Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Factors Associated With Alcohol Use Disorder Among People Living With HIV/AIDS Attending Art Clinic, Mizan Tep University Teaching Hospital, South West Ethiopia
Authors Gebre BB ![]()
Received 20 June 2019
Accepted for publication 10 September 2019
Published 10 October 2019 Volume 2019:11 Pages 239—245
DOI https://doi.org/10.2147/HIV.S220211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Bereket Beyene Gebre
School of Nursing, College of Medicine and Health Science, Hawassa University, Hawassa, Ethiopia
Correspondence: Bereket Beyene Gebre
School of Nursing, College of Medicine and Health Science, Hawassa University, Hawassa, Ethiopia
Email [email protected]
Introduction: Alcohol use is a major public health concern in global settings. It is very common among people living with HIV/AIDS, leading to physical and mental complications.
Objective: To assess the magnitude of alcohol use and factors among HIV/AIDS positive adults visiting ART clinic at Mizan Tep University Teaching Hospital (MTUTH), Southern Ethiopia from October 2017 to December 2017.
Methods: A facility based cross-sectional study was conducted with a sample of 332 HIV positive adults who came to ART clinic at MTUTH using systemic random sampling technique. Data were entered into EPidata 3.1 version and then analyzed by SPSS version 20. Binary logistic regressions have been used to identify the association between an independent variable with the dependent variable.
Result: A total of 332 participants were enrolled in the study with the prevalence of alcohol use disorder (AUD) of 18.4%. Factors associated with alcohol use disorder were sex AOR=3.48 (95% CI: 1.27, 9.59), cigarette smoking AOR=5.12 (95% CI: 4.02, 8.61), “khat” chewing AOR=3.23 (95% CI: 2.06.6.89), and CD4 count of 0–200 AOR = 19.49 (95% CI: 1.74, 218.4).
Conclusion: The prevalence of alcohol use disorder was high. It is independently associated with male patients, cigarette/tobacco smokers, khat chewers, and low CD4 count.
Keywords: magnitude, alcohol use disorder, factors
Introduction
Human immune virus (HIV) is a virus affecting more than 60 million people since the epidemic began.1 In 2013 an estimated 35.0 [33.2–37.2] million people were living with HIV worldwide. Sub-Saharan Africa is home to only 12% of the global population, yet accounts for 71% of the global burden of HIV infection.2
Ethiopia is one of the Sub-Saharan African countries where there is a high rate of HIV/AIDS infection, next to South Africa and Nigeria. The Ethiopia Demographic Health Survey (EDHS) in 2011 indicated that the Gambela region had the highest incidence of HIV/AIDS at 6%.3 Alcohol is a psychoactive substance with dependence-producing properties that has been widely used in many cultures for centuries. Harmful use of alcohol causes a large number of health problems as well as social and economic burden in societies.4
Alcohol use disorders among people living with HIV/AIDS (PLWHA) seems to be 2–4 times higher than those disorders in the general population.5
The studies also reveal that in Sub-Saharan African countries, particularly in Nigeria, infectious diseases make up 50% of the overall alcohol-attributable disease burden.6,7
Alcohol use among HIV patients plays an important role in health outcomes and complicates the infection process by contributing to co-morbid diseases and drug interactions. It also increathe likelihood of opportunistic infection among ART users. Alcohol consumption has also been shown to decrease adherence and effectiveness to highly active antiretroviral therapy (HAART). It has effects on the liver, which affects drug metabolism, enhancing viral load. In addition, it has effects on certain clinical and laboratory parameters, resulting in poor clinical outcome.8,9 So, identifying certain factors affecting alcohol abuse were amendable to intervene. The identification of these factors may be useful in the implementation of actions aimed at controlling alcohol use and providing relevant information for detecting individuals at a higher risk of adverse clinical outcomes.
Objectives
General Objective
To assess the magnitude and associated factors of alcohol use disorder among PLWHA attending ART clinic at MTUTH, Southwest Ethiopia, 2017.
Specific Objective
To determine the magnitude of alcohol use disorder among PLWHA attending ART clinic, MTUTH, Southwest Ethiopia, 2017.
To identify associated factors with alcohol use among PLWHA attending ART clinic, MTUTH, southwest Ethiopia, 2017.
Methodology And Materials
Study Area And Period
The study was conducted at Mizan Tep University Hospital from October 10 to December 9, 2017, which is located in the Southern Nation Nationality People Region (SNNPR) of Ethiopia. It is 832 km from Hawassa, the capital city of the region. It is 588 km from Addis Ababa, which is the capital city of the country. It provides different services for outpatient and inpatient population from SNNPR and the neighboring regions in Ethiopia, Gambela, and Oromia.
