Back to Journals » Clinical Ophthalmology » Volume 19
Factors Affecting Ocular Prosthetic Use Amongst Anophthalmic Patients: A Retrospective Review with Patient Interviews
Authors Parekh Z ![]() , Spisak M, Shah A, Considine SP, Shah H, Krakauer M
, Spisak M, Shah A, Considine SP, Shah H, Krakauer M
Received 9 July 2025
Accepted for publication 28 October 2025
Published 8 November 2025 Volume 2025:19 Pages 4145—4154
DOI https://doi.org/10.2147/OPTH.S552575
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zaid Parekh,1 Micaila Spisak,2 Arjav Shah,1 Sean P Considine,2 Hassan Shah,1 Mark Krakauer2
1Department of Ophthalmology and Visual Sciences, Pritzker School of Medicine, University of Chicago, Chicago, IL, USA; 2Department of Ophthalmology, Lewis Katz School of Medicine at Temple University, Philadelphia, PA, USA
Correspondence: Mark Krakauer, Department of Ophthalmology, Lewis Katz School of Medicine at Temple University, 3401 N. Broad Street Parkinson Pavilion, Suite 630, Philadelphia, PA, 19140, USA, Tel +1 215 707 3185, Email [email protected]
Purpose: To evaluate the rate of ocular prosthesis use amongst anophthalmic patients following eye removal surgery and to investigate the influence of socioeconomic factors on prosthesis acquisition.
Methods: A retrospective chart review was conducted for adults undergoing enucleation or evisceration by two surgeons at two urban trauma centers and a private practice between December 2013 and February 2024. Patients were identified using Current Procedural Terminology (CPT) codes for primary and secondary eye removal procedures. Demographic, clinical, and socioeconomic data were collected, including insurance status, employment at the time of surgery, and estimated household income by zip code. Chart data was supplemented by patient telephone interviews which assessed current prosthesis use and barriers to acquisition. Statistical analyses included chi-squared, Fisher’s exact, t-tests, and multivariate logistic regression to identify factors associated with prosthesis use.
Results: Among 152 patients screened, 138 patients were included (mean age 52; 55.8% male; 60.1% Black), and 81 (59%) obtained a prosthesis by last follow-up. Most patients (82%) had government-sponsored insurance. Employment and longer follow-up duration were significantly associated with prosthesis use (p=0.036; p< 0.001). In multivariate analysis, female sex (adjusted OR=2.06, [1.0; 4.27], P=0.052) and private insurance (adjusted OR=2.70, [0.84; 8.7], P=0.097) trended toward higher rates of prosthesis utilization but were not statistically significant. Among 41/138 (30%) interview participants, 30/41 (73%) had a prosthesis, with 26 of these 30 (87%) reporting positive impacts on quality-of-life. Cost was the most cited barrier among those without a prosthesis.
Conclusion: This study uniquely combines clinical data with direct patient interviews to provide new evidence on real-world barriers to prosthesis access among anophthalmic patients. Ocular prosthesis utilization remains limited, with fewer than 60% of anophthalmic patients obtaining prostheses despite high insurance coverage rates. Employment status and consistent follow-up care were significantly associated with prosthesis acquisition, while cost appeared as a primary barrier. Future efforts should leverage emerging technologies and integrated care pathways to improve access for all anophthalmic patients.
Plain Language Summary: Following eye removal surgery for serious injury or disease, patients typically receive an artificial eye (prosthesis) that matches their remaining eye and helps restore appearance and confidence. While ocular prostheses provide significant psychosocial benefits, research on utilization rates and barriers to obtaining them is limited. This study aimed to evaluate prosthesis usage patterns and identify factors influencing patient access. We conducted a retrospective analysis of medical records from 138 adults who underwent eye removal surgery at two trauma centers and one private practice over 10 years. We supplemented chart review with telephone interviews to ask about patients’ experiences: whether they got an artificial eye, what challenges they faced, and how it affected daily life. Only 59% of patients obtained prostheses by their last follow-up. Among interviewed patients without prostheses, cost emerged as the primary barrier despite an overwhelming majority having government health insurance (Medicare or Medicaid). Employment status at the time of surgery and consistent follow-up attendance significantly predicted prosthesis receipt. Among prosthesis recipients, 87% reported positive quality-of-life impacts, including increased confidence, “I feel like myself again”, and reduced psychological distress, “I used to feel like everyone was looking at me, but now most people can’t even tell the difference”. Our findings reveal that substantial barriers prevent many patients from accessing ocular prostheses that could meaningfully improve their well-being. This indicates the need for healthcare providers to develop comprehensive support systems, investigate cost-effective prosthetic options, and strengthen follow-up care protocols to ensure broader access to these beneficial devices.
