Back to Journals » International Medical Case Reports Journal » Volume 18
Extensive Inactive Neurocysticercosis: A Case Report in Mbeya, Southern Highlands of Tanzania
Authors Makasi CE ![]() , Ngowi BJ, Stelzle D, Kilale AM, Mahande MJ
, Ngowi BJ, Stelzle D, Kilale AM, Mahande MJ ![]() , Welte TM, Winkler AS, Mmbaga BT
, Welte TM, Winkler AS, Mmbaga BT ![]()
Received 25 July 2024
Accepted for publication 11 December 2024
Published 17 January 2025 Volume 2025:18 Pages 117—124
DOI https://doi.org/10.2147/IMCRJ.S488096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Charles Elias Makasi,1,2 Bernard James Ngowi,3 Dominik Stelzle,4 Andrew Martin Kilale,1 Michael Johnson Mahande,2,5 Tamara Margarete Welte,4 Andrea Sylvia Winkler,4,6 Blandina Theophil Mmbaga2,7
1National Institute for Medical Research, Muhimbili Medical Research Centre, Dar Es Salaam, Tanzania; 2Kilimanjaro Christian Medical University College of Tumaini University, Moshi, Tanzania; 3University of Dar Es Salaam, Mbeya College of Health and Allied Sciences, Mbeya, Tanzania; 4Department of Neurology and Center for Global Health, School of Medicine and Health, Technical University Munich, Munich, Germany; 5Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania; 6Department of Community Medicine and Global Health, Institute of Health and Society, University of Oslo, Oslo, Norway; 7Kilimanjaro Clinical Research Institute, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
Correspondence: Charles Elias Makasi, Email [email protected]
Background: Neurocysticercosis (NCC) and Acquired Human Immunodeficiency Syndrome (AIDS) are both highly prevalent in Africa. Clinical presentation of NCC ranges from asymptomatic to manifestations, including epileptic seizures, severe progressive headache, and focal neurological deficits. It is influenced by the number, size, location, and stage of the cysts, as well as the parasite’s potential to cause inflammation and the immunological response of the host. So far, little is known about how Human Immunodeficiency Virus (HIV) co-infection modifies clinical NCC presentation. We report the case of a person living with HIV presenting with extensive calcified NCC on neuroimaging without any associated signs/ symptoms.
Purpose: To contribute to the medical literature and enhance understanding of the disease’s manifestation and progression by providing a thorough documentation of a specific case of extensive inactive neurocysticercosis.
Case Presentation: A 47-year-old male African patient was recruited in the CYSTINET Africa study at Chunya District Hospital, Mbeya. He was an artisan and has been living with HIV since 2012, and he has been compliant with antiretroviral treatment, hence with undetectable viral load during 2018, 2020, and 2021. Taenia solium serology was done by LDBIO Cysticercosis IgG Western Blot test, which tested positive for antibodies, but the apDia Cysticercosis Antigen (Ag) ELISA antigen test was negative. His computed tomography (CT) scan of the brain showed approximately 138 calcified neurocysticercosis typical lesions, 108 being located in the parenchyma, 15 in the extra parenchyma, and 15 in the subarachnoid space, consistent with a diagnosis of extensive calcified NCC. He reported no history of headaches or epileptic seizures. Neurological examination did not reveal any deficit.
Conclusion: Intensively, patients with a large number of neurocysticercosis lesions may be completely asymptomatic throughout the disease. In our patient,the HIV co-infection might have contributed to the high lesion load and/or to less severe clinical signs/symptoms due to modulation of the immune system.
Plain Language Summary: An important parasite that is spread between people and pigs is the pork tapeworm. The larvae from tapeworm infections that settle in the brain are known as neurocysticercosis (NCC) and have been found to infect approximately 17 out of every 100 individuals in areas of Tanzania, where the pork tapeworm is present. There has been the assumption that NCC is more prevalent in the areas of Tanzania with a higher burden of Human Immunodeficiency Virus (HIV)/Acquired Immunodeficiency Syndrome (AIDS). The neurological signs/symptoms of NCC depend on the number, size, location, and stage of the larvae as well as the host’s immune system and the parasite’s strength to cause inflammation. Whether an HIV co-infection affects the clinical presentation of NCC is still poorly understood. We describe a case of an HIV-positive individual who showed a large number of calcified larvae from the pork tapeworm on his brain scan but without neurological manifestations. Through this comprehensive account of a particular patient with widespread inactive larvae from the pork tapeworm, we hope to add to the knowledge of why some patients with NCC and not others develop neurological manifestations.
