Back to Journals » International Journal of Women's Health » Volume 7
Factors associated with four or more antenatal care services among pregnant women: a cross-sectional survey in eight South Central Coast provinces of Vietnam
Authors Ha B, Tac P, Duc D, Duong D ![]() , Thi L
, Thi L
Received 24 April 2015
Accepted for publication 12 May 2015
Published 16 July 2015 Volume 2015:7 Pages 699—706
DOI https://doi.org/10.2147/IJWH.S87276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Bui TT Ha,1 Pham V Tac,2 Duong M Duc,1,3 Doan TT Duong,1 Le M Thi1
1Department of Reproductive Health, Hanoi School of Public Health, 2Department of Personnel and Organization, Ministry of Health, Ba Dinh, Ha Noi, Vietnam; 3International Maternal and Child Health (IMCH), Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden
Background: In Vietnam, four or more antenatal care (ANC4+) visits/services among pregnant women have not been officially reported in the health system. Moreover, the factors associated with the use of ANC4+ services have not been studied in previous studies. In this study, we conducted an exploratory analysis to identify the rate of utilization of ANC4+ services and factors associated with use of ANC4+ services among pregnant women in rural areas of Vietnam.
Methods: The study was conducted in eight provinces in the South Central Coast region of Vietnam between August 2013 and May 2014. A total of 907 women, who delivered in the past 1 year, participated in the study. Multivariate logistic regression model was used to examine the association between all potential factors and utilization of ANC4+ services.
Results: The rate of utilization of ANC4+ services by women in eight South Central Coast provinces was 53.9%. Factors negatively associated with using ANC4+ services were belonging to ethnic minority groups having lower education, doing informal works, having lower income, having lower knowledge on ANC4+ services, and receiving no financial support from the husband. In particular, financial support from the husband was considered important in improving the use of ANC4+ services by women in rural areas.
Conclusion: The study asserted an inadequacy for ANC4+ utilization and can contribute to missed opportunities to achieve better maternal outcomes for women in rural areas of Vietnam. The necessity of introducing ANC4+ services in the national guidelines on maternal health care should be disseminated to health policy-makers. Strategies to increase ANC4+ utilization should focus on knowledge improvement and on poor, low-income, and ethnic minority women.
Keywords: pregnant women, antenatal care services, ethnic minority, male involvement, South Central Coast provinces, Vietnam
Background
Antenatal care (ANC) services for pregnant women by skilled health providers improve maternal and child health outcomes.1 It is one of the most important interventions in combating maternal and newborn mortality and in achieving the Millennium Development Goals 4 and 5.2 Women attending ANC visits should receive sufficient evidence-based clinical interventions, such as tetanus toxoid immunization, deworming, iron and folic acid supplements, counseling on maternal health, and birth and emergency preparedness.3 Attending ANC visits by skilled health providers are associated with an increase in institutional deliveries and use of postnatal services.1,4 The World Health Organization recommends all women with uncomplicated pregnancies to attend four or more ANC (ANC4+) visits/services at fourth, sixth, seventh, eighth, and ninth month of pregnancy.5 Attending three or less ANC visits in uncomplicated pregnancies increases perinatal mortality in low- and middle-income countries.6,7 Having ANC4+ services among pregnant women has been widely used as a global benchmark, referring as adequacy of ANC.5
The recommended number of ANC visits/services varies between countries and is often higher in high-income countries. In Norway, a basic program of eight visits is recommended by the 40th week of pregnancy.8 In Vietnam, the National Reproductive Health Guideline recommends at least three ANC visits for uncomplicated pregnancies, one in each trimester with adequate services during each visit.9 Very recently, since September 2014, the ANC4+ services was added to the health information system in Vietnam as an official indicator.10
ANC services are recognized to be underutilized in developing countries.11,12 Although most of women (88%) have at least one ANC visit, only 55% receive the recommended ANC4+ services.13 In Vietnam, the proportion of pregnant woman having ANC4+ services has significantly increased from 29% in 200214 to more than 70% in 2014.15 To date, Vietnam has achieved the Millennium Development Goal 5 on reducing maternal mortality.16 Evidence, however, points to growing disparities in the utilization of antenatal services in recent years between disadvantaged and privileged women groups.17–19 Disadvantaged women are less likely to have access to safe, affordable, and acceptable antenatal services, which lead to higher rates of both maternal morbidity and mortality.
