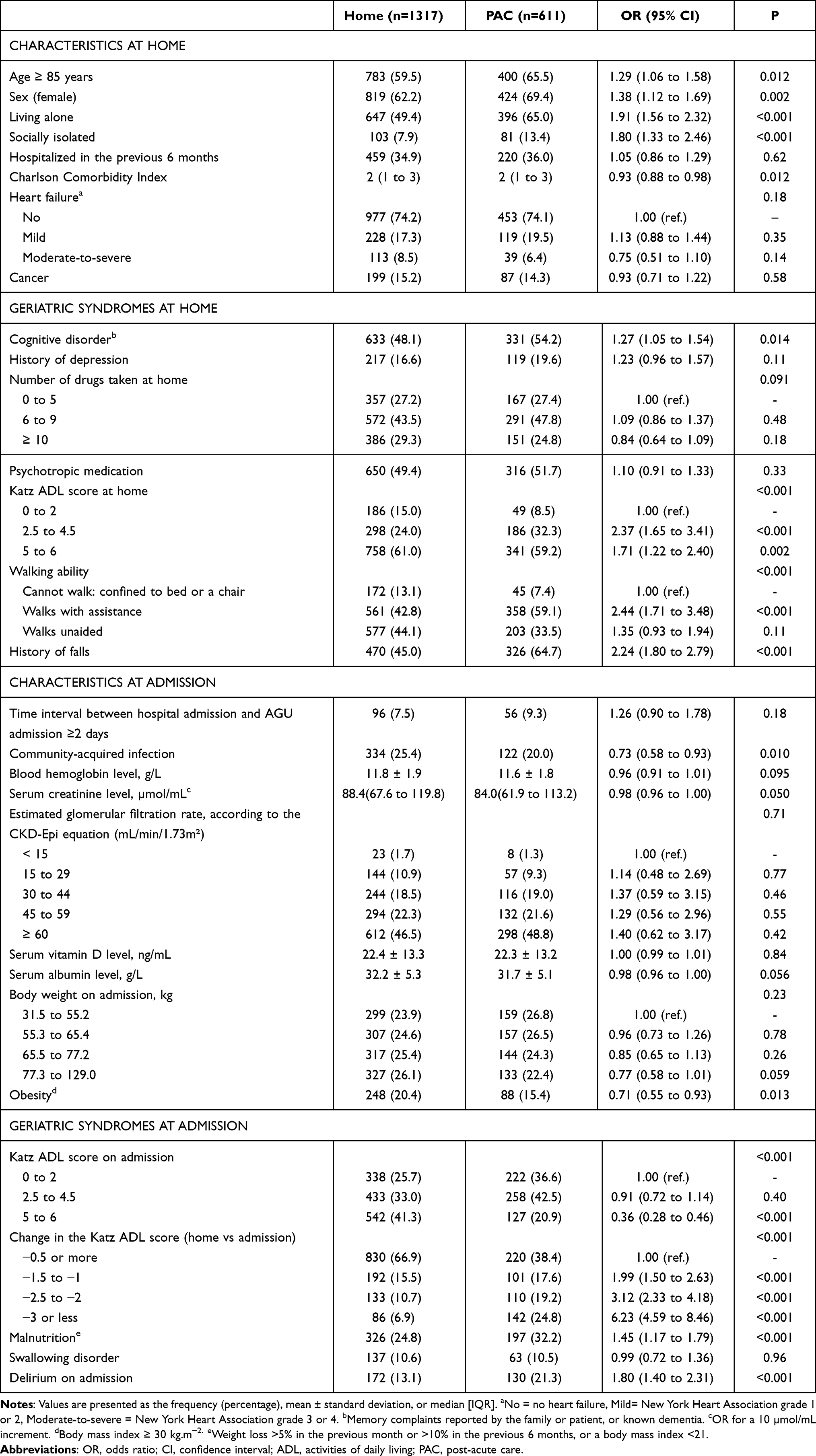 |
Table 2 Bivariate Analyses of Risk Factors for Transfer to PAC in the Overall Study Population |
Factors Associated with Discharge to PAC in AGU Patients
The results of the multivariate analysis are summarized in Table 3. (Missing data for individual variables ranged from 0 to 19.7%, leading to 33.3% of patients with missing data in multivariable model. All those missing data were imputed for the multivariable analyses). The model’s median (range) area under the curve was 0.721 (0.717 to 0.724). All the variables associated with a greater risk of transfer to PAC were related to either social conditions (living alone, and social isolation), geriatric syndromes at home (a history of falls, impaired Walking ability) and geriatric syndromes at admission (delirium on admission, and an absolute decrease in the Katz ADL score of 1 point or more between home and the AGU).