Keywords: enucleation, evisceration, ocular prosthesis, anophthalmic, socioeconomic barriers
Introduction
In cases of severe ocular trauma or intraocular tumors, blind, painful eyes may necessitate surgical removal. First described in the literature over two centuries ago, enucleation (removal of the entire globe and its intraocular contents) and evisceration (ocular contents are removed from an intact sclera) are the two mainstays of current therapeutic modalities to definitively treat blind, painful eyes stemming from ocular conditions ranging from severe trauma to infection.1–3
During these procedures, an implant is placed under the conjunctiva and Tenon’s capsule and a removable conformer is placed over the conjunctiva, which maintain the shape and volume of the eye socket.4 Most sockets are considered healed at 4–6 weeks, after which patients are typically referred to an ocularist for a series of appointments to have a custom ocular prosthesis made.4 The ocular prosthesis maintains the conjunctival fornix and is painted to match the fellow eye. Wearing the prosthesis is an important step in the reconstruction and rehabilitation of the eye socket. Disfigurement from trauma that alters one’s appearance can lead to increased risk of anxiety, depression, stigma, discrimination, social isolation, and suicide,5 and numerous studies have documented the psychosocial benefits of ocular prostheses including improved self-esteem, social interaction, and overall well-being.6–8
Previous studies have examined the characteristics of patients who undergo eye removal surgery,9,10 as well as those who wear ocular prostheses.6,11 However, current literature is limited in examining the characteristics of patients who do not attain ocular prostheses. A study by Krakauer et al found that only 10.5–25% of their patients who underwent either primary or secondary eye removal surgery wore prostheses at last follow-up.11 Makrakis et al reported on 26 anophthalmic patients who did not have a prosthesis, and hypothesized lack of finances to be the most likely barrier as the majority of participants were of low socioeconomic status.7
Whilst most major insurance plans in the United States provide partial or full coverage for an acrylic ocular prosthesis, out-of-pocket costs can range from anywhere between $2,000-$8,300 for those without insurance or with non-eligible insurance policies.12,13 Considering that ocular trauma is the leading cause of enucleation in the US,14 and low socioeconomic status has been associated with a higher incidence of globe injury,15 the cost may be deterring patients from attaining an ocular prosthesis. Additionally, recent studies underscore geographic service disparities of eye care providers as well as the increased need for skilled ocularists in resource-limited areas, which can further serve as a persistent barrier.16,17 Innovations in digital fabrication and 3D printing have enhanced customization and reduced production costs, but these methods are not yet widely accessible.4
While the global market for ocular prostheses continues to grow, utilization rates remain suboptimal and likely reflect ongoing inequities at both the patient- and system-level.18 Based on this context, the purpose of this study was to evaluate the rate of prosthesis use amongst anophthalmic patients using retrospective chart review, and to investigate the possible impact of socioeconomic factors on prosthesis usage using prospective patient interviews. To our knowledge, this is the first study to also interview patients who did not get a prosthesis. By integrating retrospective clinical data with qualitative patient-reported barriers collected via telephone interviews, this study seeks to provide a more comprehensive and patient-centered understanding of factors influencing ocular prosthetic use, which has been underexplored in prior research. We hypothesized that factors such as insurance type, employment status, and follow-up consistency significantly influence ocular prosthesis acquisition among anophthalmic patients.
Methods/Material
This study was conducted in accordance with the Declaration of Helsinki and approved by both the Institutional Review Board of the University of Chicago Medicine and the Institutional Review Board of the Lewis Katz School of Medicine at Temple University. The study was HIPAA-compliant, and there is no disclosure of identifiable health information given. A retrospective chart review was performed for all patients aged 18 years or older who underwent primary or secondary eye removal procedures (identified by CPT codes 15770, 65091, 65093, 65105, 65107, 65130, 65140) by two surgeons at two urban, level 1 trauma centers: The University of Chicago (HS) and Temple University Hospital (MK), as well as a private office in Allentown Pennsylvania (MK) from December 24th, 2013 to February 15th, 2024. Exclusion criteria included individuals under 18 years old at the time of surgery, pregnant women, and currently incarcerated persons. Furthermore, if patients underwent re-operations, only data from their initial surgery was included. A priori power calculation was not performed given the retrospective design; all eligible patients were included.
Data was collected regarding patient demographics, insurance status, surgical indications, type of surgery performed, and prosthesis status at last follow-up. Surgical indications were divided into two categories: chronic disease (eg, phthisis, infection, neovascular glaucoma) and trauma (acute or distant). Patient demographics, when available, included marital status, level of education, zip code at the time of surgery, employment status and cohabitation status at the time of surgery. Mean Household Income was estimated using US Census Bureau data from 2022 based on zip code at time of surgery.
To supplement available data, telephone interviews were conducted with patients to gather additional information on current prosthesis use or barriers to obtaining one (Box 1). Three attempts were made to contact each patient at different times throughout the day. Given minimal risk and study scale, verbal informed consent was obtained over the telephone following an IRB-approved standard script prior to survey administration. Written consent was waived by the IRB. The consent script included study purpose, confidentiality assurances, voluntary participation, and investigator contact information. Interviews were not recorded or transcribed; responses were recorded by surveyors directly. Telephone interview participants were included only after providing verbal consent.
