Back to Journals » Clinical Interventions in Aging » Volume 15
Factors Affecting the Acceptability of Technology in Health Care Among Older Korean Adults with Multiple Chronic Conditions: A Cross-Sectional Study Adopting the Senior Technology Acceptance Model
Received 20 June 2020
Accepted for publication 7 September 2020
Published 2 October 2020 Volume 2020:15 Pages 1873—1881
DOI https://doi.org/10.2147/CIA.S268606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Jiyeon Ha,1 Hyeyoung K Park2
1College of Nursing, Konyang University, Daejeon, South Korea; 2College of Nursing, University of Massachusetts Amherst, Amherst, MA, USA
Correspondence: Hyeyoung K Park
College of Nursing, University of Massachusetts Amherst, 126 Skinner Hall, 651 North Pleasant Street, Amherst, MA 01003, USA
Tel +1 413 545 1343
Fax +1 413 545 0086
Email [email protected]
Purpose: Older adults experience challenges employing technology in their health-care management due to changes in cognitive and physical functions. This study aimed to investigate the acceptance of technology among older Korean adults with multiple chronic health conditions and examine factors associated with technology acceptance, adopting the senior technology acceptance model (STAM).
Patients and Methods: In total, 226 community-dwelling older adults with more than two chronic conditions participated in this study. We conducted a survey that covered demographics, gerontechnology self-efficacy, gerontechnology anxiety, facilitating conditions, self-reported health conditions, cognitive ability, social relationships, attitude toward life and satisfaction, physical functioning, and technology acceptance.
Results: Older Korean adults with multiple chronic health conditions scored moderately high for technology acceptance (25.36± 5.28). There were significant differences in technology acceptance according to age (r=− 0.241), cognitive ability (r=0.225), gerontechnology self-efficacy (r=0.323), and facilitating conditions (r=0.288). Only age and education were significant factors predicting technology acceptance (Adjusted R2=0.151, p< 0.001).
Conclusion: Although older Korean adults with multiple chronic conditions displayed good technology acceptance, their age and education level predicted the level of acceptance. Given that some components of the STAM model have social and cultural relevance, it is necessary to conduct research across various cultures to better understand technology acceptance by older adults.
Keywords: gerontechnology, multiple chronic conditions, technology, acceptance, aged
Introduction
Information and Communication Technology (ICT) refers to technologies that provide access to information through telecommunications including the Internet, wireless networks, cell phones, and other communication mediums.1 ICT creates virtual spaces that connect people without direct interaction, which enables real-time communication without the limitation of distance. Information exchange and communication are key components to health-care delivery and ICT allows health-care providers to adopt innovative health-care delivery methods, such as telehealth or real-time health monitoring using wearable devices.2,3
The effectiveness of ICT use in health-care settings has been widely studied. For example, real-time bedside pressure mapping systems were used to assess and manage pressure injuries among orthopedic patients.4 This increased knowledge and preventative action for patients with pressure injuries by providing instant feedback.4 Another study demonstrated that the use of mobile applications improved communication and symptom reporting among older adults.5 As such, health-care providers and researchers strive to adopt ICT in medical settings to advance communication strategies and health-care delivery.
Although there are benefits to utilizing ICT in health care, older adults experience challenges employing technology due to low motivation to use technology, low computer/Internet literacy, and changes in cognitive and physical function.6,7 Many chronic illnesses experienced by older adults also result in chronic physical impairments. Chronic physical impairments such as poor vision or reduced motor control create barriers for older adults when utilizing ICT in their health-care management.7 In addition, impairments in instrumental activities of daily living (IADL) prevent older adults from using ICT.8 Psychological distress such as “technostress” or “technophobia” also discourage older adults from learning and experiencing technology and thus, from utilizing ICT in daily life and health-care settings.9
While ICT may be challenging for older adults, some studies indicate that it is advantageous to older adult populations. Telehealth using ICT could eliminate limitations due to physical location and enable older adults with mobility issues to more easily access health care from their home or a community setting.10 ICT contributes positively to the mental health of older adults dwelling in rural areas by providing mental stimulation through connections to their family, friends, and society.11,12 In addition, applied ICT in health-care delivery through wearable health monitoring systems help health-care providers meet increasing care needs.2 Thus, successful use of ICT among older adults benefits not only the older adults themselves, but all of society.
Chronological age is negatively correlated to technology acceptance; however, older adults’ digital literacy can be developed through exposure and education. In fact, older adults have a positive attitude towards using technology in their daily life and health care, despite some barriers and challenges.13,14 Gerontechnology is a new field that has emerged in response to the need to assist older adults who are willing to employ technology in their daily lives and health care. Technology has great potential to effectively address the limitations that older adults experience as a consequence of aging. Thus, to reduce barriers and help older adults take advantage of technology, evaluation of their acceptance of ICT and the factors involved is necessary.
