Back to Journals » Patient Preference and Adherence » Volume 20
Factors Associated with Non-Adherence to Blood Glucose Testing Among Non-Hispanic Black and Hispanic Men with a History of Prediabetes in the United States
Authors Bose A, Prochnow T, Bergeron CD, Park JH ![]() , Johannes BL
, Johannes BL ![]() , Sherman LD, Patterson MS, Merianos AL
, Sherman LD, Patterson MS, Merianos AL ![]() , Smith ML
, Smith ML ![]()
Received 15 December 2025
Accepted for publication 21 May 2026
Published 17 June 2026 Volume 2026:20 589075
DOI https://doi.org/10.2147/PPA.S589075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Aaheli Bose,1 Tyler Prochnow,1– 3 Caroline D Bergeron,4 Jeong-Hui Park,5 Bobbie L Johannes,6 Ledric D Sherman,1,2 Megan S Patterson,1 Ashley L Merianos,7 Matthew Lee Smith8,9
1Department of Health Behavior, School of Public Health, Texas A&M University, College Station, TX, USA; 2Center for Health Equity and Evaluation Research, Texas A&M University, College Station, TX, USA; 3Center for Community Health and Aging, Texas A&M University, College Station, TX, USA; 4LIFE Research Institute, University of Ottawa, Ottawa, Ontario, Canada; 5Department of Health Disparities Research, Division of Cancer Prevention and Population Science, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 6Department of Population Health Sciences, Geisinger, Danville, PA, USA; 7College of Education, Criminal Justice, and Human Services, University of Cincinnati, Cincinnati, OH, USA; 8Department of Applied Health Science, School of Public Health, Indiana University, Bloomington, IN, USA; 9Center for Health by Design, School of Public Health, Indiana University, Bloomington, IN, USA
Correspondence: Matthew Lee Smith, Department of Applied Health Science, School of Public Health, Indiana University, 1025 E 7th Street, Room 116, Bloomington, IN, 47405, USA, Tel +1-812-855-4041, Email [email protected]
Introduction: Rates of prediabetes are rising in the United States, especially within communities of color. Without adopting self-care behaviors and adhering to routine screenings, prediabetes is likely to progress to type 2 diabetes. This study examines factors associated with non-adherence to recommended blood glucose testing among non-Hispanic Black and Hispanic men ages ≥ 40 years with a history of prediabetes.
Methods: Using an internet-delivered survey, data were collected from 769 Black (56.7%) and Hispanic (43.3%) men with a history of prediabetes. Chi-square tests and independent sample-tests were to identify differences across study variables by race/ethnicity and blood glucose testing adherence. A logistic regression model with backward stepwise entry was fitted to assess factors associated with blood glucose testing non-adherence, adjusted for sociodemographic factors, co-morbidities, healthcare interactions, social support, and lifestyle behaviors.
Results: Approximately 11% of participants did not receive a blood glucose test in the past 12 months, and 60.9% self-reported progression from prediabetes to diabetes. Men who self-reported progressing from prediabetes to diabetes were less likely to be non-adherent to blood glucose testing recommendations (Odds Ratio [OR]=0.51, P=0.006). Each additional year of age was associated with lower odds of being non-adherent to blood glucose testing (OR=0.97, P=0.018). On average, men who engaged more with healthcare providers during visits had lower odds of being non-adherent to blood glucose testing (OR=0.87, P< 0.001). Men who reported reasons for medication non-adherence (OR=1.68, P=0.043) and used tobacco products (OR=2.39, P< 0.001) were more likely to report blood glucose testing non-adherence.
Conclusion: Findings suggest that disease progression, greater engagement with healthcare providers, and improved healthy behaviors may be associated with adherence to blood glucose testing among Black and Hispanic men with a history of prediabetes. Culturally tailored interventions and strategies are needed to improve adherence among male these sub-groups.
Plain Language Summary: Without adopting self-care behaviors and adhering to recommended screenings, prediabetes is likely to progress to type 2 diabetes. This study examined factors associated with non-adherence to recommended blood glucose testing among non-Hispanic Black and Hispanic men ages ≥ 40 years with a history of prediabetes. Findings highlight the importance of quality of patient-provider communication and improved healthy behaviors to increase adherence to blood glucose testing among Black and Hispanic men with prediabetes.
Keywords: prediabetes, blood glucose testing, non-Hispanic Black, Hispanic, men
Introduction
Diabetes is a prevalent and chronic medical condition that impacts millions of Americans each year.1 Its burden extends beyond health, affecting finances and contributing to numerous health complications.2 Recent estimates from the Centers for Disease Control and Prevention3 indicate that approximately 14.7% of U.S. adults (38.1 million) have diabetes and about 38% (97.6 million) have prediabetes, a precursor state often preceding the disease.4 Disparities exist across populations,5,6 with non-Hispanic Black and Hispanic individuals experiencing disproportionately higher rates of prediabetes compared to non-Hispanic White individuals,7 and with more men (41.0%) than women (32.0%) affected.3 Risk factors for prediabetes include a body mass index (BMI) greater than 25, history of gestational diabetes, age over 35,4 physical inactivity, hypertension, elevated cholesterol, and other predisposing conditions.
Although racial and ethnic disparities in prediabetes prevalence, diabetes risk factors, and abnormal blood glucose screening have been documented, relatively few studies have focused specifically on adherence to recommended blood glucose testing among middle-aged and older non-Hispanic Black and Hispanic men with a history of prediabetes.7–9 This gap is important because men in racial and ethnic minority groups are less likely than non-Hispanic White men to participate in diabetes prevention and management programs, despite experiencing a higher burden of type 2 diabetes risk.10 Recent evidence suggests that Hispanic men face unique barriers to diabetes prevention engagement, including limited awareness of prediabetes, skepticism about personal diabetes risk, financial constraints, and concerns about program relevance.11
Prediabetes and diabetes are primarily diagnosed with four tests, including hemoglobin A1c (HbA1c), random blood sugar, fasting blood sugar, and oral glucose tolerance test.12 Since blood glucose testing is one of the primary methods used to identify abnormal glycemia and monitor risk status over time, adherence to recommended testing is an important component of prediabetes management.13,14 For adults with prediabetes, routine follow-up testing provides opportunities for early counseling, risk communication, and referral to evidence-based diabetes prevention resources before progression to type 2 diabetes; however, prior studies suggest that prediabetes-related clinical care activities, including diagnosis, counseling, and referral to preventive interventions, remain underused in primary care settings.15,16
Early detection and intervention in prediabetes are essential to prevent progression to type 2 diabetes. Annual blood glucose testing is strongly recommended for those with prediabetes, while individuals with normal glycemia are screened very three years.4,13 Evidence-based lifestyle recommendations include smoking cessation, moderated alcohol intake, a balanced diet, regular exercise, adherence to prescribed medications, and achieving a 5–7% reduction in body weight.17 Despite the proven effectiveness of these measures, sustained behavioral changes can be difficult.18
Barriers to effective self-care and adherence to prediabetes management including routine screenings, may include socioeconomic challenges,19,20 limited access to healthcare,3 communication gaps with healthcare providers,21 medication costs,21 and inadequate social support.22 Regular follow-up and effective patient-provider communication, supported by telehealth and patient portals, are critical to sustained engagement.23 Missed appointments reduce opportunities for routine screening and ongoing education.24,25 These barriers may be reflected in multiple, interrelated adherence behaviors because chronic disease self-management requires patients to integrate clinical recommendations into daily routines while navigating health beliefs, social support, and access to resources.26,27 For example, medication non-adherence may signal challenges related to habitual behavior, treatment beliefs, self-efficacy, or financial resources.27 Tobacco use may represent a biological risk factor for diabetes-related complications and a marker of broader disengagement from preventive healthcare among men with chronic conditions.15,28 Conversely, active engagement during physician visits may reflect greater personal agency, preparedness, and capacity to navigate clinical recommendations, which are relevant to routine blood glucose testing and chronic disease prevention.26,29,30
The present study focused on non-Hispanic Black and Hispanic men aged 40 years and older because this group falls within clinically emphasized screening age ranges and reflects the parent study’s focus on chronic disease management among middle-aged and older men with chronic conditions. Current recommendations advise testing adults beginning at age 35 years, particularly among those with overweight or obesity, while prior United States Preventive Services Task Force (USPSTF) guidance recommended screening adults aged 40 to 70 years with overweight or obesity as part of cardiovascular risk assessment.14,31 This focus is also important because Black and Hispanic/Latino adults experience disproportionately high diabetes burden, and men in racial and ethnic minority groups remain underrepresented in diabetes prevention and management programs.3,10,11
Because non-Hispanic Black and Hispanic men face a dual burden of high prediabetes rates and poor diabetes-related outcomes,5,8,13 there is an urgent need to identify modifiable factors that influence adherence to recommended blood glucose testing. This study examines the behavioral, clinical, and healthcare engagement factors associated with non-adherence among non-Hispanic Black and Hispanic men aged 40 and older with a history of prediabetes. Guided by this gap, the present study examined behavioral, clinical, and healthcare engagement correlates of blood glucose testing non-adherence among non-Hispanic Black and Hispanic men with a history of prediabetes. Specifically, we assessed whether self-reported diabetes progression, patient-provider communication, engagement during physician visits, medication adherence patterns, tobacco use, and other health-related factors were associated with non-adherence to annual blood glucose testing. Understanding these factors can inform evidence-based strategies and educational interventions on regular blood glucose monitoring.
