Back to Journals » Clinical Optometry » Volume 18
Eye Health Awareness and School-Based Screening in Saudi Schools: A Systematic Literature Review
Authors Al-Atawi S ![]()
Received 23 September 2025
Accepted for publication 4 January 2026
Published 13 January 2026 Volume 2026:18 569431
DOI https://doi.org/10.2147/OPTO.S569431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Saleha Al-Atawi1,2
1Faculty of Applied Medical Science, Al-Baha University, Al-Baha, Saudi Arabia; 2Faculty of Applied Science, Tabuk University, Tabuk, Saudi Arabia
Correspondence: Saleha Al-Atawi, Email [email protected]
Background: Vision impairments are harder to diagnose among children, even though detection in childhood offers the biggest window for arresting potentially irreversible impacts on children’s socioemotional and educational performance.
Purpose: This study sought to determine the prevalence of vision impairments in school-going children in Saudi Arabia and gap between the knowledge of visual impairments in school-going children and parental care-seeking practices relating to the effectiveness of school-based eye health screening programs, implementation challenges, and best practices.
Methods: The study uses a systematic review and meta-analysis conducted in December 2024 to January 2025.
Results: The present study analyzed primary 35 studies (n = 30,277). While estimates varied materially across regions and demographics, the most prevalent eye conditions affected school-going children were (un)corrected refractive errors and amblyopia. The prevalence of refractive errors, hyperopia, myopia, and astigmatism was 27.43% [18.14,39.20], 13.01% [4.00,33.00], 8.59% [3.53,19.42], and 15.35% [4.97,38.62], respectively. Amblyopia and strabismus affected 0.07 [0.04, 0.11] and 0.05[0.01,0.18] of the population, respectively. Even so, only 23.87% [10.91,44.54] of children already had glasses or contact lenses, despite more than 61.74, 95% [46.78, 74.77] of parents being open to children having glasses/lenses. Routine screening was estimated at in 38.85%, CI [28.99, 49.71.79]. Gerental awareness about eye health and specific vision impairments is inadequate, inconsistent, and broadly varied. School-based screening is equally basic or need to be officially established.
Conclusion: Children’s immature ocular system offers good opportunities for intervening before reduced (or loss of) vision can materially affect quality of life, and education-work-life opportunities. With near universal primary school enrolment and continual engagements between children and education practitioners, schools offer an ideal institutional framework for early vision screening and intervention.
Keywords: Saudi Arabia, amblyopia, school health services, paediatric vision screening, awareness
Introduction
Vision and hearing are easily the most important senses for children as they are almost entirely dependent on visual and audio inputs for their early learning and communication.1 Visual impairment due to refractive errors, for example, affects 153 million people aged above five years, 8 million of whom have lost their vision.2 An estimated 12.8 million children (aged 5–15) struggle with visual impairment due to uncorrected refractive errors, representing a global prevalence of 0.96%.2 Most (underlying factors causing) visual impairment disorders, including cataracts, strabismus, corneal opacities, refractive errors, and poor accommodation, are preventable and treatable, especially if detected early in their onset.1,3,4 In Saudi Arabia, the most causes of visual losses included optic nerve disorders (40%), cataracts (7.5%), retinal disorders (32%), and uveitis (7.5%).4,5 Uncorrected disorders, on the other hand, can lead to irreversible vision loss and material degradations in the quality of life as well as educational, psychological, and economic attainment to individuals, families/caregivers, and even society.1 Severe disorders (eg, glaucoma) necessitate multiple post-diagnosis treatments, often with poor visual prognosis.4
Given the fact that the effectiveness of interventions to most eye health problems is best at the earliest, coupled by the fact that children are least capable of recognizing (mostly progressive) vision impairments, understanding the prevalence of vision impairments and the extent of awareness by parents/teachers/schools offers the best indicator to the possibility of arresting the problem. In Saudi Arabia, however, disparate regional empirical literature exists on prevalence, knowledge/awareness, and practices, making for poor generalizability.6,7 A systematic review helps mitigate the low generalizability. Further, the gap between prevalence on one hand, and the knowledge, awareness, and practices by parties that are most responsible for detecting (and seeking care for) vision impairments in children points to the opportunities for early detection, intervention, and even care-seeking behaviour. Specifically, this review seeks to establish the pooled prevalence of vision impairments (general and specific conditions) in children in Saudi Arabia, assess the extent of routine vision screen among school-going children in Saudi Arabia, and the extent of parental eye health awareness or practices by parents of school-going children in Saudi Arabia.
Methodology
In keeping with the research question/objectives, this review was underpinned by guidelines from Munn et al (2014), JBI (2022), and Wolfswinkel et al (2013), ie, scope definition, literature search, final sample selection, corpus analysis, and findings presentation.8–10 The researcher ran multiple queries against databases to understand the general topic coverage. To keep the size of the review manageable, the search only focused on peer-reviewed, primary research publications.
Procedures
Based on the reading of the abstracts and most cited sources, the final search criteria were determined using keywords that contained terms/phrases “prevalence” OR “teachers’ attitudes” OR “vision” OR “eye” AND “screening” OR “care”, OR “practices” OR “awareness/knowledge” AND “Saudi Arabia” AND “school(s)”. The search queries were run against each database (PubMed, ScienceDirect, Scopus, and Web of Science), following every search, the search phrases were adapted, and sources that made the inclusion criteria were downloaded into a bibliographic software (Figure 1).
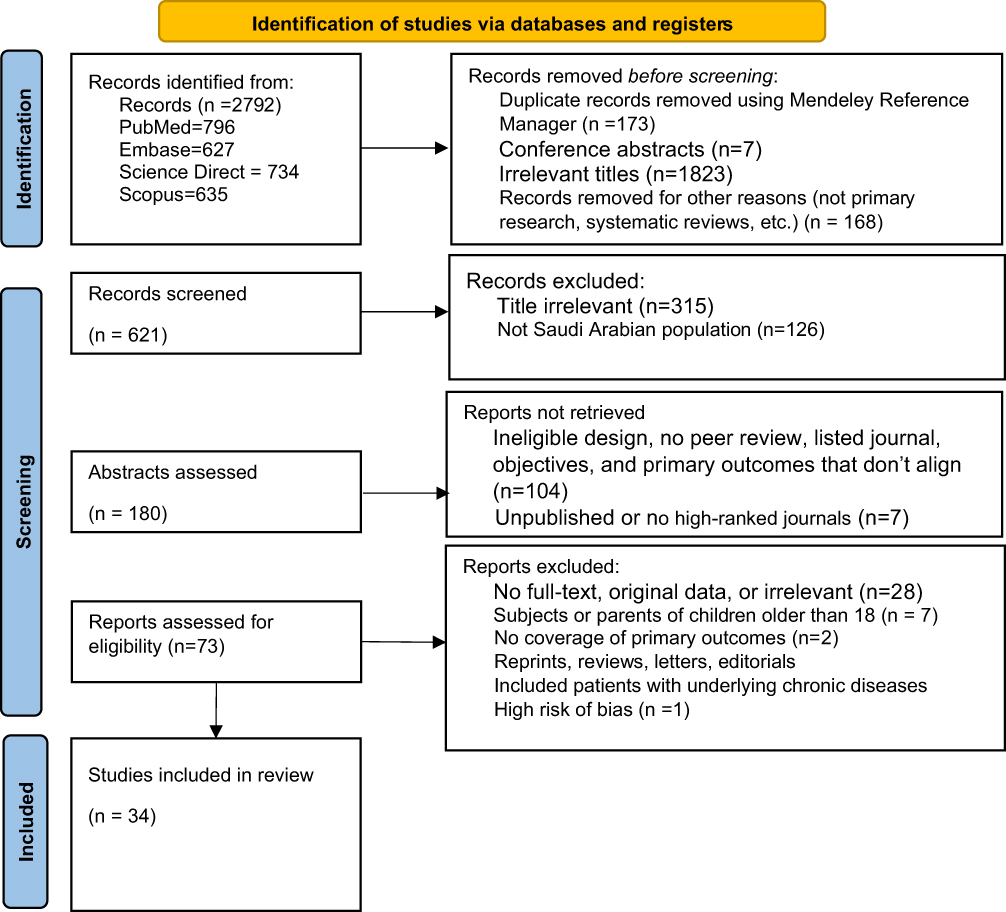 |
Figure 1 PRISMA flow diagram. |
Inclusion and Exclusion Criteria
The search, conducted in December 2024 to January 2025, included:
- Peer-reviewed primary research studies published in 2014–2025, in which the participants were children (18 or less years) or parents of children in Saudi Arabia.
- Included quantitative analysis of primary outcomes, namely, prevalence of vision impairments (either in general or any specific disorders); school-based or other routine eye screening of children; and knowledge, awareness, and practices of eye health in children.
- Works that were in progress, without full-text copies, as well as those that involved studies wholly undertaken outside Saudi Arabia, and/or were from journals that were unranked in the Journal Citation Index, were excluded.
- Vision disorders closely linked to other serious/chronic diseases such as diabetes, sickle cell, and retinopathy of prematurity were similarly excluded (for knowledge, awareness, and practices review) as patients are likely to receive information and care in their encounters with healthcare systems.
A close screening of the titles led to the selection of an initial 248 sources, before the abstracts were examined, leading to 34 sources due to, among others, duplication, coverage of subjects older than 18 or not identified as parents, and irrelevance. The references of the most cited works selected were examined for sources that meet the inclusion criteria. Six additional sources were identified. Accordingly, six more sources were identified. See Figure 1.
