Back to Archived Journals » Patient Intelligence » Volume 8
Factors associated with adolescent–parent communication of reproductive health issues among high school and preparatory students in Boditi town, Southern Ethiopia: a cross-sectional study
Authors Fanta M, Lemma S, Sagaro GG, Meskele M ![]()
Received 8 October 2015
Accepted for publication 14 June 2016
Published 14 October 2016 Volume 2016:8 Pages 57—70
DOI https://doi.org/10.2147/PI.S97838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Muluken Fanta,1 Seblewengel Lemma,2 Getu Gamo Sagaro,3 Mengistu Meskele3
1Wolaita Zone Health Department, Southern Nations Nationalities and People Region State, Wolaita Sodo, 2Addis Continental Institute of Public Health, Addis Ababa, 3School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Background: Communication from parents on reproductive health (RH) issues with their adolescent children plays a great role in preventing morbidity and mortality associated with RH. The majority of Ethiopian adolescents do not communicate on these matters with their parents. This study aimed to identify the factors that affect communication on RH issues between parents and high school and preparatory students in Boditi town, Wolaita Zone, Southern Ethiopia.
Objectives: The aim of this study was to assess the level of communication, and factors affecting communication between high school and preparatory students with their parents on RH issues in Boditi town.
Methods: A school-based cross-sectional study was conducted from February 10 to February 20, 2015 among high school and preparatory students in Boditi town. A multistage sampling technique was used to sample the study participants. Data were collected by using a self-administrated structured questionnaire, which was developed based on previous literature incorporating all variables to be assessed. Data were entered and analyzed through Epi Info version 3.5.4 and SPSS version 16.0, respectively.
Results: This study revealed that 40.70% (95% confidence interval [CI] 37.2%–44.2%) of students discussed RH issues with their parents. Factors such as being a female student (adjusted odds ratio [AOR] =1.42; 95% CI 1.00–1.95); being in the 10th grade (AOR =1.62; 95% CI 1.04–2.50); having a mother who was educated (able to read and write only; AOR =0.56; 95% CI 0.34–0.91), who had completed secondary education (AOR =0.43; 95% CI 0.22–0.80), or who had completed above secondary education (AOR =0.37; 95% CI 0.20–0.72); knowledge on RH issues (AOR =1.37; 95% CI 1–1.9); and perceived importance of discussing RH issues (AOR=3.24, 95% CI 2.00–5.18) significantly affect the communication between parents and students on RH issues.
Conclusion: This study showed that only a low proportion of students communicated on RH issues with their parents. Parents should focus on both male and female students equally, in discussing RH matters and in improving their communication skills, and should be transparent in the community to encourage open discussion among family members particularly with their adolescent children.
Keywords: communications, reproductive health issues, students, parents
Introduction
Parent communication is the part of the process of change within a family and can be positive or negative, effective or ineffective. It is very important for parents to be able to communicate openly and effectively with their adolescents. Open, effective communication benefits not only adolescents but also every member of the family.1 Many adolescents lack strong and stable relationships with their parents or other adults, which are necessary to openly discuss reproductive health (RH) concerns. As a result, many teenagers do not have access to reliable information regarding their RH needs. In most cultures, parents and family members are an influential source of knowledge, beliefs, attitudes, and values for children and young people. Parents often have the power to guide children’s development in sexual health matters, encouraging them to practice reasonable sexual behavior and develop good personal decision-making skills.1,2
Even though parents are the main sources of information for RH issues, there remains a silence between many parents and their adolescent children on these matters. Studies have shown that only 46%, 20%, and 20% of parents in the US, Lesotho, and Ethiopia, respectively, had discussed such issues with their adolescents.3–5 Many adolescents discuss RH issues with their peers (who may or may not have a proper knowledge on these matters) and as a result gain patchy knowledge. This misinformation can make adolescents vulnerable to unprotected sex, unwanted pregnancy, sexually transmitted diseases, and unsafe abortions.6
A study in Tanzania revealed that most families had some sort of communication about sexual health. These communications were usually initiated by parents and rarely by young people and was characterized by warnings or threats. The topics for discussion were mainly about abstinence, unplanned pregnancy, and HIV/AIDS. These communications reflected the worries parents had about their children’s sexual health.7 The consequence of adolescent sexual behavior is an enormous burden both for the adolescent and for the society. The problem is not that adolescents are sexually active but rather that they are inadequately prepared and guided in developing responsible sexual behaviors. While families have a major influence on other behaviors, they are not powerful in shaping adolescents’ sexual behavior due to sociocultural and religious beliefs, thereby affecting the discussion of sexual and RH issues with adolescents.8,9
