Back to Journals » Risk Management and Healthcare Policy » Volume 15
Factors Associated with Anxiety and Depression Among Micro, Small, and Medium Enterprise Restaurant Entrepreneurs Due to Thailand’s COVID-19-Related Restrictions: A Cross-Sectional Study
Authors Sornsenee P ![]() , Kongtragulsub K
, Kongtragulsub K ![]() , Watcharajiranich K, Chantanuwat R, Aungchayakul A, Mangkhalathat K
, Watcharajiranich K, Chantanuwat R, Aungchayakul A, Mangkhalathat K ![]() , Laparojkit S
, Laparojkit S
Received 22 January 2022
Accepted for publication 23 May 2022
Published 27 May 2022 Volume 2022:15 Pages 1157—1165
DOI https://doi.org/10.2147/RMHP.S359507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Kyriakos Souliotis
Phoomjai Sornsenee,1 Krittanon Kongtragulsub,2 Kraitouch Watcharajiranich,2 Ratsak Chantanuwat,2 Awika Aungchayakul,2 Kollarat Mangkhalathat,2 Siriyakorn Laparojkit2
1Department of Family Medicine and Preventive Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand; 2Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Phoomjai Sornsenee, Department of Family Medicine and Preventive Medicine, Faculty of Medicine, Prince of Songkla University, 15 Karnjanavanich Road, Hat Yai, Songkhla, 90110, Thailand, Tel +66954204713, Fax +6674451333, Email [email protected]
Purpose: COVID-19 has become a global pandemic. Since the Thai government announced its pandemic-related restrictions, economic indicators have inevitably been impacted. Micro, small, and medium enterprise (MSME) entrepreneurs have adapted to the unexpected changes, undoubtedly requiring government assistance. Therefore, this study assessed the prevalence of anxiety and depression in MSME restaurant entrepreneurs after the government announced its COVID-19-related restrictions.
Patients and Methods: An online questionnaire was developed and distributed to MSME entrepreneurs’ restaurants in Songkhla province, southern Thailand, in November 2021. Thai Hospital Anxiety and Depression Scales (Thai HADS) were used to assess the prevalence of anxiety and depression. Multiple logistic regression was used to analyze the factors associated with depression and anxiety, and the adjusted odds ratio (OR) for both variables was reported at a P-value < 0.05 for significance.
Results: In total, 181 MSME restaurant entrepreneurs responded to our online questionnaire in November 2021. The prevalence of anxiety and depression was 12.2% and 11.6%, respectively. Participants with a family history of psychological disorders (OR 34.9, P-value 0.003), an underlying disease (OR 7.14, P-value 0.032), a high debt-to-income ratio (OR 73.75, P-value 0.007), or a low education level were more likely to have anxiety. Similarly, participants who had an underlying disease (OR 14.29, P-value 0.032) and lacked access to supportive measures from the government (OR 6.94, P-value 0.009) were more likely to suffer from depression.
Conclusion: The period of restrictive policies during the COVID-19 pandemic had a negative impact on MSME restaurant entrepreneurs’ mental health. The factors that were significantly associated with anxiety were debt-to-income ratio and concern about COVID-19 prevention and treatment. The factors that were significantly associated with depression included inadequate access to government aid. Hence, the government should focus on providing and allocating healthcare resources during the COVID-19 pandemic.
Keywords: anxiety and depression and, micro, small, and medium enterprises, MSMEs, COVID-19, COVID-19 restrictions, entrepreneurs
Key Messages
- The period of restrictive policies being in place during the COVID-19 pandemic had a negative impact on MSME restaurant entrepreneurs’ mental health.
- The factors that were significantly associated with anxiety were debt-to-income ratio and concern about COVID-19 prevention and treatment. The factors that were significantly associated with depression included inadequate rights to access government aid.
- Governments should prioritize providing and allocating healthcare resources during the COVID-19 pandemic, particularly for vulnerable groups such as MSME entrepreneurs with pre-existing medical conditions, a family history of psychological disorders, or a high debt-to-income ratio.