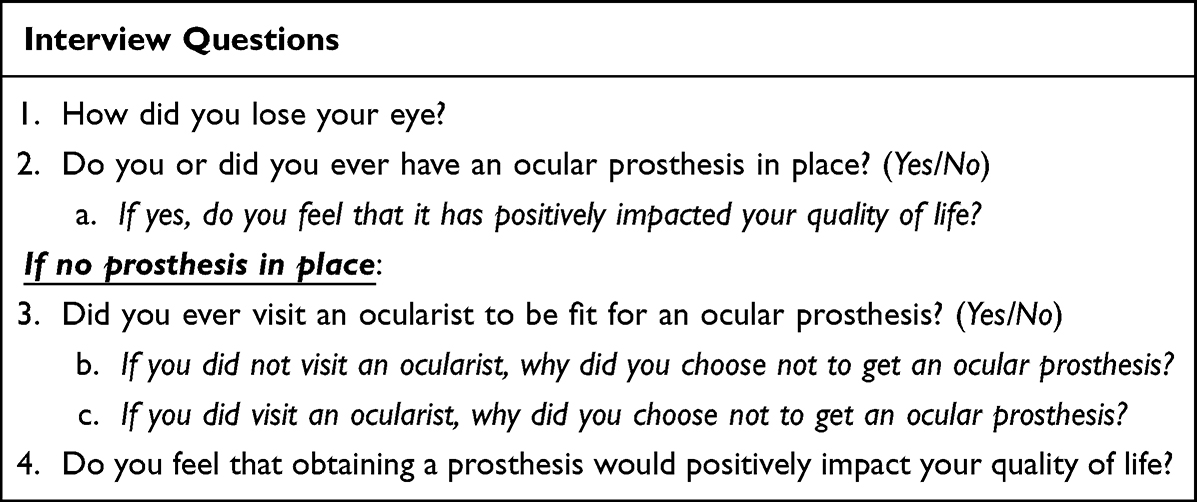 |
Box 1 List of Interview Questions to Assess Current Prosthetic Use Among Patients |
Statistical analyses were performed using R version 4.4.0. Chi-squared and Fisher’s Exact tests were used to analyze categorical variables, and continuous outcomes were compared with unpaired Student’s t-test or Mann–Whitney’s U-test according to data distribution. Normality and heteroskedasticity of continuous data were assessed with Shapiro–Wilk’s and Levene’s tests, respectively. The alpha risk was set to 5%, and two-tailed tests were used. A multivariate logistic regression was performed to assess the relation between prosthetic status and possible explanatory variables. Prespecified covariates included age, sex, race, insurance type, estimated median household income, surgical indication (chronic disease vs trauma), and length of follow-up. Adjusted odds ratios (aORs) with 95% confidence intervals were reported, statistical significance was set at α = 0.05. Patients with missing data were excluded from the analysis.
Results
Baseline Characteristics
One hundred and fifty-two total cases were initially screened across all three sites, 11 patients were excluded due to not meeting age criteria, 3 cases were excluded due to being repeat operations, with 138 unique patients (mean age 52; 55.8% male; 60.1% Black) meeting the study’s inclusion criteria (Figure 1). The mean follow-up duration was 670 days (range 0–3,347; median 232; standard deviation 844). Baseline characteristics are shown in Table 1. Across both sites, most patients were enrolled in government-sponsored health insurance programs (Medicare/Medicaid; 82%). Overall, the most common surgery performed was evisceration (84%). The most prevalent surgical indication was chronic disease leading to blind painful eye (56%). The category of chronic disease included neovascular glaucoma, proliferative diabetic retinopathy, and phthisis bulbi. Of the 138 total patients, 81 (59%) obtained a prosthesis by last follow-up.