South Korea is a leading country in terms of ICT development and wide-spread availability of equipment and services.15 Older Korean adults display positive attitudes (ie, desire to respond to the changes, convenience of up-to-date information) and negative attitudes (ie, inconvenience due to unfamiliarity with technology use, burden of expenses) toward the use of smartphones.16 Older Korean adults who have higher levels of empowerment are more likely to perceive technology use as easier and therefore more useful, resulting in positive attitudes toward using mobile applications.17 Although there are some studies that investigate older adults’ technology use in relation to health care, there is a dearth of research targeting chronically ill older adults who could benefit from technology use in their health-care management. Thus, the purpose of this study is to investigate the acceptance of technology among older Korean adults with multiple chronic conditions and to determine the factors predicting technology acceptance, using the senior technology acceptance model.
Theoretical Framework: A Senior Technology Acceptance Model
Chen and Chan proposed the senior technology acceptance model (STAM) using concepts from previous models such as the Technology Acceptance Model (TAM) and the Unified Theory of Acceptance and Use of Technology (UTAUT).18 STAM suggests 8 factors predicting technology acceptance (gerontechnology self-efficacy, gerontechnology anxiety, facilitating conditions, self-reported health conditions, cognitive ability, social relationships, attitude to life and satisfaction, and physical functioning) after controlling for socio-demographic factors such as age, gender, education level, and economic status.18 Gerontechnology is defined as
Electronic or digital products or services that can increase independent living and social participation of older persons in relatively good health, comfort, and safety.
and gerontechnology acceptance was operationally defined as positive attitudes and usage of gerontechnology.18 Gerontechnology self-efficacy is a user’s assessment of their own ability to perform a task successfully using gerontechnology, while gerontechnology anxiety refers to emotional reactions such as worry, nervousness, or uneasiness, evoked by performing a task using gerontechnology.18,19 Facilitating conditions are environmental factors that assist older adults in using gerontechnology more easily. Chen and Chan tested STAM among 1,012 older adults in Hongkong and their results supported the proposed model.18 Thus, we used STAM in our study design and interpretation of the results.
Participants and Methods
Study Design and Subjects
This cross-sectional descriptive design was employed to investigate the acceptance of technology and factors related to technology acceptance among older Korean adults with multiple chronic conditions. A convenience sample of older adults was recruited over a 1-week period in June 2019 from a community senior center in Daejeon, South Korea that has 5,333 members and approximately 300 users per day. The study participants were people over 65 who lived in Daejeon with two or more chronic diseases. The exclusion criterion was a diagnosis of dementia. The G*power (version 3.1) program was used to calculate the sample size for linear multiple regression analysis.20 The calculated sample size for this study was 208 people under the setting of a type-I error = 0.05, a power = 0.95, an effect size = 0.15, and predictor variables = 17 based on a similar prior study.21 We recruited 229 people to reach an appropriate sample size, considering a potential 10% dropout rate.
Measurements
The survey questionnaire included demographics (age, sex, education, economic status, marital status, religion, co-residence, number of children, and number of chronic illnesses), 8 independent variables (self-reported health, cognitive ability, social relationships, attitude to aging and life satisfaction, physical function, gerontechnology self-efficacy, gerontechnology anxiety, and facilitating conditions) and 1 dependent variable (technology acceptance).
Health and Ability Characteristics
Health characteristics were measured via self-reported health, cognitive ability, social relationships, attitude to life and satisfaction, and physical function based on Chen and Chan’s previous research.18 Self-reported health conditions consisted of 5 items inquiring about general health status, health status compared to others, hearing, vision, and movement. Cognitive ability was measured by 4 items inquiring about memory, learning, concentration, and thinking skills. Social relationships were measured by 3 items inquiring about satisfaction with personal relationships, satisfaction with social support, and engagement in social activities. Attitude to aging and life satisfaction were measured by a single question (ie, “Do you feel that as you get older you are less useful?”).18,22 All items were assessed on a 5-point Likert scale with answers ranging from 1 (very poor) to 5 (very good) and a higher score indicating better health and ability characteristics. Physical function was measured by the Korean-Instrumental Activities of Daily Living scale (K-IADL).23 Ten items included questions regarding grooming abilities, preparing meals, laundry, and managing money, and answers were scored as 1 (independent), 2 (needs help), and 3 (dependent). Higher scores indicate greater dependence for activities.23
Gerontechnology Self-Efficacy, Anxiety, and Facilitating Conditions
Gerontechnology self-efficacy was measured using 2 items asking whether older adults believe they are capable of completing a task using technology if they receive appropriate demonstration or instruction.18 Gerontechnology anxiety was measured using 2 items asking about apprehensive or hesitative feelings when using technology.18 Facilitating conditions were measured using 5 items asking about knowledge, assistance, financial status, accessibility, and support for technology use.18 All answers were measured on 5-point Likert scales ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate better gerontechnology self-efficacy, more gerontechnology anxiety, and better facilitating conditions.
