Back to Journals » Clinical Interventions in Aging » Volume 16
Factors Associated with Health Literacy, Self-Efficacy, Social Support, and Oral Health Care Behaviors Among Elderly in Northern Border Community Thailand
Authors Khamrin P, Boonyathee S ![]() , Bootsikeaw S
, Bootsikeaw S ![]() , Ong-Artborirak P
, Ong-Artborirak P ![]() , Seangpraw K
, Seangpraw K ![]()
Received 25 May 2021
Accepted for publication 15 July 2021
Published 22 July 2021 Volume 2021:16 Pages 1427—1437
DOI https://doi.org/10.2147/CIA.S320900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Pattaraporn Khamrin,1,2 Sorawit Boonyathee,1 Sasivimol Bootsikeaw,3 Parichat Ong-Artborirak,4 Katekaew Seangpraw3
1School of Medicine, University of Phayao, Phayao, 56000, Thailand; 2Ban Mai Health Promotion Hospital, Chiang Mai, 50180, Thailand; 3School of Public Health, University of Phayao, Phayao, 56000, Thailand; 4Faculty of Public Health, Chiang Mai University, Chiang Mai, 50200, Thailand
Correspondence: Katekaew Seangpraw
School of Public Health, University of Phayao, Phayao, 56000, Thailand
Tel +66 54 466 66
Email [email protected]
Background: Oral health problems among elderly people are an important public health issues worldwide. Oral healthcare is essential to the health and well-being of elders and is one of the key indicators determining their quality of life. This research aimed to study oral health literacy, self-efficacy, social support, and demographic characteristic factors associated with the oral health care behaviors of elderly people living in the rural areas of northern Thailand.
Methods: This research was a cross-sectional study that recruited 406 elderly participants using convenience and snowball samplings. Participants’ names were obtained from the registration list of the Java Health Center Information System (JHCIS) program, where they received a health service between 2018 and 2020. Data were obtained through face-to-face interviews with participants, while they were waiting to receive a health service or through a phone interview. Linear regression was analyzed to determine the factors associated with oral healthcare behaviors.
Results: The majority of participants (85%) had inadequate functional health literacy, 52% had moderate self-efficacy toward oral health behaviors, 91.9% had moderate social support, and 53% admitted to moderate oral health behaviors. The results from the model show that self-efficacy, social support, and oral health literacy are positively associated with oral health care behaviors among the elderly (p-value < 0.05). The multiple regression model can account for 47.2% of the variance in oral health care behaviors.
Conclusion: Improving oral health care behaviors among elderly people should be considered by health care providers and those who provide social support. Self-esteem, communication skills among service providers and service receivers, and self-management of oral healthcare should receive special attention. Moreover, social support and relevant agencies can help promote oral healthcare by collaborating with other healthcare providers for better oral health outcomes among elderly people.
Keywords: health literacy, self-efficacy, social support, oral health, elderly
Introduction
Oral health problems among elderly people are an important public health issues in Thailand and worldwide.1 Poor oral health care among the elderly is seen in the high level of tooth loss, dental caries, and the prevalence of periodontal diseases that have a major bearing on the quality of life, and lead to increasing dental and medical expenses.2,3
A Thailand report released 2017,4 found that of the elderly aged between 60–74 years (56.1%) have at least 20 active permanent teeth and (40.2%) have four pairs of posterior occlusion.4 Poor occlusion performance and periodontitis with tissue and root canal damage, increases the risk of inflammation, pain, swelling, infection, and loss of teeth among the elderly.4 The report also found untreated tooth decay and, root canal decay associated with receding gingival recession in older age is prevalent in Thailand.4,5 Furthermore, a previous report found an association between oral health and health conditions such as heart disease, stroke, and diabetes,; which become more common with increased age.6,7 Some studies have shown that poor oral healthcare among the elderly may lead to tooth loss and poor oral health function,8,9 such as reduced occlusion performance, causing digestive problems and other health complications.2 According to a study the emotional effects of tooth loss in edentulous people the pain of having oral health problems may affect the mental state of the elderly.10,11 This in turn makes them avoid socializing with people because they are worried about their image.1 Consequently, the elderly with dental problems tend to be more isolated from social gatherings than other age groups.1,10 Chiang Mai province, the largest province in northern Thailand, has the third highest aged population in the country.11 In 2018, 2019, and -2020, periodontal disease was reported to be 24.8%, 55.2%, and 57.3%, respectively, among the elderly aged 65–80 years.11,12 Periodontal disease, affects occlusion efficiency and the quality of life.11,12 Elderly people in Chiang Mai are experiencing oral health problems, due mainly to poor oral healthcare behaviors, such as wrong brushing and not cleaning their teeth regularly.4,12 The elderly also have restricted access to clinical oral examinations and services as well as communication problems with dentists.1,12 This is similar to the study which was found that dental health care problem is associated with a lack of oral health literacy.1,13 The elderly with high oral health literacy tend to have more permanent teeth than those who have low oral health literacy.13 Almost half of the elderly recognized that tooth loss can be replaced by a denture, but they ignore the importance of tooth replacement.14 Some studies have found that less than 50% of elderly people have mild oral hygiene habits such as brushing twice a day and seeing the dentist only if they experience oral health problems.15
Health literacy is the ability to obtain, process, and understand the basics of health information and, the services needed to make appropriate health decisions.16 Health literacy also facilitates the effective communication of health- related information and the importance of maintaining good health.17 An individual’s health literacy is the ability to perceive health depending upon education and knowledge adequacy, attributes that are affected by the culture, language, way of life, and health related practices of people in diverse environments.18,19 Health literacy is a strong predictor of an individual’s health, health behavior, and health outcomes.18 Limited knowledge toward health literacy is associated with poor self-ratings on health, poor adherence to medical instructions, poor self-management skills, increased mortality risks, poor health outcomes, and higher healthcare costs.19 Oral health literacy has been popular in the dental literature over the past decade.17,20 A person with limited oral health literacy has been reported to be at higher risk of oral diseases and problems associated with them.20 One study found that people with poor oral health literacy were more likely to miss dental health appointments.21 Non-adherence to dental recommendations has been reported to cause higher caries experiences22 and poor periodontal status.23 Oral health problems and poor oral health behaviors among the elderly should be an important focus in public health.24,25 Communication and preventive and therapeutic behaviors once the disease occurs are important for enhancing oral health among elderly people.15,24–26 This study applies the concept of health literacy as a person’s ability to access, understand, assess, use and communicate health information on demand to promote and maintain a healthy lifelong state.27 Moreover, in promoting oral healthcare behaviors it is important to advocate self-efficacy and social support, which affect the outcomes of self-care behaviors.28–30 This study is part of an on-going intervention research that explores oral health literacy, self-efficacy, social support, and demographic factors associated with oral health care behaviors among elderly living in a northern border community in Thailand. Importantly, this study aims to contribute to the development of oral health literacy and expectations of outcomes of their own proper oral health practice.
