Back to Journals » Open Access Emergency Medicine » Volume 14
Factors Affecting Cardiopulmonary Resuscitation Practice Among Nurses in Mizan Tepi University Teaching Hospital, Tepi General Hospital, and Gebretsadik Shawo Hospital, Southwest Ethiopia
Authors Guteta M ![]()
Received 21 December 2021
Accepted for publication 6 April 2022
Published 18 April 2022 Volume 2022:14 Pages 165—175
DOI https://doi.org/10.2147/OAEM.S350244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Mirresa Guteta
Nursing Department, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Mirresa Guteta, Email [email protected]
Background: Cardiopulmonary resuscitation is one of the basic lifesaving medical procedures which is performed for a patient with an emergency such as cardiac arrest, suffocation, near-dying, or circumstance that results in cardiac or pulmonary failure or both.
Objective: To assess factors affecting the practice of cardiopulmonary resuscitation among nurses at Mizan Tepi University Teaching Hospital, Tepi General Hospital, and Gebretsadik Shawo Hospital.
Methods: Institution-based cross-sectional study which was supported by qualitative data conducted from March 20 to April 20, 2021. Nurses who answered ≥ 7 CPR practice questions correctly were considered to have good practice. Data were entered into EpiData version 4.4 and exported to SPSS version 23 for data analysis. A multivariable logistic regression model was fitted, adjusted odds ratio (AOR) at 95% confidence interval and p-value < 0.05 were estimated to determine the statistically significant association between predictors and outcome variable. Qualitative data were analyzed based on thematic content.
Results: The prevalence of good practice towards CPR was 31.8% (95% CI: 27.5– 36.3) in the study area. Experience of 6– 10 years (AOR = 2.27, 95% CI: 1.25– 4.13) and > 10 years (AOR= 1.81, 95% CI: 1.10– 2.98), rarely (AOR = 3.77, 95% CI: 1.26– 11.30) or actively (AOR = 4.60, 95% CI: 1.51– 13.98) involved in CPR practice, assigned to emergency department (AOR = 1.02, 95% CI: 0.55– 1.90), having CPR good knowledge (AOR = 1.37, 95% CI: 0.28– 2.14) and having a nursing degree (AOR = 1.54, 95% CI: 0.93– 2.54) were predictors of CPR good practice.
Conclusion: Nurses’ good practice towards cardiopulmonary resuscitation was low. Therefore, efforts should be taken to enhance nurses’ practice towards cardiopulmonary resuscitation.
Keywords: practice, nurse, cardiopulmonary resuscitation, associated factors
Introduction
Cardiopulmonary resuscitation (CPR) is an organized medical maneuver through which chest compressions and artificial breathing are given to provide sufficient blood perfusion towards major organs including the brain and heart. Cardiopulmonary resuscitation can be a life-saving procedure performed for a patient in an emergency such as cardiac arrest, suffocation, near-drowning, electrocution injuries, or any condition in which a victim’s respiration or circulation has stopped.1–3
Health professionals including nurses working in the hospital can reduce mortality resulting from cardiac and respiratory-related problems when they are equipped with the knowledge and skill of cardiopulmonary resuscitation. As a result, nurses should be equipped with the knowledge and skill of basic life support to avert critical medical-surgical emergencies.4–6
Appropriate CPR is crucial for the survival of cardiopulmonary arrest sufferers. The chance of survival in cardiopulmonary arrest is reduced by 7–10% for each minute of CPR delay. Additionally, CPR can decrease the length of hospital stay. One of the indications for CPR in cardiac arrest is caused by failure of the blood circulation due to a cardiac problem.7–9
For the better outcome of the patients, applying CPR early is most effective. Providing frequently updated training about cardiopulmonary resuscitation for emergency care health providers can improve the survival rate of the patients.10,11
Among health professionals working in a health-care setting, nurses are the ones who face problems that need CPR procedure and perform the procedure. Even though CPR is among the important of procedures for saving the life of patients, studies depict that the skill of nurses regarding the procedure is deficient. To perform CPR procedures properly the nurse is expected to have updated knowledge and skill of cardiopulmonary resuscitation.12,13
Various international and country-based verified protocols for CPR are endorsed and official training programs depending on these guidelines have been implemented by certified training centers.14,15
Cardiopulmonary resuscitation is a rescue intervention, executed to maintain survival of patients until additional management can be given.16–19 Based on different studies nurses have good knowledge and a positive attitude toward CPR, but they have a gap in practice.4,5
The objective of this study was to assess factors affecting the application of CPR among nurses working in the selected three hospitals.
