Back to Journals » International Medical Case Reports Journal » Volume 18
Extracorporeal Membrane Oxygenation for Treatment of Immune Checkpoint Inhibitor-Related Pneumonia Complicated with Severe ARDS: A Case Report
Authors Meng Y, Yuan Y, Ma L, Wang J, Zhang B
Received 2 December 2024
Accepted for publication 15 March 2025
Published 26 March 2025 Volume 2025:18 Pages 411—419
DOI https://doi.org/10.2147/IMCRJ.S507273
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Yanfei Meng, Yamin Yuan, Li Ma, Jiaqi Wang, Bei Zhang
Department of Critical Care Medicine, Lanzhou University Second Hospital, Lanzhou University, Lanzhou City, Gansu Province, People’s Republic of China
Correspondence: Bei Zhang, Email [email protected]
Abstract: This paper utilizes a retrospective analysis to examine the diagnostic and therapeutic processes for a patient afflicted with immune-related pneumonia, which was complicated by severe acute respiratory distress syndrome (ARDS) and was triggered by Tirellizumab following a surgical procedure for a pulmonary malignancy. The patient exhibited unimproved oxygenation levels, which resulted from the implementation of a lung protective ventilation strategy through invasive mechanical ventilation during the early stages of treatment. Consequently, we opted to perform veno-venous extracorporeal membrane oxygenation (ECMO). Complications such as catheter-related infection, hemolysis, and membrane thrombosis occurred during the period under investigation. After the implementation of awake VV-ECMO, there were still difficulties in withdrawing the ventilator, and the disease was identified again and clearly diagnosed as immune checkpoint inhibitor-related pneumonia. Finally, after standardized treatment, the patient exhibited improvement. For patients with severe ARDS who have received invasive mechanical ventilation, It is imperative to standardize lung protective ventilation strategies, and to allow prone position ventilation under specific conditions. In cases where oxygenation remains unimproved, the selection of extracorporeal membrane oxygenation (ECMO) should be guided by cardiac function, with a concomitant understanding of the associated complications and management strategies. Furthermore, it is essential to thoroughly assess the benefits and drawbacks of awake ECMO, and to develop the capacity to discern diseases associated with fever and lung shadow for the purpose of precise treatment.
Keywords: awake VV-ECMO, checkpoint inhibitor-associated pneumonia, acute respiratory distress complex signs, lung protective ventilation strategy
Introduction
Immune checkpoint inhibitor pneumonitis (ICIP) is a disease associated with immune checkpoint inhibitors (ICIs) that induces lung injury with different clinical, imaging, and pathological manifestations. With the increase in the incidence and detection rate of tumors, the clinical application of ICIs has increased year by year. ICIP has been documented to account for up to 35% of anti-PD-(L)1-related deaths, ranking as one of the most prevalent fatal adverse reactions within this drug class.1 For cases of severe ICIP, patients may require ICU admission when the severity of their condition necessitates ventilator assistance. Ventilation or ECOM treatment is used when necessary.2 There have been many reports on the successful diagnosis and treatment of ICIP alone, but there are no relevant reports in China or abroad about the treatment of ARDS patients with severe ICIP combined with pulmonary infection by awake VV-ECMO. In the Department of Intensive Care Medicine at the Second Hospital of Lanzhou University, a patient with severe ARDS caused by severe ICIP combined with lung infection following surgery for a pulmonary malignant tumor was successfully treated by the skillful implementation of a lung protective ventilation strategy, VVECMO, and management of related complications, and awake VV-ECMO, as reported below.
Case Report
1.General information: male,58 years old, due to “chest stuffy breath for 5 days, aggravated with dyspnea for 1 day”. He was admitted on November 8,2023.
