Back to Journals » International Journal of Women's Health » Volume 13
Factors Associated with Successful Vaginal Birth After a Primary Cesarean Section in Women with an Optimal Inter-Delivery Interval
Authors Maroyi R ![]() , Naomi B, Moureau MK, Marceline BS, Ingersoll C, Nerville R, Mukwege D
, Naomi B, Moureau MK, Marceline BS, Ingersoll C, Nerville R, Mukwege D
Received 14 August 2021
Accepted for publication 26 September 2021
Published 5 October 2021 Volume 2021:13 Pages 903—909
DOI https://doi.org/10.2147/IJWH.S334269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Raha Maroyi,1,2 Bahaya Naomi,2 Madeline K Moureau,3 Balungwe Sifa Marceline,1 Celeste Ingersoll,4 Roselyn Nerville,5 Denis Mukwege1,2,6
1Department of Obstetrics and Gynecology, Panzi Referral Hospital, Bukavu, South Kivu, Democratic Republic of Congo; 2Université Evangélique en Afrique (UEA), Bukavu, South Kivu, Democratic Republic of Congo; 3Department of Obstetrics and Gynecology, University of Wisconsin School of Medicine and Public Health, Madison, WI, USA; 4Department of Statistics, Brigham Young University, Provo, UT, USA; 5University of Utah School of Medicine, Salt Lake City, UT, USA; 6International Center for Advanced Research and Training (ICART), Bukavu, South Kivu, Democratic Republic of Congo
Correspondence: Raha Maroyi
Université Evangélique en Afrique (UEA), PO Box: 266, Bukavu, South Kivu, Democratic Republic of Congo
Tel +243 997 254 812
Email [email protected]
Purpose: We sought to determine the success rate of VBAC and factors associated with achieving VBAC at a referral hospital in the Democratic Republic of Congo in women with a subsequent pregnancy greater than or equal to 18 months from their primary cesarean section (CS).
Patients and Methods: Patients were included for participation if they had an inter-delivery interval (IDI) of at least 18 months from their primary CS, accepted TOLAC, and had no contraindications. Information was collected about patients’ demographics, obstetric history, and factors impacting their labor process. Descriptive analyses compared patients that had a successful VBAC and those who did not. Univariate and multivariate binary logistic regression models identified factors associated with a successful VBAC.
Results: Among 231 eligible patients who attempted a VBAC, 57.6% (133) achieved VBAC. Participants had a mean age of 29 (SD 6), with the majority having a prior vaginal delivery (68.8%). VBAC was positively associated with a higher Bishop score (AOR 1.12, 95% CI 1.02, 1.23) and a spontaneous labor onset (AOR 3.06, 95% CI 1.52, 6.17). VBAC was negatively associated with a macrosomic fetus (AOR 0.21, 95% CI 0.08, 0.58).
Conclusion: TOLAC results in VBAC more than half the time and is associated with a spontaneous labor onset and a higher Bishop score. Women with a macrosomic fetus were more likely to have an unsuccessful VBAC, resulting in an RCS. An optimal IDI was not enough to ensure a successful VBAC. Upon patients’ arrival to the hospital, practitioners should re-evaluate their eligibility to attempt a VBAC based on their Bishop score and if they had a spontaneous labor onset to decrease the health risks of an RCS.
