Back to Journals » Patient Preference and Adherence » Volume 20
Factors Associated with Patient Treatment Satisfaction in Diabetes Mellitus Care Using the DTSQs: A Nationwide Cross-Sectional Study in Saudi Arabia
Authors Alqifari SF ![]() , Amirthalingam P
, Amirthalingam P ![]() , Prabahar K
, Prabahar K ![]() , Qasem KA
, Qasem KA ![]() , Alanazi FE, Alrasheed T
, Alanazi FE, Alrasheed T ![]() , Al-Ajlan NA, Aljabri A
, Al-Ajlan NA, Aljabri A ![]()
Received 8 September 2025
Accepted for publication 30 December 2025
Published 6 January 2026 Volume 2026:20 566025
DOI https://doi.org/10.2147/PPA.S566025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Saleh F Alqifari,1 Palanisamy Amirthalingam,1 Kousalya Prabahar,1 Khulood A Qasem,2 Fawaz E Alanazi,3 Tariq Alrasheed,4 Noura A Al-Ajlan,5 Ahmed Aljabri6
1Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 2College of Medicine, Sulaiman Alrajhi University, Al Bukairiyah, Saudi Arabia; 3Department of Pharmacology and Toxicology, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 4Department of Internal Medicine, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia; 5Department of Pharmacy, Dr. Sulaiman Al Habib Hospital, Riyadh, Saudi Arabia; 6Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Saleh F Alqifari, Email [email protected]
Introduction: Patient satisfaction is crucial in managing chronic diseases like diabetes mellitus (DM). This study aims to identify the key factors associated with patient satisfaction with DM treatment in the Kingdom of Saudi Arabia.
Methods: This cross-sectional study collected data from 709 participants country-wide via an online survey. Participants included patients receiving care from public and private healthcare facilities offering primary or specialized diabetes care. Patient satisfaction was assessed using the Diabetes Treatment Satisfaction Questionnaire (DTSQs), with chi-square tests for HbA1c control and Mann–Whitney U-tests for comparisons of means between groups.
Results: Governmental healthcare patients had higher satisfaction (Mean = 27.32, SD = 7.62) than private (Mean = 25.5, SD = 8.51) (p = 0.007). Patient treatment satisfaction was also greater in diabetes centers (Mean = 28.93, SD = 6.34), than in primary care (Mean = 25.45, SD = 8.51), (p= < 0.001). Although overall treatment satisfaction scores did not differ significantly between controlled and uncontrolled diabetes (p= 0.784), patients with controlled diabetes experienced significantly fewer hyperglycemic and hypoglycemic episodes, (p= < 0.001), and higher satisfaction with treatment flexibility (p= 0.006), diabetes understanding (p= 0.013) and willingness to recommend their treatment to others (p= < 0.001).
Conclusion: Mode of healthcare delivery (public or private hospitals) and choice between primary care or diabetes centers was significantly associated with treatment satisfaction with greater satisfaction in governmental healthcare and specialized diabetes centers. Glycemic control, measured by HbA1c, showed no significant association with overall treatment satisfaction but was associated with specific item scores (including satisfaction with understanding and treatment flexibility). This study is among the first in Saudi Arabia to compare DM treatment satisfaction across different healthcare settings using the DTSQs. Recognizing these associations can provide healthcare professionals with valuable insights for more successful treatment of diabetes patients and ultimately improve patient outcomes.
Keywords: treatment satisfaction, diabetes mellitus, healthcare delivery, glycated hemoglobin, HbA1c, diabetes treatment
Introduction
Diabetes Mellitus (DM) comprises a group of metabolic disorders characterized by chronic hyperglycemia resulting from impaired insulin secretion, insulin effect or both, and it stands as a prevalent chronic condition that demands comprehensive medical attention.1–5 In recent years, the Kingdom of Saudi Arabia (KSA) has witnessed a notable upsurge in diabetes cases, with a prevalence rate of 30% among the KSA population.3 This condition not only adversely impacts overall health and quality of life, but also escalates the risk of mortality.1,2,6
Patient satisfaction constitutes a vital component of delivering high-quality healthcare. In the case of DM patients, who often express dissatisfaction with the need for lifelong regular check-ups, satisfaction is influenced by patient interactions, case management, and follow-up care.7 Studies indicate a strong correlation between satisfied DM patients and favorable treatment outcomes.8–10 Various factors, including patient demographics, education, clinical aspects, treatment elements, adherence concerns, and service-related factors, impact satisfaction levels and the delivery of patient-centered care. Additionally, incorporating clear communication, interpersonal manners and comfort during encounters, and accessibility has been shown to influence how patients experience treatment.6,7,11
The World Health Organization’s (WHO) assessment places KSA as the country with the second-highest DM prevalence in the Middle East and the seventh globally. The estimated population affected comprises 7 million individuals living with DM and over 3 million with pre-diabetes.12
Monitoring satisfaction in patients with diabetes is crucial for evaluating effectiveness of diabetes therapeutic interventions. This protocol used the Diabetes Treatment Satisfaction Questionnaire status version (DTSQs), which specifically assesses patients’ satisfaction with diabetes treatment.13,14
The healthcare system in KSA comprises government-sponsored free services and commercial healthcare options. The choice of treatment setting for DM patients influences overall satisfaction with care received.8 Additionally, glycated hemoglobin (HbA1c) levels play a critical role in DM management and in evaluating DM care success. However, the relationship between HbA1c management and patient satisfaction requires further exploration.9 The study hypothesizes that treatment satisfaction will be higher in governmental healthcare, specialized diabetes centers, and that better glycemic control (HbA1c < 8%) will be associated with greater treatment satisfaction.
Despite the progress in researching the factors that affect the satisfaction of patients with diabetes, few studies have examined the influence of healthcare setting (governmental or private), healthcare type (primary or specialized diabetes center), and glycemic control on DM patient satisfaction in Saudi Arabia. This cross-sectional study aims to explore the factors influencing patient satisfaction with DM treatment among Saudi Arabian patients. Specifically, we aim to investigate the association between HbA1c management and treatment satisfaction. We also examine whether choosing specialty diabetes care centers over primary care clinics or government-sponsored healthcare services over private providers affects patient satisfaction. Our research seeks to offer valuable insights into the determinants of patient satisfaction within Saudi Arabia’s healthcare landscape.
By comprehensively examining these factors, our study can assist healthcare professionals, policymakers, and physicians in enhancing the quality of DM care, thereby improving healthcare outcomes and the well-being of individuals with DM in KSA.