Materials and Methods
Participants and Procedures
This study employed an internet-delivered, cross-sectional survey design using a non-probabilistic national sample collected through a Qualtrics Online Panel.32 The survey was part of a larger parent study examining health indicators, healthcare utilization, and barriers to disease management among non-Hispanic Black and Hispanic men ages 40 years and older who self-reported one or more chronic conditions.26 A robust online questionnaire was developed using previously validated items and scales from sources such as the Behavioral Risk Factor Surveillance System and National Study of the Chronic Disease Self-Management Program.33–35 The instrument included 105 items, which took approximately 30 minutes to complete. The survey was conducted between September and October 2019. Participants accessed the survey through an electronic link and were required to review and acknowledge an informed consent prior to participation. Participants completed the questionnaire independently online. Data quality assessments were performed by Qualtrics in terms of data completeness, reasonable time to complete, and participant uniqueness.32 Further details about the survey instrument and methodology have been published in detail elsewhere.26,29,30,36–40 This study complies with the Declaration of Helsinki and was approved by the Texas A&M University Institutional Review Board (ID: 2018–1684).
Of 2029 men who met the inclusion criteria (non-Hispanic Black and Hispanic men aged 40 years or older with one or more chronic conditions) and completed the survey, 47 cases were omitted because they self-identified as both Black and Hispanic. Among these, 958 participants self-reported a prediabetes diagnosis. To omit biases related to healthcare access and interactions with healthcare providers, 189 men were omitted for not reporting a routine check-up with a physician in the past year. The final analytic sample was 769 non-Hispanic Black and Hispanic aged 40 and over with prediabetes who had a routine check-up in the past year.
Measures
The dependent variable for this study was whether the participants received a blood glucose test in the past 12 months. Participants were asked, “When was the last time you had a blood sugar test?” Response choices were “within the past year,” “within the past two years (more than one year ago),” “within the past three years (more than two years ago),” “within the past four years (more than three years ago),” “within the past five years (more than 4 years ago),” and “five or more years ago.” This dichotomization was selected based on both clinical guidance and the observed response distribution in the analytic sample. The Centers for Disease Control and Prevention (CDC) indicates that individuals with prediabetes will likely be advised to repeat A1C testing every 1 to 2 years;41 however, the frequency distribution in the current sample indicated that most participants reported receiving a blood glucose test within the past year. Therefore, we operationalized recent blood glucose testing adherence as having received a blood glucose test within the past 12 months (0=adherent; 1=non-adherent) to distinguish men who reported recent testing from those whose most recent test occurred more than 12 months prior.
Self-Reported Progression to Diabetes
Participants were also asked, “Have you ever been told by a doctor or other health professional that you have prediabetes or borderline diabetes?” Response choices were “no” and “yes.” Participants were also asked to self-report all chronic conditions that a healthcare provider told them they had.26 The participants were provided with a list of 19 chronic conditions, of which diabetes was an option. Response choices were “no” and “yes.” Given that all participants in the current study self-reported a history of prediabetes, self-reported diabetes was included in the analyses to indicate the progression from prediabetes to diabetes. The progression to diabetes variable in this cross-sectional study was based on self-reported diagnosis from a healthcare professional and not confirmed by clinical testing.
Health Indicators
Body mass index (BMI) was calculated as self-reported weight (pounds) divided by height (inches) and multiplied by 703. The resulting BMI scores were categorized for analyses as normal weight (18.5 to 24.99 kg/m2), overweight (25 to 29.99 kg/m2), and obese (≥ 30 kg/m2).42 As mentioned above, participants were asked to self-report whether they had been diagnosed with a series of chronic conditions by a healthcare provider. Health conditions relevant to prediabetes and diabetes were included in the analyses (ie., heart disease, high cholesterol, hypertension, and thyroid condition). Each of these variables was binarily coded (no/yes) and analyzed separately.
Frequency of Help and Support Needed to Improve Health and Manage Health Problems
The frequency of participants receiving the health and support needed to improve their health and manage health problems was measured using a 5-point scale ranging from “never” (scored 1) to “always” (scored 5).43,44
Physician Quality Conversation and Joint Decision-Making Scale
This 6-item scale asked participants about the extent to which they believed their conversations with physicians were of high quality and included joint decision making.43,44 Using a 5-point scale with response options ranging from “never” to “always,” participants were asked to report how often their healthcare provider: 1) asked for their ideas about how they can take care of their health problems; 2) made plans to contact them after a visit to see how they are doing; 3) helped them get the appointments they need; 4) asked if they understood how and when to take their prescribed medications, possible medication side effects, and drug interactions; 5) talked to other doctors and nurses who are taking care of them; and 6) asked whether they had help at home to manage their health problems. Items were summed, with possible scores ranging from 6–30. Higher scores indicate higher quality conversation. The Cronbach’s alpha scale value was acceptable for the current sample (α=0.841).
Engagement During Physician Visit Scale
This 4-item scale asked participants about their engagement with physicians during healthcare visits.34,35 Using a 5-point scale with response options of “never” to “always,” participants reported how often: 1) they prepared a list of questions for their doctor; 2) their doctor asked questions about things they want to know and things they do not understand about their treatment; 3) they discussed any personal problems that may be related to their illness; and 4) their doctor asked questions until they clearly understand the purpose for taking each of their medications. The possible scores ranged from 4–20, with higher scores indicating higher engagement during physician visits. The Cronbach’s alpha scale value was acceptable for the current sample (α=0.804).
