Back to Journals » Patient Preference and Adherence » Volume 20
Factors Associated with the Transition from Discharge Preparation to Home Rehabilitation in Elderly Day Surgery: A Structural Equation Modeling Study
Authors Wu M ![]() , Huang C
, Huang C ![]() , Xu Y, Zhao L, Dai W, Xia L
, Xu Y, Zhao L, Dai W, Xia L
Received 18 March 2026
Accepted for publication 2 May 2026
Published 19 May 2026 Volume 2026:20 609521
DOI https://doi.org/10.2147/PPA.S609521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Mei Wu,1 Chunjin Huang,2 Yamin Xu,3 Liting Zhao,1 Wenbin Dai,4 Lu Xia5
1Department of Nursing, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of General Surgery, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 3Day Care Chemotherapy, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 4Medical Affairs Department, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 5Day Surgery Unit, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China
Correspondence: Lu Xia, Day Surgery Unit, Huadong Hospital, Fudan University, No. 221 West Yan’an Road, Shanghai, 200040, People’s Republic of China, Tel +8618121223980, Email [email protected]
Purpose: To explore the key factors influencing the transition from discharge preparation to home-based rehabilitation in elderly day surgery patients.
Patients and Methods: A cross-sectional study was conducted on 340 elderly patients (≥ 60 years) who underwent day surgery at Huadong Hospital Affiliated to Fudan University in Shanghai from November 2024 to September 2025. Standardized scales were used to conduct questionnaire surveys, and the collected data were analyzed by means of correlation analysis, multiple linear regression and structural equation modeling (SEM).
Results: Correlation analysis revealed that discharge readiness was positively correlated with gender, health behavior capacity and discharge teaching quality, while it presented a negative correlation with family support (P< 0.05). Multiple linear regression further verified that health behavior capacity served as a significant positive predictive factor for discharge readiness (β=0.233, P< 0.001). However, the SEM yielded inconsistent findings: family support exhibited the strongest positive direct predictive effect on discharge readiness with a path coefficient of 0.47, health behavior capacity showed a weak positive predictive effect (path coefficient = 0.31), and discharge teaching quality exerted only a trivial impact (path coefficient = 0.15). The contradictory results between correlation analysis and SEM might be attributed to the complex mediating or moderating relationships among latent variables in the holistic model.
Conclusion: Family support is the core factor, and health behavior capacity is an important factor affecting the discharge readiness of elderly day surgery patients, while the current discharge teaching has a limited direct effect. In clinical practice, it is necessary to strengthen family support, improve patients’ health behavior self-efficacy, and optimize the discharge teaching model with effective linkage to family support. Further research should adopt multi-center longitudinal studies with extended variables to obtain more comprehensive and accurate results.
Plain Language Summary: This study explores key factors affecting elderly day surgery patients’ discharge preparation and home rehabilitation transition. We surveyed 340 elderly patients (≥ 60 years) who had day surgery at Huadong Hospital (Nov 2024–Sep 2025) via standardized questionnaires and analyzed data scientifically. Results show family support has the strongest positive impact on discharge readiness, followed by patients’ self-confidence and ability to manage health (health behavior self-efficacy); hospital discharge guidance has little direct effect. Other unconsidered factors may exist. Clinically, we should strengthen family support, improve patients’ self-care ability and optimize discharge guidance. Future multi-hospital, long-term studies are needed for more comprehensive results.
Keywords: discharge, elderly, day surgery, home-based rehabilitation, structural equation modeling
Introduction
Ambulatory Surgery Centers (ASCs) deliver efficient, cost-effective, and patient-centered high-quality care, relying on multidisciplinary collaboration and continuous KPI optimization.1 Day surgery is the dominant elective surgical model in Western countries, exceeding 85% of procedures in the UK and US, while it remains nascent in developing nations. This discrepancy stems from variations in medical technology, management philosophies and reimbursement systems.2 Since 2001, China has developed day surgery services. By 2023, 83.27% of tertiary public hospitals nationwide provided day surgery, which accounted for 16.40% of all elective surgeries.3
ASC operational efficiency depends on coordinated allocation of human resources, medical equipment and scheduling, as well as standardized workflow management. These measures help shorten hospital stays and lower overall healthcare expenditures.1 However, its fast-paced model challenges discharge readiness and home rehabilitation transitions, especially for elderly patients.4 Discharge readiness—critical for post-discharge safety and successful home rehabilitation—has become a core indicator of healthcare quality management.5
Key risk factors for transition failure, including unplanned readmission (2.89% incidence) and delayed discharge, consist of organizational management problems, surgical factors, and poor patient health status. Specific patient risks include advanced age over 75 years, ASA classification ≥2, comorbidities, prolonged surgery, peripheral vascular disease, and prior deep vein thrombosis.6–8 Postoperative pain, nausea and vomiting impair discharge readiness, while morbid obesity, rather than general obesity, may delay discharge.9 Patients’ disease perception and psychological resilience are critical intrinsic factors; positive cognition and strong psychological resilience significantly enhance readiness.10 Key implementation barriers involve insufficient teamwork, limited staffing, time and funding resources, and inadequate digital capability.11,12 Discharge education quality correlates with readiness, with protective factors including clinicians’ teaching competence, physiological evaluation, and social support; patients with limited resources or low socioeconomic status have lower readiness.13,14
Patients commonly underestimate the complexity of postoperative self-care, resulting in post-discharge insecurity. Elderly individuals, in particular, exhibit lower discharge readiness than inpatients, especially following cataract day surgery.15,16 Chinese studies demonstrate that evidence-based discharge preparation improves discharge readiness and self-care capacity through targeted education, video guidance and family training, while further multicenter verification remains necessary.16 Enhancing discharge readiness requires systematic interventions: post-discharge support for high-risk groups, integrating psychological resilience training into preoperative education, multi-format health education, and nurse-led transitional care addressing medical and psychosocial needs.10,14 Discharge planning(DP) is essential for safe patient transitions from hospital to home or care facilities, directly affecting care continuity, readmission rates, and quality of life.12 Studies confirm structured DP improves key outcomes, though effects differ by intervention, patient traits, and system factors.17,18 A trial in colorectal stoma patients showed nurse-led DP enhanced education, self‑efficacy, and quality of life while lowering complications (P<0.001).19 However, evidence for its impact on mortality, emergency department visits, and overall health remains limited.17
DP implementation varies in initiation timing, follow-up methods, and team collaboration.18 Elderly patients (60–84 years) benefit from DP via shorter hospital stays (mean 0.73-day reduction) and lower readmission risk, but interventions must be individualized by comorbidities, surgical type, and social support.7,8 High-intensity, multi-component interventions yield optimal results, particularly in reducing readmissions. Clinical practice should adopt nurse-led standardized protocols and strengthen hospital-community collaboration.18,19
With the accelerating population aging in China, discharge readiness serves as a critical predictor of successful transition to home-based rehabilitation among elderly patients undergoing day surgery. According to existing theoretical foundations and empirical studies, health behaviors, family support, and discharge education were hypothesized as direct predictive factors for discharge readiness, with potential inter-variable pathways to affect patients’ home rehabilitation transition. Given the complex multi-factor interaction and hierarchical causal relationships among above latent variables, SEMcombined with path analysis was adopted in this study. Therefore, this study aims to understand discharge readiness among elderly day surgery patients, explore factors influencing the transition from discharge readiness to home rehabilitation, and establish a path analysis.