Studies were conducted to examine factors associated with the use of ANC services in Vietnam.18,20 Low maternal education, poverty, and ethnic minority status are commonly reported as the most important factors for the less use of ANC services.18,20,21 The associated factors to having ANC4+ services, to our knowledge, have not been studied in any previous studies in Vietnam. The objectives of this study are therefore to identify the rate of utilization of ANC4+ services among the pregnant women and factors that are associated with the ANC4+ services in rural areas of Vietnam.
Methods
Study setting and population
A cross-sectional household survey was conducted in the South Central Coast region of Vietnam between August 2013 and May 2014. The South Central Coast region in Vietnam encompasses a combination of eight mountainous and coastal provinces. Out of the total population of 8.93 million, a majority of Vietnamese (Kinh) people live in mainland, while most of the minority ethnic groups live in the mountainous part.
Two districts in each province representing the coastal and mountainous districts were purposively selected (n=16). In each district, two communes were randomly selected (n=32). The target population included all mothers who delivered in the past 1 year. Approximately 30 women who delivered in the past 1 year before the date of interview were systematically selected in each commune based on the lists provided by commune health centers (CHCs). A total of 907 respondents participated in this study.
Data collection
Semi-structured questionnaires were used to gather data from women, who delivered in the past 1 year before the date of interview, to identify the coverage of ANC4+ services and its associated factors of sociodemographic characteristics, social determinants, sex equality, and husband’s involvement in ANC services.
For 3 months (September–November) in 2014, trained interviewers (researchers from Hanoi School of Public Health) visited households and administered questionnaires in all eight provinces. If a selected mother could not speak Vietnamese, a village health worker helped to translate for the interviewers.
Statistical analysis
Data were entered using EpiData and double-checked before analyzing using SPSS for Windows Version 16 statistical package (SPSS, Inc., Chicago, IL, USA). Proportion for all factors were compared between different categories of ANC visits (0, 1–3, and 4+) using χ2 test of independence. This χ2 test tested the null hypothesis that the number of ANC visit is independent of the contributing factors, such as ethnicity and occupation.22 When the expected values in any of the cells of a contingency table are below 5, Fisher’s exact test was calculated as it is more accurate than the χ2 test in this situation.22 Univariate and multivariate logistic regression analyses (stepwise backward likelihood ratio method) were conducted to analyze factors associated with having ANC4+ services. The independent variables were sociodemographic, social determinant, sex equality, and male involvement. Confidence interval (CI) of 95% was calculated, and P<0.05 was considered statistically significant.
Ethical consideration
Ethical clearance was obtained from the institutional review board of Hanoi School of Public Health. Ethical guidelines were followed, and participants were recruited after obtaining a written informed consent.
Results
Basic characteristics of the study population
Socio-demographic characteristics
A total of 907 mothers with children younger than 1 year participated in the study. The majority (80.6%) were aged between 20 and 34 years. More than half (68.5%) belonged to the nonethnic group. More mothers were living in mountainous areas than in coastal areas. More than half (66.5%) had secondary or higher education, and among them, most (83.1%) were doing informal works (housework or self-employed). Nearly half of the women classified themselves in poor or near-poor group. Most of them (88.1%) were living close to the CHC (within 5 km) (Table 1).
