Back to Journals » Psychology Research and Behavior Management » Volume 15
Factors Associated with Depressive Symptoms in Elderly Individuals Living in Urban Communities
Authors Naviganuntana Y, Kerdcharoen N ![]() , Rawdaree P
, Rawdaree P
Received 28 November 2021
Accepted for publication 27 March 2022
Published 8 April 2022 Volume 2022:15 Pages 855—864
DOI https://doi.org/10.2147/PRBM.S348782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yingrat Naviganuntana,1 Nitchawan Kerdcharoen,1 Petch Rawdaree2
1Department of Psychiatry, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Internal Medicine, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand
Correspondence: Nitchawan Kerdcharoen, Department of Psychiatry, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, 10300, Thailand, Tel +66-2-24-3186, Email [email protected]
Background: Depression is one of the most significant mental illnesses in the elderly population. Societal and economic changes in the social structure, particularly in urban communities, have led to a tendency toward depression in the elderly. Therefore, understanding the factors associated with depression among the elderly living in urban areas in Thailand is important to prevent and mitigate depression.
Objective: To investigate the proportion of depression and its associated factors in the elderly living in Bangkok.
Materials and Methods: This was a cross-sectional descriptive study with a sample size of 888 people living in Thai urban communities, including those in slum, urban, suburban, and high-rise building areas. A two-parts questionnaire was used: 1) the Thai Geriatric Depression Scale (TGDS) to assess depression and 2) associated factors.
Results: The overall percentage of depression in the sample population was 7.3%, and the proportion of depression was associated with community density (p = 0.031). The factors significantly associated with depression in the elderly included anxiety about an underlying disease [adjusted odds ratio (AOR) = 7.51; 95% CI 3.47– 16.27], family conflict (AOR = 6.30; 95% CI 1.34– 29.55), family history of psychiatric illness (AOR = 5.78; 95% CI 2.35– 14.21), financial problems (AOR = 3.81; 95% CI 2.08– 6.98), living separately from a spouse (AOR = 3.31; 95% CI 1.22– 8.98), and less or no activity participation (AOR = 3.09; 95% CI 1.32– 7.26 and AOR = 3.02; 95% CI 1.29– 7.09).
Conclusion: To mitigate depression in the elderly, attention should be given to any underlying medical disease. The community also should promote more activities accessible to the elderly, especially income-earning activities. These activities might promote better relationships or ease conflict among elderly and other family members.
Keywords: elderly, depression, urban, Bangkok
Introduction
Depression is a significant mental illness in the elderly population because the prevalence of physical, mental, and societal deterioration increases with old age and leads to fewer interactions with other people and the surrounding environment. Consequently, some elderly individuals feel worthless and lonely, which often results in depression.1,2 International studies on mental illnesses and conditions have found that 10% to 15% of the elderly in England were depressed, 12.6% in the United States, and 19.47% in other western countries.3–5 In Thailand, based on studies conducted over the past 30 years, the prevalence of depression in the elderly ranged from 17.5% to 82.3% in all communities, 19.9% to 80.3% in urban areas, and 17.0% to 84.8% in rural areas.6 According to surveys on depression in the elderly living in Bangkok, the prevalence of depression was 38% in 1992, 35.1% in 1998, and 12.78% in 2001, percentages that were similar to the 14% found in a study on the prevalence of depression in Thai elderly.7–10 However, a study by Charernboon et al that focused on 15 elderly clubs in Bangkok in 2010, the prevalence of depression was only 7.7%.11 Notably, the prevalence rate of depression in each study varied over time and with different elderly groups, measurements, social structures, and other factors. Moreover, depression in the elderly can be triggered by several associated factors, including biological factors (eg, heredity, abnormal neurotransmitter, health issues, physical diseases, medication and drug reliance, smoking, and alcohol consumption), personal factors (eg, age, sex, marital status, educational level, literacy, ability to use social media), economic factors (eg, income, income sufficiency), and social factors (eg, residential condition, family relationship, group membership).12,13
In recent years, the mean age of the population of Thailand has been increasing, particularly in Bangkok. The lifestyles of the elderly have changed, and they tend to live independently or with their spouse rather than with their children as in the past. Social livelihoods have also changed with a higher proportion of dependency than in the past. Since the socioeconomic factors have changed over the last 10 years, the current prevalence and factors related to depression in the elderly may be different from those found in earlier research.14 Therefore, the study aim was to identify the factors associated with depression in elderly individuals living in the urban areas of Thailand.
Materials and Methods
This was a cross-sectional descriptive study conducted in communities living in slum, urban, suburban, and high-rise building areas in Bangkok. The sample size for a p value of 0.5 (alpha = 0.05) and power of 0.8 was required to be 1086. The stratified random sampling method was used for all elderly populations living in each area. The numbers of elderly subjects from slum, urban, suburban, and high-rise building areas were 430, 432, 108, and 116, respectively. We obtained approval from the Ethics Committee of the Faculty of Medicine. Vajira Hospital (COA 104/2017). This study was conducted in accordance with the Declaration of Helsinki.