Data Extraction and Analysis
The data extracted included the demographics (sample/population, gender, region/location, and settings) research design, disorder, and results (prevalence of vision impairments, children diagnosed with vision impairments, use of glasses/lenses, involvement in routine screening, and knowledge/attitudes/practices about eye health, including treatments). Studies with different populations/settings, eg Nawaysir et al 2020,11 were considered separate entries for each population. Quantitative data was converted into frequency. Knowledge, Awareness, and Practices studies reported diverse outcomes. For comparability, this study focused on the most commonly reported outcomes or those that could be constructed easily from the diverse outcomes reported, eg, the two primary sources of information, ie, personal (social media, Internet, media, and family/relatives) and clinical/formal sources (ophthalmologists, pharmacists, physicians, optometrists, health promotions, and formal training), could be determined by aggregating different reported sources. General knowledge rated as “Good”, “Excellent”, or “Very Good” was compared to any other forms of awareness or lack thereof. For studies that utilized Likert scales, two extreme scores of 4–5 and 1–2 for a five-point scale were aggregated. Other responses like “Do Not Know” and “Unsure/Neutral” were considered as a lack of knowledge/awareness. Studies, in which participants were tested on multiple constructs, eg, the definition, treatment, and causes of an impairment; the construct on which the highest number of participants showed awareness was taken as a proxy for awareness in cases the responses were not mutually exclusive (respondent allowed to select more than one response). Mutually exclusive responses were aggregated (ie, all responses sum up to 100%).
Data Analysis
The study used standardized templates Munn et al8 and JBI Checklist for Analytical Cross Sectional Studies10 to extract descriptive data from the studies, including the years of publication, sampling, analytical rigor, and research design. Subsequently, each study was subjected to inductive thematic analysis (Tables 1 and S1). Quantitative data (comprising of the frequency of an occurrence Microsoft Excel and subsequently analyzed using R Studio to obtain Forest Plots and pooled prevalences. The heterogeneity of the study results was determined by the I2 statistic, by which scores of less than 40%, 60%, and above 60% were considered as low, moderate, and high heterogeneity, respectively.12 A p-value of 0.05 was considered statistically significant.
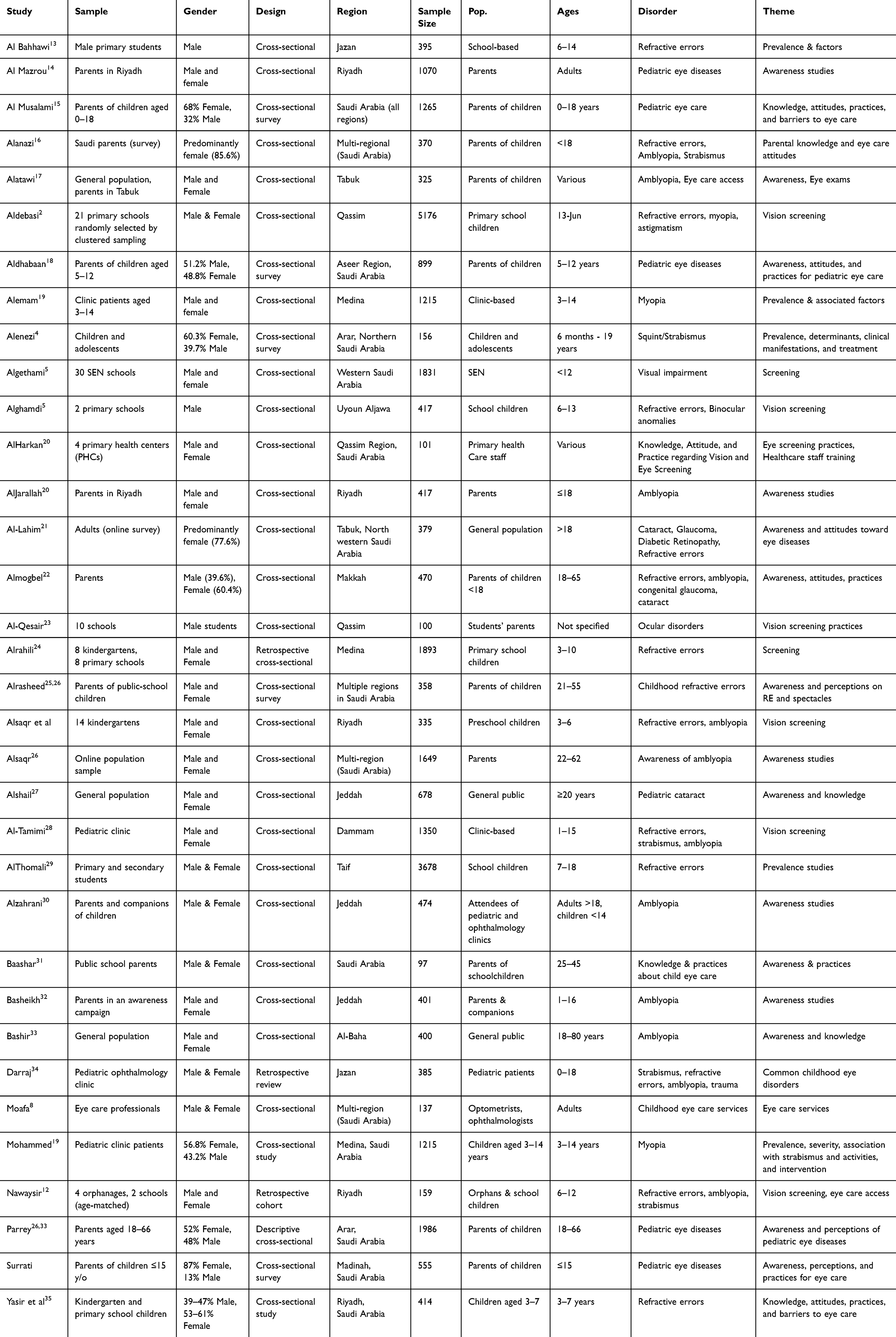 |
Table 1 Assessment criteria based on Munn et al (2014) and the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies |
Findings
Participant Characteristics
The 36 studies sampled approximately 30,277 participants. At least 20% parents of children (43.3%), children, including primary school children, school (not college), kindergarten, and pediatric clinic patients comprised 50.0%, while other subjects (under the age of 18) comprised 5.7% of the participants. The studies either investigated awareness of eye diseases in general or awareness of specific conditions like amblyopia and refractive errors.17,22,36 Nearly 51.4% and 28.6% of the studies employed cross-sectional designs and cross-sectional surveys, respectively, while retrospective cross-sectional, Retrospective cohort, and Retrospective review each accounted for 2.9%. Approximately 77.1% of the studies employed convenience sampling, while 17.1% and 2.9% used random and clustered sampling, respectively. Most of the studies were conducted in Riyadh (20%), Jeddah (14.3%), Qassim (11.4%), multi-regional (11.4%), Tabuk (8.6%) and Medina (8.6%). One study each was conducted in Western Saudi Arabia, Makkah, Dammam, Al-Baha, Aseer Region, Uyoun Aljawa, Jazan, Arar, and Taif regions.
Risk of Bias
Funnel plots were created (for primary outcomes) with more than 10 data points. The funnel plots showed moderate asymmetry, possibly due to small-study effects, publication bias, and/or methodological/population heterogeneity. The pooled estimates should, therefore, be interpreted cautiously. See Figure 2.
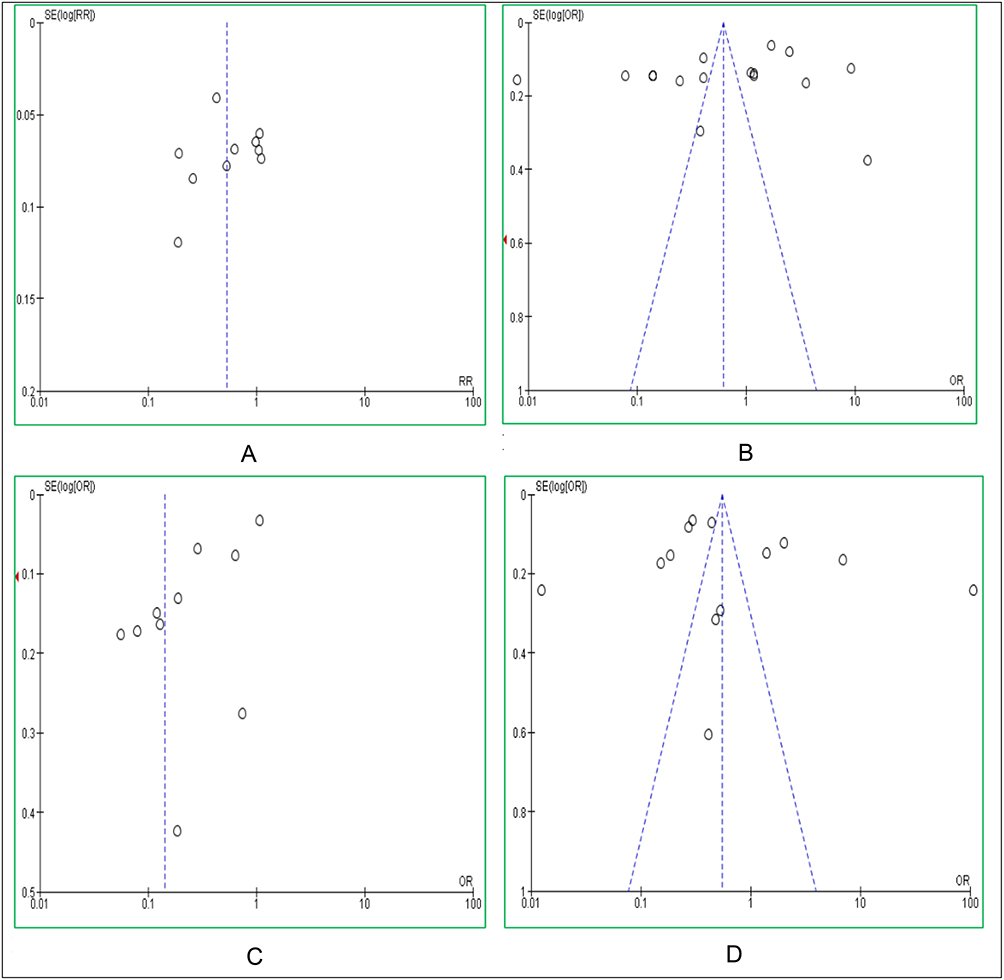 |
Figure 2 Select primary outcomes funnel plots. (A–D) show the funnel plot for knowledge and awareness of amblyopia, general knowledge of vision impairments, refractive errors, and routine visual screening, respectively. |
Using the JBI Checklist for Analytical Cross Sectional Studies, the corpus shows inconsistent sampling frames, inconsistent sampling strategies, incomplete adjustment for confounders, and diverse measurement. See Table S1.
