Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Factors Affecting the Implementation of Continuous Quality Improvement in Health Facilities in Southern Nation and Nationalities Peoples Region (SNNPR), Ethiopia
Authors Wendwessen N, Dereje T ![]() , Gize A
, Gize A ![]()
Received 2 May 2020
Accepted for publication 3 August 2020
Published 25 August 2020 Volume 2020:13 Pages 855—862
DOI https://doi.org/10.2147/JMDH.S260285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nebiyou Wendwessen,1 Teklemariam Dereje,2 Addisu Gize3
1Institute for Health Care Improvement, Addis Ababa, Ethiopia; 2Department of Development Economics and Management, CFMD, Ethiopian Civil Service University, Addis Ababa, Ethiopia; 3Department of Microbiology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Addisu Gize
Department of Microbiology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Tel +251 911 80 91 73
Email [email protected]
Background: Continuous quality improvement (CQI) has become an important aspect of healthcare organizations. The objective of this study was to identify contributing factors for implementing continuous quality improvement projects in health facilities for the better delivery of healthcare service in the region of South Nation and Nationalities Peoples Region (SNNPR), Ethiopia.
Methods: A cross-sectional study was conducted from April to May 2018 in health facilities within two districts (woredas) located in SNNPR. Descriptive, bivariate, and multivariate analyses were used. During the analysis, a P-value less than 0.05 and 95% confidence interval (CI) were used to assess the significance of the associations.
Results: A total of 144 health professionals participated in the study. The majority of the respondents (75%) were male and 35% reported that their respective health facilities have implemented continuous quality improvement projects. More than half of the leaders (51.4%) were not receptive to new ideas and the majority of leaders were not encouraging learning (62.5%) or engaged in the quality improvement project implementation process (66%). Multivariate logistic regression analysis revealed that 84% of the health facilities were implementing a continuous quality improvement project (AOR=0.138 (0.029− 0.652)). Similarly, client satisfaction was 90% (AOR=0.101 (0.019− 0.522)) and the percentage of staff who believe that the quality improvement project contributed to the improvement of work at their respective health facility was 80% (AOR=0.181 (0.047− 0.696)).
Conclusion: The following variables, “Leaders receptiveness to new ideas”, “Leaders share information/data about health facility service delivery status”, “Health facility has a quality improvement project plan”, “Staff know using indicators to tell progress about service delivery”, and “Health facility assess client satisfaction level” were found to be independent predictors of continuous quality improvement (CQI) project implementation.
Keywords: continuous quality improvement, health facilities, SNNPR, Ethiopia
Introduction
Those involved in the healthcare system, including health professionals, professionals, patients and their families, researchers, payers, programmers, and educators agree that, in order to have better patient outcomes, better system performance and better professional development through needs continuous quality improvement (CQI) projects are needed.1 Continuous quality improvement has become an important aspect of healthcare organizations as they are forced to change and improve, due to demographic pressure such as an aging population,2 technical innovations and medical treatment development,3 and financial strains and expectations from stakeholders such as governmental agencies and patients.4 Quality improvement projects which eliminate inefficiency, errors, and redundancy can continually improve critical processes and reduce costs associated with poor quality.5 Ethiopia has implemented a number of innovative and successful national interventions for improving quality of care and Water and Sanitation Hygiene (WASH) in its healthcare facilities.6 The 2015–2020 Ethiopian National Health Care Quality Strategy (NQS) was crafted as a call to action to improve quality across the entire Ethiopian health system. Formally launched in March 2016, it was developed in order to achieve the health improvement goals stated in the Health Sector Transformation Plan. The NQS was launched as part of the four transformation agendas unveiled in which Regional Health Bureaus (RHBs), representatives from health facilities, and healthcare workers were included as part of the process.7
The NQS builds on the existing quality improvement efforts in Ethiopia which includes a number of national quality initiatives and tools that have been developed and implemented over the last 20 years – all of which have been aimed at improving the quality of healthcare delivery and services.
The aim of the NQS is to consistently improve the outcomes of clinical care, patient safety, and patient-centeredness, while increasing access and equity for all segments of the Ethiopian population by 2020.7 The strategy focuses on ensuring reliable, excellent clinical care, protecting patients, staff, and attendants from harm, and improving the efficiency of the delivery of care, while increasing access, equity, and dignity of care for all Ethiopians.
The international non-governmental organization Institute for Healthcare Improvement (IHI) has proposed a 5-year project aiming to introduce continuous quality improvement (CQI) approaches and improve maternal and newborn health (MNH) care in five regions of Ethiopia, namely Tigray, Afar, Amhara, Oromia, and South Nation and Nationalities Peoples Region (SNNPR).8 Thus, the main objective of this study was to identify factors which contribute towards the implementation of CQI projects in health facilities aimed at improving delivery of healthcare services in SNNPR, Ethiopia.