The subjects were recruited between January to March 2018 by Thai Health Volunteers of each community using a purposive convenient method. The inclusion criteria were individuals aged > 60 years, residing in Bangkok for ≥ 1 year, capable of perceiving and understanding the Thai language. Elderly individuals for whom communication was difficult for any reason were also excluded. Individuals who met the criteria provided written informed consent for participation in the study.
Data were collected from administration of a questionnaire consisting of two parts: 1) A questionnaire on factors associated with depression was specifically designed on the basis of a literature review. 2) The Thai Geriatric Depression Scale (TGDS) was used to measure depression. The questionnaire was developed by the Train the Brain Forum Thailand and has been used in numerous studies on geriatric depression in Thai communities, with a Cronbach’s alpha coefficient equal to 0.93.15 The questionnaire consisted of 30 self-rated items. The presence and severity of depression were assessed according to the following scores: 0–12 points indicated no depression; 13–18 points indicated mild depression; 19–24 points indicated moderate depression, and 25–30 points indicated severe depression.
Data were analyzed using IBM SPSS Statistics for Windows, Version 22.0, IBM Corp., Armonk, NY. Descriptive data are presented as frequency, percentage, average, and standard deviation. The factors associated with depression were analyzed by performing the Chi-square test. Significant factors from the theoretical review and univariate analysis were entered into multiple logistic regression models to identify significant factors associated with depression (odds ratio and 95% confidence interval [CI]). Statistical significance was accepted for p-values <0.05.