Studies conducted in different parts of Ethiopia showed that young people aged 15–19 years were more likely to report parent communication compared to other age groups, and factors such as grade, age of students, mother’s educational status, and adolescents who ever got RH information were found to affect communications of RH matters with parents.10–12 In addition, a study conducted in Dire Dawa, Ethiopia showed that cultural taboo, shame, and lack of communication skills of parents majorly hinders communication between parents and adolescents.13 Moreover, due to lack of appropriate RH services, adolescents suffer from a number of RH problems. Every year, 2.5–3 million adolescents globally acquire sexually transmitted infections (STIs). This implies that approximately one out of every ten adolescents, even in developed countries, acquire STIs each year. Also, more than one million teenagers become pregnant each year, out of which 60% are unwanted pregnancies resulting from unprotected sexual intercourse.10 The significance of this study has helped to design appropriate interventions and programs to support and improve adolescents’ access to sexual and RH services to minimize many RH problems. Therefore, communication of RH issues with parents will equip them with the knowledge and skill to prevent different adverse RH problems. No studies have examined the factors that affect the communication of RH issues between high school and preparatory students and their parents in Boditi town and Wolaita Zone. Therefore, this study aimed to assess the communication that adolescents have with their parents on RH issues and associated factors that may help policy makers, program planners, and implementers to design appropriate interventions to address the RH issues of adolescents.
Methods
Study setting and period
The study was conducted in high schools and preparatory schools in Boditi town between February 10 to February 20, 2015. Boditi town is one of three administrative towns in Wolaita Zone, Southern Nations Nationalities and People Region State (SNNPR), Ethiopia, and has five kebeles. According to household and population census, the total population of the town is estimated to be approximately 35,116 of which 17,874 are female and 17,242 male. The town has one private primary school, two governmental primary schools, and two governmental secondary schools (Boditi Secondary and Preparatory School and Meles Zenawi Secondary School).14
Study design, participants, and sample size determination
A school-based cross-sectional study was conducted. The study population included all students attending from grade 9 to grade 12 in Boditi Secondary and Preparatory School and from grade 9 to grade 10 in Boditi Meles Zenawi Secondary School in 2007 Ethiopian calendar (EC) academic year. There are approximately 4,177 students (grade 9 [12 sections], grade 10 [18 sections], grade 11 [12 sections], and grade 12 [16 sections]) in Boditi Secondary and Preparatory School and 1,362 students (grade 9 [10 sections] and grade 10 [8 sections]) in Meles Zenawi Secondary School making a total of 5,539 students in the town in the 2007 EC academic year. All students who were attending secondary and preparatory schools at the time of data collection were included, and students who were in class but feeling sick were excluded.
Sample size was calculated using single-population proportion formula with the following assumptions: 36.9% proportion of communication on RH,11 5% margin of error, 95% confidence level, design effect of 2, and a 10% nonresponse rate. The calculated sample size was 788.
Sampling and data collection procedure
The study participants were identified by multistage sampling technique. Initially students of both schools were stratified by grade, from grades 9 to 12, and from each grade, sections and study participants were selected by using simple random sampling method. To select the study participants, student’s roster was used as a sampling frame, and to determine the number of students from each grade, proportionate allocation to their size was used.
Data were collected using a pretested, structured, and self-administered questionnaire with close-ended questions (Table S1). The questions included in the questionnaire were prepared based on various related reviews found in the literature, and variables to be measured were identified.5,9,12,13 The questionnaire was prepared in English in the beginning and then translated into Amharic and back to English to ensure consistency. Finally, the data collection was conducted by five individuals who had completed grade 10 and who had experience in data collection. To ensure the quality of data, supervisors and the data collectors were trained for 2 days on how to approach the study subjects, the objective of the study, the content of the questionnaire, selection of the study subjects, and issues related to communication on RH.
Data management and analysis
The completed questionnaires were collected back and checked for completeness and those with any missing data were rejected. The data were coded and entered into Epi Info Version 3.5.4. and then exported and analyzed using SPSS version 16. Data were checked and cleaned for its completeness and errors in coding and entering before analysis. The study population was explained based on relevant variables, frequency tables, graphs, and summary statistics. Dependent variables were computed from responses to eight RH-related topics and were dichotomized as “Yes” (coded as “1”) and “No” (coded as “0”). Then, all variables with a P-value ≤0.2 in the bivariate analyses were further analyzed by multivariate logistic regression model. Variables with a P-value <0.05 in the multivariate analysis were considered as significant predictors.
