Back to Journals » Psychology Research and Behavior Management » Volume 15
Facing a Real Threat of Death: Dynamic Changes in Death-Thought Accessibility
Authors Zhou J, Chen Y, Xu Y ![]() , Liao B, Fu W
, Liao B, Fu W
Received 22 February 2022
Accepted for publication 20 June 2022
Published 14 July 2022 Volume 2022:15 Pages 1731—1740
DOI https://doi.org/10.2147/PRBM.S361432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jia Zhou,1,* Yi Chen,1,* Yi Xu,2,* Bin Liao,3 Wenguang Fu4
1School of Humanities and Management Science, Southwest Medical University, Luzhou, SiChuan, 646000, People’s Republic of China; 2Department of Psychiatry, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 3Department of Cardiovascular Surgery, Affiliated Hospital of Southwest Medical University, Luzhou, SiChuan, 646000, People’s Republic of China; 4Department of Hepatobiliary Surgery, Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenguang Fu, Department of Hepatobiliary Surgery, Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China, Tel +86-13982770568, Email [email protected] Bin Liao, Department of Cardiovascular Surgery, Affiliated Hospital of Southwest Medical University, Luzhou, SiChuan, 646000, People’s Republic of China, Tel +86-0830-3162306, Email [email protected]
Purpose: This study explored the relationship between emotion and death-thought accessibility (DTA) in individuals experiencing true mortality salience (MS), specifically, patients with cancer.
Patients and Methods: The study included 255 participants; among them, 132 patients had cancer and represented the MS group, and 123 had dental pain and served as a control group. Participants completed the Projective Diseases Attitude Assessment Questionnaire to induce priming, completed an affect scale, completed one of four calculation tasks as manipulation of cognitive load (all four were done over several sessions), and performed a Pinyin-Chinese characters exercise to measure DTA.
Results: MS was associated with strong negative emotional arousal. When these negative emotions are generated, they enter an individual’s consciousness and activate proximal defense mechanisms. At this point, DTA can be measured. Patients with cancer had significantly higher levels of DTA in the high-frequency cognitive load condition than in the other three conditions (no task, simple delay task, and single cognitive load task). Patients with dental pain had significantly higher levels of DTA in the no task and simple delay conditions than in the single cognitive load or high-frequency cognitive load conditions. This study also found that negative experiences without MS (specifically, dental pain) are associated with higher levels of DTA.
Conclusion: These findings suggest that in addition to death-related events, both negative and stress-inducing events can produce DTA.
Keywords: mortality salience, cancer, terror management theory, proximal defense mechanisms
Introduction
Terror management theory (TMT) posits that proximal defense mechanisms help people to eliminate the idea of death from their conscious awareness, and distal defense mechanisms help people to eliminate the idea of death from their unconscious mind.1 Without these two defense mechanisms, people may fall into a spiral of fear and anxiety caused by thoughts of death. Death-thought accessibility (DTA) refers to the availability of cognitions related to death in one’s mind; measurement of DTA indicates the effectiveness of this dual-process defense mechanism.2 This measurement provides new insights into human social behavior and helps to accurately reflect the cognitive processing of death consciousness management. DTA can also help to distinguish between the processing mechanisms of proximal (ie conscious) and distal (ie unconscious) defense mechanisms in the process of death fear management.3 According to a literature review by Burke et al,4 the relationship between proximal and distal defense mechanisms is linear; that is, the distal defense does not start until the proximal defense ends. Therefore, in proximal defense, negative emotions, such as fear and anxiety, occur. These negative emotions need to be addressed by proximal defense mechanisms.5 At this stage, DTA is low, while at the distal defense level, when negative emotions, such as fear and anxiety, disappear, DTA increases.4,6,7
Several studies have tested this theory using mortality salience (MS) conditions, in which people are made conscious of death, and proximal defenses, such as denial and avoidance, are generated.8–10 These kinds of experiments require participants to imagine a scenario that triggers MS; however, as participants do not experience true MS, there are debates regarding the classical hypothesis of TMT. The psychological defense mechanisms triggered by MS serve to eliminate fear, anxiety, and other negative emotions. However, in practical research, emotion does not play the role of presupposition, and no significant emotional response is detected after death is highlighted.11–13 According to TMT, the psychological defense mechanisms caused by MS mainly serve to eliminate the fear or anxiety that accompanies consciousness of death. However, no studies have measured a significant emotional response in this regard. As a result, Lambert et al14 proposed the “affect-free claim.” For example, a physiological arousal study of 115 participants found that both the death reminder and the control groups (in this instance, a group that was reminded of a toothache) experienced physiological arousal. Bayesian factor analysis of nine physiological indexes including heart rate, mean arterial pressure, and respiratory rate showed no significant differences between the two groups.15 Furthermore, some studies have shown that the emotions triggered by death reminders are more positive than those triggered by non-death reminders16 and that the understanding of death can also promote internal growth.17
The typical emotion measure used in TMT research is the Positive and Negative Affect Schedule (PANAS), which is usually completed immediately after the death reminder.18 However, some researchers believe that this tool may not be adequately sensitive, and as a result, fails to measure emotion in some individuals. In later studies, to clarify participants’ emotional states in a more detailed manner, researchers both directly and indirectly integrated emotion measures into their study designs (eg self-report or implicit measures, false attribution paradigm, and emotional control strategies). However, even with these additional measures, the results still did not indicate that participants experienced stable and significant emotions.14,19 These results support the aforementioned affect-free claim and challenge TMT. In response to this dispute, Greenberg et al20 proposed that the initiation of death thinking due to MS does not arouse anxiety and fear consciously, but instead causes implicit emotion. The view proposed by Greenberg was supported by studies by Lu et al,21 Quirin et al,22 Wang and Liu,23 Simpson et al,24 Packard and McGaugh,25 Schwartz et al,26 and Seligman and Hager.27 The results of functional magnetic resonance imaging technology strongly support this idea, showing that MS produces an unconscious and imperceptible emotion related to fear and anxiety.
