Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Facial Seborrheic Dermatitis in HIV-Seropositive Patients: Evaluation of the Efficacy and Safety of a Non-Steroidal Cream Containing Piroctone Olamine, Biosaccharide Gum-2 and Stearyl Glycyrrhetinate – A Case Series
Authors Cortés-Correa C, Piquero-Casals J ![]() , Chaparro-Reyes D, Garré Contreras A, Granger C
, Chaparro-Reyes D, Garré Contreras A, Granger C ![]() , Peñaranda-Contreras E
, Peñaranda-Contreras E
Received 16 October 2021
Accepted for publication 2 March 2022
Published 18 March 2022 Volume 2022:15 Pages 483—488
DOI https://doi.org/10.2147/CCID.S344807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Carolina Cortés-Correa,1 Jaime Piquero-Casals,2 Daniela Chaparro-Reyes,1 Aurora Garré Contreras,3 Corinne Granger,3 Elkin Peñaranda-Contreras1
1Department of Dermatology, Hospital Universitario de la Samaritana, Bogotá, Colombia; 2Department of Dermatology, Dermik, Multidisciplinary Dermatology Clinic, Barcelona, Spain; 3Innovation and Development, ISDIN, Barcelona, Spain
Correspondence: Jaime Piquero-Casals, Department of Dermatology, Dermik Multidisciplinar Dermatology Clinic, Barcelona, Spain, Tel +34 932279867, Fax +34 932275438, Email [email protected]
Abstract: Facial seborrheic dermatitis is common in HIV-positive patients, and the presence of facial lesions can affect quality of life. The management and control of lesions can be frustrating for both physicians and patients. In this pilot clinical study, we clinically evaluated the effectiveness of a topical non-steroidal cream in treating mild to moderate facial seborrheic dermatitis in 20 HIV-positive patients. The patients applied a twice-a-day topical cream containing zinc PCA, piroctone olamine, hydroxyphenyl propamidobenzoic acid, biosaccharide gum-2, and stearyl glycyrrhetinate for 12 weeks with no topical or oral antifungal or corticosteroid treatment. Signs and symptoms and tolerance were assessed before, during, and at the end of treatment. All of the patients showed clinical improvement after 4 and 12 weeks of treatment. None of the patients had no response to treatment, and no adverse effects were reported. No rescue therapy with corticosteroids was needed. The patients reported a very noticeable improvement in their skin which contributed to high compliance with the protocol requirement.
Keywords: facial seborrheic dermatitis, acquired immunodeficiency syndrome, AIDS, topical therapy, Malassezia, piroctone olamine, human immunodeficiency virus, HIV, microbiome
Introduction
Facial seborrheic dermatitis (FSD) clinically manifests with discrete, mild erythema and scaling in seborrheic areas such as above the eyebrows, the nasolabial fold, behind the ears and around the hairline.1 SD is more prevalent in immune-compromised patients such as HIV-seropositive patients, organ transplant recipients, and lymphoma patients. In HIV-positive patients an incidence of FSD of up to 80% is described.2 Patients with HIV may present more severe and extensive forms of seborrheic dermatitis (SD) as reported in a recent series of 20 African patients:3 exuberant erythema and desquamation were described with a typical distribution on the face and scalp but also with extension to other less common areas such as armpits, inguinal region and flexural surfaces, as well as marked and thicker yellowish scaling.3 It has also been reported that low CD4+ lymphocyte counts can influence severity of SD.2,4
The etiopathogenesis of this chronic inflammatory disease is complex. In addition to host immunity, other predisposing factors are overactivity of the sebaceous gland, neuroendocrine disorders, and epidermal barrier alteration. The different strains of Malassezia yeast and various alterations of the skin microbiome also play a fundamental role.5 Malassezia feeds on sebum on the skin surface, producing an aberrant epidermal differentiation, a barrier defect and inflammatory response. However, there are some controversies regarding sebaceous gland activity and SD. It is true that lesions occur in areas of the face with the presence of more sebaceous glands and that SD patients often have oily skin, however, there are SD patients who have normal sebum levels and there are also individuals with oily skin who do not develop SD. Malassezia is not the only factor to be considered, as various alterations of the skin microbiome have also been observed such as Staphylococcus epidermidis and aureus. Skin microbiota is extremely important for maintaining skin health and the dysbiosis of skin microbiota is important in the pathogenesis of SD.6
The presence of lesions on the face can affect quality of life and limit patients’ daily activities and interpersonal relationships. The management and control of lesions can be frustrating for both physicians and patients.