Adherence to Medications
Participants were asked to report on their medication taking. Three items were asked: 1) Do you ever have problems remembering to take your medicine? 2) When you feel better, do you sometimes stop taking your medicine? and 3) Sometimes if you feel worse when you take your medicine, do you stop taking it? Response choices for each item were “no” and “yes.” These items were summed to create a count variable, then dichotomized to identify whether participants had one or more reasons why they did not adhere to their prescribed medications (ie., 0=adherent; 1=one or more reasons for not being adherent).
Health-Related Behaviors
Participants were asked to report their use of any tobacco product in the past 30 days and the number of alcoholic beverages consumed weekly.26,33 Tobacco use was dichotomized to reflect whether the participant had reported using tobacco in the past month (no/yes). Alcohol consumption was dichotomized to reflect if the participant consumed one or more alcoholic beverages in a typical week (no/yes).
Sociodemographics
The sociodemographic measures included in this study included race and ethnicity (ie., non-Hispanic Black, Hispanic), age (range 40 to 88 years), educational attainment (ie., high school education or less, some college/2-year degree, 4-year college degree or more), marital status (ie., married/partnered, never married, divorced/separated, widowed), number of persons living in the household (including self), and annual household income level (in mostly $10,000 USD increments).
Statistical Analyses
Data were analyzed using SPSS 29.0 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were computed to identify sample characteristics, which were compared by race and ethnicity and blood glucose testing adherence in the past 12 months. Proportional differences were compared using Chi-square tests for categorical variables. Mean differences were compared using independent-sample t-tests for continuous variables. Three binary logistic regression models with backward stepwise entry were fitted to identify factors associated with non-adherence to blood glucose testing (ie., getting a blood glucose test in the past 12 months served as the reference category). Logistic regression with backward stepwise entry was used to identify parsimonious models of significant variables while avoiding potential issues of multicollinearity. One model examined the factors associated with non-adherence for all men who met the inclusion criteria. Then, separate models were fitted to examine the associations among non-Hispanic Black men and Hispanic men independently. For each model, the full and reduced models are presented; however, the reported results focus only on the reduced models. Odds ratios (OR) with corresponding p-values and 95% confidence intervals (CIs) are reported. A p-value <0.05 was used to identify statistically significant associations in all analyses.
Results
Among the 769 men with self-reported prediabetes, 56.7% were non-Hispanic Black, 43.3% were Hispanic, and 10.8% were non-adherent because they had not received a blood glucose test in the past year. About 61% of participants reported that they progressed from prediabetes to diabetes. On average, participants were aged 57.80 (±9.52) years and resided with 2.54 (±1.45) people in their household. Over half were married/partnered (56.2%), had some college education or a 2-year degree (41.7%) or a 4-year college education (38.4%), and were obese (50.2%). Over 16% of the participants self-reported a heart disease diagnosis, 55.9% reported high cholesterol, 65.7% reported hypertension, and 10.1% reported a thyroid problem. Nearly half (48.0%) of the participants reported one or more reasons for not adhering to their prescribed medications, 30.9% reported using tobacco in the past 30 days, and 59.9% reported drinking one or more alcoholic beverages each week. Table 1 reports the characteristics of the participants in the current sample, which were compared by race and ethnicity and blood glucose adherence in the past year.
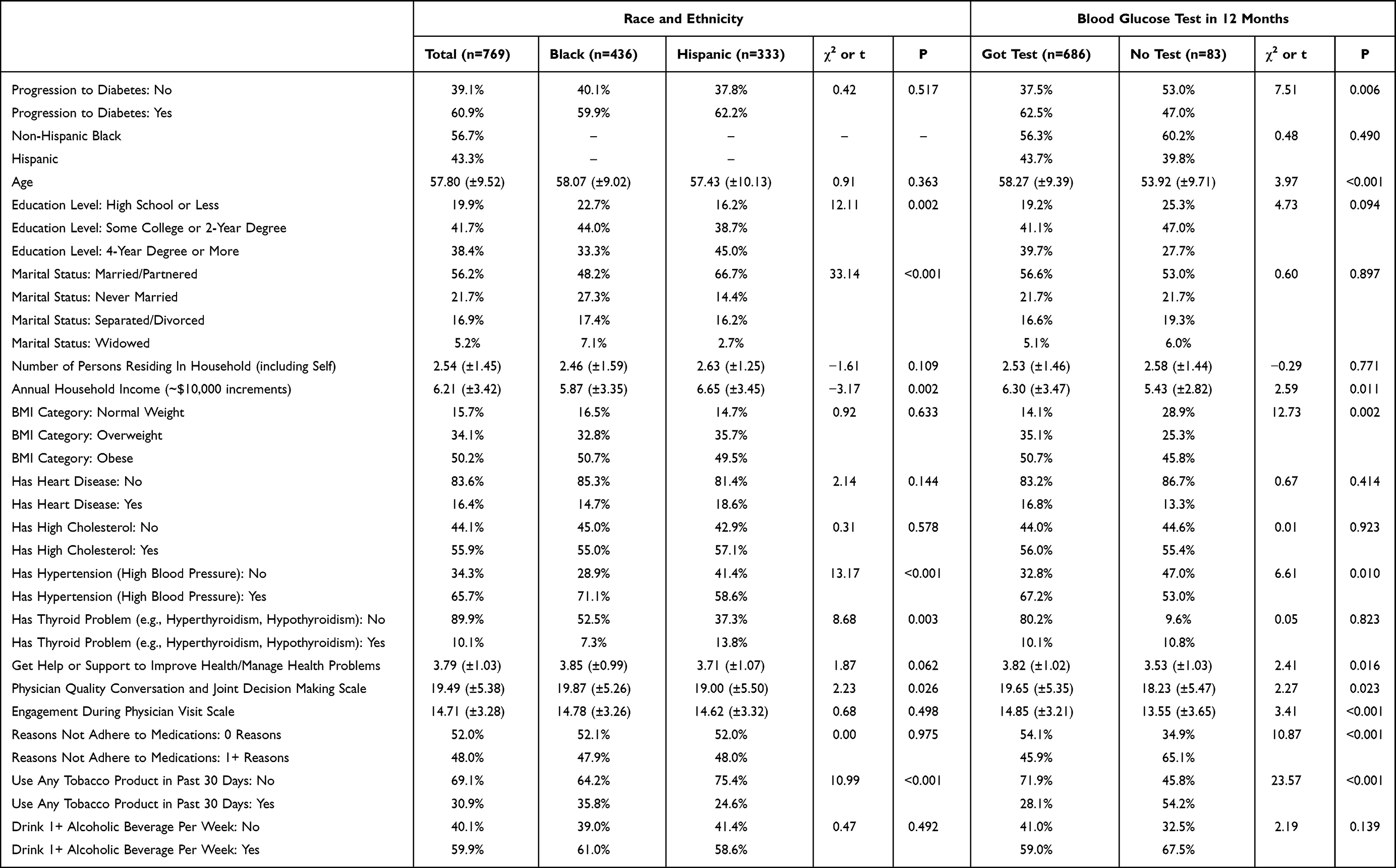 |
Table 1 Sample Characteristics by Race and Ethnicity and Blood Glucose Testing |
When comparing the sample by race and ethnicity, a larger proportion of Hispanic men had higher educational levels (χ2=12.11, P=0.002) and were married/partnered (χ2=33.14, P<0.001). On average, Hispanic men reported higher annual household incomes (t=−3.17, P=0.002). A larger proportion of non-Hispanic Black men self-reported hypertension (χ2=13.17, P<0.001), while a larger proportion of Hispanic men reported a thyroid problem (χ2=8.68, P=0.003). Relative to Hispanic men, a larger proportion of non-Hispanic Black men used a tobacco product in the past 30 days (χ2=10.99, P<0.001).