The definitions of the operational terms are as follows:
- Communication on RH issues: students who discussed at least two RH issues (eg, contraception, STIs/HIV/AIDS, sexual intercourse, unwanted pregnancy, avoiding premarital sex, condom, changes during puberty, and menstrual cycle) were considered to have communicated on RH issues.
- Parents: parents in this study refers to biological parents, step parents, or foster parents but does not include elder siblings.
- Knowledgeable on RH: a student whose cumulative response rate for six RH-related questions was greater than or equal to the summed mean score value is considered to be knowledgeable on RH.
Ethical consideration
This study was approved by the Ethics Review Board of Wolaita Sodo University, School of Public Health, College of Health Science and Medicine. At the time of data collection, verbal consent was obtained from the students, or their parents if they are a minor, to confirm whether they were willing to participate or not. Those who were not willing to participate had the sole right to do so. Confidentiality of the responses was ensured throughout the research process by gathering participants in different classes by sex during the time of data collection.
Results
Sociodemographic characteristics of respondents
A total of 755 students completed the questionnaires, among whom 740 students completely filled out the questionnaires, with a response rate of 95.81%. Fifteen questionnaires were rejected due to incomplete data. Of the total 740 respondents, 385 (52%) were males. The mean age (±SD) of the respondents was 16.28±1.59 years. Most of the students (266, 35.90%) were in grade 10 followed by grade 9 (230, 31.10%). The majority of respondents (684, 92.40%) belonged to the Wolaita ethnic group and 465 (62.80%) were Protestant by religion. A total of 588 respondents (79.50%) were living with both parents. The majority of the respondents’ parents (635, 85.80%) were living together. The mean (±SD) family size of respondents was 6.29±1.94. Nearly 188 (25.40%) participants’ mothers were illiterate, and 300 (40.50%) participants’ mothers were housewives. A total of 166 (22.40%) participants’ fathers were degree holders, and 242 (32.7%) participants’ fathers were government employees (Table 1).
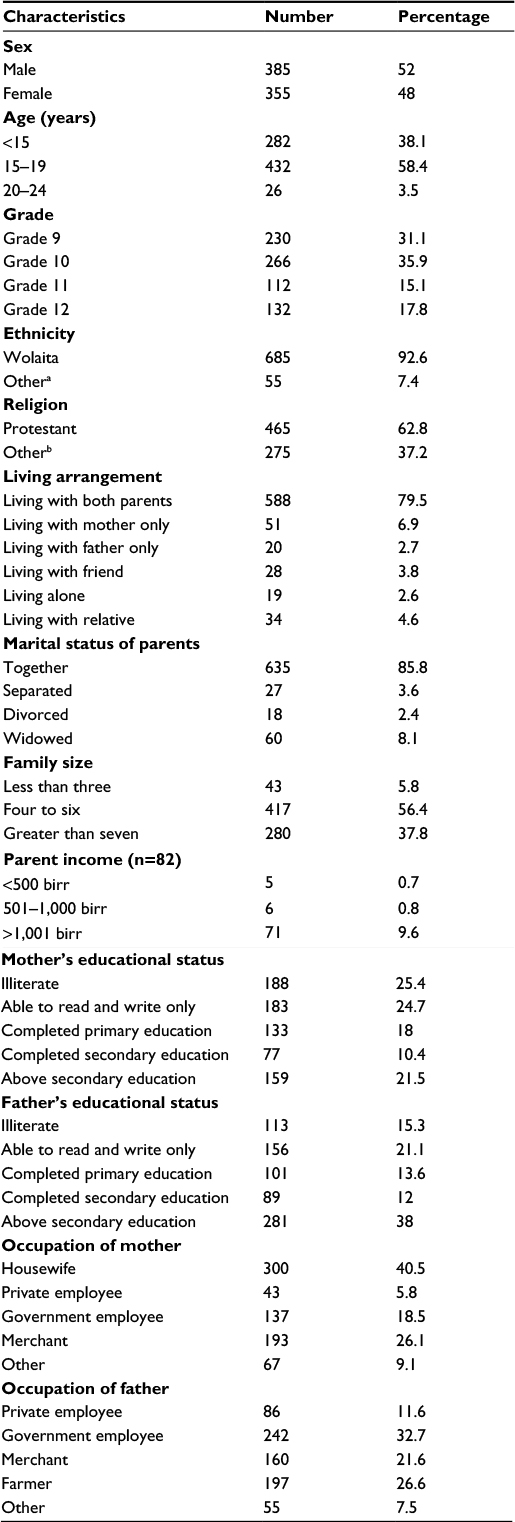 | Table 1 Sociodemographic characteristics of secondary and preparatory students in Boditi town, Wolaita Zone, SNNPR, Ethiopia; March 2015 (n=740) Notes: aKambata Tambaro, Gammogofa, etc; bCatholic, Orthodox Christian. Abbreviation: SNNPR, Southern Nations Nationalities and People Region State. |
Knowledge on selected RH issues
A total of 527 (71.20%) respondents knew about their first menstrual period (menarche), and the reported mean age (±SD) of menarche was 13.31±1.83 years. Of the respondents, 405 (54.70%) knew about STIs (Figure 1) and 582 (78.60%) about contraceptive methods, among whom 286 (49.10%) knew about injectable contraception, followed by the contraceptive pill 278.24 (37.60%) (Figure 2).