Materials and Methods
Study Participants and Elicitation Method
This cross-sectional study employed consecutive sampling to enroll elderly patients who underwent ambulatory surgery in the Ambulatory Surgery Ward of Huadong Hospital between November 2024 and September 2025.
Inclusion criteria were: aged 60 years or older were in stable condition meeting discharge criteria with discharge orders issued by attending physicians, opted for home-based rehabilitation post-discharge, and voluntarily participated in the study by signing an informed consent form. Exclusion criteria included patients with communication disorders or other conditions preventing study cooperation, and patients transferred to specialized wards for further treatment after surgery. This study involved 5 latent variables and 20 measurable indicators. Following the rule of thumb of 10–15 respondents per indicator, the minimum sample size was determined to range from 200 to 300. A total of 340 elderly patients were enrolled in this study. All eligible participants received standardized discharge education delivered by trained nurses following the standardized discharge guidance protocol. A questionnaire survey was conducted within 4 hours prior to their discharge. Before distributing the questionnaires, the purpose and significance of the study were explained to the participants. After obtaining their consent, the participants completed the questionnaires anonymously, with the questionnaires distributed and collected on-site.
Self-Rated Abilities for Health Practices Scale (SRAHP)
The culturally adapted and reliability-validated Chinese version of the Self-Rated Abilities for Health Practices Scale (SRAHP)20,21 was employed to evaluate the self-efficacy of health behaviors among elderly patients undergoing day surgery. The SRAHP consists of 28 items covering four dimensions, including health responsibility (8 items), physical exercise (7 items), healthy diet (6 items), and psychological adjustment (7 items).
A 5-point Likert scale was employed for scoring, where 1 point indicated “no confidence at all” and 5 points signified “extremely confident.” The scale’s total score ranges from 28 to 140 points, with higher scores reflecting stronger self-efficacy in implementing health-promoting behaviors. To examine the relationship between different dimensions of health behavior self-efficacy and home rehabilitation outcomes, each dimension score was calculated separately, and the total score was categorized into three levels: low self-efficacy (28–62 points), moderate self-efficacy (63–105 points), and high self-efficacy (106–140 points) based on the percentile method. In this study, the Cronbach’s α coefficient of the total scale was 0.95, and the Cronbach’s α coefficients of each dimension ranged from 0.86 to 0.89, confirming good internal consistency reliability.
Perceived Social Support from Family Scale (PSS-FA)
The Perceived Social Support from Family Scale22 was adopted to evaluate the level of perceived family support among elderly ambulatory surgery patients during the home-based rehabilitation phase. This scale consists of 15 items, covering four core dimensions: emotional support, daily living care support, information and decision-making support, and economic and resource support. A binary scoring method was employed, with response options of “Yes” and “No” assigned 1 point and 0 points respectively. The scale’s total score ranges from 0 to 15, with higher scores indicating a greater level of perceived family support among patients. Psychometric testing revealed that the Kuder-Richardson 21 (KR-21) reliability coefficient of the scale was 0.75, demonstrating good internal consistency reliability and meeting psychometric requirements.
Quality of Discharge Teaching Scale (QDTS)
The Quality of Discharge Teaching Scale (QDTS), developed by Weiss et al23 and translated into Chinese by Binghua Wang, comprises 24 items scored on a 0 to 10 scale. It encompasses three dimensions: the content patients need before discharge (6 items), the content patients actually receive before discharge (6 items), and the guidance skills and effectiveness (12 items). Since the first two dimensions form six pairs of items, the score of the dimension of the content actually received minus the score of the dimension of the content needed can be defined as the “content difference” dimension. The combined scores of the “content actually received” and “guidance skills and effectiveness” dimensions measure the quality of discharge teaching, with a higher total score indicating better quality of discharge guidance received by the patient.
Readiness for Hospital Discharge Scale (RHDS)
The Chinese version of the Readiness for Hospital Discharge Scale (RHDS)23 was employed to assess participants’ readiness for discharge. This scale was originally developed by Weiss et al based on Transition Theory and subsequently localized and revised for Chinese contexts by Zhao Huiling et al.
Comprising 23 items, the RHDS encompasses four dimensions: physical condition (7 items), disease-related knowledge (8 items), post-discharge coping capacity (3 items), and perceived social support (4 items). As a self-report summative scale, the first item is a binary (yes/no) question and excluded from the total score calculation. The remaining 22 items are rated on a 0–10 Likert-type scale, where “0” denotes “complete unawareness/total inability” and “10” indicates “full awareness/excellent ability.” Notably, items 3 and 6 are reverse-scored.