When comparing the sample by blood glucose testing non-adherence in the past 12 months, a larger proportion of men who progressed from prediabetes to diabetes were less likely to be non-adherent to blood glucose testing (χ2=7.51, P<0.006). On average, non-adherent men were younger (t=3.97, P<0.001) and had lower annual household income levels (t=2.59, P=0.011). A larger proportion of men of normal weight were non-adherent to blood glucose testing (χ2=12.73, P=0.002). A smaller proportion of men with hypertension were less likely to be non-adherent to blood glucose testing (χ2=6.61, P=0.010). On average, men who were non-adherent to blood glucose testing reported less help/support to improve their health and manage their health problems (t=2.41, P=0.016), lower quality conversations and joint decision making with physicians (t=2.27, P=0.023), and lower engagement during physician visits (t=3.41, P<0.001). A larger proportion of men who reported one or more reasons they do not adhere with prescribed medications (χ2=10.87, P<0.001) and used tobacco in the past 30 days (χ2=23.57, P<0.001) were non-adherent to blood glucose testing.
Table 2 reports the logistic regression models that examined non-adherence to blood glucose testing among non-Hispanic Black and Hispanic men. As seen in the reduced model, compared to men with prediabetes, men who progressed from prediabetes to diabetes were significantly less likely to not adhere to blood glucose testing (OR=0.51, P=0.006). Each additional year of age lowered the odds of non-adherence to blood glucose testing (OR=0.97, P=0.018). Higher engagement during physician visits was associated with lower odds of being non-adherent to blood glucose testing (OR=0.87, P<0.001). Men who reported having one or more reasons for medication non-adherence (OR=1.68, P=0.043) and used tobacco in the past 30 days (OR=2.39, P<0.001) were significantly more likely to be non-adherent to blood glucose testing, respectively.
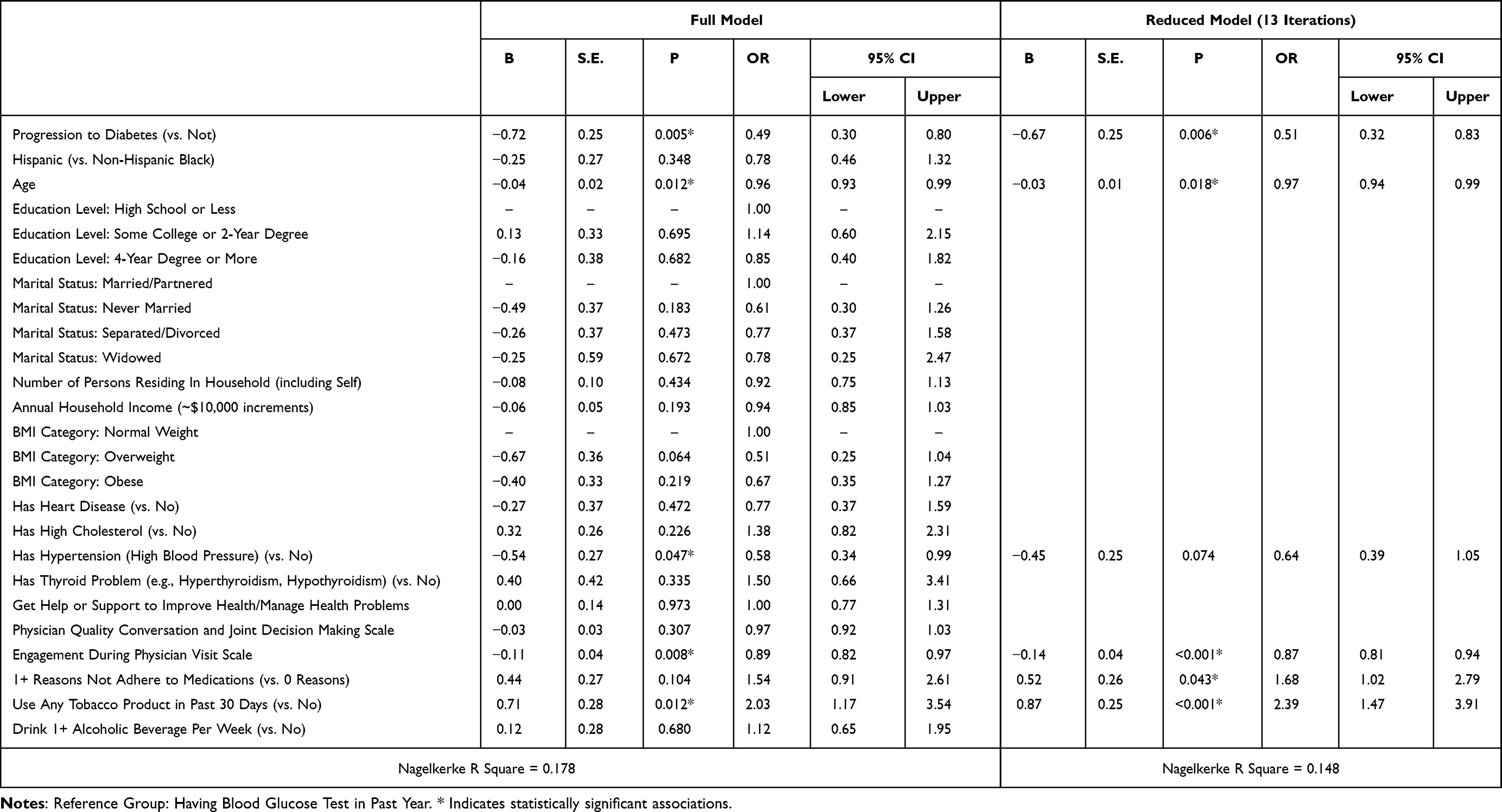 |
Table 2 Factors Associated with Blood Glucose Testing Non-Adherence - All Men (n=769) |
Table 3 reports the logistic regression models that examined non-adherence to blood glucose testing among non-Hispanic Black men. As seen in the reduced model, compared to men of normal weight, overweight men were less likely to be non-adherent to blood glucose testing (OR=0.35, P=0.026). Each additional unit on the Engagement During Physician Visit Scale was associated with lower odds of being non-adherent to blood glucose testing (OR=0.89, P=0.019). Men who reported having one or more reasons for medication non-adherence (OR=2.28, P=0.017) and used tobacco in the past 30 days (OR=3.06, P=0.001) were significantly more likely to be non-adherent to blood glucose testing, respectively.