 | Figure 1 Diagrammatic presentation of knowledge of secondary and preparatory students on sexually transmitted infections. Notes: Students from Boditi town, Wolaita Zone, SNNPR, Ethiopia; March 2015 (n=740). Abbreviations: SNNPR, Southern Nations Nationalities and People Region State; LGV, lymphogranuloma venereum. |
 | Figure 2 Diagrammatic presentation of knowledge of secondary and preparatory students on contraceptive methods. Notes: Students from Boditi town, Wolaita Zone, SNNPR, Ethiopia; March 2015 (n=740). Abbreviations: SNNPR, Southern Nations Nationalities and People Region State; IUCD, intrauterine contraceptive device. |
Communications on RH matters
The majority of respondents (597, 80.70%) accepted the importance of discussing RH issues with their parents. However, only 301 (40.7%) students had discussed with either of their parents on at least two topics of RH issues. More than two-thirds (439, 59.3%) of the respondents reported that they had discussed contraceptive methods. Moreover, 496 (67%) of the respondents had discussed STDs/HIV/AIDS, and half of the respondents 373 (50.4%) on sexual intercourse. In addition, 411 (55.5%) respondents claimed to have discussed unwanted pregnancy; 213 respondents (51.80%) with friends, followed by 109 respondents (26.50%) with their mother (Table 2). The reasons reported by the respondents for not discussing RH issues were cultural taboos, lack of parents’ knowledge on such topics, shame, lack of communication skills, and difficulty faced while discussing the issues (Table 3). Nearly 309 (41.80%) of the respondents preferred to discuss RH issues with their friends, 185 (25%) preferred their mothers, 133 (18%) their fathers, 72 (9.70%) their brothers, 37 (5%) their sisters, and four (0.50%) preferred others.
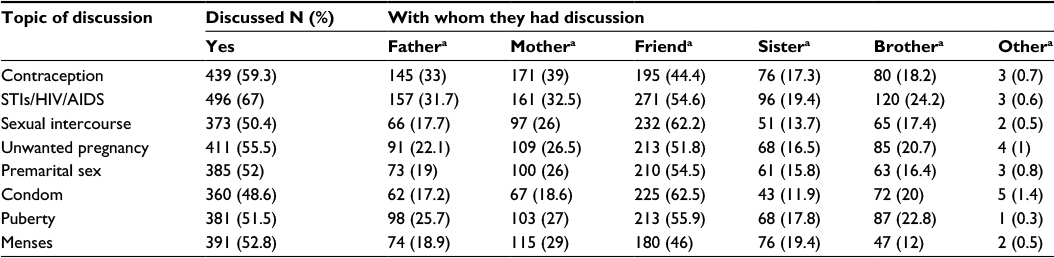 | Table 2 Secondary and preparatory school students from Boditi town, Wolaita Zone, SNNPR, Ethiopia, and with whom they had discussions of different topics of reproductive health; March 2015 Notes: aMultiple responses were possible. Data presented as n (%). Abbreviations: SNNPR, Southern Nations Nationalities and People Region State; STIs, sexually transmitted diseases. |