All participants completed the scale independently within 4 hours prior to hospital discharge. The total RHDS score was derived from the sum of scores across the four dimensions, with higher total scores indicating greater discharge readiness. The scale has demonstrated robust reliability and validity, making it suitable for evaluating discharge readiness among elderly patients undergoing day surgery.
Covariables
Patient basic information extracted from the electronic medical record system included gender, age, height, weight, chronic disease history, residence, educational attainment, disease type, pain assessment, choice of surgical anesthesia method, and surgical classification. Independent variables comprised patient characteristics (age: continuous variable/interval-coded; educational attainment: illiterate=1, elementary school=2, junior high school and above=3), quality of discharge preparation (measured by QDTS total score, where higher scores indicate better discharge instruction quality), readiness for discharge (measured by RHDS total score, where higher scores indicate greater preparedness), and family care capacity (measured by PSS-FA, where higher scores indicate higher perceived levels of family social support).
Data Analysis
First, descriptive statistical analysis was conducted on the baseline demographic characteristics (including gender, age, education level, monthly income, medical payment type, marital status, place of residence, and housing status) and chronic disease history of the 340 elderly patients included in the study. Categorical variables are presented as frequencies and percentages (%), while continuous variables are expressed as mean ± standard deviation (Mean ± SD).
To preliminarily explore the relationships among health behavior capacity, family support level, quality of discharge instructions, and discharge readiness, as well as the associations between these variables and other demographic factors, Spearman’s rank correlation analysis was employed. This method was selected because Shapiro–Wilk normality tests indicated that the scores for health behavior capacity, family support level, quality of discharge instructions, and discharge readiness did not follow a normal distribution. Additionally, some demographic data were categorical or ordinal variables. The Spearman correlation coefficient (rs) ranges from −1 to 1, with values closer to 1 indicating stronger correlation; rs>0 denotes positive correlation, while rs<0 indicates negative correlation. A p-value <0.05 was considered statistically significant.
To further investigate the independent effects of health behavior capacity, family support level, and discharge teaching quality on discharge readiness while controlling for potential confounders, a multiple linear regression model was constructed. The dependent variable was the discharge readiness score. Independent variables included health behavior capacity scores, family support scores, discharge teaching quality scores, and gender as a control variable (included as a dummy variable, with males as the reference group). Preliminary analysis indicated that some variables were non-significant when all independent variables were initially included in the model. Furthermore, correlation analysis suggested that family support and discharge teaching quality might indirectly influence discharge readiness through complex pathways. Therefore, stepwise regression was employed to screen independent variables, retaining only those with significant contributions to the final model. Overall model significance was assessed via analysis of variance (F-test). Regression coefficients (B) and their standard errors (SE), standardized regression coefficients (β), t-values, and 95% confidence intervals (95% CI) were used to evaluate the magnitude and direction of each independent variable’s effect. P-values <0.05 were considered statistically significant.
Given multiple latent variables in this study, including health behavior capacity, family support, discharge teaching quality, and discharge readiness, as well as complex multi-path associations with direct and indirect effects, SEM was adopted to simultaneously evaluate the measurement quality of latent constructs and examine structural pathways. SEM combines factor analysis with path analysis, making it suitable to validate measurement models linking observed indicators and latent variables, and to estimate structural associations across latent variables. AMOS 24.0 was used to conduct all SEM analyses. A total of 340 elderly patients were included in the current study. The sample size met the classic SEM requirement of 10–15 times the number of questionnaire items and achieved the recommended threshold for stable model convergence. Model fit was assessed using χ2/df, CFI, TLI, RMSEA, and SRMR. The acceptable fit criteria were defined as χ2/df <3.0, CFI and TLI >0.90, and RMSEA and SRMR <0.08. Standardized path coefficients and corresponding P-values were used to interpret inter-variable relationships. Bootstrap estimation with 5000 resamples and 95% confidence intervals was performed to test mediating and indirect effects. Prior to model construction, the Harman single-factor test was used to detect common method bias, and Mardia’s coefficient was calculated to evaluate multivariate normality. Rigorous assessments of these two key methodological assumptions were completed to guarantee overall model validity.
Results
Characteristics of Participants
A total of 340 participants were invited to participate in the present study. All 340 invited individuals consented to enrollment and completed the questionnaires. No participants were excluded because of missing data, resulting in a final sample size of 340 for analysis. The baseline characteristics of the study participants are summarized in Table 1. The average age of the participants was 68.14±9.207 years. With respect to chronic disease history, most participants had 1 or 2 chronic diseases (34.1% and 32.4% respectively), 27.9% of participants had 3 or more chronic diseases, and only 5.6% of participants had no chronic disease history.