Methodology
This research was a cross-sectional study conducted in the rural Mae Rim district, Chiang Mai province, in northern Thailand between March – and May 2021. Chiang Mai was selected because it has the third highest number of elderly people living in Thailand according to the Department of Older Persons Thailand.11 The number of elderly people living in the province is expected to increase continuously.4,11 The mountainous area in which the study was conducted is located 30 kilometers from Chiang Mai city. Simple random sampling was employed using the drawing technique to select sub-districts out of 14 sub-districts. San Pong sub-district, Rim Tai sub-district, and Mae Rim sub-district were selected. The research was carried out at primary health service centers run by the Ministry of Public Health, where dentists can provide oral health examinations and services in the study area’s Health Promoting Hospital. Eligible participants were selected through convenience and snowball samplings. The inclusion criteria were: 1) Both males and females aged 60 years and older; 2) Living in the area of Mae Rim district for at least two years and having their names in the civil registry; 3) Registered as a patient in the Java Health Center Information System (JHCIS) 2018–2020 and received health services from the primary health center; 4) Ever received oral health service at the study area’s Health Promoting Hospitals; 5) No severe periodontitis, such as loose teeth, oral lesions, and swelling of the face or jaw; 6) The absence of any cognitive disorders; 7) Able to communicate in the local language; and 8) Willing to participate in the study. The sample size was calculated using the correlation coefficient formula31 with a 95% confidence level, 90% test power, and a correlation coefficient (r) = 0.163.32 The sample size was increased by five percent to address potential dropouts from the study by participants. The total number of participants in the study was 410 based on the calculation.
The study procedures started by recruiting 10 research assistants who were able to communicate in the local northern language. These assistants were public health personnel comprising three dental nurses, four public health scholars, and three nurses. A meeting was organized by the researcher on a single day from 9:00 am-12:00 pm to clarify the study’s objectives, data collection techniques, and the procedure for answering the questionnaires, schedule appointments, and to outline the rights and privacy of the participants. The researcher ensured that everyone obtained a common understanding regarding the research process. The researcher translated research materials into the local northern language so the research assistants could better understand the research context. In the process of data collection, the researcher contacted and cooperated with the director of the District Health Office, Health Promoting Hospital, and key persons in the community before data collection. Once the researcher obtained the written informed consent form, the research team started performing data collection in the study area. In the process of data collection, the elderly were interviewed face-to-face while waiting to receive health services at a health center. A telephone interview was performed in some cases when elderly participants could not come to a health center due to the COVID-19 pandemic situation. The process of data collection was conducted during the hours of 9:00 am and 16:00 pm; and the duration of each interview was approximately 20–30 minutes.
The questionnaires were used as an instrument to collect research information. The questionnaires were checked and validated by three experts in the field of dental and oral health, health behavioral science, and aging. The questionnaires comprised five parts including: 1) Part 1: Demographic characteristics such as gender, age, marital status, occupation, education level, chronic health conditions, current medication, smoking, alcohol consumption, income, and health and treatment benefits. 2) Part 2: An oral health literacy questionnaire adapted from related literature reviews to be suitable for the context of elderly people living in a rural community.25 The questionnaire comprised 37 items, and six components including: a) Assessing skills toward health information and services, which consisted of six questions; b) Cognitive skills, perceived knowledge and understanding of health information, which consisted of 10 questions; c) Communication skills, which consisted of four questions; d) Self-management skills, which consisted of seven questions;, e) Media literacy skills, which consisted of six questions; and f) Decision-making skills, which consisted of four questions. There were three choices for selecting an answer: Yes, “No”, and “Do not know.” The elderly people were allowed to choose only one answer. The scoring criteria were one point for a correct answer and 0 points for a wrong or “do not know” answer. The criteria for scoring were divided into three levels: scores ranging from 80–100% are considered as good; 60–69% is considered moderate; and 0–59% is considered poor. Therefore, scores greater than, or equal to, 30 indicates Adequate Health Literacy); scores of 22–29 indicate Marginal Functional Health Literacy; and scores less than, or equal to, 21 indicates Inadequacy Functional Health Literacy.33
3) Part 3: The Self-efficacy questionnaire on oral health behaviors was modified to be suitable for the context of elderly people living in a rural community.34 The questionnaire focused on the ability to regularly maintain oral healthcare behaviors, such as eating healthy food, cleaning or brushing teeth, and regular oral health check-ups. The questionnaire comprised 10 items. The questionnaire is a rating scale with three levels. The elderly participants could only select one answer from “Agree,” “Uncertain,” and “Disagree”. Scores between 24 and 30 indicates a good level, 18–23 indicates a moderate level, and 0–17 indicates a poor level.34,35 4) Part 4: A social support questionnaire toward periodontal status among elderly people which was adapted from related research and literature reviews to be suitable for the context of the elderly living in a rural community.36,37 Examples of social support questions were: 1. Have you ever received dental health information from dentists?; 2. Have you ever been supported, encouraged or reinforced by public health workers, family members or caregivers toward teeth brushing; and 3.Have you ever communicated with family caregivers regarding oral healthcare. The questionnaire comprised of 10 items using a Likert scale. Participants could choose one of the following answers: “Regularly,” “Sometimes,” and “Never”. Social support questionnaire was divided into three levels: Low (scores ≤ 17), Moderate (scores of 18–23), and High (scores ≥24). 5) Part 5: The oral healthcare behaviors questionnaire was modified from previous studies34,38 and included cleaning or brushing teeth, using dental floss, oral healthcare check-up, and healthy food consumption. The questionnaire comprises 12 items, and elderly participants could choose only one answer for activities they did during the previous week. The questionnaire is characterized by three scale levels: “Always Practice,” (5–7 times/week), “Sometimes Practice,” (2–4 times/week), and “Never Practice.” The scoring criteria are classified as follows: 28–36 indicates good oral healthcare behaviors; 21–27 indicates moderate oral health care behaviors; 0–20 indicates poor oral healthcare behaviors that need to be improved. The overall questionnaires were tested in a pilot study on 30 elderly people who had similar characteristics and lived in a rural community. A reliability test was performed on parts 2–5 of the questionnaires, with Cronbach’s alpha coefficient at 0.82, 0.87, 0.84, and 0.85, respectively.
