Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
External ventricular drainage combined with continuous lumbar drainage in the treatment of ventricular hemorrhage
Authors Xia D ![]() , Jiang X, Li Z, Jin Y
, Jiang X, Li Z, Jin Y ![]() , Dai Y
, Dai Y
Received 6 March 2019
Accepted for publication 30 April 2019
Published 30 May 2019 Volume 2019:15 Pages 677—682
DOI https://doi.org/10.2147/TCRM.S207750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Dayong Xia,1 Xiaochun Jiang,1 Zhenbao Li,1 Yuelong Jin,2 Yi Dai1
1Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical College, Wuhu 241000, Anhui Province, People’s Republic of China; 2School of Public Health, Wannan Medical College, Wuhu 241000, Anhui Province, People’s Republic of China
Objective: Intraventricular hemorrhage (IVH) is characterized by acute onset, rapid progression, and high disability and mortality rates. In this study, we investigated the clinical effect of external ventricular drainage combined with continuous lumbar drainage in IVH treatments.
Methods: 114 patients with IVH treated at the Department of Neurosurgery, First Affiliated Hospital of Wannan Medical College from January 2015 to December 2017, were included in the study. Based on the different surgical methods, patients were divided into control (n=79) and study groups (n=35). The control group was treated with external ventricular drainage, whereas the study group was treated with external ventricular drainage combined with continuous lumbar drainage. The incidence of intracranial infection and hydrocephalus was compared between the two groups. The Glasgow coma scale (GCS) and the Glasgow outcome scale (GOS) were compared between the two groups 7 days postoperatively and at follow-up visits, respectively.
Results: The incidence of intracranial infection and hydrocephalus in the study group was significantly lower compared with those in the control group (P<0.05). Seven days postoperatively, the GCS score of the study group was significantly higher than that of the control group (P<0.05). At the 3-month follow-up visit, the GOS score of the study group was higher than that of the control group (P<0.05).
Conclusions: Using external ventricular drainage combined with continuous lumbar drainage can reduce the incidence of intracranial infection and hydrocephalus and improve the prognoses and quality of life in patients with IVH.
Keywords: intraventricular hemorrhage, external ventricular drainage, continuous lumbar drainage, intracranial infection, hydrocephalus
Introduction
Intraventricular hemorrhage (IVH) is one of the most common acute and critical disorders in the department of neurosurgery and is most prevalent in middle-aged and older people. IVH can be divided into primary intraventricular hemorrhage (PIVH) and secondary intraventricular hemorrhage (SIVH). The causes of IVH include ruptured vascular lesions such as aneurysms and vascular malformations in the ventricular choroid plexus and the intraventricular and ventricular walls. Due to the complex etiologies and rapid progression caused by IVH, high disabilities and mortalities are seen if not treated promptly. Studies have shown that 10–15% of all stroke patients have IVH,1 and the 30-day mortality rate after onset is as high as 35–50%.2 The main clinical symptoms of IVH are intracranial hypertension and meningeal irritation caused by abnormal cerebrospinal fluid circulation.3,4 Therefore, timely and effective removal of ventricular hematomas and early cerebrospinal fluid circulation recovery are the key points of IVH treatment. This study retrospectively investigated the efficacy of using external ventricular drainage combined with continuous lumbar drainage by comparing external ventricular drainage alone vs external ventricular drainage combined with continuous lumbar drainage for the treatment of IVH. This study strives to provide an alternative method for the future treatment of IVH.
Materials and methods
Research subjects
One hundred and fourteen patients with IVH treated at the Department of Neurosurgery, First Affiliated Hospital of Wannan Medical College from January 2015 to December 2017, were included in this study. All patients were confirmed to have IVH using cranial computed tomography (CT) scans at the time of admission. Patients with the following characteristics were excluded: cranial CT scans that showed mainly parenchymal hemorrhage, supratentorial hematoma volumes that were ≥30 mL, subtentorial hematoma volumes that were ≥l0 mL, and patients that required surgical interventions. The patients and their relatives were well informed of the surgical options and their expected outcomes and complications. Based on their choices and the surgical methods, patients were divided into two groups, the control group and the study group.