Materials and Methods
Study Area
The study was conducted in health facilities located across two woredas (districts) within the Southern Nation Nationalities People Region (SNNPR), namely Dugana fango Woreda (Wolita zone) and Chencha Woreda (Gamogofa zone).
Study Design and Period
A cross-sectional study design with quantitative approach was employed to conduct the investigation on CQI project implementation factors in the health facilities of SNNPR, Ethiopia; from April to May 2018.
Sample Size Determination and Sampling Procedure
The convenient sampling technique was used to select the study participants from health facilities across the two woredas due to limitations in both time and resources. Accordingly, six health centers (Dorze, Ezzo, Doko Zolo, Wobera, Zozo, and Dokomesho) and two hospitals (Chencha Primary Hospital & Arbaminch General Hospital) from Chencha Woreda as well as five health centers (Dendo, Edo, Kerchech, Dimitu, and Anka) and one hospital (Bitena Primary Hospital) from Dugana Fango Woreda, were included in the study. Thus, 144 conveniently selected healthcare providers and health facility leaders working in IHI supported health facilities were invited to participate in the study.
Data Collection Instrument and Procedure
After obtaining informed verbal consent, data on factors contributing towards quality improvement project implementation, the health professional’s level of involvement, challenges faced during CQI project implementation, and stakeholder involvement within CQI project implementation in the health facilities were collected through the Malcolm Bridge National Quality Award Criteria (MBNQAC). This pre-tested, structured, and self-administered questionnaire was adopted from the National Institute of Standards and Technology (NIST) of the United States.9
Data Analysis
Data was checked manually for completeness, and then coded, entered, and analyzed using SPSS version 20 software. After the data was explored and cleaned, descriptive analyses such as percentages, frequency distribution, and measures of central tendency were conducted. Bivariate analysis between dependent and independent variables was then performed using bivariate logistic regression. Finally, variables that were found to have a significant association on the bivariate analysis were entered into multiple logistic analyses to control for possible confounding variables and to identify independent predictor variables. During the analysis, a 0.05 P-value and 95% confidence interval (CI) were used to assess the significance of the associations.