While some studies suggest that MS is followed by emotion, others suggest that it is not. This contradiction has been prevalent during the COVID-19 pandemic; that is, different countries have adopted different countermeasures to adapt to increased MS in their population. Several countries have experienced various levels of MS among their populations, leading to different levels of emotional arousal,28–30 defense mechanisms, and coping styles in each country. For example, China has considered COVID-19 a significant threat to life and has thus adopted a strict proximal defense. By contrast, some countries did not adopt strict defensive measures at the beginning of the pandemic. These countries did not believe that the disease would cause high mortality and were unwilling to adopt various defensive measures; specifically, people thought that COVID-19 would not threaten their lives. Other countries have fluctuated between strict and relaxed defense mechanisms. When the number of infected individuals increased, anxiety and fear rose, and strict defense mechanisms were adopted. When the number of infected individuals decreased, death thoughts reduced, and the defense mechanisms were gradually relaxed. This phenomenon can be understood through TMT, which shows that different degrees of MS result in different emotional states and drive people to produce corresponding behaviors.31,32
An observation of the current pandemic shows that the existence of emotion depends on the degree of MS. If the level of MS is low, there will be no explicit emotional response. On the contrary, there will be obvious explicit emotion and a strict proximal defense mechanism if the level of MS is high. Therefore, in this study, we not only tested our hypothesis and clarified a debated component of TMT but also sought to explain current social phenomenon. In this study, we examined a group of individuals who were experiencing real MS: patients with cancer, that is, patients with high levels of MS; and individuals experiencing a toothache that is not life-threatening, that is, patients with low levels of MS. We expected to detect differences in mood under the conditions of the current study. Further, we hypothesized that fear and anxiety do occur after MS, as posited in TMT (for a review, see Pyszczynski,1 Greenberg et al,33 and Grossman34).
Materials and Methods
Participants
The study sample included two groups: a cancer group and a dental pain control group. Patients with cancer were recruited from the Department of Oncology at Southwest Medical University. Eligible participants were those who had been clinically diagnosed with any type of cancer and were aware of their disease status. The following exclusion criteria were applied: (a) experiencing recurrence or metastasis, (b) being < 18 or > 70 years old, and (c) having lost the ability to walk. The dental pain group participants were recruited from the Southwest Medical University Affiliated Stomatological Hospital. The following exclusion criteria were applied for the control group: (a) having cancer or other serious diseases and (b) being < 18 or > 70 years old. We selected 255 eligible adult participants (age range = 18–69 years, Mage = 39.70, SDage = 12.95; 64.1% women, 35.9% men). The experimental group consisted of 132 patients with cancer (Mage = 43.42, SDage = 12.68, range: 18–69 years; 59.0% female, 41.0% male). The control group included 123 patients with dental pain (Mage = 35.65, SDage = 12.54, range: 18–64 years; 69.6% women, 30.4% men). The two groups did not differ significantly in age, educational background, or socioeconomic status.
Procedure
The experiment utilized a 2×4 between-group experimental design. Upon arrival, the experimenter described the study as an observation of personality characteristics to the participants and explained the reason for using the affect scale, calculation task (ie delay or cognitive load task), and the Pinyin-Chinese characters exercise (ie DTA measure). Participants were divided into two groups: patients with cancer and patients with dental pain. First, both groups needed to perform MS tasks. Second, all participants had to complete an emotion measure and one of the four different tasks before their DTA was measured: (a) no task, (b) simple delay task, (c) single cognitive load task, and (d) high-frequency cognitive load task. These four tasks represent different levels of delayed tasks. In this study, the emotion test is not a part of the delayed task. Emotional tasks were executed immediately after the MS tasks, and delayed tasks were executed immediately after the emotional tasks. Participants were randomly assigned to one of the four tasks in each session. Finally, all participants completed the DTA test and were tested in sessions comprising 4–6 patients each. Participants were notified that because they would not require the full hour to complete the personality questionnaires, they would be undertaking some additional measures that were being pretested for upcoming studies. The participants were required to respond to the questionnaires based on their initial natural responses and were assured that their answers would be anonymous. They were then provided a consent form to read and sign, followed by a questionnaire packet and a blank envelope. Participants were required to put the completed questionnaire into the envelope and then place the envelope in a box to indicate that the task had been completed. All participants completed the tasks at individual workstations to ensure their privacy.
Materials and Measures
Salience Manipulation Task
The Projective Diseases Attitude Assessment Questionnaire was used to induce the prime, using two open-ended questions under the guise of an innovative measure of personality. The open-ended instructions for the MS condition35,36 were: (a) please briefly describe the emotions that the thought of your disease arouses in you and (b) please briefly describe what happened to your body after your illness. Salience manipulation was performed in both cancer and dental pain groups. After the salience task was completed, the emotion measurement task was performed.
Emotion Measurement Task
Previous research indicates that MS sometimes increases DTA after a delay. Therefore, the thought of death can be prevented before it occurs.37 Thus, after the MS manipulation, participants were presented with PANAS as a distraction task before DTA was measured.20 In this study, PANAS is not only a part of the delayed tasks but also measures participants’ emotions. All participants in cancer and dental pain groups were tested using PANAS. PANAS18 consists of 20 items, including 11 adjectives describing negative emotions and 9 adjectives describing positive emotions. Participants were asked to rate the degree to which they experienced these emotions after the MS manipulation. Each item was rated on a 5-point rating scale, ranging from 1 (not at all) to 5 (very strong).