2.The patient’s medical history includes hypertension that has persisted for over a decade, with a maximum recorded blood pressure of 146/126 mmHg. The patient has been administered regular oral nifedipine sustained-release tablets at a dosage of 20 mg once daily. Additionally, the patient has a history of lung malignancy (squamous cell carcinoma of the lower lobe of the right lung) for 7 months, he underwent “right lower lobe resection” in Gansu Cancer Hospital on April 23, 2023; and recovered well after surgery. He received a regular intravenous infusion of tirellizumab at a dosage of 200 mg every three weeks to one month before admission. Additionally, he underwent long-term family aerobic therapy. SpO2 fluctuated at approximately 94%. The patient had a history of atrial fibrillation for six months, for which no standard diagnosis or treatment had been established.
3.The patient’s medical history, as documented in the patient’s electronic medical record, indicates the following:Five days prior to admission, the patient began to experience a new onset of chest tightness and shortness of breath. These symptoms were accompanied by a significant amount of expectoration, which was described as yellow and containing dark red blood. The patient also reported a fever, with a maximum temperature of 37.9°C. The patient also exhibited signs of weakness and poor tolerance. The patient was admitted to the Emergency Department of the Second Affiliated Hospital of Lanzhou University. The following day, the patient exhibited a further exacerbation of the aforementioned symptoms, accompanied by an elevated fever (39.5°C), the presence of blood in the sputum, an increased respiratory rate of 40 breaths per minute, and the development of dyspnea. The patient’s oxygen saturation levels (SpO2) exhibited a progressive decline, reaching 40%, necessitating the administration of oral intubation and ventilator assistance by the emergency center.
4.The patient’s physical examination upon admission revealed the following vital signs: body temperature of 36°C, pulse rate of 160 beats per minute, blood pressure of 147/76 mmHg (aramine 3.6ug/kg.min), respiratory rate of 34 times per minute, and SpO2 of 45% (FiO2 100%). The patient exhibited signs of drug-induced calm, with a general state of poor spirits. The patient’s skin exhibited a scattered speckled pattern, with the trunk predominating, and the extremities manifesting cyanosis. The bilateral pupils were noted to be large and round, measuring approximately 2 millimeters in diameter. The light reflex was sluggish, and cyanosis was observed in the oral and facial regions. The thorax demonstrated symmetry, and the lungs exhibited low exhalation sounds, which were audible and scattered, predominantly in the right lung. The auscultation of the heart revealed a strong first heart sound, an uneven rhythm, and a heart rate of 196 beats per minute. No pathological murmurs were detected in the auscultation area of each valve, and mild edema was observed in the lower limbs.
5.The patient underwent an auxiliary inspection, which revealed the following results: blood gas analysis indicated a pH of 7.13, a pCO2 of 54.6 mmHg, a pO2 of 41 mmHg, a lactate level of 9.2 mmol/L, a HCO3- level of 14.8 mmol/L, a BE level of −11.6 mmol/L, and an A-aDO2 of 492.3 mmHg. Additionally, cardiac muscle markers were examined. DDIM 2.4mg/L,NT-proBNP 189.0ng/L; Blood routine: WBC 13.35*10~9/L,NE% 0.71,RBC 5.15*10~12/L,HGB 154g/L; Infection index: CRP 57.93mg/L,PCT 0.19ng/mL; Biochemical: TG 3.89mmol/L,LDH 370U/L; Immunoglobulin IgG 7.25g /L; ECG: rapid ventricular rate, atrial fibrillation, ventricular rate 134bpm,ECG axis non-biased +38°; CT: interstitial fibrosis with infection in both lungs, slight effusion in the right pleural cavity.
6.Preliminary diagnosis: acute respiratory failure severe pneumonia ARDS, septic shock metabolic acidosis, arrhythmia atrial fibrillation atrial premature beat, pulmonary interstitial fibrosis, postoperative pulmonary malignancy, hypertension grade 3 (extremely high-risk group).