Statistical Analysis
Statistical analysis was performed using the SPSS software version 17, licensed from Chiang Mai University (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to describe the demographic characteristics and general information among older adults. Linear regression was analyzed to determine the factors associated with oral health care behaviors. Initially, each independent variable was investigated using univariate analysis, with a p-value of 0.20. The significant variables were then included in a multivariate analysis to examine factors that were still linked to oral health care behaviors. The predictors, which were statistically significant at the 0.05 level, were put into the final regression model.
Results
According to Table 1, the results represent the demographic characteristics of the total of 406 elderly participants in the study. The average age of the participants was 66.97 years (SD = 4.34), and more than half of them were female (52.5%). Just over half (50.7%) of the participants had obtained primary education; 73.6% were married, and 56.2% were employed. More than half of the participants (50.7%) had insufficient income. In terms of health behaviors and health status, just over a third (34.2%) of participants smoked cigarettes and drank alcohol (46.6%). Half of the participants had a medical history, involving one or more of the following: hypertension (HT), stress, diabetes mellitus (DM), chronic kidney disease (CKD), hyperlipidemia, stroke, coronary heart disease (CHD), and tuberculosis (TB).
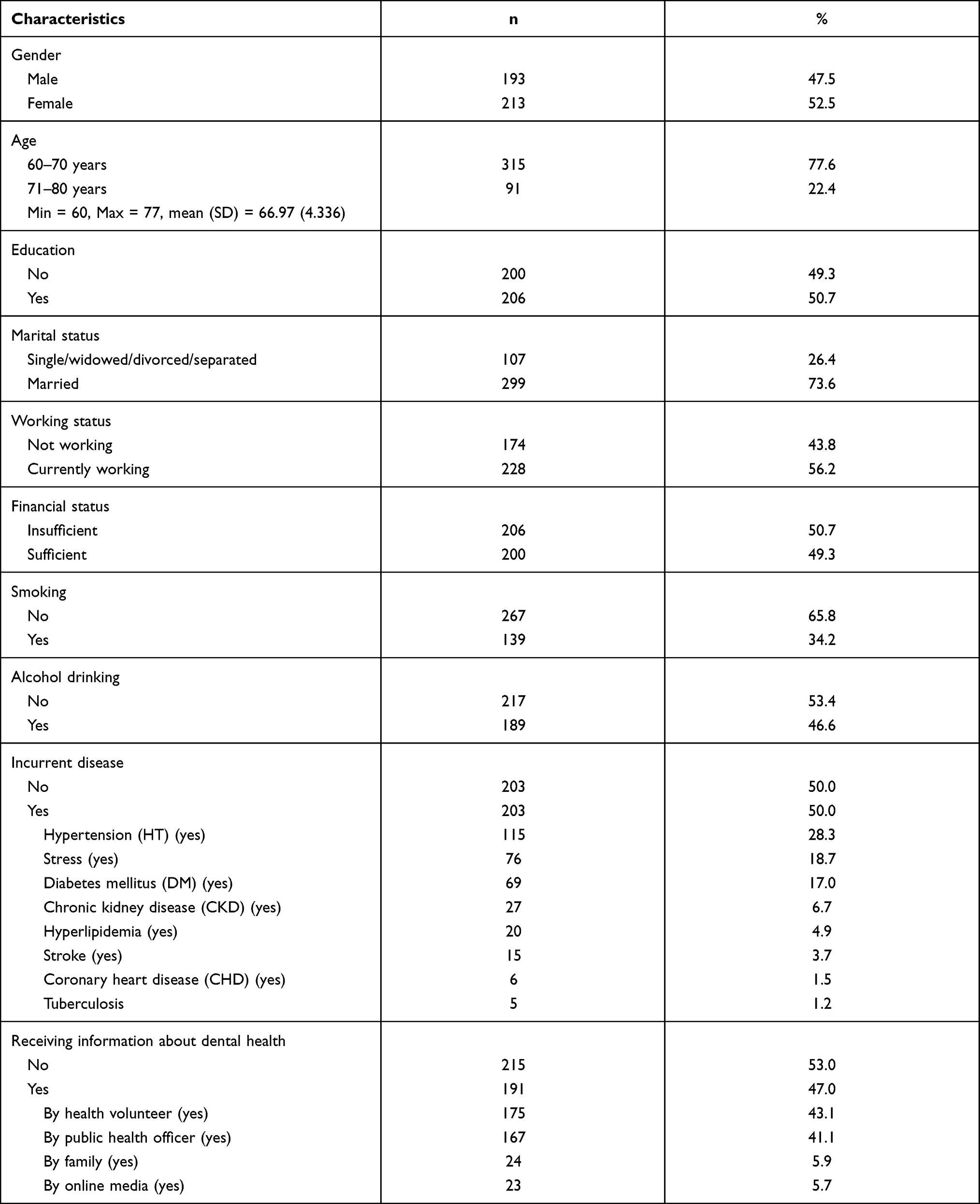 |
Table 1 Demographic Characteristics of Elderly (N=406) |
In terms of perceived health information, nearly half (47%) of the participants had ever received oral health information. The sources of health information came from village health volunteers, public health officers, family members, and online media. The oral health characteristics of the elderly are shown in Table 2. For health check-ups and health services, it was reported that over a third (37.4%) of participants had ever received an oral health examination; and the last check-up was over a year previously. The elderly had received services that included tooth extraction, denture and tooth replacement, cleaning and polishing teeth, fillings, addressing toothache, and other problems related to oral health.