Simple Delay Task
Previous research suggests that MS induction increases DTA after a delay; this allows death thoughts to drift outside focal attention.37 Therefore, after the MS task, participants were asked to quickly complete five two-digit addition problems (eg 24 + 33 = ?).
Difficult Delay Task-Cognitive Load Task
Arndt et al38 suggested that if MS does indeed prompt the suppression of death thoughts, denying people the cognitive resources required for suppression should lead to an immediate increase in DTA. When MS manipulation was coupled with cognitive load manipulation, effectively occupying controlled processing resources and thereby hindering suppression, DTA was high immediately after MS manipulation. There were two cognitive load manipulations: a single cognitive load task and a high-frequency cognitive load task. After the salience manipulation, participants were presented with a single cognitive load task (eg 21×12 – 13×11 = ?), effectively using up controlled processing resources, thereby hindering suppression.
The difference between the high-frequency and single cognitive load tasks was that the high-frequency cognitive load task was conducted before each Pinyin task. Participants were required to complete a set of tasks in 30 seconds (eg 21×12 – 13×11 = ?). At the end of 30 seconds, regardless of whether the cognitive load task was completed, one Pinyin word-filling task was immediately presented. There were 26 word-filling tasks in the Pinyin version of the DTA measure, and thus, 26 cognitive load tasks.
DTA Measure
We utilized a Pinyin version of the DTA measure in this study.39 In this instrument, if the Pinyin sound is not marked with a tone, different tones could produce different Chinese characters and meanings. The given Pinyin sounds could spell both death-related and neutral words, and the frequencies of these words were equalized in a pilot study. All participants completed 26 tasks of writing Chinese characters using Pinyin. These 26 Pinyin sounds had no tone, and participants could write down the first Chinese character that they thought of. The 26 tasks were divided into two parts. One part included 13 Pinyin sounds, which could spell Chinese characters related to death depending on the tone (see Table 1). These 13 Pinyin sounds were as follows: si (the third tone of this can spell “死”, which means death; the fourth tone can spell “四”, which means four), sha (the first tone of this can spell “杀”, which means kill; the first tone also can spell “沙”, which means sand), mai (the second tone of this can spell “埋”, which means bury; the third tone can spell “买”, which means buy), mu (the fourth tone of this can spell “墓”, which means grave; the fourth tone can also spell “木”, which means wood), wang (the second tone of this can spell “亡”, which means death; the second tone can also spell “王”, which means king), zang (the fourth tone of this can spell “葬”, which means funeral; the first tone can spell “脏”, which means dirty), shi (the first tone of this can spell “尸”, which means corpse; the fourth tone can spell “是”, which means yes), fen (the second tone of this can spell “坟”, which means tomb; the first tone can spell “分”, which means divide), sang (the fourth of this can spell “丧”, which means mourning; the first tone can spell “桑”, which means mulberry), beng (the first tone of this can spell “崩”, which means pass away; the fourth can spell “蹦”, which means jump), ai (the first tone of this can spell “哀”, which means sorrow; the fourth can spell “爱”, which means love), cu (the fourth tone of this can spell “猝”, which means die suddenly; the fourth tone also can spell “醋”, which means vinegar), ku (the first tone of this can spell “骷”, which means skull; the fourth tone can spell “酷”, which means cool). The next 13 Pinyin sounds could not spell out characters related to death.