7.Diagnosis and Treatment Process: Following admission, the patient was placed on a ventilator assisted ventilation protocol, which employed a lung protective ventilation strategy. This strategy comprised synchronous intermittent command ventilation (SIMV) in conjunction with volume-controlled ventilation. The positive end-expiratory pressure (PEEP) was meticulously adjusted according to the PEEP/FiO2 table, with the parameters set as follows: Tidal volume (VT) 400 mL, positive end-expiratory pressure (PEEP) 22 cmH2O, inhaled oxygen concentration (FiO2) 100%, respiratory rate (RR) 20 times/min (ideal body mass 70 kg), and full analgesic, sedative, and muscle relaxation. Fluid correction, acid, and vasoactive drugs were used to increase pressure, control ventricular rate, and manage volume. Imipenem and cilastatin were combined with acyclovir for anti-infection. Methylprednisolone was administered at 40 mg every 12 hours, and pirfenidone was given at 200 mg tid to treat pulmonary interstitial fibrosis. Acetyl cysteine effervescent tablet 0.6g bid),phlegm-relieving asthma; correcting electrolyte metabolism disorder and hypoproteinemia; improving immunity (intravenous injection of human immunoglobulin 10g qd*2 days, subcutaneous injection of thymoxin 1.6mg ih qd).
Phase 1 Awfully Deep Day 1 (D1)
D1 Adjusted ventilator parameters as described above after admission, progressive deterioration of oxygenation, blood gas: pH 7.25,pCO2 45.2mmHg,pO2 37.2mmHg,Lac 8.6mmol/L,HCO3-17.6mmol /L,BE 7.5mmol/L,A-aDO2 505.4mmHg; Pulmonary protective ventilation strategy was implemented (prone position, VT 5.7mL/kg, Flow 1L/S,PEEP 10cmH2O,Peak 25cmH2O,Pplat 20cmH2O,Raw 5,rP 10cmH2O,Crs 40L/cmH2O,SpO2 68%,Chest radiographs showed exudative changes in both lungs and bilateral pleural effusion (Figure 1).
 |
Figure 1 Chest CT before treatment. |
Phase 2 Twists and Turns D1-D14
D1 At 2:00 p.m., veno-venous extracorporeal membrane oxygenation (VV-ECMO) treatment was initiated, involving percutaneous puncture with a 19-French (Fr). Cannula for left and right femoral vein drainage and a 17-Fr cannula for right internal jugular vein reflux. The treatment parameters are as follows: The speed was set at 3120 RPM, the flow at 3.5 liters per minute, the ventilation at 3 liters per minute, and the FiO2 at 100%. The ECMO was functioning optimally. Concurrently, heparin was administered with an anticoagulant agent. The activated whole blood coagulation time (ACT) was monitored at 4-hour intervals to ensure its maintenance at 180–240 seconds. The patient exhibited gradual improvement in oxygenation after 1 hour on ECMO. However, after 2 hours of VV-ECMO, oxygenation remained suboptimal, and the partial pressure difference of alveolar artery oxygen was elevated. Consequently, CRRT was initiated. On the first day, the overall balance was −2112mL, and norepinephrine was reduced from 0.26 to 0.13ug/kg-min. On the second day, alveolar lavage fluid was collected and sent to NGS, and bright red, purulent sputum was observed in the lung under bronchoscopy. Given the patient’s history of repeated hormone use, caspofungin was added to the original Tenone combined with acyclovir.
D3 The patient exhibited recurrent fever and chills, accompanied by a substantial increase in the infection index. The catheter-related infection did not resolve, and the patient received vancomycin in accordance with the original anti-infection prescription. Additionally, the patient exhibited brown urine, a decrease in hemoglobin and platelets, and a subsequent adjustment in ECMO speed and discontinuation of anticoagulation therapy.
D4 In the morning, the eyes directed their gaze upward, and the muscle tone of the limbs increased. The patient was considered to be at risk of seizure. The antibiotic treatment was changed from imipenem and cilastatin to meropenem, and the patient was given anti-epileptic treatment. At 11:00 p.m., the patient’s oxygen saturation (SpO2) decreased from 90% to 75%, and the patient’s partial pressure of oxygen (PO2) decreased from 55 mmHg. The patient also had pneumopulmonary thrombosis, extracorporeal membrane oxygenation (ECMO) was initiated, and pneumopulmonary replacement was initiated.