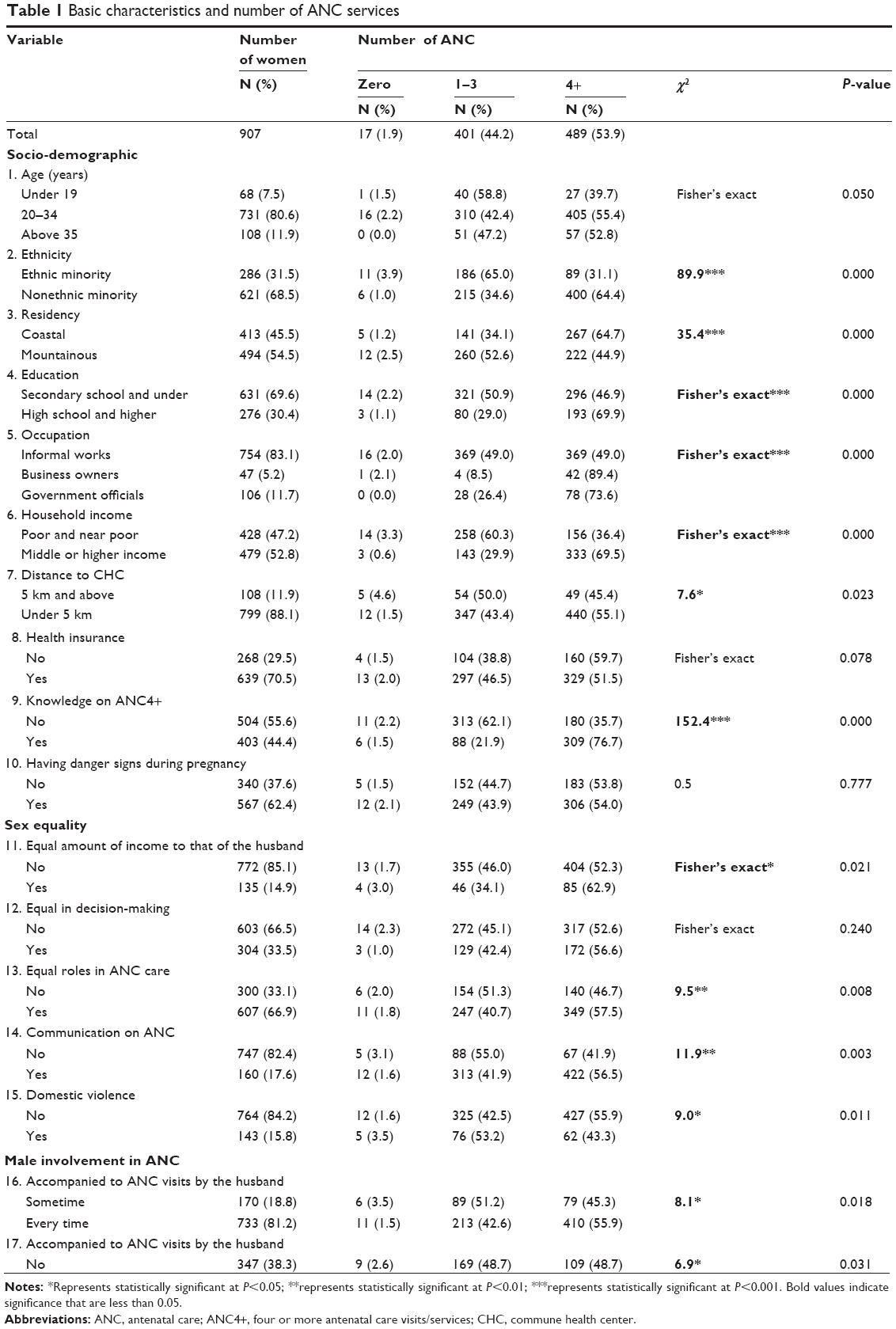 | Table 1 Basic characteristics and number of ANC services |
Sex equality
A majority of the women (85.1%) had unequal income compared to their husbands. Likewise, two-third of women (66.5%) were not equal to their husbands in decision-making. There was also almost no communication between husbands and wives regarding ANC. However, two-third (66.9%) of women perceived equal roles of men and women in ANC (Table 1). Few husbands accompanied their wives to all ANC visits, and only one-third of them provided financial support to their wives during pregnancy (Table 1). At the bivariate level, several basic characteristics of the women had significant differences to the use of ANC. For instance, women with higher income were more likely to utilize the recommended ANC4+ services compared with those with lower income (68.1% vs 30.9%).