Introduction
COVID-19 was declared a pandemic in March 2020.1 Many governments implemented measures such as wearing masks, social distancing, lockdowns,2 and providing vaccinations3 aimed at curbing the spread of the virus. Economic indicators such as household income, urban job loss, reduced market interaction, and labor market activity, including global supply chains, have inevitably been impacted, resulting in widespread business disruptions since the measures were implemented.4,5 Although Thailand was relatively successful in containing the first wave of the pandemic in 2020,6 the country has been experiencing an uncontrollable resurgent second outbreak since early 2021. Due to the negative economic impact of the previous complete lockdown, the government adopted a targeted strategy, locking down specific areas and tracing positive cases.7 As a result, although Thailand’s response to COVID-19 was effective in containing the disease’s spread, it fell short of addressing the multiple dimensions of the crisis, including its economic and social consequences.8
Micro, small, and medium-sized enterprises (MSMEs) are an important driver of Thailand’s economy. According to a recent report, MSMEs accounted for 69% of the Thai labor market. Since the beginning of the COVID-19 pandemic, MSME entrepreneurs have adapted to unexpected changes in consumer behavior, product safety, social isolation, and the government’s disease prevention policy. Throughout the COVID-19 crisis, the Office of Small and Medium Enterprises Promotion (OSMEP) and other agencies financially assisted MSME entrepreneurs by implementing policies that encourage entrepreneurs nationwide to register and take advantage of the government’s stimulus packages.9 Supportive policies include soft loan facilities for MSMEs, debt restructuring with buy-back options, cash transfers to employees covered by the social security system, and a half-and-half co-payment scheme (the government subsidizing 50% of receipts).10 Most entrepreneurs reported that they had shifted their focus to online promotion and 79.3% of MSMEs have adapted to accepting online payments; however, a recent report revealed that MSMEs’ GDP fell by 3.3% in the first quarter of 2020, particularly in the hospitality and food services sector, which fell by 21.1%.9,11 According to a recent study, entrepreneurs’ stress levels increased significantly during the pandemic, with 72% developing mental illness and 30% struggling with anxiety and depression, thus increasing their risk of developing general anxiety disorder (GAD) and major depressive disorder (MDD).12 Entrepreneurs must overcome numerous obstacles for their businesses to stay afloat,13 and so, the ability to receive government assistance is necessary.14
Therefore, the present study evaluated the prevalence and factors associated with anxiety and depression in MSME entrepreneurs after the announcement of the government’s restriction policies during the COVID-19 pandemic. Additionally, we focused on the restaurant sector because it was the most affected by the restrictions.
Methods
Study Design and Setting, and Participants
We conducted a prospective cross-sectional study with MSME restaurant entrepreneurs in Songkhla province, southern Thailand, who were at least 18 years old and had never been diagnosed with a psychiatric disorder.
Data Collection and Questionnaire
An online questionnaire for the survey participants was developed and responses were collected via Google Forms in November 2021. The questionnaire was divided into five sections—demographic data, business information, psychosocial information, government support measures, and mental status. The following characteristics of entrepreneurs were collected: gender, age, religion, marital status, income, expenses, level of education, drinking and smoking habits, medical history, medication use, family history of mental disorders, and family violence. The second section collected business-related information, such as primary occupation, revenue, debt-to-income ratio, adaptability, and financial liquidity. The third section elicited data related to their psychosocial well-being, including health insurance, family members with COVID-19, stressors, and coping mechanisms. The fourth section sought to collect data on their participation in the government’s assistance programs, to assess factors such as barriers to accessing the government’s economic stimulus packages or health care resources.
The final section is the primary objective of this study, which was to assess participants’ anxiety and depression levels using the Thai Hospital Anxiety and Depression Scale (Thai HADS).15 The Thai HADS has been evaluated for reliability (alpha = 0.89), sensitivity (MDD = 85.7%, GAD = 100%), and specificity (MDD = 91.3%, GAD = 86.7%), and has been widely used in previous research.16,17 It is a fourteen-item scale with seven items each for the anxiety and depression subscales. Each item is scored on a scale of 0 to 3, with 3 indicating the highest level of anxiety or depression. A total subscale score of more than 11 points indicates a significant MDD or GAD diagnosis.
The questionnaire was distributed to MSME restaurant entrepreneurs with the permission of the Songkhla MSMEs union via online platforms such as direct email messages and the Line instant messaging application. Google’s cloud platform was used to collect and encrypt the data. All questionnaire records were fully computerized and accessible only to the principal investigator.