D6 Alveolar lavage fluid NGS return: Streptococcus pneumoniae sequence number 13, candida albicans sequence number 1924; Virus-related test results were negative. Acyclovir was discontinued and meropenem was downgraded to cefoperazone and sulbactam sodium.
D10 Etiology review and GGM test showed no fungus, so stop carpofungin and give fluconazole.
D13-D14 The patient’s fever resurgence prompted the collection of etiological samples, the exclusion of carbapenem-resistant Acinetobacter baumannii infection, and the administration of minocycline. The anti-infection regimen prior to these adjustments comprised Suprozon, minocycline, vancomycin, and fluconazole.
Following the diagnosis and treatment of D1-D14, a strict pulmonary protective ventilation strategy was implemented, resulting in fluctuations in the static lung compliance wave between 29–45, PO2 fluctuations between 71–85.7 mmHg, and an increase in the transparency of both lungs, a decrease in the B-line of both lungs, and the appearance of the A-line (see Figure 2). Analgesic sedation muscle relaxation: from deep sedation and muscle relaxation to shallow sedation, and then transition to prevention of delirium; Circulatory system: strict volume management, maintain negative fluid balance, reduce D8 vasoactive drugs; Digestive system: The dose of enteral nutrition should be gradually increased, and TP-HE with higher energy should be selected, as it is suitable for cancer patients. With regard to extracorporeal membrane oxygenation (ECMO), the D14 deventilator test was passed and awake VV-ECMO was initiated after repeatedly considering the advantages and disadvantages of awake VV-ECMO.
 |
Figure 2 (A) From left to right, the ultrasound changes in the right lung were observed between November 10 and November 20. (B) From left to right are the changes in the left lung ultrasound between November 10 and November 20. |
The Third Stage Dispel the Clouds and See the Sun D14-D29
On the 14th day of treatment, the patient was supported by VV-ECMO (at a speed of 3700 RPM, with a flow of 4.8 L/min, ventilation of 3.5 L/min, and an FiO2 of 21%), HNFO (with an FiO2 of 40%, a flow of 60 L/min), The patient exhibited respiratory rate fluctuations between 13 and 20 times per minute. Blood gas analysis revealed a pH of 7.41, a pCO2 of 43 mmHg, a pO2 of 87 mmHg, a lactate level of 2.3 mmol/L, and an A-aDO2 of 144 mmHg.
D15 Sputum culture pre-report: G-bacillus, Supraxen upgraded to Meping; post-admission blood cultures were negative, vancomycin was discontinued, sputum smear showed no fungal spores or mycelium, GGM test was negative, and antifungal treatment was stopped for 14 days.
D16 Sputum culture: hydrocarbase-resistant enfec, pneumogenic FEc, taminol, plus amikacin, that is, mepin combined with amikacin.
D17 Initiate bedside respiratory muscle and diaphragm function exercise. There was a significant decrease in the amount of sputum, an increase in the transparency of the chest film, and the presence of an A line on lung superscan. Rheumatism and immunity-related tests were negative. However, extracorporeal membrane oxygenation (ECMO) is challenging to wean off. Following a repeated review of data, the diagnosis was immune checkpoint inhibitor-related pneumonia. Methylprednisolone 500 mg qd 3 d impact therapy was administered; D18 Blood culture results: carbapenem resistant enterococci bacteria - Feimke, according to drug sensitivity to continue mepine combined with amikacin anti-infection;
D21 Evacuate ECMO and give oxygen to HNFO and mask;
D26 Oxygen was given through nasal catheter and mask;
D28 Nasal tube oxygen.