Ethical Consideration
The study was reviewed and the acceptability of verbal informed consent was approved by the Institutional Review Committee, department of project management, Addis Ababa University. The ethical clearance was obtained and submitted to each Zonal Health Administration. Management officials of the health facilities involved in the study were informed verbally about the study. In addition, verbal informed consent was taken from each respondent prior to enrollment and gathering of relevant information.
Results
Socio-Demographic Characteristics
A total of 144 health professionals were approached to participate in this study, of which all were willing to be interviewed, giving a response rate of 100%. The majority of the respondents (75%) were male. Regarding age group, the majority of respondents (54.9%) fell between 22 and 30 years of age. In terms of health professions and education, the highest numbers of respondents (34%) were nurses, and the majority of respondents (52%) had received their diploma (Table 1).
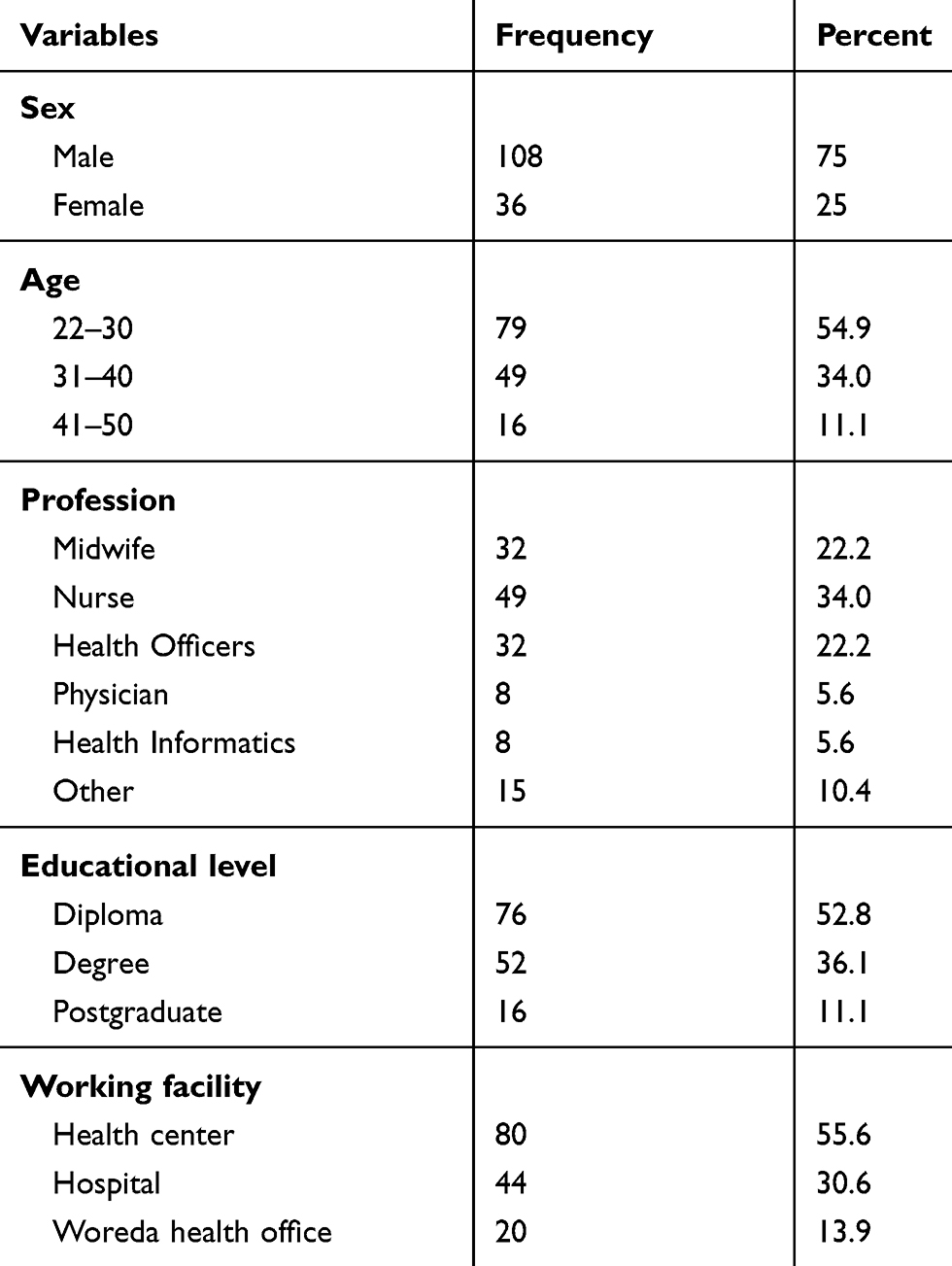 |
Table 1 Socio-Demographic Characteristics of Health Professionals Working in SNNPR, Ethiopia, (N=144) |
Implementation Status of Continuous Quality Improvement Projects
Among the 144 respondents, 65% said that their respective health facility implemented a continuous quality improvement project. The rest of the participants' facilities (35%) have not started the preliminary implementation process to improve the healthcare service delivery system.
Leadership Factors That Contribute to the Implementation of CQI Projects
Leadership factors that contribute towards CQI project implementation were assessed through leader’s receptiveness for new ideas, use of organization values, creating a safe work environment, etc. Accordingly, as shown in Table 2, more than half (51.4%) of the leaders were not receptive to new ideas. Moreover, the majority of leaders (62.5%) were not encouraging of learning, and 66% were not engaged in any quality improvement project implementation process ( Table 2).