Study Design
An institutional based cross-sectional study design was used.
Source Population
All HIV positive patients who had follow up at ART Clinic in MTUTH, southwest Ethiopia during the data collection period.
Study Population
Those sampled HIV positive patients who attended the ART clinic during the study period in the hospital.
Eligibility Criteria
Inclusion Criteria
Sampled HIV positive patients with age greater than or equal to 18 years were included in the study.
Exclusion Criteria
Sampled patients who were unwilling to give informed consent or who were severely ill.
Sample Size Determination
The required sample size was calculated using a single population proportion formula. The proportion of alcohol use disorder among PLWHA was taken from a cross-sectional study done at Jimma in 2012, i.e., 32.6%10 with 5% marginal error and 95% confidence interval (CI) of certainty (alpha=0.05).
where: n= sample size, Z α/2= critical value=1.96
P= prevalence of alcohol use among PLWHA=0.326 (32.6%)
d= precision (marginal error) =0.05
Therefore, n = (Zα/2)2 P (1-P) / d2, n = (1.96)2 *0.326 (1 -0.326)/ (0.05)2 =338
Since the total number of HIV positive patients visiting the ART clinic at HUCSH is <10,000, we used correction formula to know the final sample size as follows:
 where: ni = Initial sample size
where: ni = Initial sample size
nf = Final sample size

N = Total number of PLWHA visiting ART clinic

Ten percent of the calculated value of non-respondents will be 30.2.

Sampling Technique
Study participants were selected by a systematic sampling method that involved drawing those ART patients having follow-up in the ART registration book by establishing the sampling frame. The sample size for the study was 332 patients who were selected by systematic random sampling, calculating sampling interval K= (N/Tsz). N denotes total numbers of patients having ART follow-up during the study period in MTUTH, and was 1024, and Tsz is the total sample size. So, every 3rd patient was selected from the sampling frame. The sampled ART outpatients were present and exit interviews were carried out.
Study Variables
Dependent Variable
Alcohol use disorder.
Independent Variables
Age, sex, marital status, occupational, educational status, religion, ethnicity, living condition, and income.
Stage of HIV, year of serostatus, CD4 count, viral load, HIV/AIDS stage, on ART or not, social support and HIV related stigma.
Substance use: Tobacco, khat, cocaine, alcohol.
Data Collection Instruments
Data were collected by a semi-structured self-administered questionnaire prepared in English and translated into Amharic and retranslated to English to ensure its consistency. The questionnaires are adopted and modified from a WHO substance use survey questionnaire. It consists of socio-demographic variables, substance use, health status, and stigma related questions. The structured questioner, Oslo-3 social support scale, perceived HIV stigma scale and Alcohol Use Disorder Identification Test (AUDIT) was used to assess alcohol use disorder. Supervision was done while data collectors collected data and the information was checked for completeness and internal consistency.
Data Processing And Analysis
Data were checked and coded for completeness and entered into Epidata version 3.1, then Statistical Package for Social Sciences (SPSS) version 20 was used for analysis. Both descriptive and inferential statistical procedures were undertaken. Tables and figures were used to present the data. A binary logistic regression model was used to identify factors associated with alcohol use disorder. Crude and adjusted odds ratios with 95% confidence interval were used to determine the strength of association between dependent and independent variables. Variables with P value <0.05 were considered as significant.
Operational Definition
Social drinker: The total AUDIT score of the drinker is 1–7.
Hazardous drinking: The total AUDIT score of the drinker is 8–15.
Harmful drinking: The total AUDIT score of the drinker is –19.
Alcohol dependence: The total AUDIT score of the drinker is 20–40.
Alcohol use disorder: A patient who scored AUDIT scores >8.
Poor support: Those who score <8 in Oslo-3 Social Support Scale (OSS-3).
Perceived stigma: Those who score >11 in HIV Stigma Scale.
Dissemination And Utilization
The result from this study was disseminated to MTUTH.
Ethical Consideration
Ethical clearance was obtained from Mizan Aman Health Science College and permission was obtained from MTUTH. All participants of the study signed an informed consent after the objectives of the study had been elaborated clearly. All participants had the right to refuse.