Keywords: trial of labor, delivery, repeat cesarean section, sub-Saharan Africa, Democratic Republic of Congo
Introduction
The rates of cesarean sections (CS) have increased worldwide and are projected to continue to increase, with countries in sub-Saharan Africa experiencing the lowest rates.1 In the World Health Organization’s most recent statement on CS, they advised that no region should have a CS higher than 10% and that CS should only be conducted when medically necessary, as CS can result in significant and permanent complications.2 Although the CS rate in the Democratic Republic of Congo (DRC) is within the recommended CS rate, women in developing countries experience a higher rate of complications due to CS compared to women in developed countries.3
In a recent study conducted in low- to middle-income countries, CS were found to be associated with an increase in all adverse outcomes, including postpartum hemorrhage, infection, dilation and curettage, hysterectomy, unplanned hospitalization, and maternal mortality.4 African countries experience significantly higher adverse outcomes compared to non-African countries.4 In addition, maternal mortality, after having a CS in Africa, has been estimated to be 50 times higher than the rates in high-income countries.5 A vaginal birth after cesarean (VBAC) has been recommended to limit maternal health risks that a repeat cesarean section (RCS) may result in.2,6–9 The major complication of attempting a VBAC is uterine rupture; however, studies have found that women with an inter-delivery interval (IDI) longer than 18 months had a decreased risk of uterine rupture.10−13
In low- to middle-income countries, a trial of labor after cesarean (TOLAC) can reduce maternal morbidity by allowing women to achieve a vaginal birth after cesarean (VBAC). The primary objective of this analysis is to determine the success rate of VBAC in women in the DRC with an IDI of at least 18 months, and the secondary objective is to analyze factors associated with a successful VBAC in this population.
Patients and Methods
Study Design
This study was approved by the DRC National Health Ethics Committee (Comité National D’éthique de la Santé, CNES/001/DPSK/1018PP/2018). We conducted a prospective cohort study from January 1, 2018, to December 31, 2018, in the maternity wards of Panzi Hospital, Bukavu, South-Kivu, DRC. Patients that had a primary CS during their previous pregnancy were advised during their prenatal care consultations on their delivery options and risk factors associated with both options, VBAC and RCS. Patients were eligible if they had an IDI of at least 18 months from their primary CS and agreed to attempt a trial of labor after cesarean (TOLAC). Patients were excluded from this analysis if they had more than one CS and if they had contraindications to a VBAC, such as a prior uterine rupture, a prior T-incision, and multiple gestations. Once informed consent was obtained from patients, they were followed throughout their pregnancy and labor; eight women elected not to participate in this study and were thus excluded.
Data was collected regarding (1) demographics (age, occupation, marital status, and regional location); (2) obstetrical history (parity, previous vaginal delivery, IDI, and indications for their primary CS); and (3) current obstetrical characteristics (gestational age, estimated fetal weight, uterine height, spontaneous labor onset, oxytocin use, Bishop score, delivery mode, and indications for RCS). The Bishop score was calculated using cervical dilation, effacement, station, consistency, and position.14
Definitions
For this study, individuals that had accepted TOLAC attempted a VBAC. Women who had a vaginal delivery were categorized as having a VBAC, a successful VBAC, or a successful TOLAC. Individuals that had an RCS were categorized as having failed VBAC or having an unsuccessful VBAC.
Acknowledging that the DRC may have different estimates for macrosomia compared to high-income countries, fetal birth weights in the 90th percentile and greater were classified as macrosomic in this analysis. Therefore, a macrosomic fetus was defined as a fetus weighing 3.65 kg or more.
Statistical Analysis
Descriptive statistics characterized the sample overall. Chi-square testing and t-testing were used to compare patients who had a successful VBAC (vaginal delivery) and those who did not (RCS). Univariate and multivariate logistic regression were used to identify factors associated with a successful VBAC. Variables were included for analysis in the regression model based on previous research findings and biological plausibility. Analyses were performed using SPSS version 27.0. A p-value less than 0.05 was considered statistically significant.
Results
Among 231 women who underwent TOLAC, 133 (57.6%) had a successful VBAC and 98 (42.4%) had an RCS. Table 1 describes demographic and maternal characteristics of the sample overall and compares those who did and did not have a successful VBAC. The mean age of the sample was 29 (SD 6). The majority of participants were from Ibanda, Bukavu, South-Kivu, DRC (54.5%). Most patients reported being married (93.5%) and working within their households (71.4%). Women who had a successful VBAC were significantly more likely to have a higher parity and a prior vaginal delivery. The indications for women’s primary CS are shown in Table 2; no previous indications for participant’s primary CS significantly increased the likelihood of failing VBAC. Table 3 breaks down indications for participant’s RCS.