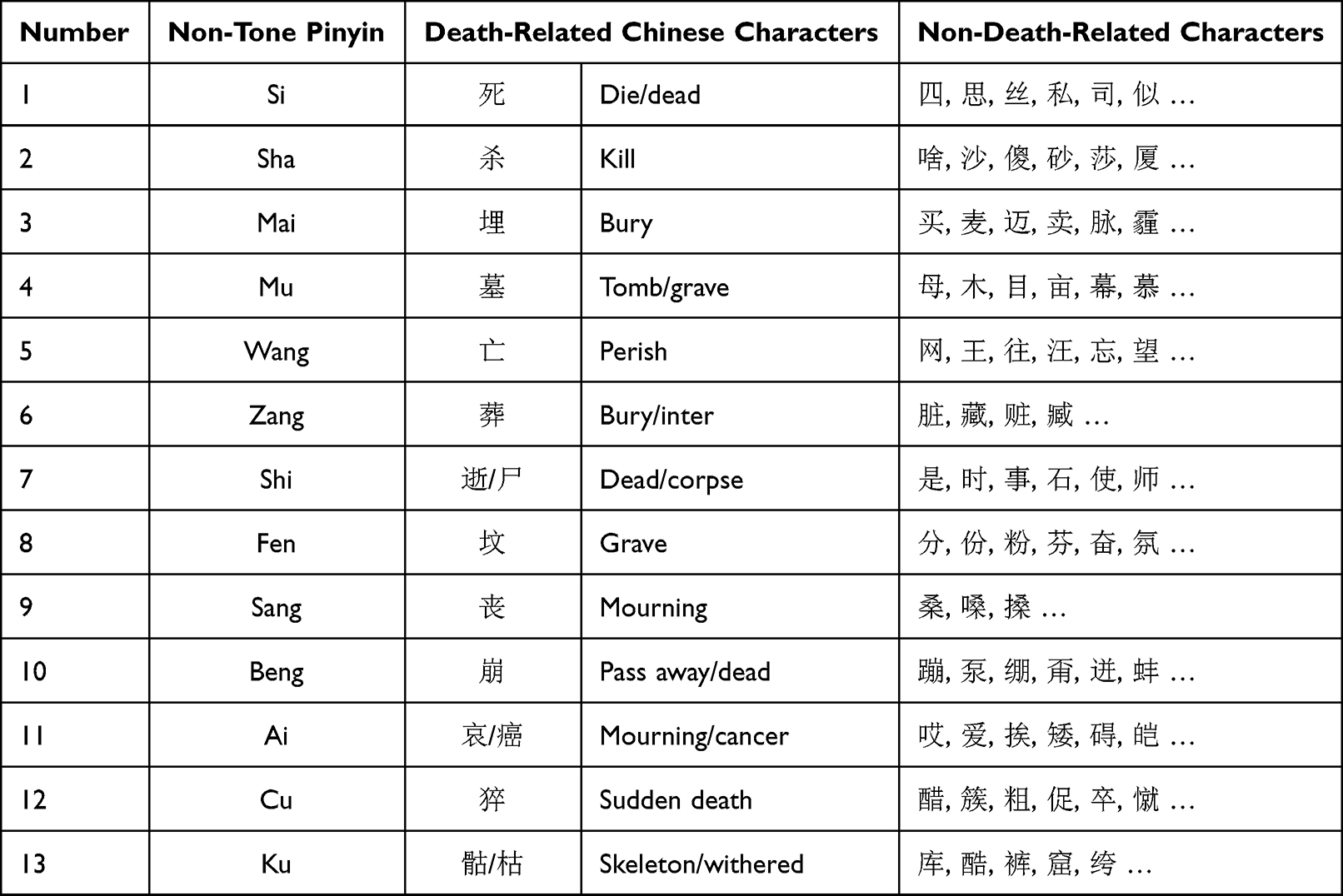 |
Table 1 Pinyin-Chinese Version of the DTA Measurement Tool |
Results
In the analysis of the experimental data, age was used as a covariate for statistical control. The covariate effect of age was: F(1, 246) = 0.830, p = 0.053, η2 = 0.015. To assess whether the conditions differed in self-reported affect following the MS manipulation, we performed a one-way analysis of variance for the negative and positive mood subscales; the results were significant. F(1, 253) = 263.81, p < 0.001, η2 = 0.51: the negative emotion score of patients with cancer (M = 34.06) was significantly higher than that of patients with dental pain (M = 19.72). F(1, 253) = 224.34, p < 0.001, η2 = 0.47: the positive emotion score of patients with dental pain (M = 31.85) was significantly higher than that of patients with cancer (M = 19.89). The results support our hypothesis. Further, we measured very significant emotional experiences using the seemingly insensitive PANAS. The descriptive statistics for the results are presented in Table 2.
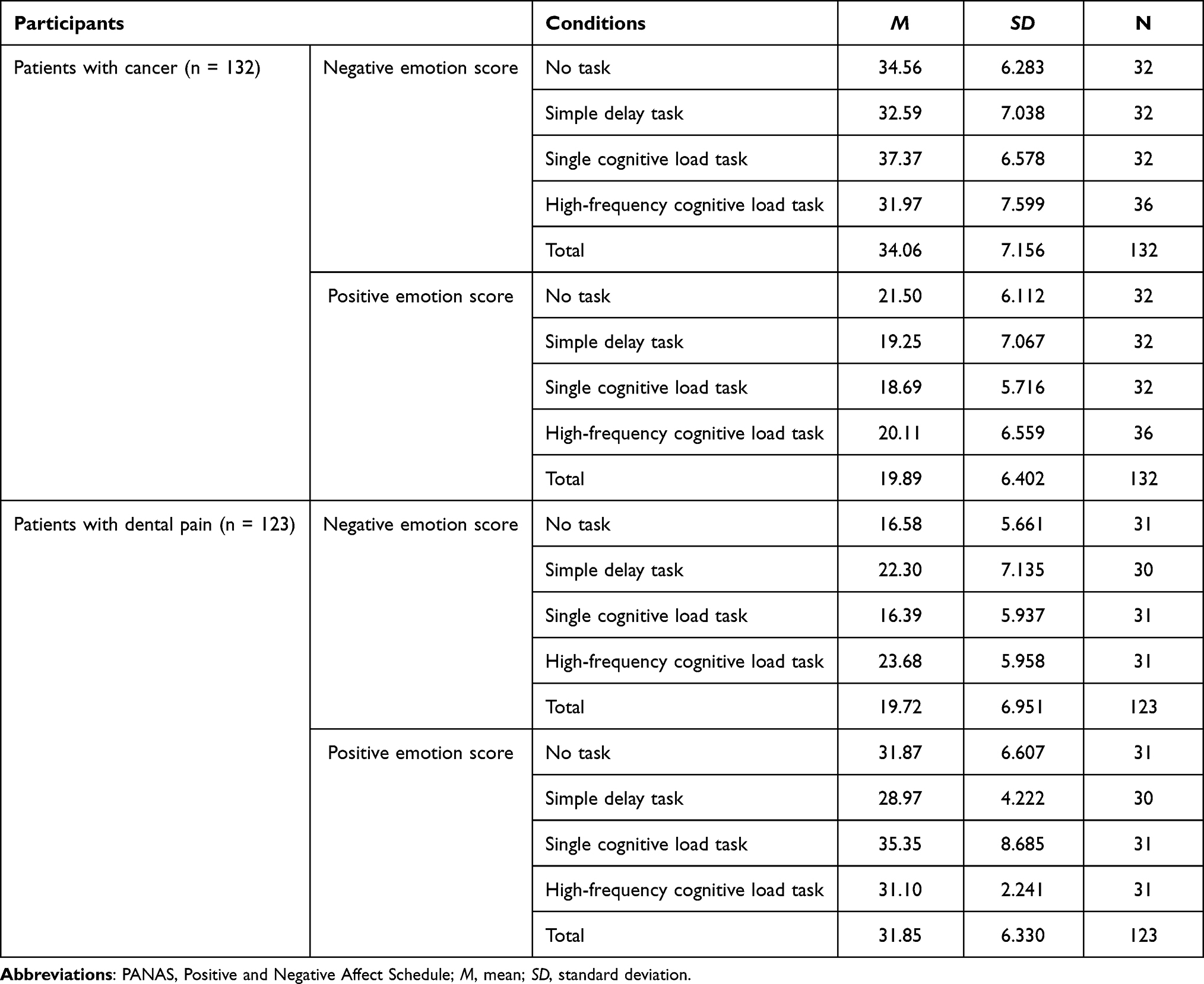 |
Table 2 Descriptive Statistics for the PANAS Data |
We examined DTA by performing a multivariate analysis of covariance. SPSS version 21 was used for statistical analyses. The analysis revealed a significant effect for manipulation: F(3, 246) = 23.85, p < 0.001, η2 = 0.225. Subsequently, we examined the simple effects of the independent variables using a Bonferroni correction. The results indicated that patients with cancer had significantly higher levels of DTA in the high-frequency cognitive load condition (M = 2.06, SD = 1.04) than in the other three conditions: the no task condition (M = 0.78, SD = 1.01), p < 0.001, 95% CI [0.72, 1.93], the delayed task condition (M = 0.47, SD = 0.80), p < 0.001, 95% CI [1.03, 2.24], and the single cognitive load task condition (M = 0.72, SD = 0.81), p < 0.001, 95% CI [0.81, 2.04]. However, there was no significant difference in pairwise comparisons between the no task, delay task, and single cognitive load task conditions. Patients with dental pain had significantly higher levels of DTA in the no task condition (M = 1.77, SD = 1.06) than in the single cognitive load task condition (M = 0.84, SD = 0.64), p < 0.001, 95% CI [0.29, 1.54], or the high-frequency cognitive load condition (M = 0.77, SD = 0.72), p < 0.001, 95% CI [0.36, 1.62]. In the delay condition (M = 1.60, SD = 1.25), DTA levels were significantly higher than in the single cognitive load task condition (M = 0.84, SD = 0.64), p < 0.01, 95% CI [0.13, 1.39], and the high-frequency cognitive load condition (M = 0.77, SD = 0.72), p < 0.01, 95% CI [0.20, 1.47]. However, there was no significant difference in the pairwise comparison between the no task and delay task conditions, or between the single cognitive load task and the high-frequency cognitive load task conditions. The within-participant results revealed that different tasks could affect the level of DTA.