Materials and Methods
Study Area and Period
The study was carried out in Mizan Tepi University Teaching Hospital (MTUTH), Tepi General Hospital, and Gebretsadik Shawo Hospital located in Bench Sheko, Sheka, and Kefa Zones from March 20 to April 20, 2021. MTUTH is in Bech Sheko Zone 560 km distant from the capital city of Ethiopia, Addis Ababa; Tepi General Hospital is in Sheka Zone, 565 km away from Addis Ababa; and Gebretsadik Shawo Hospital is located in Kefa Zone which is 411 km away from Addis Ababa. The three hospitals provide surgical, gynecological and obstetric, general medical, pediatrics, minor and major operations, ophthalmologic and diagnostic services. They have different health professionals in different fields of study and qualifications.
Study design: Institution-based cross-sectional study design which included both qualitative and quantitative data collection methods was used.
Inclusion and exclusion criteria: All nurses’ working in the three hospitals were incorporated in the study whereas those nurses on permitted leave or assigned to the hospital for less than 6 months were excluded from the study.
Sample size and sampling procedure: All available nurses in the three hospitals during the data collection period were incorporated in the study by using a census (Figure 1).
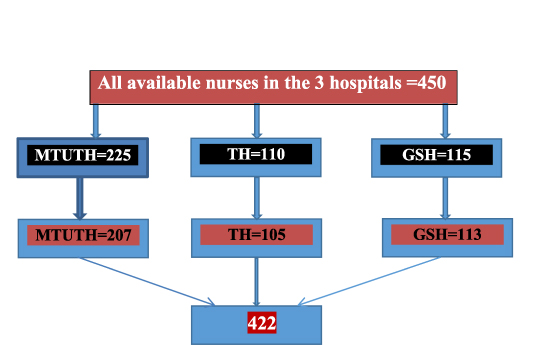 |
Figure 1 Schematic presentation of sampling procedure in MTUTH, Tepi General Hospital and Gebretsadik Shawo Hospital, Southwest Ethiopia. Abbreviations: CPR, cardiopulmonary resuscitation; MTUTH, Mizan Tepi University Teaching Hospital. |
Operational Definition
CPR knowledge: Cardiopulmonary resuscitation knowledge questions comprise 12 questions which were coded as 1 for the right answer and 0 for the wrong answer by SPSS. The maximum and minimum knowledge scores were 12 and 0; knowledge scores were categorized whereby scores from 9–12 were grouped as good knowledge while scores from 0–8 were grouped as poor knowledge.
CPR practice: Cardiopulmonary resuscitation practice questions comprise 9 questions which were coded as 1 for right answer and 0 for the wrong answer. The maximum and minimum practice scores were 9 and 0, practice scores were categorized whereby scores from 7–9 were grouped as good practice while scores from 0–6 were grouped as poor practice.
CPR training: Nurses who have taken CPR training for the last year are counted as having regular training.
Work experience: Total years of experience after nurses graduate and start working.
CPR involvement: Those nurses who frequently participated in the CPR procedure were considered as actively involved, those involved seldom were considered as rarely involved, and those not involved at all were considered as never involved.
Data Collection instrument: The data were gathered through a pretested and organized tool which was adopted from other similar studies done before, and the English version was used. The tool consists of three parts. Part I: socio-demographic characteristics comprising 7 items. Part II: Cardiopulmonary resuscitation knowledge questions comprising 12 questions which were coded as 1 for the right answer and 0 for the wrong answer. The maximum and minimum knowledge scores were 12 and 0, knowledge scores were categorized whereby scores from 9–12 were grouped as good knowledge while scores from 0–8 were grouped as poor knowledge. Part III: Cardiopulmonary resuscitation practice questions comprising 9 questions which were coded as 1 for right answer and 0 for the wrong answer. The maximum and minimum practice scores were 9 and 0, practice scores were categorized whereby scores from 7–9 were grouped as good practice while scores from 0–6 were grouped as poor practice. Data collection was undertaken by six data collectors and three supervisors.
Data Collection technique: The data were gathered through an interviewer-administered tool. Qualitative data collection was conducted by the researcher himself using a checklist.