Technology Acceptance
This study employed Chen and Chan’s operational definition of technology acceptance, which measured technology acceptance according to attitude towards use, perceived usefulness, and perceived ease of use.18 Attitude towards use (AT) contained 2 items (ie, You like the idea of using technology), perceived usefulness (PU) contained 3 items (ie, Using technology would make your life more convenient), and perceived ease of use (PEOU) contained 2 items (ie, You could be skillful at using technology).18 All answers were measured on 5-point Likert scales ranging from 1 (strongly disagree) to 5 (strongly agree). Higher total scores indicate better technology acceptance.
Procedure
The study protocol to recruit and collect data were approved by the director of the community senior center in Daejeon. Flyers and banners were displayed at the entrance of the senior center to recruit potential study participants. Those who were interested in participating received a detailed explanation of the procedure and contents of the study from the research assistant.
Research assistants with knowledge of the characteristics and health issues of older adults were trained to assist participants with the completion of written consent forms and questionnaires. Data were collected face-to-face to eliminate difficulties for older adults with reduced visual and auditory functions. Each survey took approximately 30–40 minutes to complete. After the questionnaire was completed, each participant received a pain relief patch as reimbursement for their time and effort. Data collection was conducted for one week in June 2019. A total of 229 people responded to the questionnaire; 226 questionnaires were used for statistical analysis, and 3 were excluded due to incomplete responses.
Statistical Analysis
Statistical analyses were conducted using SAS 9.3 software (SAS, Cary, NC). Results for descriptive analyses are presented as means and standard deviations for continuous variables (age, number of children, number of chronic disease, self-reported health conditions, cognitive ability, social relationships, attitude to aging and life satisfaction, physical function, gerontechnology self-efficacy, gerontechnology anxiety, facilitating conditions) and frequencies and percentages for categorical variables (sex, education, economic status, marital status, religion, residence). The acceptance of technology was described using mean and standard deviations as well as frequency and percentage for the data from the 5-point Likert scales.
A Kolmogorov–Smirnov test was conducted to test the normality of the dependent variable (technology acceptance) and indicated that it was not normally distributed (p<0.01); so non-parametric tests such as Spearman correlation, Cramer-von Mises Statistics, or Kolmogorov–Smirnov test were used to analyze the associations between independent variables and the dependent variable (technology acceptance). The significance level was set as p<0.05. A multiple linear regression model was created to determine the predictors of gerontechnology acceptance, and a stepwise technique was used to select the predictors and variables left in the model, which were significant at the p<0.15 level. For nominal level independent variables, dummy coding was used in the regression analysis. To test the mediation effects between independent variables and dependent variable(technology acceptance), the Sobel test was conducted.24
Ethics
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Konyang University in Daejeon, South Korea (No. KYU-2019-265-01). Data were collected only for those who understood the purpose and content of the study and who signed the informed consent form voluntarily. Participants in this study were informed that they could cease participation at any time during the research period and there would be no disadvantages in any way in relation to their withdrawal from the study.
Results
The mean age of the 226 participants was 79.44 years, with ages ranging from 66 to 96 years. More than half of the participants were female (66.37%) and currently married (54.42%). Most of the participants were either living with their spouse (41.15%) or lived by themselves (34.51%). On average, they were diagnosed with 2.5 chronic diseases including hypertension, diabetes, heart disease, thyroid disease, and cancer (Table 1).