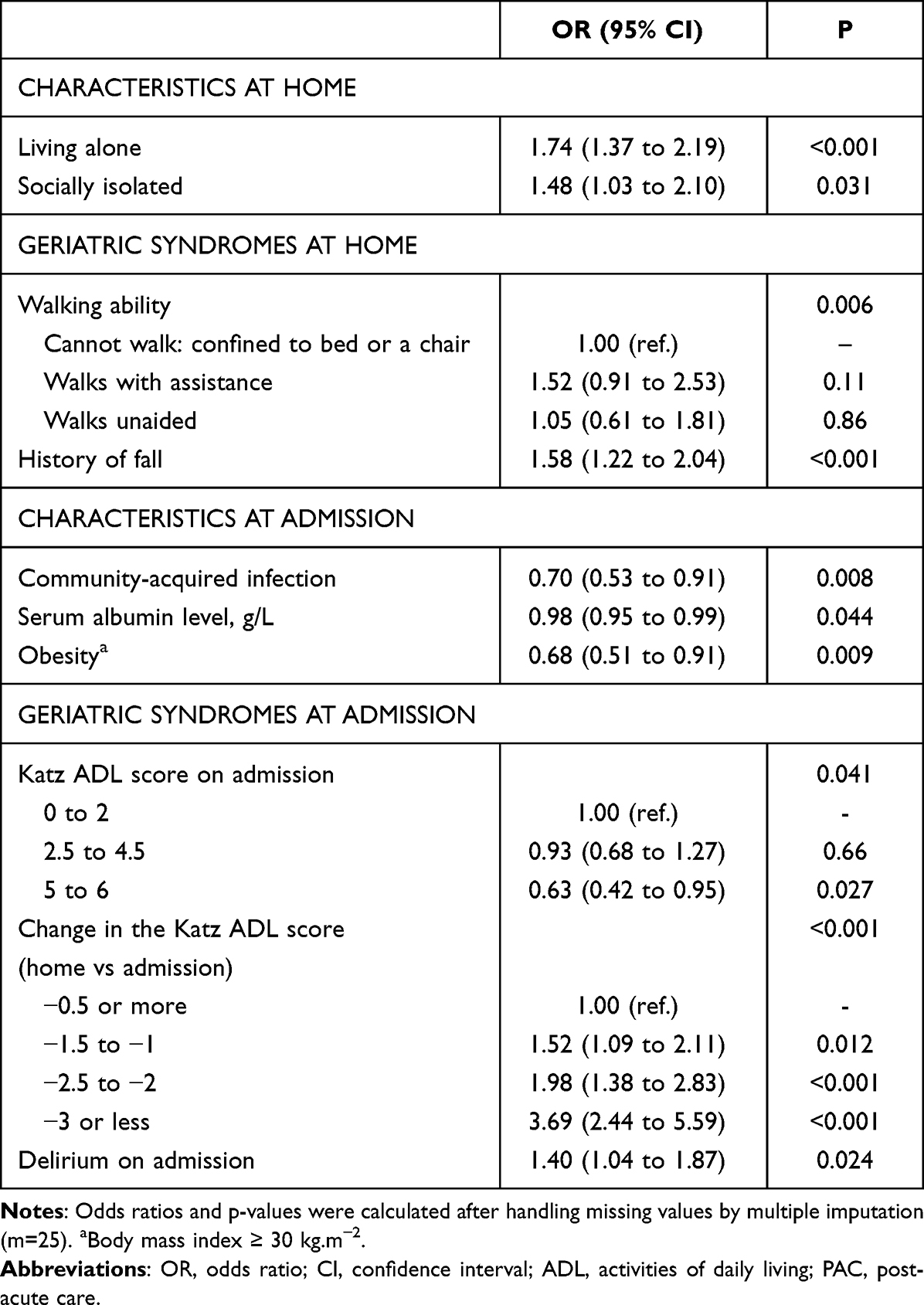 |
Table 3 Multivariable Analysis of Risk Factors for Transfer to PAC in the Overall Population |
Conversely, most of the variables associated with a lower risk of transfer to PAC were medical conditions: obesity, community-acquired infection, and an elevated serum albumin level. The only geriatric syndrome associated with a lower risk of transfer to PAC was a high Katz ADL score on admission. Neither sex nor age was a risk factor for transfer to PAC or to home.