Current treatment options include topical treatment with low-potency steroids, calcineurin inhibitors, and several antifungals.7 The use of antifungal shampoos in conjunction with intermittent topical antifungal therapy, low-potency corticosteroids, and tacrolimus or pimecrolimus are part of routine clinical practice. General care with specific emollients and sun protection are fundamental pillars to distance and limit the use of topical medications and corticosteroids.8 In resistant and severe cases, oral ketoconazole can eventually be proposed.9
In SD patients without HIV, various publications have shown the usefulness of a non-steroidal, antifungal, anti-inflammatory and antiseborrheic cream marketed under the name Nutradeica (ISDIN, Spain).10–12 This combines several ingredients including piroctone olamine, which has antifungal properties;10,13 the zinc salt of l-pyrrolidone carboxylate (zinc PCA), which has antifungal and anti-inflammatory properties; biosaccharide gum-2, which has anti-inflammatory and antifungal properties; and stearyl glycyrrhetinate, which has anti-inflammatory, antioxidant, and skin-soothing properties.14 This topical treatment has previously been reported to accelerate recovery and prevent flare-ups.11,12
In HIV-seropositive patients, SD can be atypical and refractory to standard treatment, requiring prolonged courses of oral and topical antifungals as well as corticosteroids.15 Treatment failure and recurrence of lesions is common.15 There are no specific management guidelines in this population group; what is known is that SD is more resistant to treatment and tends to have more relapses. The control of CD4+ values with antiretrovirals could be of interest for the control of the disease.16 Previous investigators have suggested that these recalcitrant forms should be classified as a distinct entity.15
In this cases series, we clinically evaluated the effectiveness of this topical non-steroidal cream in treating mild to moderate FSD in 20 HIV-seropositive patients. The cream was applied twice a day for 12 weeks with no topical or oral antifungal or corticoid treatment.
Materials and Methods
This was an open, prospective case series with clinical evaluation. Twenty patients older than 18 years, with HIV on antiretroviral therapy, with a CD4 count > 200 and an undetectable viral load or < 200 copies/mL, who had mild or moderate FSD were recruited. No treatment with topical corticosteroids or calcineurin inhibitors for at least 12 weeks before the initiation visit was allowed.
All patients were treated with a twice-a-day topical non-steroidal cream containing zinc PCA, piroctone olamine, hydroxyphenyl propamidobenzoic acid, biosaccharide gum-2, and stearyl glycyrrhetinate for 12 weeks. The clinical evaluations were performed by the dermatologist before treatment (T0), after 4 weeks of treatment (T4) and after twelve weeks of treatment (T12). The patient global assessment (PGA) was performed at these same times.
Severity of signs and symptoms were assessed using the Investigator’s Global Assessment (IGA) score (5 item score: 0–no disease; 1–almost fully resolved; 2–mild disease; 3–moderate disease; 4–severe disease). An IGA score ≤1 was considered treatment success. The PGA was a 5-point scale: excellent response (>80% improvement); good response (50–80% improvement); mild response (<50% improvement); no response (no change); worsening.
This study was approved by the Research Ethics Committee of Hospital Universitario La Samaritana, Bogotá, Colombia. This study was conducted according to the guideline for Good Clinical Practice and the Declaration of Helsinki. All subjects gave written informed consent.
