Back to Journals » Clinical Interventions in Aging » Volume 18
Factors Associated with In-Hospital Mortality in Elderly Internal Medicine Patients with Nasogastric Tube Feeding
Authors Plotnikov G ![]() , Sharif S, Buturlin G
, Sharif S, Buturlin G ![]() , Segal I, Gorelik O, Kagansky N
, Segal I, Gorelik O, Kagansky N ![]()
Received 11 February 2023
Accepted for publication 2 May 2023
Published 9 May 2023 Volume 2023:18 Pages 729—735
DOI https://doi.org/10.2147/CIA.S408207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Galina Plotnikov,1,2 Saleh Sharif,2,3 Gleb Buturlin,2 Inbal Segal,1 Oleg Gorelik,2 Nadya Kagansky2,4
1Geriatric Assessment Unit, Yitzhak Shamir Medical Center, Zerifin, 7033001, Israel; 2Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel; 3Department of Internal Medicine C, Yitzhak Shamir Medical Center, Zerifin, 7033001, Israel; 4Shmuel Harofe Geriatric Medical Center, Beer Yaakov, Israel
Correspondence: Galina Plotnikov, Geriatric Assessment Unit, Yitzhak Shamir Medical Center, Zerifin, 7033001, Israel, Tel +972-8-9542271, Fax +972-8-9779597, Email [email protected]
Purpose: To evaluate demographic, clinical, and laboratory variables, and their associations with in-hospital mortality, among elderly internal medicine patients with nasogastric tube (NGT) feeding.
Patients and Methods: Demographic, clinical, and laboratory data were collected retrospectively for 129 patients aged ≥ 80 years who initiated NGT feeding during their hospitalization in internal medicine wards. The data were compared between survivors and non-survivors. Multivariate logistic regressions were performed to identify the variables most significantly associated with in-hospital mortality.
Results: The in-hospital mortality rate was 60.5%. Compared to survivors, non-survivors more often presented with pressure sores (P=0.005) and lymphopenia (P< 0.001), were more often treated with invasive mechanical ventilation (P< 0.001), and less often underwent geriatric assessment (P< 0.001). Non-survivors demonstrated higher mean levels of C-reactive protein, and lower mean values of serum cholesterol, triglycerides, total protein, and albumin (P< 0.001 for all comparisons). On multivariate analysis, the following variables were most significantly associated with in-hospital mortality in the entire cohort: the presence of pressure sores (odds ratio [OR], 4.34; 95% confidence interval [CI], 1.68– 11.48; P=0.003) and lymphopenia (OR, 4.09; 95% CI, 1.51– 11.08; P=0.006), and serum cholesterol (OR, 0.98; 95% CI, 0.96– 0.99; P=0.003).
Conclusion: Among elderly acutely ill patients who initiated NGT feeding during hospitalization, in-hospital mortality was extremely high. The factors most strongly associated with in-hospital mortality were the presence of pressure sores and lymphopenia, and lower serum cholesterol levels. These findings may provide useful prognostic information for decision-making regarding initiation of NGT feeding in elderly hospitalized patients.
Keywords: aging, enteral feeding, hospitalization, prognosis
Introduction
Advances in healthcare contribute to the rising of the older people population in the world. Malnutrition is common in the elderly, ranging from 5–30% in community-dwelling individuals to 16–70% in residential aged and acute care settings.1 The etiology of malnutrition in the elderly is multifactorial, and mainly related to dysphagia and anorexia, that result from age-dependent changes in muscle mass and such comorbidities as follows: dementia, stroke, depression, cancer, heart failure, and chronic lung disease.1–3 Malnutrition is associated with adverse outcomes such as increased risk of infections and falls, poorer quality of life, prolonged length of hospital stay, and shorter survival.1,3 For patients with insufficient or impossible oral nutrition, enteral feeding is recommended, to meet nutritional requirements and improve nutritional status.3–5 However, tube feeding is not recommended for elderly patients with advanced dementia and poor functional status.4–6 Most studies of the prognosis of older patients on enteral tube feeding were performed in ambulatory and geriatric care settings,7–11 and focused on long-term mortality in specific disorders, such as dementia,7–10 stroke,12,13 and cancer of the head and neck.13,14
Initiation of artificial nutrition, mainly via a nasogastric tube (NGT), is not rare among elderly patients admitted for acute illness in internal medicine wards. In this patient population, indications for NGT placement include impaired consciousness and respiratory failure, in addition to dysphagia and malnutrition.15,16 Feeding tubes are more commonly used in Israel than in other countries in the world.17 This discrepancy is explained by Israeli legal and ethical considerations. Accordingly, even for a patient who is prone to death, artificial nutrition must be provided, unless excepted by the presence of a medical contraindication for artificial nutrition or the stated refusal of such nutrition in a written advanced directive. Identifying the in-hospital mortality rate and the influencing factors of elderly patients hospitalized in internal medicine wards with NGT feeding may help physicians in decision-making regarding their care and management. Therefore, the aim of the current study was to evaluate demographic, clinical, and laboratory variables, and their associations with in-hospital mortality, among elderly patients who initiated NGT feeding during hospitalization in internal medicine wards.