Discussion
Geriatric Syndromes and Risk Factors for PAC
The present study is the first to have looked at risk factors for transfer to PAC among older patients in the AGU. Ideally, the main risk factors for transfer to PAC should be easily identifiable upon admission to the AGU; this would enable the AGU’s discharge planning team to forecast and plan the patients’ care trajectories more accurately. Most of the risk factors in the present study were geriatric syndromes; the main factor was the absolute decrease in the Katz ADL score between home and the AGU. The likelihood of AGU-PAC transfer was more influenced by the presence of a geriatric syndrome (acute loss of functional independence, delirium, falls, malnutrition, etc.) and social conditions (living alone or social isolation) than by the community-dwelling patients’ other characteristics (eg age, sex, cancer, or heart failure). The risk factors sometimes reported in the literature (age, low functional dependence at home, the number of comorbid conditions, and cognitive disorders) were not statistically significant in our AGU patient population.24–26
Most previous studies of risk factors associated with transfer to PAC were conducted in other clinical settings and units (surgical wards, stroke units, internal medicine wards, etc.). In a study of surgical wards, Sacks et al25 showed that older age, admission from another acute care facility, partial or full functional dependency before surgery, and a higher number of comorbidities were all associated with a greater risk-adjusted OR for transfer to PAC after various operations. The studies by Yeates10 and Sattler24 (in a trauma setting and after total knee arthroplasty, respectively) gave similar results. Chang27 showed that the Activity Measure for Post-Acute Care “6-Clicks” Basic Mobility Inpatient Short Form score at admission to an acute stroke unit was the only significant predictor of transfer a post-acute inpatient rehabilitation facility. A score developed by Louis-Simonet et al took account of many aspects (including age, and functional independence in hospital on day 1 and day 3) with good sensitivity and specificity in a population whose mean age ranged from 62 to 71.28 Our present study of older patients in the AGU gave some novel results. Firstly, partial or full functional dependency before hospital admission (ie confinement to bed or a chair) was associated with discharge to home. Moreover, the change in the Katz ADL score was strongly associated with transfer to PAC - especially if the acute loss of functional independence was marked. This result highlights the need to know the patient’s level of functional dependency at home and on admission to the AGU when selecting the best care trajectory. The other risk factors identified were living alone, social isolation, delirium on admission, a history of falls, and impaired walking ability. Conversely, obesity, an elevated albumin level, and community-acquired infections were AGU-specific risk factors for home discharge and have not been flagged up by studies in other settings.
Benefits and Tools for Discharge Planning Teams
Taken as a whole, our results suggest that discharge planning teams could apply a specific patient score or selection process on admission to the AGU. Holland et al showed that older age, walking limitation, living alone before admission, and the level of disability indicate the need for a specialized discharge planning team in surgery units.8,29–31 A specialized discharge planning team may also be of value in the management of cancer patients.7 Indeed, discharge is often delayed by the lack of a suitable care facility.32,33 Various studies have shown the benefits of discharge planning in PAC units34–38 or at home with a care network.39 However, the effectiveness of in-hospital rehabilitation in deconditioned, older subjects is still under investigation.40 The risk-benefit ratio of discharge to PAC or to home is not easy to assess and raises ethical issues. Although many discharge planning programs are in operation, there are no guidelines or clinical trial evidence on the risk-benefit ratio.41 This lack of decision-making guidelines prompts the adoption of subjective approaches based on organizational factors and the clinicians’ preferences and characteristics.42
Strengths
The present study had several strengths. Firstly, the study cohort was large, with more than 1900 patients out of a prospective cohort of 3500 consecutively included subjects. Secondly, the proportion of missing data at baseline was low. Thirdly, we performed a multicenter study of AGUs; there are few studies of this type. Fourthly, the DAMAGE trial included a CGA and a standardized evaluation of the main geriatric syndromes. Lastly, the small number of exclusion criteria and the ability to include patients with cognitive disorders enabled us to minimize selection bias and thus study a population that was highly representative of patients receiving routine care in the AGUs.