The between-participant results indicated that patients with cancer had significantly lower DTA levels than those with dental pain in the no task condition (Mcancer = 0.78, SDcancer = 1.01; Mdental = 1.77, SDdental = 1.06), p < 0.001, 95% CI [0.47, 1.40], delayed task condition (Mcancer = 0.47, SDcancer = 0.80; Mdental = 1.60, SDdental = 1.25), p < 0.001, 95% CI [0.62, 1.55]. Meanwhile, in the high-frequency cognitive load condition, patients with cancer had significantly lower DTA levels than those with dental pain (Mcancer = 2.06, SDcancer = 1.04; Mdental = 0.77, SDdental = 0.72), p < 0.001, 95% CI [0.92, 1.85]. However, there was no significant difference in the pairwise comparison between patients with cancer and dental pain in the single cognitive load task condition (Mcancer = 0.72, SDcancer = 0.81; Mdental = 0.84, SDdental = 0.64). The descriptive statistics for the results are presented in Table 3.
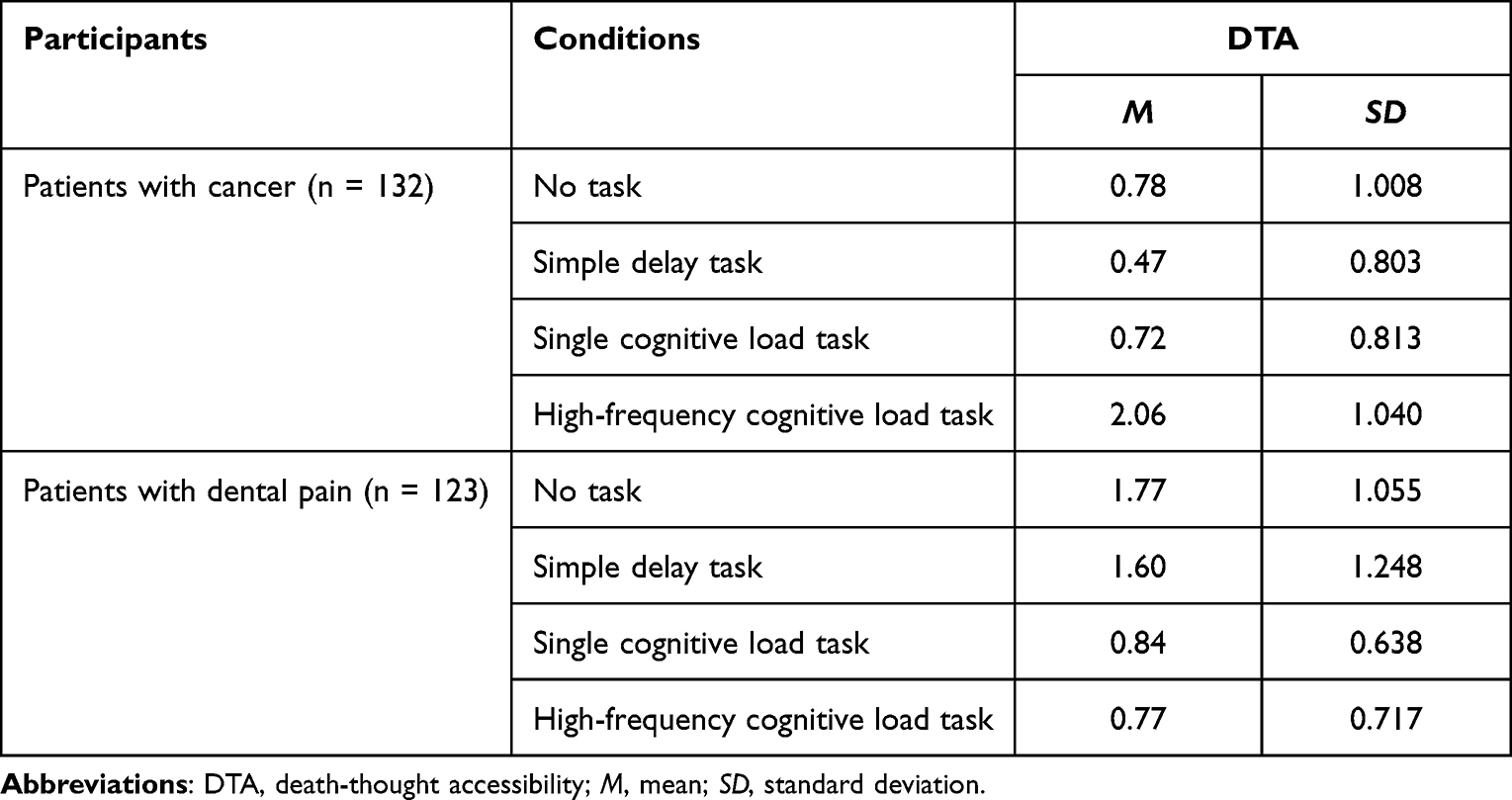 |
Table 3 Descriptive Statistics for the DTA Values Under Four Conditions |
Discussion
In this study, we aimed to investigate changes in emotion and DTA in people experiencing real disease conditions. Our findings imply that simple delayed and single cognitive load tasks had no effect on cancer and could not trigger death thoughts out of consciousness. The level of authenticity of MS conditions determines whether implicit and/or explicit emotions are triggered in an individual. Therefore, the assumption that MS does not trigger emotions or that MS only triggers implicit emotions is biased.
For patients with cancer, death thoughts remain part of their conscious thoughts or can easily enter their conscious thoughts, which leads to ultra-low DTA levels. Because the thought of death always remains at the level of consciousness, the proximal defense mechanism of patients with cancer is very strong. In particular, avoidance and denial defense mechanisms were so active that patients with cancer tended to avoid filling in death-related words when completing the Pinyin DTA test. Further, their DTA levels only increased when they performed high-frequency cognitive load tasks. Arndt et al’s35 study pointed out that having participants imagine that they were suffering from cancer had a more significant effect on MS than having them imagine their death; that is, it elicited a more active proximal defense mechanism. Therefore, the value of DTA was very low under the conditions of no delay task, simple delay task, and single cognitive load task in individuals experiencing cancer-related MS, but the DTA value increased under the condition of cognitive load task, as seen in this study. This phenomenon further shows that patients with cancer have a high degree of MS. High levels of MS produce a strong emotional response, leading to high-intensity proximal defense. In Arndt et al’s35 study, the DTA levels of participants increased after a cognitive load task. By contrast, when measuring the DTA levels of patients with cancer, a high-frequency cognitive load task is needed to suppress the proximal defense mechanism. A single cognitive load task cannot occupy the cognitive resources of patients with cancer.