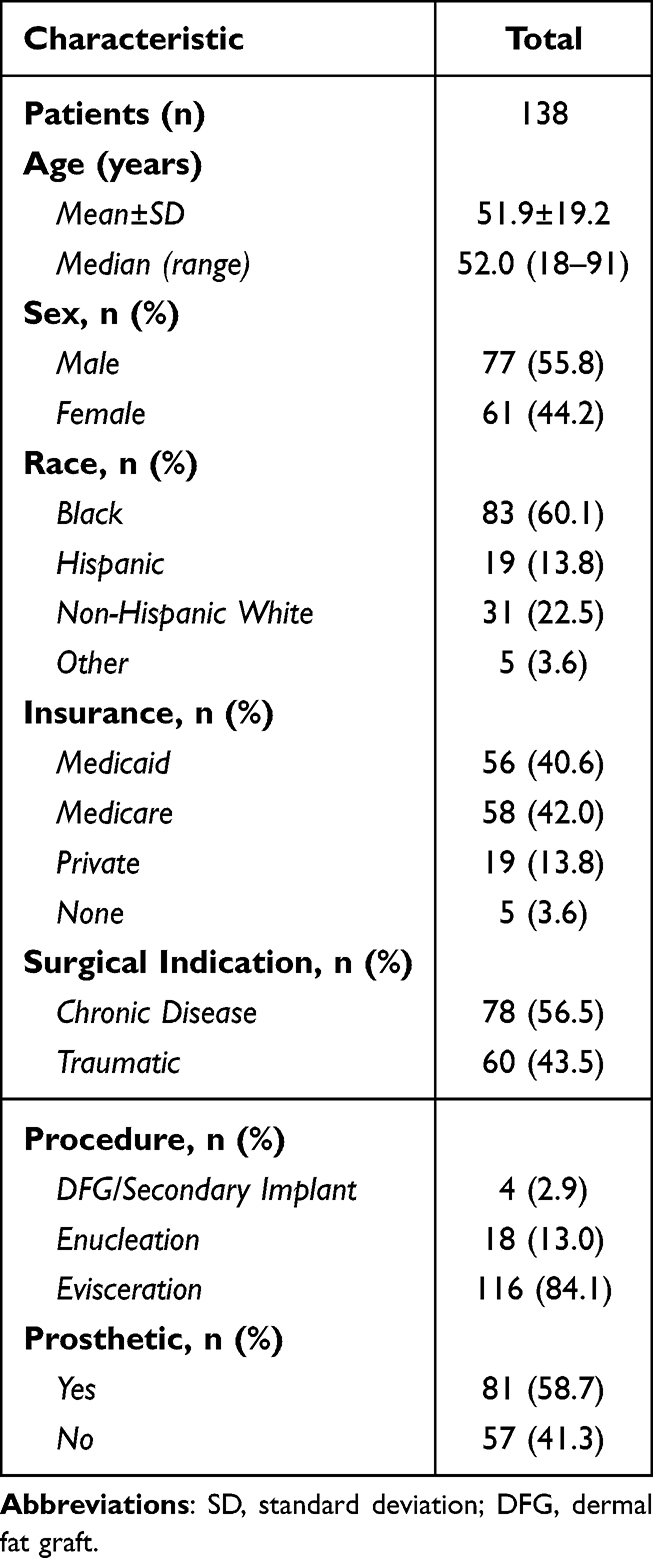 |
Table 1 Baseline Clinical Characteristics and Surgical Indications |
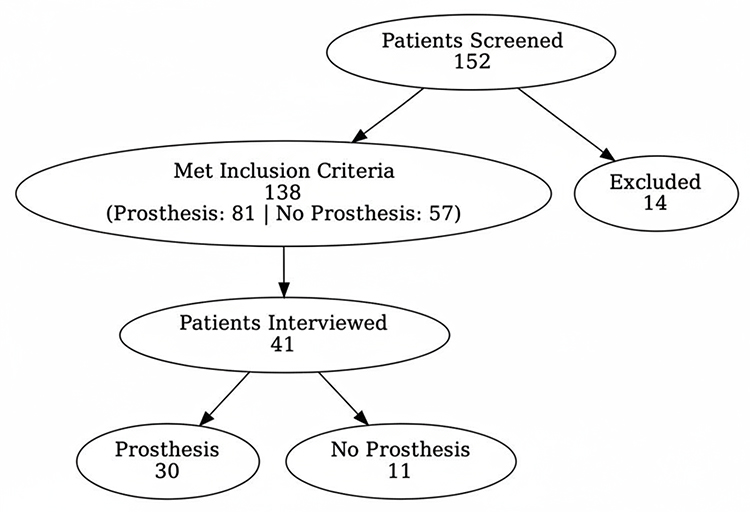 |
Figure 1 Flowchart outlining participant screening, eligibility, and inclusion in interviews. A total of 152 patients were screened, of whom 138 met inclusion criteria (81 with prostheses and 57 without) and 14 were excluded. Among eligible patients, 41 were interviewed (30 with prostheses and 11 without). |
Patients were also grouped by prosthesis status. Compared to the 81 patients with prosthesis, the remaining 57 patients either had the conformer from the operating room in place (n=51) or neither a conformer nor a prosthesis (n=6) at the last follow-up visit (Table 2). There was no significant difference in base demographics and surgical indications between those who received a prosthetic and those who did not. However, patients with a prosthesis were more likely to be employed at the time of surgery, had greater length of follow-up, and were able to be reached for the telephone interview (p=0.036; p<0.001; p=0.008). Additionally, when controlling for age, race, and median income in multivariate analysis, female sex (aOR=2.06, [1.0; 4.27]) and having private insurance (aOR=2.70, [0.84; 8.7]) were slightly predictive of prosthetic status, although not significantly so (p= 0.0516; p=0.0968). One patient had missing data on zip code and estimated household income and was therefore excluded from multivariate analysis.
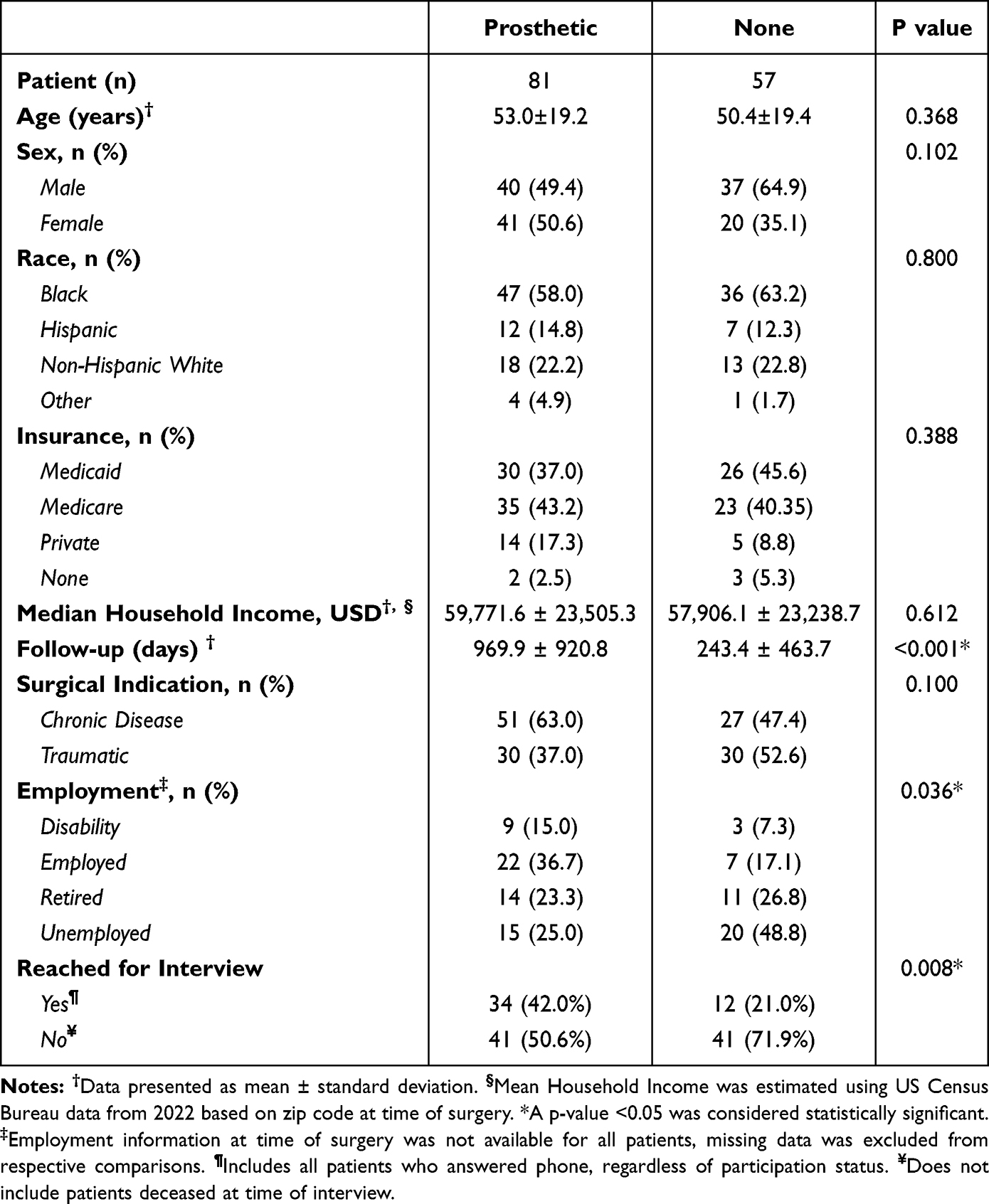 |
Table 2 Demographics of Patient’s Who Acquired Prosthetic Compared to Those Without One |