Materials and Methods
Study Population and Design
The study was conducted in the Department of Internal Medicine “C”, one of seven Departments of Internal Medicine in Yitzhak Shamir Medical Center, a tertiary care university hospital located at Zerifin, Israel. This department includes 34 general and four intensive care beds. The patients were randomly admitted from the emergency department or transferred from other departments due to a variety of acute internal medicine conditions. The eligible population for the study comprised 539 adult patients hospitalized during January 2018–December 2019 who had NGT during their hospitalization. The end of the year 2019 was chosen as the end of the research period so as to eliminate the possible effect of the corona pandemic on study results. Exclusion criteria were as follows: age under 80 years, surgical reasons for NGT placement, such as intestinal obstruction or a mesenteric event, and initiation of NGT feeding prior the current hospitalization. Included in the study were 129 patients aged ≥80 years in whom NGT feeding was started during the index hospitalization. In a retrospective comparative study, characteristics of patients who did not survive the current hospitalization were compared to characteristics of patients who survived.
Data Collection
The following data for the index hospitalization were collected from electronic hospital records: demographic, clinical, and laboratory variables, and in-hospital death. For patients who were readmitted during the study period, only the data of their first hospitalization were obtained. Functional status was assessed by the Norton Scale. The Malnutrition Universal Screening Tool (MUST) score was used for malnutrition risk assessment. The data were compared between survivors and non-survivors during the index hospitalization.
Statistical Analysis
The results were expressed as numbers (percentages) for qualitative data. Quantitative data were tested for normal distribution using a histogram and the Kolmogorov–Smirnov test. Normally distributed variables were described as means and standard deviations, and variables that were not normally distributed were expressed as medians and interquartile ranges. The chi-square test or Fisher’s exact test was applied for comparison of discrete variables. Continuous variables were compared using the t-test for independent samples or the Mann–Whitney test. Variables that were found to be associated with in-hospital mortality on univariate analysis were included in stepwise logistic regression analysis. All statistical tests were two sided, and a P-value <0.05 was considered statistically significant. Statistical analysis was performed using SPSS statistical software (IBM SPSS Statistics for Windows, version 24, IBM Corp., Armonk, NY, USA, 2016).
The sample size was calculated for a significance level of 5% and a power of 80%. The assumption underlying the calculation of the sample size was that the mortality rate would be about 50%. To identify a moderate effect on in-hospital mortality, 128 patients were needed for continuous variables (effect size d = 0.5), and 126 patients were required for dichotomous categorical variables (effect size h = 0.5). Effect size d is equal to one unit of standard deviation. Thus, an effect of 0.5 represents a difference of one-half a standard deviation between the survivors and non-survivors. Accordingly, at least 128 patients should be included in the study.
Results
The Entire Sample
The demographic, clinical, and laboratory characteristics of the 129 patients included in the study are presented in Table 1. The mean age was 88.5 ± 4.9 years, 32.6% were males. The most common reason for admission was infectious disease. The most prevalent comorbidities were dementia, pressure sores, congestive heart failure, coronary artery disease, cerebrovascular disease, and diabetes mellitus. The mean age-adjusted Charlson Comorbidity Index was 7.95 ± 2.5. The mean Norton Scale score for functional assessment was 11.20 ± 2.8. The most common reasons for initiation of NGT feeding were respiratory failure and malnutrition. In the instance of respiratory failure, aspiration was suspected or treatment with invasive mechanical ventilation was started. The median length of hospital stay was 19 days. During hospitalization, 78 (60.5%) of 129 patients died. For the first week and for the first 19 days following NGT insertion, death was registered in 33 (25.6%) and 65 (50.4%) of the study population, respectively.