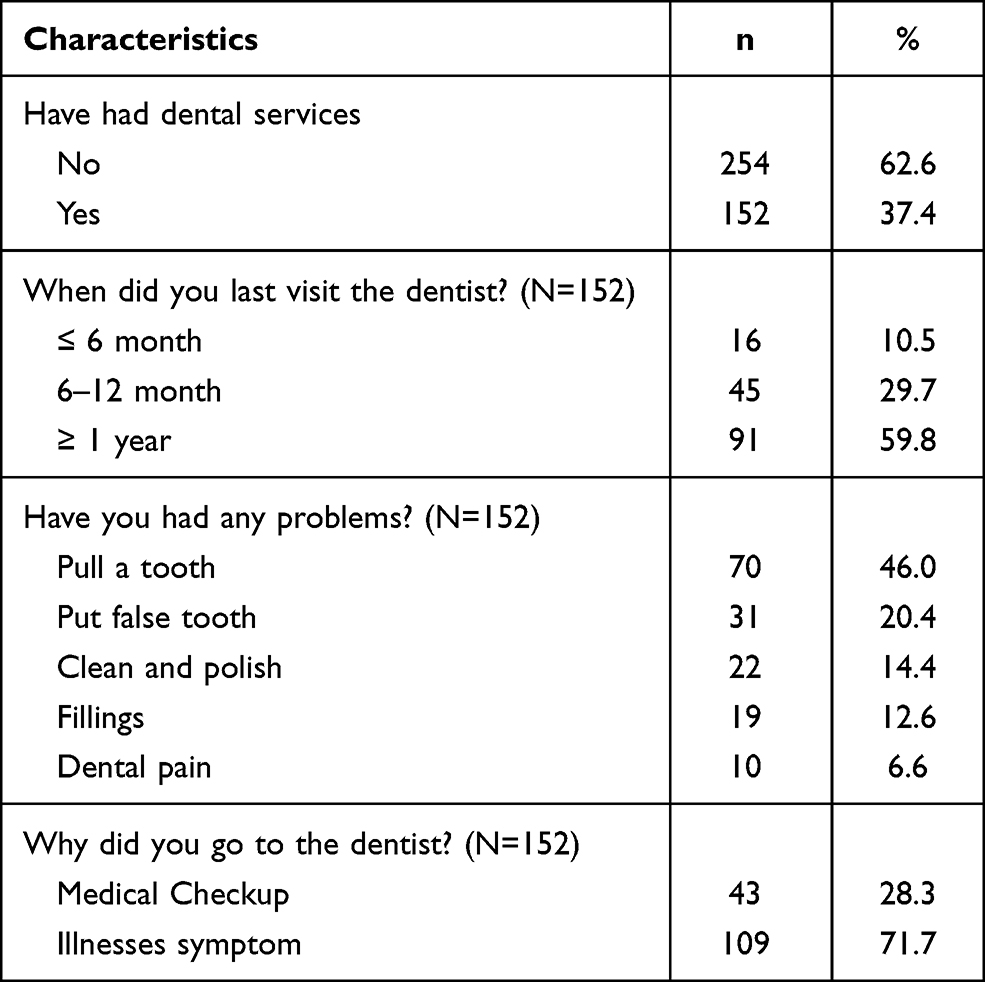 |
Table 2 Oral Health Characteristics of Elderly (N=406) |
Table 3 illustrates the percentages and scores of the studied variables. Participants had inadequate functional health literacy scores (85%), moderate functional health literacy scores (13.3%), and good functional health literacy scores (1.7%), respectively; and the mean score of functional health literacy was 17.63 (SD = 3.92). In terms of self-efficacy toward oral health behaviors, we found that more than half of the participants obtained scores at a moderate level (52.5%), poor level (45.8%), and high level (1.7%), respectively, with a mean score of 17.75 (SD = 2.28). In terms of social support, most of the participants obtained scores at the moderate level (91.9%), followed by poor and high levels (6.4% and 1.7%), respectively; with a mean score of 20.11 (SD = 1.58). In terms of oral health behaviors, more than half of participants (53%) obtained scores at the moderate level, (43%) obtained scores at the poor level, and 3.9% received a high level. The mean score was 21.16 (SD = 3.21).
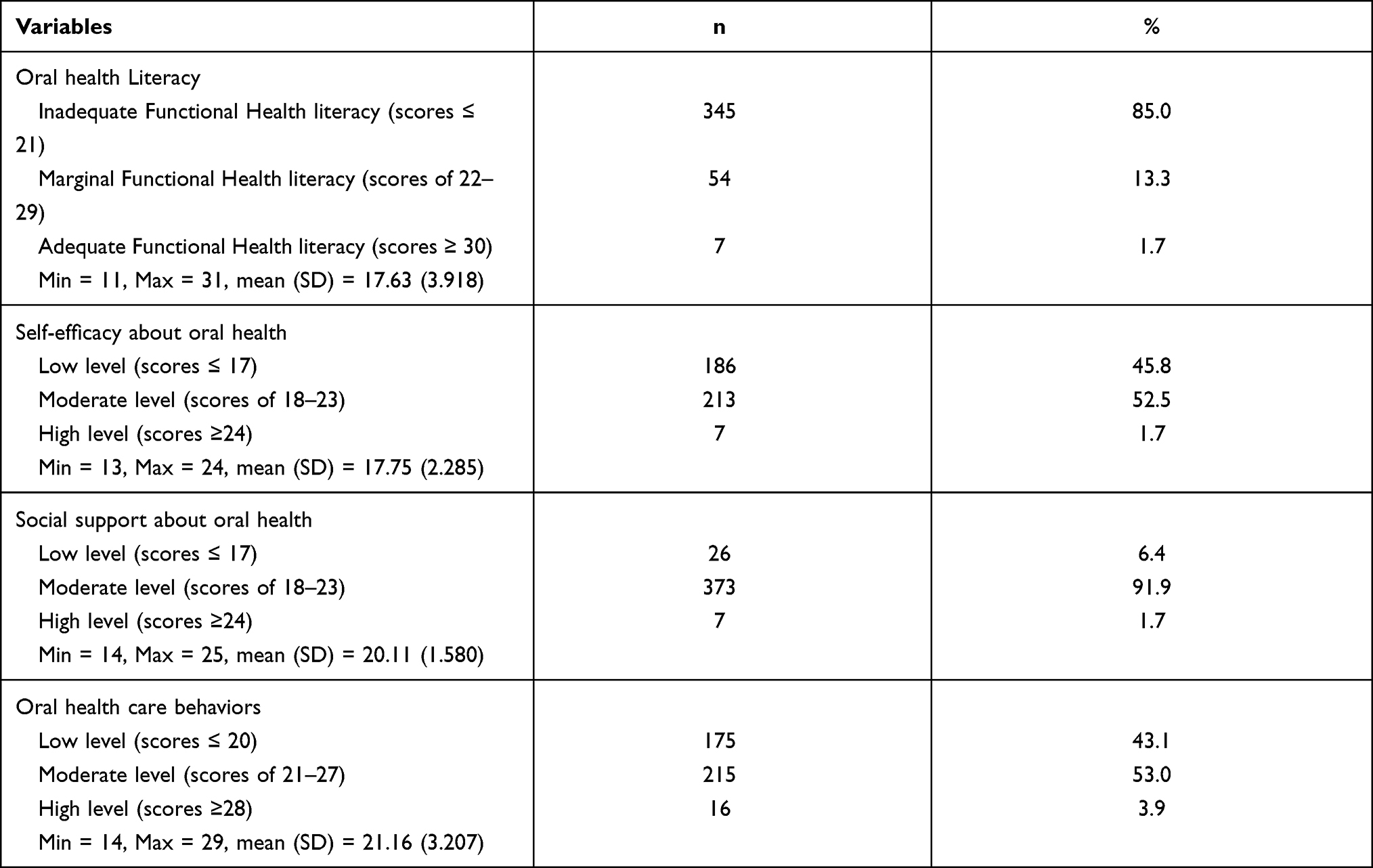 |
Table 3 Oral Health Literacy, Self-Efficacy, Social Support and Oral Health Care Behaviors of Elderly (N=406) |
Oral Health Literacy, Self-Efficacy and Social Support Associated with Oral Health Care Behaviors Among Elderly
Linear regression analysis was used to investigate factors associated with oral health care behaviors among older adults (Table 4). The results of the univariate analysis revealed that significant factors at a p-value=0.20 included gender, financial status, current disease, smoking, drinking alcohol, receiving information about oral health, oral health literacy, self-efficacy, and social support about oral health. These variables were entered into the multivariate analysis. The results from the last model showed that self-efficacy, social support, and oral health literacy, were positively associated with oral health care behaviors among the elderly (p-value<0.05). The single factor of oral health literacy can explain 40.7% of the variance in oral health care behaviors, whereas the multiple regression models can account for 47.2%.