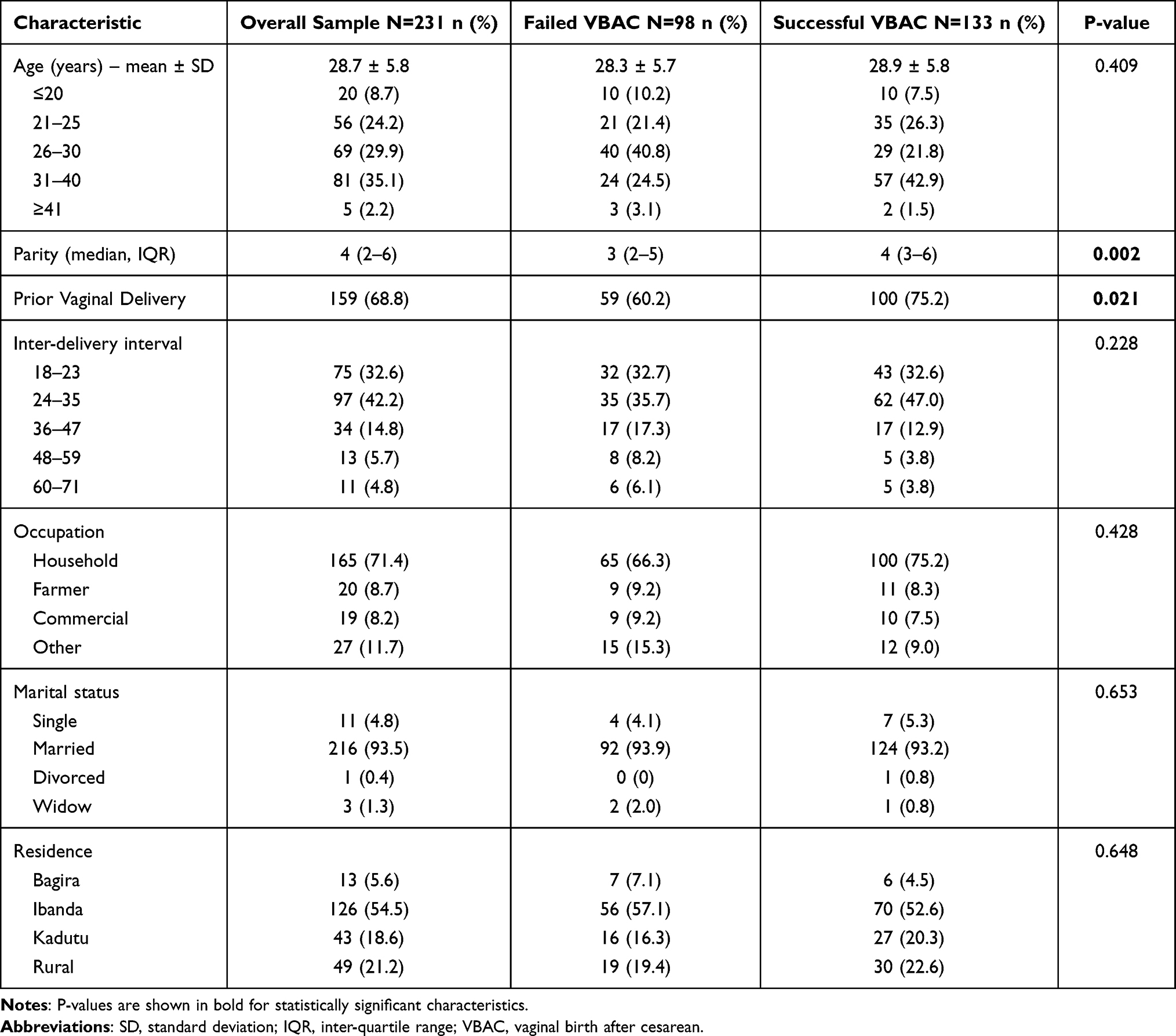 |
Table 1 Sample and Maternal Characteristics Stratified by Success or Failure of Vaginal Birth After Cesarean (VBAC) |
 |
Table 2 Indication for Primary Cesarean Section, Stratified by Delivery Mode |
 |
Table 3 Indication for Repeat Cesarean Section (RCS) |
Table 4 displays obstetrical and neonatal characteristics of patients stratified by success or failure of VBAC. Women who were carrying a fetus with a higher birth weight were more likely to fail their VBAC and, thus, women who had a macrosomic fetus (weighing 3.65 kg or more) were also more likely to fail their VBAC. Patients with a greater uterine height were also significantly more likely to fail their VBAC. Participants with a spontaneous labor onset and a higher Bishop score were more likely to have a successful VBAC.