Prevalence of Eye Impairments Among Children in Saudi Arabia
Eleven studies, comprising 18,156 events, measured refractive errors.1,5,6,11,13–19 The prevalence rate was 27.43%, 95% CI [18.14, 39.20]. Excluding, Surrati et al5 and Almogbel et al17 which relied on self-reported questionnaires/non-clinical measures, the pooled prevalence rate was 27.32%, 95% CI [16.29, 42.07], even though the model still exhibited extreme heterogeneity, (Tau2 = 4; χ2(8) = 2040.02, I² = 100%, p<0.05). Ten studies,1,11,13–16,18–20 comprising 14,108 events, reported myopia as an outcome. The pooled prevalence rate was 8.59%, 95% CI [−3.53, 19.42]. See Figure 3. Hyperopia was reported in 10 studies,1,11,13–16,18,19 only one of which used self-reported questionnaires instead of tests.1 The prevalence of hyperopia was 0.13, 95%, CI [0.04, 0.33], Tau² = 2.6595; χ2(9) = 1336.10; I² = 99%, p<0.05). Astigmatism was reported in 10,628 events. The pooled prevalence was 15.35%, 95% CI [4.97, 38.62], χ2(9) = 853.33; Tau² = 2.4358; I² = 99%, p < 0.05). See Table 2.
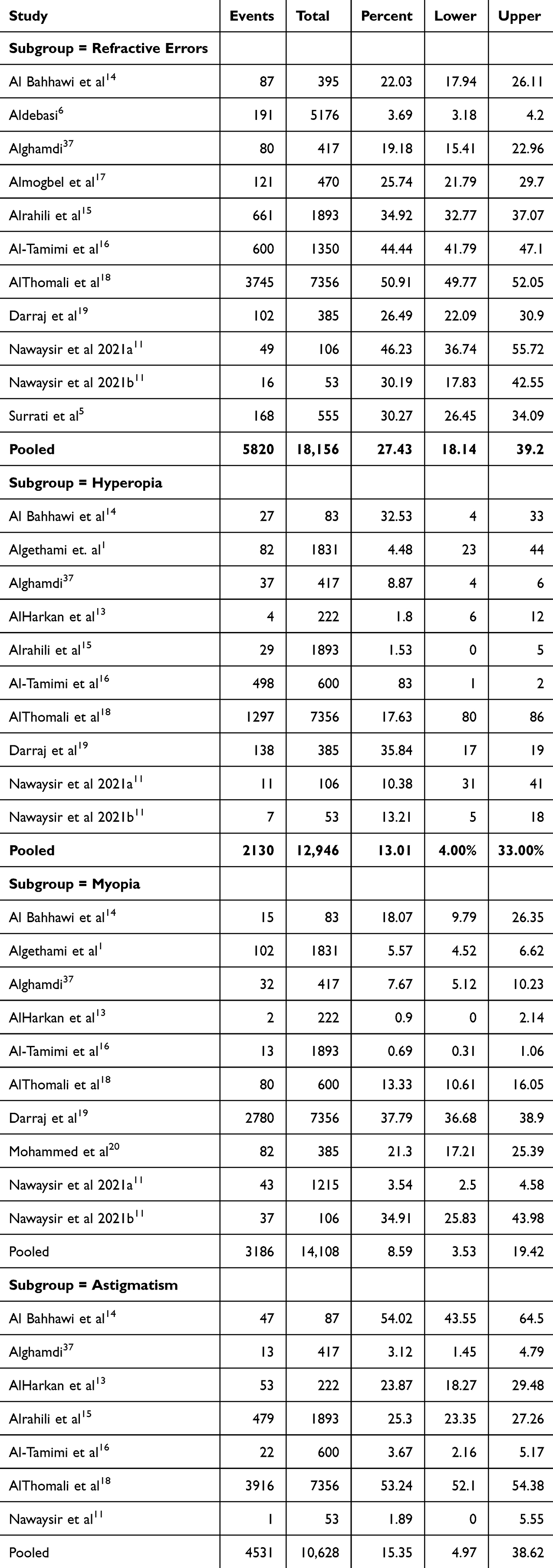 |
Table 2 Pooled Prevalence Rates for Refractive Errors |
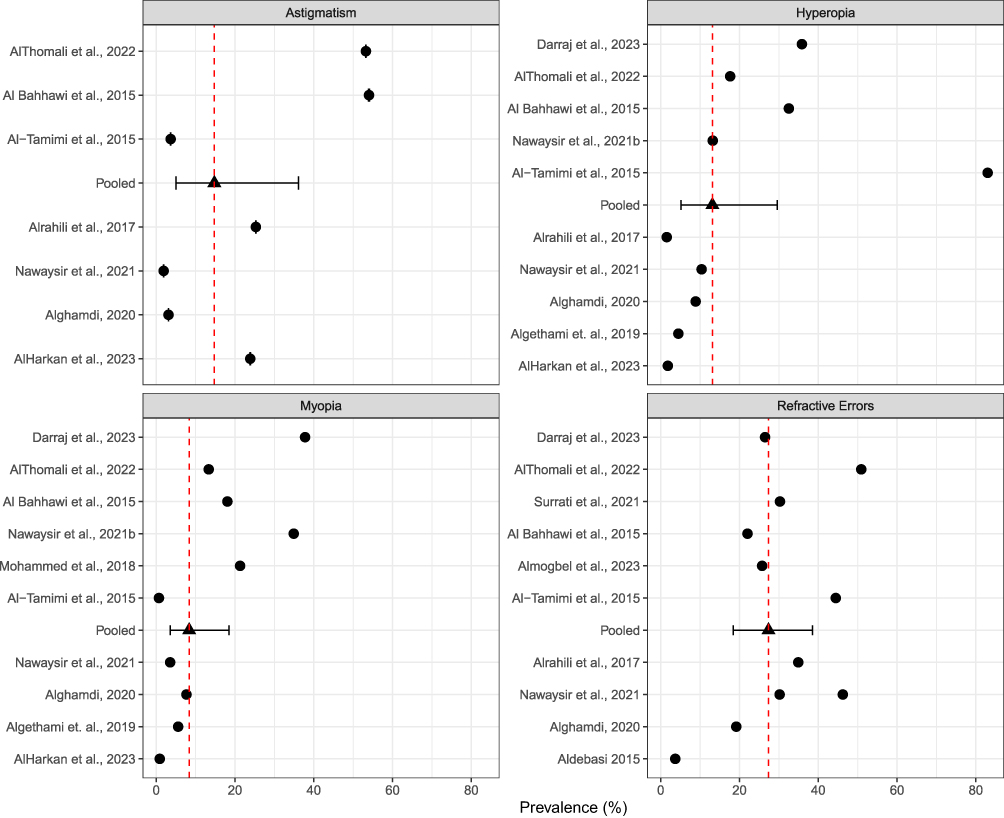 |
Figure 3 Gives the forest plots for the refractive errors prevalence rates. See below. |
Amblyopia was reported in 7 studies (8921 events).5,6,11,13,16,21 The pooled prevalence was 0.07, 95%, [0.04, 0.11], Tau² = 0.4329; χ2(6) = 98.61; I² = 93.9%, p < 0.05). Strabismus, which was reported in eight studies,5,7,11,13,16,19,21 was even less prevalent than amblyopia, 0.05[0.01,0.18], Tau² = 14.4537; χ2(7) = 496.59; I² = 98.6, p<0.05. Excluding Surrati et al5 and Alenezi et al7 for self-reported prevalence, strabismus prevalence rate increased from marginally, but heterogeneity remained high. Lastly, the pooled prevalences of less-reported conditions, including glaucoma and cataract could not be meaningfully estimated given the few events and works in which they were reported.5,17 See Figures 4 and 5.