The control group consisted of 79 patients, including 45 males and 34 females with ages that ranged from 26 to 85 years old (mean, 56.30±14.62 years old). 28 patients are regular smokers and 30 are regular alcoholics. The Glasgow coma scale (GCS) at admission was 3–5 in 26 patients, 6–8 in 26 patients, and 9–15 in 27 patients. The study group consisted of 35 patients, including 13 males and 22 females with ages that ranged from 29 to 72 years old (mean, 54.74±11.35 years old). 11 patients are regular smokers and 14 are regular alcoholics. The GCS at admission was 3–5 in 9 patients, 6–8 in 14 patients, and 9–15 in 12 patients. The amount of IVH is compared between the two groups according to the standard of Graeb score. The control group scores range from 3 to 12 (mean, 7.90±1.58) and the study group scores range from 4 to 12 (mean, 7.74±1.87). No statistically significant differences between the two groups regarding gender, age,GCS scores,and Graeb scores at admission were seen (P>0.05).
Research methods
1) The external ventricular drain was placed through the frontal horn of the lateral ventricle under general anesthesia. The burr hole was 2–2.5 cm in front of the coronal suture and 2–3 cm from the middle line. The puncture direction was parallel to the sagittal plane and perpendicular to the hypothetical line connecting the external auditory meatus. A puncture was created with an 18 G drainage catheter possessing a needle core. The needle core was retracted when bloody cerebrospinal fluid flowed out, and the drainage catheter was advanced another 1–2 cm. The scalp was then sutured, and the internal drainage tube was fixed and connected to the external drainage tube.5 After the surgery, the drainage tube was elevated and placed 10–15 cm above the level of external auditory canals, and drainage was maintained unobstructed. The characteristics of the cerebrospinal fluid were observed, while CSF flow was controlled at about 200–250 mL per 24 hrs. For patients with drainage of cast hemorrhages or clotted blood, 1–20,000 U of urokinase was diluted in 5 mL saline and slowly injected into the lateral ventricles; then, the drainage tube was closed for 1–2 hrs.6 The color of the lumbar drain fluid changes with time from being bloody to being light yellow and to being clear. Depending on the color and volume of the drained fluid, this process was repeated once or twice daily for 2–3 consecutive days. Postoperative cranial CT scans were examined, and cerebrospinal fluid was regularly taken for biochemical and routine testing. The drainage tube was closed for 24 hrs when most of the intraventricular hematoma was removed, the third and fourth ventricles were unobstructed, and no signs of an intracranial infection could be seen. The external ventricular drainage tube was removed if the ventricles were not dilated on cranial CT scans. Patients were followed for 3months after discharge.
2) The study group underwent external ventricular drainage combined with continuous lumbar drainage, and insertion of the external ventricular drain was performed similarly to that of the control group. The lumbar drainage was carried out 24–48 hrs after the ventricular drains were placed. Patients were set in the position for lumbar anesthesia, and routine disinfection and draping were performed. The puncture point was at the L3-L4 or L4-L5 disc space.7 After cerebrospinal fluid flowed out, the drainage tube was placed in the lumbar cistern. The lumbar drainage tube was sutured on the back and extended to the shoulder. The drainage tube was connected to a three-way valve and a drainage bag. The height of the drainage tube was adjusted depending on the flow rate and the height of cerebrospinal fluid water column. Cerebrospinal fluid was regularly taken for biochemical and routine tests if the lumbar drainage flow was smooth and sufficient. Cranial CT scans were performed to assess the IVH status. The external ventricular drainage tube was removed when most of the IVH was cleared, the third and fourth ventricles were unobstructed, and ventricular enlargements were no longer observed. The lumbar drainage was maintained until the IVH disappeared. The lumbar drainage tube was removed when cerebrospinal fluid circulation was smooth, the cerebrospinal fluid white blood cell numbers were normal, and the protein content was almost normal. Both groups received routine supportive treatments to control blood pressure, nourish brain nerves and cells, protect the stomach by inhibiting gastric acid secretion, and prevent vasospasms.
Assessments
The incidence of intracranial infection and hydrocephalus between the two groups was compared. The treatment efficacy was evaluated by comparing GCS scores before surgery and 7 days postoperatively within and between the two groups. Patients were followed for 3 months after discharge, and the Glasgow outcome scale (GOS) was used to evaluate patient neurologic recovery. The rating criteria are indicated in Table 1.
 | Table 1 Glasgow outcome scale |
Statistical analyses
SPSS18.0 software was used for statistical analyses. Measurement data were expressed as the mean ± the SD, and the paired t-test was used for the comparisons within the groups. Two independent sample t-tests were used for the comparisons between the groups. Counting data were expressed as a percentage (%) and compared with the x2 test. Results were considered statistically significant with a P<0.05.