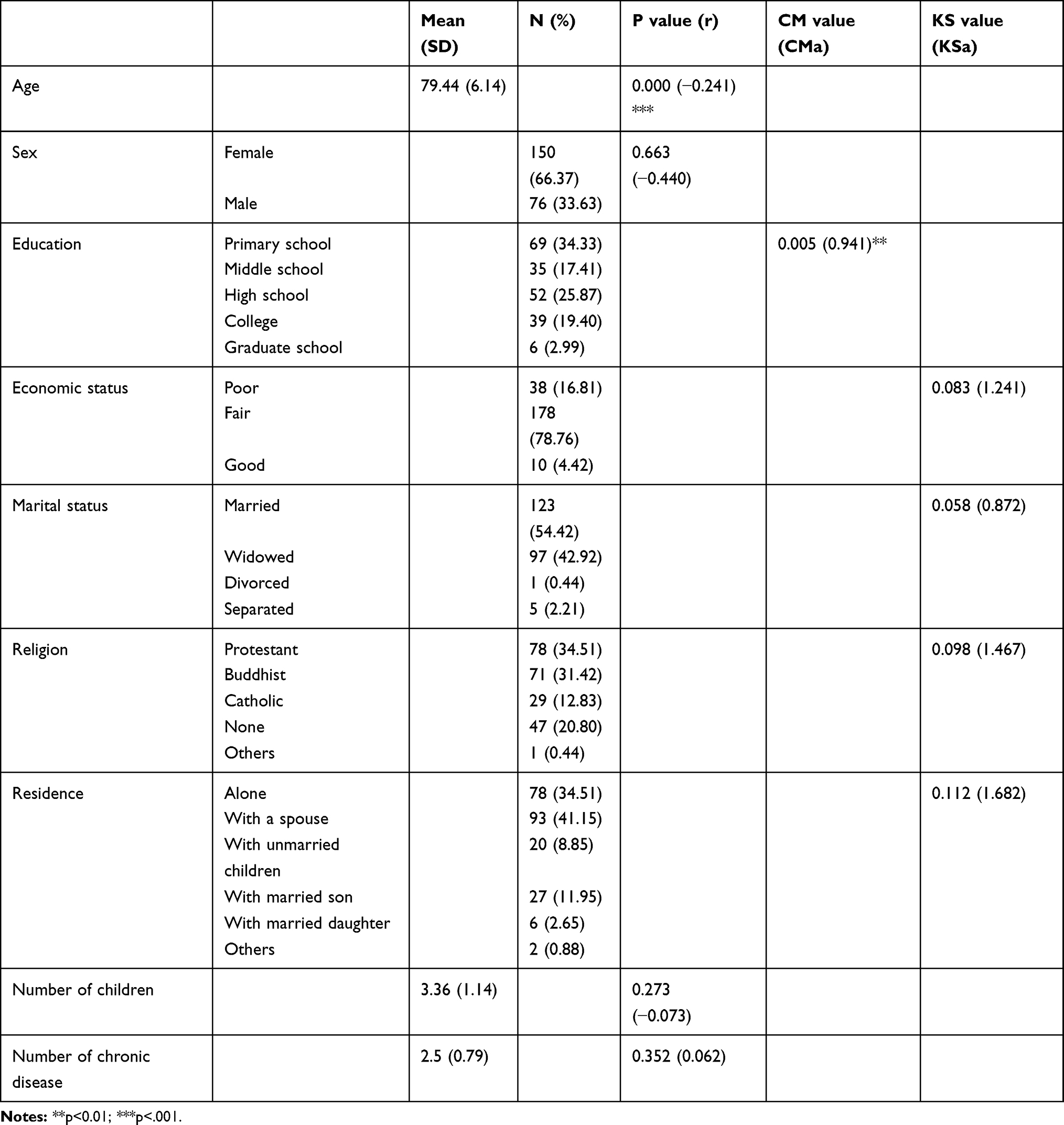 |
Table 1 Correlations Between Participants’ Demographics and Technology Acceptance (n=226) |
Older Korean adults in this study reported fair health condition scores (16.24±3.83; 6–25) and the average scores for cognitive ability and social relationship were 13.28 and 11.13, respectively. On average, participants displayed fairly independent IADL scores (11.14±2.29; 10–22) and had fair psychological function (6.47±1.51; 2–10). Their gerontechnology self-efficacy (6.23±2.03; 2–10) was slightly higher than their gerontechnology anxiety (5.39±2.10; 2–10). The average score for facilitating conditions was 16.89 (Table 2).