Statistical Analysis
The analyses were conducted using R 4.1.2 and the epiDisplay package. To describe categorical variables, the baseline characteristics of the participants were calculated and expressed in terms of numbers and percentages. The prevalence of anxiety and depression using the Thai HADS was calculated, resulting in binary data with a cut-off of adjusted odds ratio of more than 11 points for each domain. The binary data from the Thai HADS were then classified into variables, and the relationships between the variables were analyzed using multiple logistic regression for the anxiety and depression domains. The adjusted odds ratio for both the depression and anxiety variables and their 95% confidence intervals (95% CI) were reported. Statistical significance was considered when P-values were < 0.05.
Results
Out of 558 MSME restaurant entrepreneurs in the Songkhla province, we enrolled 181 entrepreneurs who responded to the online questionnaire. Table 1 shows the baseline characteristics of participants: 63% were female, 43.9% of them were aged below 30, and 62.6% were married. Most participants held bachelor’s degrees, and their monthly income and expenses ranged between 15,000 and 29,999 baht. Most participants had no medical conditions or family history of psychological disease. However, those who smoked and drank alcohol accounted for 89.5% and 64.6%, respectively. Table 2 shows the prevalence of anxiety and depression in participants during the period of restrictions using the Thai HADS score.
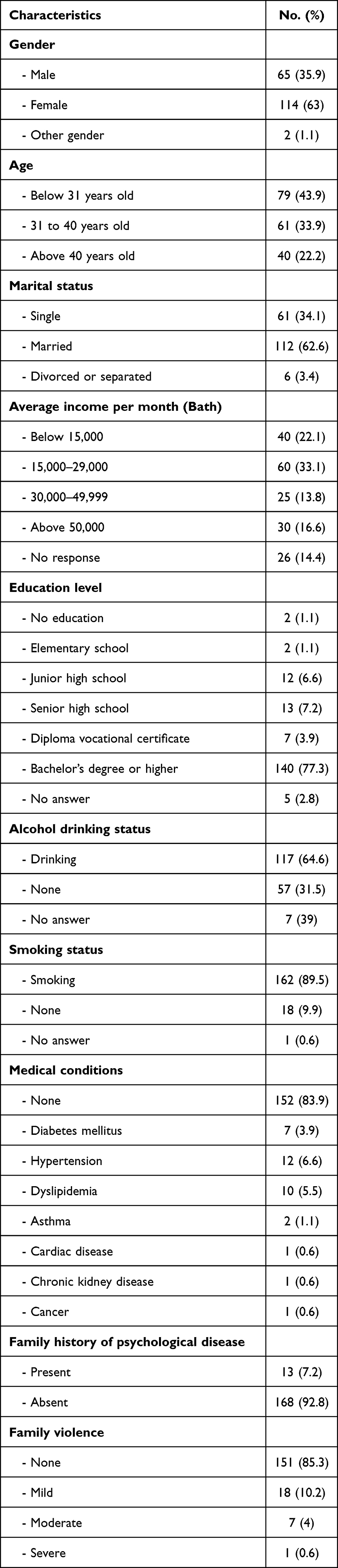 |
Table 1 Baseline Characteristics of MSME Restaurant Entrepreneurs |
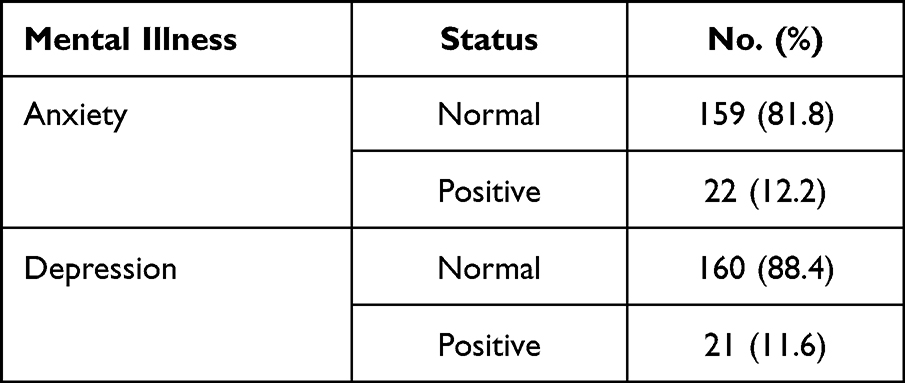 |
Table 2 Prevalence of Anxiety and Depression Using the Thai HADS Among MSME Restaurant Entrepreneurs |
Table 3 illustrates the relationships between anxiety and factors associated with the government’s restriction policies using multiple logistic regression analysis. The following were significantly associated with anxiety: those with a family history of psychological disorders, a medical condition, a history of substance abuse to cope with anxiety, a high debt-to-income ratio, a low education level, and those who expressed concerns about COVID-19 prevention and treatment. Participants with a family history of psychological disorders were more likely to experience anxiety (OR 34.9, P-value 0.003), as were those with a medical condition (OR 7.14, P-value 0.032). Participants who were concerned about obtaining resources and securing a hospital bed for COVID-19 were at an increased risk of anxiety (OR 5.26, P-value 0.038). Additionally, those who used substances to cope with anxiety were at a higher risk of developing anxiety (OR 8.59, P-value 0.019). Anxiety was more common in those with a high debt-to-income ratio (OR 73.75, P-value 0.007). In contrast, participants with a bachelor’s degree or higher had a lower risk of anxiety (OR 0.1, P-value 0.09).