Having ANC4+ services
Out of 907 women who were involved in the study, 408 (46.1%) had zero or one to three ANC visits, whereas 489 (53.9%) had ANC4+ services. There were significant relationships between ANC visits and ethnicity, residency, education, occupation, household income, distance to CHC, knowledge on ANC4+, having equal amount of income to that of the husband, perceived equal roles in ANC, couple communication on ANC, experiencing domestic violence, being accompanied to ANC visits by the husband, and receiving financial supports from the husband during pregnancy (P<0.05) (Table 1). Women, who attended ANC4+ services, were more likely to be in the nonethnic group, live in coastal region, have higher education, have a business or be a government official, have better off income, have better knowledge on ANC, have equal amount of income to that of the husband, have perceived equal roles in ANC care, have couple communication on ANC, have not experienced domestic violence, be accompanied frequently to ANC by their husbands, and receive financial support from the husband during pregnancy ( Table 2).
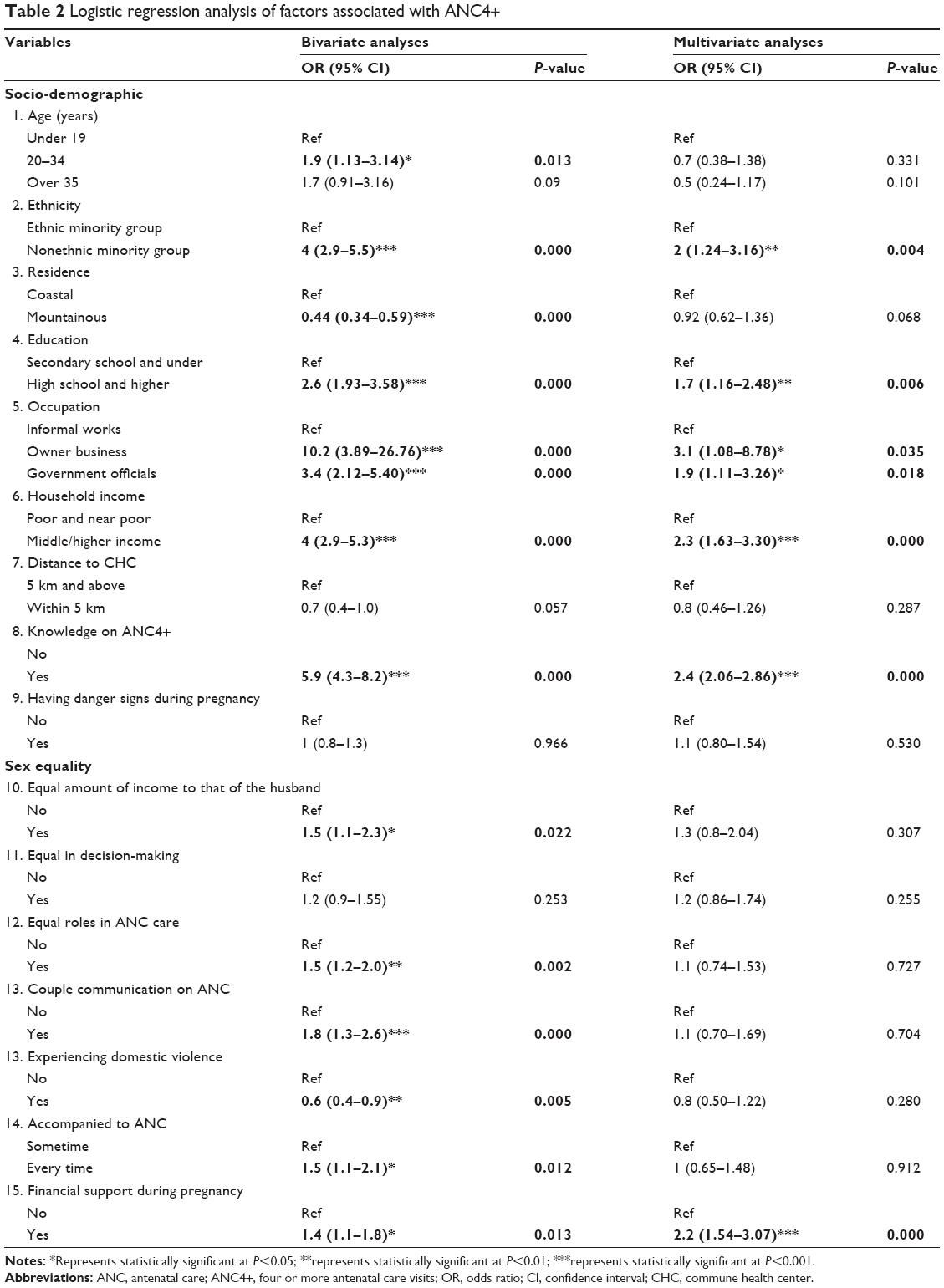 | Table 2 Logistic regression analysis of factors associated with ANC4+ |
Factors associated with having ANC4+ services
The multivariate analyses adjusted for all factors were included in the final model (Table 2). Age, residency, distance to the CHC, having danger signs during pregnancy, having equal amount of income to that of their husbands, perceived equal roles in decision-making, perceived equal roles in ANC, having couple communication on ANC, experiencing domestic violence, and being accompanied to ANC by their husbands were not significantly associated with ANC4+. The remaining variables, ethnicity, education, occupation, household income, knowledge on ANC4+, and financial support from the husband, were significantly associated with ANC (P<0.05). Nonethnic women were two times more likely to have ANC4+ services than those of ethnic origin (adjusted odds ratio [aOR] =2.0, CI =1.24–3.16). Women with higher education were 1.7 times more likely to have ANC4+ services than those with lower education (aOR =1.7, CI =1.16–2.48). Women who were having formal job (business owners or government officials) were more likely to have ANC4+ services than those having informal job. Women with high income were 2.3 times more likely to have ANC4+ services than those in poor or near-poor group (aOR =2.3, CI =1.63–3.3). Women who had better knowledge on ANC were 2.4 times more likely to have ANC4+ services than those with poor knowledge (aOR =2.4, CI =2.06–2.86). Women who received financial support from their husbands were 2.2 times more likely to have ANC4+ services than those who did not receive financial support (aOR =2.2, CI =1.54–3.07) (Table 2).