Following diagnosis and treatment with D14-D29, the patient exhibited fluctuations in respiratory system PO2, ranging from 48–77.6 mmHg prior to the removal of ECMO. Chest radiographs revealed an enhancement in lung transparency, while lung overshot demonstrated line A (refer to Figure 3). Subsequent to the removal of ECMO, PO2 fluctuated within the range of 53–80.6 mmHg. CT imaging revealed that the extent of infection in both lungs had diminished compared to the initial admission, and the right pleural effusion had been absorbed. Infection side: no fever, infection index decreased gradually;
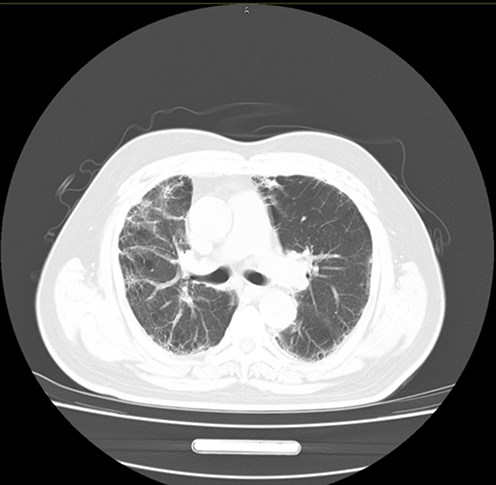 |
Figure 3 Post-treatment chest CT. |
The following is the patient’s hormone dosing regimen: Methylprednisolone: D17-19 500mg/day; D20-22 250mg/day; D23-25 160mg/day; D26-28 80mg/day; D29 40mg/day; Subsequently, reduce 5mg per week until discontinued.
D29 Discharged from hospital.
The patient was discharged with the following diagnoses: acute respiratory failure, severe pneumonia, ARDS (acute respiratory distress syndrome), immune checkpoint inhibitor-related pneumonia, septic shock, metabolic acidosis, heart failure, arrhythmia, atrial fibrillation, atrial premature beat, pulmonary malignancy, postoperative pulmonary interstitial fibrosis, hypertension (grade 3, very high risk), hypertensive heart disease, hypoproteinemia, moderate anemia, electrolyte imbalance, metabolic disorder, hyponatremia, and lower limb venous thrombosis (Table 1).
 |
Table 1 Indicators of Patients Before and After ECMO |
Discharge Doctor’s Advice
Pay close attention to rest, strengthen nutrition, and enhance lung function, respiratory muscle, and limb function rehabilitation exercise, while taking measures to avoid infection. The patient should receive long-term home oxygen therapy (3–4L/min). The patient should take 0.6g/q1. The patient should be advised to prioritize rest, prioritize adequate nutrition, and engage in rehabilitation exercises to strengthen lung and limb function, in addition to avoiding infection. Long-term home oxygen therapy is recommended at a rate of 3–4 liters per minute. The patient should be advised to take 0.6 grams of the IVIG treatment on the 18th of December 2023.
For the treatment of anti-pulmonary interstitial fibrosis, the patient should be prescribed a regimen of pirfenidone capsules at a dosage of 600 milligrams, three times per day, and acetylcysteine effervescent tablets at a dosage of 0.6 grams, twice per day. The tablets should be taken warm.
For the treatment of kinin, the patient should be prescribed a regimen of prednisone acetate tablets at a dosage of 40 milligrams, eight tablets, which should be reduced by 5 milligrams, one tablet, every Saturday until the reduction is stopped. To protect the gastric mucosa, esomeprazole magnesium enteric-coated capsule 20mg (1 tablet) is administered once a day. A calcium supplement, dicocal calcium 1 tablet/day, is also recommended, but it should be discontinued simultaneously with hormones. To control ventricular rate, betaloc 25mg is prescribed three times a day. For atrial fibrillation and lower limb venous thrombosis, rivaroxaban 20mg is administered once a day (taken with food). To improve immunity, thymosin enteric-coated capsule is recommended. The patient was administered a dosage of 10 milligrams, three times per day. Following a substantial improvement in his condition, he was referred to the respiratory department for ongoing evaluation and treatment of a lung malignancy. This involved a comprehensive review of chest CT scans and blood vessel ultrasounds of both lower limbs.