Materials and Methods
Study Design and Questionnaire
A cross-sectional approach with a convenience sampling technique was employed in this research to explore factors influencing patient satisfaction regarding DM care in 13 regions throughout KSA from April 2023 to February 2024. This was a cross-sectional survey using DTSQs. Specifically designed and validated to measure treatment satisfaction in people with diabetes, the DTSQs comprises eight items, allowing respondents to evaluate their satisfaction with various aspects of their DM treatment using Likert scale scoring (0–6) for each item.13–15 Six items (1, 4, 5, 6, 7, 8) measure treatment satisfaction (satisfaction with current treatment, convenience, flexibility, satisfaction with own understanding of diabetes, likelihood of recommending the treatment to others and satisfaction to continue with the treatment), and the sum of these items is taken to generate a DTSQ scale score. The remaining two items (2,3) measure perceived frequency of hyperglycemia and frequency of hypoglycemia. The six DTSQs scale items are scored on seven-point response scales ranging from, for example, “very satisfied” (scored 6) to “very dissatisfied” (scored 0). Higher DTSQs scores indicate greater satisfaction with treatment (range 36 to 0). With respect to the two items measuring perceived frequency of hyperglycemia and hypoglycemia, the items are scored on seven-point response scales ranging from “most of the time” (scored 6) to “none of the time” (scored 0). In this case, the lower DTSQs scores indicate more ideal blood glucose levels. For access to the DTSQ linguistically validated in Arabic for Saudi Arabia and in more than 120 other languages, visit www.healthpsychologyresearch.com.
Study Participants
Adult patients aged ≥ 18 with either type 1 or type 2 diabetes mellitus were included, and we excluded patients who did not consent to participate in the study.
After ethical approval, a nationwide master list of individuals with type 1 or type 2 diabetes mellitus was obtained from the MOH which included 4795 patients, of which 709 patients consented and filled out the survey with a survey response rate of 14.79%. Volunteers were from diverse healthcare facilities, encompassing government-run clinics, private hospitals, specialized diabetes centers, and primary care clinics. This selection aimed to ensure the comprehensive representation of individuals receiving DM treatment across various healthcare settings. By including participants from different healthcare contexts, the study aimed to provide a holistic understanding of patient satisfaction with diabetes treatment and its influencing factors, considering the distinct dynamics of government and private healthcare services in KSA.
Data Collection
The online survey was prepared using the survey tool Google Forms. It encompassed an extensive array of demographic characteristics besides capturing information regarding treatment satisfaction. Variables included age, gender, educational level, marital status, employment status, income level, DM type (Type 1 or Type 2), duration of DM diagnosis, and the number of DM medications prescribed. The collection of these broad demographic data was crucial to understand the intricate factors influencing patient satisfaction with DM treatment across diverse healthcare settings in KSA. All survey fields were mandatory, and due to the convenience sampling approach, no follow-up for missing responses was conducted.
Study Outcome
The outcome of interest was to study the key factors associated with patient satisfaction with DM treatment, which include: healthcare settings (government vs private), healthcare types (specialized diabetes centers vs primary care), and glycemic control (< 8% vs ≥ 8%). Moreover, the association of various treatment sectors and Diabetes Care with glycemic control was also evaluated. The study hypothesizes that treatment satisfaction varies by healthcare sector, with expected higher satisfaction in governmental hospitals and diabetes centers where diabetes care is provided free of charge. Additionally, better glycemic control (HbA1c < 8%) is expected to correlate with higher satisfaction. Demographic factors are also explored as potential influences on satisfaction.
Data Analysis
The Statistical Package for Social Sciences (SPSS version 26.0) was used for data analysis. Descriptive statistics, including means and standard deviations, were computed to outline the characteristics of the research population. Associations between categorical factors like gender, method of healthcare delivery, and HbA1c control were analyzed using chi-square tests. Additionally, comparisons of means between different groups were conducted using the Mann–Whitney U-test. Univariate logistic regression analysis was used to investigate the association between treatment sector or diabetes care and HbA1C. Further, the model was adjusted for the basic characteristics of the study participants, including age, sex, marital status, education, employment status, income, and residence. These analytical methods helped understand the associations and differences within the study’s variables.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Regional Research Ethics Committee at the Ministry of Health, Saudi Arabia, with protocol number (6-7-43-6007). Before involving any participants, we obtained informed consent from each individual. This approach ensured participants fully understood the study’s objectives and methodologies. We emphasized the importance of protecting their privacy and maintaining confidentiality throughout the research process. These ethical measures were implemented to comply with established ethical standards and guidelines, prioritizing values such as respect, beneficence, and fairness in human research.
Statistical Significance
Throughout this investigation, a consistent alpha level of p < 0.05 was employed to assess the statistical significance. This predetermined significance level was applied uniformly to all statistical tests and analyses conducted within the study. Adhering to this criterion enabled us to derive dependable conclusions from the data, allowing for the identification of meaningful relationships and distinctions. By maintaining this standard, our findings were rigorously assessed in line with established statistical norms, ensuring the reliability of our results.
Results
Characteristics of Study Participants
The survey was sent to 3200 patients with DM, of whom 709 participants consented to participate in the study. An overview of the demographic characteristics of the study participants, categorized by the type of healthcare facility at which they receive treatment, whether it is a governmental or a private sector facility, diabetes care or primary care, and their corresponding HbA1C level is provided in (Table 1). It encompasses marital status, gender, age, place of residence, education, employment status, income level, type of DM (Type 1 or Type 2), duration of diabetes, and the number of medications in their regimen.