Discussion
In this study, we have analyzed the proportion of women having ANC4+ services and the association between having ANC4+ services and other determinants of health. Our findings demonstrated that nearly one-half of the women in rural areas did not have ANC4+ services. This inadequacy for ANC can contribute to missed opportunities to achieve better maternal outcomes. Having ANC4+ services was significantly associated with ethnicity, education, occupation, household income, knowledge on ANC4+, and the financial support from the husband.
Proportion of having ANC4+ services
ANC4+ visit is a programmatically useful indicator to point out how services are utilized by pregnant women.23 In our study and other previous studies, the research on ANC+ services asserted an observed trend of increasing rate of utilization of ANC4+ services in Vietnam. The rate of utilization of ANC4+ services increased from 11% in 199914 to 30% in 2002,24 to 59.6% in 2010,25 and to 73.7% in 2014.15 Compared to other countries, it can be seen that the rate of utilization of ANC4+ services in Vietnam is higher than that in other developing countries (52%), but lower than that in Southeast Asian countries (80%) in 2012.26 This could be due to the economic growth and better investment and awareness on maternal and child health care in the past 3 decades.27
Our study presented a general picture of current situation and the associated factors with having ANC4+ services in eight coastal provinces in Vietnam. Compared to national level, the rate of utilization of ANC4+ services in our study was much lower (59.6%) in 2010 and in 2014 (73.7%). In Vietnam, only recently, the Ministry of Health introduced the ANC4+ services indicator in the maternal health program, and women might not be aware of this program. This could be a reason for the low rate of utilization of ANC4+ services in our study. Moreover, women in rural and mountainous areas often have many disadvantages, including low quality of health services. Other studies asserted the low percentage of women who have received antenatal health education during ANC visits.20,28 They tend to seek for ANC services in private clinics, although these clinics have higher cost than that in the public clinics.20 Women tend to seek services, such as ultrasound examination, that are not widely provided in all CHCs.28 Owing to the high out-of-pocket payment, they would have fewer visits at private clinics than they could have received in the public clinics. Therefore, to improve utilization of ANC4+ services in the rural areas, the quality of care in public centers should be improved in parallel with the education program to improve the awareness of using ANC services in public primary health-care facilities.