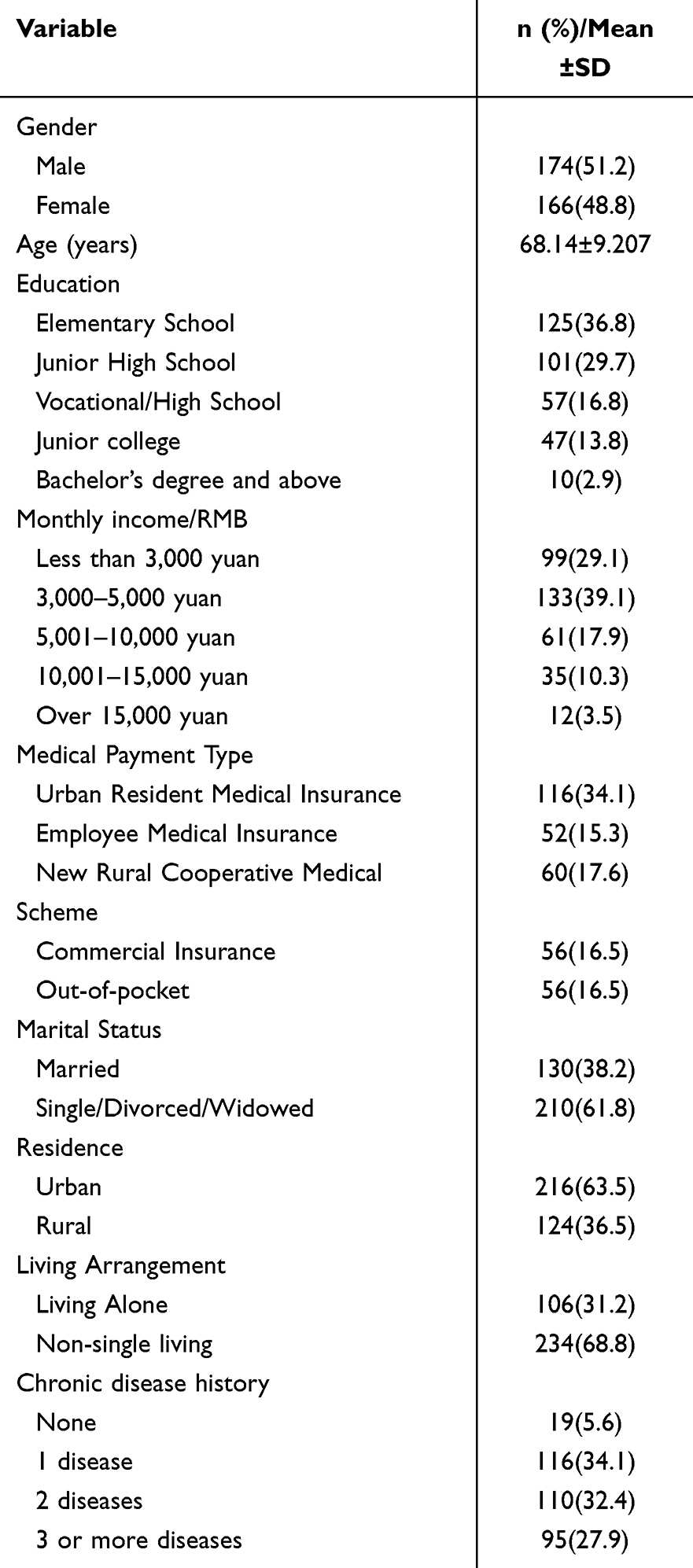 |
Table 1 Characteristics of the Elderly Patients Who Underwent Day Surgery |
Correlations Between Demographic Characteristics, Health-Related Factors and Readiness for Discharge
Results indicate (Table 2) that discharge readiness significantly correlates with gender, with a correlation coefficient rs=0.119. Since rs>0, this indicates a positive correlation between variables. P=0.029, less than 0.05, confirms a statistically significant positive correlation between discharge readiness and gender at the 0.05 level. Readiness for discharge was significantly correlated with health behavior capacity, with a correlation coefficient rs=0.226. Since rs>0, this indicates a positive correlation between variables. P<0.001 indicates that readiness for discharge and health behavior capability are significantly positively correlated at the 0.01 level. Readiness for discharge was significantly correlated with family support, with a correlation coefficient rs =−0.178. Since rs<0, the variables showed a negative correlation. P<0.001 indicates a significant negative correlation between readiness for discharge and family support at the 0.01 level. Readiness for discharge was significantly correlated with quality of discharge teaching, with a correlation coefficient rs=0.178 and rs>0, indicating a positive relationship between variables. P<0.001 confirmed a significant positive correlation between readiness for discharge and quality of discharge teaching at the 0.01 level.
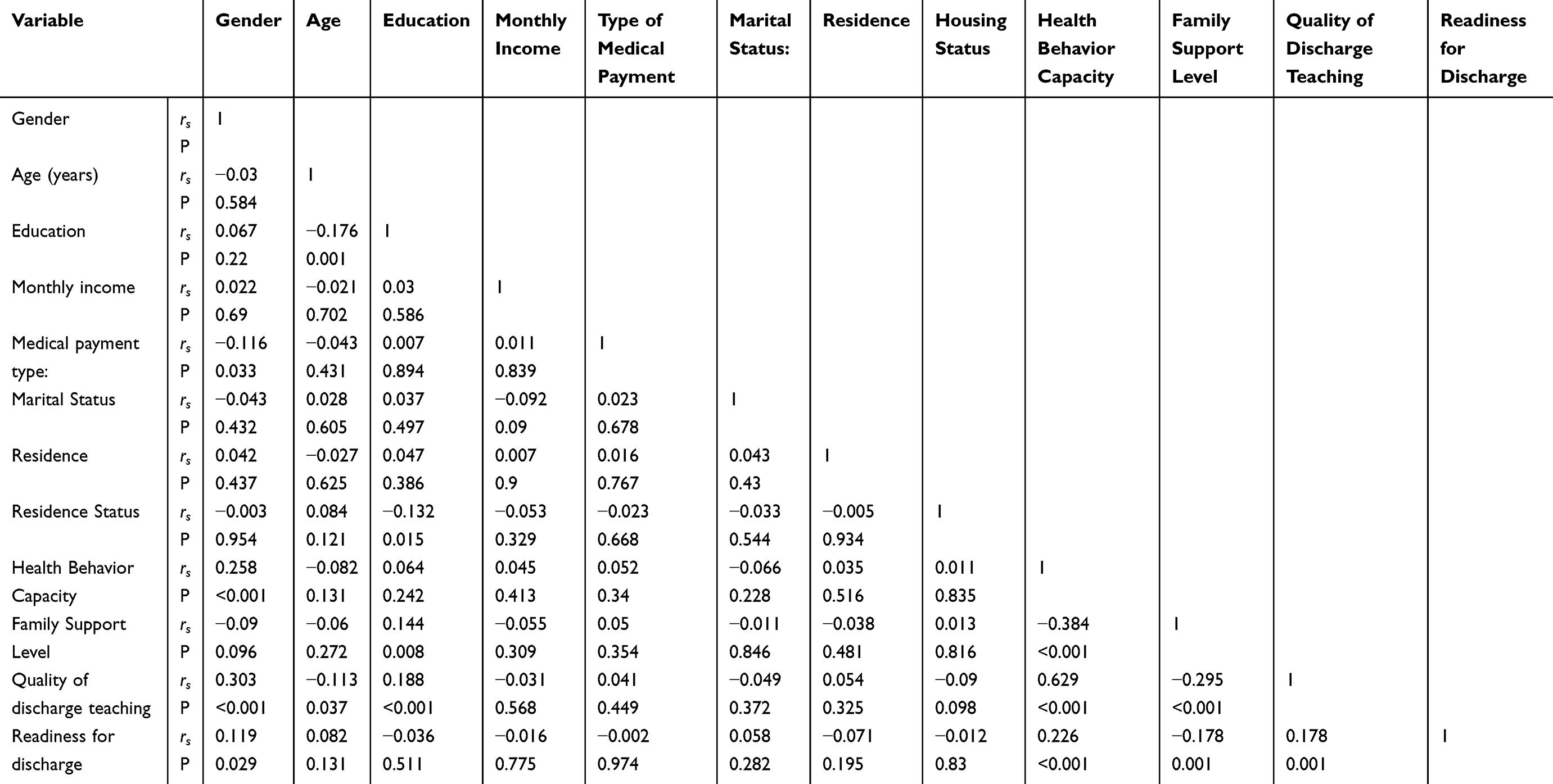 |
Table 2 Correlations Among Variables and Readiness for Discharge |
Factors Associated with Readiness for Discharge
This study employed readiness for discharge as the dependent variable, with health behavior capacity, family support level, and quality of discharge instructions as independent variables. Demographic gender was used as a control variable, treated as a categorical variable. Therefore, gender was included as a dummy variable in the regression model. A multiple linear regression model was established, and the stepwise method was used to screen independent variables, retaining only statistically significant factors in the model. Table 3 shows the model statistic F=19.386 with