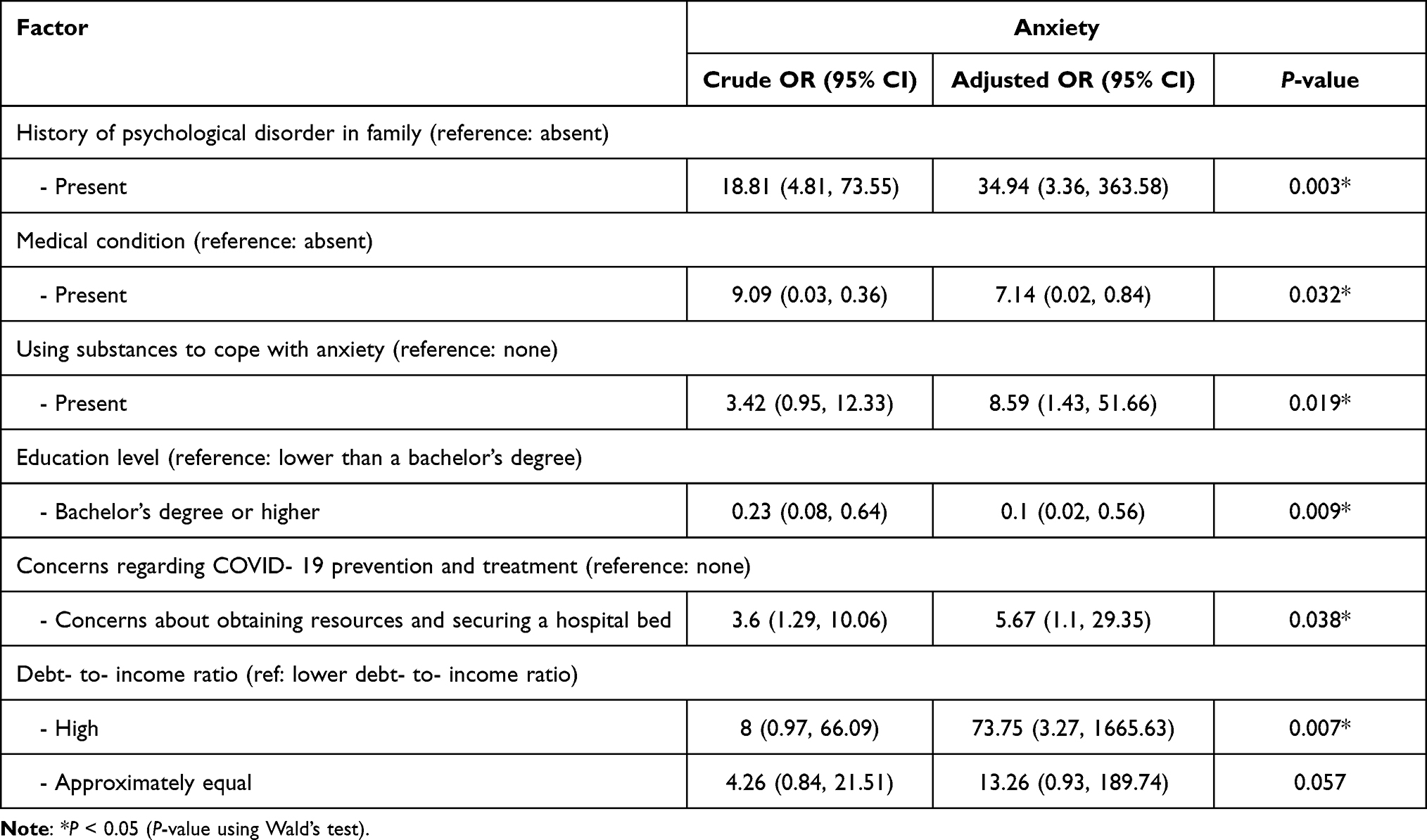 |
Table 3 Factors Associated with Anxiety Among MSME Restaurant Entrepreneurs Using Multiple Logistic Regression |
The results showed that depression was associated with having an underlying disease as well as insufficient rights to access government support. Table 4 illustrates the OR of the factors. Participants with a prior medical condition faced an increased risk of depression (OR 14.29, P-value 0.032). Additionally, the risk of depression increases in those with insufficient access to government support (OR 6.94, P-value 0.009).