Limitations
Firstly, our models were based on data collected in a single national cohort, and most of the investigating centers were teaching hospitals whose care provision and population profiles are not necessarily representative of France as a whole. In fact, the significance of certain variables may depend on the context of care. Secondly, we did not take account of in-hospital complications or study the process of deciding whether to transfer to home or to a PAC. Consequently, we were not able to stratify our analysis according to the care the AGU patients would need in PAC; however, our study’s objective was to identify risk factors that could be recorded upon admission to the AGU. Thirdly, the variables collected here corresponded to our standard geriatric practice and the specific context of nursing care and disease prevention in the AGU. Hence, the models should be used with caution with frail older patients hospitalized in units other than an AGU in France. Fourthly, we only considered a single incoming care pathway (patients admitted to the emergency department from home and then transferred to the AGU) and two discharge outcomes (home vs PAC); these pathways can be more diversified and the use of more complex statistical models (eg multinomial regression models or multistate models) may have allowed to analyze more pathways, such as direct admission to the AGU from home or from another acute service, discharge to post-acute care at home, transfer to a nursing home, etc. However, such models provide complex results that may be difficult to implement in clinical practice, especially since care structures (eg resources, funding systems, uses, and organizational aspects) differ from one country to another and may change rapidly.43–45
Perspectives
The changes in ADL and functional independence upon admission appear to have important roles and should be investigated further. Such studies might enable (i) the development of new tools for optimized planning, patient flow and care pathways in AGU, (ii) the production of new guidelines, and (iii) a better understand of decision-making process for transfer to PAC or to home.
Conclusion
We conducted a prospective, multicenter study of a large cohort of frail, older patients hospitalized in the AGU. The present study is the first to have identified several risk factors for AGU-PAC transfer that can be recorded on admission. Living alone, social isolation, a marked loss of functional independence between home and AGU admission, a low Katz ADL score on admission, and delirium at admission are risk factors for transfer to PAC. In contrast, obesity, an elevated serum albumin level and community-acquired infection are factors associated with discharge to home. These results might help clinicians and discharge planning teams to identify at-risk patients more reliably and promptly.
Acknowledgments
We thank all the physicians who helped to recruit patients in the centres, and notably Julien Moyet, Véronique Gallopin, Sanaa Hannat, Saliha Sid Idris, Claire Delmas, Mélissa Pierre, Wilhelm Pommier, Rozenn Hequette, Eric Boulanger, Aurélie Moraud, Elisabeth Brocquet, Pierre Robinet, Francois Maladry, Fouad El Dirani, Christine Yves, Jean Mari Nkunzimana, Yassine Benhammacht, Celine Boufflet, Karim Boulanouar. We also thank the members of the clinical research support team at Lille University Hospital for their help and logistical support throughout the study, and notably Sara Frade, Martin Wojcik, Aurélie Gozdziaszek and Samir Boukla. We thank David Fraser PhD (Biotech Communication SARL, Ploudalmézeau, France) for copy-editing assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by the French Ministry of Health.
Disclosure
Professor Jean-Baptiste Beuscart reports grants from French government’s interregional hospital-based clinical research program, during the conduct of the study. No authors have any conflicts of interest to declare.
References
1. Nowak NA, Rimmasch H, Kirby A, Kellogg C. Right care, right time, right place, every time. Healthc Financ Manag J Healthc Financ Manag Assoc Avr. 2012;66(4):82–88.
2. Goodman DM, Burke AE, Livingston EH. Discharge planning. JAMA. 2013;309(4):406–406. doi:10.1001/jama.2012.145192
3. Gonçalves-Bradley DC, Lannin NA, Clemson LM, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2016;1:CD000313.
4. Lin CJ, Cheng SJ, Shih SC, Chu CH, Tjung JJ. Discharge Planning. Int J Gerontol. 2012;6(4):237–240.
5. Shepperd S, Doll H, Broad J, et al. Early discharge hospital at home. Cochrane Database Syst Rev. 2009;1:CD000356.
6. Jette DU, Stilphen M, Ranganathan VK, Passek SD, Frost FS, Jette AM. AM-PAC « 6-Clicks » functional assessment scores predict acute care hospital discharge destination. Phys Ther. 2014;94(9):1252–1261.
7. Socwell CP, Bucci L, Patchell S, Kotowicz E, Edbrooke L, Pope R. Utility of Mayo Clinic’s early screen for discharge planning tool for predicting patient length of stay, discharge destination, and readmission risk in an inpatient oncology cohort. Support Care Cancer. 2018;26(11):3843.