Interview Responses
Table 3 presents a subset of key responses from the follow-up phone interview, in which patients were asked about their prosthesis or lack thereof. Out of the 138 patients that were contacted by phone, 41 (29.7%) were able to be reached and consented to participate, 50 (36.2%) were not able to be reached after multiple attempts, 32 (23.2%) had disconnected phone lines or outdated contact information, 10 (7.2%) were deceased at time of interview, and 5 (3.6%) declined participation. Thirty out of 41 patients (73.2%) who participated in the survey had received a prosthesis. Twenty-six of the 30 patients with a prosthesis agreed that the prosthesis positively impacted their quality of life, with stated reasons ranging from reduced pain to satisfaction with fit and increased self-confidence. Patients who were not fully satisfied with their prosthesis cited reasons such as irritation (n=3), misalignment/improper sizing (n=2), and it not looking similar enough to their other eye (n=1).
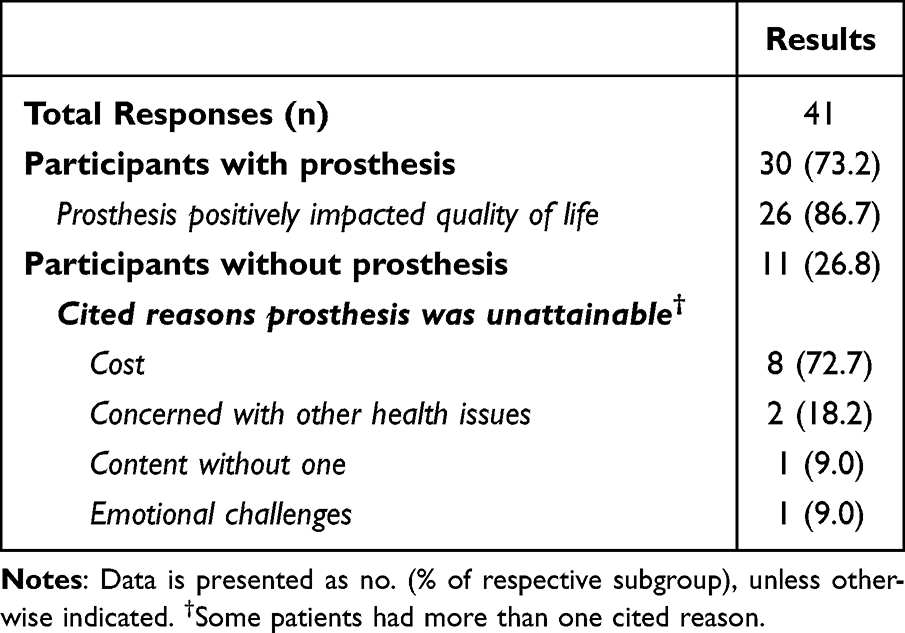 |
Table 3 Phone Interview Results |
For the eleven respondents (26.8%) who had not attained a prosthesis, the most cited barrier was cost (72.7%). Other reasons included greater concern with comorbid health issues which took precedence, emotional challenges adjusting to new monocular baseline, as well as patient contentment without one. In multivariate analysis, patients with a prosthesis and those who had trauma as a surgical indication were associated with increased rate of interview response (aOR=4.32, [1.71; 10.94], p< 0.01; aOR=2.79, [1.13; 6.88], p= 0.0265), while age (p= 0.374), sex (p= 0.591), median household income (p= 0.592), and length of follow-up (p= 0.256) did not show any association.