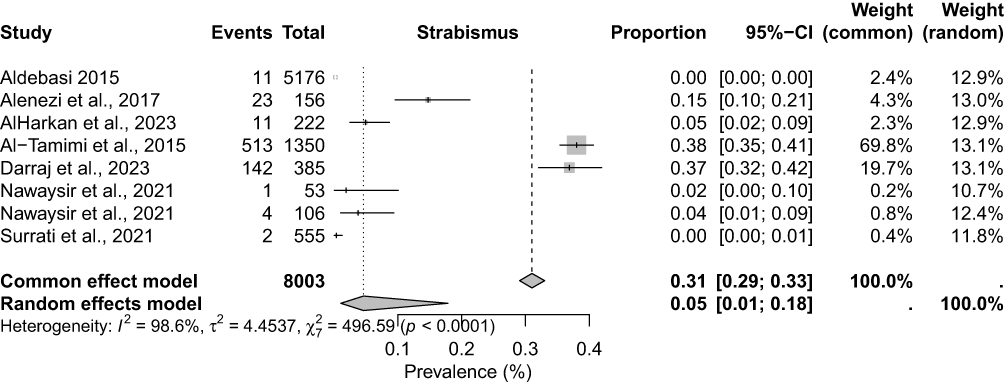 |
Figure 4 Strabismus Forest plot. |
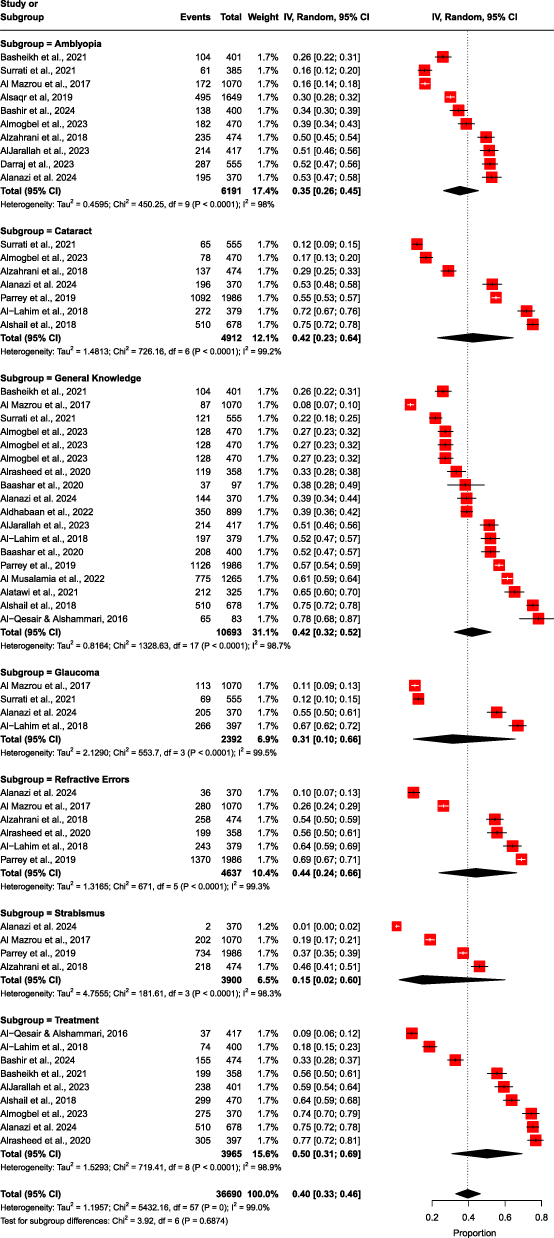 |
Figure 5 Knowledge, awareness, and practices forest plot. |
A total of eight studies,1,11,17,23–26,37 including 4587 events, reported on whether children were already using glasses or contact lenses. An estimated 23.87% of children already wear glasses or contact lenses (23.87, 95% [10.91,44.54], Tau² = 2.01, I² = 99%; Z = 930.84, p < 0.05) while 61.74%of respondents in 5616 events were open to their children wearing or contact lenses, (61.74, 95% [46.78, 74.77], Tau² = 0.85, I² = 99%; Z = 608.32, p < 0.05). Nearly the same number of parents believed surgery was acceptable or would be willing to have their children undergo surgery, 60.30, 95% [2.75,82.57], tau2 = 1.66; I² = 99%; Z = 506.16). See Table 3 below.
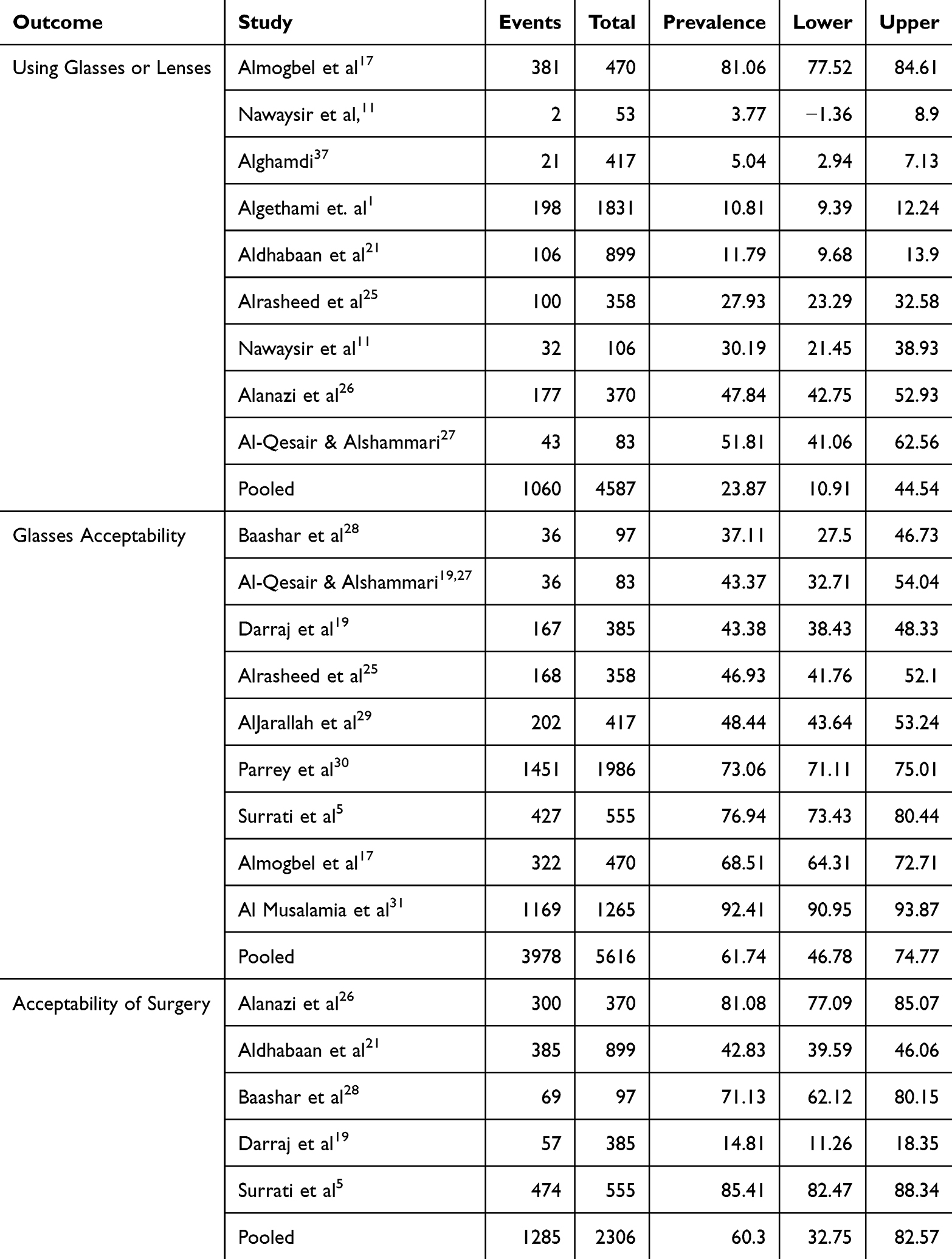 |
Table 3 Interventions and Acceptability |
While Darraj et al19 found age and gender to insignificant, Aldebasi6 and AlThomali et al18 found myopia was more prevalent with increasing age and female children, while Mohammed Alemam et al20 found it was more prevalent in males and those engaged in weekday indoor near work activities. Hyperopia was higher in boys and younger children, while astigmatism increased with age but was higher in boys.6,19,20 The relationship between age and increasing prevalence of conditions like myopia coincide with the years of schooling in 7–8- and 11–12-year-old children (or less outdoors time).6,18 While gender has been shown to be a factor, Aldebasi include multi-country evidence that differences in vision disorders’ onset and progression are linked to growth spurts as both girls and boys with earlier peak height velocity post similar onsets and progression.6
Among patients in Jazan, Darrajet al established that strabismus accounted for 36.9% of all disorders, while RE, ocular trauma, corneal infection, and keratoconus accounted for 26.5%, 7.5%, 7.3%, and 6.2% of cases, respectively.6,14,19 Further, Bahhawi et al hyperopia made up 32.2% of uncorrected refractive errors (URE) in Jazan, while myopic astigmatism, hyperopic astigmatism, and myopia made up 31%, 16.1%, and 17.2%, respectively.
Studies that inferentially tested age, gender, geographical, and other demographic risk factors effects permit a more nuanced understanding of eye disorders, and thus more targeted interventions.14,15 Some literature indicates that some conditions’ prevalence is affected by socio-demographic and geographical factors, eg, refractive errors were more likely to occur in females (15.5% versus 11.7%) and rural children (21.9%), with older children (12–14 years) at significantly higher risk. Even so, just 9.4% of participants with refractive errors had corrective glasses. Even so, the evidence is inconclusive, and studies mostly fail to account for confounders, thereby undermining causal inferences and generalizability. As a case in point, while Alrahili et al modelled gender and age, they did not account for broader demographic factors such as socioeconomic status, screen time, and parental knowledge.15 Bahhawi et al found that hereditary factors, living in rural areas, and screen time causally affected refractive errors affected prevalence.14
Vision Screening Status and Effectiveness
Screening and Effectiveness of School-Based Eye Screening
Routine vision screening was reported in 12 studies comprising 7491 events,1,5,21,24–31,36 of which 2911 routinely took children for screening, representing 38.85%, CI [28.99, 49.71.79], Tau² = 0.5826; I² = 100%. Thus, as many as 38.85% of respondents had or were likely to take children for screening. See Table 4.