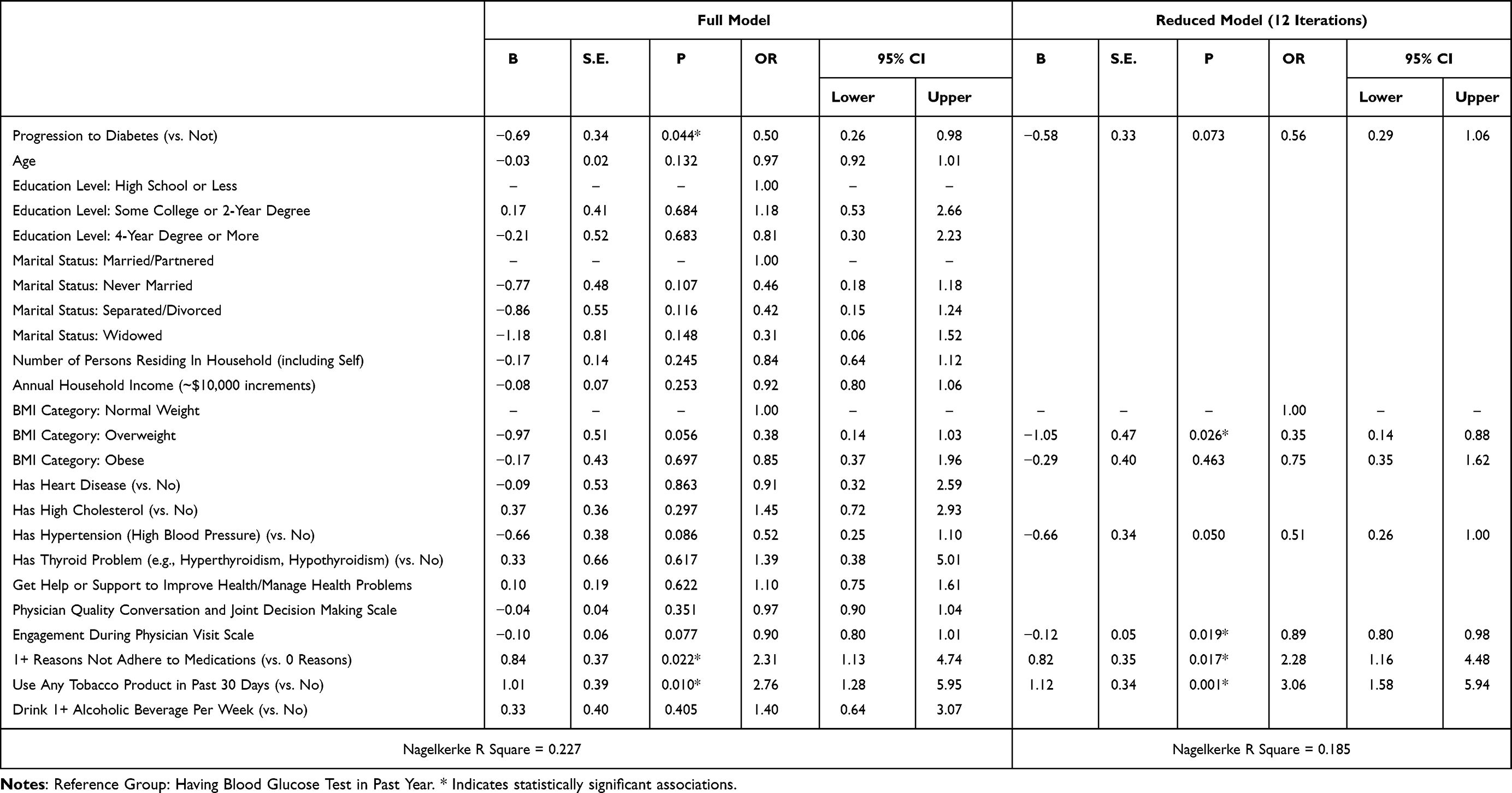 |
Table 3 Factors Associated with Blood Glucose Testing Non-Adherence - Non-Hispanic Black Men (n=436) |
Table 4 reports the logistic regression models that examined non-adherence to blood glucose testing among Hispanic men. As seen in the reduced model, men who progressed from prediabetes to diabetes were significantly less likely to be non-adherent to blood glucose testing compared to men with prediabetes (OR=0.43, P=0.027). Each additional year of age was associated with lower odds of being non-adherent to blood glucose testing (OR=0.95, P=0.016). Each additional unit on the Engagement During Physician Visit Scale reduced the odds of being non-adherent to blood glucose testing (OR=0.87, P=0.010).
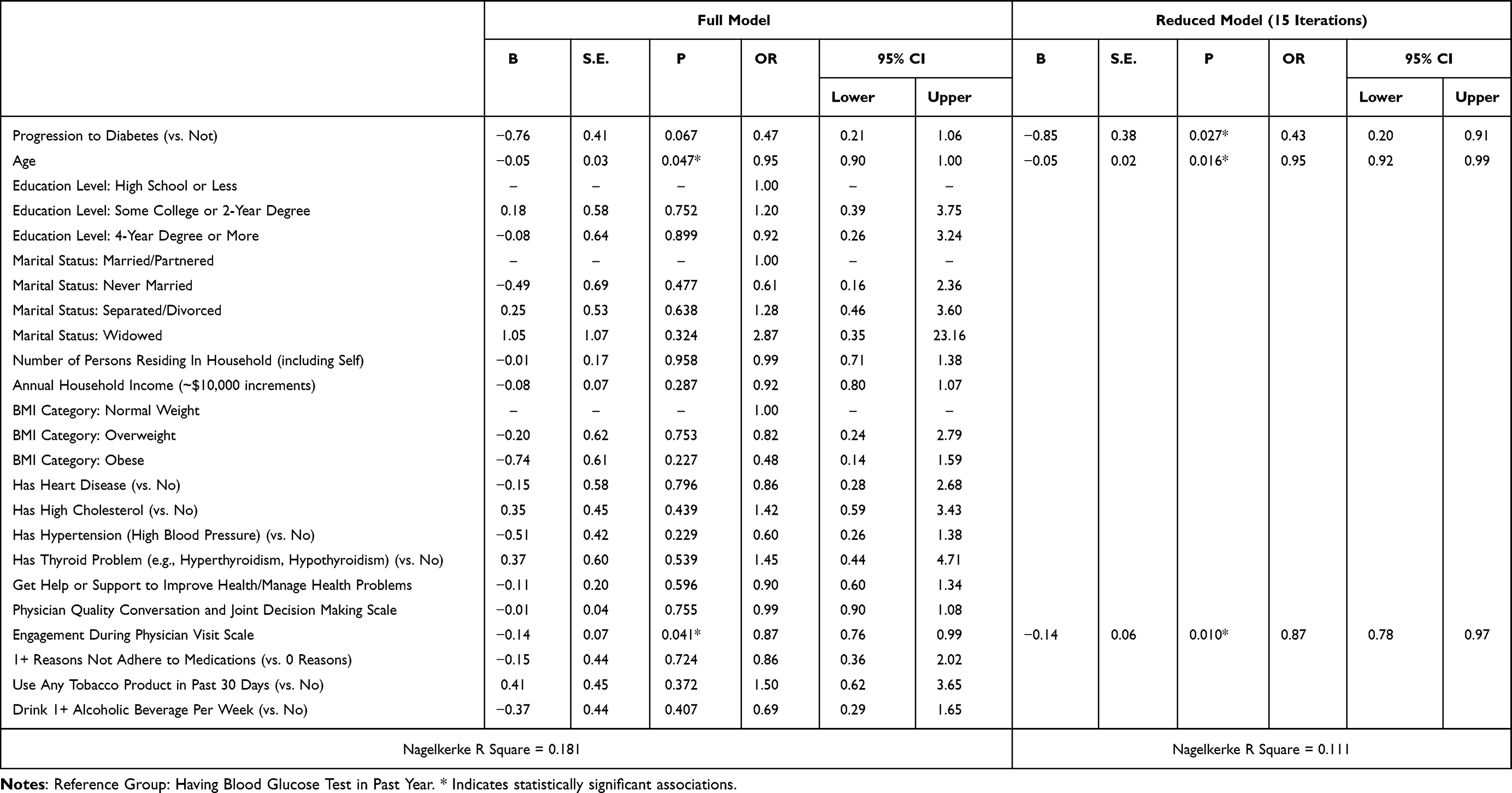 |
Table 4 Factors Associated with Blood Glucose Testing Non-Adherence - Hispanic Men (n=333) |
Discussion
This study identified factors associated with non-adherence to annual blood glucose testing in a large sample of non-Hispanic Black and Hispanic men with prediabetes, a group known to be at high risk but often underrepresented in adherence research.9 In a diverse sample of 769 men with prediabetes, approximately 11% of men did not meet the recommended testing frequency, highlighting an important gap in preventive care.9,13,15 The findings suggest four primary factors were significantly associated with testing non-adherence: progression to type 2 diabetes, quality of patient-provider communication with shared decision-making, medication adherence patterns, and tobacco use.