Results
Demographic data were compared between the two groups and showed no significant differences in gender or age between the study and the control groups (P>0.05) (Table 2). GCS scores were compared before surgery and 7 days postoperatively between the two groups and showed no significant differences in the GCS scores at admission (8.09±2.74 vs 7.62±3.42) (P>0.05). The GCS scores of both groups 7 days postoperatively were higher (11.80±4.62 and 9.19±5.47) compared with those at admission (8.09±2.74 and 7.62±3.42, respectively), and the difference was statistically significant (P<0.05). The GCS scores 7 days postoperatively in the study group were higher compared with those in the control group, and the difference was statistically significant (P<0.05) (Table 3). The duration that the external ventricular drainage tube was placed with the control group ranges from 6 to16 days (9.48±2.75) and the duration that the external ventricular drainage tube was placed with the study group ranges from 3 to12 days (5.66±1.81). There is a statistically significant difference between the two groups (P<0.05). The incidence of intracranial infection and hydrocephalus between the two groups was compared. We found that in the study group, the incidences (2.9% and 5.7%) were significantly lower than those in the control group (19.0% and 21.5%), and the differences were statistically significant (P<0.05) (Table 4). GOS scores were compared at follow-up visits and 3-month postdrainage between the two groups. The GOS score of the study group was higher (3.49±1.38) compared with that of the control group (2.89±1.41), and the difference was statistically significant (P<0.05) (Table 5).
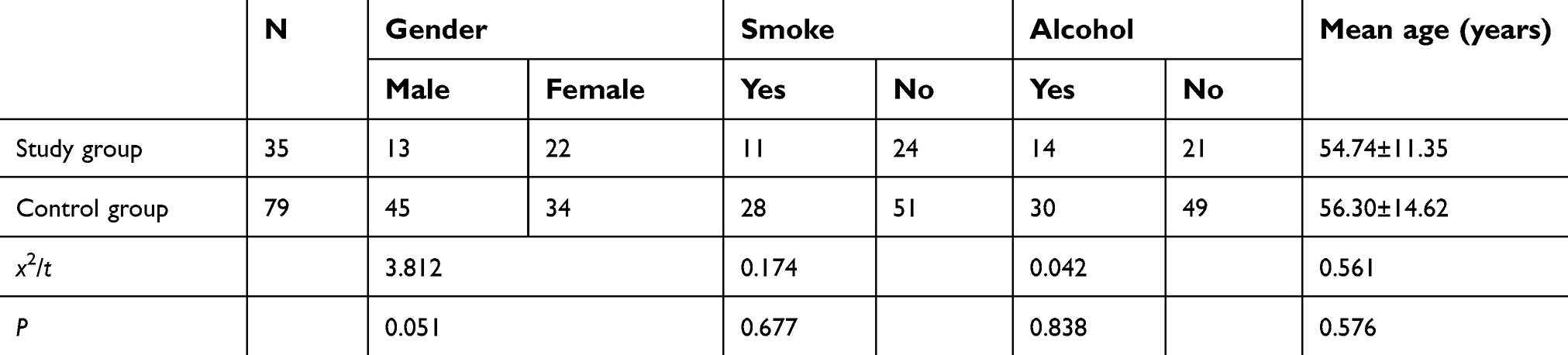 | Table 2 Demographic data were compared between the two groups |
 | Table 3 GCS scores were compared before surgery and 7 days postoperatively between the two groups |
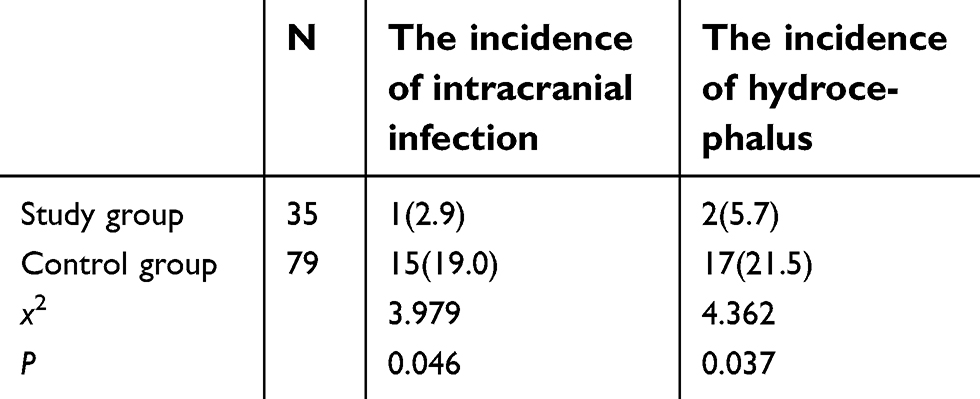 | Table 4 The incidence of intracranial infection and hydrocephalus between the two groups, n (%) |
 | Table 5 GOS scores were compared at follow-up visits and 3-month postdrainage between the two groups |
Discussion
IVH usually has an acute onset and progresses rapidly.8 Blood entering the ventricles rapidly solidifies or even forms casts, which causes disorders in cerebrospinal fluid circulation and absorption by blocking the foreman of Monro or the aqueducts.9–11 Disease outcomes include acute obstructive hydrocephalus, sudden increases in intracranial pressure, cerebral vasospasm, and compression of the periventricular tissues, which result in poor patient prognoses.12–14 Therefore, timely and effective removal of ventricular hematomas and the early recovery of cerebrospinal fluid circulation are vital in reducing secondary brain injuries and improving prognoses and survival rates. At present, the surgical options for IVH include craniotomy, external ventricular drainage, neuroendoscopic surgeries, and continuous lumbar drainage.13,15,16