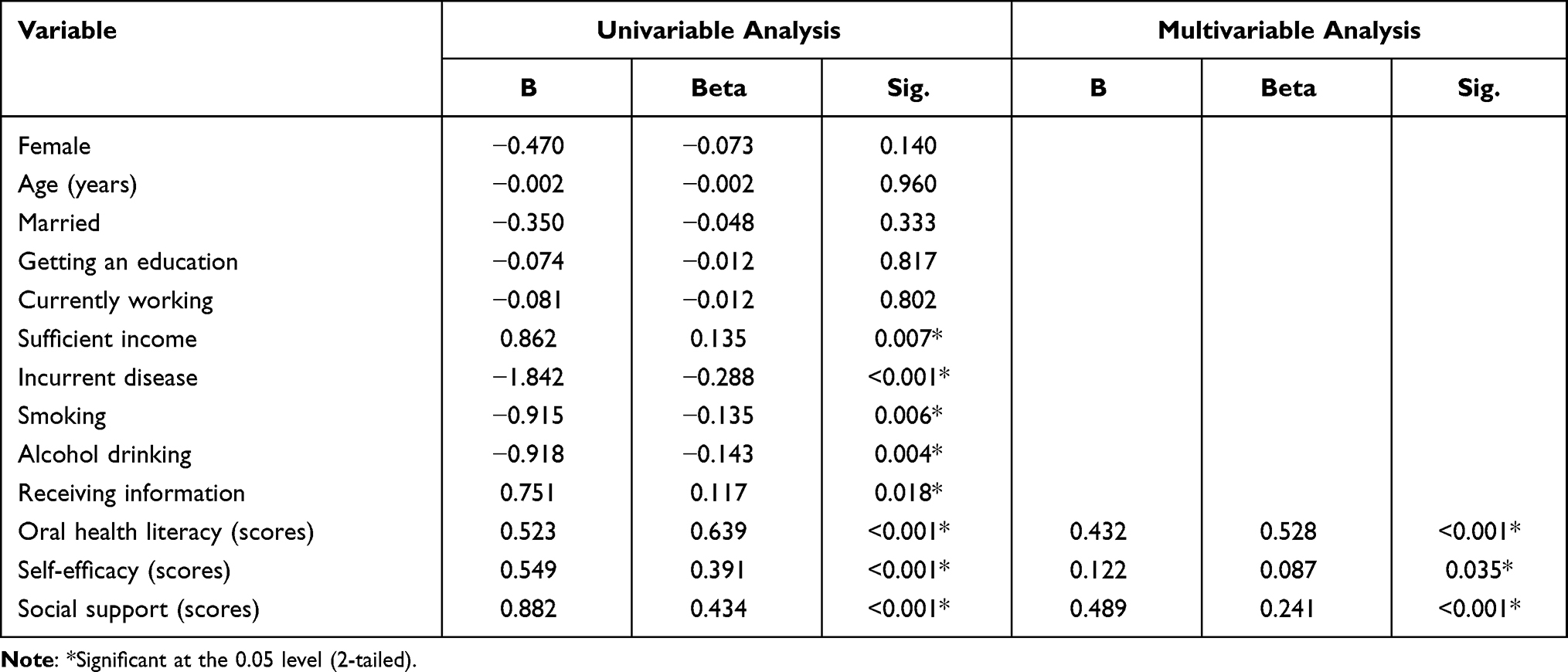 |
Table 4 Factors Associated with Oral Health Care Behaviors Among Elderly by Linear Regression (N=406) |
Discussion
The study’s findings show that there was a statistically significant association between the primary variables and oral healthcare behaviors among elderly people living in a rural area of Thailand. The majority of the elderly had scores that revealed inadequate and moderate functional health literacy, which suggests the majority of these people obtained education at a primary level. Moreover, the way they manage their health is aligned with their perceived traditional way of life. These issues limit their ability to understand and seek health information, as well as to decide on their own oral healthcare behaviors. This is consistent with a previous study, which found that elderly participants had poor oral health literacy scores because they had limited knowledge of oral health information.39 Even though health providers communicated with the elderly in their local language, their limited health literacy prevented them from understanding health information.39 One study similar to ours also found that one third of elderly people had poor health literacy regarding oral healthcare behaviors.22 It was also found that elderly people with an insufficient level of health literacy could have a decreased ability to learn and understand knowledge related to oral healthcare behaviors. As a result, they would practice self-care behaviors toward oral healthcare incorrectly; for instance, they would brush their teeth incorrectly, not use dental floss, and consume sugary food, which leads to cavities and tooth decay.39,40 Poor health literacy is one of the barriers that prevents oral health hygiene and appropriate oral healthcare practices among the elderly.40
Oral health literacy was found to be a highly significant positive predictor of oral healthcare behaviors. The results are consistent with the concept of cognitive behaviors.28 Cognitive skills have positive effects on the practice of self-healthcare behaviors,28 which is consistent with the principle of functional health literacy that demonstrates that cognitive and social skills could defines a person’s motivation and ability to understand health information.41 As a previous study reported, a positive correlation between oral health knowledge and health behaviors resulted in people implementing correct practices, such as teeth brushing skills and maintaining personal oral hygiene.39,42 Therefore, to increase cognitive skills, specific communication methods to improve the elderly’s oral hygiene should be appropriate in their context and should be easy to understand and comprehend.