Discussion
This study provides valuable insights into the utilization of ocular prostheses following eye removal procedures. Interviews with anopthalmic patients showed that the use of a prosthetic eye is an accessible and satisfactory outcome for most patients who seek to get one.
While patients who received a prosthesis were more likely to be employed at the time of their surgery, we found no significant differences between having a prosthesis and demographic factors such as race, age, or estimated median household income. While the link between employment status and prosthetic use aligns well with previous reports on the interplay of high socioeconomic standing and prosthetic acquisition, the lack of significant difference between groups in other demographic factors may be attributed to other reasons.7,11 First, a high proportion (82%) of our patients were enrolled in government-assisted medical insurance programs, which often have benefits to provide full or partial coverage for eye prostheses.12 Additionally, these results may also indicate that zip code is a poor proxy for ability to afford a prosthesis, since income can vary widely within a zip code. Five percent of patients did not have health insurance at the time of eye removal surgery (Table 1), which is less than the percent of uninsured in these zip codes based on data available from the National Institutes of Health.19 The vast majority of surgery was done as an outpatient, and only patients with insurance could reasonably afford the cost of this surgery.
Interestingly, when controlling for other variables, female sex and private insurance trended towards increased likelihood of obtaining a prosthetic. The association between female sex and higher rates of prosthetic use may be related to societal factors and psychological considerations. Trends in existing literature suggest women generally place higher importance on facial appearance and are more likely to pursue cosmetic interventions.20,21 This tendency may extend to ocular prostheses, which serve both psychosocial and aesthetic purposes.
The correlation between private insurance and higher prosthetic use rates may not only reflect greater financial resources that allow for increased spending but also a higher reimbursement rate to the ocularist compared to Medicare or Medicaid, and thereby greater access to ocularists.22 This also highlights the potential beneficial role of consistent follow-up, which was found to have a strong association with increased prosthetic use in our study. The postoperative period following eye-removal surgery can be difficult, with most eyes not considered healed until 4–6 weeks later.23 Consistent follow-up appointments with an ophthalmologist can support patients in their recovery process and in eventually connecting them to their local ocularist for creation of a prosthesis. Decreased follow-up time or loss to follow-up status has been associated with increased complication rates and can negatively impact candidacy for prosthesis in the future.24
Phone interviews were also conducted with a subset of patients to assess sentiment towards prosthetics. The majority of respondents (87%) reported positive impacts of their ocular prosthetic on their quality of life, citing reduced pain and increased self-confidence – which aligns with previous literature on the psychosocial benefits of facial prosthetics.8 Cost was cited as the most common barrier to obtaining a prosthesis among those who did not receive one. This barrier encompasses not only the cost of the product but also expenses associated with follow-up visits, ocularist appointments, and fittings, which can all be prohibitive – especially in resource-limited settings or amongst patients with multiple other comorbid issues such as in our patient population. Although financial limitations were common among our cohort, recent literature underscores that barriers to ocular prosthesis access extend beyond financial constraints, encompassing significant psychological factors. For example, anxiety, social isolation, and adjustment to monocular vision can impede patients’ pursuit of prosthetic rehabilitation, suggesting the need for integrated psychological support alongside clinical care.5,6 This sentiment was shared explicitly by one young interview participant who mentioned that he “mentally wasn’t ready [for a prosthesis] at the time.” Healthcare access disparities also persist, with geographic shortages of skilled ocularists and variable insurance reimbursement rates further limiting prosthesis acquisition, especially in underserved populations.16,17
Despite providing insightful information, telephone questionnaires notably yielded low response rates despite multiple attempts and voicemails. In some capacity, these findings are to be expected due to a general reluctance to answer unknown phone numbers or discuss medical information.25 However, although a small portion of patients actively declined to participate due to privacy concerns, a significant portion of patients (23.2%) also had disconnected numbers or outdated contact information. While these changes may have been made intentionally, the high rates of disconnected numbers may also obscure the prevalence of SIM turnover - a generally involuntary phenomenon in which consumers of pre-paid plans lose or fail to retain their SIM card and have to obtain a replacement to use mobile services.26 High rates of phone number turnover have also been associated with low socioeconomic status and may arise from losing possession of a phone (lost, stolen, broken, etc) and the subsequent inability to obtain a replacement due to resource constraints.27 As survey respondents identified cost as the most significant barrier to obtaining an ocular prosthesis, these findings from non-respondents may serve as a proxy to further suggest that a large proportion of our patient population face socioeconomic instability and therefore would benefit from meaningful interventions to improve post-operative care.
Lastly, we observed a trend of higher prosthetic use among patients with chronic eye disease compared to those with traumatic eye loss (63.0% vs 37.0%). Although not statistically significant, this may be attributed to the established routine of follow-up visits for disease progression, allowing patients more time to understand their condition and consider prosthetic options. Additionally, the later onset of many chronic eye diseases coincides with Medicare eligibility or established private insurance coverage, potentially mitigating cost barriers. This finding underscores the potential need for improving patient education and support systems for trauma patients, which may help increase prosthetic utilization in this group.
Overall, our study provides valuable insights into the factors influencing ocular prosthetic use following eye removal surgery. The findings underscore the importance of consistent follow-up care, comprehensive insurance coverage, and addressing additional financial barriers to improve prosthetic utilization rates.