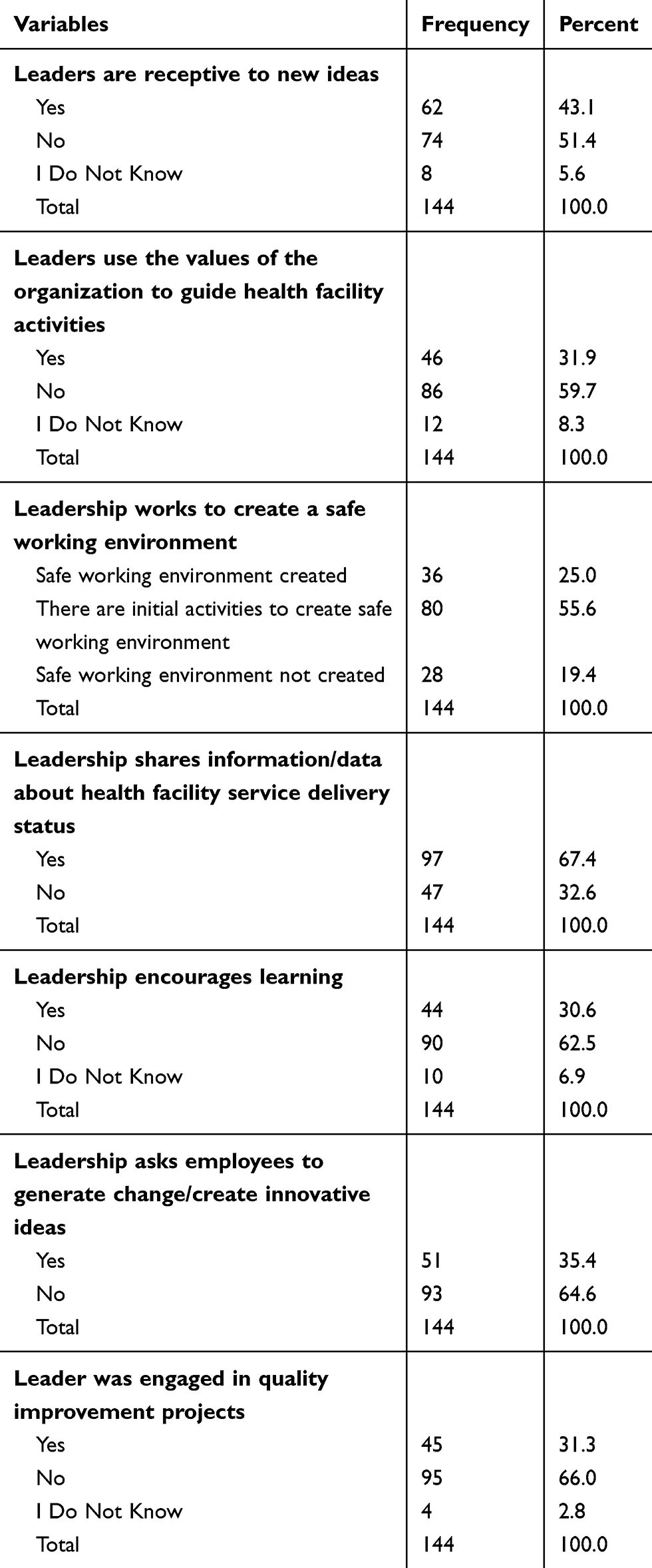 |
Table 2 Leadership Factors That Contribute Towards the Implementation of a Continuous Quality Improvement Project in Health Facilities in SNNPR, Ethiopia, 2018 |
Customer Factors That Contribute Towards the Implementations of CQI Projects
In order to implement quality improvement projects, customer related factors are ultimately needed for identifying quality related problems and possible solutions. According to the respondents, 50% stated that their respective health facilities have a mechanism for receiving client feedback, while 38.4% stated that their health facilities measure client satisfaction regularly, as shown in Table 3.
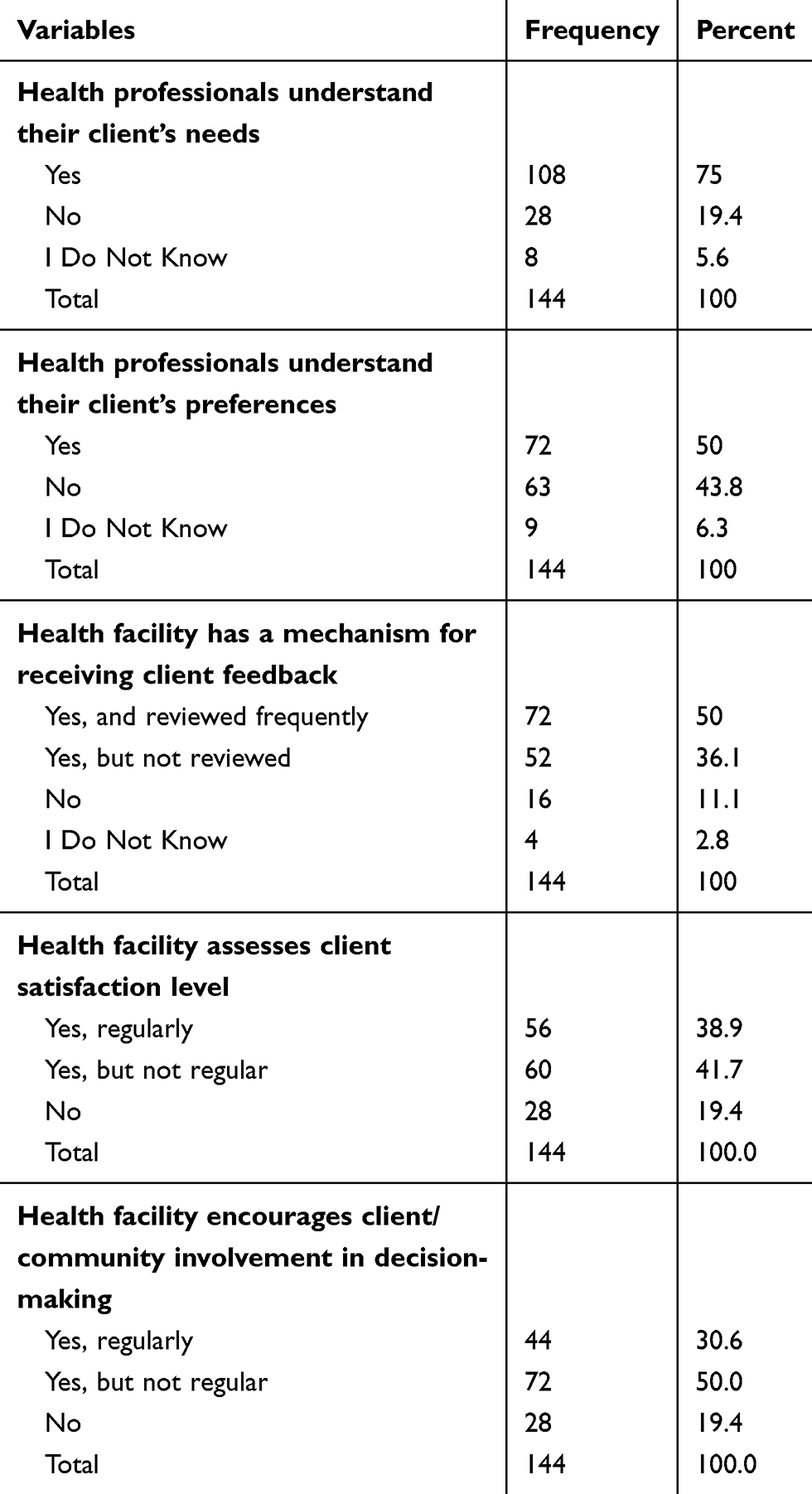 |
Table 3 Customer Factors That Contribute Towards the Implementation of a Continuous Quality Improvement Project in the Health Facilities in SNNPR, Ethiopia, 2018 |
Human Resource Factors That Contribute to Implementations of CQI Projects
Only 12 (8.3%) respondent said their respective health facility staff were fully trained on quality improvement project implementation. The majority of respondents (61.1%) mentioned that staff recognition for the work they performed in the health facilities was available. Quality improvement teams for project implementation were available according to 63.9% of respondents. Only 27.3% of respondent said that their respective health facilities had enough health staff to implement CQI projects, as shown in Table 4.
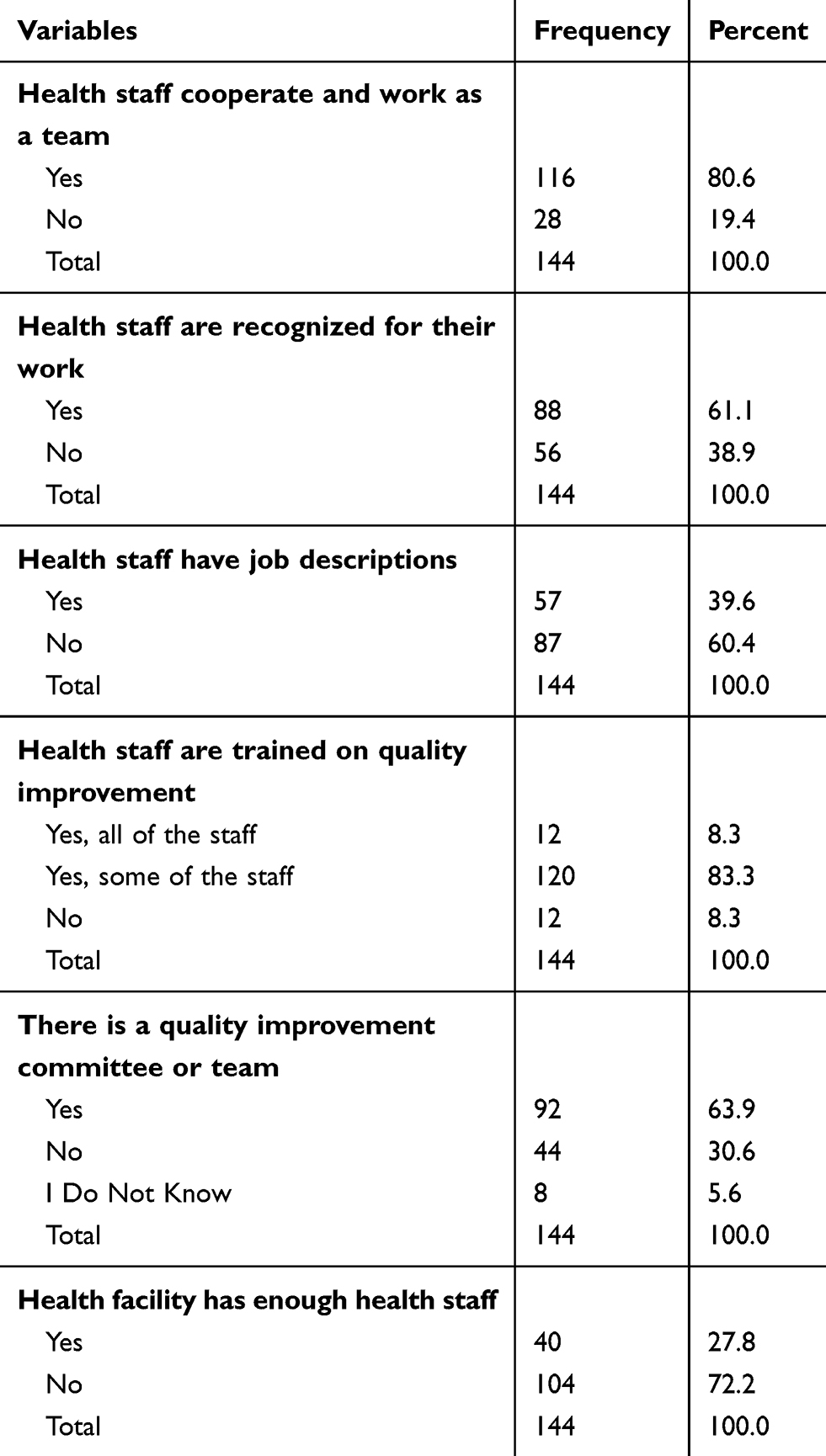 |
Table 4 Distribution of Human Resource Factors That Contribute Towards the Implementation of CQI Projects in the Health Facilities in SNNPR, Ethiopia, 2018 |