significance (P<0.001), indicating overall statistical significance. This confirms the model can identify factors influencing discharge readiness. Table 4 demonstrates the significant effect of health behavior capacity (P<0.001), with regression coefficient B=0.396 and standardized regression coefficient β=0.233. Greater than 0, indicating that health behavior capacity is a significant positive factor influencing discharge readiness. Higher health behavior capacity scores correlate with higher discharge readiness:
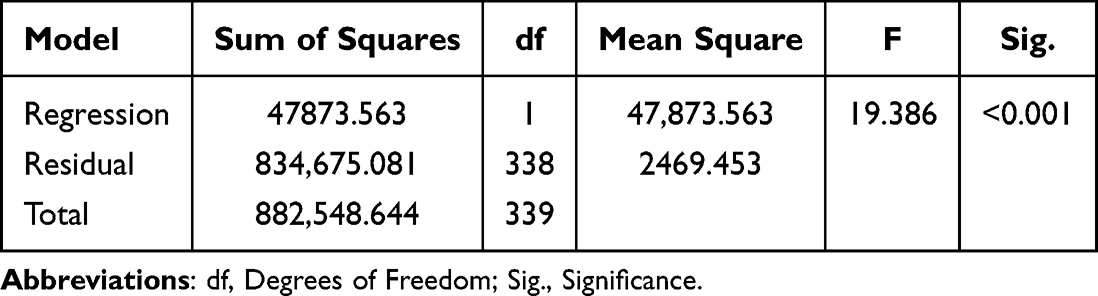 |
Table 3 ANOVA of the Simple Linear Regression Model |
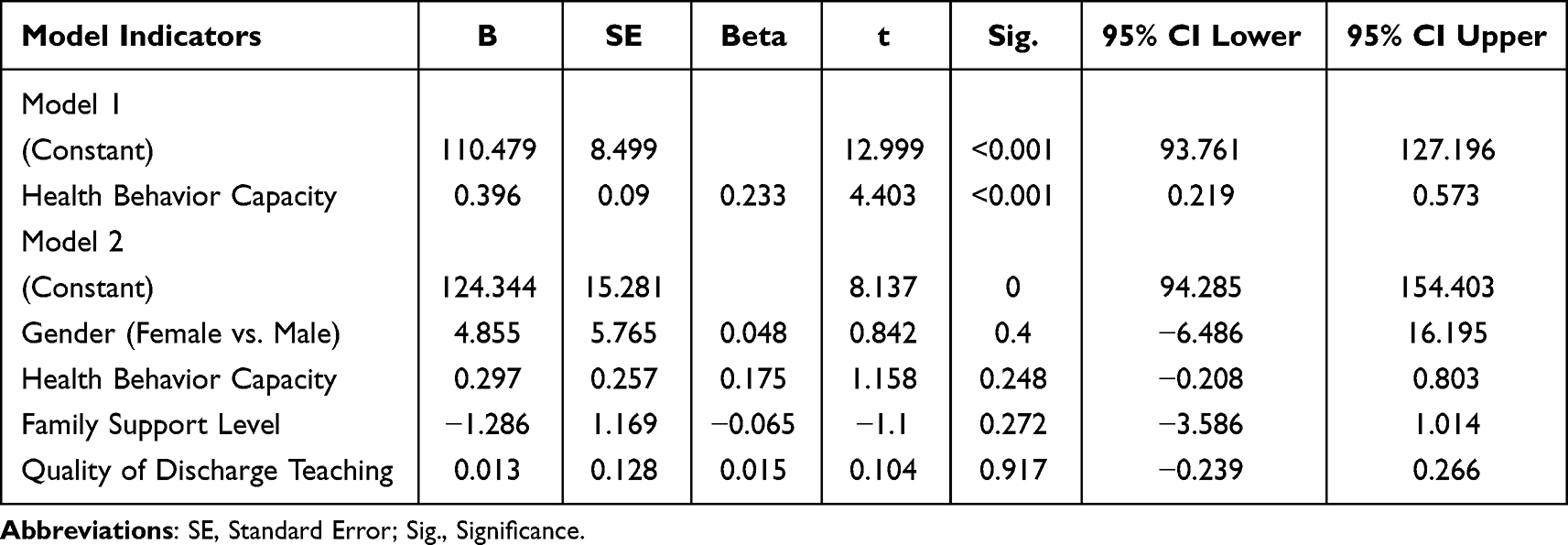 |
Table 4 Univariate Regression Analysis of Health Behavior Capacity on Readiness for Discharge |
Regression Model: Readiness for Discharge = 110.479 + 0.233 × Health Behavior Capacity
Path Analysis of Factors Influencing Discharge Readiness
After multicollinearity treatment and data standardization, the SEM (Figure 1), demonstrated adequate fit to the data (χ2/df =1.78, CFI =0.952, TLI =0.943, RMSEA =0.047, SRMR =0.042). Three exogenous latent variables directly predicted discharge readiness. The standardized path coefficients indicated that: Family support exhibited the strongest positive direct effect on discharge readiness (β =0.47, P<0.001). Health behavior capacity showed a significant positive direct effect (β = 0.31, P<0.001). Discharge teaching quality had a weak but statistically significant positive direct effect (β =0.15, P<0.05). Correlations among the exogenous variables were all statistically significant (P<0.001): the correlation between health behavior capacity and family support was r =0.51, between health behavior capacity and discharge teaching quality was r =0.37, and between family support and discharge teaching quality was r =0.44. The residual variance of discharge readiness was 0.33, indicating that the model explained 67% of the variance in discharge readiness. Overall, family support is the key factor enhancing discharge readiness, health behavior capacity has a modest positive effect, while the impact of discharge teaching quality is negligible. Further research may explore whether mediating or chain effects exist among the exogenous variables.