Results
Among the 1086 individuals sampled from the population, 992 elderly individuals participated in the research study in total, of which 888 (81.8% of the initially calculated sample group) completed the entire questionnaire. The overall prevalence of depression was 7.3%, with a higher prevalence in women than in men (8.1% and 5.4%, respectively). Table 1 shows that 5.5% of the participants had mild depression, 1.8% had moderate depression, and 0% had severe depression. The type of community was significantly associated with the prevalence of depression (p = 0.031). The prevalence of depression in the elderly living in suburban, slum, urban, and high-rise building areas were 10.4%, 8.3%, 7.3%, and 1.7%, respectively. The highest prevalence of mild depression (8.7%) was in suburban areas, and the highest prevalence of moderate depression (2.4%) was in slum areas.
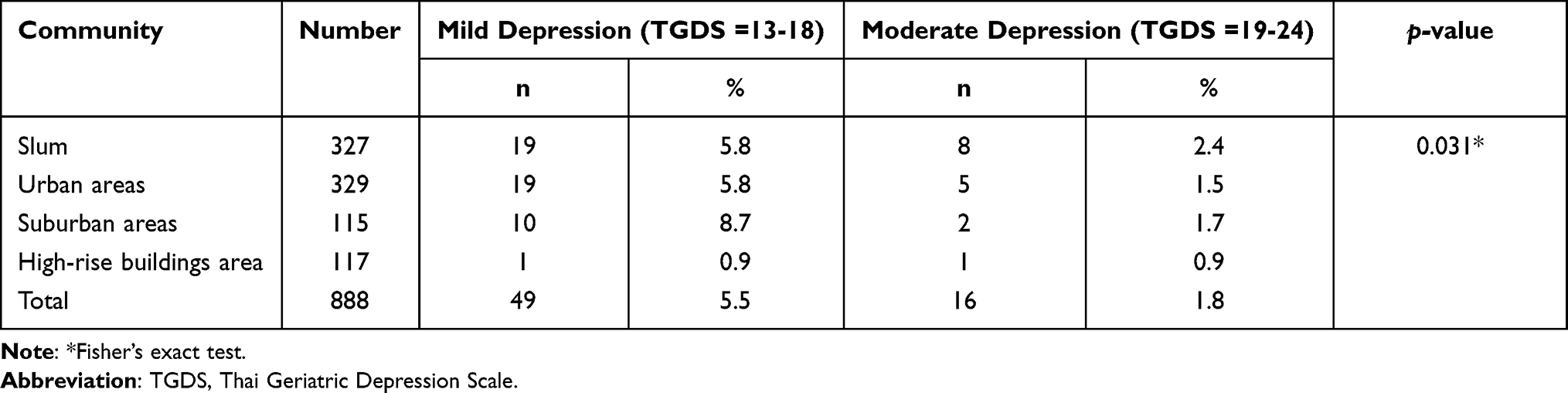 |
Table 1 Proportion of Depression (TGDS>12) |
Table 2 shows the factors associated with depression in the elderly, which included the following categories:
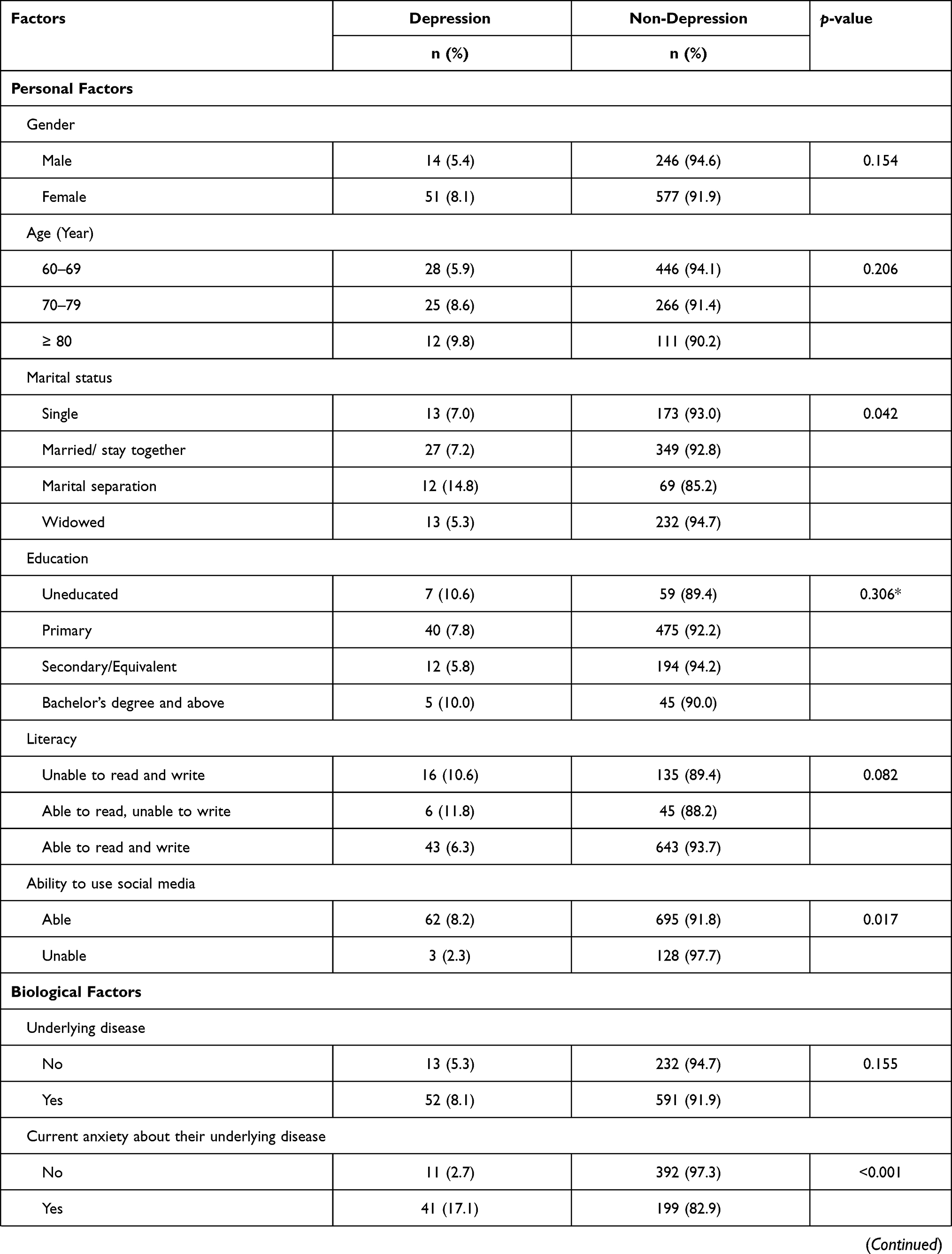 | 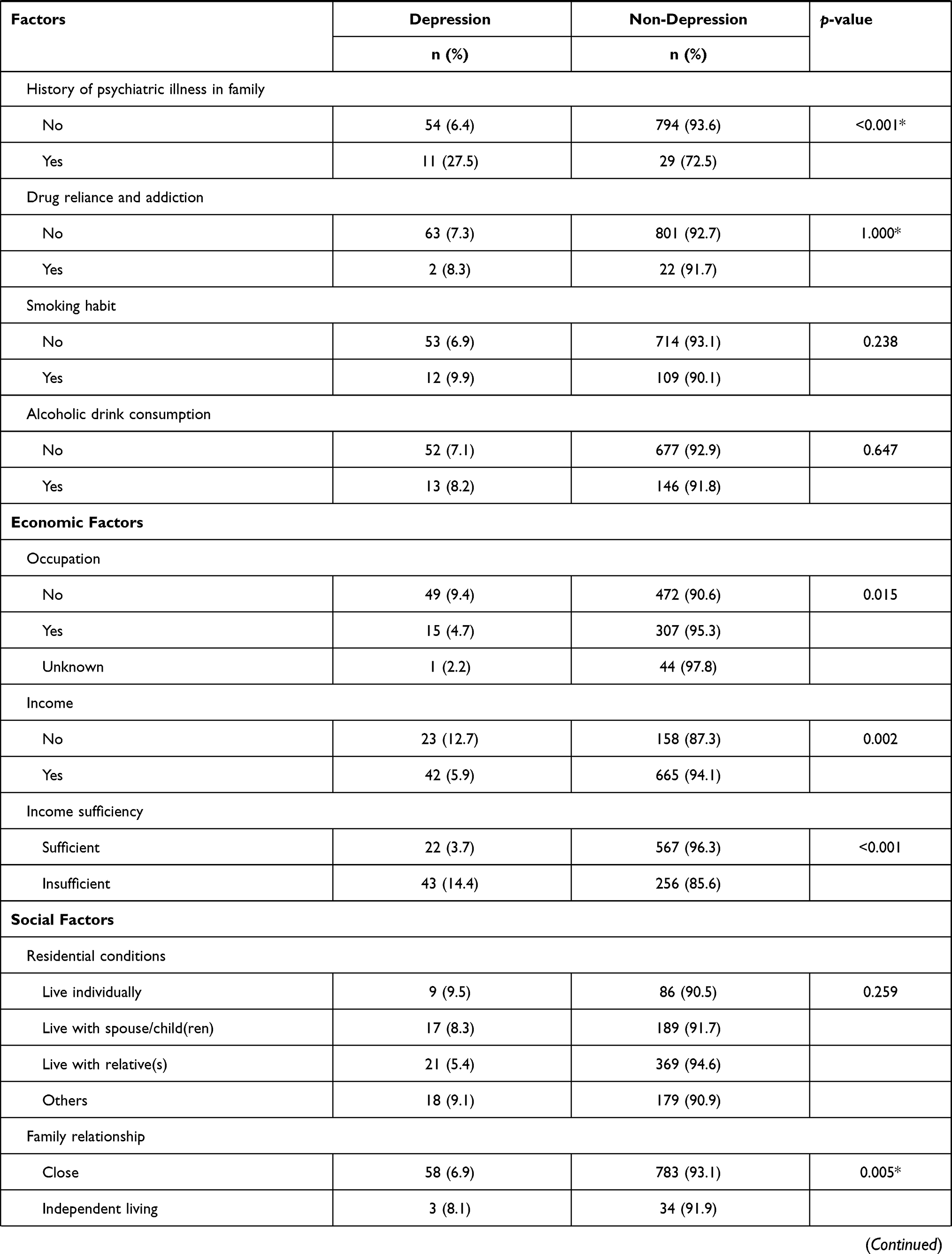 |  |
Table 2 Associated Factors of Depression |
Personal Factors
The prevalence of depression was higher in elderly individuals who had separated in their marital relationship than in the other groups. The prevalence of depression was higher in elderly individuals who were unable to use social media than in those who did use social media (8.2% and 2.3%, respectively).
Biological Factors
The prevalence of depression was higher in elderly individuals with anxiety about their underlying disease (17.1%) than in those without. Underlying diseases were defined as chronic medical conditions, such as diabetes, hypertension, cardiovascular diseases, cancer, stroke, and arthritis. However, older people with a history of psychiatric illness in the family had the highest prevalence of depression (27.5%) among the elderly.