Results
Twenty patients were recruited: 3 women and 17 men, with ages ranging from 19 to 60 years old (mean age 38 years). Seven had a baseline IGA score of 2 (mild FSD) and 13 had a score of 3 (moderate FSD). The time since onset of FSD was between 3–16 years. Three out of the 20 patients had FSD before their HIV diagnosis.
All patients showed a decrease in the severity of desquamation, erythema (Figure 1) and itching (Figure 2) at 4 and 12 weeks. Fourteen patients had complete symptom resolution. None of the patients required rescue therapy with corticosteroids or antifungals. The improvement in skin quality produced high patient satisfaction. No adverse events were recorded.
 |
Figure 1 Improvement of desquamation and erythema symptoms evaluated by the dermatologist using IGA score. (+) Statistically significant (p <0.001). |
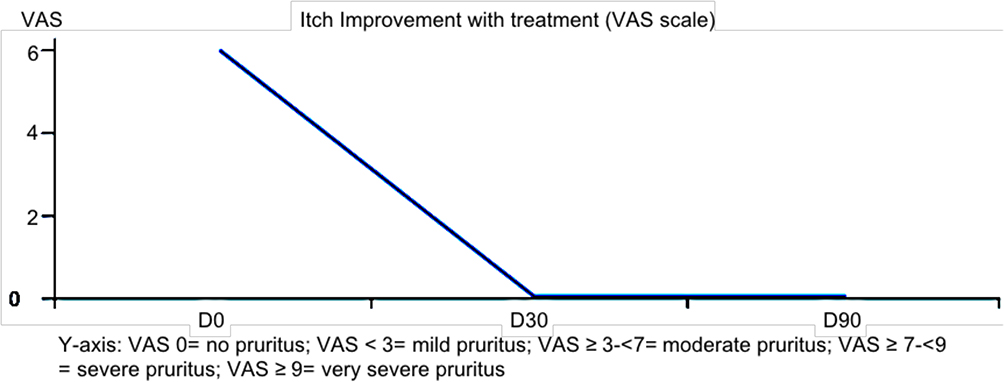 |
Figure 2 Improvement of itch evaluated by the patient using VAS scale (+) statistically significant (p <0.001). |
Discussion
This study reports the clinical outcomes in FSD in a population of HIV-positive patients treated with a non-steroidal cream containing zinc PCA, piroctone olamine, hydroxyphenyl propamidobenzoic acid, biosaccharide gum-2, and stearyl glycyrrhetinate for 12 weeks with no topical or oral antifungal or corticosteroid treatment. The clinical results were good, with 14 of 20 patients having complete resolution of symptoms.
Previous studies10–12 have assessed this topical treatment in populations without HIV, but this case series provides specific information on the HIV-positive population group, which can be resistant to treatment.
In the literature there is a lack of studies describing management of SD in HIV patients. In a single center study, De Moraes et al evaluated 21 HIV-infected patients with mild to severe SD treated with twice-daily pimecrolimus cream 1% for 5 weeks.17 This non-steroid calcineurin inhibitor has an excellent safety profile, low systemic absorption and does not induce skin atrophy; however after the discontinuation of treatment, erythema and scaling recurred in approximately 50% of patients around day 35. In our study, patients were not scheduled for follow-up after the 12-week treatment, however no patients returned in the next two months to report relapse. In another series of 20 cases with diffuse HIV-associated SD,3 most of the patients were refractory to standard SD treatments and required prolonged courses of topical and systemic antifungals plus topical or oral corticosteroids. In our study, even in the patients with long history of FSD, a noticeable improvement was observed and no other topical or systemic treatment was needed during the 3-month treatment.