This study aimed to investigate the efficacy of external ventricular drainage combined with continuous lumbar drainage in the treatment of IVH. At present, external ventricular drainage is widely used for these treatments.17 This simple operation can effectively lower intracranial pressure and remove ventricular hematomas. However, using this surgical option alone has disadvantages such as long drainage times, increased ventricular infection rates, and drainage of clotted blood in the third and fourth ventricles and the subarachnoid spaces.18,19 In contrast, external ventricular drainage combined with continuous lumbar drainage is effective in removing blood and can shorten the duration of drainage catheter placements. Meanwhile, continuous lumbar drainage can effectively drain blood in the subarachnoid spaces and the third and the fourth ventricles to decrease clotting.7,20 Thus, hematomas are cleaned more effectively, and the risk of leakage from cerebrospinal fluid incisions and the rates of ventricular infection and hydrocephalus are reduced, which is consistent with the results of this study.
In this study, we showed that the incidence of intracranial infection and hydrocephalus was lower in the study group compared with the control group. The GCS scores of the study group were higher compared with those of the control group 7 days postoperatively. And, the GOS scores of the study group 3 months after discharge were significantly higher than those of the control group. All differences were statistically significant (P<0.05). This study demonstrates that external ventricular drainage combined with continuous lumbar drainage can significantly reduce the rates of ventricular infection and hydrocephalus and can improve treatment efficacies and the long-term quality of life in patients with IVH.
Conclusions
In summary, early intervention using external ventricular drainage combined with continuous lumbar drainage is practical and effective at improving cerebrospinal fluid circulation, reducing secondary brain injuries, and improving the quality of life of patients with IVH.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College. All patients provided written informed consent.
Acknowledgments
This study was supported by the Natural Science Research Project in Higher Education of Anhui Province (No. KJ2018A0253) and the Science Research Project of Professional Personnel of the First Affiliated Hospital of Wannan Medical College (No. YR201911).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hwang JH, Han JW, Park KB, Lee CH, Park IS, Jung J-M. Stereotactic multiplanar reformatted computed tomography-guided catheter placement and thrombolysis of spontaneous intracerebral hematomas. J Korean Neurosurg Soc. 2008;44:185–189. doi:10.3340/jkns.2008.44.4.185
2. Caceres JA, Goldstein JN. Intracranial hemorrhage. Emerg Med Clin North Am. 2012;30:771–794. doi:10.1016/j.emc.2012.06.003
3. Webb AJ, Ullman NL, Morgan TC, et al. Accuracy of the ABC/2 score for intracerebral hemorrhage: systematic review and analysis of MISTIE, CLEAR-IVH, and CLEAR III. Stroke. 2015;46:2470–2476. doi:10.1161/STROKEAHA.114.007343
4. Murthy SB, Awad I, Harnof S, et al. Permanent CSF shunting after intraventricular hemorrhage in the CLEAR III trial. Neurology. 2017;89:355–362. doi:10.1212/WNL.0000000000004155
5. Morita T, Maki Y, Yamada D, Ishibashi R, Chin M, Yamagata S. External ventricular drainage preceding the removal of a nail from the intracranial space as a safe management strategy for predicted secondary intraventricular hemorrhage. World Neurosurg. 2017;106:1056 e1059–1056 e1013. doi:10.1016/j.wneu.2017.07.104
6. Fu C, Liu L, Chen B, et al. Risk factors for poor outcome in hypertensive intraventricular hemorrhage treated by external ventricular drainage with intraventricular fibrinolysis. World Neurosurg. 2017;102:240–245. doi:10.1016/j.wneu.2017.03.029