Factors associated with having ANC4+ services
Six factors were positively associated with the utilization of ANC4+ services: mothers with better education, with formal job (business or officials), with better off economic conditions, of nonethnic origin, having more knowledge on ANC, and receiving financial support from their husbands were more likely to have ANC4+ services. Consistent with other studies, mothers having lower education level often have lower income and have less knowledge on ANC services.21,28 These women often face difficulties, including intellectual and financial disadvantages, to get access to ANC services.21,28 Sufficient knowledge on the necessity of ANC services and the complications occurring during pregnancy could increase the accessibility to ANC services.29 Notably, in our study, many women with high-risk pregnancy did not have higher rate of utilization of ANC4+ services than that of low-risk pregnant women. The explanation is likely to be that high-risk pregnant women do not recognize these risks.28
Consistent with our findings about occupation, a previous study points out that informal working women (housework or self-employed) are underutilizing ANC services.30 These women do not have health insurance, and this may be one of the reasons that they hesitate to seek ANC.30 Although Vietnamese government has the policy to expand health insurance for the poor and near-poor groups,27 the utilization of health services is still low in the highland and difficult regions due to several reasons, including geographical, transport, and financial barriers.27,31 Therefore, there was a need to improve the universal health coverage for informal groups, especially in difficult regions, including coastal and mountainous areas.
Mothers of nonethnic origins were likely to have higher rate of utilization of ANC4+ services than those of ethnic origins. Despite the overall improvement in the use of maternal health care, the disparity among the ethnic and nonethnic origins is growing in Vietnam.17,32 Ethnic minority women, who live in remote and mountainous areas, tend to have lower income, lower education,33 and less knowledge on maternal health care. They have the following difficulties: fewer physical assets, longer travel distance, lack of transportation, and high indirect costs of seeking and utilizing health-care services.34 Although there are many policies to support the most difficult districts and communes, there exist many challenges such as poor accessibility and acceptability of services.27 Thus, programs with specific strategies for ethnic women in hard-to-reach areas, such as the mobile health communication and services,35 should be considered.
In Vietnam, with Confucius influence, men are expected to be the decision-maker in the family.36 Pregnancy and delivery are considered as female matters. Men are often not expected to accompany their wives ANC visit. Moreover, men in decision-making position were found to be associated with low utilization of ANC and more home-based deliveries in other studies.37,38 This could be explained why our sex equality variables, such as equal amount of income to that of husband and equal in decision-making position, were not reported as significant factors to ANC4+ services in our study.
Women who received financial support from their husband were more likely to have higher ANC4+ services. This finding is consistent with other studies in Vietnam and other developing countries, which identified the importance of male involvement in reproductive health care for women.30,39,40 The 1994 International Conference on Population and Development pointed that men’s involvement in the improvement of reproductive health outcomes is crucial as without their engagement, change would be very difficult or impossible. Male involvement should be included in all frameworks and plans for improving women’s reproductive health.39 Men could be involved as clients, as partners, and as agents of positive changes in reproductive health care.41 However, there is no one-size-fits-all strategy to involve men in reproductive health programs.42 Programs that intend to incorporate male involvement should aim for adequate involvement with specific measures.41 Thus, programs should be evaluated based on the sex dynamics, how decisions are made and implemented, and the changing needs of both sexes and their interaction.
Methodological considerations
This study was conducted with a large sample size, which was adequate to gain general estimates of having ANC4+ visits/services and its associated factors. With a cluster sampling strategy for data collection in eight South Central Coast provinces, the studied subjects were expected to be reasonably representative of not only South Central Coast region but also rural areas in Vietnam. All associated factors were taken in compliance with the theoretical framework.
This study also has limitations. The data were collected by interviewing mother who delivered within 1 year, which could be prone to recall biases. Some of the ethnic minority respondents, Vietnamese, may not fully understand some of the questions. There could have been some socially desirable responses, especially questions related to the equality in decision-making and sex equality. To accommodate this, interviews were conducted confidentially, in the absence of spouses, to avoid biased responses.