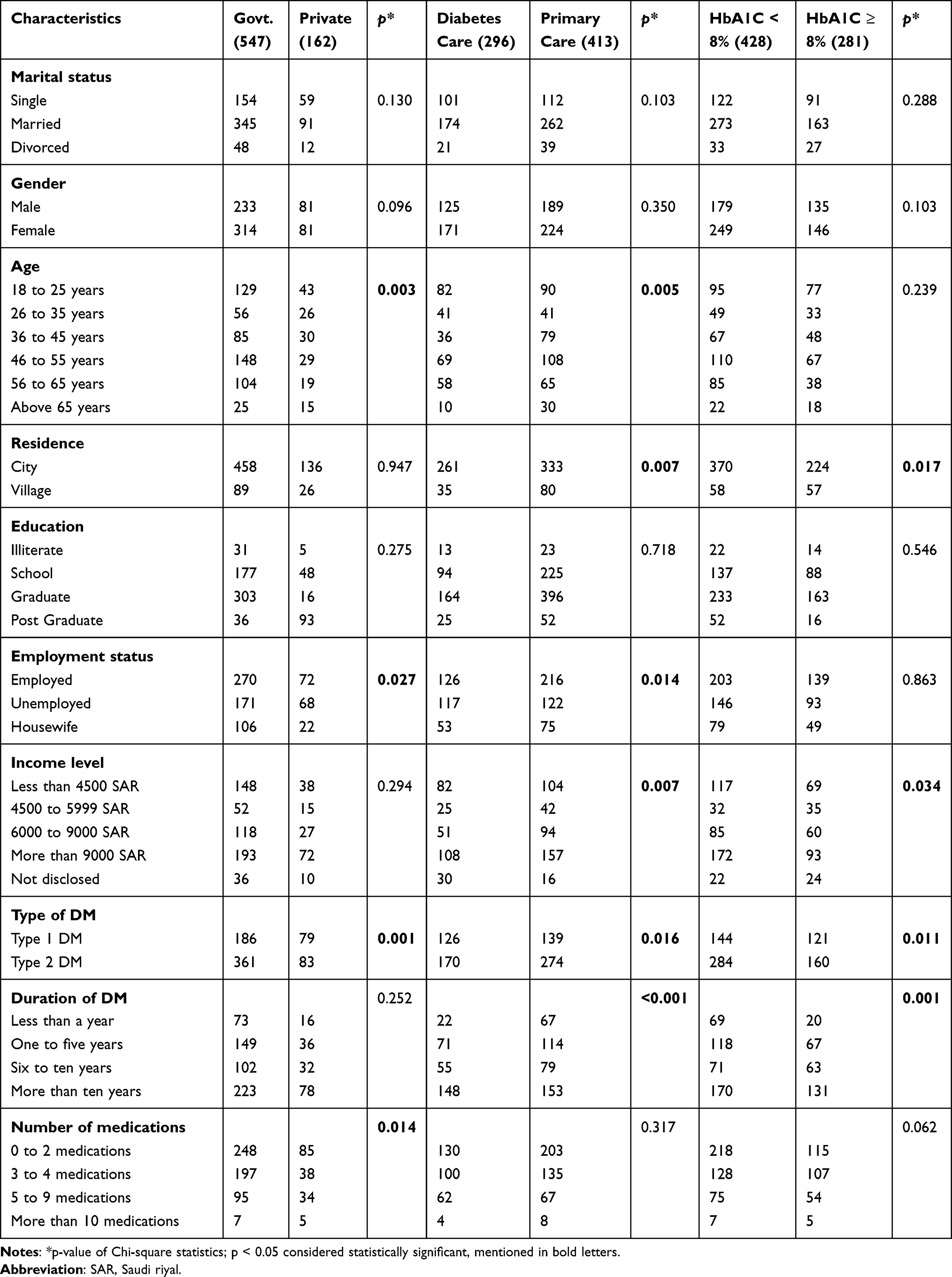 |
Table 1 Characteristics of the Study Participants and DTSQs Score Among the Study Participants |
Marital status among patients did not significantly differ between the government and private sectors, diabetes and primary care centers, and HbA1C level (p = 0.130, p = 0.103, and p =0.288, respectively). Similarly, gender representation was not significantly different between those groups (p = 0.096, p = 0.350, and p = 0.103, respectively).
Regarding age demographics, a significant difference was found between the healthcare sectors, with varying age distributions between the government and private sectors (p = 0.003). Similarly, there was a significant difference in age across the types of centers (p = 0.005)., but there was no significant association between age and HbA1c level (p = 0.239).
Moreover, the distribution of diabetic patients between city and village residences did not exhibit significant variation concerning healthcare sector distribution (p = 0.947). However, its association with the type of care and the level of HbA1c was found to be statistically significant (p = 0.007 and p = 0.017, respectively).
While no significant difference was found between education level and sector distribution, care type, and HbA1c level (p = 0.275, p = 0.718, and p = 0.546), significant differences were observed between employment status and types of sectors and centers (p = 0.027 and p = 0.014, respectively).
Income level had no significant correlation with the type of sector (p = 0.294), but a significant difference was found regarding the center type and the level of HbA1c (p = 0.007 and p = 0.034, respectively). Moreover, the type of diabetes was significantly different between sector type, center type, and level of HbA1C (p = 0.001, p = 0.016, and p = 0.011 respectively).
The duration of diabetes did not show a significant difference between the sectors, in contrast to the significant difference with center types and HbA1c level (p = 0.252, p = <0.001, and p = 0.001, respectively). Furthermore, a significant difference was noted between the number of prescribed medications and the healthcare sector (p = 0.014), while its relation to the type of healthcare center and the level of HbA1c was not significant (p = 0.317 and p = 0.062, respectively).
Diabetes Treatment Satisfaction: Healthcare Settings Association
We analyzed patients’ replies to the DTSQs using a Mann–Whitney U-test to assess the impact of healthcare environments on their satisfaction with diabetes treatment (Table 2). Patients receiving care in government healthcare settings had a statistically significant higher mean (SD) satisfaction score compared to those in private healthcare settings in four items that include satisfaction with current treatment (p = 0.032), convenience of treatment for current condition (p = 0.002), flexibility of recent treatment (p = 0.004), and satisfaction to continue current treatment (p = 0.013). However, the mean (SD) perceived frequency of hyperglycemia/hypoglycemia did not differ significantly between the government and private sectors. Moreover, the mean (SD) score of satisfaction was not statistically different (p = 0.468) regarding understanding of diabetes between government and private clinical settings. Although the mean (SD) score of the recommendation of government services was higher than that of private services, this difference was not statistically significant (p = 0.223) as shown in (Table 2).