Results
A total of 332 participants were enrolled with a response rate of 100%. Most of the participants, 184 (55.4%), were females. The mean age of the respondents was 37.89 (SD 10.27). Ninety-five (28.6%) were Kaffa and 66 (19.9%) Amhara by ethnicity. The educational level of 126 (38%) respondents was found to be primary school (see Table 1).
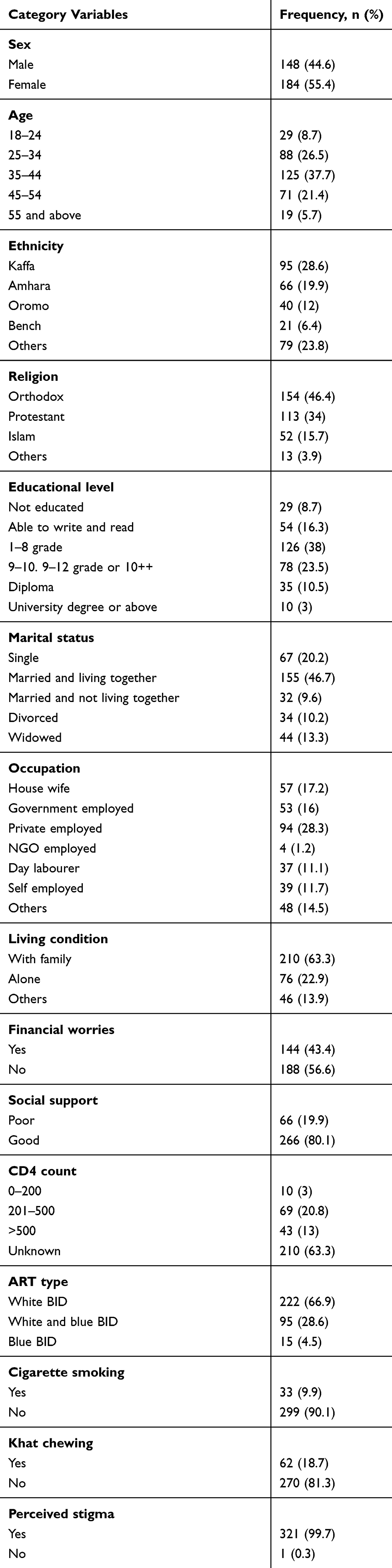 |
Table 1 Socio-Demographic And Clinical Variables Of AUD Among PLWHA Attending ART Clinic At HUCSH In 2017 |
Prevalence Of Alcohol Use Disorder
The prevalence of alcohol use disorder was found to be 18.4%. The prevalence of social drinkers, hazardous drinkers, harmful alcohol users, and alcohol dependents was computed to be 32.2%, 11.4%, 1.8%, and 0.9%, respectively. Most of the respondents, 178 (53.6%) were non-alcohol users.
Associated Factors For AUD Among PLWHA
In the binary logistic regression, sex, age, education level, occupation, cigarette smoking, “khat” chewing, and CD4 count were significantly associated with alcohol use disorder. However, in multivariate analysis, sex, cigarette smoking, khat chewing, and CD4 count were independently associated with alcohol use disorder (see Table 2).
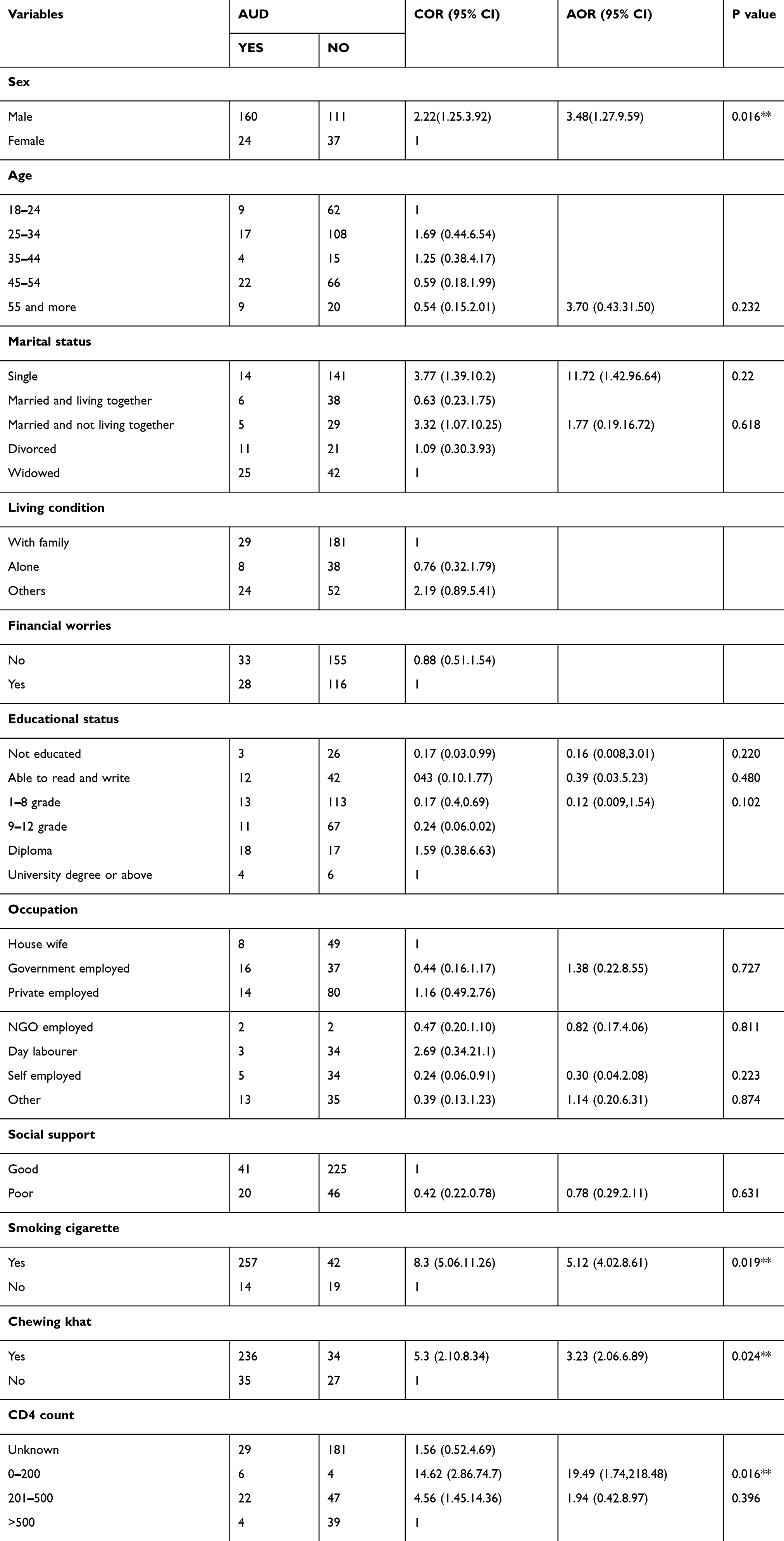 |
Table 2 Bivariate And Multivariate Logistic Regression: Factors Independently Associated With AUD Among PLWHA Attending ART Clinic At MTUTH In 2017 |
Discussion
This study reveals that the prevalence of alcohol use disorder (AUD) was 18.4%, which is higher than the figure from a similar study done in 2015 at Bishoftu in Ethiopia, which was 14.2%.11 It was in line with that of a Jimma study, which found 32.6% of PLWHA to have alcohol use disorder.10 Therefore, this study gives additional evidence for designing interventions for alcohol use disorder among HIV infected patients due to being uniformly distributed throughout the southwestern part of the country.