Conclusion
The study asserted the low ANC4+ services among pregnant women in eight South Central Coast provinces. It was found that having ANC4+ services was negatively associated with lower education, having informal job (simple work or unemployed), lower economic conditions, belonging to ethnic minority group, having less knowledge on ANC, and receiving no financial support from the husband. There was a demand on concerted efforts from all relevant stakeholders to improve socioeconomic conditions in the difficult regions, targeting ethnic minority people, to reduce the existing disparity in the use of ANC4+ services.
Acknowledgments
This study was completed with financial support by grants from Asian Development Bank and Vietnam Ministry of Health. We are grateful to all other field workers and pregnant women in the eight South Central Coast provinces of Vietnam for their contributions to data collection and participation.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Campbell OM, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368(9543):1284–1299. | ||
World Health Organization. Standards for Maternal and Neonatal Care. Provision of Effective Antenatal Care. Geneva: World Health Organization; 2006. | ||
World Health Organization. Pregnancy, Childbirth, Postpartum and Newborn Care – A Guide for Essential Practice. Geneva: World Health Organization; 2009. | ||
Chakraborty N, Islam MA, Chowdhury RI, Bari W. Utilisation of postnatal care in Bangladesh: evidence from a longitudinal study. Health Soc Care Community. 2002;10(6):492–502. | ||
World Health Organization. Antenatal Care; 2015. Available from: http://www.who.int/gho/maternal_health/reproductive_health/antenatal_care_text/en/. Accessed January 15, 2014. | ||
Ayoola AB. Reducing the number of antenatal care visits in low-risk pregnancies increases perinatal mortality in low- and middle-income countries; women in all settings prefer the standard visit schedule. Evid Based Nurs. 2011;14(2):55–56. | ||
Dowswell T, Carroli G, Duley L, et al. Alternative versus standard packages of antenatal care for low-risk pregnancy. Cochrane Database Syst Rev. 2010;10:CD000934. | ||
Directorate for Health and Social Affairs Norway a National Clinical Guideline for Antenatal Care. Short Version; 2005. | ||
Vietnam Ministry of Health. National Guidelines on Reproductive Health Care Services (4620/QD-BYT). Hanoi: Vietnam Ministry of Health; 2009. | ||
Vietnam Ministry of Health. Circular on Promulgation of Health Statistic Indicators at Commune, District, and Provincial Levels (32/2014/TT-BYT); 2014. | ||
Pallikadavath S, Foss M, Stones RW. Antenatal care: provision and inequality in rural north India. Soc Sci Med. 2004;59(6):1147–1158. | ||
Magadi MA, Madise NJ, Rodrigues RN. Frequency and timing of antenatal care in Kenya: explaining the variations between women of different communities. Soc Sci Med. 2000;51(4):551–561. | ||
World Health Organization, United Nations Children’s Fund. Building a Future for Women and Children – The 2012 Report. Geneva: World Health Organization; 2012. | ||
Trinh LT, Michael John D, Byles J. Antenatal care adequacy in three provinces of Vietnam: Long An, Ben Tre, and Quang Ngai. Public Health Rep. 2006;121(4):468–475. | ||
General Statistic Office of Vietnam, UNICEF. Viet Nam Multiple Indicator Cluster Survey 2014. Geneva: World Health Organization; 2015. | ||
World Health Organization, United Nations Children’s Fund, United Nations Population Fund, World Bank. Trends in Maternal Mortality: 1990–2010. Geneva: World Health Organization; 2012. | ||
Malqvist M, Lincetto O, Du NH, Burgess C, Hoa DT. Maternal health care utilization in Viet Nam: increasing ethnic inequity. Bull World Health Organ. 2013;91(4):254–261. | ||
Malqvist M, Hoa DT, Thomsen S. Causes and determinants of inequity in maternal and child health in Vietnam. BMC Public Health. 2012;12(1):641. | ||