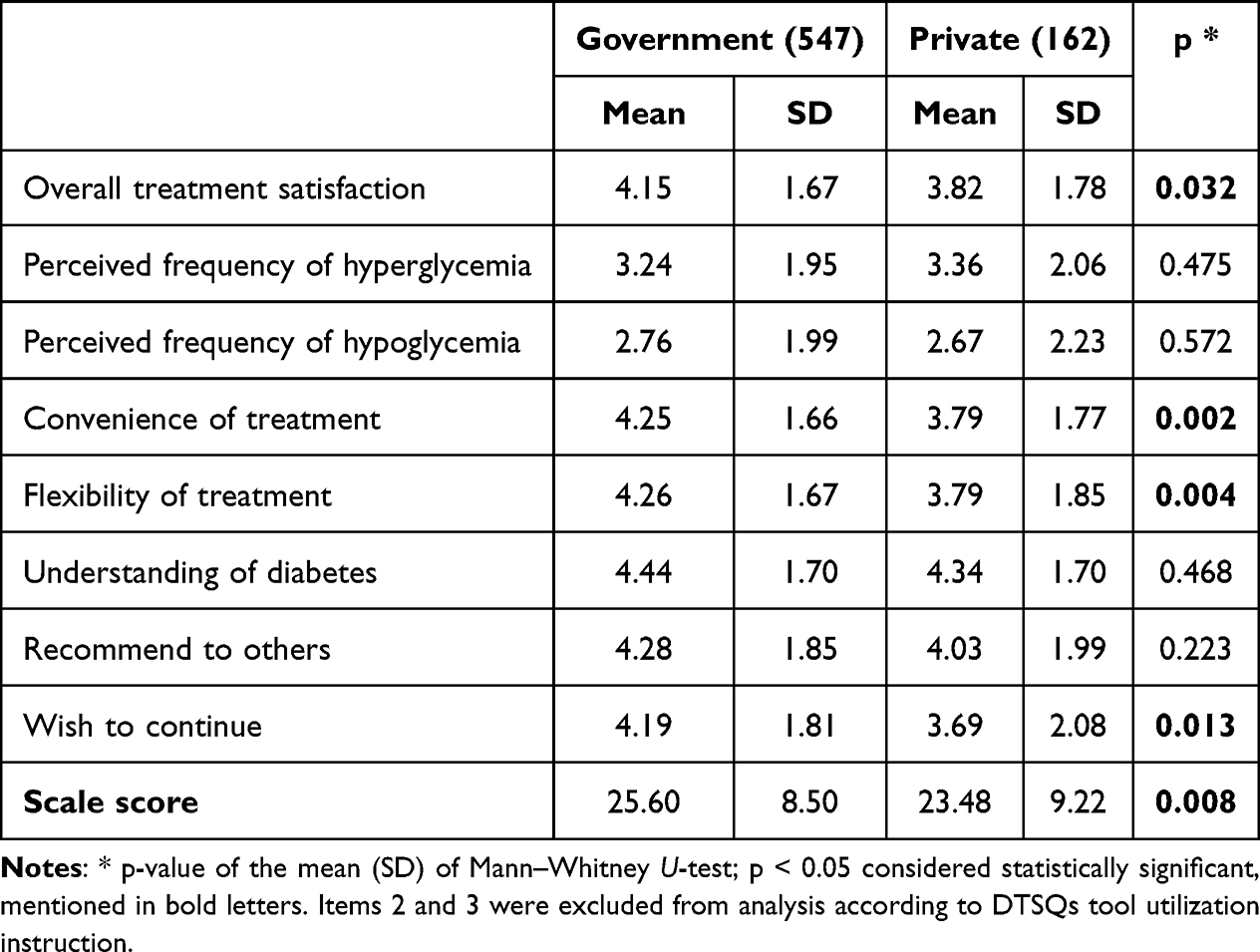 |
Table 2 Diabetes Treatment Satisfaction Questionnaire (DTSQs) Score Among Patients in Government and Private Healthcare |
Diabetes Treatment Satisfaction: Healthcare Type Association
By contrasting patients in specialized diabetes centers and primary care settings, we looked more closely at the effects of different healthcare delivery models on treatment satisfaction (Table 3). The mean (SD) satisfaction scale score was significantly higher in specialized DM centers (p<0.001). Four of the items differed significantly including current treatment satisfaction (p < 0.001), convenience of treatment (p = 0.001), flexibility of treatment (p < 0.001), and wish to continue with current treatment (p < 0.001). However, the mean (SD) score of the patient’s responses regarding unacceptably low blood sugar levels was significantly higher in the specialized DM centers than in primary care (p < 0.001). Meanwhile, the mean (SD) score of patients’ responses regarding unacceptably high blood sugar levels has no statistically significant difference (p = 0.133). The mean score for understanding of diabetes and recommending the treatment to others was significantly higher from patients attending the specialized DM centers than from primary care patients (p < 0.001) as shown in (Table 3).
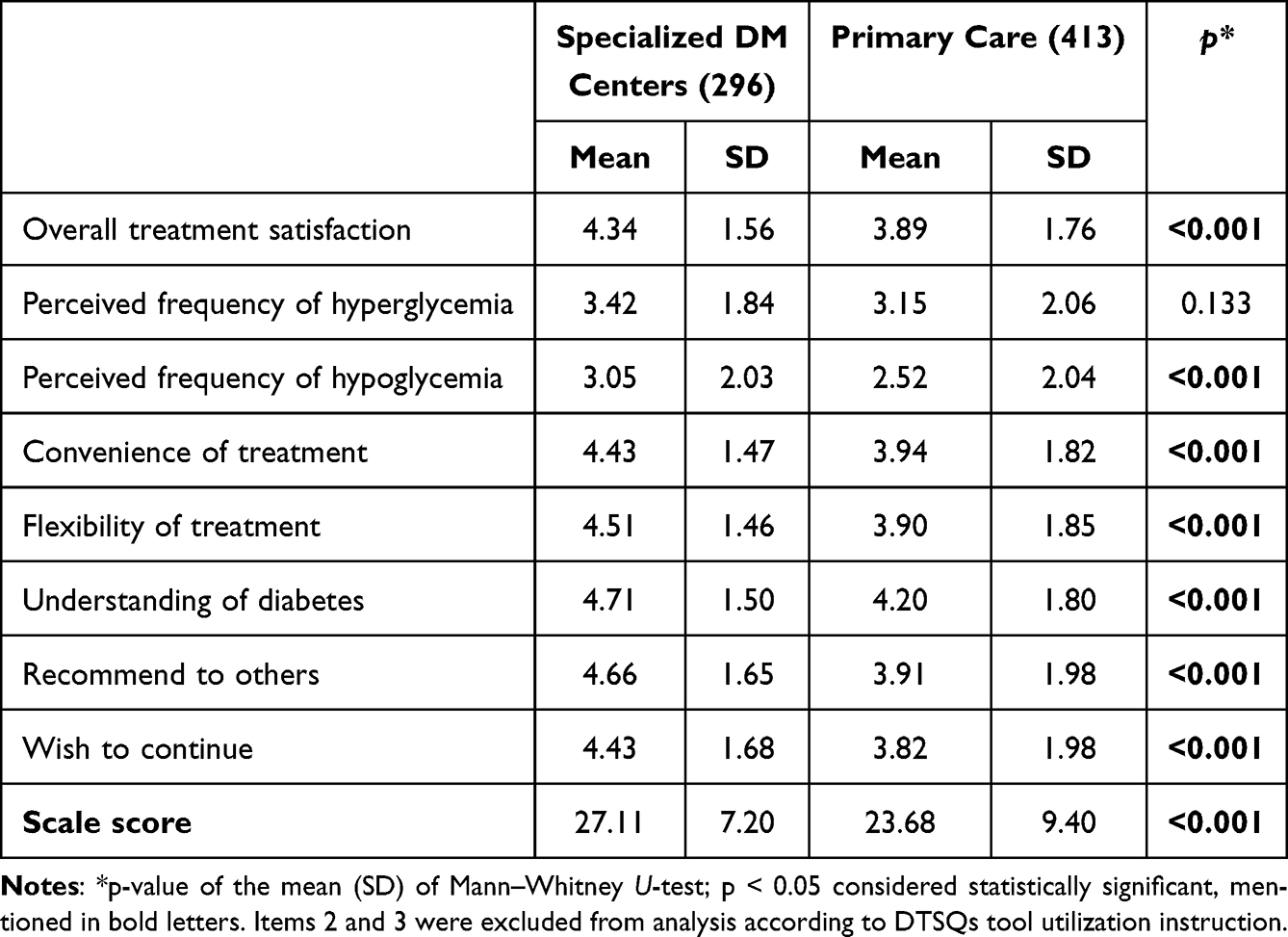 |
Table 3 Diabetes Treatment Satisfaction Questionnaire (DTSQs) Score Among Patients in Specialized Diabetes Centers and Primary Care |
Diabetes Treatment Satisfaction: Glycemic Control Association
We compared patients with controlled (HbA1C< 8%) and uncontrolled (HbA1C≥ 8%) diabetes in order to investigate the link between glycemic control and treatment satisfaction (Table 4). Patients with controlled diabetes were significantly more satisfied with their current treatment in comparison