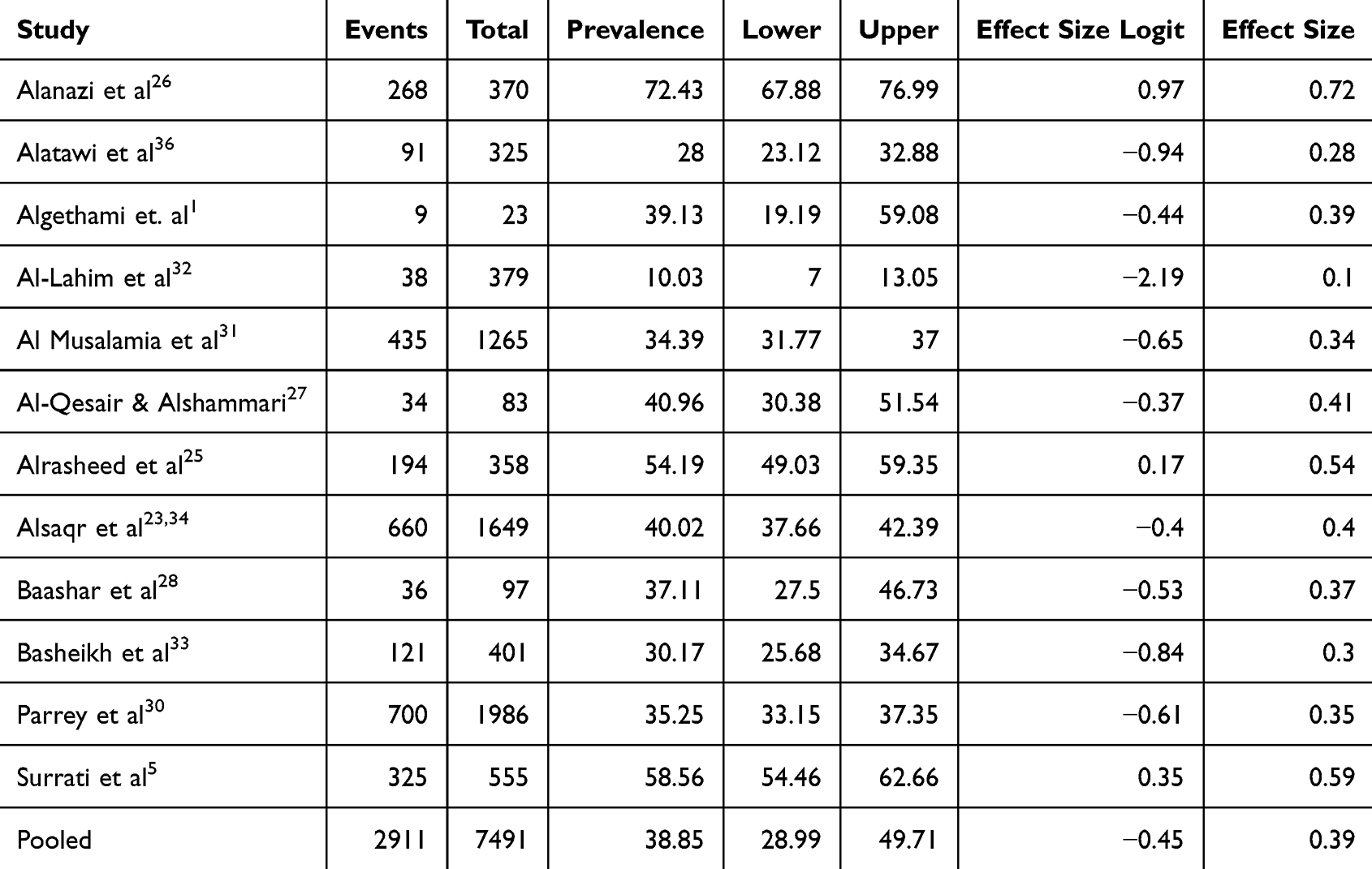 |
Table 4 Routine Vision Screening |
Knowledgeable parents are more proactive in seeking eye care.17,20,32 There is no evidence in the sampled studies of the existence or coverage of school-based vision screening programs and follow-up care in Saudi Arabia. According to Al-Qesair et al, school health units, particularly in rural areas, are under-resourced to either detect many eye disorders or offer follow-up care.26 Effectiveness hinges on just the pre-enrolment screening, but on follow-up, service access, and referrals for further care.6,26 The majority of the literature indicate a lack of vision screening by school health units contributing to low detection of vision disorders. Routine screening is critical for detecting, preventing, and effective treatment of eye disorders,6,15,24 but there is only little evidence that such programs exist, are effective,26 or have been institutionalized across Saudi Arabia.1,4,11,15
In one study, at least 50% of parents had been to see an ophthalmologist for their children to be screened.5 More than 70% of parents only sought care when they had a specific eye problems, while up to 37% sought no treatment or resorted to home remedies.27 Just 10% reported having routine screening.27 As many as 58.6–60% of parents report not visiting eye clinics with their children for screening.21,31 A single study claims that routine visual screening programs in Saudi Arabia. According to Al-Qesair et al (2016), school health units are mandated to conduct vision screening for children before school enrolment. Even so, the screenings are basic (rely on the Logarithm of the Minimum Angle of Resolution charts or Snellen Visual Acuity charts) and improperly conducted that they miss many eye disorders (eg, hyperopia).26 Others, including Alanazi et al,32 Alsaqr et al21 and Nawaysir et al,11 state that standardized age-related eye screening programs are non-existent in Saudi Arabia even though highly limited and basic school health programs may exist on some regions. Instead, screening occurs through health fairs, community outreaches, and school-based assessments.21,32
Parental Knowledge of Screening
According to Alanazi et al,32 half of parents understand the need for yearly eye screening for their children but still exhibited gaps in knowledge on symptoms of vision impairment and frequency of screenings. While 38.85% of parents either had or would take children for screening if they complained,23,29,33,36 only 13.8% of parents took children for annual screening and as many as 40–64% of parents did not see the utility of routine screening.33,36 One study found that two thirds of parents did not take children for eye screening.28 Only 14.2% and 30.2% of parents in Tabuk City and Jeddah, respectively, had their children screened before starting school.33,36 Others reported having no financial resources (23.3%), or believed their children had good vision (59.0%).23 Most guardians/parents and teachers would only seek eye care when the problem is severe21,33,34,36 and nearly as a third did not know of the need to proactively seek vision care for their children.23,33 Knowledge/perceptions varied broadly across regions and demographics.28
Knowledge, Awareness, and Practices
Knowledge, awareness, and practices were reported in more than 35,000 events. The available studies determined awareness of general vision impairments in children ranging from 38.9% to 62.5%,23 with awareness of specific disorders varying significantly. While there is material heterogeneity across studies and outcomes, general knowledge about vision impairments or eye health was good or excellent in 42% of 10,693 events, (95%, 0.42[0.32,0.52], Tau² = 0.8164; I² = 98.7%, p < 0.05). The belief that the eye impairments were either treatable or the scope of effectiveness of treatment was good or excellent in 50% of the population, 95% [0.31,0.69], Tau² = 1.5293; χ2(8) = 719.41; I² = 98.9, p < 0.05).
The level of awareness varied across impairments, with most common and/or serious conditions like cataracts than milder conditions like refractive errors that have not advanced.26,27 The pooled estimate of cataract and refractive errors awareness were the highest, (0.44, 95%, [0.24,0.66], Tau² = 1.3165; χ2(5) = 671; I2 = 99.3%, p < 0.05) and (0.42, 95%, [0.23,0.64], Tau² = 1.4813; χ2(6) = 726.16; I² = 99.2, p < 0.05), respectively. See Figure 4.