Economic Factors
The prevalence of depression in elderly individuals who had no occupation, no income, or insufficient income were 9.4%, 12.7%, and 14.4%, respectively, which were higher than the rates in other groups.
Social Factors
Elderly individuals with family conflicts had the highest prevalence of depression (40%) among all groups. Elderly individuals with no or less activity participation than elderly in other groups within the past year had a prevalence of depression of 10.5%.
Table 3 shows the analysis of factors associated with depressive symptoms. Univariable regression analysis was performed to analyze the data. The factors significantly associated with depression were marital status, ability to use social media, anxiety about their underlying disease, family history of psychiatric illness, occupation, income, income sufficiency, family relationship, and activity participation within the past year. Next, the factors significantly associated with depression identified in the univariable regression analysis were subsequently analyzed in multiple logistic regression analysis, which showed that the factors significantly associated with depression in the elderly were anxiety about their current disease (AOR = 7.51, 95% CI 3.47–16.27), family conflicts (AOR = 6.30, 95% CI 1.34–29.55), family history of psychiatric illness (AOR = 5.78, 95% CI 2.35–14.21), insufficient income (AOR = 3.81, 95% CI 2.08–6.98), marital separation relationship (AOR = 3.31, 95% CI 1.22–8.98), and less or no activity participation (AOR = 3.09; 95% CI 1.32–7.26 and AOR = 3.02; 95% CI 1.29–7.09).