to patients with uncontrolled diabetes (p < 0.001). Perceived frequency of hyper- and hypoglycemia was significantly greater (p < 0.001) in those with less well-controlled diabetes. The patients with controlled diabetes reported significantly higher satisfaction regarding understanding of diabetes (p = 0.013) and were more likely to recommend their treatment to others (p < 0.001) as illustrated in (Table 4).
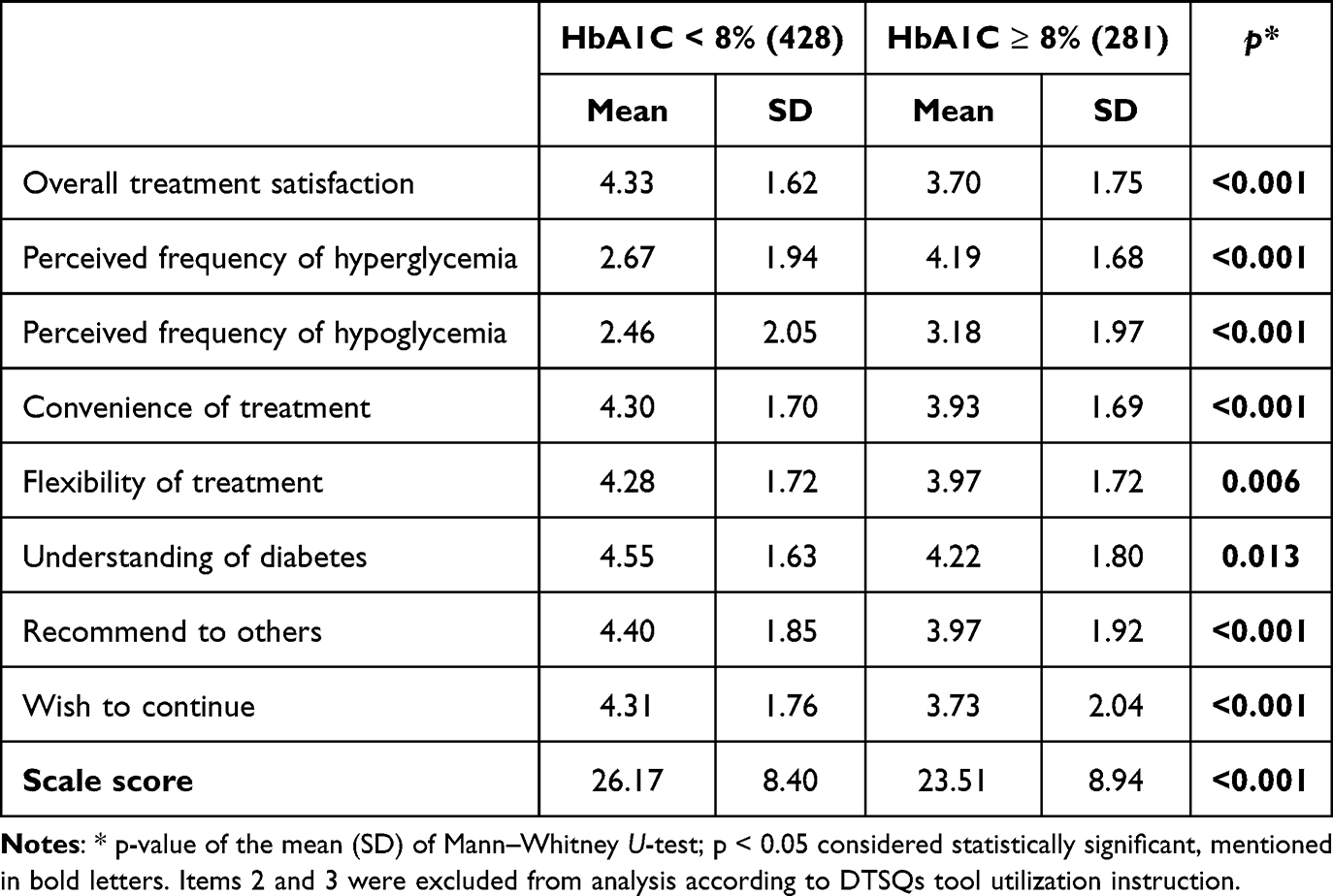 |
Table 4 Diabetes Treatment Satisfaction Questionnaire (DTSQs) Score Among Patients with Better Controlled (HbA1c <8%) and Less Well-Controlled (HbA1c>/=8%) Diabetes |
Treatment Sectors and Diabetes Care: Glycemic Control Association
The association between healthcare sector types (governmental vs private) and healthcare setting types (diabetes center vs primary healthcare) with the glycemic control levels (<8 vs ≥ 8) was explored in (Table 5). Both unadjusted ratio (uOR) and adjusted odds ratio (aOR) were calculated to compare the likelihood of achieving HbA1C < 8 across these factors. In terms of treatment sectors, there was no difference between sector types in achieving control of HbA1C (uOR = 0.898, p = 0.558) and adjusted odds ratios (aOR = 0.888, p = 0.520). Similarly, no significant difference was noted between diabetes centers and primary healthcare centers in terms of glycemic control, although patients in primary healthcare centers had slightly higher odds of HbA1C ≥ 8 compared to patients in diabetes centers, in both unadjusted (uOR = 1.318, p = 0.078) and adjusted odds ratios (aOR = 1.322, p = 0.075). This result indicates that there were no confounding variables, as the basic characteristics of study participants (age, sex, marital status, education, employment status, income, and residence) did not influence HbA1C in either the treatment sector or diabetes care.