Finlayson K, Downe S. Why Do Women Not Use Antenatal Services in Low- and Middle-Income Countries? A Meta-Synthesis of Qualitative Studies. PLoS Med. 2013;10(1):e1001373. | ||
Tran TK, Nguyen CT, Nguyen HD, et al. Urban – rural disparities in antenatal care utilization: a study of two cohorts of pregnant women in Vietnam. BMC Health Serv Res. 2011;11(1):120. | ||
Trinh LT, Dibley MJ, Byles J. Determinants of antenatal care utilization in three rural areas of Vietnam. Public Health Nurs. 2007;24(4):300–310. | ||
McDonald JH. Handbook of Biological Statistics. Vol 2. Baltimore, MD: Sparky House Publishing; 2009. | ||
World Health Organization. Pregnancy, Childbirth, Postpartum, and Newborn Care: A Guide for Essential Practice. Geneva: World Health Organization; 2003. | ||
General Statistic Office of Vietnam. Vietnam Demographic and Health Survey 2002. Hanoi: General Statistic Office of Vietnam; 2003. | ||
General Statistic Office of Vietnam, UNICEF. Viet Nam Multiple Indicator Cluster Survey 2010–2011. Geneva: World Health Organization; 2011. | ||
United Nations. The Millennium Development Goals Report 2014; 2015. Available from: http://www.un.org/millenniumgoals/2014%20MDG%20report/MDG%202014%20English%20web.pdf. Accessed March 20, 2015. | ||
Vietnam Ministry of Health, Health Partnership Group. Joint Annual Health Review 2013: Towards Universal Health Coverage. Hanoi: Vietnam Medical Publishing House; 2013. | ||
Tran TK, Gottvall K, Nguyen HD, Ascher H, Petzold M. Factors associated with antenatal care adequacy in rural and urban contexts-results from two health and demographic surveillance sites in Vietnam. BMC Health Serv Res. 2012;12:40. | ||
Gupta S, Yamada G, Mpembeni R, et al. Factors associated with four or more antenatal care visits and its decline among pregnant women in Tanzania between 1999 and 2010. PLoS One. 2014;9(7):e101893. | ||
Graner S, Mogren I, Duong le Q, Krantz G, Klingberg-Allvin M. Maternal health care professionals’ perspectives on the provision and use of antenatal and delivery care: a qualitative descriptive study in rural Vietnam. BMC Public Health. 2010;10:608. | ||
Lofgren C, Thanh NX, Chuc NT, Emmelin A, Lindholm L. People’s willingness to pay for health insurance in rural Vietnam. Cost Eff Resour Alloc. 2008;6:16. | ||
Goland E, Hoa DT, Malqvist M. Inequity in maternal health care utilization in Vietnam. Int J Equity Health. 2012;11:24. | ||
General Statistic Office of Vietnam. The 1/4/2013 Time-Point Population Change and Family Planning Survey: Major Findings. Hanoi: General Statistic Office of Vietnam; 2013. | ||
World Bank. Country Social Analysis: Ethnicity and Social Development in Vietnam. Summary Report. Washington, DC: World Bank; 2009. | ||
Le H, Luong T, Velden TD, Le B. mHealth: an effective education channel for hard-to-reach ethnic minority populations in Vietnam. J Mob Technol Med. 2012;1(4S):17. | ||
Pham BN, Hall W, Hill PS, Rao C. Analysis of socio-political and health practices influencing sex ratio at birth in Viet Nam. Reprod Health Matters. 2008;16(32):176–184. | ||
Hou X, Ma N. The effect of women’s decision-making power on maternal health services uptake: evidence from Pakistan. Health Policy Plan. 2013;28(2):176–184. | ||
Mrisho M, Schellenberg JA, Mushi AK, et al. Factors affecting home delivery in rural Tanzania. Trop Med Int Health. 2007;12(7):862–872. | ||
Pachauri S. Male involvement in reproductive health care. J Indian Med Assoc. 2001;99(3):138–141. | ||
Ha BT, Jayasuriya R, Owen N. Male involvement in family planning in rural Vietnam: an application of the transtheoretical model. Health Educ Res. 2003;18(2):171–180. | ||
Greene ME, Mehta M, Pulerwitz J, Wulf D, Bankole A, Singh S. Involving Men in Reproductive Health: Contributions to Development. United Nations; 2006. | ||
Sternberg P, Hubley J. Evaluating men’s involvement as a strategy in sexual and reproductive health promotion. Health Promot Int. 2004;19(3):389–396. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.