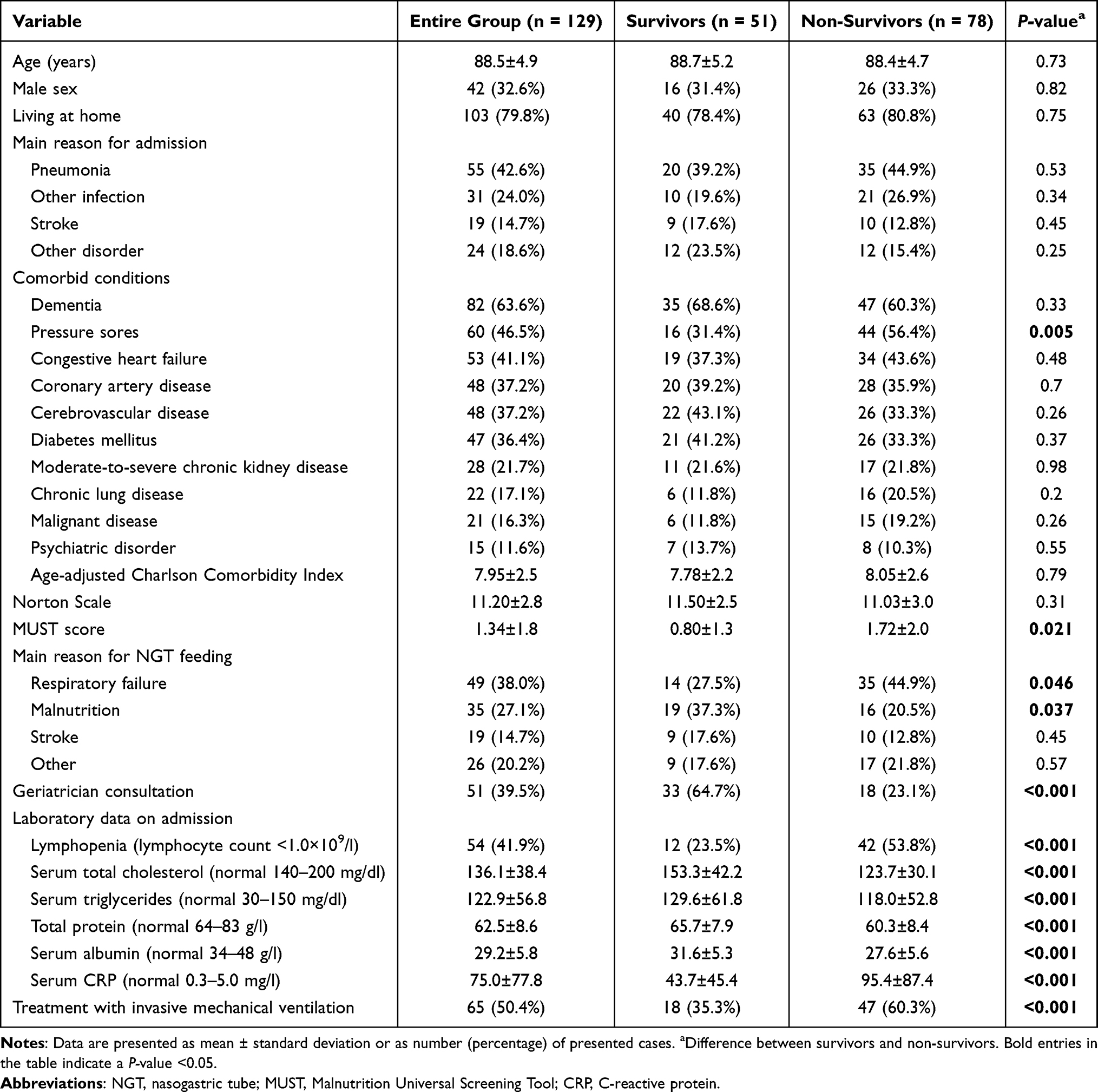 |
Table 1 Characteristics of the Patients Included in the Study, According to In-Hospital Survival |
Comparison of Patients’ Characteristics, According to In-Hospital Survival
Table 1 compares data between survivors and non-survivors. The demographic characteristics and main causes for admission were comparable between the groups. Of the various comorbidities examined, only pressure sores showed statistically significant differences in the proportions of non-survivors and survivors (56.4% vs 31.4%, P = 0.005). The mean value of the MUST score was higher among non-survivors than survivors (P = 0.021). In non-survivors compared to survivors, NGT feeding was initiated more often due to respiratory failure (P = 0.046) and less often due to malnutrition (P = 0.037). Non-survivors compared to survivors were less likely consulted by a geriatrician, more often presented with lymphopenia, and more often treated with invasive mechanical ventilation (P < 0.001 for all three comparisons). Non-survivors compared to survivors demonstrated higher mean levels of C-reactive protein (CRP), and lower mean levels of serum cholesterol, triglycerides, total protein, and albumin (P < 0.001 for all the comparisons).