7. Staykov D, Kuramatsu JB, Bardutzky J, et al. Efficacy and safety of combined intraventricular fibrinolysis with lumbar drainage for prevention of permanent shunt dependency after intracerebral hemorrhage with severe ventricular involvement: A randomized trial and individual patient data meta-analysis. Ann Neurol. 2017;81:93–103. doi:10.1002/ana.24834
8. Gilard V, Chadie A, Ferracci FX, et al. Post hemorrhagic hydrocephalus and neurodevelopmental outcomes in a context of neonatal intraventricular hemorrhage: an institutional experience in 122 preterm children. BMC Pediatr. 2018;18:288. doi:10.1186/s12887-018-0993-2
9. Li Q, Huang YJ, Zhang G, et al. Intraventricular hemorrhage and early hematoma expansion in patients with intracerebral hemorrhage. Sci Rep. 2015;5:11357. doi:10.1038/srep11357
10. Romero JM, Brouwers HB, Lu J, et al. Prospective validation of the computed tomographic angiography spot sign score for intracerebral hemorrhage. Stroke. 2013;44:3097–3102. doi:10.1161/STROKEAHA.113.002752
11. Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol. 2012;11:307–314. doi:10.1016/S1474-4422(12)70038-8
12. Del Giudice A, D’Amico D, Sobesky J, Wellwood I. Accuracy of the spot sign on computed tomography angiography as a predictor of haematoma enlargement after acute spontaneous intracerebral haemorrhage: a systematic review. Cerebrovasc Dis. 2014;37:268–276. doi:10.1159/000360754
13. Dowlatshahi D, Brouwers HB, Demchuk AM, et al. Predicting intracerebral hemorrhage growth with the spot sign: the effect of onset-to-scan time. Stroke. 2016;47:695–700. doi:10.1161/STROKEAHA.115.012012
14. Sprigg N, Flaherty K, Appleton JP, et al. Tranexamic acid for hyperacute primary intracerebral haemorrhage (TICH-2): an international randomised, placebo-controlled, phase 3 superiority trial. Lancet. 2018;391:2107–2115. doi:10.1016/S0140-6736(18)31033-X
15. Ovesen C, Jakobsen JC, Gluud C, et al. Prevention of haematoma progression by tranexamic acid in intracerebral haemorrhage patients with and without spot sign on admission scan: a statistical analysis plan of a pre-specified sub-study of the TICH-2 trial. BMC Res Notes. 2018;11:379. doi:10.1186/s13104-018-3481-8
16. Brouwers HB, Falcone GJ, McNamara KA, et al. CTA spot sign predicts hematoma expansion in patients with delayed presentation after intracerebral hemorrhage. Neurocrit Care. 2012;17:421–428. doi:10.1007/s12028-012-9765-2
17. Dey M, Jaffe J, Stadnik A, Awad IA. External ventricular drainage for intraventricular hemorrhage. Curr Neurol Neurosci Rep. 2012;12:24–33. doi:10.1007/s11910-011-0231-x
18. Ayubi E, Safiri S. Risk factors for poor outcome in hypertensive intraventricular hemorrhage treated by external ventricular drainage with intraventricular fibrinolysis: statistical and methodologic issues. World Neurosurg. 2017;104:1018. doi:10.1016/j.wneu.2017.04.044
19. Johnson JR, Idris Z, Abdullah JM, Alias A, Haspani MS. Prevalence of shunt dependency and clinical outcome in patients with massive intraventricular haemorrhage treated with endoscopic washout and external ventricular drainage. Malays J Med Sci. 2017;24:40–46. doi:10.21315/mjms2017.24.1.5
20. Staykov D, Huttner HB, Struffert T, et al. Intraventricular fibrinolysis and lumbar drainage for ventricular hemorrhage. Stroke. 2009;40:3275–3280. doi:10.1161/STROKEAHA.109.551945
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.