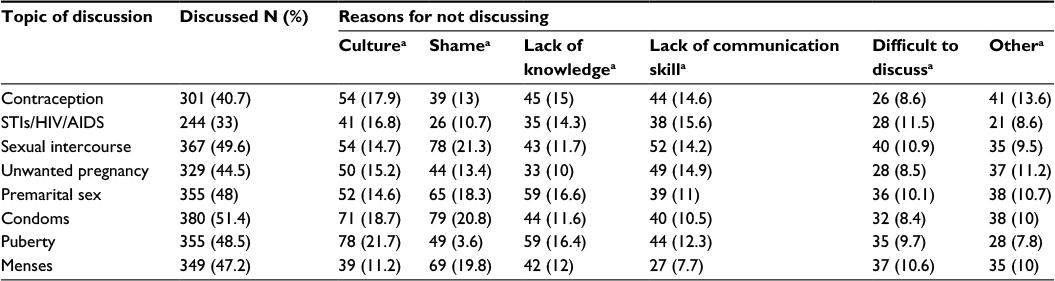 | Table 3 Major reasons by the secondary and preparatory students from Boditi administrative town, Wolaita Zone, SNNPR, Ethiopia for not discussing reproductive health matters with parents; March 2015 Notes: aMultiple responses were possible. Data presented as n (%). Abbreviations: SNNPR, Southern Nations Nationalities and People Region State; STIs, sexually transmitted diseases. |
Factors associated with RH issues
Bivariate analysis
Bivariate analysis was conducted for sociodemographic variables, family factors, student’s knowledge on RH issues, grade of students, living conditions of students, and students perceived importance of discussing RH matters. P-value <0.05 was considered significant for independent variables.
The results show that being female (crude odds ratio [COR] =1.42; 95% confidence interval [CI] 1.05–1.90), being in grade 10 (COR =1.53; 95% CI 1.06–2.20), having mothers who had completed secondary education (COR =0.55; 95% CI 0.31–0.98) and above secondary education (COR =0.58; 95% CI 0.30–0.91), mothers being housewives (COR =1.85; 95% CI 1.04–3.30), students being knowledgeable on RH matters (COR =1.55; 95% CI 1.15–2.00), and students perceived importance of discussing RH matters (COR =2.98; 95% CI 1.94–4.58) were significant variables that affect communication between the students and parents. All variables with a P-value ≤0.2 in the bivariate analyses were further analyzed by multivariate logistic regression mode (Table 4).
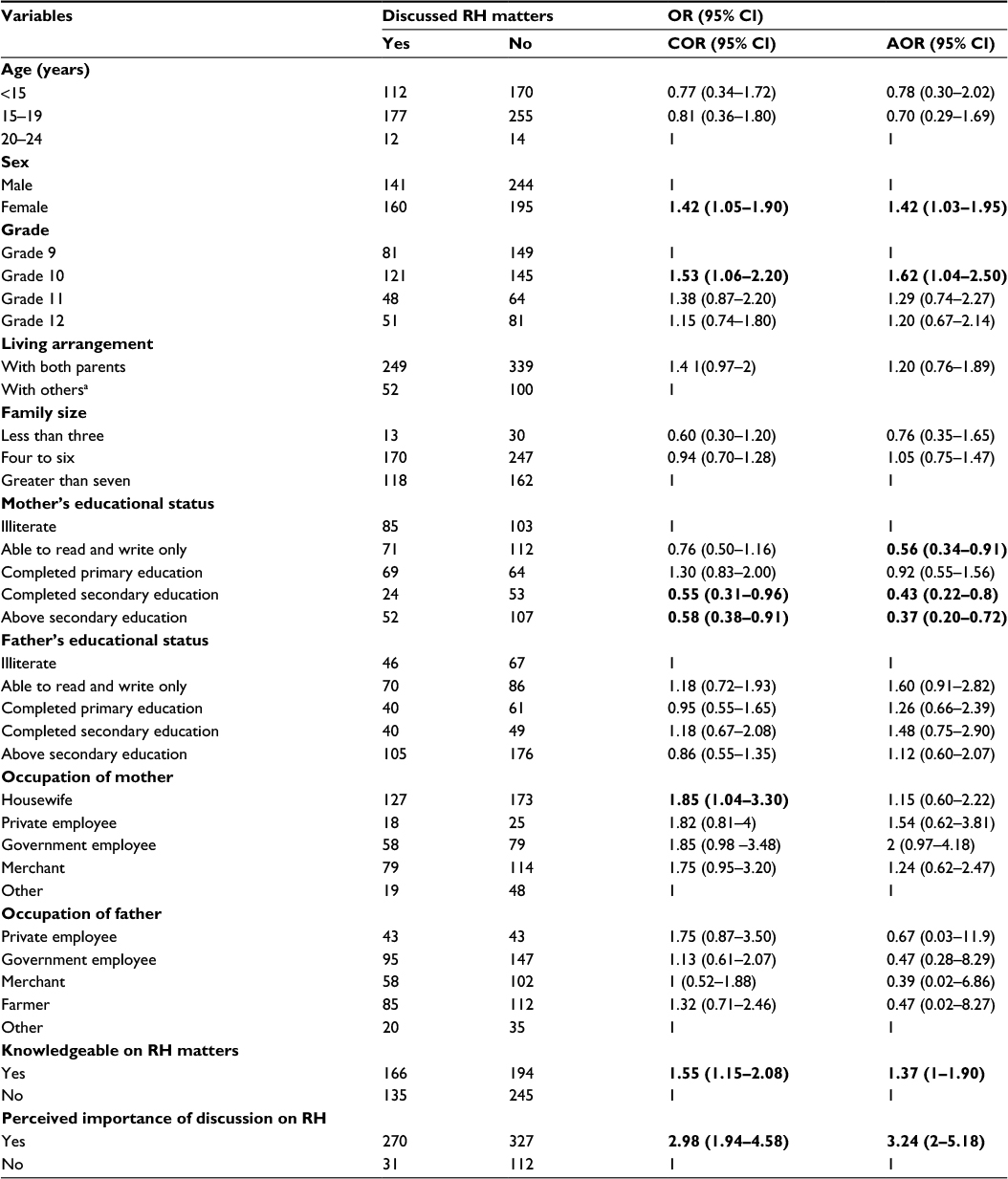 | Table 4 Bivariate and multivariate analysis of factors associated with communication of RH issues between parents and secondary and preparatory schools students from Boditi town, Wolaita Zone, SNNPR, Ethiopia; March 2015 Notes: Significant values are given in bold font; auncle, aunt, grandfather, and grandmother. Abbreviations: CI, confidence interval; OR, odds ratio; COR, crude odds ratio; AOR, adjusted odds ratio; RH, reproductive health; SNNPR, Southern Nations Nationalities and People Region State. |
Multivariate analysis