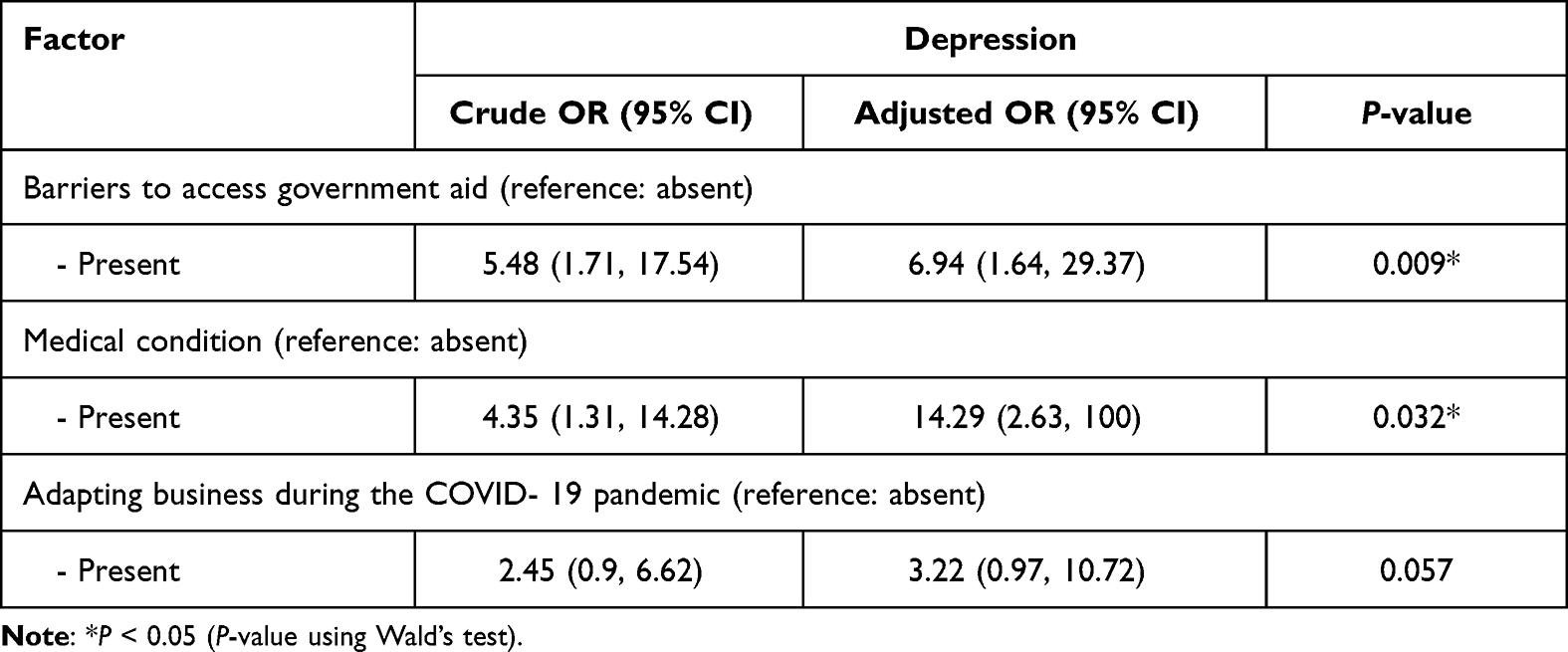 |
Table 4 Factors Associated with Depression Among MSME Restaurant Entrepreneurs Using Multiple Logistic Regression |
Discussion
Statement of Principal Findings
The period of restrictive policies being in place during the pandemic had a negative impact on the mental health of MSME restaurant entrepreneurs in our study setting. Our findings indicate that approximately 12% of MSME restaurant entrepreneurs in Songkhla suffered from anxiety and depression during COVID-19. Participants with a family history of psychological disorders, an underlying disease, a high debt-to-income ratio, or a low education level were more likely to have anxiety. Similarly, participants who had an underlying disease and lacked access to government support were more likely to suffer from depression.