Other studies have looked at the characteristics within HIV-positive populations with SD to determine those affecting disease severity and features. A prospective study with sixty HIV-positive patients, 30 with FSD and 30 without, determined the presence and amount of Malassezia spp yeasts.16 Patients with FSD had a CD4 count between 200 and 499 and a higher number of Malassezia spp yeasts. HIV-positive patients without FSD, on the other hand, had CD4 cell counts above 500 and a significantly lower number of Malassezia yeasts on smear and on culture. Therefore, although the role of Malassezia is not fully understood, the number of yeast colonies appears to have a relevant role in the development of FSD.16 In another study,15 the composition of Malassezia spp was analyzed in 96 patients with FSD, among them 48 were HIV-seropositive. Samples were collected from four anatomical sites: face, chest, back and scalp. More quantity and diversity of Malassezia species colonies was found in the HIV-positive group of patients. The most frequent Malassezia species were M. Sympodialis, M. Globosa and M. Furfur.15
While the relationship between CD4 count and incidence of SD has been questioned,2 an association between CD4 count and FSD severity has been reported.4 Our patients all had CD4 counts above 200 and with mild or moderate FSD at baseline. Future studies could focus on patients with more poorly controlled HIV/lower CD4 count and more severe FSD.
The key advantages of this topical treatment are that it 1) avoids systemic drug treatment and the associated potential side effects or drug interactions, something which is particularly pertinent in HIV-positive patients who are commonly polymedicated,18 2) allows avoidance of prolonged topical steroids, 3) contains multiple ingredients to work on the various factors that contribute to the development of FSD, fundamentally regulating inflammation, sebum production and the microbiome, and 4) being a single combined product with good cosmetic qualities it is straightforward and pleasant for patients to use, which is likely to maximize adherence.
This non-pharmacological topical treatment could be considered as part of the management of SD in HIV-positive patients, alone or in combination with the use of conventional rescue therapies such as topical drugs.
The study limitations include the number of subjects, the open design and the lack of long-term follow up for measuring potential recurrence of symptoms; however, the results are encouraging.
Conclusion
This cases series provides clinical data on the efficacy of this non-steroidal cream for SD in the population group of HIV-seropositive patients, who can be prone to more recalcitrant or difficult-to-treat SD. The treatment gave good clinical results and was well-tolerated, with good adherence to treatment, influenced by the efficacy and cosmetic qualities of the cream. Additional studies are being considered to evaluate the efficacy in a larger population and the long-term efficacy, as well as its place within the therapeutic options for these polymedicated patients.
Consent Statements
Patients gave written consent for publication of photographs. All the patients signed a written informed consent to participate in this study, in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank all the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Sponsorship for this paper was funded by ISDIN® (Barcelona, Spain).
Disclosure
Dr Carolina Cortés-Correa reports personal fees, non-financial support from ISDIN as a clinical investigator, during the conduct of the study. Dr Jaime Piquero-Casals reports fees from ISDIN during the conduct of the study and grants from ISDIN outside the submitted work. Dr Corinne Granger is an employee of and reports grants from ISDIN during the conduct of the study. Dr Aurora Garré Contreras is an employee of and reports personal fees from ISDIN outside the submitted work. Dr Elkin Peñaranda-Contreras is a speaker for ISDIN, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Mameri ACA, Carneiro S, Mameri LMA, Telles da Cunha JM, Ramos-E-Silva M. History of seborrheic dermatitis: conceptual and clinico-pathologic evolution. Skinmed. 2017;15(3):187–194.