To eliminate the effect on mortality of the need for invasive mechanical ventilation, we compared the data between survivors and non-survivors in a subgroup of 64 patients who were not treated with invasive mechanical ventilation (Table 2). Compared to survivors, non-survivors were more likely to have pressure sores (P < 0.047) and lymphopenia (P = 0.012), and were less often assessed by a geriatrician (P < 0.001). The mean value of the MUST score tended to be higher among the non-survivors than the survivors (P = 0.063). In addition, among the non-survivors compared to the survivors, the mean level of CRP was higher (P = 0.005), and the mean levels of serum cholesterol, total protein, and albumin were lower (P < 0.001 for all the comparisons).
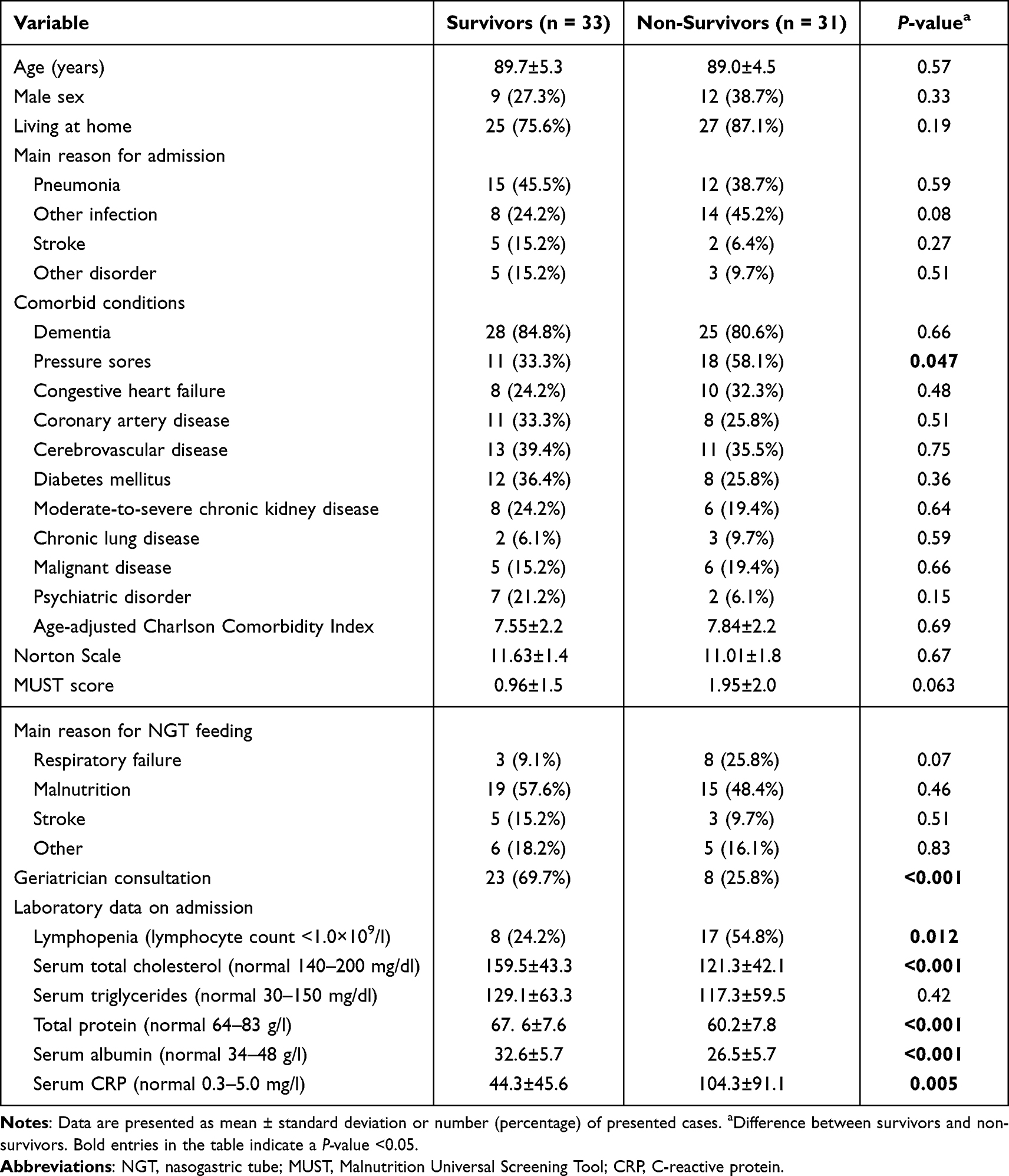 |
Table 2 Characteristics of the Patients Not Treated with Invasive Mechanical Ventilation, According to In-Hospital Survival |
In stepwise logistic regression analysis, the following variables were most significantly associated with in-hospital mortality in the entire cohort: the presence of pressure sores (odds ratio [OR], 4.34; 95% confidence interval [CI], 1.68–11.48; P = 0.003), lymphopenia (OR, 4.09; 95% CI, 1.51–11.08; P = 0.006), serum cholesterol (OR, 0.98; 95% CI, 0.96–0.99; P = 0.003), and treatment with invasive mechanical ventilation (OR, 2.41; 95% CI, 0.97–6.11; P = 0.059). Pressure sores (OR, 4.42; 95% CI, 1.73–11.30; P = 0.002), lymphopenia (OR, 4.07; 95% CI, 1.54–10.75; P = 0.005), and serum cholesterol (OR, 0.97; 95% CI, 0.95–0.99; P = 0.002) were strongly associated with mortality in a subgroup of patients not treated with invasive mechanical ventilation.
Discussion