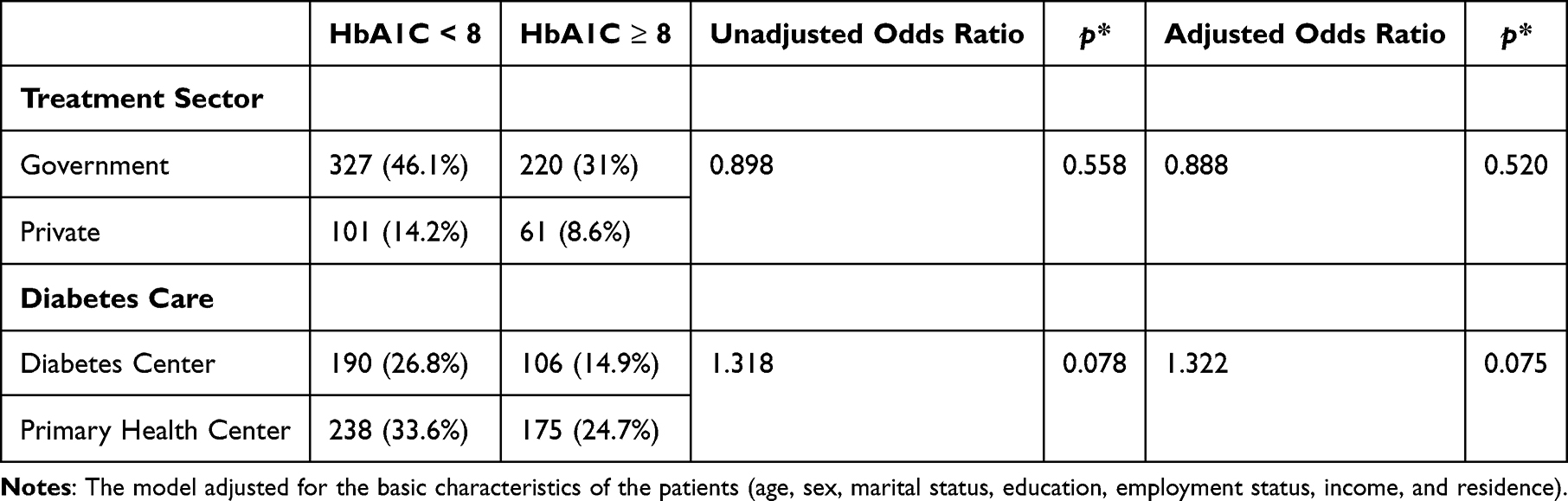 |
Table 5 Association of Various Treatment Sectors and Diabetes Care with Glycemic Control |
Discussion
This cross-sectional survey highlights the satisfaction level of patients with diabetes mellitus in in Saudi Arabia. In the glycemic control domain, the present study findings reflects previous findings regarding the association of treatment satisfaction and glycemic control.16–18
This study did not investigate any barriers related to dissatisfaction that need to be identified in future investigations. Our findings also highlight the significant hypoglycemic risk among the uncontrolled patients with diabetes mellitus (HbA1C ≥ 8%). This might be due to reasons including lower treatment satisfaction of patients or poor control of blood sugar, as already reported in previous studies.19,20 Also, our study agrees with the previous findings that poor understanding of diabetes mellitus treatment is often associated with lower glycemic control. Hence, patient education regarding diabetes mellitus, among many other factors, can enhance glycemic control.21
The mean (SD) patient’s treatment satisfaction score with the specialized diabetic centers was significantly higher, coinciding with the previous findings from Saudi Arabia related to consultations, information about the disease, and medications.6 A multidisciplinary approach in specialized DM centers in Saudi Arabia often leads to higher satisfaction since it provides optimal glycemic control and protection from complications of diabetes mellitus.22 Also, the quality of diabetes care, services, and health educational resources strongly influences patient satisfaction.23 As of now, only specialized diabetes centers can fulfil these factors, and primary care centers have yet to do so. Therefore, the Ministry of Health must also pay more attention to ensuring the above-mentioned care in primary health centers.
The patients treated in the government sector had significantly higher mean (SD) satisfaction than those in the private sector regarding their current treatment. Government hospitals in managing diabetes mellitus in Saudi Arabia offer patient-focused care, an integrated care plan by a multidisciplinary health team, active surveillance, and education, which could be the potential factors for higher patient satisfaction.24 Communication between healthcare practitioners and patients, the technical skills of healthcare providers, the doctor’s availability, and the patient’s accessibility to healthcare services were addressed as potential domains for higher patient satisfaction in previous studies from Saudi Arabia.25–27 The mean (SD) score of patient satisfaction related to unacceptable hyper- or hypoglycemia was not significantly different between the government and private healthcare sectors. This needs further investigation to address the other potential barriers for avoiding hyper- or hypoglycemia, including medication adherence, knowledge of healthcare practitioners, and patient refusal of treatment in the government sector, even though medications are free of charge, and their satisfaction with the treatment.28
Recommendations and Future Directions
The results of this study have several consequences for Saudi Arabian scholars, politicians, and healthcare professionals for enhancing patient satisfaction with diabetes treatment in Saudi Arabia:
Enhancing Healthcare Settings
In order to ensure better quality and accessibility of diabetes care, invest in improving infrastructure, education, and adopting patient-centered care.
Expanding Specialized Care
Considering the higher satisfaction levels observed in specialized care, we recommend extending access to specialized diabetes centers and educational programs for better diabetes management.