Data Quality Assurance
Before conducting actual data collection, the tool was pretested on 5% of samples at Chena primary hospital. The pretest aimed to assure the study participants can understand the questions and to check the sequence of the tool. Based on the result of pretest mitigation was done. The training was given for data collectors and supervisors on the intention of the study, approach to contact with study participants, and data collection techniques. Completeness, precision and coherence of data were verified by supervisors who also provided feedback accordingly throughout data gathering time. Finally, data were coded, cleaned, entered, and checked for completeness before analysis.
Processing and Analysis of the Data
EpiData version 4.4 was used for data entry and SPSS version 23 was utilized for analysis. Data exploration was conducted to examine different characteristics of the data and descriptive statistics were used to describe the data depending on its nature. After cleaning of the data, descriptive statistics such as frequencies, proportions, and percentages were done.
After checking all assumptions of logistic regression such as independent observations (multicollinearity among independent variables, linearity of independent variables, and log odds of the dependent variable), bivariable logistic regression was carried out to select a candidate for multivariate logistic regression analysis with a p-value <0.25 at 95% confidence level. Then, candidate variables were entered into a multivariable logistic regressions model using the backward method to identify the statistically significant factors for cardiopulmonary resuscitation by controlling possible confounders. The degree of association between dependent and independent variables was assessed using odds ratio and statistically significant factors were declared at 95% confidence interval and a p-value <0.05.
Computation
The multiple-choice questions which assess the knowledge were changed into yes and no which stand for correct and incorrect answers respectively. This choice question which was assessing the practice was also transformed into yes and no to represent good practice and poor practice respectively.
Results
Demographic and Socio-Economic Characteristics
In this study, 422 nurses working in the selected three hospitals participated and yielded a 100% response rate. Among these 250 (59.2%) were female and 172 (40.8%) were male. Regarding marital status and age of the study participants, 276 (65.4%) were married and 289 (68.5%) of them were aged between 26–30 years. Out of the total, 218 (51.6%) had 6–10 years of working experience. Regarding their qualifications and working unit, 318 (75.5%) had degrees and 282 (66.8%) worked on inpatient wards (Table 1).