 |
Table 4 Obstetrical and Neonatal Characteristics Stratified by Success or Failure of Vaginal Birth After Cesarean (VBAC) |
Factors associated with a successful VBAC are reported in Table 5 on univariate and multivariate logistic regression. Parity, prior vaginal delivery, spontaneous labor onset, and a higher Bishop score were statistically significantly more likely to result in a successful VBAC on univariate analysis, while fetal macrosomia decreased the likelihood of a successful VBAC. On multivariate analysis, individuals that had a spontaneous labor onset and a higher Bishop score were more likely to have a successful VBAC, whereas patients with a macrosomic fetus were less likely to have a successful VBAC.
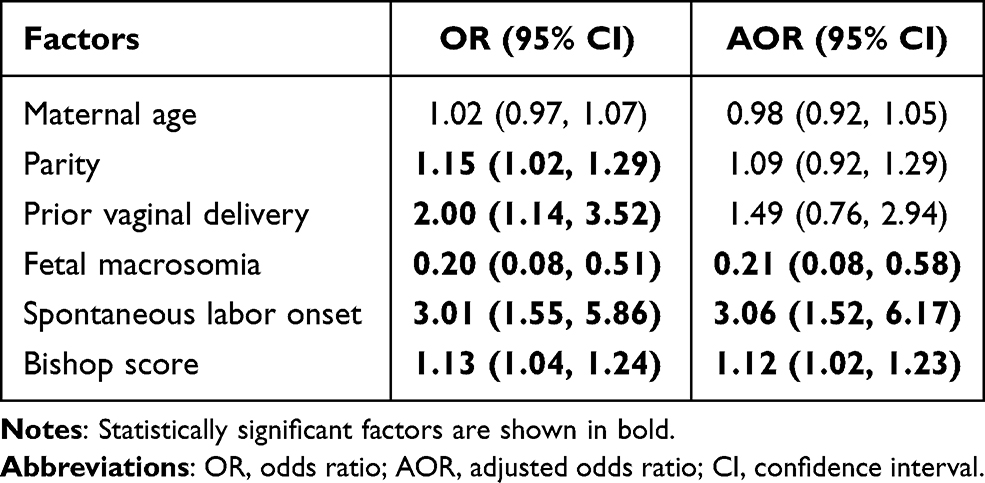 |
Table 5 Factors Associated with a Successful Vaginal Birth After Cesarean (VBAC) |
Discussion
In this analysis of 231 women from the DRC with a subsequent pregnancy greater than or equal to 18 months from their primary CS, 58% had a successful VBAC. A successful VBAC was associated with a spontaneous labor onset and a higher Bishop score. Women with a macrosomic fetus were less likely to have a successful VBAC. On multivariate analysis, no associations were found between a successful VBAC and the following variables: maternal age, parity, and a prior vaginal delivery.
The rate of VBAC success found in this analysis (58%) aligns with results found in other low- to middle-income countries. In a meta-analysis of hospitals in sub-Saharan Africa, Boulvain et al found that women with one prior CS had a VBAC success rate between 60% to 80%.15 More recent studies in sub-Saharan African countries have reported similar results, with studies reporting a VBAC success rate of 61% in Ghana, 67% in Nigeria, and 50–69% in Ethiopia.16–19 The range of VBAC success rates may be a result of different methodologies used in these studies.
Similar to our findings, other research has found that a spontaneous labor onset and higher Bishop score were associated with a successful VBAC.20–23 Gupta et al previously reported that, of patients who had a spontaneous labor onset, 91% had a successful VBAC, similar to our findings of 87% achieving a VBAC.22 Lin et al also found that both a spontaneous labor onset and Bishop score were associated with a successful VBAC.24 Both of these variables need to be assessed upon patients’ admission to the hospital, suggesting that health care providers need to re-evaluate patients’ eligibility for VBAC based on whether or not the patient had a spontaneous labor onset and their Bishop score when admitted.