2. Schaub NA, Drewe J, Sponagel L, et al. Is there a relationship between risk groups or initial CD4 T cell counts and prevalence of seborrheic dermatitis in HIV-infected patients? Dermatology. 1999;198:126–129. doi:10.1159/000018087
3. Forrestel AK, Kovarik CL, Mosam A, Gupta D, Maurer TA, Micheletti RG. Diffuse HIV-associated seborrheic dermatitis - a case series. Int J STD AIDS. 2016;27(14):1342–1345. doi:10.1177/0956462416641816
4. Schechtman RC, Midgley G, Hay RJ. HIV disease and Malassezia yeasts: a quantitative study of patients presenting with seborrheic dermatitis. Br J Dermatol. 1995;133:694–698. doi:10.1111/j.1365-2133.1995.tb02740.x
5. Adalsteinsson JA, Kaushik S, Muzumdar S, Guttman-Yassky E, Ungar J. An update on the microbiology, immunology and genetics of seborrheic dermatitis. Exp Dermatol. 2020;29(5):481–489. doi:10.1111/exd.14091
6. Chen P, He G, Qian J, Zhan Y, Xiao R. Potential role of the skin microbiota in inflammatory skin diseases. J Cosmet Dermatol. 2021;20(2):400–409. doi:10.1111/jocd.13538
7. Gupta A, Versteeg S. Topical treatment of facial seborrheic dermatitis: a systematic review. Am J Clin Dermatol. 2017;18(2):193–213. doi:10.1007/s40257-016-0232-2
8. Purnamawati S, Indrastuti N, Danarti R, Saefudin T. The role of moisturizers in addressing various kinds of dermatitis: a review. Clin Med Res. 2017;15(3–4):75–87. doi:10.3121/cmr.2017.1363
9. Gupta AK, Richardson M, Paquet M. Systematic review of oral treatments for seborrheic dermatitis. J Eur Acad Dermatol Venereol. 2014;28(1):16–26. doi:10.1111/jdv.12197
10. Dall’Oglio F, Lacarruba F, Luca M, Boscaglia S, Granger C, Micali G. Clinical and instrumental evaluation of a new topical non-corticosteroid antifungal/anti-inflammatory/antiseborrheic combination cream for the treatment of mild-to-moderate facial seborrheic dermatitis. Clin Cosmet Investig Dermatol. 2019;12:103–108. doi:10.2147/CCID.S186621
11. Balato A, Caiazzo G, Di Caprio R, Scala E, Fabbrocini G, Granger C. Exploring anti-fungal, anti-microbial and anti-inflammatory properties of a topical non-steroidal barrier cream in face and chest seborrheic dermatitis. Dermatol Ther. 2020;10(1):87–98. doi:10.1007/s13555-019-00339-w
12. Piquero-Casals J, La Rotta-higuera E, Francisco Mir-Bonafé J, Rozas-Muñoz E, Granger C. Non-steroidal topical therapy for facial seborrheic dermatitis. J Drugs Dermatol. 2020;19(6):658–660. doi:10.36849/JDD.2020.5121
13. Granger C, Goni F, Martinez G, Garre A. Ex-vivo determination of antifungal activity of a new prescription non-steroidal facial cream against Malassezia furfur in human skin explants. Skin J Cutan Med. 2017;1:137. doi:10.25251/skin.1.supp.136
14. Oyama K, Kawada-Matsuo M, Oogai Y, Hayashi T, Nakamura N, Komatsuzawa H. Antibacterial effects of glycyrrhetinic acid and its derivatives on Staphylococcus aureus. PLoS One. 2016;11(11):e0165831. doi:10.1371/journal.pone.0165831
15. Krzyściak P, Bakuła Z, Gniadek A, et al. Prevalence of Malassezia species on the skin of HIV-seropositive patients. Sci Rep. 2020;10(1):17779. doi:10.1038/s41598-020-74133-6
16. Moreno-Coutiño G, Sánchez-Cárdenas CD, Bello-Hernández Y, Fernández-Martínez R, Arroyo-Escalante S, Arenas R. Isolation of Malassezia spp. in HIV-positive patients with and without seborrheic dermatitis. An Bras Dermatol. 2019;94(5):527–531. doi:10.1016/j.abd.2019.09.012
17. de Moraes AP, de Arruda EA, Vitoriano MA, et al. An open-label efficacy pilot study with pimecrolimus cream 1% in adults with facial seborrhoeic dermatitis infected with HIV. J Eur Acad Dermatol Venereol. 2007;21(5):596–601. doi:10.1111/j.1468-3083.2006.01923.x
18. Edelman EJ, Rentsch CT, Justice AC. Polypharmacy in HIV: recent insights and future directions. Curr Opin HIV AIDS. 2020;15(2):126–133. doi:10.1097/COH.0000000000000608
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.