To the best of our knowledge, this is the first study to investigate in-hospital mortality and factors influencing survival in elderly patients with NGT feeding in internal medicine wards. We report an extremely high rate (60.5%) of in-hospital mortality. Two studies on patients aged ≥65 years and admitted from nursing care facilities to a general hospital for acute illness reported shorter long-term survival among patients on enteral tube feeding than on oral nutrition.18,19 Those studies included a small number of patients with feeding tubes (16 and 79, respectively) and in-hospital mortality was not investigated. Of our 129 patients with NGT feeding who were admitted to an internal medicine ward, the majority were living at home. Our very low rate of in-hospital survival may be explained by the patients’ advanced age, poor functional and nutritional status, and high prevalence of preexisting comorbidities. In addition, the poor prognosis may be related to the severity of acute illness that was cause for hospitalization in internal medicine wards. Indeed, half our patients were treated with invasive mechanical ventilation. However, also among patients who were not mechanically ventilated, the mortality rate was high (48.4%). Associations were found of several indicators of malnutrition and increased inflammation with in-hospital mortality. Specifically, compared to survivors, non-survivors more often presented with pressure sores and lymphopenia, and demonstrated lower levels of serum cholesterol, total protein, and albumin, and higher values of CRP and the MUST score. Moreover, the presence of pressure sores and lymphopenia, and the lower levels of cholesterol were the variables that most strongly associated with in-hospital mortality.