Addressing these disparities and improving outcomes for all patients can be approached through a variety of potential interventions. Based on these findings, we propose healthcare providers could consider offering standard-sized premade prostheses as an alternative to conformers placed during surgery, particularly for high-risk patients who may be unlikely to get a prosthesis. These pre-manufactured ocular prostheses comes in various sizes and shapes, can be fitted quickly, and are generally less expensive than custom-made prosthesis.28 However, to our knowledge, there is not a mainstream supplier of stock ocular prostheses at this time. Stryker Corporation used to make one but has discontinued it. 3D printing has recently been used to make ocular prostheses in a pilot study, however they are not yet commercially available.4 Other potential methods include a “sew-on iris” technique described by Ganokwalai et al that offers a more affordable, yet effective, alternative to traditional methods of fabricating prostheses.29
Additional interventions to target disparities in prosthesis obtainment include integrating ocularist visits with surgeon follow-ups. In addition to financial constraints, many low-income patients also face additional barriers to care such as transportation and limited time off.30,31 Coordinated care reduces logistical barriers and provides a more accessible and streamlined care pathway to improve outcomes in marginalized populations. However, this may not be practical for the ocularist, given the relatively low volume of prospective patients at a single office, and unreliable patient follow-up. Finally, providing transparent cost information from ocularists and exploring payment plan options could help dispel cost anxiety and address financial barriers that prevent some patients from obtaining prostheses.
While our study provides valuable and novel insights, limitations include the retrospective nature, which introduces recall bias and imposes limitations on causal interpretation, a relatively small sample size, which potentially limited our ability to make statistically significant correlations in our data analysis, and potential lack of generalizability particularly to rural and suburban populations. Additionally, voluntary phone interviews are prone to response bias which was evident by a significant proportion of respondents having a prosthesis and may have skewed these results to a more positive perspective. A large proportion of phone numbers were disconnected or no longer in service, which may have masked responses from patients of lower socioeconomic standing or other high-risk populations (non-response bias).32 Future research should focus on larger, multi-center studies in diverse locations to improve generalizability, prospective studies evaluating the impact of proposed interventions, and long-term follow-up studies assessing the impact of prosthetic use on quality of life over time. Additionally, telephone questionnaires could be administered at post operative appointments to reduce potential bias and increase response numbers.
In conclusion, this study adds to the understanding of ocular prosthetic use and identifies key factors influencing prosthetic acquisition and utilization. Prosthesis acquisition remained limited (<60%) despite high rates of government-sponsored insurance. While lack of prosthesis among our population was common, factors such as female sex, employment, private insurance, or consistent follow-up may all increase the likelihood of attainment. Unreachable patients and poor follow-up likely reflect socioeconomic instability that constrains postoperative care and access. Due to the retrospective cohort design, however, this study can only demonstrate associations between variables and prosthesis use, and causal inferences should thus be made cautiously. Clinically, these findings emphasize the need for ophthalmologists and ocularists to prioritize coordinated care pathways, ensure patient education regarding prosthesis benefits, and address financial barriers proactively. Future research should focus on prospective studies to validate these associations, evaluate interventions to improve prosthesis access, and longitudinally assess quality-of-life outcomes post-prosthesis acquisition, particularly in diverse and underserved populations. We hope that these results can guide future work predicated on improving access and outcomes for all anophthalmic patients, particularly through innovative prosthetic technologies and streamlined care pathways.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was not supported by any external funding agencies.
Disclosure
The authors report no competing interests in this work.
References
1. Phan L, Hwang T, McCulley T. Evisceration in the modern age. Middle East Afr J Ophthalmol. 2012;19(1):24. doi:10.4103/0974-9233.92113
2. Sami D, Young S, Petersen R. Perspective on orbital enucleation implants. Surv Ophthalmol. 2007;52(3):244–265. doi:10.1016/j.survophthal.2007.02.007
3. Nazar NA, Hendriati. Evisceration versus enucleation in ocular globe injury. Bioscmed. 2022;6(6):1837–1851. doi:10.37275/bsm.v6i6.524
4. Reinhard J, Urban P, Bell S, Carpenter D, Sagoo MS. Automatic data-driven design and 3D printing of custom ocular prostheses. Nat Commun. 2024;15(1):1360. doi:10.1038/s41467-024-45345-5
5. Keys J, Dempster M, Jackson J, Williams M, Coyle S. The psychosocial impact of losing an eye through traumatic injury and living with prosthetic restoration: a thematic analysis. Acta Psychol. 2021;219:103383. doi:10.1016/j.actpsy.2021.103383
6. Boele FW, Kawalek JC, Nicklin E, et al. Living with an artificial eye: qualitative insights into patient and family member experiences. Int Ophthalmol. 2024;44(1):227. doi:10.1007/s10792-024-02933-0
7. Makrakis LR, de Araújo CB, Macedo AP, Silva-Lovato CH. The impact of an ocular prosthesis on the quality of life, perceived stress, and clinical adaptation of anophthalmic patients: a clinical and longitudinal trial. J Prosthodont. 2021;30(5):394–400. doi:10.1111/jopr.13332
8. Goiato MC, Dos Santos DM, Bannwart LC, et al. Psychosocial impact on anophthalmic patients wearing ocular prosthesis. Int J Oral Maxillofac Surg. 2013;42(1):113–119. doi:10.1016/j.ijom.2012.05.028
9. Gauthier AC, Oduyale OK, Fliotsos MJ, et al. Clinical characteristics and outcomes in patients undergoing primary or secondary enucleation or evisceration after ocular trauma. OPTH. 2020;14:3499–3506. doi:10.2147/OPTH.S273760
10. Serbest Ceylanoglu K. A decade of evisceration: investigating the influence of demographic, clinical, and psychosocial factors. Beyoglu Eye J. 2024;115–119. doi:10.14744/bej.2023.48640
11. Krakauer M, Jennings E, Gupta L, et al. A comparison of primary and secondary eye removal after open globe injury: a multi-centre study. Eye. 2023;37(6):1249–1253. doi:10.1038/s41433-022-02098-z
12. Centers for Medicare & Medicaid Services. Eye prostheses - policy article. Medicare coverage database, Article ID: A52462, Version 30.