Oral health literacy was found to be a highly significant positive predictor of oral healthcare behaviors. The results are consistent with the concept of cognitive behaviors.28 Cognitive skills have positive effects on the practice of self-healthcare behaviors,28 which is consistent with the principle of functional health literacy that demonstrates that cognitive and social skills could defines a person’s motivation and ability to understand health information.41 As a previous study reported, a positive correlation between oral health knowledge and health behaviors resulted in people implementing correct practices, such as teeth brushing skills and maintaining personal oral hygiene.39,42 Therefore, to increase cognitive skills, specific communication methods to improve the elderly’s oral hygiene should be appropriate in their context and should be easy to understand and comprehend.
In terms of self-efficacy toward oral healthcare behaviors, the findings of the study show that most of the elderly participants obtained moderate to poor scores on self-efficacy. Most of them had a poor perception of self-managing their healthcare, which leads to a decrease in decision making regarding their own healthcare. Self-efficacy determines a person’s behavioral expression and the trend that drives their health outcomes.43 In this study, the elderly participants had poor and moderate self-efficacy in preventing oral health problems, which resulted in inappropriate oral healthcare behaviors and an increase in oral health problems, such as tooth decay, and cavities.44 One study showed that low self-efficacy indicates poor self-assessment toward oral health and is associated with a high risk of caries and periodontal disease.44,45
In the analysis of factors, the study showed that self-efficacy was statistically significant and positively associated with oral healthcare behaviors. Consistent with previous studies, it is believed self-efficacy is a predictor of teeth brushing behaviors of the elderly. Self-efficacious elders are confident in their ability to brush their teeth regularly and believe in the results, which are called outcome-expectancy; moreover, they are able to brush their teeth successfully on their own and observe oral health hygiene. One study highlighted that people’s improved ability to manage their own oral healthcare is associated with better outcomes; for instance, improved brushing time, associated with having less plaque and bleeding, reduces the risk of long-term periodontal treatment.46,47 Therefore, encouraging elderly people to recognize the importance of self-management is one effective way of helping the individuals develop good healthcare behaviors.43 This is consistent with the concept of self-efficacy, which allows a person to achieve expected behaviors through cognitive motivation, the use of persuasive speech and emotional stimulation, and the decision-making process.28,43 This enhances the elderly’s ability to decide on or determine any behaviors that are appropriate for managing care by themselves.
In terms of social support, this study found that the majority of the elderly obtained a moderate score level. The study shows that they need help from people around them to take care of themselves. In addition, there is limited access to dental care in rural areas, and dental health information is not yet comprehensive.40 As one study mentioned, if elderly people were encouraged by social support, including receiving health information from healthcare providers and getting help from family members and information from media, it would positively impacts the elderly’s self-management of oral healthcare.44 This is consistent with a study which found that the role of social support influenced the elderly’s attitude toward oral healthcare and self-management skills.40
Social support is one of the important variables we found to be significantly positively associated with oral health behaviors.30,37 Social support consists of groups of people in society; in which individuals interact with family members, neighbors, and key persons in the community, such as health personnel and, health volunteers. Such interactions have a positive impact on individuals’ health and well-being.37,48 One study found that social support toward elders oral health behaviors is significantly associated with good behaviors on dental healthcare, wearing dentures, and other health-related behaviors among the elderly.49 This finding is consistent with the social support concept, which states that social support has a direct impact on one’s health. Social support networks enhance individuals’ ability to manage their own health by boosting confidence and increasing motivation.36,37,44
In terms of oral healthcare behaviors, we found that the majority of the elderly obtained moderate and poor scores. This group generally did not go to a health center for an annual check-up or receive an oral examination. Generally, they only visit health centers when illness occurs or they need to have a tooth extracted, false teeth made, or cleaning and polishing teeth and fillings. Their self-efficacy scores regarding oral healthcare behaviors were at a moderate level and need to be improved. Elders may experience an increase in medical expenses, which could be a barrier to visiting a health center for oral health check-ups.50 Similar to a study on oral health among the elderly, we found that oral healthcare behaviors among older people may become inappropriate due to them having developed low self-confidence and low self-efficacy in performing self-healthcare behaviors, resulting in performing inappropriate or, irregular behaviors.32,36,50 Therefore, supporting, promoting, and providing educations for the elderly on how to implement self-care behaviors on a continuous basis is important; and oral hygiene, primary oral care, and oral health knowledge among the aging population should receive attention.
When analyzing the demographic characteristics of the elderly participants, this study found that sufficient income and perceived health information had statistically significant relationships with oral healthcare behaviors. This is consistent with a previous study, which mentioned that the elderly with high incomes demonstrated better healthcare behaviors than those with low incomes; and insufficient economic status was associated with elders’ healthcare behaviors.38,50 In terms of perceived health information, it is similar to a previous study which mentioned that elders who were advised by public health workers had significantly higher oral healthcare behaviors than those who were not advised by public health workers.38,50 Our study also found that chronic health conditions, smoking, and drinking alcohol, had statistically significant relationships with oral healthcare behaviors among the elderly. This is consistent with previous studies that have shown chronic health conditions may lead to poorer oral healthcare behaviors and decreased quality of life.22,50 Moreover, smoking was significantly associated with periodontal health conditions. Smoking and drinking alcohol had negative relationships with healthcare behaviors, resulting in increased oral health problems.22,50,51 Oral healthcare should be promoted among elderly people with underlying disease so that they can manage their care properly.