Interpretation Within the Context of the Existing Literature
Our study found that the prevalence of anxiety and depression could have been influenced by several factors during the COVID-19 situation, similar to other studies.18–21
Individuals with a family history of psychological disorders and medical conditions were at an increased risk of anxiety and depression during the pandemic. Consistent with other studies,19,20 vulnerable people at risk of mental illness were identified during the COVID-19 period. Entrepreneurs who were diagnosed with medical conditions during the pandemic expressed distress when they realized that adapting to new business conditions made it more difficult to continue their businesses,12 which may have resulted in an increased risk of mental health problems.
MSME restaurant entrepreneurs with a high debt-to-income ratio had a significantly increased risk of anxiety (OR 73.75, P-value 0.007) compared to those with a low debt-to-income ratio. This finding is consistent with a systematic review,22 which discovered that participants who reported being in debt experienced the greatest level of anxiety. Despite the fact that the government has attempted to institute policies that provide significant financial assistance, this appears to be a sizable and complicated issue.10 However, our study showed that higher education might help entrepreneurs cope with their stress and anxiety, similar to a previous study.23
Concerns about obtaining resources and securing a hospital bed for COVID-19 treatment increased the risk of anxiety (OR 5.26, P-value 0.038). During the pandemic, demand for sanitizers, masks, and other protective agents increased, and thus, a shortage of these items could cause significant stress and anxiety.18,24 The restrictions on mobility and physical activity during the pandemic may also make hospitalization more difficult and lead to anxiety.25
Using substances to cope with stress increases one’s risk of developing anxiety (OR 18.81, P-value 0.003). According to prior studies,26,27 anxiety disorders and substance use disorders frequently coexist, and this is especially common during the pandemic. A pandemic is an environmental factor that can encourage people to channel their anxiety and stress into substance abuse.28 However, our research found that this coping method may not be effective. As a result of the government’s policy of prohibiting night parties and limiting alcohol consumption, community interaction was inhibited. Because most people use substances in their homes, their feelings of fear, loneliness, anxiety, and stress may have been stimulated.26,29
Among MSME restaurant entrepreneurs, a lack of government support appeared to increase the risk of depression. Those who were unable to obtain government assistance were more prone to depression (OR 6.94, P-value 0.003). This finding corroborates a previous study conducted on the general population in Ghana,30 which reported that low levels of government support were associated with increased rates of depression and mental distress.
Strengths and Limitations
Our study is the first to investigate the mental health of restaurant entrepreneurs after the government’s announcement of COVID-19-related restrictions in Thailand. Our findings provide information that the government can directly implement, with a focus on MSME restaurant entrepreneurs.
Due to the study’s small sample size, certain potentially significant factors, such as adapting the business during the COVID-19 pandemic, were found to be insignificant (OR 3.22, P-value 0.057), also resulting in a wide 95% CI for other factors. However, we focused on real pandemic situations that affect actual economic sectors, as several restaurants were closed during our survey. Additionally, because this is a cross-sectional study, certain causes and effects cannot be explained, such as the outcome in those with a family history of psychological illnesses or a history of substance misuse to cope with anxiety. In fact, factors in the population should be measured before and after the policy implementation and compared OR between the normal situation and the policy implementation period.
Implications for Policy, Practice, and Research
The government should place more focus on providing and allocating healthcare resources during the COVID-19 pandemic. Additionally, an increasing number of governments should provide aid for healthcare or modify and extend criteria for more comprehensive assistance. The government should also implement more surveillance for mental illness in vulnerable groups such as MSMEs who have medical conditions or a higher debt-to-income ratio. The government should provide adequate business support to MSMEs to help them manage their businesses and mitigate the negative impact of COVID-19 on their mental health. Similar to OSMEP,11 our study found that the primary challenges and barriers to obtaining government assistance faced by MSMEs were ineligibility, followed by delays, validation errors, and bureaucratic procedures associated with the relief measure system.