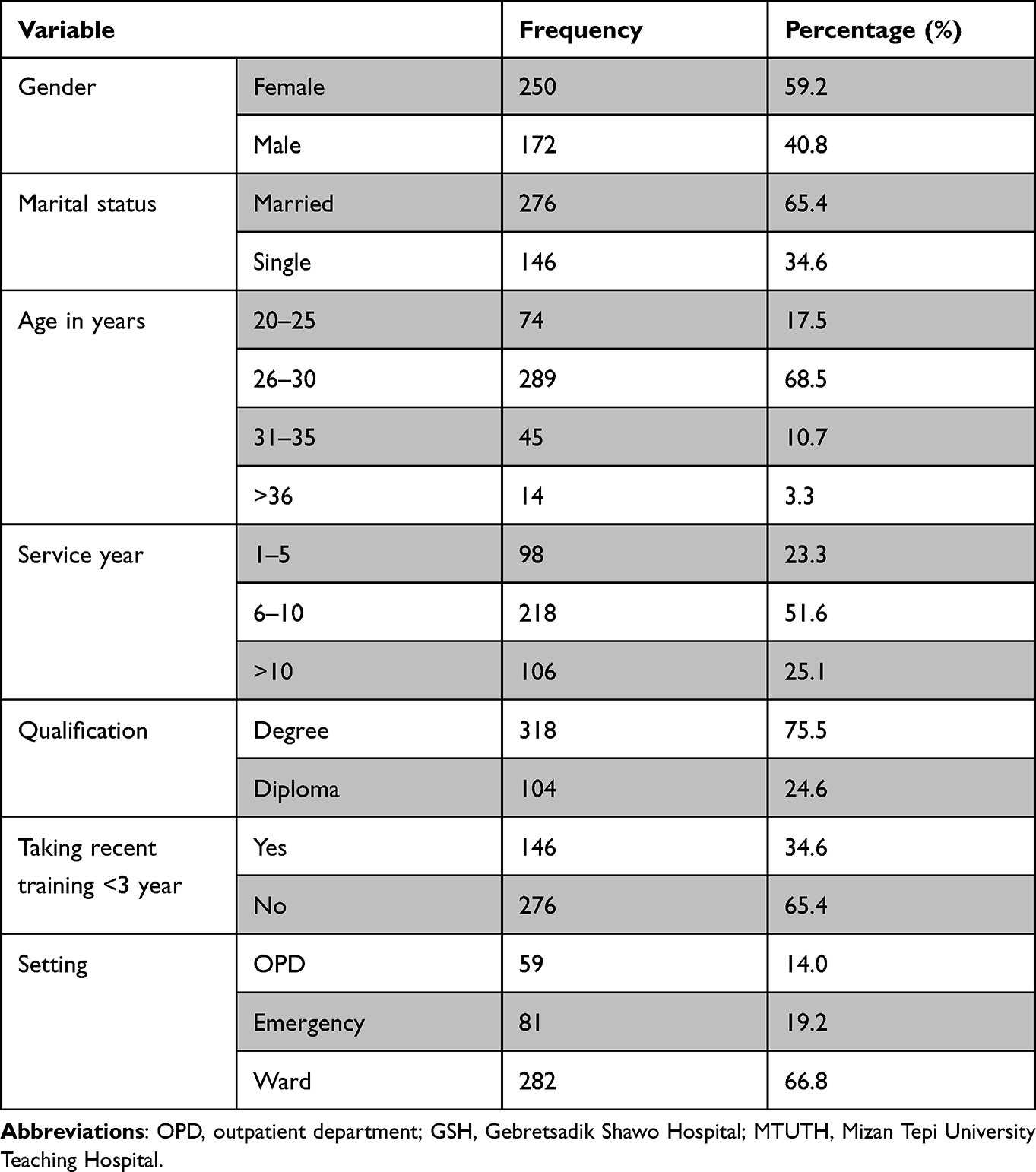 |
Table 1 Demographic and Socio-Economic Characteristics of Nurses Working in MTUTH, Tepi General Hospital and GSH, Southwest Ethiopia |
Knowledge of Nurses Towards CPR
In this study, the level of good knowledge about cardiopulmonary resuscitation was found to be 70.2% among nurses who work in MTUTH, Tepi General Hospital, and Gebretsadik Shawo Hospital. More than half of the respondents responded with the right answer to questions regarding when CPR is most effective, the right way to open the airway before providing mouth-to-mouth respiration, the chance of survival of a victim when CPR is given properly, rescue breaths per cycle, depth of compression and correct placement of hand on the sternum (Table 2).
 |
Table 2 Participants’ Knowledge Response About CPR in MTUTH, TGH, and GSH, SNNPR, Southwest f Ethiopia |
The Practice of Nurses Towards CPR
The prevalence of good practice towards CPR among nurses working in the selected three hospitals was 31.8% (95% CI: 27.5–36.3). The study revealed that 35.7% of the participants had performed cardiopulmonary resuscitation on a patient in cardiac emergencies, 62.9% of the participants checked a patient’s pulse rate before commencing CPR, and 53.6% ensured that the patient was in a supine position on a relatively hard surface before commencing cardiopulmonary resuscitation (Table 3).
 |
Table 3 Participants’ Practice Response About CPR in MTUTH, Tepi General Hospital and Gebretsadik Shawo Hospital, Southwest Ethiopia |
Level of Involvement in Cardiopulmonary Resuscitation
Based on this study 18, 228, and 176 nurses were never, rarely, or actively involved in CPR procedures, respectively (Figure 2).
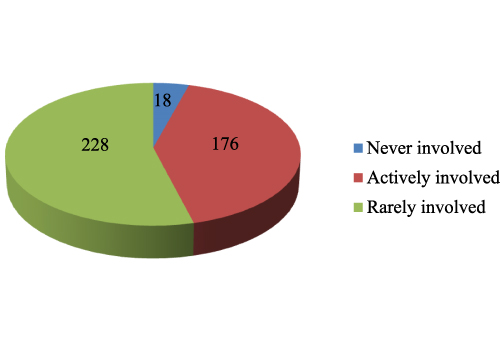 |
Figure 2 Level of involvement in CPR in MTUTH, Tepi General Hospital and Gebretsadik Shawo Hospital, Southwest Ethiopia. Abbreviations: CPR, cardiopulmonary resuscitation; MTUTH, Mizan Tepi University Teaching Hospital. |
Cardiopulmonary Resuscitation and Its Associated Factors
Those independent variables having p-values <0.25 were analyzed in multivariable logistic regression. In bivariable logistic regression analysis, sex, marital status, experience, knowledge, taking CPR training recently, assigned ward, qualification, level of CPR involvement and confidence had p-values <0.25, so were retained for multivariable logistic regression analysis.