This study has strengths and limitations. Many variables are being studied in this paper, including oral health literacy, self-efficacy, social support, and other demographic characteristics associated with oral healthcare behaviors of the elderly. This is the strength of this research. On the other hand, there are several limitations, which include 1) The data obtained from non-probability samplings may not be proven by the registered list in the public health center and primary care system (Java Health Center Information System: JHCIS). Therefore, the results are representative only of elderly people living in the Mae Rim District, Chiang Mai Province, Thailand. However, this study has provided critical information that can be extended to large-scale multistage studies to identify key trends for promoting policy and intervention activities. Secondly, other important factors such as health insurance rights, psychosocial factors, and social capital are not included in the data set used in the study. Thirdly, the outcome variables reported in the study are specific to oral healthcare behaviors; future studies could switch this focus to other factors, such as the (DMFT index, the number of natural teeth, or occluding pairs of teeth). Future research could consider focusing on brushing teeth skills that influence oral health status; for instance, forced brushing, the frequency of toothbrush replacement, and self-efficacy in the proper use of brushing techniques among the elderly. Other aspect of oral healthcare, such as flossing, could be studied in greater depth.
Conclusion
In conclusion, oral healthcare behavior among elderly people is an important issue within public health. Many aspects must be considered when assessing the elderly’s health, including health behaviors, health knowledge, and other related factors. In addition, oral health literacy, self-efficacy, and social support have a significant impact on the elderly’s oral healthcare behaviors. As age progresses, oral health problems among older people increase so comprehensive oral healthcare services should be made available to the elderly. Dental clinics can use health information to organize training and create key strategies for appropriate oral healthcare behaviors among elderly people living in rural areas. Therefore, accessibility to comprehensive services and policy plans should cover the areas of program activities, health campaigns, and media and public relations. Related information should be simple, understandable, and suitable for the context of elderly people living in the rural community. Moreover, family members, relatives, or other people from relevant agencies should provide social support to promote oral healthcare among elderly people and offer integrated programs, such as organizing health activities through clubs for the elderly in conjunction with family care and home visits. Also, appropriate healthcare behaviors should be included in community activities to enhance the skills of the elderly regarding self-health care management, decision-making, following medical advices from health personnel, and accessing health information.
Ethical Approval and Consent
Ethical consideration was approved by the University of Phayao Human Ethics Committee, Thailand (No. 1.3/003/64). Participants gave informed consent prior to data collection. This study was conducted in accordance with the Declaration of Helsinki, the Belmont Report, CIOMS Guideline, and International Conference on Harmonization in Good Clinical Practice (ICH-GCP).
Acknowledgments
The Health Promoting Hospitals of Health Promoting Hospitals in Baan Mai sub-district and Khon Tan sub-district, Mae Rim district, Chiang Mai province, are acknowledged. The authors also wish to thank all participants for sharing their experience in this study.
Funding
This research project was supported by the Thailand science research and innovation fund and the University of Phayao the Unit of Excellence named “Health Promotion and Quality of Life” grant number FF64-UoE009 and Unit from School of Medicine, University of Phayao.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Suraseranivong R. Oral cavity in elderly. J Charoenkrung Pracharak Hosp. 2018;14(1):87–100.
2. World Health Organization. Oral health. Available from: https://www.euro.who.int/en/health-topics/disease-prevention/oral-health.
3. Wong MF. Factors associated with knowledge, attitudes, and practices related to oral care among the elderly in Hong Kong community. Int J Environ Res Public Health. 2020;17(21):1–15. doi:10.3390/ijerph17218088
4. Bureau of Dental Health, Department of Health. Annual Report of Dental Health Performance for Working and the Elderly. Thailand: Ministry of Public Health; 2017.
5. Bureau of Dental Health, Department of Health. Dental health program for the Thai elderly. Thailand: Ministry of Public Health; 2015. Available from: https://dental.anamai.moph.go.th/oralhealth/elderly/2558/elderly_plan_2558-2563.pdf.
6. Legislative Council Secretariat (LCS). Dental care services for elderly in Hong Kong. Available from: www.legco.gov.hk/research-publications/english/1617rb02-dental-care-services-for-elderly-in-hongkong-20161220-e.pdf.
7. Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2005;33(2):81–92. doi:10.1111/j.1600-0528.2004.00219.x
8. Buaban K. The relationship between oral conditions on the quality of life in the elderly Mae Ramat district, Tak province. J Gerontol Geriatr Med. 2017;16:45–56.
9. Locker D. Concepts of oral health, disease and the quality of life. In: Measuring Oral Health and Quality of Life. Chapel Hill: University of North Carolina; 1997.
10. Fiske J, Davis DM, Frances C, Gelbier S. The emotional effects of tooth loss in edentulous people. Br Dent J. 1998;184(2):90–93. doi:10.1038/sj.bdj.4809551
11. Department of Older Persons. Statistics of the Thai elderly. Ministry of Social Development and Human Security; 2017. Available from: http://www.dop.go.th/th/know/side/1/1/275.
12. Health Data Center. Dental health report for the Thai elderly. Thailand: Ministry of Public Health; 2020. Available from: https://hdcservice.moph.go.th/hdc/main/index.php.
13. Blizniuk A, Ueno M, Zaitsu T, Kawaguchi Y. Association of oral health literacy with oral health behavior and oral health status in Belarus. Commun Dent Health. 2015;32(3):148–152.
14. Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX. Oral health knowledge, attitudes and behaviour of adults in China. Int Dent J. 2005;55(4):231–241. doi:10.1111/j.1875-595X.2005.tb00321.x
15. Li XL, Liu MY, Cheng L, Zhu HF, Shang SH, Cui D. Impact of comprehensive health education on oral care knowledge, attitude and practice in the elderly in long-term care institutions. Shanghai Kou Qiang Yi Xue. 2018;27(2):181–184.
16. Ratzan SC, Parker RM. Introduction. In: Selden CR, Zorn M, Ratzan SC, Parker RM, editors. National Library of Medicine Current Bibliographies in Medicine: Health Literacy NLM Publ. No. CBM 2000–1. Bethesda: National Institutes of Health; 2000:v–viii.