The results of multiple logistic regression model showed that being female, being in grade 10, having mothers able to read and write only, mothers who had completed secondary education, mothers whose educational status was above secondary education, being knowledgeable on RH issues, and the perceived importance of students to discuss RH issues with parents are factors significantly associated with communication of RH issues with parents.
Females were 1.42 times more likely to discuss RH issues with their parents compared to males (adjusted odds ratio [AOR] =1.42; 95% CI 1.03–1.95). Grade 10 students were 1.62 times more likely to discuss RH issues with their parents when compared to grade 9 students (AOR =1.62; 95% CI 1.04–2.50). Students whose mothers were able to read and write only, who had completed secondary education, and who had completed above secondary education were less likely (AOR =0.56; 95% CI 0.34–0.91; AOR =0.43; 95% CI 0.22–0.80; AOR =0.37; 95% CI 0.20–0.72, respectively) to discuss RH issues with their parents compared to those whose mothers were unable to read and write. Students who were knowledgeable on RH matters were 1.37 times more likely to discuss when compared to those who were not knowledgeable (AOR =1.37; 95% CI 1.10–1.90). Students who perceived the importance of discussing RH issues with their parents were 3.24 times more likely (AOR =3.5; 95% CI 2.00–5.18) to discuss RH issues with their parents compared to those who did not perceive the importance of discussion (Table 4).
Discussion
This study showed that 40.70% (95% CI 37.2–44.2) of students had discussed at least two topics of RH issues with either of their parents. This finding is higher than that of studies conducted in Benishangul Gumuz (29%), Debremarkos (36.90%), Dire Dawa (37%), and Lesotho (20%) but lower than the study conducted in Zimbabwe (44%) and Malawi (74%).10,12,13,15 This may be due to demographic and cultural difference and difference in accessing RH information.
Being female, being in grade 10, perceived importance of discussing RH issues with parents, being knowledgeable on RH matters, having mothers who were able to read and write only, having mothers who had completed secondary education, and having mothers who had completed above secondary education were found to be the factors significantly associated with communication of RH matters with parents.