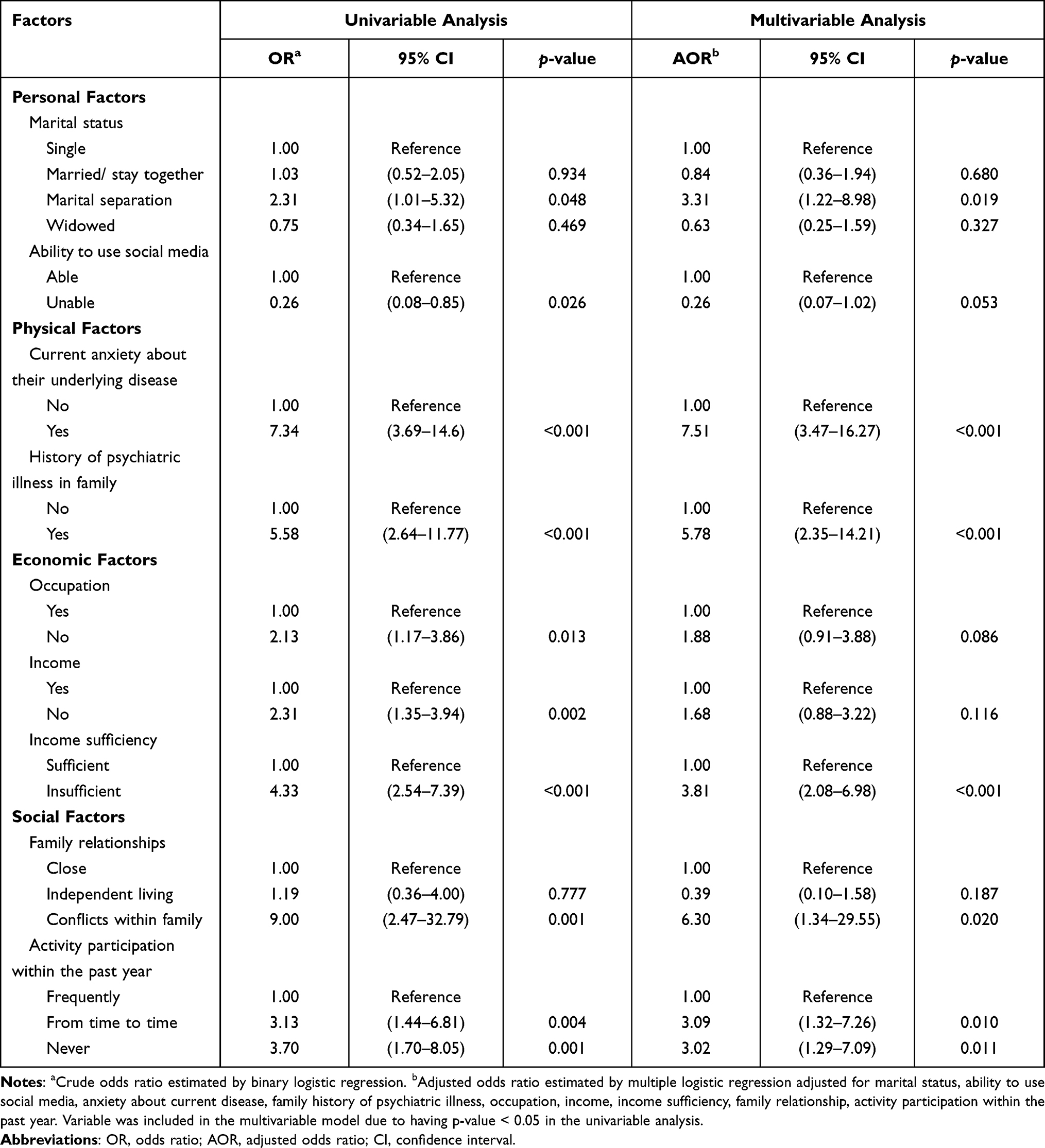 |
Table 3 Factors Affecting Depression Analyzed by Multiple Logistic Regression |
Discussion
Prevalence of Depression
There have been few reported studies on the prevalence of depression in the general elderly population living in Thailand, especially in Bangkok. Most of the reported studies focused on specific elderly groups, such as those with chronic diseases or those who visited an outpatient department. Therefore, this study aimed to determine the prevalence of depression in general groups of the elderly population living in Bangkok at a specific point in time, as determined using the TGDS assessment tool. Our results showed that the overall percentage of depression was 7.3%, of which 5.5% was mild depression, 1.8% was moderate depression, and there was 0% severe depression. These results were relatively lower than the prevalence rates obtained from different studies conducted within Bangkok with the same tool.8–11 However, the results obtained in this study were similar to those of a study of Charernboon et al, which found that the prevalence of depression was 7.7%.11 The reason why the prevalence rate in the study of Charernboon was lower than those of other studies might be that their study focused solely on the elderly population participating in elderly clubs, whereas other studies focused on the elderly population in general. Similarly, the lower prevalence rate in our study might be because the elderly who participated were persuaded to by the Health Volunteers of each community. Therefore, since this group consisted of elderly who were willing and eager to participate in the community’s activities, the depression rate was low. In other words, those who had depression were generally isolated, unwilling to take part in any activity, and would be less likely to participate in the research study in the first place.16–18 Another reason might be that the studied communities were strong and the Health Volunteers had played a crucial role in providing health services. Therefore, the prevalence of depression in this study was low. Consequently, there should be field visits to reach out to the groups of elderly who did not participate in the present study, including the elderly who preferred staying at home and bedridden elderly, to obtain accurate data reflecting the actual prevalence of depression among the broader elderly population. We noted that the prevalence of depression varied in different community areas. In our study, 70% of the sample was female, and the prevalence of depression in females was higher than in males, similar to the sex difference in other community-based studies. The probable reason for the high number of females in our study is that all district areas in Bangkok have more females than males. In suburban areas, the prevalence of depression was 10.4%, primarily mild depression, and higher than in other areas, whereas the prevalence of moderate depression was 2.4% and highest in slum areas. We think this was because most of the people living in slums had lower socioeconomic status than others, and many studies have shown a negative relationship between socioeconomic status and depression.19,20 Nevertheless, our study was unable to identify the specific causes of these differences. For that reason, there should be further in-depth studies that focus on the factors that lead to differences in depression.