Meanwhile, in the control group, there was no significant difference in DTA levels between the no delay and delayed task condition groups; however, the DTA levels of both groups were significantly higher than those in the cancer group. We propose two explanations for this result. One explanation is that dental pain produced negative physical and emotional reactions, which led to an increase in the level of unconscious DTA. However, these negative emotions are not directly caused by the threat of death because there are no thoughts of death in the consciousness of patients with dental pain. Another explanation is that the negative experiences and emotions of patients with dental pain were not inhibited by the delayed task in this experiment. The results showed that the level of DTA in patients with dental pain decreased significantly after the cognitive load task. We believe that the cognitive load task inhibited the consciousness of patients with dental pain to their body’s negative reaction, reduced their levels of anxiety and fear, and further reduced the level of DTA at the unconscious level.
Overall, the findings suggest that true MS awakens negative emotions. More importantly, MS may have a degree of problem, which is a continuous variable that can become larger or smaller. The higher the degree of truth, the greater the negative emotion at the level of consciousness. When negative emotions are generated, they will produce a corresponding intensity of proximal defense mechanism. The higher the strength of the proximal defense mechanism, the harder it is to measure the value of DTA. The high-intensity proximal defense mechanism needs a high-intensity cognitive load to inhibit it. For patients with cancer, the occupation of cognitive resources to inhibit the role of proximal defense mechanisms is needed to increase DTA.
The findings also suggest that tasks that do not trigger MS but bring negative experiences (eg a toothache) can also enhance DTA. Based on this finding, we believe that both negative and stressful events can also produce DTA, not just death-related events; however, in this case, the level of explicit emotion is relatively low and often is not delectable In this study, dental pain did not cause measurable conscious negative emotions, so there was no activation of the proximal defense mechanism. Therefore, when there was no delayed task, a certain amount of DTA could still be measured directly. High-frequency cognitive load tasks led to a decrease in DTA levels in patients with toothaches, indicating that negative emotions were also suppressed. In conclusion, these results suggest that disease-related death reminders can produce responses similar to true MS.40,41
Conclusions
This study shows that the threat of real death does produce obvious emotional responses, and emotion may be an important factor in determining defensive behaviors after MS events. Additionally, the level of authenticity of a death threat appears to determine the level of emotion.
There are several limitations to the study. First, this study did not explore the relationship between true MS and emotional attribution, that is, whether patients with cancer can reduce their emotional responses and defense mechanisms after good cognitive attribution of cancer. If the emotion is reasonably and effectively attributed, the defensive behavior is not obvious.19 Second, as pointed out in a study by Hayes and Schimel,42 when using measures of DTA, assessing whether an idea is activated will inevitably affect the activation of the idea. For this reason, research that involves measuring the idea of death unconsciously is particularly difficult.