Since adolescence is a transition period that is marked by profound changes in life cycle, adolescents can be engaged in different sexual health–related problems such as early pregnancy, abortion, and STIs. They engage in health-risking behaviors because they think that they are not vulnerable, due to a lack of knowledge. Their decision-making skills can be improved by providing appropriate and timely advice. Therefore, parents can be a source of information for their adolescents to make appropriate decisions. This study showed that only a low proportion of students communicated with their parents on RH issues, whereas the majority of students had no communication, which can make them vulnerable to a variety of poor sexual and RH outcomes.
This study showed that female students were more likely to communicate with their parents than male students, which might be due to the fact that females spend more time in the home where they can easily access their parents. Grade 10 students were more likely to communicate, compared to grade 9 students, which might be due to the fact that parents have a special focus on these children and they fear that children of this age might engage in risky sexual behavior. Students who perceived the importance of discussing RH matters with their parents were more likely to engage in discussion, which could be due to their perceived importance to discussion. Students who were knowledgeable on RH matters were more likely to communicate with their parents, which might be due to their interest in knowing more about RH matters. Students whose mothers were able to read and write were less likely to communicate with their parents than those whose mothers were unable to read and write; this might be due to the fact that mothers who were educated spend most of their time outside the home (eg, workplace).
A study in Tanzania revealed that female students were more likely to communicate on RH matters with their parents due to a parental focus on abstinence and pregnancy avoidance for females, but not males.8 In line with this, our study showed that females were 1.42 times (AOR =1.42; 95% CI 1.03–1.95) more likely to communicate with their parents. This study revealed that grade 10 students were more likely to discuss RH issues with their parents compared to grade 9 students, which is different from the findings of the Debremarkos study in which grade 12 students were less likely to discuss RH issues with their parents.12
Students who were knowledgeable on RH matters were 1.37 times (AOR =1.37; 95% CI 1–1.90) more likely to discuss with their parents, which is in line with the Debremarkos study.12 Students who perceived the importance of discussing RH issues with their parents were 3.24 times (AOR =3.24; 95% CI 2–5.18) more likely to discuss RH issues than those who did not accept the importance, which is in line with the Debremarkos study.12 This might be due to the perceived importance of communications on RH issues. Students whose mothers were able to write and read only were 44% (AOR =0.56; 95% CI 0.34–0.91) less likely to discuss RH matters compared to students whose mothers were unable to read and write. This study also revealed that students whose mothers had completed secondary education were 57% (AOR =0.43; 95% CI 0.22–0.80) and students whose mothers were above secondary education were 63% (AOR =0.37; 95% CI 0.20–0.72) less likely to discuss RH matters compared to those whose mothers were unable to read and write. This is in line with a study conducted in Kenya, which showed that most educated mothers reported experiencing sociocultural and religious inhibitions that make them challenging to provide sex education to their daughters. Mothers also reported a reliance on the school system to provide sex education.16
Limitation of the study
Communication on RH, sexual behaviors, and attitude outcomes are based on self-reported information, which is subject to reporting errors and missed values. The study did not explore factors from parents’ perspective; this is a cross-sectional study and hence it was difficult to imply cause–effect relationship.
Conclusion and recommendation
This study showed that only a low proportion of students communicated on RH matters with their parents. Female students, grade 10 students, students knowledgeable on RH matters, and students who perceived the importance of discussing RH matters with parents were more likely to discuss RH issues with parents. Students whose mothers were able to read and write only, who had completed secondary education, and who had completed above secondary education were less likely to discuss RH issues with their parents. Most discussions regarding RH were held with friends, who may have no full understanding of RH issues. Culture, shame, and parents’ lack of knowledge about RH were frequently reported to be the barriers of discussion.
Parents should focus on both male and female students equally in discussing RH matters. Responsible bodies like district health office, town administrative office and others should equip parents with appropriate information, education, and communication material, and communication skill on RH-related issues and be transparent in the community to encourage open discussion among family members particularly with their adolescents. In addition, it is better to equip students with appropriate RH information several ways such as encouraging them to participate in different health clubs in school and outside school. Policy makers should initiate comprehensive family life education for students and parents in school, home, churches, mosques, and health facilities. In conclusion, further studies should be carried out from the parents’ perspective to identify factors that affect the discussion of RH issues between students and parents.