Discussion
The mortality rate associated with ICIP is high,3 and the treatment difficulty is significantly increased after the combination of ARDS, with no improvement in the patient’s oxygen levels after the setting of PEEP with the PEEP/FiO2 tableStudies have shown that, in actual clinical work, the PEEP value of moderate to severe ARDS patients is lower than the theoretical value.4 However, compared with low PEEP, high PEEP did not improve clinical outcomes or reduce mortality.5 Furthermore, elevated driving pressure has been identified as an independent predictor of mortality in patients with ARDS.6 Currently, there is a lack of a definitive guideline on how to enhance alveolar compliance while ensuring oxygenation and hemodynamic stability.7 Given the absence of a significant difference in prognosis when compared with an oxygenation-oriented approach, the simple, rapid, and minimally invasive approach is predominantly favored in clinical practice: the calculation of driving pressure (ΔP).8 Furthermore, a comparative analysis of the P-V curve and ΔP was conducted by Chengfen Yin et al, revealing that the latter significantly reduces the duration of hospital stay.9 Consequently, pulmonary protective ventilation strategies for ARDS were rigorously implemented before and after VV-ECMO, encompassing adequate positive end-expiratory pressure (PEEP) and regulated ΔP at approximately 15 cmH2O.10
This case study has provided a comprehensive understanding of the indications and parameter settings for VV-ECMO, as outlined in the guide and will not be reiterated here.11 The study has also emphasized the necessity of personalized anticoagulation therapy, recommending the selection of different anticoagulant drugs for distinct patients, primarily heparin, bivaludin, and agatrol.12 However, it is imperative to acknowledge that the anticoagulation process inherently carries the risk of bleeding and thrombosis, necessitating adjustments to the anticoagulation program based on the underlying etiology.13 Furthermore, infection constitutes a prevalent complication in ECMO patients, with an increased incidence of infection observed as the operation time prolongs. Among patients receiving ECMO treatment, the incidence of nosocomial infection reaches up to 50%, with bloodstream infection being the most prevalent infection site. As demonstrated by relevant studies, the reported incidence of bloodstream infection during VV-ECMO was 16.56 times per 1000 ECMO days.14,15 The following list enumerates the pathogenic bacteria associated with bloodstream infection during VV-ECMO:Respiratory tract: Staphylococcus aureus, Pseudomonas, Klebsiella, etc. These bacteria are similar to other VAP bacteria in the ICU. Blood flow: Coagulase-negative Staphylococcus, yeast, Enterococcus, Staphylococcus aureus, and Klebsiella were the most prevalent. In the urinary tract, yeast, Escherichia coli, and Enterococcus were more common.16,17 When a bloodstream infection is suspected or confirmed, early administration of antibiotics is recommended, and anti-infection protocols are developed in conjunction with local bacteriology. The possibility of infective endocarditis should be actively evaluated.18 Linezolid exhibits reduced efficacy in the treatment of bloodstream infections when compared with vancomycin; however, it demonstrates superiority in the penetration of lung epithelial fluid.19 With regard to adverse reactions, the incidence of decreased blood platelets caused by linezolid is comparatively high, while the incidence of kidney damage and rash caused by vancomycin is also high.20 Additionally, linezolid intravenous and oral formulations are readily interchangeable. The patient received vancomycin and exhibited no adverse reactions. A comprehensive review of the diagnostic and therapeutic process was conducted, encompassing the stages of analgesia and sedation during ECMO, including pre-boarding, catheterization, transfer, and withdrawal. The selection of appropriate drugs should be informed by factors such as drug protein binding rate, lipophilicity, and adsorption in the ECMO loop.21
In instances where oxygenation remains unimproved following anti-infection treatment in accordance with the results of etiological drug sensitivity testing, the consideration of non-infectious diseases becomes imperative. These non-infectious diseases are primarily classified into three categories: air cavity/pulmonary parenchymal diseases, pulmonary vascular diseases, and pulmonary interstitial diseases. Among the latter, those accompanied by fever primarily include: For connective tissue-associated interstitial lung disease, idiopathic pulmonary fibrosis, and acute interstitial pneumonia, the patient’s rheumato-immune-related tests were all negative. After a repeated review of the data, the patient was definitively diagnosed as immune-checkpoint inhibitor-related pneumonia, and the diagnosis and treatment were based on the expert consensus on the diagnosis and treatment of immune-checkpoint inhibitor-related pneumonia.2
The patient exhibited capacity overload, which has the potential to result in prolonged mechanical ventilation and intensive care unit (ICU) stay, and increased mortality.22 Therefore, it is of great importance to take measures to reduce fluid accumulation in the lung interstitium and alveolar cavity, on the basis of stable cardiac, liver, and renal functions. The early administration of diuretics has been demonstrated to reduce the 28-day mortality of patients with acute respiratory distress syndrome (ARDS).23,24 Consequently, the patient was administered continuous renal replacement therapy (CRRT) on the day of admission, with a subsequent daily infusion of furosemide and a static vein pump to address volume management. A subsequent evaluation of the patient’s lung ultrasound revealed a gradual decrease in the B-line of both lungs, a gradual emergence of the A-line, and a concomitant improvement in oxygenation.