13. Healthline. Prosthetic Eye: cost, Care, Surgery, and More; 2018. Available from: https://www.healthline.com/health/prosthetic-eye.
14. Furdova A, Horkovicova K, Furda R, et al. Two 11-years periods statistics and trends of enucleation and evisceration. J Craniofac Surg. 2021;32(8):2701–2705. doi:10.1097/SCS.0000000000007727
15. Kousiouris P, Klavdianou O, Douglas KA, et al. Role of socioeconomic status (SES) in globe injuries: a review. OPTH. 2022;16:25–31. doi:10.2147/OPTH.S317017
16. Gibson DM. The geographic distribution of eye care providers in the United States: implications for a national strategy to improve vision health. Prev Med. 2015;73:30–36. doi:10.1016/j.ypmed.2015.01.008
17. Changal N, AlRasheed W, Khandekar R. Ocularists the less known mid eye care professionals and their contribution in eye health care. Saudi J Ophthalmol. 2020;34(3):195–197. doi:10.4103/1319-4534.310403
18. Modugno A, Mantelli F, Sposato S, Moretti C, Lambiase A, Bonini S. Ocular prostheses in the last century: a retrospective analysis of 8018 patients. Eye. 2013;27(7):865–870. doi:10.1038/eye.2013.97
19. HDPulse: an ecosystem of minority health and health disparities resources. National Institute on Minority Health and Health Disparities; 2025. Available from: https://hdpulse.nimhd.nih.gov.
20. Alotaibi AS. Demographic and cultural differences in the acceptance and pursuit of cosmetic surgery: a systematic literature review. Plastic Reconstructive Surg. 2021;9(3):e3501. doi:10.1097/GOX.0000000000003501
21. Cash TF, Cash DW. Women’s use of cosmetics: psychosocial correlates and consequences. Intern J Cosmetic Sci. 1982;4(1):1–14. doi:10.1111/j.1467-2494.1982.tb00295.x
22. Fan C, Li C, Song X. The relationship between health insurance and economic performance: an empirical study based on meta-analysis. Front Public Health. 2024;12:1365877. doi:10.3389/fpubh.2024.1365877
23. Koch KR, Trester W, Müller-Uri N, Trester M, Cursiefen C, Heindl LM. Augenprothetische Versorgung: anpassung, Handhabung und Komplikationen. Ophthalmologe. 2016;113(2):133–142. doi:10.1007/s00347-015-0091-x
24. Verhoekx JSN, Tse WHW, Rengifo Coolman A, van Kinderen YB, Wubbels RJ, Paridaens D. Complications following enucleations and subsequent oculoplastic surgeries. Ophthalmic Plast Reconstr Surg. 2018;34(4):320–323. doi:10.1097/IOP.0000000000000966
25. Glass D, Kelsall H, Slegers C, et al. A telephone survey of factors affecting willingness to participate in health research surveys. BMC Public Health. 2015;15(1):1017. doi:10.1186/s12889-015-2350-9
26. Roessler P. The mobile phone revolution and digital inequality: scope, determinants and consequences. Prosperity Comm Backgr Pap Ser. 2018;15:1–39.
27. Rhoades H, Wenzel S, Rice E, Winetrobe H, Henwood B. No digital divide? Technology use among homeless adults. J Soc Distress Homeless. 2017;26(1):73–77. doi:10.1080/10530789.2017.1305140
28. Cevik P, Dilber E, Eraslan O. Different techniques in fabrication of ocular prosthesis. J Craniofacial Surgery. 2012;23(6):1779–1781. doi:10.1097/SCS.0b013e31826701bb
29. Ganokwalai N, Towithelertkul C, Punyawattananon V, Srithavaj T. A sew-on iris technique for the fabrication of ocular prostheses. J Prosthetic Dent. 2024;S0022391324007091. doi:10.1016/j.prosdent.2024.10.016
30. Solomon SD, Shoge RY, Ervin AM, et al. Improving access to eye care. Ophthalmology. 2022;129(10):e114–e126. doi:10.1016/j.ophtha.2022.07.012
31. Hemmerich C, Jones G, Staggs J, Anderson RM, Bacani R, Vassar M. Inequities and research gaps in ophthalmology: a scoping review. JAMA Ophthalmol. 2023;141(1):63. doi:10.1001/jamaophthalmol.2022.5237
32. Thomas S, Heinrich S, Kühnlein A, Radon K. The association between socioeconomic status and exposure to mobile telecommunication networks in children and adolescents. Bioelectromagnetics. 2010;31(1):20–27. doi:10.1002/bem.20522
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.