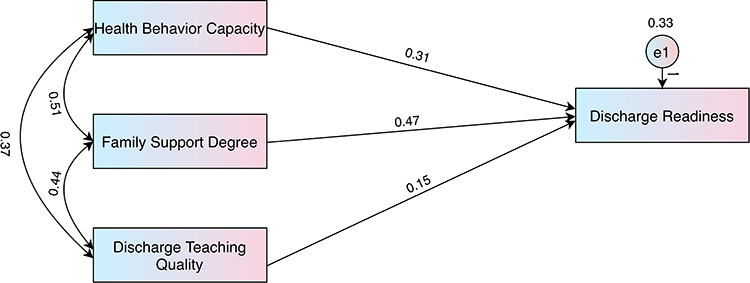 |
Figure 1 Path analysis of health behavior capacity, family support, and discharge teaching quality on discharge readiness. |
Discussion
This study aims to explore key factors influencing the transition from discharge readiness to home-based rehabilitation among elderly day surgery patients. Through comparative analysis of multiple linear regression and structural equation modeling results, we found that patients’ social support systems and self-management capabilities play complex and dynamic roles during the discharge preparation process.
In the multiple linear regression analysis, health behavior capacity was identified as a significant positive predictor of discharge readiness (β=0.233, Р<0.001). This finding aligns with conventional wisdom: patients with strong self-management skills who actively seek health information and adhere to medical instructions typically express greater confidence in managing post-discharge life. Health behavior competence extends beyond physical self-care to emphasize patients’ capacity for active disease management.24 For instance, among schizophrenia patients, this encompasses medication management, symptom control, daily life maintenance, and utilization of health resources.25 Research indicates that ostomy patients with higher self-efficacy demonstrate greater readiness for discharge and more effective management of complications and daily living.26 However, when introducing structural equation modeling for more complex path analysis, the direct effect coefficient of health behavior competence on discharge readiness decreased to 0.31. This discrepancy suggests that while health behavior capacity is crucial, it may not operate in isolation. Instead, it likely functions as a “mediating variable” or “moderating variable” that translates into actual readiness through family support and discharge instructions. During the transition from hospital to home, patients require “coping” abilities—accepting reality, assuming responsibility, and actively adjusting their mindset. Lack of this psychological behavioral capacity leads to maladaptive outcomes.24 Simultaneously, patients with lower education or poorer economic status can still achieve high discharge readiness if they possess strong family motivation and high adaptive capacity.27 This demonstrates that health behavioral ability does not exist in isolation but is embedded within the family system.
According to structural equation modeling results, although family support did not show significant independent predictive power in regression analysis (Р=0.272), it exhibited the strongest positive predictive effect (path coefficient of 0.47) in the SEM model. Correlation analysis and SEM produced inconsistent results regarding the association between family support and discharge teaching quality. Bivariate correlation showed family support was negatively linked to discharge readiness, while adjusted SEM identified its positive protective effect. This discrepancy stemmed from unadjusted confounders such as demand bias and sample traits in simple correlation analysis, whereas SEM reflected true relationships after confounding control. Though discharge teaching quality was positively correlated in bivariate analysis, its effect size diminished in SEM due to multicollinearity, common method bias and indirect effects. These results demonstrate that bivariate analysis only reveals superficial correlations, and multivariate adjusted models yield more robust, credible outcomes. Clinically, more attention should be paid to the independent predictive roles of family support and health behavioral ability in patients’ discharge readiness. Family care, as a form of social support, can buffer the negative impact of stigma on patients. High levels of family support help patients build confidence (psychological resources), thereby enhancing their self-management capabilities after discharge.28 Conversely, lack of support exacerbates stigma and reduces self-efficacy.29 Research indicates that patients and caregivers form an inseparable unit. Caregiver readiness (an extension of self-management capacity) directly impacts patients.30 Family members’ understanding, encouragement, and emotional reassurance significantly boost patient confidence. Perceived social support (especially familial) partially mediates the relationship between psychological resilience and discharge readiness.31
This finding profoundly reveals the “social attributes” of disease management. Within the Chinese cultural context, the family often serves as the core bastion for patients battling illness. The SEM model captures the latent variable role of family support in profoundly empowering patients’ psychological capital and practical coping abilities. This indicates that family support is not merely emotional solace but the cornerstone upon which patients build confidence for discharge. The regression model failed to capture this aspect, likely because family support often exerts its influence indirectly by affecting patients’ health behavior capabilities (such as medication adherence reminders, rehabilitation assistance). This complex chain of mediating effects can only be clearly identified through the holistic model perspective offered by SEM.