17. Baskaradoss JK. Relationship between oral health literacy and oral health status. BMC Oral Health. 2018;18(1):172. doi:10.1186/s12903-018-0640-1
18. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(Sup 2):9–19. doi:10.1080/10810730.2010.499985
19. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. doi:10.7326/0003-4819-155-2-201107190-00005
20. Horowitz AM, Kleinman DV. Oral health literacy: a pathway to reducing oral health disparities in Maryland. J Public Health Dent. 2012;72(Sup 1):S26–30. doi:10.1111/j.1752-7325.2012.00316.x
21. Baskaradoss JK. The association between oral health literacy and missed dental appointments. J Am Dent Assoc. 2016;147(11):867–874. doi:10.1016/j.adaj.2016.05.011
22. Wehmeyer MM, Corwin CL, Guthmiller JM, Lee JY. The impact of oral health literacy on periodontal health status. The impact of oral health literacy on periodontal health status. J Public Health Dent. 2014;74(1):80–87. doi:10.1111/j.1752-7325.2012.00375.x
23. Wigen TI, Skaret E, Wang NJ. Dental avoidance behaviour in parent and child as risk indicators for caries in 5-year-old children. Int J Paediatr Dent. 2009;19(6):431–437. doi:10.1111/j.1365-263X.2009.01014.x
24. Sabbahi DA, Lawrenc HP, Limeback H, Rootman I. Development and evaluation of an oral health literacy instrument for adults. Commun Dent Oral Epidemiol. 2009;37(5):451–462. doi:10.1111/j.1600-0528.2009.00490.x
25. Jittimanee P, Rodjakpai Y, Maharatchapong N. Development of an oral health literacy instrument for elderly. J Public Health Nurs. 2019;33(3):114–131.
26. Blizniuk A, Ueno M, Furukawa S, Kawaguchi Y. Evaluation of a Russian version of the oral health literacy instrument (OHLI). BMC Oral Health. 2014;14(1):1–7. doi:10.1186/1472-6831-14-141
27. Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67:2072–2078. doi:10.1016/j.socscimed.2008.09.050
28. Bandura A. Exercise of human agency through collective efficacy. Curr Dir Psychol Sci. 2000;9:75–78. doi:10.1111/1467-8721.00064
29. McCaul KD, Glasgow RE, Gustafson C. Predicting levels of preventive dental behaviors. J Am Dent Assoc. 1985;111(4):601–605. doi:10.14219/jada.archive.1985.0169
30. Dahlan R, Ghazal E, Saltaji H, Salami B, Amin M, Kamperman AM. Impact of social support on oral health among immigrants and ethnic minorities: a systematic review. PLoS One. 2019;14(6):e0218678. doi:10.1371/journal.pone.0218678
31. Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing Clinical Research: An Epidemiologic Approach.
32. Katanyutanon T, Timtong P, Sukyanudit W, et al. Association between protection motivation and oral health care behaviors among the elderly in Bangsaothong Sub-district, Bangsaothong District, Samutprakarn. HCU J. 2020;24(2):161–171.
33. Auttama N, Seangpraw K. Factors predictor health literacy among older adults with risk hypertension disease, Phayao Province. J Health Educ. 2019;42(2):75–85.
34. Chainant K, Chanthamolee S, Suwan P, Srisuphanunt M. The development of an oral health care model for older adults with chronic diseases in Rangsit City Municiplaity, Patum Thani Province. South Coll Netw J Nurs Public Health. 2018;5(1):91–107.
35. Kunawisarut S. A self-esteem affecting dental health condition of the elderly in Thaptilek sub-district, Muang district, Suphanburi province. Thai Dent Nurse J. 2016;27(2):97–109.
36. Ruangdej Chaosuansreecharoen K, Kluebklay P, Prasert L. Factors predicting dental health care behaviors among elderly in Royal Denture Project, Trang Province. South Coll Netw J Nurs Public Health. 2018;5(3):152–168.
37. Kahn RL. Aging and social support. In: Riley MW, editor. Aging from Birth to Death: Interdisciplinary Perspectives. Boulder: Westview Press; 1979:77–91.
38. Phudphong S. Factors related to oral and dental health care behaviors of the elderly in Muang Sam Sip District, Ubon Ratchathani Province. J Health Sci Boromarajajonani Coll Nurs Sunpasitthiprasong. 2020;4(1):101–119.
39. Cho HA, Im AJ, Sim YR, Jang HB, Lim HJ. The association between oral health literacy and oral health behaviors in North Korean defectors: a cross-sectional study. BMC Public Health. 2020;20(1):1074. doi:10.1186/s12889-020-08550-7
40. Kongsri S. The component of oral health literacy among elderly in Khon Kaen Province, Thailand. Thai Dent Nurse J. 2018;29(2):55–68.
41. World Health Organization. Health literacy and health promotion. Definitions, concepts and examples in the Eastern Mediterranean region. Individual empowerment conference working document.
42. Ueno M, Takeuchi S, Oshiro A, Kawaguchi Y. Relationship between oral health literacy and oral health behaviors and clinical status in Japanese adults. J Dent Sci. 2013;8(2):170–176. doi:10.1016/j.jds.2012.09.012
43. Bandura A. Self-Efficacy: The Exercise of Control. New York: W.H. Freeman and Company; 1997.
44. Suwakhon N, Wongsawat P. Factors influencing tooth cleaning behaviors for dental caries prevention of grade 6 students in Muang District, Phitsanulok Province. EAU Herit J Sci Technol. 2018;12(2):273–286.
45. Jamieson LM, Parker EJ, Roberts-Thomson KF, Lawrence HP, Broughton J. Self-efficacy and self-rated oral health among pregnant aboriginal Australian women. BMC Oral Health. 2014;14:29. doi:10.1186/1472-6831-14-29
46. Anagnostopoulos F, Buchanan H, Frousiounioti S, Niakas D, Potamianos G. Self-efficacy and oral hygiene beliefs about toothbrushing in dental patients: a model-guided study. Behav Med. 2011;37(4):132–139. doi:10.1080/08964289.2011.636770
47. Kakudate N, Morita M, Yamazaki S, Fukuhara S, Sugai M, Nagayama M. Association between self-efficacy and loss to follow-up in long-term periodontal treatment. J Clin Periodontol. 2010;37:276–282. doi:10.1111/j.1600-051X.2009.01529.x
48. House JS, Umberson D, Landis KR. Structure and processes of social support. Annu Rev Sociol. 1988;14(1):293–318. doi:10.1146/annurev.so.14.080188.001453
49. McGrath C, Bedi R. Influences of social support on the oral health of older people in Britain. J Oral Rehabil. 2002;29(10):918–922. doi:10.1046/j.1365-2842.2002.00931.x
50. Subbowon U. Oral health care behaviors among the elderly in Nakhonchaisi Sub-district, Nakhonchaisi District, Nakhon Pathom. Region 4–5 Med J. 2019;38(4):244–255.
51. Cervino G, Fiorillo L, Cervino G, et al. Oral health impact profile in celiac patients: analysis of recent findings in a literature review. Gastroenterol Res Pract. 2018;2018:1–9. doi:10.1155/2018/7848735
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.