Abbreviations
DTA, death-thought accessibility; MS, mortality salience; TMT, terror management theory; PANAS, Positive and Negative Affect Schedule.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Southwest University and the Affiliated Hospital of Southwest Medical University (reference no. XNYD2017268). The study’s purpose, procedures, and benefits were explained to all participants. Participants were also informed of their right to confidentiality and withdrawal. Our study complies with the principles outlined in the Declaration of Helsinki. All the participants provided written informed consent in accordance to the human participants’ guidelines of the institutional ethics committee. Participants were offered a gift (one set of bowls valued at about 3 USD) and monetary rewards (about 16 USD) for their participation, after completing the experiments.
Acknowledgments
We thank the Postdoctoral Research Startup Foundation of Southwest Medical University (08/002300602) and the School-level Project of Southwest Medical University (08/00031508).
Funding
This research was supported by a fellowship from the China Postdoctoral Science Foundation (2020M683363), and the Humanity and Social Science Youth Foundation of the Ministry of Education (20YJC190032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pyszczynski T, Greenberg J, Solomon S. A dual-process model of defense against conscious and unconscious death-related thoughts: an extension of terror management theory. Psychol Rev. 1999;106(4):835–845. doi:10.1037/0033-295x.106.4.835
2. Pyszczynski T, Solomon S, Greenberg J. Chapter one—thirty years of terror management theory: from genesis to revelation. In: Olson JM, Zanna MP, editors. Advances in Experimental Social Psychology. Cambridge: Academic Press; 2015:1–70. doi:10.1016/bs.aesp.2015.03.001
3. Hayes J, Schimel J, Arndt J, Faucher EH. A theoretical and empirical review of the death-thought accessibility concept in terror management research. Psychol Bull. 2010;136(5):699–739. doi:10.1037/a0020524
4. Burke BL, Martens A, Faucher EH. Two decades of terror management theory: a meta-analysis of mortality salience research. Pers Soc Psychol Rev. 2010;14(2):155–195. doi:10.1177/1088868309352321
5. Kosloff S, Anderson G, Nottbohm A, Hoshiko B. Proximal and distal terror management defenses: a systematic review and analysis. In: Routledge C, Vess M, editors. Handbook of Terror Management Theory. Amsterdam: Elsevier; 2019:31–63. doi:10.1016/B978-0-12-811844-3.00002-0
6. Burke BL, Kosloff S, Landau MJ. Death goes to the polls: a meta-analysis of mortality salience effects on political attitudes. Pol Psychol. 2013;34(2):183–200. doi:10.1111/pops.12005
7. Yen CL, Cheng CP. Researcher effects on mortality salience research: a meta-analytic moderator analysis. Death Stud. 2013;37(7):636–652. doi:10.1080/07481187.2012.682290
8. Pyszczynski T, Greenberg J, Solomon S, Arndt J, Schimel J. Why do people need self-esteem? A theoretical and empirical review. Psychol Bull. 2004;130(3):435–468. doi:10.1037/0033-2909.130.3.435
9. Goldenberg JL, Arndt J. The implications of death for health: a terror management health model for behavioral health promotion. Psychol Rev. 2008;115(4):1032–1053. doi:10.1037/a0013326
10. Greenberg J, Vail K, Pyszczynski T. Three–terror management theory and research: how the desire for death transcendence drives our strivings for meaning and significance. Adv Motiv Sci. 2014;1:85–134. doi:10.1016/bs.adms.2014.08.003
11. Jonas E, Sullivan D, Greenberg J. Generosity, greed, norms, and death—differential effects of mortality salience on charitable behavior. J Econ Psychol. 2013;35(1):47–57. doi:10.1016/j.joep.2012.12.005
12. Wisman A, Heflick NA. Hopelessly mortal: the role of mortality salience, immortality and trait self-esteem in personal hope. Cogn Emot. 2016;30(5):868–889. doi:10.1080/02699931.2015.1031643
13. Zaleskiewicz T, Gasiorowska A, Kesebir P, Luszczynska A, Pyszczynski T. Money and the fear of death: the symbolic power of money as an existential anxiety buffer. J Econ Psychol. 2013;36(2):55–67. doi:10.1016/j.joep.2013.02.008
14. Lambert AJ, Eadeh FR, Peak SA, Scherer LD, Schott JP, Slochower JM. Toward a greater understanding of the emotional dynamics of the mortality salience manipulation: revisiting the “affect-free” claim of terror management research. J Pers Soc Psychol. 2014;106(5):655–678. doi:10.1037/a0036353
15. Klackl J, Jonas E. Effects of mortality salience on physiological arousal. Front Psychol. 2019;10:1893. doi:10.3389/fpsyg.2019.01893
16. DeWall CN, Baumeister RF. From terror to joy: automatic tuning to positive affective information following mortality salience. Psychol Sci. 2007;18(11):984–990. doi:10.1111/j.1467-9280.2007.02013.x
17. Wei QW, Zhou XM, Yu GL. 死亡心理: 外部防御还是内在成长? [The psychology of death: external defense or internal growth?]. Adv Psychol Sci. 2015;23(2):338–348. doi:10.3724/SP.J.1042.2015.00338
18. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the Panas scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037/0022-3514.54.6.1063
19. Webber D, Schimel J, Faucher EH, Hayes J, Zhang R, Martens A. Emotion as a necessary component of threat-induced death thought accessibility and defensive compensation. Motiv Emot. 2015;39(1):142–155. doi:10.1007/s11031-014-9426-1
20. Greenberg J, Martens A, Jonas E, Eisenstadt D, Pyszczynski T, Solomon S. Psychological defense in anticipation of anxiety: eliminating the potential for anxiety eliminates the effect of mortality salience on worldview defense. Psychol Sci. 2003;14:516–519. doi:10.1111/1467-9280.03454
21. Lu K, Shen K, Li H. 恐惧管理理论中情绪的作用. [The role of emotion in terror management theory]. Adv Psychol Sci. 2017;25(1):76–85. doi:10.3724/SP.J.1042.2017.00076
22. Quirin M, Loktyushin A, Arndt J, et al. Existential neuroscience: a functional magnetic resonance imaging investigation of neural responses to reminders of one’s mortality. Soc Cogn Affect Neurosci. 2012;7(2):193–198. doi:10.1093/scan/nsq106
23. Wang CY, Liu C. 杏仁核情绪功能偏侧化的成像研究述评. [Review of imaging research on amygdala lateralization of emotional function]. Adv Psychol Sci. 2007;15:313–318.