We did not conclude that a prior vaginal delivery was associated with a successful VBAC. While a prior vaginal delivery was associated with a successful VBAC independently, this was not observed on multivariate analysis. This differs from previous studies that found an association between a prior vaginal delivery and a successful VBAC.6,23,25–28 This indicates there are stronger predictors for a successful VBAC than a prior vaginal birth in our analysis. Furthermore, a weak correlation was observed between parity and a prior vaginal delivery which may account for this discrepancy. Research has also identified a prior VBAC as a factor associated with a successful VBAC,29 however, women in this analysis were attempting a VBAC for the first time so a prior VBAC was not applicable to women in this study. These findings suggest that further research is needed to better understand the association between a prior vaginal birth and VBAC success, as well as a prior VBAC and VBAC success.
Several VBAC prediction models have been developed; however, at the time this study was conducted, no prediction models were validated in sub-Saharan Africa.30–33 In 2020, the Grobman prenatal VBAC calculator was validated in Ethiopia.18 This Grobman model uses information that is able to be assessed at patients’ first prenatal consultation.30 Importantly, in this study, the variables that were found to be significantly associated with a woman having a successful VBAC could not have been assessed at their first consultation. Other prediction models do incorporate intrapartum factors, however, to our knowledge, these models have yet to be validated in any sub-Saharan African country.32–34 Future research should validate a prediction model that uses intrapartum factors or develop a new prediction model specific to sub-Saharan African countries.
Strengths of this study include its prospective cohort design and, to our knowledge, is the first to analyze the success rate of VBAC and factors associated with a successful VBAC in women from the DRC. This study uses appropriate analyses to make a meaningful contribution to this population. This study is limited as it was conducted at a single medical center in the DRC with a relatively small number of women attempting a VBAC. The low rate of women attempting a VBAC may be a result of the low CS rate in the DRC. Additionally, the weight and height of women were not recorded, so patients’ Body Mass Index (BMI) was not able to be taken into consideration when analyzing factors associated with a successful VBAC. Previous studies have found that maternal obesity is associated with a lower VBAC success rate.18,35,36 Future research should examine how BMI and a prior VBAC in patients from the DRC influence the rate of VBAC success and adjust VBAC recommendations appropriately. In addition, future research efforts should incorporate multiple hospitals to obtain a greater, more representative sample.
Conclusion
In conclusion, more than half of the patients who accepted TOLAC had a VBAC; an optimal IDI was not enough to ensure a successful VBAC. Factors associated with a successful VBAC include a spontaneous labor onset and a higher Bishop score, while having a macrosomic fetus was shown to be negatively associated with a successful VBAC. Practitioners should offer TOLAC to all patients who only have one prior CS and do not have a macrosomic fetus. Upon patients’ admission to the hospital, practitioners should re-evaluate patients based on their Bishop score and if they had a spontaneous labor onset to reduce the effects that an RCS may have on maternal health.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; m, meter; CS, cesarean section; DRC, Democratic Republic of Congo; kg, kilogram; IDI, inter-delivery interval; IQR, inter-quartile range; OR, odds ratio; RCS, repeat cesarean section; SD, standard deviation; SPSS, Statistical Package for Social Science; TOL, trial of labor; TOLAC, trial of labor after cesarean; VBAC, vaginal birth after cesarean.
Acknowledgments
The authors acknowledge the medical staff and patients for participating in this study. We especially thank Dr. Heidi W. Brown for her contribution to this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6:6. doi:10.1136/bmjgh-2021-005671
2. World Health Organization Human Reproduction Programme A. WHO Statement on caesarean section rates. Reprod Health Matters. 2015;23(45):149–150. doi:10.1016/j.rhm.2015.07.007
3. Kwawukume EY. Caesarean section in developing countries. Best Pract Res Clin Obstet Gynaecol. 2001;15(1):165–178. doi:10.1053/beog.2000.0155
4. Harrison MS, Pasha O, Saleem S, et al. A prospective study of maternal, fetal and neonatal outcomes in the setting of cesarean section in low- and middle-income countries. Acta Obstet Gynecol Scand. 2017;96(4):410–420. doi:10.1111/aogs.13098
5. Bishop D, Dyer RA, Maswime S, et al. Maternal and neonatal outcomes after caesarean delivery in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet Glob Health. 2019;7(4):e513–e522.