8. Holland DE, Brandt C, Targonski PV, Bowles KH. Validating performance of a hospital-discharge planning decision tool in community hospitals. Prof Case Manag. 2017;22(5):204–213.
9. Bowles KH, Ratcliffe SJ, Holmes JH, et al. Using a decision support algorithm for referrals to post-acute care. J Am Med Dir Assoc. 2019;20(4):408–413.
10. Yeates EO, Grigorian A, Kuza CM, et al. The DEPARTS Score: a Novel Tool for Predicting Discharge Disposition in Geriatric Trauma Patients. Am Surg. 2021;9:31348211029843.
11. Bowles KH, Hanlon A, Holland D, Potashnik SL, Topaz M. Impact of discharge planning decision support on time to readmission among older adult medical patients. Prof Case Manag. 2014;19(1):29–38. doi:10.1097/01.PCAMA.0000438971.79801.7a
12. Baztán JJ, Suárez-García FM, López-Arrieta J, Rodríguez-Mañas L, Rodríguez-Artalejo F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: meta-analysis. BMJ. 2009;338:b50. doi:10.1136/bmj.b50
13. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316
14. Conroy SP, Turpin S. New horizons: urgent care for older people with frailty. Age Ageing. 2016;45(5):577–84. doi:10.1093/ageing/afw135
15. Deschasse G, Bloch F, Drumez E, et al. Development of a predictive score for mortality at 3- and 12-month after discharge from an acute geriatric unit as a trigger for advanced care planning. J Gerontol a Biol Sci Med Sci. 2021;77:glab217.
16. Visade F, Babykina G, Puisieux F, et al. Risk factors for hospital readmission and death after discharge of older adults from acute geriatric units: taking the rank of admission into account. Clin Interv Aging. 2021;16:1931–1941. doi:10.2147/CIA.S327486
17. Les soins de suite et de réadaptation en 2008: patientèle traitée et offre de soins | direction de la recherche, des études, de l’évaluation et des statistiques [Post-acute and rehabilitation care in 2008: patients treated and supply of care | Directorate for Research, Studies, Evaluation and Statistics] [Internet]. Available from: https://www.drees.solidarites-sante.gouv.fr/publications/dossiers-solidarite-et-sante-1998-2016/les-soins-de-suite-et-de-readaptation-en-2008.
18. Soins de suite et de réadaptation: les personnes de 70 ans ou plus effectuent la moitié des séjours | direction de la recherche, des études, de l’évaluation et des statistiques [Post-acute and rehabilitation care: people aged 70 or over make half of the stays | Directorate for Research, Studies, Evaluation and Statistics] [Internet]. Available from: https://drees.solidarites-sante.gouv.fr/publications/etudes-et-resultats/soins-de-suite-et-de-readaptation-les-personnes-de-70-ans-ou-plus.
19. Harrell FE, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15(4):361–387. doi:10.1002/(SICI)1097-0258(19960229)15:4<361::AID-SIM168>3.0.CO;2-4
20. Allison PD Multiple regression: a primer [Internet]. Thousand Oaks, Calif; London: Pine Forge Press; 1999. Available from: https://trove.nla.gov.au/version/10302679.
21. Buuren S, Groothuis-Oudshoorn C. MICE: multivariate imputation by chained equations in R. J Stat Softw. 2011;2021:45.
22. Toutenburg H, Rubin DB. Multiple imputation for nonresponse in surveys. Stat Pap. 1990;31(1):
23. Marshall A, Altman DG, Holder RL, Royston P. Combining estimates of interest in prognostic modelling studies after multiple imputation: current practice and guidelines. BMC Med Res Methodol. 2009;9:57. doi:10.1186/1471-2288-9-57
24. Sattler L, Hing W, Rathbone E, Vertullo C. Intrinsic patient factors predictive of inpatient rehabilitation facility discharge following primary total knee arthroplasty: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2020;21(1):481. doi:10.1186/s12891-020-03499-5
25. Sacks GD, Lawson EH, Dawes AJ, Gibbons MM, Zingmond DS, Ko CY. Which patients require more care after hospital discharge? An analysis of post-acute care use among elderly patients undergoing elective surgery. J Am Coll Surg. 2015;220(6):1113–1121.e2. doi:10.1016/j.jamcollsurg.2015.02.029
26. Van der Cruyssen K, Vereeck L, Saeys W, Remmen R. Prognostic factors for discharge destination after acute stroke: a comprehensive literature review. Disabil Rehabil. 2015;37(14):1214–1227. doi:10.3109/09638288.2014.961655
27. Chang FH, Lin YN, Liou TH, Lin JC, Yang CH, Cheng HL. Predicting admission to post-acute inpatient rehabilitation in patients with acute stroke. J Rehabil Med. 2020;52(9):jrm00105. doi:10.2340/16501977-2739
28. Louis Simonet M, Kossovsky MP, Chopard P, Sigaud P, Perneger TV, Gaspoz J-M. A predictive score to identify hospitalized patients risk of discharge to a post-acute care facility. BMC Health Serv Res. 2008;8(1):154. doi:10.1186/1472-6963-8-154
29. Holland DE, Harris MR, Leibson CL, Pankratz VS, Krichbaum KE. Development and validation of a screen for specialized discharge planning services. Nurs Res. 2006;55(1):62–71.