Factors Associated with Depression
Among personal factors, marital status and the ability to use social media were significantly related to depression. Specifically, the prevalence of depression was higher in the elderly who were in a marital separation relationship than in other groups. Moreover, marital separation has also been used to predict depression in the elderly. This outcome corresponded to a study conducted in elderly living in foster care in Bangkok, which showed that the marital separation an elderly person had gone through before entering into foster care was a factor that led to depression.21 The probable reason for this finding is that spouses encourage their partners to take better take care of themselves.22 Additionally, spouses make the elderly feel a sense of responsibility to take care of other people and help generate their sense of self-esteem. Having spousal support can help a person overcome loneliness and feel comforted knowing that they have someone to rely on, which leads to higher emotional stability.23 Similarly, a study of Wongpoom et al found that older people living with their spouses were more stable emotionally and in life activities than those who had gone through divorce or separation from their spouses.24 Since widows, divorcees, and separated couples lack encouragement from their spouses, they tend to have a lower sense of self-esteem and need someone from whom they can seek advice. Therefore, these factors could simply lead to depression.
Among social factors, our findings showed that family relationships and participation in activities within the past year were significantly associated with depression. Weissman and Markowitz recognized that interpersonal relationship problems were associated with depression. These problems were divided into four categories: 1) sorrow from loss, 2) conflict in interpersonal relationships, 3) role transmission, and 4) deficits in interpersonal relationships.25 Most of the elderly population probably encounters at least one of these four categories, which would lead to conflicts within the family that affect participation in social activities.16,18,26 The present study revealed that elderly who had never or seldom participated in activities within the past year had a higher prevalence of depression than elderly who often participated in activities. The elderly who rarely or never participated in activities had a three times higher risk of depression. A possible explanation for this could be that the elderly who regularly participated in activities felt that they could perform useful activities and were not a burden to anyone, which made them feel empowered and consequently led to good mental health. For that reason, isolated elderly individuals who had little to no socialization with other people while also being affected by their age-related physical decline could more easily become depressed.
Our study also found that the ability to use social media was significantly associated with depression. That is, depression was more likely to be found in the elderly population who were unable to use social media. Similarly, a study by Shaw et al found that internet usage by the elderly helped strengthen their self-esteem and enabled them to feel supported by society while mitigating loneliness and depression.27 Sangon et al discovered that loneliness was a factor in predicting the occurrence of depression.28 A study of Sum et al found that increasing social networking and social activities had an inverse relationship with social loneliness. On the other hand, the volume of internet usage for contacting or meeting new people varied based on emotional loneliness, so the increase in social relationships would not be able to help mitigate this type of loneliness.29 It was noted that social media usage could help with depression by reducing the feeling of loneliness since it involves social interaction resulting in a sense of self-esteem. The researchers deliberated that there should be a further in-depth study on formats and objectives of social media usage to see how they correlate with depression since it might be useful as guidelines prevention efforts.
For biological factors, we found that having a family history of psychiatric illness could potentially cause depression. Beekman et al found that depression was more likely to occur in the elderly with a family history of psychiatric illness due to heredity than in elderly without that family history. Moreover, having anxiety about an underlying disease also affected depression.30 Similar to several studies, we found that elderly who were less satisfied with their health conditions had a higher prevalence of depression.24,31,32 This finding might be because of age-related physical decline in the elderly, which led to illness and discomfort that made the elderly think they were a burden, further leading to stress, anxiety, and emotional effects.24,33,34 After having suffered from these feelings for a long time, the elderly may feel weary, unhappy, or depressed at a later stage.