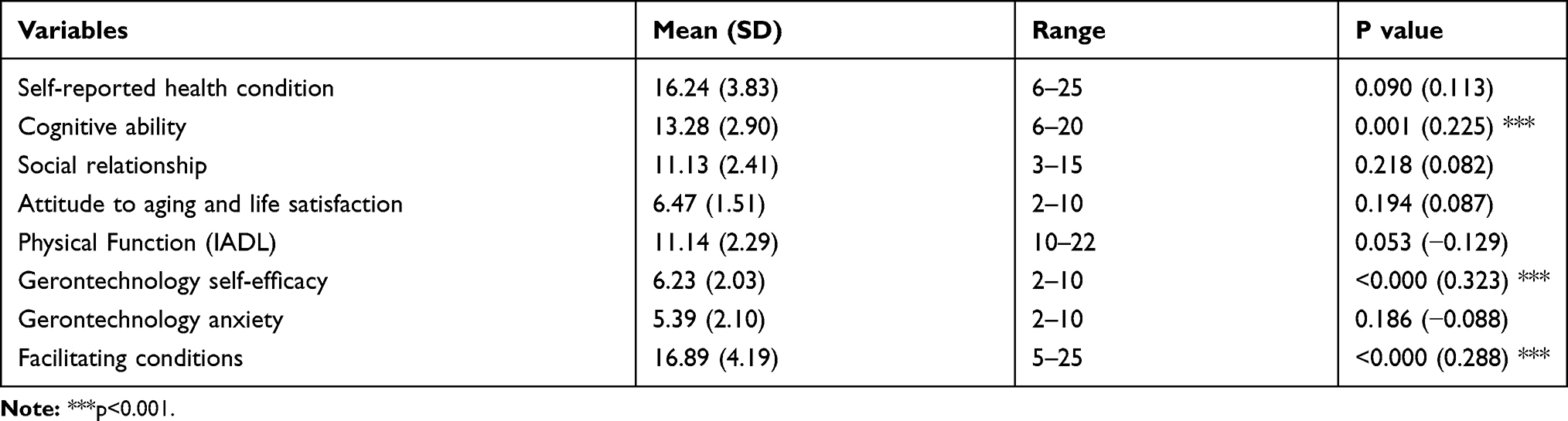 |
Table 2 Independent Variables |
Overall, participants demonstrated good technology acceptance (25.36±5.28; 7–35). They were in favor of the idea of using technology and believed that technology would benefit them. However, they found using technology was not easy or considered themselves lacking in the skills to use it (Table 3). Among the demographic characteristics, only age (r=−0.241) and education (r=0.941) were significantly associated with technology acceptance. Among independent variables, cognitive ability (r=0.225), gerontechnology self-efficacy (r=0.323), and facilitating condition (r=0.288) were significantly associated with the older adults’ acceptance of technology (Table 1,2).
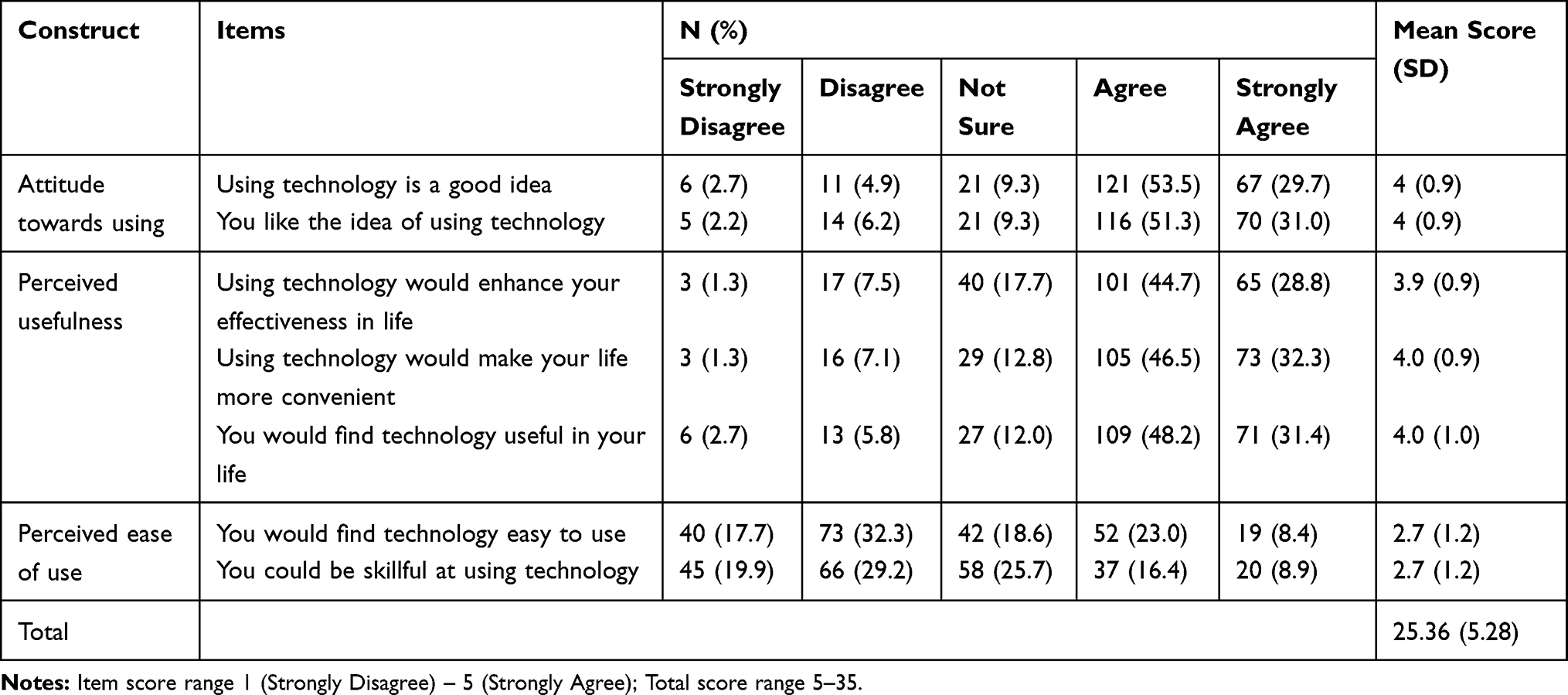 |
Table 3 Acceptance of Technology |
A multiple regression model was proposed using variables that were significantly associated with technology acceptance, which included only age and education (Adjusted R2=0.151, p<0.001, Table 4). Additionally, gerontechnology self-efficacy was a mediator between age and technology acceptance (p<0.01). Gerontechnology self-efficacy was also a mediator between education and technology acceptance (p<.000), and facilitating condition was a mediator between education and technology acceptance (p=0.014).