Determinants of CQI Project Implementation
In order to determine the independent variables associated with the implementation of CQI projects, a multivariate analysis was used. Variables that showed an association with the outcome variables in the bivariate analysis were selected for multivariate analysis. Variables which were found to be independent predictors of CQI project implementation included the following: leaders receptiveness to new ideas, leaders share information/data about health facility service delivery status, health facility has a quality improvement project plan, staff know how to use indicators to tell progress about service delivery, health facility assess client satisfaction level, health staff are recognized for their work, health staff are satisfied with their work, and leadership encourages learning (Table 5).
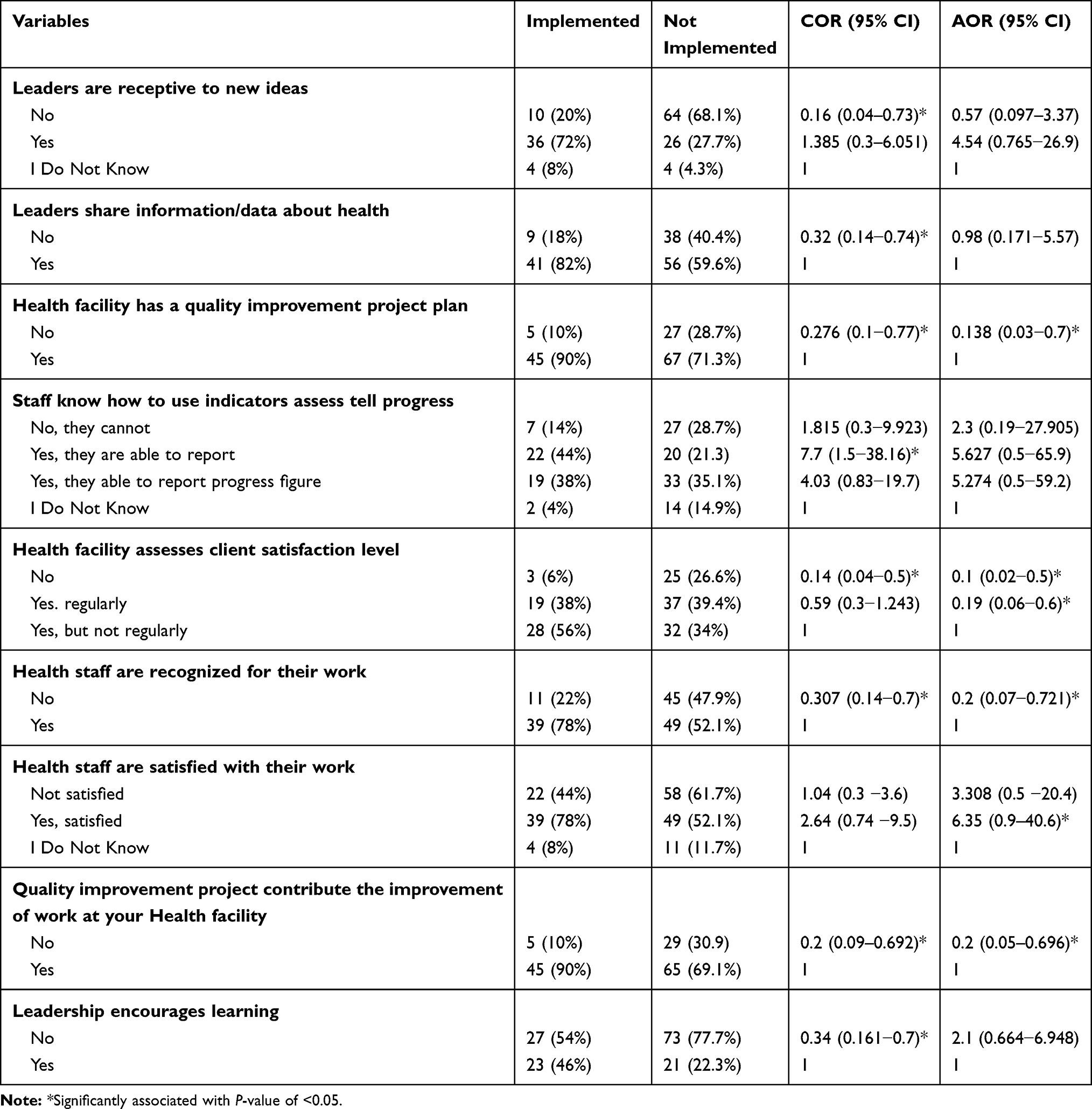 |
Table 5 Factor Associated with CQI Project Implementation in the Health Facilities of SNNPR, Ethiopia, 2018 |
According to the multivariate logistic regression analysis, if the health facility has a strategic quality improvement project plan, 84% of the health facility will implement a continuous quality improvement project (AOR=0.138 (0.029−0.652)). Similarly, if the health facility assesses client satisfaction, even if the assessment is not regular, 90% (AOR=0.101 (0.019−0.522)) of the health facility will implement a continuous quality improvement project as compared to health facilities which were not able to assess the satisfaction level of clients. Moreover, if