Regarding economic factors, occupation, income, and income sufficiency had significant associations with depression. The prevalence of depression was greater among the elderly who had no occupation and income than in the elderly with occupations and incomes. Moreover, income insufficiency was also a factor in predicting depression. The elderly who had insufficient income had a higher prevalence of depression. The results of this study were consistent with the findings of other previous studies.10,13,16,17,24,31,35 In addition, one study revealed that sufficient income was a factor that promoted convenience in life, the ability to rely on themselves, the desire to help other people, and less anxiety about their livelihood, which established a sense of self-esteem and stability in life.36,37 Thus, there was less tendency to develop depression in this group than in the elderly with insufficient income. It is clear that being independent, even with an underlying disease, having the ability to perform daily activities, and having sufficient income are factors that reduced the prevalence of depression.
A limitation of this study was selection bias and the use of a self-rated questionnaire as a proxy for psychiatric diagnosis. Due to the nature of depression, some depressed individuals may not have wanted to participate, as told to us by Health Volunteers, so they were not included in our sample population. Second, the obtained sample had a much higher proportion of females (70.7%), so the results may not reflect the findings in the whole elderly population in Bangkok. Finally, the use of a self-rated questionnaire may have underestimated the prevalence of depression because of self-reporting bias.
Conclusion
Communities should pay attention to the elderly who have underlying diseases because the prevalence of depression was higher in that group than in other groups in general. Depression may make it more likely that this group of elderly does not take care of themselves as well as they would if they were not depressed. Moreover, the general community should promote more activities that the elderly can participate in, especially income-earning activities. To mitigate depression in the elderly, a community program focusing on family relationships should be organized to enhance good relationships and ease conflict among the elderly and family members.
Acknowledgments
The present study was supported by a grant from the Faculty of Medicine Vajira hospital, Navamindradhiraj University. The authors would like to thank all participants of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh A, Misra N. Loneliness, depression and sociability in old age. Ind Psychiatry J. 2009;18(1):51–55. doi:10.4103/0972-6748.57861
2. Cacioppo JT, Cacioppo S. The growing problem of loneliness. Lancet. 2018;391(10119):426. doi:10.1016/S0140-6736(18)30142-9
3. Anderson AN. Treating depression in old age: the reasons to be positive. Age Ageing. 2001;30(1):13-17. doi:10.1093/ageing/30.1.13
4. Barua A. Trend of the prevalence of geriatric depression: A modern silent epidemic. Int J Collab Res Intern Med Public Health. 2013;5:37–47.
5. Volkert J, Schulz H, Härter M, Wlodarczyk O, Andreas S. The prevalence of mental disorders in older people in Western countries-a meta-analysis. Ageing Res Rev. 2013;12(1):339-353. doi:10.1016/j.arr.2012.09.004
6. Liang G, Arunpongpaisal S, Kessomboon P, Pinitsoontorn S, Kuhirunyaratu P. Depression and cognitive impairment among the community of Khon Kaen: a primary care setting descriptive study. J Psychiatr Assoc Thailand. 2009;54:357–366.
7. Retty A. Prevalence of depression and related factors among the elderly people in Dindang sudistrict, Bangkok Metropolitan, Thailand. Thesis for Master of Public Health, Mahidol University; 1992.
8. Tubmanee M. Depression and dementia in Thai community dwelling elderly in Bangkok. J Clin Psychol. 2001;2:43–57.
9. Thongtang O, Sukhatunga K, Nagmthipwatthana T, et al. Prevalence and incidence of depression in the Thai elderly. J Med Assoc Thai. 2002;85:540–544.
10. Stawathumrong P. Prevalence and Factors Associated with Dementia and Depression Among Thai Elderly. Bangkok: Somdet Chaopraya Institute of Psychiatry; 2001.
11. Charernboon T, Phanasathit M, Tangwongchai S, Hemrungrojn S, Worakul P. Depression and dementia among members of 15 elderly clubs in Bangkok. Thammasat Med j. 2010;10(4):428–436.
12. Stettens DC, Blazer DG, Beyer IL. Mood disorders. In: Thakur ME, Blazer DG, Steffens DC, editors. Clinical Manual of Geriatric Psychiatry. Arlington: American psychiatric publishing; 2014:125–156.
13. Bunloet A. Prevalence and factors associated with depression among the elderly community residents with chronic diseases in Samliam Urban Primary Care Unit, Khon Kaen. Srinagarind Med J. 2016;31(1):25–33.