Men who had progressed from prediabetes to diabetes demonstrated greater adherence to blood glucose testing, consistent with clinical guidelines recommending more frequent monitoring once diabetes is diagnosed.42 This higher adherence may reflect personalized diabetes management and increased patient awareness following disease progression.45,46 These adherence differences between groups emphasize the need for early and sustained engagement with individuals diagnosed with prediabetes to encourage routine monitoring to prevent disease progression.12,16,47
Quality of patient-provider communication was consistently associated with adherence across both racial groups. Men reporting higher scores on conversation quality and engagement scales were significantly more likely to adhere to blood glucose testing. The association between patient-provider communication and testing adherence is a key finding, suggesting that high-quality clinical interactions, specifically those that facilitate joint decision-making, may be an important correlate of patient engagement and adherence in this population.48,49 However, while perceived physician conversation quality and joint decision-making were associated with testing adherence in bivariate comparisons, engagement during physician visits remained in the reduced multivariable models. This pattern may indicate that active patient participation, such as preparing questions, discussing illness-related concerns, and clarifying medication purpose, is more proximally related to completing recommended testing than global perceptions of communication quality, consistent with the Chronic Care Model emphasis on informed, activated patients and productive patient-provider interactions.26 This pattern may also partly reflect conceptual overlap between the communication and engagement scales, with the engagement measure capturing more actionable patient behaviors related to personal agency and chronic disease self-management.26,30
Medication non-adherence was significantly associated with blood glucose testing non-adherence. Nearly half of participants reported reasons for not adhering to prescribed medications, including skipping doses, stopping when feeling better, or discontinuing due to side effects. These patterns suggest barriers beyond simple refusal, such as lack of symptom recognition, concerns about medication effects, and insufficient provider guidance.50 Addressing these barriers through patient education, regular follow-up, and tailored interventions may improve both medication and screening adherence.50
Tobacco use was strongly associated with non-adherence to annual blood glucose testing. Nearly one-third of participants reported recent tobacco usage, yet only 28.1% of this group had received a blood sugar test in the past year, compared to 71.9% of non-users. This finding is concerning because tobacco use is associated with insulin resistance,51 inflammation and oxidative stress,2 and diabetes progression.51,52 Although tobacco use is biologically relevant to diabetes risk and complications, smoking cessation is associated with lower risks of diabetes-related complications and is emphasized as an important component of diabetes care.28,53 Tobacco use may also serve as a marker of broader preventive-care disengagement, as current tobacco use patterns have been associated with healthcare utilization among non-Hispanic Black and Hispanic men aged 40 years and older with chronic conditions.54 These findings support integrating smoking cessation support into diabetes and prediabetes-related preventive care to help identify and support men who may be at risk for non-adherence to routine blood glucose testing.53,54 This supports the potential value of integrated interventions that combine culturally tailored diabetes education with robust smoking cessation support.53
Race- and ethnicity-specific analyses revealed both shared and unique factors associated with non-adherence. For non-Hispanic Black men, overweight status was associated with lower odds of non-adherence, and medication non-adherence and tobacco use were prominent factors. Among Hispanic men, progression to diabetes, age, and physician engagement were associated with non-adherence, with quality patient-provider communication standing out as a cross-cutting facilitator of adherence. These distinctions highlight the necessity of culturally tailored interventions that address population-specific challenges while promoting universally important elements such as effective communication.
Culturally responsive interventions for non-Hispanic Black and Hispanic men should move beyond generic education and address the social, cultural, and structural contexts that shape preventive care engagement, including social networks, trust, access barriers, and community norms around chronic disease self-management.10,11,55 DSMES programs may provide a practical framework for these efforts because they can address glucose monitoring, medication-taking, healthy eating, physical activity, problem solving, and risk-reduction behaviors in culturally responsive ways.53 For example, CHWs or promotoras could support DSMES-related outreach by explaining prediabetes risk and blood glucose testing recommendations, reinforcing medication adherence, and connecting men to tailored physical activity and nutrition programs.56,57 For Hispanic men, promotora-supported strategies may help address limited prediabetes awareness, financial barriers, language preferences, and perceived program relevance.11 For non-Hispanic Black men, peer-supported and community-based approaches may help build trust, address stigma or masculine norms around help-seeking, and strengthen self-management confidence.55,58 Partnerships with faith communities, church-affiliated barbershops, community centers, worksites, and other trusted local organizations may also help reach Black and Hispanic men in familiar settings where diabetes education, screening promotion, and lifestyle-focused programs can be normalized.10,59,60
Limitations
This study has several limitations that should be considered when interpreting the findings, including its cross-sectional design, which precludes causal inferences and reliance on self-reported data which may be subject to recall and reporting biases. The online data collection method may have introduced selection bias toward individuals with internet access and greater health literacy. Future research should explore the use of mixed methods to capture both quantitative outcomes and patient-centered experiences. Our exclusive focus on non-Hispanic Black and Hispanic men with chronic conditions limits generalizability to other demographic groups. Adherence was operationalized as having any blood glucose test within the past year, which does not capture testing frequency. The progression from prediabetes to diabetes was based on self-reported healthcare professional diagnoses and not confirmed by laboratory testing, which may be subject to recall and reporting bias. Further, the survey instrument did not capture the diagnosis date related to prediabetes or diabetes, which prevented examining the temporal relationship between prediabetes history and self-reported progression to diabetes. The Nagelkerke R-square values for the reduced logistic regression models ranged from 0.111 to 0.185, indicating that the variables in the model only explain a modest amount of variance in the dependent variable. Future studies should incorporate additional predictor variables that may more robustly explain blood glucose testing adherence (eg., diagnosis temporality, cultural beliefs, mental health issues, access to diabetes education programs). Finally, our reliance on self-reported testing without verification through medical records or actual glucose values limits our ability to assess how effectively participants were managing their condition despite adherence to screening recommendations. Future longitudinal studies should follow men with prediabetes across repeated clinical encounters to determine whether changes in healthcare engagement, medication adherence, tobacco use, and social support precede changes in blood glucose testing adherence. Linking survey data with electronic health records, laboratory values, and appointment histories would allow researchers to track the timing of prediabetes diagnosis, repeat glycemic testing, referral to diabetes prevention programs, intervention participation, and progression to type 2 diabetes. Such designs could also test whether culturally tailored interventions improve testing adherence over time and whether improved adherence is associated with earlier risk management or delayed diabetes progression.
Conclusion
This study examined important behavioral, clinical, and communicative factors associated with blood glucose testing non-adherence among at-risk minority men with prediabetes. Findings suggest that enhancing patient-provider communication quality may be an actionable strategy to promote screening adherence and potentially reduce diabetes progression. While patient-provider communication is important, our results indicate that it is one of several potential factors associated with adherence, which warrants further research. Integrated interventions addressing medication adherence and tobacco cessation, tailored to the cultural contexts of non-Hispanic Black and Hispanic men, may play a critical role in closing adherence gaps. Ultimately, multifaceted approaches that prioritize healthcare engagement, address concurrent health behaviors and acknowledge diversity within groups are essential for reducing diabetes disparities and improving outcomes among non-Hispanic Black and Hispanic men.