the health facilities staff believed that the quality improvement project contributed to the improvement of work at their respective health facility, 80% (AOR=0.181 (0.047−0.696)) of the health facilities more likely implement a continuous quality improvement project as compared to those health facilities with staff who did not believe a CQI project had contributed to their work.
Discussion
In this study factors associated with continuous quality improvement project implementation were explored using health professional responses. From the findings, 35% of the respondents mentioned their respective health facilities had implemented CQI projects, which is lower than comparison studies conducted in Sri Lanka (43%).10
In this study the logistic regression identified factors associated with continuous quality improvement project implementation. Facilities with leaders that were receptive to new ideas were 1.4-times more likely than health facilities without such leaders in implementing CQI projects (AOR=1.385 (0.317–6.051)). Notably, only 72% of respondents indicated that their health facilities had leaders that were receptive to new ideas, a lower finding when compared to other studies.11 This discrepancy might be due to differences in the setting and assessment tools.
The majority (77.8%) of respondents indicated that their respective health facilities had a quality improvement project plan. Of these respondents, 86% also reported that their health facilities had specifically implemented CQI projects (AOR=0.138 (0.029–0.652)).
The questionnaire results showed that the majority of the respondents were not satisfied with their work (54%) and what they had accomplished. Furthermore, those who were satisfied with their work were 7-times more likely to work within health facilities that were implementing CQI projects (AOR=6.349 (0.993–40.588)). This finding is similar to a study conducted in a Swedish County,12 where the quality improvement project had contributed towards improvement of the work at the unit, and progress was assessed. The item “How much commitment do you feel toward the improvement idea?” showed a large engagement in the quality improvement initiative. In line with the above idea, the majority of respondents believe that CQI will contribute towards improvements in their work. Moreover, of the 82% of respondents who believed that their work would be improved through CQI, 82% work within facilities that have implemented CQI projects (AOR=0.181 (0.047−0.696)). This finding is also similar to the previously mentioned study conducted in a Swedish County.12
Overall, staff training on QI, team work, and leadership engagement did not show significant associations with CQI implementation, despite mentions by various previous studies as important determinant factors.13
Limitations of the Study
One of the challenges in conducting this research was the absences of adequate local studies in the area of continuous quality improvement projects in the health facilities which were used to compare to our findings. In addition, the sampling method we used may have a potential effect on our result, and also the finding is not generalizable as far as we used a convenient sampling method.