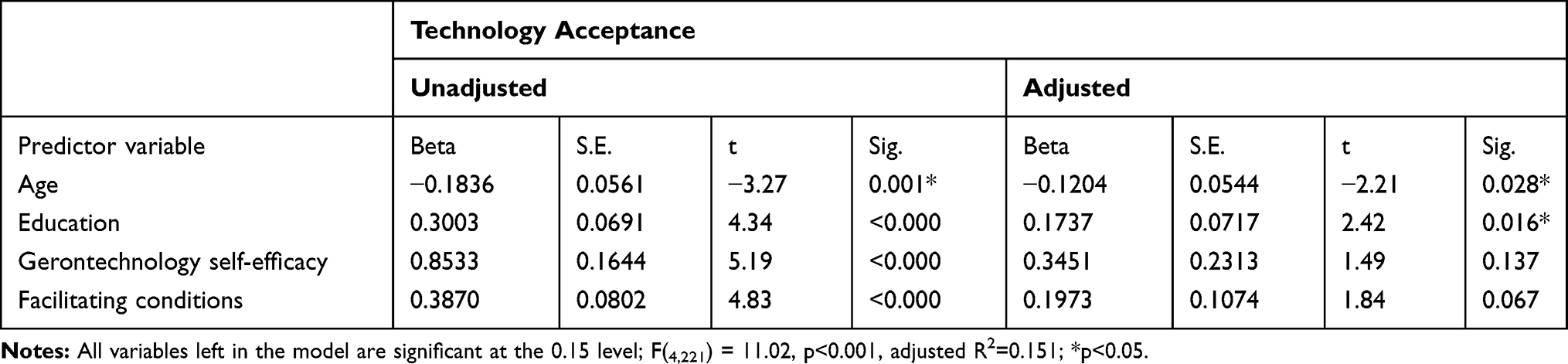 |
Table 4 Stepwise Multiple Regression Model |
Discussion
This study aimed to investigate the acceptance of technology among older Korean adults with multiple chronic health conditions and the factors predicting this technology acceptance, using the senior technology acceptance model. Our results indicate that participants have good technology acceptance despite the assumption that older adults are reluctant to adapt and use new ICT.25 Participants recognized that the use of ICT was helpful in their lives and felt favorable toward the adoption of new technology. In addition, our findings suggest that technology use is well accepted by older adults with multiple chronic diseases and who often have difficulties in their daily lives due to poor physical function and frequent hospital use.
Age and education level were significant factors predicting the acceptance of technology in a multivariate regression model. This is similar to the results of previous studies that demonstrate that age directly affects technology use, and the higher the level of education, the greater the use of technology.18 A recent study in South Africa also reported that age and education had a significant influence on the acceptance of communication technology.26 There are many obstacles associated with technology acceptance by older adults; one of these is the physical barrier, which is an aging-related factor and includes cognitive, motor, and sensory deficits that accompany the aging progress.25 In other words, as people age, they become more likely to experience these restrictions. Health-care providers should evaluate older adults for these barriers, consider how it may affect their acceptance of ICTs, and provide proper technical support for improving mobile health accessibility. In addition, compared to younger individuals, who have had compulsory education, older adults in Korea have various levels of educational background. Hence, it is necessary to recognize that lower education levels affect the digital and information gap,26,27 and to consider diversification of education and technical support according to education level.
Our further analyses indicate that gerontechnology self-efficacy (GSE) and facilitating conditions (FC) mediate the influence of education on technology acceptance among older adults. While the effects of GSE and FC on technology acceptance are still controversial with regard to direct or indirect effects,18,26 our study findings are consistent with previous results that GSE and FC have a positive effect on technology acceptance.