24. Simpson JR, Snyder AZ, Gusnard DA, Raichle ME. Emotion-induced changes in human medial prefrontal cortex: I. During cognitive task performance. Proc Natl Acad Sci U S A. 2001;98(2):683–687. doi:10.1073/pnas.98.2.683
25. Packard MG, McGaugh JL. Double dissociation of fornix and caudate nucleus lesions on acquisition of two water maze tasks: further evidence for multiple memory systems. Behav Neurosci. 1992;106(3):439–446. doi:10.1037/0735-7044.106.3.439
26. Schwartz JM, Stoessel PW, Baxter LR, Martin KM, Phelps ME. Systematic changes in cerebral glucose metabolic rate after successful behavior modification treatment of obsessive-compulsive disorder. Arch Gen Psychiatry. 1996;53(2):109–113. doi:10.1001/archpsyc.1996.01830020023004
27. Seligman ME, Hager JL. Biological Boundaries of Learning. New York: Appleton-Century-Crofts; 1972.
28. Arndt J, Goldenberg JL. Where health and death intersect: insights from a terror management health model. Curr Dir Psychol Sci. 2017;26(2):126–131. doi:10.1177/0963721416689563
29. Courtney EP, Goldenberg JL, Boyd P. The contagion of mortality: a terror management health model for pandemics. Br J Soc Psychol. 2020;59(3):607–617. doi:10.1111/bjso.12392
30. Fu L. 突发危机事件下的公众心理特征及干预疏导策略——基于新冠肺炎疫情的调查分析. [Public psychological characteristics and intervention strategies in emergencies: a survey during the COVID-19 epidemic]. Study Ideol Educ. 2020;27:60–65.
31. Greenberg J, Schimel J, Martens A, Solomon S, Pyszcznyski T. Sympathy for the devil: evidence that reminding whites of their mortality promotes more favorable reactions to white racists. Motiv Emot. 2001;25(2):113–133. doi:10.1023/A:1010613909207
32. Menzies RE, Menzies RG. Death anxiety in the time of COVID-19: theoretical explanations and clinical implications. Cogn Behav Therap. 2020;13:e19. doi:10.1017/S1754470X20000215
33. Greenberg J, Arndt J, Schimel J, Pyszczynski T, Solomon S. Clarifying the function of mortality salience-induced worldview defense: renewed suppression or reduced accessibility of death-related thoughts? J Exp Soc Psychol. 2001;37(1):70–76. doi:10.1006/jesp.2000.1434
34. Grossman CH, Brooker J, Michael N, Kissane D. Death anxiety interventions in patients with advanced cancer: a systematic review. Palliat Med. 2018;32(1):172–184. doi:10.1177/0269216317722123
35. Arndt J, Cook A, Goldenberg JL, Cox CR. Cancer and the threat of death: the cognitive dynamics of death-thought suppression and its impact on behavioral health intentions. J Pers Soc Psychol. 2007;92(1):12–29. doi:10.1037/0022-3514.92.1.12
36. Rosenblatt A, Greenberg J, Solomon S, Pyszczynski T, Lyon D. Evidence for terror management theory: i. The effects of mortality salience on reactions to those who violate or uphold cultural values. J Pers Soc Psychol. 1989;57(4):681–690. doi:10.1037/0022-3514.57.4.681
37. Greenberg J, Pyszczynski T, Solomon S, Simon L, Breus M. Role of consciousness and accessibility of death-related thoughts in mortality salience effects. J Pers Soc Psychol. 1994;67(4):627–637. doi:10.1037/0022-3514.67.4.627
38. Arndt J, Greenberg J, Cook A. Mortality salience and the spreading activation of worldview-relevant constructs: exploring the cognitive architecture of terror management. J Exp Psychol Gen. 2002;131(3):307–324. doi:10.1037/0096-3445.131.3.307
39. Zhou J. Research on death threat and defense mechanism of cancer patients [Unpublished doctoral dissertation]. Southwest University; 2019. Available from: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CDFD&dbname=CDFDLAST2020&filename=1019914784.nh&uniplatform=NZKPT&v=srZcTi0VK1bqtfBkQk9pG_uKerew5HQYLiprvt6TZinI4C_qOEXYqZ-SIVwF7Eu5.
40. Arrowood RB, Cox CR, Kersten M, Routledge C, Shelton JT, Hood RW. Ebola salience, death-thought accessibility, and worldview defense: a terror management theory perspective. Death Stud. 2017;41(9):585–591. doi:10.1080/07481187.2017.1322644
41. Cui YX, Zhou X, Zu C, et al. Benevolent creativity buffers anxiety aroused by mortality salience: terror management in COVID-19 pandemic. Front Psychol. 2020;11:601027. doi:10.3389/fpsyg.2020.601027
42. Hayes J, Schimel J. Unintended effects of measuring implicit processes: the case of death-thought accessibility in mortality salience studies. J Exp Soc Psychol. 2018;74:257–269. doi:10.1016/j.jesp.2017.10.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.