However, in multivariable logistic regression, experience, knowledge, qualification, assigned ward, and level of CPR involvement were independent predictors of CPR good practice (Table 4).
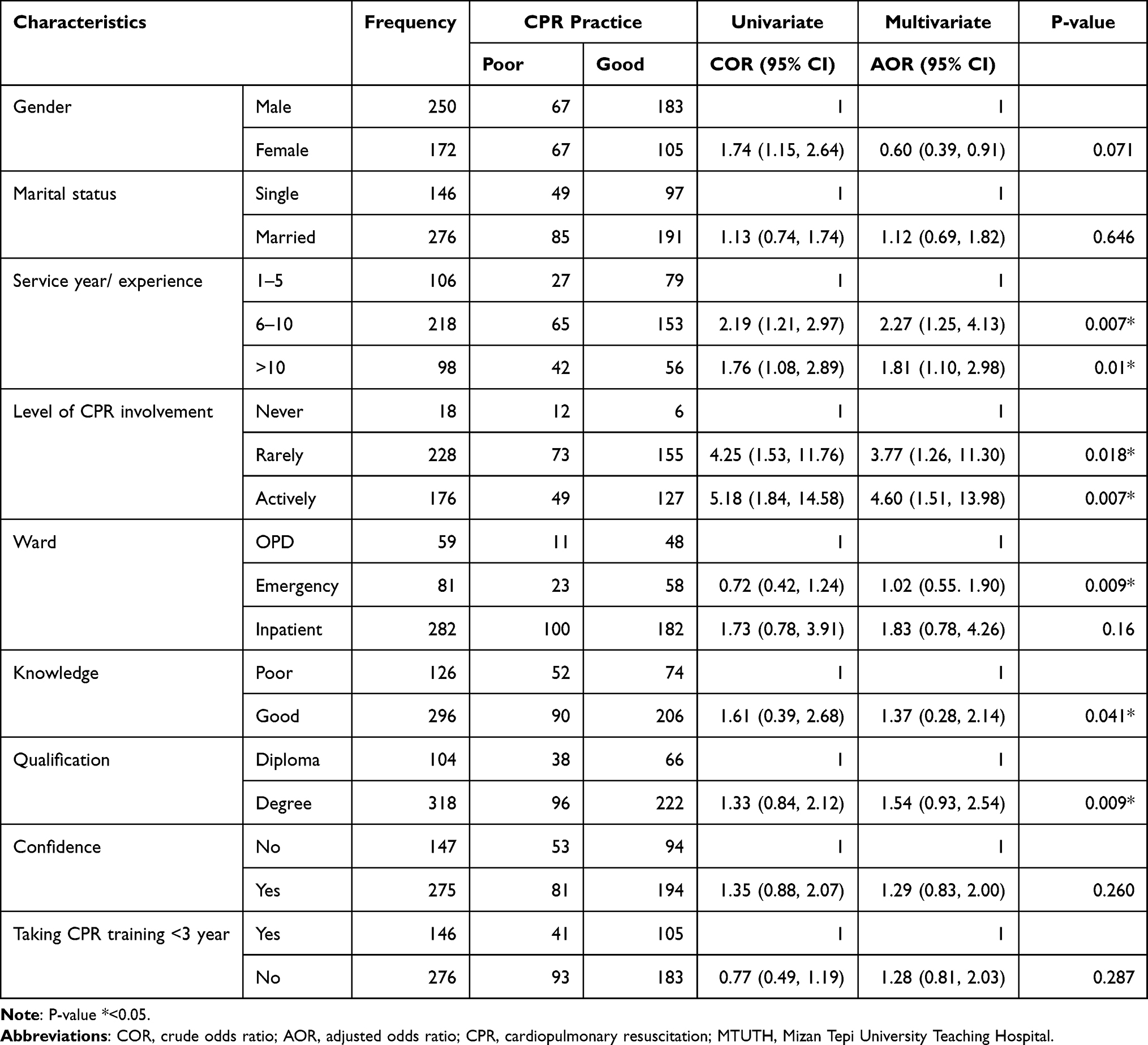 |
Table 4 Bi-Variable and Multi-Variable Logistic Regression Analysis Outcome of Factors Affecting CPR Practice Among Nurses in MTUTH, Tepi General Hospital and Gebretsadik Shawo Hospital, Southwest Ethiopia |
The likelihood of good practice was higher among nurses having 6–10 years experience (AOR = 2.27, 95% CI: 1.25–4.13) and having >10 years experience (AOR = 1.81, 95% CI: 1.10–2.98) compared with those nurses having 1–5 years of work experience.