14. Bretschneider J, Janitza S, Jacobi F, et al. Time trends in depression prevalence and health-related correlates: results from population-based surveys in Germany 1997–1999 vs. 2009–2012. BMC Psychiatry. 2018;18(1):394. doi:10.1186/s12888-018-1973-7
15. Poungvarin N. Train The Brain Forum Committee. Thai geriatric depression scale-TGDS. Siriraj Hosp Gaz. 1994;46:1–9.
16. Sasithorn N, Lueboonthavatchai P. Depression and Associated Psychosocial Factors of Elderly at the Elderly Associate of Public Health Center 48 Nakwatchara-utid. Chula Med J. 2015;59(6):717–730.
17. Linsuwanont P. A Study of Elderly Depression in Rongmuang Subdistrict, Pratumwan, Bangkok Metropolis [Dissertation]. Bangkok: Mahidol University; 2000.
18. Phainrungruang R, Lueboonthavatchai P. Interpersonal problems and depression of the elderly at the Elderly Associate in Phitsanulok Province. J Psychiatr Assoc Thailand. 2015;60(1):23–34.
19. No authors listed. Cross-national comparisons of the prevalences and correlates of mental disorders. WHO International Consortium in Psychiatric Epidemiology. Bull World Health Organ. 2000;78(4):413-426.
20. Jo S-J, Yim HW, Bang MH, et al. The association between economic status and depressive symptoms: an individual and community level approach. Psychiatry Investig. 2011;8(3):194–200. doi:10.4306/pi.2011.8.3.194
21. Promjun T, Suppapitiporn S. Depression loneliness and self-esteem of the elderly in Bangkae Home and private homes for the aged in Bangkok. Chula Med J. 2014;58(5):545–561.
22. Hanucharurnkul S. Social Support, Self-Care, and Quality of Life in Cancer Patients Receiving Radiotherapy in Thailand [Dissertation]. Michigan: Wayne State University; 1988.
23. Joung IMA, Stronks K, van de Mheen H, van Poppel FWA, van der Meer JBW, Mackenbach JP. The contribution of intermediary factors to marital status differences in self-reported health. J Marriage Fam. 1997;59(2):476–490. doi:10.2307/353484
24. Wongpoom T, Sukying C, Udomsubpayakul U. Prevalence of depression among the elderly in Chiang Mai Province. J Psychiatr Assoc Thailand. 2011;56(2):103–116.
25. Weissman MM, Markowitz JC. Interpersonal psychotherapy: principles and applications. World Psychiatry. 2004;3(3):136–139.
26. Yaiyong O, Lueboonthavatchai P. Depression and grief of the elderly at the elderly associate in Nonthaburi province. J Psychiatr Assoc Thailand. 2011;56:117–128.
27. Shaw LH, Gant LM. In defense of the internet: the relationship between Internet communication and depression, loneliness, self-esteem, and perceived social support. Cyberpsychol Behav. 2002;5(2):157-171.
28. Sangon S, Sampao P, Malathum P. Relationships of health status, family relations, and loneliness to depression in older adults. Rama Nurs J. 2007;13(1):54–69.
29. Sum S, Mathews RM, Hughes I, Campbell A. Internet use and loneliness in older adults. Cyberpsychol Behav. 2008;11(2):208–211. doi:10.1089/cpb.2007.0010
30. Beekman ATF, Deeg DJH, van Tilburg TG, Smit JH, Hooijer C, van Tilburg W. Major and minor depression in later life: a study of prevalence and risk factors. J Affect Disord. 1995;36:65–75. doi:10.1016/0165-0327(95)00061-5
31. Paungrod N. The study on depression in Nonthaburi province elderly. Princess Naradhiwas Univ J Humanities Social Sci. 2015;2(1):63–74.
32. Kitthanarut R, Thoppradit R. Factors related to depression of elders who had non-communicable chronic diseases in subdistrict health promoting hospital of Sa Takhian, Soeng Sang, Nakhon Ratchasima. JCDLQ. 2019;7(1):69–80.
33. Borglin G, Jakobsson U, Edberg AK, Hallberg IR. Self-reported health complaints and their prediction of overall and health-related quality of life among elderly people. Int J Nurs Stud. 2005;42(2):147–158. doi:10.1016/j.ijnurstu.2004.06.003
34. Tongdee J, Rongmuang D, Nakchatree C. Health status and quality of life among the elderly in the southern border provinces of Thailand. Nursing J Ministry Public Health. 2011;22(3):88–99.
35. Freeman A, Tyrovolas S, Koyanagi A, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. 2016;16(1):1098. doi:10.1186/s12889-016-3638-0
36. Chou KL, Chi I, Chow NW. Sources of income and depression in elderly Hong Kong Chinese: mediating and moderating effects of social support and financial strain. Aging Ment Health. 2004;8(3):212–221. doi:10.1080/13607860410001669741
37. Litwin H, Sapir EV. Perceived income adequacy among older adults in 12 countries: findings from the survey of health, ageing, and retirement in Europe. Gerontologist. 2009;49(3):397–406. doi:10.1093/geront/gnp036
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.