6. Place K, Kruit H, Tekay A, Heinonen S, Rahkonen L. Success of trial of labor in women with a history of previous cesarean section for failed labor induction or labor dystocia: a retrospective cohort study. BMC Pregnancy Childbirth. 2019;19(1):176. doi:10.1186/s12884-019-2334-3
7. Tsakiridis I, Mamopoulos A, Athanasiadis A, Dagklis T. Vaginal birth after previous cesarean birth: a comparison of 3 national guidelines. Obstet Gynecol Surv. 2018;73(9):537–543. doi:10.1097/OGX.0000000000000596
8. Wingert A, Hartling L, Sebastianski M, et al. Clinical interventions that influence vaginal birth after cesarean delivery rates: systematic review & meta-analysis. BMC Pregnancy Childbirth. 2019;19(1):529. doi:10.1186/s12884-019-2689-5
9. Siddiqui SA. Obstetric factors for unsuccessful trial of labor in second-order birth following previous cesarean. Ann Saudi Med. 2013;33(4):356–362. doi:10.5144/0256-4947.2013.356
10. Wesson A, Assefa E. Maternal outcome following uterine rupture and its associated factors among mothers who delivered at Felege-Hiwot referral hospital, Amhara-Ethiopia. Int J. 2018;5(1):8.
11. Bujold E, Gauthier RJ. Risk of uterine rupture associated with an interdelivery interval between 18 and 24 months. Obstet Gynecol. 2010;115(5):1003–1006. doi:10.1097/AOG.0b013e3181d992fb
12. Huang WH, Nakashima DK, Rumney PJ, Keegan KA, Chan K. Interdelivery interval and the success of vaginal birth after cesarean delivery. Obstet Gynecol. 2002;99(1):41–44.
13. Ye L, Cao W, Yao J, Peng G, Zhou R. Systematic review of the effects of birth spacing after cesarean delivery on maternal and perinatal outcomes. Int J Gynaecol Obstet. 2019;147(1):19–28. doi:10.1002/ijgo.12895
14. Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol. 1964;24:266–268.
15. Boulvain M, Fraser WD, Brisson-Carroll G, Faron G, Wallast E. Trial of labour after caesarean section in sub-Saharan Africa: a meta-analysis. Br J Obstet Gynaecol. 1997;104(12):1385–1390. doi:10.1111/j.1471-0528.1997.tb11008.x
16. Seffah JD, Adu-Bonsaffoh K. Vaginal birth after a previous caesarean section: current trends and outlook in Ghana. J West Afr Coll Surg. 2014;4(2):1–25.