Our results also revealed that perceived ease of use (PEU) was relatively lower than attitude towards using or perceived usefulness. Conci and colleagues reported that the relationship between PEU and behavioral intention is highly significant and PEU is an important factor in the early stage of technology adoption.28 A variety of technology education and training programs would improve self-efficacy and motivate elderly users.29 In addition, PEU was strongly negatively correlated with support; in other words, when PEU was low, the demand for support was high.30 This indicates that older people are more likely to adopt gerontechnology if there is enough environmental support to make it easier to use.30 Therefore, providing the environmental support that the elderly need at the right time is an important way to reduce the obstacles to acceptance of gerontechnology.
As physical and socio-psychological conditions change with the aging process, the needs and requirements for the use of technology among the elderly may differ from younger generations.18 McLeod reported that the obstacles to mobile phone use were complexity, small device size, cost of use, lack of usefulness, and privacy infringement.31 Most ICT technology seems to be targeted at young adults. The development and application of various methods to reduce the difficulty of adopting new technology for older people is urgently needed.
The results of this study suggest ways to reduce prejudice towards older people. Technological acceptance by older adults will change with the times, and intention to use technology is also influenced by sociocultural characteristics, such as subjective norms, trust, and uncertainty avoidance in each society.32 To better understand technology acceptance among the older adults, similar research should be repeated and expanded in various cultures. These findings provide important clues to develop support and technology that will be tailored to older adults’ needs.
The results of this study should be interpreted in light of several limitations. First, study participants were recruited using convenience sampling from a senior center in South Korea; thus, our results may not be generalizable to older adults in other regions or countries. It is necessary to conduct large-scale studies that can reduce selection bias using random sampling. Secondly, while this study identified a wide range of general technology acceptance, the types of gerontechnology vary according to their purpose. Further research is needed to identify the acceptance of gerontechnology by specific type or purpose of use. Third, socioeconomic status factors were investigated using self-reported answers ranging from good, fair, and poor, which resulted in skewed distributions. Economic status should be investigated using more detailed scales to achieve a comprehensive understanding of technology acceptance among older Korean adults. Moreover, the measurements used in this study originated from the STAM model; however, psychometrics (such as validity or reliability) were not presented. Further research including various settings and populations is needed to confirm the reliability and validity of the measurements implemented in this study. Lastly, the adjusted R2 of the regression model was low. Each component that forms the STAM model has substantial social and cultural relevance. Future research will need to take those sociocultural influences into consideration and conduct qualitative research or employ a mixed-methods design to verify other relevant predictors and to better understand the phenomenon.
Conclusions
Older adults at high risk of poor physical function due to multiple chronic diseases exhibited good acceptance of new technology and recognized that the usage of ICT was helpful. Old age and education level were significant predictors of technology acceptance. Gerontechnology self-efficacy and facilitating conditions were positively associated with technology acceptance among older Korean adults with multiple chronic conditions. Given that some components of the STAM model have social and cultural relevance, and because the intention to use technology is influenced by sociocultural characteristics, it is necessary to conduct research across various cultures to better understand technology acceptance by older adults.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2018R1C1B5085248). The authors would like to thank Dr. Joohyun Chung, assistant professor at the College of Nursing, UMass Amherst for her statistical consult.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christensson P. ICT definition; 2010. Available from: https://techterms.com.
2. Li J, Ma Q, Chan AH, et al. Health monitoring through wearable technologies for older adults: smart wearables acceptance model. Appl Ergon. 2019;75:162–169. doi:10.1016/j.apergo.2018.10.006
3. Kamei T. Information and communication technology for home care in the future. Jpn J Nurs Sci. 2013;10(2):154–161. doi:10.1111/jjns.12039
4. Hultin L, Karlsson AC, Öhrvall M, et al. Information and communication technology can increase patient participation in pressure injury prevention: a qualitative study in older orthopedic patients. J Wound Ostomy Continence Nurs. 2019;46(5):383–389. doi:10.1097/WON.0000000000000568
5. Göransson C, Eriksson I, Ziegert K, et al. Testing an app for reporting health concerns-experiences from older people and home care nurses. Int J Older People Nurs. 2018;13(2):e12181. doi:10.1111/opn.12181
6. Adebayo B, Durey A, Slack-Smith LM. Role of information and communication technology in promoting oral health at residential aged care facilities. Aust J Prim Health. 2017;23(3):216–222. doi:10.1071/PY15168
7. Wildenbos G, Peute L, Jaspers M. Aging barriers influencing mobile health usability for older adults: a literature based framework (MOLD-US). Int J Med Inform. 2018;114:66–75. doi:10.1016/j.ijmedinf.2018.03.012
8. Rikard RV, Berkowsky RW, Cotten SR. Discontinued information and communication technology usage among older adults in continuing care retirement communities in the United States. Gerontology. 2018;64(2):188–200. doi:10.1159/000482017
9. Nimrod G. Technostress: measuring a new threat to well-being in later life. Aging Ment Health. 2018;22(8):1086–1093. doi:10.1080/13607863.2017.1334037
10. Soar J, Seo Y. Health and aged care enabled by information technology. Ann N Y Acad Sci. 2007;1114(1):154–161. doi:10.1196/annals.1396.040
11. Berg T, Winterton R, Petersen M, et al. ‘Although we’re isolated, we’re not really isolated’: the value of information and communication technology for older people in rural Australia. Australas J Ageing. 2017;36(4):313–317. doi:10.1111/ajag.12449
12. Damant J, Knapp M, Freddolino P, Lombard D. Effects of digital engagement on the quality of life of older people. Health Soc Care Community. 2017;25(6):1679–1703. doi:10.1111/hsc.12335
13. Wandke H, Sengpiel M, Sönksen M. Myths about older people’s use of information and communication technology. Gerontology. 2012;58(6):564–570.