Conclusion
The period of restrictive policies being in place during the COVID-19 pandemic had a negative impact on MSME restaurant entrepreneurs’ mental health. The factors that were significantly associated with anxiety were debt-to-income ratio and concern about COVID-19 prevention and treatment. The factors that were significantly associated with depression included inadequate access to government aid. The government focus more on providing and allocating healthcare resources during the COVID-19 pandemic.
Ethics and Other Permissions
The study was approved by the Human Research Ethics Committee (HREC), Faculty of Medicine, Prince of Songkla University, on October 23, 2021. (Approval Number: REC 64-366-9-1). HREC is an official institute responsible for ethical review and supervision of human research. The study was conducted in accordance with the Declaration of Helsinki. All questionnaires were fully computerized by the researchers and confidentially reported.
Informed Consent Statement
Before this research began, HREC approved the requirement for informed consent. The data were gathered using anonymous methods that could not be used to identify the participants. Before the participants could fill out the research questionnaire, they had to sign an online informed consent form. The risk associated with participation is negligible. However, the research protocol includes a procedure for advising participants if they require mental consultation after completing the questionnaire. Participants have the right to decline to participate in this study without negatively impacting their rights to services and benefits.
Acknowledgments
We would like to express our gratitude to the Department of Family Medicine and Preventive Medicine at Prince of Songkla University for developing the instruction for medical students to conduct research in the Community Medicine III and IV courses, which resulted in the conduct of this study. We would also like to thank Assistant Professor Dr. Napakkawat Buathong, who provided us with useful advice for conducting this research.
Author Contributions
All authors made a significant contribution to the reported work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
No funding was received for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324(8):782–793. doi:10.1001/jama.2020.12839
2. Haug N, Geyrhofer L, Londei A, et al. Ranking the effectiveness of worldwide COVID-19 government interventions. Nature Human Behaviour. 2020;4(12):1303–1312. doi:10.1038/s41562-020-01009-0
3. Finney Rutten LJ, Zhu X, Leppin AL, et al. Evidence-based strategies for clinical organizations to address COVID-19 vaccine hesitancy. Mayo Clinic Proc. 2021;96(3):699–707. doi:10.1016/j.mayocp.2020.12.024
4. Brodeur A, Gray D, Islam A, Bhuiyan S. A literature review of the economics of COVID‐19. J Econ Surv. 2021;35(4):1007–1044. doi:10.1111/joes.12423
5. Lu Y, Wu J, Peng J, Lu L. The perceived impact of the Covid-19 epidemic: evidence from a sample of 4807 SMEs in Sichuan Province, China. Environ Hazards. 2020;19(4):323–340. doi:10.1080/17477891.2020.1763902
6. Triukose S, Nitinawarat S, Satian P, et al. Effects of public health interventions on the epidemiological spread during the first wave of the COVID-19 outbreak in Thailand. PLoS One. 2021;16(2):e0246274. doi:10.1371/journal.pone.0246274
7. Rajatanavin N, Tuangratananon T, Suphanchaimat R, Tangcharoensathien V. Responding to the COVID-19 second wave in Thailand by diversifying and adapting lessons from the first wave. BMJ Glob Health. 2021;6(7):e006178. doi:10.1136/bmjgh-2021-006178
8. Marome W, Shaw R. Covid-19 response in Thailand and its implications on future preparedness. Int J Environ Res Public Health. 2021;18(3):1089. doi:10.3390/ijerph18031089
9. Office of Small and Medium Enterprises promotion (OSMEP). EXECUTIVE SUMMARY white paper on MSME 2020 [Internet]. Utopia Media International (Thailand) Co., Ltd.; 2020 [cited January 5, 2021]. Available from: https://www.sme.go.th/upload/mod_download/download-20201005123037.pdf.
10. Bank of Thailand. Government measures in response to COVID-19 from February 2020 to March 2021. Bank of Thailand. Available from: https://www.bot.or.th/English/MonetaryPolicy/MonetPolicyComittee/MPR/BOX_MRP/BOX1_MPRMarch2021_MeasuresCOVID19.pdf.
11. Office of Small and Medium Enterprises promotion (OSMEP). OSMEP annual report 2019 [Internet]. HUAYAI Creative Media House; 2020 [cited January 5, 2021]. Available from: https://www.sme.go.th/upload/mod_download/download-20201103152522.pdf.