The available studies determined awareness of general vision impairments in children ranging from 38.9% to 62.5%,23 with awareness of specific disorders varying significantly. There is low parental awareness of vision disorders in children and the need for screening.4,36 The level of awareness varied across impairments, with most common and/or serious conditions like cataracts than milder conditions like refractive errors that have not advanced.26,27 The available studies determined awareness of general vision impairments in children ranging from 38.9% to 62.5%,23 with awareness of specific disorders and sociodemographics varying significantly. For example, awareness of amblyopia was as low 3% and about 50% showed acceptable knowledge about vision impairments.27 Alsaqr et al21 and Basheikh et al33 estimated amblyopia awareness among 25.9–30% of parents, with 70% of parents having no prior knowledge of the condition. In Jeddah, as many as 49.7% were knowledgeable about amblyopia.33 As many as 35% of parents were considered to have a poor awareness of amblyopia compared to 3.0% and 62% that had a good and fair level of awareness, respectively. Up to 56.7% of parents had sufficient knowledge, with the highest awareness for refractive errors (69%) and the lowest for strabismus (37%).31
An estimated 19.1% and 51.7% of parents in Riyadh and Madinah, respectively, had a basic understanding of amblyopia,5,33 11.7% and 12.4% of parents in Madinah having a good grasp of childhood cataract and glaucoma, respectively.5 Up to 51.3% understood what lazy eye was, while 55.6% of parents in Jeddah believed children could be fully cured if they complied with amblyopia medication.26,33 Less than 8.9% of parents in Riyadh understood that amblyopia was untreatable after age 10,34 even though 59.4 in Jeddah understood that age affected treatment outcomes.33 Alshail et al 39.7% of participants in Jeddah did not know whether cataracts were treatable and even more did not recognize its symptoms.26
Sociodemographic factors, including family exposure (members had vision impairments), older,5,22,24,29 occupation,22,27 female parentage,24 Saudi nationality, social status/higher income,5 geographical region, education level, Internet access, education level,24,27 and clinic visits; had a statistically significant relationship with parent knowledge/awareness of eye conditions, but the majority of the evidence shows that such relationship largely lacked statistically significant support in the majority of works analysed.4,32–35 While the parents’ overall knowledge is low, older parents or took children for eye examinations had more information about eye health, but no statistically significant effect was shown for parents’ level of education levels.29 As a case in point, Baashar et al29 found 24.7% of parents had a visually impaired child, half of whom had received advice from the doctor on visual impairment. The majority of the patients (61.9%) did not see the need for routine screening, and even more (69.1%) thought their children had excellent vision. Between 54.6% and 63.3% believed blind children could cope with their condition even though 48.5% thought that such children could not learn and 42.3% of parents did not know of any school for the blind.23,29
Equity and Access
According to Moafa et al (2022), eye care professionals believed paediatric eye screening services across Saudi Arabia to be satisfactory, with minor regional discrepancies. While paediatric facilities may be equipped, but without routine screening, coupled with health-seeking behaviour, the general population of children would still have limited access.4 The Eastern region was more endowed in paediatric teams and eye care services compared to the Southern and Northern regions.4 There is some evidence from Nawaysir et al (2020) that gaps in service coverage for schools and orphanages exist, thereby highlighting a need for equitable eyecare services, but there is no research exploring causality with eye health outcomes.11
Vision Screening in Saudi Arabia
There is more research focused on regional vision disorder prevalence that vision screening and/or effectiveness.26 The need for improved coverage is emphasized, but lack of school-based initiatives defeats the ability to reduce the delay between symptom manifestation and clinical presentation.33 The literature emphasizes the necessity of routine vision screening at enrolment and throughout schooling to minimize disease advancement and prevent lifelong complications.26,36
Teachers and Schools
While teachers are capable of detecting problems (eg, colour vision, distance/near vision, and visual acuity), more severe disorders remain undetected. Given the high prevalence of ocular disorders,6,14,38 basic and ineffective screening by school health units is inadequate.26 Health services offered by the Saudi Ministry of Education include inadequate vision health screening/care. Al-Qesair et al found that while 62.7% of sampled children in Qassim Province had eye problems, only 59% of children were evaluated by school health units on enrolment, and as many as 65.1% were not screened for vision problems or had no access to school health units.26 Up to 86.7% of parents were not informed by the school health units of the necessity of periodic screenings in the preceding two years and 80.7% thought the screenings undertaken were inadequate. Schools hardly communicated, engaged, and/or coordinated with parents about vision screening or problem cases, contributing to ineffectiveness of school health units. Even when schools informed parents of cases, referrals were poor. The majority of eye problems were detected by families, as against school health units.26
The few studies that explored the status of vision planning in Saudi Arabia.1,26,38 In a cross-sectional study involving 23 of 30 special education schools in the Western region of Saudi Arabia, 60.9% of schools did not offer vision screening. Despite 86% of special education needs (SEN) children facing heightened risks of oculo-visual disorders none of the staff received training on supporting vision-impaired children (and under 2.7% of the children required vision aids). SEN schools that routinely screened children for visual impairments were more likely to refer students for further management. As many as 5.6% of students were thought to have visual impairments but did not wear glasses, but 78.3% of staff lacked training for supporting visually impaired students. Where vision screening was done in schools, it was limited in scope and mostly conducted by teachers, optometrists, nurses, and ophthalmologists, who offer different degrees of clinical accuracy.1 In Algethami et al (2019), the majority of children that had underwent screening, were screened by the age of 7.1 Children that underwent vision screening recorded visual impairment as their primary impairment. Participants felt routine screenings using accessible tools, specialized physicians for SEN, mandated eye screenings during school admissions, and parental awareness.1
While Algethami et al1 meet the target sample size, its limited geographical scope and reliance on self-reported data limits the generalizability of the findings outside SENs and Western Saudi Arabia.2 Works such as Al-Wadaani et al,2 Algethami et al,1 AlThomali et al,18 and Alrahili et al15 employ descriptive statistics adequately, they do not utilize robust statistical modelling that would make it possible to explore predictive value of the relationships in the findings (eg, staff training and screening efficacy) in dynamic contexts. The heightened prevalence of refractive errors in females,2,6 for example, could benefit from inferential analyses of hypotheses and variables. According to Aldebasi, ascertaining axial length and subjects’ heights could help evaluate the effect of gender-dependent growth spurts on vision disorders onset and progression.
Practitioners’, Teachers’ and Parents’ Attitudes and Behaviours Toward School Children’s Eye Health
Teachers Awareness
Informed professionals in schools and primary healthcare settings can detect problems in their infancy and counsel parents or arrange for opportunistic tests. They can similarly ensure that children reduce screen time, near wok activities, and other activities that heighten the risks of eye problems.7,20 Compared to younger staff, AlHarkan et al13 determined that doctors above 40 years have relatively higher knowledge, practices, and attitude scores than nurses, while staff above 40 years generally had higher scores.
Resource Constraints
A deficit of vision specialists across (some) regions in Saudi Arabia is a contributing factor to low awareness, late detection, and low access to care.26 The ophthalmologist-to-population ratio in the northern region and western regions was 1:12,900 and 1:80,300, respectively, with the country being in need of 4,400 allied eye care personnel by 2020. Diagnosis and treatment equipment are similarly inadequate in some regions.4
Parental and Societal Challenges
The dynamics of vision care in Saudi Arabia is shaped by the healthcare infrastructure, regional disparities, and social beliefs.17,32,33 Lack of knowledge and/or sociocultural stigma about, among others, vision disorders, wearing glasses (and their effects on social, educational, work, and physical activities), eye conditions, and eye surgery are injurious to care seeking behaviour.23,29,32 It is notable that in a study where 50% of parents had taken their children to ophthalmologist clinics for screening also had largely positive beliefs about wearing glasses and other treatment.5
Information Channels
Social media and the Internet, friends/family, community members, and healthcare practitioners are more effective sources of information than one-off public service campaigns.22,27,32,34–36 The primary sources of information included eye care practitioners, eye clinics, family doctors, eyecare training, journals, medical education, search engines, and social media.21,29,31,34,35 Only a minority (1% in one study) indicated that they received information from radio.29 Overall, social media and relatives or friends were more likely to provide information compared to clinical and formal or clinical sources, (OR = 1.43, 95%, CI [0.64,3.19], I2 = 99.2%, Tu2 = 0.0404, p < 0.05). See Table 5 below.