14. Papa F, Cornacchia M, Sapio B, et al. Engaging technology-resistant elderly people: empirical evidence from an ICT-enabled social environment. Inform Health Soc Care. 2017;42(1):43–60. doi:10.3109/17538157.2016.1153477
15. Organisation for Economic Co-operation and Development. OECD digital economy outlook 2015. OECD. 2015;42.
16. Kim MY, Kang YH, Jung DY, et al. Older adults’ smart phone use and access to health information. J Qual Res. 2013;14(1):13–22. doi:10.22284/qr.2013.14.1.13
17. An ST, Kang HN, Chung SD. Older adults’ adoption of health-related mobile application: the role of empowerment. J Public Relat. 2018;22(6):53–74. doi:10.15814/jpr.2018.22.6.53
18. Chen K, Chan AHS. Gerontechnology acceptance by elderly Hong Kong Chinese: a senior technology acceptance model (STAM). Ergonomics. 2014;57(5):635–652. doi:10.1080/00140139.2014.895855
19. Venkatesh V, Morris MG, Davis GB, et al. User acceptance of information technology: toward a unified view. MIS Q. 2003;27(3):425–478. doi:10.2307/30036540
20. Buchner A, Erdfelder E, Faul F, et al. G* Power 3.1 Manual. Düsseldorf, Germany: Heinrich-Heine-Universitat Dusseldorf; 2017.
21. Choi IS, Park K. The effects of pain, sleep, and depression on quality of life in elderly people with chronic pain. J Digit Converg. 2017;15(8):289–299.
22. Lawton MP. The Philadelphia geriatric center morale scale: a revision. J Gerontol. 1975;30(1):85–89. doi:10.1093/geronj/30.1.85
23. Won CW, Rho YG, SunWoo G, et al. The validity and reliability of Korean instrumental activities of daily living (K-IADL) scale. J Korean Geriatr Soc. 2002;6(4):273–280.
24. Preacher KJ, Leonardelli GJ. Calculation for the sobel test: an interactive calculation tool for mediation tests; 2001. Available from: http://quantpsy.org/sobel/sobel.htm.
25. Fletcher J, Jensen R. Mobile health: barriers to mobile phone use in the aging population. Online J Nurs Inform. 2015;19(3).
26. Jarvis MA, Sartorius B, Chipps J. Technology acceptance of older persons living in residential care. Inf Dev. 2019;36(3):1–15.
27. Hong SG, Trimi S, Kim DW. Smartphone use and internet literacy of senior citizens. J Assist Technol. 2016;10(1):27–38. doi:10.1108/JAT-03-2015-0006
28. Conci M, Pianesi F, Zancanaro M. Useful, social and enjoyable: mobile phone adoption by older people. In:
29. Peng L, Ma Q, Yu RWL, et al. Facilitating gerontechnology adoption: observational learning with live models. In: Rau PL, editor. Cross-Cultural Design. Applications in Cultural Heritage, Creativity and Social Development. Cham: Springer; 2018:334–345.
30. Mcgaughey RE, Zeltmann SM, Mcmurtrey ME. Motivations and obstacles to smartphone use by the elderly: developing a research framework. IJEF. 2013;7(3/4):177–195. doi:10.1504/IJEF.2013.058601
31. McLeod E. The use (and disuse) of mobile phones by baby boomers. iJETS. 2009;7(1):28–38.
32. Mohamed AHHM, Tawfik H, Al-Jumeily D, et al. MoHTAM: a technology acceptance model for mobile health applications.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.