Personalizing Treatment Approaches
Based on the findings of this protocol, we also recommend tailoring treatment plans according to individual patient needs, considering factors such as age, income levels, and complexity of medication regimens. In line with this approach, a study by Othman et al found a statistically significant relationship between satisfaction and factors such as age, sex, nationality, education, marital status, occupation, duration of diabetes, treatment regimen, and complications.
Continued Research
Further studies are needed to explore other influential factors on treatment satisfaction, such as cultural elements, psychosocial elements, other comorbidities, complications, and different treatment methods. Evaluating the long-term impact of patient satisfaction on diabetes management and overall outcomes to gain a more comprehensive understanding.
These recommendations aim to address the specific areas identified in the study that could significantly impact patient satisfaction with DM treatment in Saudi Arabia. They provide a framework for healthcare professionals, policymakers, and scholars to enhance diabetes care and ultimately improve patient outcomes.
Limitations
While this study provides valuable insights into the factors associated with patient satisfaction with diabetes treatment in KSA, it is important to acknowledge its limitations. The cross-sectional design restricts our ability to establish causal relationships between variables, and the use of convenience sampling may introduce selection bias. Furthermore, reliance on self-reported data from the online survey and the DTSQS self-assessment may also contribute to self-reporting bias.
Future studies could consider longitudinal research methods and qualitative investigations to gain a more comprehensive understanding of patients’ experiences and contentment with diabetes treatment in KSA. Longitudinal studies could track changes over time, offering a clearer view of causal relationships, while qualitative inquiries could delve deeper into patients’ lived experiences and perceptions.
Understanding the diverse variables associated with patient treatment satisfaction is vital for enhancing diabetes care and achieving better patient outcomes. This study has highlighted significant associations between treatment satisfaction among diabetes patients in KSA related to healthcare settings, glycemic control, age, income, and medication complexity.
Healthcare professionals and policymakers can work collaboratively to implement the above recommendations derived from this study. Additionally, investing in further research endeavors will continue to refine our understanding and aid in improving diabetes care and patient satisfaction in the region.
Conclusions
The mode of healthcare delivery (public or private hospitals) and the choice between primary care and diabetes centers exhibited a significant association with patient treatment satisfaction, which was higher in governmental healthcare and specialized diabetes centers. Our thorough analysis of the variables affecting DM treatment satisfaction in KSA has uncovered crucial findings that are extremely important for healthcare providers and policymakers. Our study provides helpful recommendations for enhancing the standard of diabetes care by diving into the subtleties of patient opinions.
Factors Impacting DM Treatment Satisfaction
Our study has shed light on a number of variables that have an association with the satisfaction of patients with their DM treatment. Notably, we discovered that healthcare delivery, governmental or private hospitals, and the choice between primary care clinics and specialized diabetes centers are associated with higher satisfaction observed in governmental healthcare and specialized diabetes centers. However, glycemic control was not significantly associated with patient satisfaction. This highlights the critical role of personalized and patient-centric diabetes care. Healthcare providers should consider socioeconomic factors and the complexity of medication regimens when devising treatment plans. Moreover, adapting treatment protocols to better suit patient preferences may positively impact satisfaction levels among patients.8,29–31
Implications for Healthcare Delivery
Our findings have broad ramifications, emphasizing the necessity for specialized interventions and tactics to deal with the numerous difficulties DM patients confront. The job of healthcare professionals includes thorough patient education, support, and individualized care plans in addition to prescribing medications. To ensure patient-centric care, it is important to consider the diverse needs that may exist across patient demographics such as age, healthcare setting, and socioeconomic status while continuing to recognize and respond to each patient as an individual. Specialized care models, such as diabetes centers, have demonstrated improved patient satisfaction, underscoring the importance of specialized care. Furthermore, by ensuring flexibility in management plans and maintaining a focus on individualized variations of each patient’s care, patients with diabetes can have an improved long-term health outcome and quality of life. Future research might further explore additional factors influencing treatment satisfaction and evaluate long-term outcomes to strengthen diabetes care.
Institutional Review Board Statement
The study received ethical approval from the Regional Research Ethics Committee at the Ministry of Health, Saudi Arabia, protocol number (6-7-43-6007).
Data Sharing Statement
To promote openness and future investigation of this topic, the authors will make the data underlying the conclusions of this article available without unnecessary delay, and it can be obtained from the corresponding author. We also confirm that the data, in whole or in part, have not been published elsewhere.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Participants provided written consent for the use and publication of their anonymized data.
Acknowledgments
Our deepest thanks go to Professor Clare Bradley for the invaluable contributions to diabetes mellitus care, and for creating the DTSQs, licensed by Health Psychology Research Ltd. (HPR). We are grateful for the support of HPR, enabling our work through license reference CB1290, which helps improve the lives of people with diabetes mellitus, globally.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10:14790. doi:10.1038/s41598-020-71908-9
2. Ong KL, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–12. doi:10.1016/S0140-6736(23)01301-6
3. Tokalı P, Demir Y, Çakır F, Şenol H, Tokalı FS. Design, synthesis, and aldose reductase inhibition assessment of novel Quinazolin-4 (3H)-one derivatives with 4-Bromo-2-Fluorobenzene functionality. Bioorg Chem. 2025;108614.
4. Tokalı FS, Demir Y, Tokalı P, Ateşoğlu Ş, Şenol H. New Quinazolin‐4 (3H)‐One–Thiazolidine‐2, 4‐dione hybrids as dual inhibitors of α‐glycosidase and aldose reductase: the synthetic, in vitro, and in silico approaches. J Biochem Mol Toxicol. 2025;39(8):e70412. doi:10.1002/jbt.70412
5. Tokalı FS, Demir Y, Ateşoğlu Ş, Tokalı P, Şenol H. Development of phenolic Mannich bases as α-glucosidase and aldose reductase inhibitors: in vitro and in silico approaches for managing diabetes mellitus and its complications. Bioorg Med Chem. 2025;118264.