30. Holland DE, Mistiaen P, Bowles KH. Problems and unmet needs of patients discharged « home to self-care ». Prof Case Manag. 2011;16(5):240–250.
31. Holland DE, Rhudy LM, Vanderboom CE, Bowles KH. Feasibility of discharge planning in intensive care units: a pilot study. Am J Crit Care off Publ Am Assoc Crit Care Nurses. 2012;21(4):e94–e101.
32. Katsaliaki K, Brailsford S, Browning D, Knight P. Mapping care pathways for the elderly. J Health Organ Manag. 2005;19(1):57–72.
33. Meo N, Bann M, Sanchez M, Reddy A, Cornia PB. Getting unstuck: challenges and opportunities in caring for patients experiencing prolonged hospitalization while stable for discharge. Am J Med. 2020;133(12):1406–1410.
34. Thalmann M, Tröster T, Fischer K, et al. Do older adults benefit from post-acute care following hospitalisation? A prospective cohort study at three Swiss nursing homes. Swiss Med Wkly. 2020;150:w20198.
35. Young J, Green J, Forster A, et al. Postacute care for older people in community hospitals: a multicenter randomized, controlled trial. J Am Geriatr Soc. 2007;55(12):1995–2002.
36. Chen LK, Chen YM, Hwang SJ, et al. Effectiveness of community hospital-based post-acute care on functional recovery and 12-month mortality in older patients: a prospective cohort study. Ann Med. 2010;42(8):630–636.
37. Lee WJ, Peng LN, Cheng YY, Liu CY, Chen LK, Yu HC. Effectiveness of short-term interdisciplinary intervention on postacute patients in Taiwan. J Am Med Dir Assoc. 2011;12(1):29–32.
38. Abrahamsen JF, Haugland C, Nilsen RM, Ranhoff AH. Three different outcomes in older community-dwelling patients receiving intermediate care in nursing home after acute hospitalization. J Nutr Health Aging. 2016;20(4):446–452.
39. Verweij L, van de Korput E, Daams JG, et al. Effects of postacute multidisciplinary rehabilitation including exercise in out-of-hospital settings in the aged: systematic review and meta-analysis. Arch Phys Med Rehabil. 2019;100(3):530–550.
40. Timmer AJ, Unsworth CA, Taylor NF. Rehabilitation interventions with deconditioned older adults following an acute hospital admission: a systematic review. Clin Rehabil. 2014;28(11):1078–1086.
41. Wong SP, Sharda N, Zietlow KE, Heflin MT. Planning for a safe discharge: more than a capacity evaluation. J Am Geriatr Soc. 2020;68(4):859–866.
42. Longley V, Peters S, Swarbrick C, Bowen A. What factors affect clinical decision-making about access to stroke rehabilitation? A systematic review. Clin Rehabil. 2019;33(2):304–316.
43. Grund S, Gordon AL, van Balen R, et al. European consensus on core principles and future priorities for geriatric rehabilitation: consensus statement. Eur Geriatr Med. 2020;11(2):233–238.
44. Papanicolas I, Figueroa JF, Schoenfeld AJ, et al. Differences in health care spending and utilization among older frail adults in high-income countries: ICCONIC Hip fracture persona. Health Serv Res. 2021;56(Suppl 3):1335–1346.
45. de Groot AJ, Wattel EM, van Dam CS, van Balen R, van der Wouden JC, Hertogh CMPM. Referral to geriatric rehabilitation: a scoping review of triage factors in acutely hospitalised older patients. Age Ageing. 2022;51(2):afac015.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.