Another interesting aspect of the present study is that non-survivors were less likely to have undergone geriatric assessment than survivors. Possible explanations for this finding include the palliative approach and optimization of drug treatment provided by geriatricians, which may have improved survival. Benefits of comprehensive geriatric assessment for internal medicine inpatients have been reported.19,20 The geriatrician-led care model showed shorter length of hospital stay and lower costs, without increasing mortality.20 However, only 39.5% of our patients received consultation with a geriatrician. This is probably because geriatricians were invited for consultation by physicians, and the need for such consultation is less in critically ill patients. Indeed, patients who were not mechanically ventilated were more often consulted by geriatricians than those mechanically ventilated (48.4% vs 30.8%). Considering the data together, we suggest that geriatric consultation may be considered in prognostic assessment for elderly patients hospitalized in internal medicine wards and needing NGT feeding.
The decision for or against starting NGT feeding, specifically in a population of elderly hospitalized patients with acute illness, is often controversial.15,19 The current international guidelines propose avoiding initiation of tube feeding in elderly patients with advanced dementia and poor functional status.4–6 For older patients with insufficient or impossible oral nutrition, enteral feeding is recommended, to meet nutritional requirements and improve nutritional status.3–5 However, the decision regarding enteral nutrition should be individualized and based on general prognosis, and also on ethical and legal considerations.4,5,15 Prior to NGT placement, predicting the prognosis of an acutely ill elderly patient is not easy. The prognosis demonstrated in the current study, of elderly patients hospitalized for acute illness in internal medicine wards and fed with NGT, was similar to that reported among patients with terminal cancer.21,22 The poor prognosis of our patients may prompt questions regarding the initiation of NGT feeding. Possibly, some of our patients could have been better managed by assisted hand feeding or other palliative treatment. We suggest that our findings of associations of a number of clinical and laboratory variables with mortality may help physicians in their decisions regarding the provision of NGT nutrition for elderly hospitalized patients. However, according to Israeli law, food and fluids must be provided, even by artificial nutrition, to a patient who is prone to death. Exceptions include clear and specific medical contraindications for artificial nutrition, or refusal of such nutrition in written advanced directives. Therefore, feeding tubes are more commonly used in Israel than in other countries in the world.17 There may be reason to reconsider indications for artificial feeding in the Israeli law or to encourage people to write advanced directives regarding artificial nutrition in the end of life.
Limitations
Our study has a number of limitations. First, as a single-center study, the results may not be generalizable to other medical centers. Second, due to the retrospective design, full functional, nutritional, and cognitive assessments were not possible, and missing data may have affected the results. Third, the relatively small sample size may have affected the statistical power for comparing some relevant data.
Conclusions
Among elderly acutely ill patients in whom NGT feeding was started during hospitalization in internal medicine wards, in-hospital mortality was extremely high. The presence of pressure sores and lymphopenia, and lower levels of serum cholesterol were the factors that most strongly associated with in-hospital mortality. These findings may provide useful prognostic information for physicians in decision-making regarding initiation of artificial nutrition in elderly hospitalized patients, and the care of such patients on NGT feeding.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was carried out in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Yitzhak Shamir (Assaf Harofeh) Medical Center, Zerifin, Israel (approval number 0049-20-ASF). Informed consent was not obtained from the patients because it was not requested for this retrospective study. In this design, patients were evaluated and treated according to the discretion of the treating physicians rather than research considerations. Moreover, data were collected from electronic medical records and the data used were anonymous.