Conclusion
Implementing a quality improvement project is a pillar for improving client satisfaction. However, in SNNPR only small numbers of health facilities have active projects to improve service delivery. The implementation of continuous quality improvement projects was associated with factors such as leadership receptiveness, leadership encouragement for learning, health facility assesses for client satisfaction level, and the level of satisfaction of health staffs with their work. Strategic quality improvement plans should be developed by each respective health facility in the SNNPR in order to implement a CQI project effectively.
A client satisfaction survey and client engagement in CQI project should also be conducted regularly to identify quality problems and to effectively implement appropriate quality improvement projects.
Abbreviations
AIDS, Acquired Immuno Deficiency Syndrome; CQI, Continuous Quality Improvement; IHI, Institute for Healthcare Improvement; FMOH, Federal Ministry of Health; MNH, Maternal and Newborn Health; NQS, National Health Care Quality Strategy; QI, Quality Improvement; RHB, Regional Health Bureaus; SNNPR, South Nation and Nationalities People Region.
Data Sharing Statement
The data that supported the findings of this study will be available from the corresponding author upon reasonable request in the form of Statistical Package for Social Sciences (SPSS).
Ethics Approval and Consent to Participate
Ethical approval was obtained from Department of Project Management, Addis Ababa University and submitted to the appropriate management officials of the health facilities involved in the study. In addition, verbal consent was obtained from the respondents by explaining the objective of the study and confidentiality.
Acknowledgment
The authors would like to thank all study participants for their collaboration by giving their valuable time and information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Batalden PB, Davidoff F. What is “quality improvement” and how can it transform healthcare? BMJ Qual Saf. 2007;16(1):2–3. doi:10.1136/qshc.2006.022046
2. Nolte E, Britton A, McKee M. Trends in mortality attributable to current alcohol consumption in east and west Germany. Soc Sci Med. 2003;56(7):1385–1395. doi:10.1016/S0277-9536(02)00136-3
3. Grol R. Improving the quality of medical care: building bridges among professional pride, payer profit, and patient satisfaction. JAMA. 2001;286(20):2578–2585. doi:10.1001/jama.286.20.2578
4. Anell A. Swedish healthcare under pressure. Health Econ. 2005;14(S1):S237–S254. doi:10.1002/hec.1039
5. Riley WJ, Moran JW, Corso LC, Beitsch LM, Bialek R, Cofsky A. Defining quality improvement in public health. J Public Health Manag Pract. 2010;16(1):5. doi:10.1097/PHH.0b013e3181bedb49
6. Organization WH. Achieving Quality Universal Health Coverage Through Better Water, Sanitation and Hygiene Services in Health Care Facilities: A Focus on Ethiopia. 2017.
7. Ababa A. Federal democratic republic of Ethiopia ministry of health. Ethiop Postnatal Care. 2003.
8. Workie NW, Ramana GN. The Health Extension Program in Ethiopia. UNICO Study Series Number 10. Washington, DC: The World Bank; 2013. Availble from: http://documents1.worldbank.org/curated/en/356621468032070256/pdf/749630NWP0ETHI00Box374316B00PUBLIC0.pdf. Accessed August 14, 2020.
9. Haddad D, Seifert F, Chao LS, et al. Measurement of the planck constant at the National Institute of Standards and Technology from 2015 to 2017. Metrologia. 2017;54(5):633. doi:10.1088/1681-7575/aa7bf2
10. Somatunga LC, Sridharan S, Refai M, Malavige KK, Gamini LPS. Factors influencing continuous quality improvement programme in Government Hospitals of Sri Lanka. Int J Sci Technol Res. 2015;4(6):118–123.
11. Chen L-W, Nguyen A, Jacobson JJ, Ojha D, Palm D. Effectiveness and challenges for implementing quality improvement activities in Nebraska’s local health departments. Front Public Health Serv Syst Res. 2012;1(3):7.
12. Andersson A-C, Elg M, Perseius K-I, Idvall E. Evaluating a questionnaire to measure improvement initiatives in Swedish healthcare. BMC Health Serv Res. 2013;13(1):48. doi:10.1186/1472-6963-13-48
13. Ugo O, Ezinne E-A, Modupe O, Nicole S, Winifred E, Kelechi O. Improving quality of care in primary health-care facilities in rural Nigeria: successes and challenges. Health Serv Res Manag Epidemiol. 2016;3:2333392816662581.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.