6. Al Anazi KS, Mohamed AE, Hammad SM. Services satisfaction of type 2 diabetic patients attending Arar’s diabetic center, Saudi Arabia. Saudi Med J. 2019;40:183–188. doi:10.15537/smj.2019.2.23677
7. Al Hayek AA, Robert AA, Al Saeed A, Alzaid AA, Al Sabaan FS. Factors associated with health-related quality of life among Saudi patients with type 2 diabetes mellitus: a cross-sectional survey. Diabetes Metab J. 2014;38:220–229. doi:10.4093/dmj.2014.38.3.220
8. Alqarni AM, Alrahbeni T, Qarni AA, Qarni HMA. Adherence to diabetes medication among diabetic patients in the Bisha governorate of Saudi Arabia - a cross-sectional survey. Patient Prefer Adherence. 2019;13:63–71. doi:10.2147/PPA.S176355
9. Al Shahrani A, Baraja M. Patient satisfaction and it’s relation to diabetic control in a primary care setting. J Fam Med Primary Care. 2014;3(1):5–11. doi:10.4103/2249-4863.130254
10. Best JH, Boye KS, Rubin RR, Cao D, Kim TH, Peyrot M. Improved treatment satisfaction and weight-related quality of life with exenatide once weekly or twice daily. Diabet Med. 2009;26:722–728. doi:10.1111/j.1464-5491.2009.02752.x
11. Elias A, Abdalkarim S, Mohammed MW, et al. Patient satisfaction and its predictors in the general hospitals of Southwest Saudi Arabia: a cross-sectional survey. Sudan JMS. 2022;17:15–27. doi:10.18502/sjms.v17i1.10682
12. Robert AA, Al Dawish MA, Braham R, Musallam MA, Al Hayek AA, Al Kahtany NH. Type 2 diabetes mellitus in Saudi Arabia: major challenges and possible solutions. Curr Diabetes Rev. 2017;13:59–64. doi:10.2174/1573399812666160126142605
13. Bradley C. Diabetes treatment satisfaction questionnaire (DTSQ). In: Handbook of Psychology and Diabetes. Routledge; 2013:111–132.
14. Bradley C, Lewis KS. Measures of psychological well‐being and treatment satisfaction developed from the responses of people with tablet‐treated diabetes. Diabetic Med. 1990;7(5):445–451. doi:10.1111/j.1464-5491.1990.tb01421.x
15. Saisho Y. Use of diabetes treatment satisfaction questionnaire in diabetes care: importance of patient-reported outcomes. Int J Environ Res Public Health. 2018;15:947. doi:10.3390/ijerph15050947
16. Sayed Ahmed HA, Abdelsalam NE, Joudeh AI, Abdelrahman AG, Eldahshan NA. Association of treatment satisfaction and physician trust with glycemic control among primary care patients with type 2 diabetes in Egypt. Diabetol Int. 2023;15(1):67–75. doi:10.1007/s13340-023-00653-x
17. AlSlail FY, Akil YA. Treatment patterns, effectiveness, and satisfaction among patients with type 2 diabetes treated with insulin in Saudi Arabia: results of the RIMODIS study. Diabetes Ther. 2021;12(7):1965–1978. doi:10.1007/s13300-021-01089-9
18. Khdour M, Awadallah HB, Al-Hamed DH. Assessment of treatment satisfaction and adherence amongst diabetic patients in governmental primary care clinic of Ramallah, West-Bank. Hosp Pract. 2021;49(1):27–33. doi:10.1080/21548331.2020.1822083
19. Hakimi H, Afsaneh Abadi P, Momeni M. Association between fear of hypoglycemia and treatment satisfaction among patients with diabetes mellitus. JCCNC. 2024;10(1):35–44. doi:10.32598/JCCNC.10.1.452.1
20. Alvarez Guisasola F, Tofé Povedano S, Krishnarajah G, Lyu R, Mavros P, Yin D. Hypoglycaemic symptoms, treatment satisfaction, adherence and their associations with glycaemic goal in patients with type 2 diabetes mellitus: findings from the real-life effectiveness and care patterns of diabetes management (RECAP-DM) study. Diabetes Obes Metab. 2008;10(Suppl 1):25–32. doi:10.1111/j.1463-1326.2008.00882.x
21. Ruszkiewicz K, Jagielski P, Traczyk I. Glycemic control and awareness among diabetic patients of nutrition recommendations in diabetes. Rocz Panstw Zakl Hig. 2020;71(2):191–196. doi:10.32394/rpzh.2020.0116
22. Aldahash R, Aldossari K, Aljohanni N, et al. Type 2 diabetes mellitus in Saudi Arabia: prevalence, risk factors, and management strategies: a review. Endocr Metab Immune Disord Drug Targets. 2025;25. doi:10.2174/0118715303361062250122100238
23. Itumalla R, Kumar R, Perera B, Elabbasy MT, Cg SK, Kundur R. Patient’s perception of diabetes care services in Hail, Kingdom of Saudi Arabia. Health Psychol Res. 2022;10(3):38119. doi:10.52965/001c.38119
24. Alotaibi YK, Al-Nowaiser N, Al Harbi TJ, Tourkmani AM, Moharram M. Improving type 2 diabetes mellitus management in Ministry of Defense Hospitals in the Kingdom of Saudi Arabia 2018-2021. BMJ Open Qual. 2023;12(2):e002037. doi:10.1136/bmjoq-2022-002037
25. Bokhary DH, Saggaf OM, Baabdullah AM, et al. Assessment of patient experiences in an academic hospital in Saudi Arabia. Cureus. 2022;14:e24203. doi:10.7759/cureus.24203
26. AlHarethy S, Al-Angari SS, Syouri F, et al. Assessment of satisfaction based on age and gender in functional and aesthetic Rhinoplasty. Eur Arch Otorhinolaryngol. 2017;274:2809–2812. doi:10.1007/s00405-017-4566-z
27. Mahrous MS, Hifnawy T. Patient satisfaction from dental services provided by the college of dentistry, Taibah University, Saudi Arabia. J Taibah University Med Sci. 2012;7:104–109. doi:10.1016/j.jtumed.2012.12.002
28. Alhagawy AJ, Yafei S, Hummadi A, et al. Barriers and attitudes of primary healthcare physicians to insulin initiation and intensification in Saudi Arabia. Int J Environ Res Public Health. 2022;19(24):16794. doi:10.3390/ijerph192416794
29. Wu P, Liu N. Association between patients’ beliefs and oral antidiabetic medication adherence in a Chinese type 2 diabetic population. Patient Prefer Adherence. 2016;10:1161–1167. doi:10.2147/PPA.S105600
30. Speight J, Reaney MD, Barnard KD. Not all roads lead to Rome-a review of quality of life measurement in adults with diabetes. Diabet Med. 2009;26:315–327. doi:10.1111/j.1464-5491.2009.02682.x
31. Pourhabibi N, Mohebbi B, Sadeghi R, et al. Factors associated with treatment adherence to treatment among in patients with type 2 diabetes in Iran: a cross-sectional study. Front Public Health. 2022;10:976888. doi:10.3389/fpubh.2022.976888
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.