Acknowledgments
Our special thanks go to Wolaita Sodo University and Addis Continental Institute of Public Health for cooperation and support in different stage of the research process. We would like to extend our gratitude to Boditi town education unit for supporting us by providing available information, and thanks also go to study participants, data collectors, and supervisors.
Author contributions
Muluken Fanta conceived the study, obtained ethical clearance and permission for study, participated in the design of the study, and performed the statistical analysis. Seblewengel Lemma guided the research, involved in the design of the study, and performed the statistical analysis. Getu Gamo Sagaro and Mengistu Meskele involved in the design of the study and statistical analysis, and drafted the article and rechecked it critically for important intellectual content. All authors read and approved the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
Kristen Z. Parent–adolescent communication. Center for Effective Parenting. 2006;2(1). Available from: www.parenting-ed.org. Accessed August 29, 2016. | ||
Sime A, Wirtu D. Premarital sexual practice among school adolescents in Nekemte town, East Wollega. Ethiop J Health Dev. 2008; 22(2):167–173. | ||
Miller KS, Kotchick BA, Dorsey S, Forehand R, Ham AY. Family communication about sex: what are parents saying and are their adolescents listening? Family Planning Perspectives. 1998;30(5):218–235. | ||
Dittus AJ. Parent attitude to adolescent sexual behavior in Lesotho. African Journal of Reproductive Health. 2003;17(2):25–28. | ||
Taffa N, Haimanot R, Desalegn S, Tesfaye A, Mohamed K. Do parents and young people communicate on sexual matters? The situation of Family Life Education (FLE) in rural town in Ethiopia. The Ethiopian Journal of Health Development. 1999;13(3):205–216. | ||
Ministry of Youth, Sports & Culture of Ethiopia (MYSC). Youth Policy. Ethiopia: MYSC; 2005. Available from: www.Chilot.me. Accessed August 29, 2016. | ||
Wamoyi J, Fenwick A, Urassa M, Zaba B, Stones W. Parent-child communication about sexual and reproductive health in rural Tanzania: implications for young people’s sexual health interventions. Reprod Health. 2010;7:6. | ||
Kumi-Kyereme A, Awusabo-Asare K, Biddlecom A, Tanle A. Influence of social connectedness, communication and monitoring on adolescent sexual activity in Ghana. Afr J Reprod Health. 2007;11(3):133–149. | ||
Damalie, N. Communication between Mothers and Their Adolescent Daughters on the Subject of Sexuality and HIV/AIDS in Uganda. Gender issue research report series, number 14. Addis Ababa, Ethiopia: Organization for Social Science Research in Eastern and Southern Africa; 2001. | ||
Gebreyesus D. Assessing communication on sexual and reproductive health issues among high school students with their parents, Bullen Woreda, Benishangul Gumuz Region, North West Ethiopia. Ethiop J Health Dev. 2010;24(2):89–95. | ||
Sime A, Wirtu D. Premarital sexual practice among school adolescents in Nekemte town, East Wollega. Ethiop J Health Dev. 2008;22(2):167–173. | ||
Shiferaw K, Getahun F, Asres G. Assessing communication on sexual and reproductive health issues among secondary and preparatory students with their parents in Debremarkos. Reprod Health. 2014;11(1):2. | ||
Ayalew M, Mengistie B, Semahegn A. Communication of sexual and reproductive health issues among high school students in Diredawa. Reprod Health. 2014;11(1):77. | ||
Boditi Town Administration Office, Annual plan report. 2015. Available from: http://www.snnprlabourandsocial.gov.et/notes/NGO’s%20working%20with%20BOLSA.pdf. Accessed August 29, 2016. | ||
Federal Ministry of Health of Ethiopia. Standard on Youth Friendly Reproductive Health Services. Service Delivery Guidelines and Minimum Service Delivery Package on YFRH Services. Adds Ababa, Ethiopia: FMOH; 9–26. Available from: http://phe-ethiopia.org/resadmin/uploads/attachment-159-Stds_&_Serv_GL_YFRH.pdf. Accessed August 29, 2016. | ||
Kiragu K, Obwaka E, Odallo D, Van Hulzen C. Communicating about sex: adolescents and parents in Kenya. AIDS STD Health Promot Exch. 1996;(3):11–13. |
Supplementary material
 | Table S1 English version questionnaire; questionnaires on adolescents and parent communication on reproductive issues Abbreviations: S No, serial number; IUCD, intrauterine contraceptive device; STI, sexually transmitted infection; LGV, lymphogranuloma venereum. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.