The severity of the disease and long-term bed rest caused the patient’s ICU acquired weakness, but there is still no effective treatment. Through early active respiratory function exercise, we improved the patient’s respiratory status and the strength and endurance of the respiratory muscle, shortened the mechanical ventilation time, achieved awake ECMO, and avoided the occurrence of ventilators related pneumonia. Promote the communication between patients and the outside world, and strengthen their medical adherence.25,26
In summary, for patients with immune checkpoint inhibitor-related pneumonia complicated with severe ARDS caused by PD-1 monoclonal antibody after pulmonary malignant tumor surgery, the implementation of lung protective ventilation strategies, the selection of appropriate timing for VV-ECMO, and the rapid treatment of related complications are beneficial to patient recovery. Post-evaluation of awake VV-ECMO, identification of non-infectious diseases with interstitial lesions with fever and pulmonary shadow as the first symptom, intervention capacity with diuretics, and early initiation of bedside rehabilitation are beneficial to patient recovery.
Consent Statement
Written informed consent for publication of their details was obtained from the patient. The patient has signed a written informed consent form allowing the release of case details and any accompanying images and agency approval is not required to release case details.
Acknowledgment
We would like exhibit honest perception to the reviewers for essential remarks regarding this article.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4(12):1721–1728. doi:10.1001/jamaoncol.2018.3923
2. Lung Cancer Group. Society of respiratory medicine, Chinese medical association. Expert consensus on diagnosis and treatment of pneumonia associated with immune checkpoint inhibitors. Chin J Tubercu Respir. 2019;42(11):820–825. in Chinese.
3. Altan M, Soto F, Zhong LL, et al. Incidence and risk factors for pneumonitis associated with checkpoint inhibitors in advanced non-small cell lung cancer: a single center experience. Oncologist. 2023;28(11):e1065–e1074. doi:10.1093/oncolo/oyad118
4. Brown NJ. Incorrect language and list in the supplement. JAMA. 2016;316(3):350. doi:10.1001/jama.2016.6956
5. Sahetya SK. Searching for the optimal positive end-expiratory pressure for lung protective ventilation. Curr Opin Crit Care. 2020;26(1):53–58. doi:10.1097/MCC.0000000000000685
6. He S, Leng W, Du X, et al. Diagnostic significance of heart-type fatty acid-binding protein as a potential biomarker to predict the mortality rate of patients with sepsis: a systematic review and meta-analysis. Expert Rev mol Diagn. 2022;221–8.