An overview of global studies on the topic reveals that the prevalence ranges from 1.4% in Uganda to 49.5% in Brazil.12 The possible explanation for this might be cultural, socioeconomic and contextual differences. Sample size variation and instruments used to assess AUD differences are also possible reasons for the dissimilarity.12
Our study showed that males had 3 times higher risk for AUD than females. This result is higher than the studies done in Jimma and Nigeria.10,13 A possible explanation for this is the cultural and economic dominance of males in Africa.
This study also showed that those who smoke cigarettes had 5 times greater risk than nonsmokers to alcohol use disorder. This finding is higher than the study done in Bishofitu and Jimma in Ethiopia.10,14 Therefore, this study gives additional evidence for planning appropriate intervention in smoking among HIV infected patients.
In this study, participants who chew khat were 3 times more likely to had AUD as compared to those non khat chewers. This finding is higher than the study done in Jimma, Ethiopia.14 This might be due to one of more “khat” growing region and a chewing practice is prevalent region in Ethiopia. So, designing strategies will be vital to minimizing Khat chewing prevalence since it is associated with alcohol use disorder.
This study also indicated that PLWHA having a CD4 count of <200 were 19 times more likely to have alcohol use disorder when compared to PLWHA having >500 CD4 count. This result is also supported by studies done in Brazil in 2013. This is due to the direct immune suppressive effect of alcohol.12
Conclusion
The prevalence of alcohol use disorder was high. Alcohol use disorders were independently associated with male patients, cigarette smokers, khat chewers, and those with low CD4 count.