In this study the likelihood of good practice was higher among nurses either rarely involved in CPR practice (AOR = 3.77, 95% CI: 1.26–11.30) or actively involved in CPR practice (AOR = 4.60, 95% CI: 1.51–13.98) compared with never involved in CPR practice.
The likelihood of good practice was higher among nurses assigned to the emergency department (AOR = 1.02, 95% CI: 0.55–1.90) compared with those assigned to the outpatients department. Similarly, the odds of good practice were higher among nurses having good knowledge about CPR (AOR = 1.37, 95% CI: 0.28–2.14) than in nurses having poor CPR knowledge.
The odds of good practice were higher among nurses with a nursing degree (AOR = 1.54, 95% CI: 0.93–2.54) than nurses with a diploma.
Qualitative Result
Twelve in-depth interviews were done among the heads of nurses from each unit. As a result, the qualitative results were merged into three thematic areas. Those are the provision of CPR training in the study hospital, the personal attitude of study participants toward CPR, and the confidence of nurses to perform the CPR maneuver.
Provision of CPR Training
Cardiopulmonary resuscitation is one of the pivotal lifesaving procedures and detailed knowledge and skills are required to perform it. To acquire the knowledge and skill needed for the practice of CPR procedure requires intensified education in the theoretical class as well as during practical attachment in a real environment through contact with the patients in a health setting. After graduating and beginning professional work in the health setting continuous upgrading of the knowledge and skill of cardiopulmonary resuscitation is very crucial because the maneuvers need recurrent rehearsal since its science is updated through time. Regarding training, there is a gap in providing the training about CPR which has direct or indirect effects on practice of the procedure.
Perception of Nurses About CPR
Conducting cardiopulmonary resuscitation for patients having respiratory or cardiac arrest or both has a great contribution in saving patient lives. Nurses are among the front-line health profession identifying the need for and initiating cardiopulmonary resuscitation. The procedure has a great importance but it needs knowledge, courage, experience, and skill to perform.
Nurses’ Confidence to Perform CPR
Self-confidence is very important to carry out cardiopulmonary resuscitation. Nurses should have self-confidence equally with good knowledge, attitude, skill, and experience to apply CPR. Nurses may have good knowledge about CPR but hesitation in applying the procedure due to lack of confidence in carrying out the maneuver may impose harm on the patient.
Discussion
This study assessed the practice of cardiopulmonary resuscitation and its associated factors among nurses working in the three selected hospitals. The prevalence of good practice towards CPR among nurses was 31.8% (95% CI; 27.5–36.3) in the selected hospitals. The finding was lower than a study carried out in Nigeria which foun 65.2% of the study participants had performed CPR while 34.80% had not practiced CPR.20 Possible explanations might be because of study tool variation in using the cut points, service year variation, and due to their qualification status. The majority of the study participants in this study have not taken enough satisfactory training as they were not able to remember information important to applying CPR.
The finding of this study was higher than a study done in Amhara region referral hospital which was 28.4%.21 The possible explanations might be study tool variation in using the cut points and service year variation. The abovementioned study was done on Basic Life Support which is a vast lifesaving maneuver including CPR.
In this study, the level of good knowledge about cardiopulmonary resuscitation was found to be 70.2%. The result was similar to a study done in Wolaita Sodo Teaching Hospital.18 The possible explanation might be because both studies were done in a similar setting and the study participants’ profiles are similar. In addition, the tool used in both studies was similar.
Based on this study those nurses having good knowledge of CPR are one times more likely to have good practice CPR procedures than nurses having poor knowledge. This finding is supported by a study conducted in Amhara region referral hospitals.21 The possible explanation might be that in order to practice the procedure the grounding is the theoretical knowledge which means knowing might be the driving force to apply it into practice. However, a study done did not reveal a significant association between knowledge and CPR practice.
This study shows an association between CPR good practice and experience. Those nurses who had work experience of 6–10 years and >10 years were 2 and one times more likely to have good CPR practice than those nurses who had 1–5 years of experience, respectively.