7. Hess DR. Recruitment maneuvers and PEEP titration. Respir Care. 2015;60(11):1688–1704. doi:10.4187/respcare.04409
8. Rezaiguia-Delclaux S, L R, Gruner A, et al. Oxygenation versus driving pressure for determining the best positive end-expiratory pressure in acute respiratory distress syndrome. Crit Care. 2022;26(1):214. doi:10.1186/s13054-022-04084-z
9. Individualized positive end expiratory pressure setting source perfusion 267659120946728.PDF>. 2020.
10. Amato MB, Meade MO, Slutsky AS, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747–755. doi:10.1056/NEJMsa1410639
11. Tonna JE, Abrams D, Brodie D, et al. Management of adult patients supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021;67(6):601–610. doi:10.1097/MAT.0000000000001432
12. Levy JH, Staudinger T, Steiner ME. How to manage anticoagulation during extracorporeal membrane oxygenation. Intensive Care Med. 2022;48(8):1076–1079. doi:10.1007/s00134-022-06723-z
13. Thomas J, Kostousov V, Teruya J. Bleeding and thrombotic complications in the use of extracorporeal membrane oxygenation. Semin Thromb Hemost. 2018;44(1):20–29. doi:10.1055/s-0037-1606179
14. Corley A, Lye I, Lavana JD, et al. Nosocomial infection prevalence in patients undergoing extracorporeal membrane oxygenation (ECMO): protocol for a point prevalence study across Australia and New Zealand. BMJ Open. 2019;9(7):e029293. doi:10.1136/bmjopen-2019-029293
15. Menaker J, Galvagno S, Rabinowitz R, et al. Epidemiology of blood stream infection in adult extracorporeal membrane oxygenation patients: a cohort study. Heart Lung. 2019;48(3):236–239. doi:10.1016/j.hrtlng.2019.01.004
16. Allou N, Lo Pinto H, Persichini R, et al. Cannula-related infection in patients supported by peripheral ECMO: clinical and microbiological characteristics. Asaio J. 2019;65(2):180–186. doi:10.1097/MAT.0000000000000771
17. Kim HS, Park S, Ko HH, et al. Different characteristics of bloodstream infection during venoarterial and venovenous extracorporeal membrane oxygenation in adult patients. Sci Rep. 2021;11(1):9498. doi:10.1038/s41598-021-89108-4
18. Tong HJ, Deng HS, Peng W, et al. Expert consensus on infection prevention and control during extracorporeal membrane oxygenation in adults. Chin J Circ. 2024;39(03):209–216.
19. Conte JE, Golden JA, Mcquitty M, et al. Effects of gender, AIDS, and acetylator status on intrapulmonary concentrations of isoniazid. Antimicrob Agents Chemother. 2002;46(8):2358–2364. doi:10.1128/AAC.46.8.2358-2364.2002
20. Li J. Clinical efficacy and safety analysis of linezolid, Teicolanin and vancomycin in the treatment of nosocomial methicillin-resistant Staphylococcus aureus (MRSA) pneumonia. Strait Pharm. 2018;30(01):187–188.
21. Crow J, Lindsley J, Cho SM, et al. Analgosedation in critically Ill adults receiving extracorporeal membrane oxygenation support. ASAIO J. 2022;68(12):1419–1427. doi:10.1097/MAT.0000000000001758
22. Vignon P, Evrard B, Asfar P, et al. Fluid administration and monitoring in ARDS: which management?. Intensive Care Med. 2020;46(12):2252–2264. doi:10.1007/s00134-020-06310-0
23. Seitz KP, Caldwell ES, Hough CL. Fluid management in ARDS: an evaluation of current practice and the association between early diuretic use and hospital mortality. J Intensive Care. 2020;8:78. doi:10.1186/s40560-020-00496-7
24. Zhang R, Chen H, Gao Z, et al. The effect of loop diuretics on 28-day mortality in patients with acute respiratory distress syndrome. Front Med Lausanne. 2021;8:740675. doi:10.3389/fmed.2021.740675
25. Mendez-Tellez PA, Needham DM. Early physical rehabilitation in the ICU and ventilator liberation. Respir Care. 2012;57(10):1663–1669. doi:10.4187/respcare.01931
26. Pohlman MC, Schweickert WD, Pohlman AS, et al. Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Crit Care Med. 2010;38(11):2089–2094. doi:10.1097/CCM.0b013e3181f270c3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.