Recommendations
Providing health education about alcohol use disorder and its devastating effect of alcohol in the health institution as well in the community will be essential to decrease those who have alcohol use disorder. In addition, proper screening of alcohol use disorder among patients with HIV/AIDS is crucial. Moreover, strengthening the referral linkage with psychiatric units for psycho-behavioural therapy will decrease the burden of the problem and bring changes for ART patients.
Limitation
There may be recall bias and social desirability bias.
Ethical Statement
Mizan Aman Health Science College ethical review committee approved this study to be conducted in MTUTH.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; AUDIT, Alcohol Use Disorder Identification Test; HIV, human immunodeficiency virus; HAART, highly active antiretroviral therapy; MTUTH, Mizan Tep University Teaching Hospital; OSS-3, Oslo-3 Social Support Scale; PLWHA, people living with HIV/AIDS; UNICEF, United Nations International Children’s Emergency Fund; WHO, World Health Organization.
Availability Of Data And Materials
The data supporting this study will be available from the editorial office if necessary and will be available from the corresponding author.
Acknowledgments
First, I would like to acknowledge Mizan Aman Health Science College for the provision of the ethical clearance. I would also like to acknowledge Mizan Tep University Teaching Hospital for providing permission for the study to be conducted.
My gratitude also goes to data collectors and friends for all their support throughout the gathering of the data.
Disclosure
The author reports no conflicts of interest in this work.
References
1. UNAIDS/WHO, AIDS Epidemic Update. Geneva, Switzerland: UNAIDS/WHO 2001; December 2001.
2. Joint United Nations Programme on HIV/AIDS (UNAIDS). The Gap Report ISBN: 978-92-9253-062-4; 2014
3. Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa (Ethiopia) and Calverton (MD): Central Statistical Agency and ICF International; 2012
4. WHO. Global Status Report on Alcohol and Health-2014. WHO: Geneva.
5. Mariana KB, Carlin R, Shenghan L, et al. Alcohol Use Accelerates HIV Disease Progression. 2009;26(5):5118.
6. Hahn JA, Woolf-King SE, Muyindike W. Adding fuel to the fire: alcohol’s effect on the HIV epidemic in Sub-Saharan Africa. Current HIV/AIDS Rep. 2011;8(3):172–180. PMID: 21713433. doi:10.1007/s11904-011-0088-2
7. Farley J, Miller E, Zamani A, et al. Screening for hazardous alcohol use and depressive symptomatology among HIV-infected patients in Nigeria: prevalence, predictors, and association with adherence. J Int Assoc Phy- Sicians AIDS Care. 2010;9(4):218–226. doi:10.1177/1545109710371133
8. Pandrea I, Happel KT, Amedee AM, Bagby GJ, Nelson S. Alcohol’s Role in HIV Transmission and Disease Progression. Alcohol Res Health. 2010;33(3):203–218.
9. Braithwaite R, Bryant KJ. Influesnce of alcohol consumption on adherence to and toxicity of antiretroviral theraphy and survival. Alcohol Res Health. 2010;33(33):280–286.
10. Soboka M, Tesfay M, Tolu G, Hanlon C. Alochol use disorder and associated factors among people liv- ing with HIV who are attending services in Southwest Ethiopia. BMC Res Notes. 2014;7:828. PMID: 25417542. doi:10.1186/1756-0500-7-828
11. Bultum JA, Yigzaw N, Demeke W, Alemayehu M. Alcohol use disorder and associated factors among human immunodeficiency virus infected patients attending antiretroviral therapy clinic at Bishoftu General Hospital. Oromiya Region, Ethiopia. PLoS ONE. 2018;13(3):e0189312. doi:10.1371/journal.pone.0189312
12. Silva CM, et al. Alcohol use disorders among people living with HIV/AIDS in Southern Brazil. BMC Infec Dis. 2017;17:263. doi:10.1186/s12879-017-2374-0
13. Goar SG, Audu MD, Abbir MT, Dochalson E. prevalence and sociodemographic correlates of alcohol use disorder among HIV patients. AfrJ Drug Alcohol Stud. 2011;10(1):42–47.
14. Znenbe Y, Negash A, Feyissa G, Krahl W. Alcohol use disorders and its associated factors among pychatric outpatients in Jimma University specialized hospital Southwest Ethiopia. J Alcohol Drug Depend. 2015;3:3.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.