Data Sharing Statement
The data accessed compiled with relevant data protection and privacy regulations. The dataset used during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Texas A&M University Institutional Review Board (ID: 2018-1684). All participants viewed an informed consent page prior to the start of the study.
Consent for Publication
Written consent and assent were obtained from all participants involved in this study.
Acknowledgments
Dr. Matthew Lee Smith is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The abstract of this paper was presented at the 2025 American Public Health Association (APHA) annual conference as a poster presentation with interim findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Texas A&M University through their Texas A&M Triads for Transformation (T3) initiative.
Disclosure
The authors declare that there is no conflicts of interest in this work.
References
1. Standl E, Khunti K, Hansen TB, Schnell O. The global epidemics of diabetes in the 21st century: current situation and perspectives. Eur J Preventi Cardiol. 2019;26(2_suppl):7–15. doi:10.1177/2047487319881021
2. Caraballo C, Valero-Elizondo J, Khera R, et al. Burden and consequences of financial hardship from medical bills among nonelderly adults with diabetes mellitus in the United States. Circ Cardiovasc Qual Outcomes. 2020;13(2):e006139. doi:10.1161/CIRCOUTCOMES.119.006139
3. Centers for Disease Control and Prevention [CDC]. National Diabetes Statistics Report. Available from: https://www.cdc.gov/diabetes/php/data-research/index.html.
4. Alvarez S, Coffey R, Mathias PM, Algotar AM. Prediabetes. Treasure Island (FL): StatPearls Publishing; 2026.
5. Cheng YJ, Kanaya AM, Araneta MRG, et al. Prevalence of diabetes by race and ethnicity in the United States, 2011–2016. JAMA. 2019;322(24):2389–2398. doi:10.1001/jama.2019.19365
6. Spanakis EK, Golden SH. Race/ethnic difference in diabetes and diabetic complications. Curr Diabet Rep. 2013;13(6):814–823. doi:10.1007/s11892-013-0421-9
7. Formagini T, Brooks JV, Roberts A, et al. Prediabetes prevalence and awareness by race, ethnicity, and educational attainment among US adults. Front Public Health. 2023;11:1277657. doi:10.3389/fpubh.2023.1277657
8. Koyama AK, Bullard KM, Onufrak S, et al. Risk factors amenable to primary prevention of type 2 diabetes among disaggregated racial and ethnic subgroups in the US. Diabetes Care. 2023;46(12):2112–2119. doi:10.2337/dci23-0056
9. Thomas TW, Golin C, Samuel-Hodge CD, Kirkman MS, Golden SD, Lightfoot AF. Race and gender differences in abnormal blood glucose screening and clinician response to prediabetes: a mixed-methods assessment. Preventive Med. 2021;148:106587. doi:10.1016/j.ypmed.2021.106587
10. Hulbert L, Mensa-Wilmot Y, Rutledge S, Owens-Gary M, Skeete R, Cannon MJ. Interests and preferences in programs to improve health among men with or at risk for type 2 diabetes in racial and ethnic minority groups, 2019. Preventing Chronic Dis. 2025;22:E04. doi:10.5888/pcd22.240268
11. Gonzalez CJ, Perez-Mejia CN, Hernandez N, et al. Engagement in the National Diabetes Prevention Program Among Hispanic Men. JAMA Netw Open. 2025;8(6):e2515046. doi:10.1001/jamanetworkopen.2025.15046
12. National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK]. Insulin Resistance & Prediabetes. Available from: https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/prediabetes-insulin-resistance.
13. Echouffo-Tcheugui JB, Perreault L, Ji L, Dagogo-Jack S. Diagnosis and management of prediabetes: a review. JAMA. 2023;329(14):1206–1216. doi:10.1001/jama.2023.4063
14. Bajaj M, McCoy RG, Balapattabi K. Diagnosis and Classification of Diabetes: standards of Care in Diabetes-2026. Diabetes Care. 2026;49(Supplement_1):S27–S49. doi:10.2337/dc26-S002
15. Mainous IIIAG, Rooks BJ, Wright RU, Sumfest JM, Carek PJ. Diabetes Prevention in a US Healthcare System: a portrait of missed opportunities. Am J Preventive Med. 2022;62(1):50–56. doi:10.1016/j.amepre.2021.06.018
16. Tseng E, Durkin N, Clark JM, Maruthur NM, Marsteller JA, Segal JB. Clinical care among individuals with prediabetes in primary care: a retrospective cohort study. J Gen Intern Med. 2022;37(16):4112–4119. doi:10.1007/s11606-022-07412-9
17. Centers for Disease Control and Prevention [CDC]. What is the National DPP? Available from: https://www.cdc.gov/diabetes-prevention/programs/what-is-the-national-dpp.html.
18. Group DPPR. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403. doi:10.1056/NEJMoa012512
19. Mogre V, Johnson NA, Tzelepis F, Paul C. Barriers to diabetic self-care: a qualitative study of patients’ and healthcare providers’ perspectives. J Clin Nurs. 2019;28(11–12):2296–2308. doi:10.1111/jocn.14835
20. Woodward A, Walters K, Davies N, et al. Barriers and facilitators of self-management of diabetes amongst people experiencing socioeconomic deprivation: a systematic review and qualitative synthesis. Health Expectations. 2024;27(3):e14070. doi:10.1111/hex.14070
21. Yoon S, Goh H, Phang JK, Kwan YH, Low LL. Socioeconomic and behavioral determinants of non-compliance with physician referrals following community screening for diabetes, hypertension and hyperlipidemia: a mixed-methods study. Sci Rep. 2023;13(1):20554. doi:10.1038/s41598-023-47168-8
22. Barber S, Hayhoe B, Richardson S, Norton J, Karki M, El-Osta A. Drivers and barriers to promoting self-care in individuals living with multiple long-term health conditions: a cross-sectional online survey of health and care professionals. BMC Public Health. 2025;25(1):884. doi:10.1186/s12889-025-21737-0
23. Stowell M, Dobson R, Garner K, Baig M, Nehren N, Whittaker R. Digital interventions for self-management of prediabetes: a scoping review. PLoS One. 2024;19(5):e0303074. doi:10.1371/journal.pone.0303074
24. Amat M, Duralde E, Masutani R, Glassman R, Shen C, Graham KL. “Patient lost to follow-up”: opportunities and challenges in delivering primary care in academic medical centers. J Gen Intern Med. 2022;37(11):2678–2683. doi:10.1007/s11606-021-07216-3
25. Karter AJ, Parker MM, Moffet HH, et al. Missed appointments and poor glycemic control: an opportunity to identify high-risk diabetic patients. Med Care. 2004;42(2):110–115. doi:10.1097/01.mlr.0000109023.64650.73
26. Smith ML, Bergeron CD, Sherman LD, Goidel K, Merianos AL. Contextualizing the chronic care model among non-Hispanic Black and Hispanic men with chronic conditions. Int J Environ Res Public Health. 2022;19(6):3655. doi:10.3390/ijerph19063655
27. Zhang J, Hu J, Zheng Y, Dai T. Factors affecting medication adherence in patients with chronic diseases: a systematic literature review. Chin General Pract J. 2025;2(3):100072. doi:10.1016/j.cgpj.2025.100072
28. Walicka M, Krysiński A, La Rosa GRM, et al. Influence of quitting smoking on diabetes-related complications: a scoping review with a systematic search strategy. Diabetes Metab Syndr. 2024;18(5):103044. doi:10.1016/j.dsx.2024.103044
29. Bergeron CD, Cisneros Franco CL, Sherman LD, et al. Health Care Engagement in Disease Prevention and Management: factors Influencing Chronic Disease Program Referral Adherence Among Non-Hispanic Black and Hispanic Men With Chronic Conditions. Am J Mens Health. 2024;18(5):15579883241288978. doi:10.1177/15579883241288978
30. Sherman LD, Cisneros-Franco CL, Prochnow T, et al. Personal Agency and Social Supports to Manage Health Among Non-Hispanic Black and Hispanic Men With Diabetes. Am J Mens Health. 2023;17(6):15579883231211057. doi:10.1177/15579883231211057
31. Davidson KW, Barry MJ, Mangione CM, et al. Screening for Prediabetes and Type 2 Diabetes: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;326(8):736–743. doi:10.1001/jama.2021.12531
32. Qualtrics. Online Panels. Available from: https://www.qualtrics.com/support/survey-platform/distributions-module/online-panels/.