This finding is in line with a study done in Japan.22 Experience has an impact to apply the knowledge into practice. Those experienced nurses face a lot of challenges in health settings which provide the courage, strength, and skill to apply cardiopulmonary resuscitation.
In this study, good practice had a significant association with the assigned ward, where those nurses assigned to the emergency department were more likely to have good CPR practice than those nurses assigned to the outpatients department. This finding conforms with a study done in Turkey.23 The possible justification for this might be that most of the time patients visiting emergency departments are those who are severe cases which require cardiopulmonary resuscitation to sustain the life of the victims. As a result, nurses assigned to the emergency department have more chances to face patients who need CPR procedures and perform the maneuvers repeatedly than nurses assigned to another ward.
According to this study frequency of CPR involvement had a significant association with good practice, where nurses rarely or actively involved in CPR practice were three and four times more likely to have good practice than those nurses never involved in CPR practice. This finding conforms with a study conducted in Amhara region referral hospitals and Japan.21,22 This finding may be justified by the fact that when professionals frequently apply their knowledge they have a greater tendency to use their knowledge to practice the skill (behavior).
Findings from this study revealed that nurses’ qualifications had a significant association with good practice, where degree nurses are one times more likely to have good CPR practice than diploma nurses. This finding is in harmony with a study done in Amhara region referral hospitals.21 When a qualified professional nurse is advanced the scope of theoretical as well as practical sessions they cover is increased. Due to this, they begin to apply different procedures including cardiopulmonary resuscitation. Unlike the current finding, research work in Kuwait19 did not show a significant association between good CPR knowledge and nurses’ qualifications.
Limitation
This study has strengths and limitations. Using both qualitative and quantitative data methods and incorporating three different health facilities is considered a strength. Among the possible limitations of the study are recall bias and no indication of source and consequence association.
Conclusion
The prevalence of good practice towards cardiopulmonary resuscitation was 31.8%. Having experience of 6–10 and >10 years, actively or rarely involved with cardiopulmonary resuscitation, being assigned to the emergency department, having good CPR knowledge and having a nursing degree were predictors of cardiopulmonary resuscitation good practice. Nurses’ practice towards cardiopulmonary resuscitation was low. Therefore, efforts should be taken to enhance nurses’ practice towards cardiopulmonary resuscitation.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; CPR, cardiopulmonary resuscitation; GSH, Gebretsadik Shawo Hospital; MTUTH, Mizan Tepi University Teaching Hospital; SPSS, Statistical Package for Social Sciences; TGH, Tepi General Hospital; WHO, World Health Organization.
Data Sharing Statement
The corresponding author will make data available upon reasonable request.
Ethics Approval and Consent to Participate
Institutional Review Board of Mizan Tepi University was providing ethical clearance with the (Ref. No. Nur/0040/13). An official permission letter was secured from the three hospitals. The verbal consent which was approved by Institutional Review Board was taken from study participants after explaining the objective of the study, the risk, and benefit, issues of confidentiality, and the right of participation. Assurance was given for participants to withdraw or not to participate in the study without any hesitancy. This study was conducted per the Declaration of Helsinki.
Acknowledgments
First of all, I would like to thank Mizan Tepi University Teaching Hospital, Tepi General Hospital, and Gebretsadik Shawo Hospital and staff for their support and cooperation. Next, I extend my gratitude to study participants, data collectors, and supervisors.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Catherine AB, Schechter J, Berzon B, Windle ML. Cardiopulmonary resuscitation (CPR). Practical essentials [homepage on the Internet]. [
2. Cass A, Bartz A. Why it remains difficult for remote cardiologist to obtain the locus of control for ambulatory health care conditions such as congestive heart failure? A tug of war between general practice, administrators and implementable research findings. J General Pract. 2014;02. doi: 10.4172/2329-9126.1000146
3. American Heart Association. The American Heart Association guidelines for cardiopulmonary resuscitation. Emerg Cardiovasc Care Elvister. 2020;4:1–5.
4. Raghava S, Nazir R. Adult Basic Life Support (BLS) awareness and knowledge among medical and dental interns completing internship from Deemed University. Resuscitation. 2006;70:416–422.