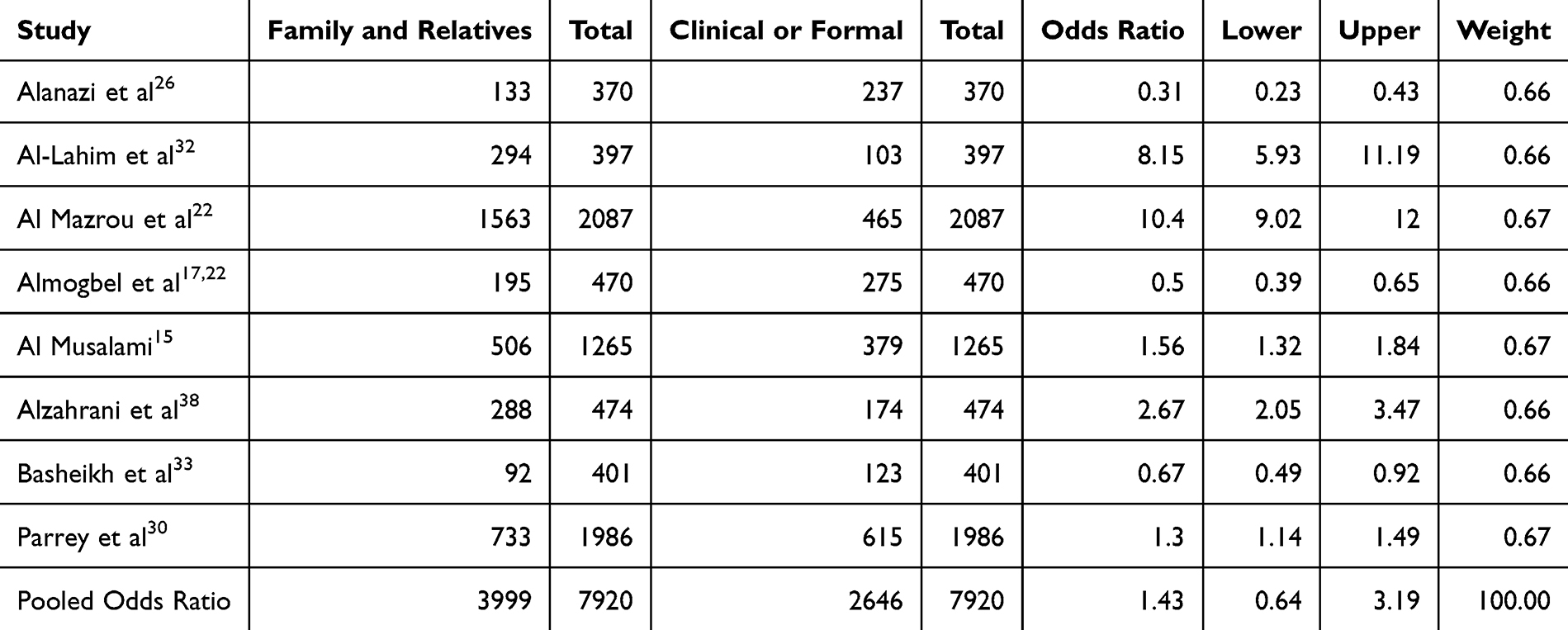 |
Table 5 Family/relative sources of information were compared with clinical sources |
Discussion
Prevalence
The pooled prevalence rates are broadly consistent with other larger studies beyond Saudi Arabia, including Loulidi et al,39 Alrasheed40 and Yekta et al.41 As a case in point, Yekta et al’s41 review covering 28 countries determined that visual impairment afflicted 7.26% of the population, with presenting visual acuity, amblyopia, and congenital cataract prevalences of 3.82%, 7.60%, and 0.60%, respectively. The estimated prevalence of different conditions varies broadly across many studies, largely because of methodological differences (eg, sampling, measurement, and definitional differences), but also because of equally broad ocular, environmental/geographical, genetic, access to care, and other factors affecting onset, advancement, and mitigation.18 The high heterogeneity in the pooled estimates necessitate extreme caution in interpreting the findings. The most prevalence causes of vision impairment in children in Saudi Arabia refractive errors (including keratoconus, astigmatism, hyperopia, and myopia), cataracts, amblyopia, and glaucoma.11,14–16,18,22,25 Rare conditions, including congenital cataract and congenital glaucoma had a low prevalence, which underscores the need for improved parental awareness of these sight-threatening conditions.5
Screening and Screening Effectiveness
Despite the availability of diagnostic resources/methods, many conditions like amblyopia go undetected,33 leading to severe impairments that may interfere with the children’s learning, career attainment, and social/mental health.33 This is, in part, because children hardly complain of vision problems because they are unaware of (ab)normal vision, leading to problems going unnoticed.26 The finding that general knowledge about vision impairments is only good or excellent in about 42% of the population and that only about 38.85% of parents realize the importance of routine screening and/or routinely have their children screened points to the necessity of ensuring that both guardians and teachers are alive to vision disorders, risk factors, and available resources to either prevent or offer requisite help.24,26 The evidence suggests vigilant and informed parents are more likely to arrest unusual vision issues and seek care.11 The evidence emphasizes the need for school-based vision screening programs for early detection and intervention.15
Screening Systems in Schools (and Childhood)
Visual screening in schools is, at best, inconsistent.1,3 The vast majority of children miss critical windows for detecting visual impairments even at special education schools, where disproportionately higher number of children struggle with visual impairments.1 Screening in non-clinical settings, especially when done by untrained teachers and school health unit practitioners, may have negatives, including false positives, resource wastage, and unwarranted anxiety.32 Coordination between schools, guardians, and the healthcare system is unclear to ensure high awareness and/or routine screening.29,34 The lack of vision screening guidelines for children or their non-implementation contributes to the inconsistent screening.26
Knowledge and Awareness
Providing parents, teachers, and even children with the requisite information empowers them to make informed decisions about their conditions and options before eye diseases advance or even become irreversible.26 Failures in ocular development may, however, go unnoticed, effectively losing opportunities to correct them as some advanced conditions are irreversible.34
The literature shows that a small minority of parents had acceptable knowledge and positive attitudes toward preschool vision screening, actual practice was poor due to the lack of specific training in eye care, lack of guidelines, and specialist support.42 The evidence points to an awareness deficit at the individual, family, school, community, and even public health levels.17,24,26
The level of awareness varied across impairments, with most common and/or serious conditions like cataracts than milder conditions like refractive errors that have not advanced.26,27
Screening in Schools
Arguably, the inadequacy of school screening programs undermines the potency of their diagnosis and the seriousness with which parents consider identified cases for further care.26 Requiring children to undergo mandatory eye exams early on, before school admission, and throughout their schooling is effective in arresting possible problems before they advance or become irreversible. Even so, parents’ lack of knowledge about eye health defeats routine school-based screening particularly given the lack of direct coordination between schools and the healthcare system.26 Increased parental/teacher awareness/knowledge and proactive attitudes could materially reduce delays between symptom manifestation and clinical manifestation, helping achieve early detection and intervention.33
Training and Awareness
Teachers are the first line of contact, especially for learning-related vision impairments, with primary school-aged children because they spend most of the daytime with the kids.26 The literature points to urgency of ramping up school-based resources and community awareness campaigns across demographics of parents (with primary-aged children).32 Providing teachers and healthcare practitioners with vision screening training and information would enhance their capacity for greater effectiveness.4,18,35,36
Information Channels
Structured public awareness and screening campaigns are needed to bridge the knowledge/information gaps among parents and practitioners in schools. The research evidence similarly reveals critical channels through which vision information may be shared for greater reach and efficacy. Specifically, the role of the Internet and new media are evident.4,33
Gaps, Limitations, and Areas of Further Research
The majority of studies employed non-random sampling, small samples, cross-sectional designs, and relied on limiting self-reported data collection methods along with subjective assessments of attitudes/familiarity.33,36 The vast majority of the studies employ adequately large and robustly selected samples, backed by standardized tools for measuring ocular diseases (for validity and reliability of results),6,15,34,42 but mostly fail to account for confounders (eg, socioeconomic status, awareness, parental education level, and health-seeking behaviours).11 Some studies employed highly limited online surveys.5 Most cross-sectional designs are inadequate in capturing the full scope of vision screening practices in schools across childhood, as well as the causal factors for diverse practices. Longitudinal design would not only offer more in-depth understanding of the nature of screening practices and underpinning drivers, they would make it possible to ascertain the efficacy of different interventions as well as how the same impact children’s academic and quality of life outcomes. Longitudinal research into the implementation of school- and institutional-based eye screening programs, including innovative screening models (eg, telemedicine), their coverage, cost, and effectiveness as well as the socioeconomic drivers/barriers would be valuable. As a case in point, it would be insightful to study the effectiveness of providing teachers and (primary) health practitioners with training to screen, detect, and refer children for care.
Large, random samples would equally improve on the present research evidence. Further, there is a case for standardizing definitions for different disorders for measurement to render it easier to compare studies across Saudi Arabia as it is unlikely that a single study to cover the entire country.15,18 Validated tools (including questionnaires and interview schedules) could be equally useful to facilitate comparability.33
Apart from the lack of a proactively registered protocol, which may have introduced selection, reproducibility, and reporting biases; the meta-analytical analysis in the present study is limited by the materially high and statistically significant heterogeneity. Studies that do not utilize the recommended protocol for refractive error studies, for example, result in heterogeneous estimates.41 The heterogeneity could similarly be cured by more robust age-specific research, particularly for conditions where prevalence or incidence varies significantly across different age demographics.6,14,19 Other sociodemographic variables need to be studied to ascertain their impact on vision impairments, awareness, and potential interventions.14,15
Policy Implications
There is a gap between the prevalence of vision impairments, especially relating to causes like refractive errors, and the number of children already using glasses or contact lenses. This, in turn, points to large numbers of children who could benefit from glasses. School health units could offer an effective institutional framework for eye care if coupled with firm screening protocols and adequate staff training.5,26 Deepening eye health programs in routine school health programs would create a robust information, support, and referral network across the country.6,26 The extant literature emphasizes the need for better training and systemic reforms but falls short, in part because of the low generalizability and internal validity for most of the primary works, in proposing detailed, actionable strategies for stakeholders.2 Arguably, routine vision screening initiatives (in school settings and) throughout childhood and expanded access to correction care, coupled with public education campaigns on vision impairments would be useful to promote eye care in Saudi Arabia.2,6
Conclusion
This study sought to ascertain a more generalizable prevalence rate of vision impairments in school-going children as well as estimate the gap between prevalence and knowledge, awareness, and practices (including routine screening). The findings confirm fairly high prevalence of vision impairments and causes like refractive errors, amblyopia, and strabismus, coupled by a deficit in knowledge/awareness and care (as shown only 23.87% of children already had glasses or contact lenses. This present study offers clues to eliminating preventable causes of visual impairment in Saudi Arabia. Consistent with other studies outside the Kingdom, the findings suggest refractive errors represent the most prevalent cause of visual impairment in the sources reviewed. It is notable that general knowledge about vision impairments (and even specific conditions) and openness to treatments like surgery and glasses/lenses are acceptably high in the studies reviewed. These could be exploited to foster health-seeking behaviour, early detection, and treatment.3,13,23,40 The lack of structured programs to routinely screen and identify children that require eye interventions transfers a heavier burden to parents.29 Other than children having difficulties self-diagnosing vision impairments, especially for asymptomatic conditions (in unadvanced states), the lack of routine school-based screening loses significant opportunity windows. The present study highlights the potential of peer-to-peer communication (including social media, friends, and relatives) in increasing awareness of visual impairments, despite their higher risk of misinformation and inaccuracy. It may help, therefore, the find ways of impregnating peer-to-peer communications with relevant and accurate information to bolster knowledge, awareness, and practices among the population in Saudi Arabia.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Algethami MR, Student M, Raffa LH, Alhibshi RH, Baabdullah MY, Alobudi AH. Vision screening services in special needs schools in Western Saudi Arabia. Saudi Med J. 2019;40(4):385–21. doi:10.15537/smj.2019.4.24076
2. Al Wadaani FA, Amin TT, Ali A, Khan AR. Prevalence and pattern of refractive errors among primary school children in Al Hassa, Saudi Arabia. Glob J Health Sci. 2012;5(1). doi:10.5539/gjhs.v5n1p125
3. Bardisi WM, Bin Sadiq BM. Vision screening of preschool children in Jeddah, Saudi Arabia. Saudi Med J. 2002;23(4):445–449.