33. Centers for Disease Control and Prevention [CDC]. Behavioral Risk Factor Surveillance System. Available from: https://www.cdc.gov/brfss/index.html.
34. Ory MG, Ahn S, Jiang L, et al. National study of chronic disease self-management: six-month outcome findings. J Aging Health. 2013;25(7):1258–1274. doi:10.1177/0898264313502531
35. Ory MG, Ahn S, Jiang L, et al. Successes of a national study of the chronic disease self-management program: meeting the triple aim of health care reform. Med Care. 2013;51(11):992–998. doi:10.1097/MLR.0b013e3182a95dd1
36. Park JH, Franco CLC, Bergeron CD, et al. Assessing Situational Awareness for Healthful Behaviors and the “Self-Care Gap” Among Non-Hispanic Black and Hispanic Men With Chronic Conditions. Health Promot Pract. 2025:15248399251370369. doi:10.1177/15248399251370369.
37. Park JH, Bergeron CD, Ness M, et al. Associations of depressive symptoms, social engagement and support, and lifestyle behaviors among non-Hispanic black and Hispanic men with chronic conditions in the United States. Front Public Health. 2025;13:1600818. doi:10.3389/fpubh.2025.1600818
38. Cudjoe TKM, Taylor HO, Sherman LD, et al. Challenges to Social Connection Among Black Men with Chronic Conditions: examination of Structural, Functional, and Quality Domains. Ethn Dis. 2025;35(1):41–47. doi:10.18865/EthnDis-2024-8
39. Oloruntoba O, Bergeron CD, Zhong L, et al. Pharmacological Prescribing and Satisfaction with Pain Treatment Among Non-Hispanic Black Men with Chronic Pain. Patient Prefer Adherence. 2024;18:187–195. doi:10.2147/ppa.S435652
40. Kew CL, Washington TR, Bergeron CD, et al. Caregiver strain among non-Hispanic Black and Hispanic male caregivers with self-reported chronic health conditions. Ethn Health. 2023;28(8):1161–1177. doi:10.1080/13557858.2023.2222341
41. Centers for Disease Control and Prevention [CDC]. A1C Test for Diabetes and Prediabetes. Available from: https://www.cdc.gov/diabetes/diabetes-testing/prediabetes-a1c-test.html.
42. Centers for Disease Control and Prevention [CDC]. Adult BMI Categories. Available from: https://www.cdc.gov/diabetes/diabetes-testing/prediabetes-a1c-test.html.
43. Smith ML, Ory MG, Ahn S, Miles TP. Factors Associated with Women’s Chronic Disease Management: associations of Healthcare Frustrations, Physician Support, and Self-Care Needs. J Aging Res. 2013;2013(1):982052. doi:10.1155/2013/982052
44. Philanthropies A. NCOA issues call-to-action for national chronic care reform based on survey of Americans with chronic conditions. PRNewswire. 2009;2009:1.
45. Abdulrahman M, Husain ZS, Abdouli KA, Kazim MN, Ahmad FSM, Carrick FR. Association between knowledge, awareness, and practice of patients with type 2 diabetes with socio-economic status, adherence to medication and disease complications. Diabetes Res Clin Pract. 2020;163:108124. doi:10.1016/j.diabres.2020.108124
46. Williams DM, Jones H, Stephens JW. Personalized type 2 diabetes management: an update on recent advances and recommendations. Diabet Metab Syndrome Obesity. 2022;2022:281–295. doi:10.2147/DMSO.S331654
47. Njeru JW, Castro MR, Carta KG, Simon G, Caraballo PJ. Clinical recognition and management of patients with prediabetes. Endocr Pract. 2019;25(6):545–553. doi:10.4158/EP-2018-0485
48. Piette JD, Schillinger D, Potter MB, Heisler M. Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population. J Gen Intern Med. 2003;18(8):624–633. doi:10.1046/j.1525-1497.2003.31968.x
49. Reid HW, Lin OM, Fabbro RL, et al. Racial differences in patient perception of interactions with providers are associated with health outcomes in type II diabetes. Patient Educ Couns. 2021;104(8):1993–2003. doi:10.1016/j.pec.2021.01.031
50. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155. doi:10.5001/omj.2011.38
51. Chen Z, X-a L, Kenny PJ. Central and peripheral actions of nicotine that influence blood glucose homeostasis and the development of diabetes. Pharmacol Res. 2023;194:106860. doi:10.1016/j.phrs.2023.106860
52. Facchini FS, Hollenbeck CB, Jeppesen J, Chen Y-DI, Reaven G. Insulin resistance and cigarette smoking. Lancet. 1992;339(8802):1128–1130. doi:10.1016/0140-6736(92)90730-Q
53. Care D. Facilitating Positive Health Behaviors and Well-being to Improve Health Outcomes: standards of Care in Diabetes—2026. Diabetes Care. 2026;49:S89.
54. Merianos AL, Mahabee-Gittens EM, Montemayor BN, et al. Current tobacco use patterns associated with healthcare utilization among non-Hispanic Black and Hispanic men with chronic conditions. Addict Behav. 2023;143:107695. doi:10.1016/j.addbeh.2023.107695
55. Prochnow T, Smith ML, Patterson MS, Park JH, Sherman LD. Making the connection: social networks and type 2 diabetes among Black/African American Men: mixed-methods study protocol. Front Public Health. 2025;13:1483880. doi:10.3389/fpubh.2025.1483880
56. Ruggiero L, Quinn L, Castillo A, Monahan C, Boughton Price L, Hernandez W. Community Health Worker Diabetes Prevention Awareness Training in an Immersive Virtual World Environment: mixed Methods Pilot Study. JMIR Form Res. 2025;9:e64051. doi:10.2196/64051
57. Johnson CM, Allicock MA, Sharkey JR, et al. Promotoras de Salud in a Father-Focused Nutrition and Physical Activity Program for Border Communities: approaches and Lessons Learned from Collaboration. Int J Environ Res Public Health. 2022;19(18):11660. doi:10.3390/ijerph191811660
58. Ewen AM, Hawkins JM, Kloss KA, et al. The Michigan men’s diabetes project: perspectives on a peer-led diabetes self-management and support intervention for Black men with type 2 diabetes. BMC Health Serv Res. 2024;24(1):1612. doi:10.1186/s12913-024-11884-2
59. Samuel-Hodge CD, Keyserling TC, France R, et al. A church-based diabetes self-management education program for African Americans with type 2 diabetes. Prev Chronic Dis. 2006;3(3):A93.
60. Balls-Berry J, Watson C, Kadimpati S, et al. Black Men’s Perceptions and Knowledge of Diabetes: a Church-Affiliated Barbershop Focus Group Study. J Racial Ethn Health Disparities. 2015;2(4):465–472. doi:10.1007/s40615-015-0094-y
 © 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.