5. Simmes FM, Schoonhoven L, Mintjes J, Fikkers BG, Van der Hoeven JG. Incidence of cardiac arrests and unexpected deaths in surgical; patients before and after implementation of a rapid response system. Ann Intensive Care. 2012;2(1):141–147. doi:10.1186/2110-5820-2-20
6. Hamilton R. Nurses Knowledge and skills following cardio-pulmonary resuscitation training: a review of the literature. J Adv Nurs. 2005;51(3):
7. Cooper S, Johnston E, Priscott D. Immediate life support training. Impact in a primary care setting? Resuscitation. 2007;72:92–99. doi:10.1016/j.resuscitation.2006.06.004
8. Oh S-I II, Han -S-S. A study on the sustainable effect of reeducation on CPR on nurses’ knowledge and skill. J Korean Acad Nurs. 2008;38(3):383–392. doi:10.4040/jkan.2008.38.3.383
9. Rea Thomas D, Carol F, Linda C, Donohoe Racheal T, Cindy H, Jennifer I. CPR with chest compression alone or with rescue breathing. Engl J Med. 2010;36(5):423–433.
10. Ratha K, Panda S, Pradhan R. “Evaluate the effectiveness of planned teaching program regarding basic life support(BLS) among intern (BSc nursing) student at selected nursing college”, Bhubaneswar, Odisha. Nurse Health Sci. 2014;3(1):16–19.
11. Dariush M, Benjamin Emelia J, Go Alan S, Arnett Donna K, Blaha Michael J. Heart diseases and stroke statistics-2015 update a report from the American heart association. Circulation. 2015;131(4):e329–e329.
12. Weisfeldt ML. Public access defibrillation: good or great? BMJ. 2004;328:E271–272. doi:10.1136/bmj.328.7438.E271
13. Wenzel V, Lehmkuhl P, Kubilis PS, Idris AH, Pichlmayr I. Poor correlation of mouth-to-mouth ventilation skills after BLS training and 6 Month later. Resuscitation. 1999;35:129–134. doi:10.1016/S0300-9572(97)00044-0
14. Zaheer H, Haque Z. Awareness about BLS (CPR) among medical students: status and requirements. J Pak Med Assoc. 2009;59(1):57–59.
15. Gombotz H, Weh B, Mitterndorfer W, et al. In-hospital cardiac resuscitation outside the ICU by nursing staff equipped with automated external defibrillators–the first 500 cases. Resuscitation. 2006;70(3):416–422. doi:10.1016/j.resuscitation.2006.02.006
16. Nagwa I, Abass N, Soliman M. Effect of implementing Advanced Cardiovascular Life Support (ACLS) Guidelines 2016 on nurse’s knowledge and performance. Am J Biomed Res. 2020;8:534–542.
17. American Heart Association. Cardiopulmonary resuscitation: statement by the Ad Hoc Committee on cardiopulmonary resuscitation of the division of medical science, national academy of sciences, national research council. JAMA. 1966;198:372–379. doi:10.1001/jama.1966.03110170084023
18. Marsha Assefa D, Tilahun S. Assessment of Knowledge, Attitude and Practice towards CPR among Nurses Working in Wolaita Sodo University Teaching Hospital Wolaita Sodo, Southern Ethiopia. Int J Biotech Trends Technol. 2017;4:54.
19. AL-Kandary S, AL-Jeheidli A, Ghayath T, et al. Perceived competence in cardiopulmonary resuscitation, knowledge and practice among qualified nurses in Kuwait. Alexandria Bulletin. 2007;43(2):294–295.
20. Marzooq H, Lyneham J. Cardiopulmonary resuscitation knowledge among nurses working in Bahrain. Int J Nurs Pract. 2009;15(4):294–302. doi:10.1111/j.1440-172X.2009.01752.x
21. Ihunanya OM, Oke Michael RN, Babcock BN. Knowledge, attitude, and practice of cardiopulmonary resuscitation among nurses in Babcock university teaching hospital in Ilishan-Remo, Ogun State, Nigeria. Int J Caring Sci. 2020;13:1773–1782.
22. Mengistu Mekonnen K. Knowledge, practice and associated factors towards basic life support among nurses working in Amhara region referral hospitals, northwest Ethiopia; 2016.
23. Tanigawa K, Iwami T, Nishiyama C, et al. Are trained individuals more likely to perform bystander CPR? An observational study. Resuscitation. 2011;82(5):523–528. doi:10.1016/j.resuscitation.2011.01.027
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.