4. Moafa MA, Alrasheed SH. Status of childhood eye care services in the Kingdom of Saudi Arabia: eye care professionals’ perspectives. Open Ophthalmol J. 2022;16(1). doi:10.2174/18743641-v16-e2206200
5. Surrati AM, Almuwarraee SM, Mohammad RA, et al. Parents’ awareness and perception of children’s eye diseases in Madinah, Saudi Arabia: a cross-sectional study. Cureus. 2022. doi:10.7759/cureus.22604
6. Aldebasi Y. Prevalence of amblyopia in primary school children in Qassim province, Kingdom of Saudi Arabia. Middle East Afr J Ophthalmol. 2015;22(1):86. doi:10.4103/0974-9233.148355
7. Alenezi HM, Abo El-Fetoh NM, Alruwaili AS. Squint in children and adolescents, Arar, Northern Saudi Arabia. Egypt J Hosp Med. 2018;70(2):298–302. doi:10.12816/0043093
8. Munn Z, Moola S, Riitano D, Lisy K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014;3(3):123–128. doi:10.15171/ijhpm.2014.71
9. Wolfswinkel JF, Furtmueller E, Wilderom CPM. Using grounded theory as a method for rigorously reviewing literature. European J Inform Sys. 2013;22(1):45–55. doi:10.1057/ejis.2011.51
10. JBI. Critical Appraisal Tools - JBI. 2022. Available from: https://www.medrxiv.org/content/medrxiv/early/2024/08/01/2024.07.31.24311260/DC1/embed/media-1.docx?download=true.
11. Nawaysir S, Al Saeedan A, AlMusa S, Albalawi A, Khandekar R. Comparison of outcomes of vision and eye screening of children of four orphanages and school children of Riyadh. Middle East Afr J Ophthalmol. 2020;27(3):172. doi:10.4103/meajo.MEAJO_241_20
12. Kong F, Wu T, Dai J, et al. Glucagon-like peptide 1 (GLP-1) receptor agonists in experimental Alzheimer’s disease models: a systematic review and meta-analysis of preclinical studies. Front Pharmacol. 2023:14. doi:10.3389/fphar.2023.1205207
13. AlHarkan DH. Amblyogenic risk factors and validity of vision screening using spot-screener among kindergarten children in Qassim region, Saudi Arabia. Saudi J Ophthalmol. 2024;38(3):268–274. doi:10.4103/sjopt.sjopt_246_23
14. Al Bahhawi T, Makeen AM, Daghreeri HH, et al. Refractive error among male primary school students in jazan, Saudi Arabia: prevalence and associated factors. Open Ophthalmol J. 2018;12(1):264–272. doi:10.2174/1874364101812010264
15. Alrahili NHR, Jadidy ES, Alahmadi BSH, et al. Prevalence of uncorrected refractive errors among children aged 3-10 years in western Saudi Arabia. Saudi Med J. 2017;38(8):804–810. doi:10.15537/smj.2017.8.20412
16. Al-Tamimi E, Shakeel A, Yassin S, Ali S, Khan U. A clinic-based study of refractive errors, strabismus, and amblyopia in pediatric age-group. J Family Community Med. 2015;22(3):158. doi:10.4103/2230-8229.163031
17. Almogbel AH, Al Shanbari N, Alibrahim IS, et al. Parents’ awareness and attitude toward pediatrics eye diseases in makkah, Saudi Arabia: a cross-sectional study. Cureus. 2023. doi:10.7759/cureus.38366
18. AlThomali TA, AlQurashi M, AlGhamdi AS, Ibrahim A, AlSwailmi FK. Prevalence of refractive errors in school-going children of Taif region of Saudi Arabia. Saudi J Ophthalmol. 2022;36(1):70–74. doi:10.4103/sjopt.sjopt_46_21
19. Darraj A, Barakat W, Kenani M, et al. Common eye diseases in children in Saudi Arabia (Jazan). Ophthalmol Eye Dis. 2016;8. doi:10.4137/OED.S39055
20. Mohammed Alemam A, Aldebasi MH, Rehmatullah A, Alsaidi R, Tashkandi I. Prevalence of myopia among children attending pediatrics ophthalmology clinic at Ohud hospital, Medina, Saudi Arabia. J Ophthalmol. 2018;2018:1–7. doi:10.1155/2018/3708409
21. Aldhabaan W, Alkhammash ZM, Al Zomia AS, et al. Knowledge and practices of child eye healthcare among parents in Aseer Region, Saudi Arabia. Cureus. 2022. doi:10.7759/cureus.30404
22. Al Mazrou A, Alsobaie NA, Bin AAK, AlObaidan O. Do Saudi parents have sufficient awareness of pediatric eye diseases in Riyadh? Saudi J Ophthalmol. 2020;34(3):171–176. doi:10.4103/1319-4534.310415
23. Alsaqr AM, Masmali AM. The awareness of amblyopia among parents in Saudi Arabia. Ther Adv Ophthalmol. 2019;11. doi:10.1177/2515841419868103
24. Alghamdi W. Prevalence of refractive errors among children in Saudi Arabia: a systemic review. Open Ophthalmol J. 2021;15(1):89–95. doi:10.2174/1874364102115010089
25. Alrasheed SH, Alghamdi WM. Parents’ awareness of and perspectives on childhood refractive error and spectacle Wear in Saudi Arabia. Sultan Qaboos Univ Med J. 2022;22(4):532–538. doi:10.18295/squmj.10.2021.141
26. Alanazi SRG, Alanazi HWH, Alanazi WG, et al. Parents’ knowledge and attitudes toward pediatric ophthalmic disorders in Saudi Arabia: a cross-sectional study. Pediatr Rep. 2024;16(4):902–920. doi:10.3390/pediatric16040077
27. Al-Qesair HF, Alshammari A. Parents’ perceptions towards the role of school health units at early detection of ocular disorders among students in Qassim Province, Saudi Arabia. Mediterr J Soc Sci. 2016;7(4):198–213.
28. Baashar A, Yaseen A, Halawani M, et al. Parents’ knowledge and practices about child eye health care in Saudi Arabia. Int J Med Develop Countri. 2020:454–460. doi:10.24911/IJMDC.51-1577288335
29. AlJarallah OJ, AlFehaid MS, Alnadawi AA, et al. Knowledge and awareness regarding amblyopia among parents in Riyadh, Saudi Arabia: a cross-sectional study. Cureus. 2024. doi:10.7759/cureus.53308
30. Parrey MUR. Parents’ awareness and perception of children’s eye diseases in Arar City. Ann Clin Analytic Med. 2019;10(06). doi:10.4328/ACAM.6133
31. Al Musalami SN, Al Qasim RJ, Alshuhayb BS, Al-Somali AI. Insights into parental perspectives: children’s eye care in Saudi Arabia. Heliyon. 2025;11(1):e41179. doi:10.1016/j.heliyon.2024.e41179
32. Al-Lahim WA, Al-Ghofaili RS, Mirghani H. Evaluation of awareness and attitudes towards common eye diseases among the general population of Northwestern Saudi Arabia. Egypt J Hosp Med. 2018;70(11):1983–1989. doi:10.12816/0044854
33. Basheikh A, Alhibshi N, Bamakrid M, Baqais R, Basendwah M, Howldar S. Knowledge and attitudes regarding amblyopia among parents in Jeddah, Saudi Arabia: a cross-sectional study. BMC Res Notes. 2021;14(1):60. doi:10.1186/s13104-021-05478-y
34. Alsaqr A, Ibrahim G, Sharha A, Fagehi R. Investigating the visual status of preschool children in Riyadh, Saudi Arabia. Middle East Afr J Ophthalmol. 2017;24(4):190. doi:10.4103/meajo.MEAJO_123_17
35. Alshail R, Basheikh A, Alharbi A, et al. Assessment of the level of awareness about paediatric cataract among the general population of Jeddah. Australasian Med J. 2020;13(1). doi:10.35841/1836-1935.13.1.4-9
36. Alatawi A, Alali N, Alamrani A, et al. Amblyopia and routine eye exam in children: parent’s perspective. Children. 2021;8(10):935. doi:10.3390/children8100935
37. Alghamdi W. Refractive errors and binocular anomalies in primary schools in uyoun Aljawa: a Small Urban Town in Saudi Arabia. Glob J Health Sci. 2020;12(10):116. doi:10.5539/gjhs.v12n10p116
38. Alzahrani N. Awareness, perceptions and knowledge of amblyopia among pediatrics and ophthalmology clinics attendees in King Abdulaziz University Hospital, Jeddah. Int J Adv Res. 2018;6(2):1506–1517. doi:10.21474/IJAR01/6583
39. Bashir M, Taishan SS, Alghamdi BM, et al. Knowledge and awareness of amblyopia among the adult population of the Al-Baha Region, Saudi Arabia. Cureus. 2024. doi:10.7759/cureus.73374
40. Loulidi S, Loukid M, Boussaa S. Visual impairment and blindness among children: a literature review. Clin Epidemiol Glob Health. 2025;34:102094. doi:10.1016/j.cegh.2025.102094
41. Alrasheed S. Systematic review and meta-analysis of childhood visual impairment in the Eastern Mediterranean Region. Eastern Mediterranean Health Journal. 2023;29(6):482–490. doi:10.26719/emhj.23.020
42. Yekta A, Hooshmand E, Saatchi M, et al. Global prevalence and causes of visual impairment and blindness in children. J Curr Ophthalmol. 2022;34(1):1–15. doi:10.4103/joco.joco_135_21
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.