17. Oboro V, Adewunmi A, Ande A, Olagbuji B, Ezeanochie M, Oyeniran A. Morbidity associated with failed vaginal birth after cesarean section. Acta Obstet Gynecol Scand. 2010;89(9):1229–1232. doi:10.3109/00016349.2010.499448
18. Misgan E, Gedefaw A, Negash S, Asefa A. Validation of a vaginal birth after cesarean delivery prediction model in teaching hospitals of Addis Ababa University: a cross-sectional study. Biomed Res Int. 2020;2020:1540460. doi:10.1155/2020/1540460
19. Birara M, Gebrehiwot Y. Factors associated with success of vaginal birth after one caesarean section (VBAC) at three teaching hospitals in Addis Ababa, Ethiopia: a case control study. BMC Pregnancy Childbirth. 2013;13:31. doi:10.1186/1471-2393-13-31
20. Li YX, Bai Z, Long DJ, et al. Predicting the success of vaginal birth after caesarean delivery: a retrospective cohort study in China. BMJ Open. 2019;9(5):e027807. doi:10.1136/bmjopen-2018-027807
21. Kalok A, Zabil SA, Jamil MA, et al. Antenatal scoring system in predicting the success of planned vaginal birth following one previous caesarean section. J Obstet Gynaecol. 2018;38(3):339–343. doi:10.1080/01443615.2017.1355896
22. Gupta S, Jeeyaselan S, Guleria R, Gupta A. An observational study of various predictors of success of vaginal delivery following a previous cesarean section. J Obstet Gynaecol India. 2014;64(4):260–264. doi:10.1007/s13224-014-0519-2
23. Madaan M, Agrawal S, Nigam A, Aggarwal R, Trivedi SS. Trial of labour after previous caesarean section: the predictive factors affecting outcome. J Obstet Gynaecol. 2011;31(3):224–228. doi:10.3109/01443615.2010.544426
24. Lin J, Hou Y, Ke Y, Zeng W, Gu W. Establishment and validation of a prediction model for vaginal delivery after cesarean and its pregnancy outcomes-based on a prospective study. Eur J Obstet Gynecol Reprod Biol. 2019;242:114–121. doi:10.1016/j.ejogrb.2019.09.015
25. Wu Y, Kataria Y, Wang Z, Ming WK, Ellervik C. Factors associated with successful vaginal birth after a cesarean section: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19(1):360. doi:10.1186/s12884-019-2517-y
26. Haumonté JB, Raylet M, Sabiani L, et al. Quels facteurs influencent la voie d’accouchement en cas de tentative de voie basse sur utérus cicatriciel ?Predictive factors for vaginal birth after cesarean section [Predictive factors for vaginal birth after cesarean section]. J Gynecol Obstet Biol Reprod (Paris). 2012;41(8):735–752. French. doi:10.1016/j.jgyn.2012.09.032
27. Familiari A, Neri C, Caruso A, et al. Vaginal birth after caesarean section: a multicentre study on prognostic factors and feasibility. Arch Gynecol Obstet. 2020;301(2):509–515. doi:10.1007/s00404-020-05454-0
28. Trojano G, Damiani GR, Olivieri C, et al. VBAC: antenatal predictors of success. Acta Biomed. 2019;90(3):300–309.
29. Stamilio DM, Shanks A. Vaginal birth after cesarean (VBAC) outcomes associated with increasing number of prior VBACs. Womens Health (Lond). 2008;4(3):233–236. doi:10.2217/17455057.4.3.233
30. Grobman WA, Lai Y, Landon MB, et al. Development of a nomogram for prediction of vaginal birth after cesarean delivery. Obstet Gynecol. 2007;109(4):806–812. doi:10.1097/01.AOG.0000259312.36053.02
31. Grobman WA, Sandoval G, Rice MM, et al. Prediction of vaginal birth after cesarean delivery in term gestations: a calculator without race and ethnicity. Am J Obstet Gynecol. 2021. doi:10.1016/j.ajog.2021.05.021
32. Flamm BL, Geiger AM. Vaginal birth after cesarean delivery: an admission scoring system. Obstet Gynecol. 1997;90(6):907–910. doi:10.1016/S0029-7844(97)00531-0
33. Metz TD, Stoddard GJ, Henry E, Jackson M, Holmgren C, Esplin S. Simple, validated vaginal birth after cesarean delivery prediction model for use at the time of admission. Obstet Gynecol. 2013;122(3):571–578. doi:10.1097/AOG.0b013e31829f8ced
34. Grobman WA, Lai Y, Landon MB, et al. Does information available at admission for delivery improve prediction of vaginal birth after cesarean? Am J Perinatol. 2009;26(10):693–701. doi:10.1055/s-0029-1239494
35. Sentilhes L, Vayssière C, Beucher G, et al. Delivery for women with a previous cesarean: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol. 2013;170(1):25–32. doi:10.1016/j.ejogrb.2013.05.015
36. Wilson E, Sivanesan K, Veerasingham M. Rates of vaginal birth after caesarean section: what chance do obese women have? Aust N Z J Obstet Gynaecol. 2020;60(1):88–92. doi:10.1111/ajo.13003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.