Funding
The study was not funded by any commercial, non-profit or public organizations.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Agarwal E, Miller M, Yaxley A, Isenring E. Malnutrition in elderly: a narrative review. Maturitas. 2013;76(4):296–302. doi:10.1016/j.maturitas.2013.07.013
2. Morley JE. Anorexia of ageing: a key component in the pathogenesis of both sarcopenia and cachexia. J Cachexia Sarcopenia Muscle. 2017;8(4):523–526. doi:10.1002/jcsm.12192
3. Mundi MS, Patel J, McClave SA, Hurt RT. Current perspective for tube feeding in the elderly: from identifying malnutrition to providing of enteral nutrition. Clin Interv Aging. 2018;13:1353–1364. doi:10.2147/CIA.S134919
4. Volkert D, Beck AM, Cederholm T, et al. ESPEN guideline: clinical nutrition and hydration in geriatrics. Clin Nutr. 2022;41(4):958–989. doi:10.1016/j.clnu.2022.01.024
5. Schwartz DB, Barrocas A, Annetta MG, et al. Ethical aspects of artificially administered nutrition and hydration: an ASPEN position paper. Nutr Clin Pract. 2021;36(2):254–267. doi:10.1002/ncp.10633
6. American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. American geriatrics society feeding tubes in advanced dementia position statement. J Am Geriatr Soc. 2014;62(8):1590–1593. doi:10.1111/jgs.12924
7. Teno JM, Gozalo PL, Mitchell SL, et al. Does feeding tube insertion and its timing improve survival? J Am Geriatr Soc. 2012;60(10):1918–1921. doi:10.1111/j.1532-5415.2012.04148.x
8. Bentur N, Sternberg S, Shuldiner J, Dwolatzky T. Feeding tubes for older people with advanced dementia living in the community in Israel. Am J Alzheimers Dis Other Demen. 2015;30(2):165–172. doi:10.1177/1533317514539726
9. Chou HH, Tsou MT, Hwang LC. Nasogastric tube feeding versus assisted hand feeding in home healthcare older adults with severe dementia in Taiwan: a prognosis comparison. BMC Geriatr. 2020;20(1):60. doi:10.1186/s12877-020-1464-9
10. Davies N, Barrado-Martín Y, Vickerstaff V, et al. Enteral tube feeding for people with severe dementia. Cochrane Database Syst Rev. 2021;8(8):CD013503. doi:10.1002/14651858.CD013503.pub2
11. Tsugihashi Y, Akahane M, Nakanishi Y, et al. Long-term prognosis of enteral feeding and parenteral nutrition in a population aged 75 years and older: a population-based cohort study. BMC Geriatr. 2021;21(1):80. doi:10.1186/s12877-020-02003-x
12. Dennis MS, Lewis SC, Warlow C. Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): a multicenter randomized controlled trial. Lancet. 2005;365(9461):764–772. doi:10.1016/S0140-6736(05)17983-5
13. Gomes CAR Jr, Andriolo RB, Bennett C, et al. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2015;5:CD008096. doi:10.1002/14651858.CD008096.pub4
14. Corry J, Poon W, McPhee N, et al. Randomized study of percutaneous endoscopic gastrostomy versus nasogastric tubes for enteral feeding in head and neck cancer patients treated with chemo (radiation). J Med Imaging Radiat Oncol. 2008;52(5):503–510. doi:10.1111/j.1440-1673.2008.02003.x
15. Stroud M, Duncan H, Nightingale J. Guidelines for enteral feeding in adult hospital patients. Gut. 2003;52(Suppl7):vii1–vii12. doi:10.1136/gut.52.suppl_7.vii1
16. Smith HA, Kindell J, Baldwin RC, Waterman D, Makin AJ. Swallowing problems and dementia in acute hospital settings: practical guidance for the management of dysphagia. Clin Med. 2009;9(6):544–548. doi:10.7861/clinmedicine.9-6-544
17. Clarfield AM, Monette J, Bergman H, et al. Enteral feeding in end-stage dementia: a comparison of religious, ethnic, and national differences in Canada and Israel. J Gerontol a Biol Sci Med Sci. 2006;61(6):621–627. doi:10.1093/gerona/61.6.621
18. Tokuda Y, Koketsu H. High mortality in hospitalized elderly patients with feeding tube placement. Intern Med. 2002;41(8):613–616. doi:10.2169/internalmedicine.41.613
19. Veronese N, Cella A, Cruz-Jentoft AJ, et al. Enteral tube feeding and mortality in hospitalized older patients: a multicenter longitudinal study. Clin Nutr. 2020;39(5):1608–1612. doi:10.1016/j.clnu.2019.07.011
20. Merchant RA, Ho VWT, Chen MZ, et al. Outcomes of care by geriatricians and non-geriatricians in an academic hospital. Front Med. 2022;9:908100. doi:10.3389/fmed.2022.908100
21. Feliu J, Jiménez-Gordo AM, Madero S, et al. Development and validation of a prognostic nomogram for terminally ill cancer. J Natl Cancer Inst. 2011;103(21):1613–1620. doi:10.1093/jnci/djr388
22. Wang M, Jing X, Cao W, et al. A non-lab nomogram of survival prediction in home hospice care patients with gastrointestinal cancer. BMC Palliat Care. 2020;19(1):185. doi:10.1186/s12904-020-00690-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.