Research findings indicate that while discharge teaching quality shows a statistically significant positive correlation with discharge readiness, its path coefficient in the SEM model is extremely low (0.15) and may suffer from multicollinearity issues. This suggests that current discharge instruction models may exhibit a tendency toward “formalization.” Research has shown that even patients who are young, less educated, low-income, and have low adaptive capacity (such as extremely weak personal capabilities) can achieve “high discharge readiness” if they receive high-quality discharge instructions.28 Healthcare providers’ teaching skills in discharge instruction can significantly enhance patients’ self-management abilities.32 However, mere verbal instruction or distribution of written materials, if not effectively integrated with the patient’s family support system and failing to tangibly improve their health behavior capabilities, will have very limited direct impact on enhancing discharge readiness. This suggests that discharge instructions should be provided promptly during the discharge assessment process, rather than solely at the time of discharge. Furthermore, standardized discharge instructions often lack detailed guidance tailored to specialized patients, failing to identify genuine risks.33
Limitations of the Study
Several limitations of the present study should be acknowledged. As a single-center cross-sectional survey recruiting participants from a single day surgery ward only, the restricted sampling scope may limit sample representativeness and constrain the generalizability of the findings to other regions and clinical populations. Convenience sampling and self-reported questionnaire data collection may introduce potential selection bias and common method bias, as subjective self-assessments might not fully reflect objective clinical conditions. While structural equation modeling was used to examine direct relationships among key variables, potential mediating and moderating pathways were not further explored, leaving the complex underlying mechanisms insufficiently clarified. This study primarily focused on demographic and psychosocial factors without incorporating objective clinical indicators, which may partially reduce the model’s explanatory power. Additionally, the cross-sectional design precludes definitive causal inference. Further longitudinal studies are warranted to validate causal associations and dynamic changes in discharge readiness over time.
Conclusion
In summary, this study adopted structural equation modeling to preliminarily explore the influencing mechanisms of discharge readiness, offering empirical references for optimizing hospital-to-home transitional care. Notably, this cross-sectional design cannot confirm definite causal relationships, and the constructed model only explains partial influencing pathways with certain limitations. Although the findings offer implications for reducing postoperative risks and improving home rehabilitation among elderly day surgery patients, relevant conclusions should be interpreted cautiously. Further multi-center longitudinal research is required to verify causal links, resolve statistical discrepancies, and enrich the model by incorporating psychological status and healthcare resource accessibility. Clinically, targeted interventions should focus on improving patients’ health behaviors and consolidating family support. Such combined measures may serve as a promising strategy to promote discharge readiness in this vulnerable elderly group.
Abbreviations
SEM, Structural Equation Modeling; OR, Odds Ratio; KPI, Key Performance Indicator; DP, Discharge planning.
Data Sharing Statement
The data associated with this article are not publicly available, but can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Huadong Hospital Affiliated to Fudan University Review Board (approval No. 20240166). All patients signed informed consent.
Consent for Publication
All Authors have read and approved the final version.
Acknowledgments
We would like to thank all of the participants who volunteered their time to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Approved Management Research Project of Shanghai Hospital Association (X2024173), Nursing Talent Training Program of Huadong Hospital (HLXX2202).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen X, Bian H, Li M, Zhou Y, Yang Y, Wu Z. Construction of discharge preparation service for patients undergoing cataract day surgery based on evidence and its empirical application. Geriatric Nursing. 2025;66(Pt A):103556. doi:10.1016/j.gerinurse.2025.103556
2. Sig JR, Nielsen C, Bille C, Thomsen JB, Sorensen JA. Patients’ experiences of day surgery: a qualitative systematic review. J Adv Nurs. 2026;82(1):247–12. doi:10.1111/jan.16930
3. Ning PT, Liu XN. Analysis of the development drivers and prospects of day medicine in China. West China Med J. 2026;41(2):182–185. doi:10.7507/1002-0179.202601031
4. Kucharczuk C, Lightheart E, Kodan A, et al. Standardized discharge planning tool leads to earlier discharges and fewer readmissions. J Nurs Care Qual. 2022;37(1):54–60. doi:10.1097/NCQ.0000000000000558
5. Maryani N, Amsriza FR, Wahyuni A, Lutfa R. The effectiveness of patient discharge time in one-day care (ODC) surgical patients based on PADSS scoring. Anaesthesia Pain Intensive Care. 2024;28(2). doi:10.35975/apic.v27i2.2196
6. Van Caelenberg E, De Regge M, Eeckloo K, Coppens M. Analysis of failed discharge after ambulatory surgery: unanticipated admission. Acta Chir Belg. 2019;119(3):139–145. doi:10.1080/00015458.2018.1477488
7. Lin L, Fang Y, Wei Y, Huang F, Zheng J, Xiao H. The effects of a nurse-led discharge planning on the health outcomes of colorectal cancer patients with stomas: a randomized controlled trial. Int J Nurs Stud. 2024;155:104769. doi:10.1016/j.ijnurstu.2024.104769