12. Stephan U, Zbierowski P, Pérez-Luño A, et al. Entrepreneurship during the Covid-19 pandemic: a global study of entrepreneurs’ challenges, resilience, and well-being. J Occup Health Psychol. 2021;26(6):459–468. doi:10.1037/ocp0000316
13. Syriopoulos K. The impact of COVID-19 on entrepreneurship and SMEs. J Int Acad Case Stud. 2020;26(2):1–2.
14. Fitriasari F. How do Small and Medium Enterprise (SME) survive the COVID-19 outbreak? J Inov Ekon. 2020;5(2). doi:10.22219/jiko.v5i3.11838
15. Nilchaikovit T. Development of Thai version of Hospital Anxiety and Depression Scale in cancer patients. J Psychiatr Assoc Thai. 1996;4:18–30.
16. Phabphal K, Sattawatcharawanich S, Sathirapunya P, Limapichart K. Anxiety and depression in Thai epileptic patients. J Med Assoc Thai. 2007;90(10):2010.
17. Lueboonthavatchai P. Prevalence and psychosocial factors of anxiety and depression in breast cancer patients. J Medi Assoc Thai. 2007;90(10):2164.
18. Choi EPH, Hui BPH, Wan EYF. Depression and anxiety in Hong Kong during COVID-19. Int j Environ Res Public Health. 2020;17(10):3740. doi:10.3390/ijerph17103740
19. Bawankule S, Khatib MN, Quazi Syed Z, Gaidhane A, Telrandhe S, Godhiwala P. Depression, anxiety and stress among the general population in the time of COVID-19 lockdown: a cross-sectional study protocol. Int j Res Pharm Sci. 2020;11:360–364. doi:10.26452/ijrps.v11iSPL1.2726
20. Tasnim R, Sujan MSH, Islam MS, et al. Depression and anxiety among individuals with medical conditions during the COVID-19 pandemic: findings from a nationwide survey in Bangladesh. Acta Psychol. 2021;220:103426. doi:10.1016/j.actpsy.2021.103426
21. Shahriarirad R, Erfani A, Ranjbar K, Bazrafshan A, Mirahmadizadeh A. The mental health impact of COVID-19 outbreak: a Nationwide Survey in Iran. Int J Ment Health Sys. 2021;15(1):19. doi:10.1186/s13033-021-00445-3
22. Amit N, Ismail R, Zumrah AR, et al. Relationship between debt and depression, anxiety, stress, or suicide ideation in Asia: a systematic review. Front Psychol. 2020;11:1336. doi:10.3389/fpsyg.2020.01336
23. Bjelland I, Krokstad S, Mykletun A, Dahl AA, Tell GS, Tambs K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc Sci Med. 2008;66(6):1334–1345. doi:10.1016/j.socscimed.2007.12.019
24. Liu C, Lee Y, Lin Y, Yang S. Factors associated with anxiety and quality of life of the Wuhan populace during the COVID-19 pandemic. Stress Health. 2021;37(5):887–897. doi:10.1002/smi.3040
25. Chirico A, Lucidi F, Galli F, et al. COVID-19 outbreak and physical activity in the Italian population: a cross-sectional analysis of the underlying psychosocial mechanisms. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.02100
26. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24 –30, 2020. Morb Mortal Wkly Rep. 2020;69(32):1049. doi:10.15585/mmwr.mm6932a1
27. Rogers AH, Shepherd JM, Garey L, Zvolensky MJ. Psychological factors associated with substance use initiation during the COVID-19 pandemic. Psychiatry Res. 2020;293:113407. doi:10.1016/j.psychres.2020.113407
28. Goldmann E, Galea S. Mental health consequences of disasters. Annu Rev Public Health. 2014;35:169–183. doi:10.1146/annurev-publhealth-032013-182435
29. Sher L. The impact of the COVID-19 pandemic on suicide rates. QJM- Int J Med. 2020;113(10):707–712. doi:10.1093/qjmed/hcaa202
30. Adu MK, Wallace LJ, Lartey KF, et al. Prevalence and correlates of likely major depressive disorder among the adult population in Ghana during the covid-19 pandemic. Int j Environ Res Public Health. 2021;18(13):7106. doi:10.3390/ijerph18137106
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.