8. Mhof L, Heber R, Blume KS, Schreyoegg J, Winter V. Hospital discharge planning—an investigation of outcomes and interventions. Health Serv Res. 2026;61(1):e70060. doi:10.1111/1475-6773.70060
9. You H, Lei A, Li X, Liao X, Chang J. Discharge teaching, patient-reported discharge readiness and postsurgical outcomes in gynecologic patients undergoing day surgery: a generalized estimating equation. BMC Surg. 2022;22(1):166. doi:10.1186/s12893-022-01607-x
10. Güven B, Karaaslan Sevinç C. Examining the relationship between perceived readiness for hospital discharge and quality of perioperative nursing care in ambulatory surgery patients. Bakirkoy Tip Dergisi. 2024;271–279. doi:10.4274/BMJ.galenos.2024.2024.4-2
11. Rahayu U, Ibrahim K, Herman H. Application of normalization process theory in discharge planning: a systematic review of implementation strategies and outcomes. J Multidiscip Healthc. 2025;18:2997–3008. doi:10.2147/JMDH.S523495
12. Xiao S, Dai Y, Huang M. Association between obesity and risk of delayed discharge and unplanned readmission for day surgery: a systematic review and meta-analysis. Int J Nurs Prac. 2024;30(3):e13203. doi:10.1111/ijn.13203
13. McEwan K, Sanders T, Carr S, et al. Co-producing personalised discharge planning: developing a toolkit to improve caregiver involvement in hospital transitions. Health Expect. 2025;28(6):e70483. doi:10.1111/hex.70483
14. Yang J, Ge L, Ju -X-X, Liu -X-X. Status and influencing factors of discharge readiness in day surgery lung cancer patients under a fast-track rehabilitation pathway. J Clin Nurs. 2025;34(11):4779–4787. doi:10.1111/jocn.17743
15. Eckhardt H, Kreutzberg A, Busse R. Day surgery—International experiences, remuneration systems and financial incentives in England, France and Austria. Arthroskopie. 2024;37(1):3–10. doi:10.1007/s00142-023-00650-x
16. Luo J, Xie C, Fan D. Historical development and experience of day surgery in China: from the perspective of anesthesiologists. Paediatr Anaesth. 2025;35(6):412–423. doi:10.1111/pan.15078
17. Shah S, Qureshi F, Stanley S, Bennett-Guerrero E. Unplanned hospital admissions within 24 h after 53,185 surgical procedures at a U.S. ambulatory surgery center. Perioperative Medicine. 2024;13(1):88. doi:10.1186/s13741-024-00447-y
18. Van Caelenberg E, Benoit D, Verhaeghe R, Coppens M. Unanticipated admission after ambulatory surgery in the pediatric population: a single-center retrospective analysis. Acta Chir Belg. 2022;122(3):178–184. doi:10.1080/00015458.2021.1893579
19. Goncalves-Bradley DC, Lannin NA, Clemson L, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2022;2(2):CD000313. doi:10.1002/14651858.CD000313.pub6
20. Becker H, Stuifbergen A, Oh H, Hall S. Self-rated abilities for health practices: a health self-efficacy measure. Health Values. 1970;17(5):42–50.
21. Hu YQ, Zhou LS. Reliability and validity of the Chinese version of the health self-management ability scale. Chin J Nurs. 2012;47(3):261–262. doi:10.3761/j.issn.0254-1769.2012.03.026
22. Procidano ME, Heller K. Measures of perceived social support from friends and from family: three validation studies. Am J Commun Psychol. 1983;11(1):1–24. doi:10.1007/BF00898416
23. Candela L, Piacentine LB, Bobay KL, Weiss ME. Teaching students to teach patients: a theory-guided approach. J Nurs Educ Pract. 2018;8(11):92–101. doi:10.5430/jnep.v8n11p92
24. Rababah JA, Al-Hammouri MM, Radaideh A. The association between health literacy and readiness for hospital discharge among family caregivers of acute myocardial infarction patients. Appl Nurs Res. 2025;83:151950. doi:10.1016/j.apnr.2025.151950
25. Uwera A, Yang Q, Zhang S, et al. Factors influencing readiness for hospital discharge among patients with schizophrenia: a cross-sectional study. J Eval Clin Pract. 2025;31(7):e70277. doi:10.1111/jep.70277
26. Lin L, Zheng J, Lin Z, Xiao H. Understanding the challenges of readiness for hospital discharge in stoma patients: a mixed-methods study. J Clin Nurs. 2025;34(5):1704–1712. doi:10.1111/jocn.17654
27. Qin Y-H, Shi X-M. Status quo and influencing factors of readiness for hospital discharge in patients with brain tumours after surgery. Front Oncol. 2024;14:1324810. doi:10.3389/fonc.2024.1324810
28. Chen D, Xu L, Lee G, Wang X. Complex determinants of hospital discharge readiness among patients with acute myocardial infarction: a fuzzy-set qualitative comparative analysis. Int J Nurs Stud. 2025;170:105172. doi:10.1016/j.ijnurstu.2025.105172
29. Xu Y, Fei X, Qi Q, Chen Y, Wang Z, Yang R. Exploring the interplay of stigma, family care, and discharge readiness in patients with malignant obstructive jaundice undergoing percutaneous transhepatic cholangial drainage recovery. BMC Psychol. 2025;13(1):775. doi:10.1186/s40359-025-03085-1
30. Wang L, Zhang Q, Li J, et al. The effect of tailored nursing interventions based on the IKAP model on the discharge readiness of the spouses or children of breast cancer patients: a randomized controlled trial. Support Care Cancer. 2025;33(9):765. doi:10.1007/s00520-025-09819-6
31. Fuentes-Ramirez A, Carvajal-Carrascal G, Roa-Lizcano KT, Pena-Mancera LX, Sanchez-Herrera B. Patient and family caregiver adaptation during hospital-home transition: a concept analysis. Revista da Escola de Enfermagem da USP. 2025;59:e20240363. doi:10.1590/1980-220X-REEUSP-2024-0363en
32. Shu P, Xuan L, Jiang X. Discharge readiness and associated factors among patients with coronary heart disease after stent implantation: a cross-sectional single center study. Patient Prefer Adherence. 2024;18:1373–1383. doi:10.2147/PPA.S465918
33. Chen C, Sun Y, Chen C, et al. Development and validation of a patient discharge readiness scale for daytime cataract surgery (DRS-CAT). J Peri Anesthesia Nurs. 2024;39(2):195–201,e3. doi:10.1016/j.jopan.2023.07.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.