Keywords: case study, calcified neurocysticercosis, HIV, CYSTINET Africa, Taenia solium
Introduction
Taenia solium, the pork tapeworm, can cause two different diseases in humans: taeniasis and cysticercosis. If humans eat undercooked cyst-infested pork, they may develop a tapeworm in the intestines (taeniasis). If eggs of the tapeworm are ingested, larvae (cysticerci) may settle in tissues (cysticercosis). If they settle in the central nervous system, the disease is known as neurocysticercosis (NCC).1 The period between infection with Taenia solium and clinical manifestation, as well as the clinical presentation itself, depends on the immunological response of the host, the virulence of the parasite, and the number, size, location, and stage of the cysts.2 Neurocysticercosis may present with viable, degenerating, or calcified lesions in cerebral imaging. The first two are considered active stages, and the last (calcified) is considered an inactive stage.3 The evolvement of cysts from the active to the inactive stage may occur spontaneously, which can take several years. This process can also be induced by antiparasitic medication, eg, albendazole or praziquantel.4,5 Most patients become symptomatic when cysts degenerate, but calcified lesions can also cause persistent signs/symptoms.
Epileptic seizures, severe progressive headaches, focal neurological deficits, and mental state alterations are the most common CNS signs/symptoms.6 Neurocysticercosis is associated with about 30% of acquired, preventable epilepsy in Taenia solium highly endemic areas.7,8 However, there is insufficient information on which proportion of NCC patients will develop signs/symptoms, and with multiple lesions may remain asymptomatic.9,10 In contrast, some individuals with low cyst loads are highly symptomatic and develop permanent sequelae, especially recurrent seizures, chronic headaches, or focal neurological deficits.9,11 The variation in the manifestation of neurocysticercosis poses a challenge in the diagnosis since multiple parameters are needed to establish the degree of diagnostic certainty. Computed tomography (CT) scan and magnetic resonance imaging (MRI) are pillars for diagnosis of NCC but should ideally be supported by serological testing as suggested by the Del Brutto criteria.12 Both, neuroimaging and serological testing, are obstacles to diagnosis, especially in low-income settings where neuroimaging (CT scan and MRI) and serological services are often not affordable to affected people as they commonly have a low socio-economic status.13
It has been observed that areas with a high HIV prevalence are also highly endemic to Taenia solium infection, although the evidence of this interaction is not well supported.7 Some individuals with neuro/cysticercosis and HIV co-infection react poorly to serological tests and others with higher cyst load become asymptomatic, especially in advanced stages of HIV.14 Thus, it is postulated that HIV might modulate presenting features of neuro/cysticercosis depending on the levels of the host’s immunity.15
We report a case study detailing the unusual manifestations of neurocysticercosis in a person living with HIV, and contrast this with typical patients uninfected with HIV.
Case Presentation
We present a case of extensive calcified neurocysticercosis in an asymptomatic 47-year-old male living with HIV. The patient was recruited through the CYSTINET-Africa study in January 2021. In this study, people living with HIV (PLHIV) attending HIV Care and Treatment Centers (CTC) clinics in Chunya and Tossamaganga (southern highlands of Tanzania) were offered serological testing for T. solium cysticercosis. If results were positive (but also for a subset of serological negatives), patients were offered a CT scan. For every PLHIV, also an HIV-negative control (matched by age, sex, and location of residence) was recruited to compare the accuracy of the serological test and NCC disease presentation between HIV-positive and negative persons. The patient we presented was recruited through the HIV care and treatment center clinic in Chunya.
In 2012, he was diagnosed with HIV. His CD4 count at diagnosis was 31 cells per cubic millimeter of blood, and he was categorized as in WHO stage II. Immediately after diagnosis and complete medical assessment, he was started on antiretroviral therapy consisting of Azidothymidine (AZT) + Lamivudine (3TC) + Efavirenz (EFZ) on the 3rd April 2012. In 2017, he was changed to another ARV drug combination ie, started on a new drug combination consisting of Tenofovir disoproxil fumarate (TDF) +3TC+EFZ; this was due to the changes in the national guidelines in the first-line ARV treatment. Six months after the initiation (TDF +3TC+EFZ) combination, his viral load was undetectable. On the 5th of August 2019, his antiretroviral treatment regime was again changed into Tenofovir disoproxil fumarate (TDF) + Lamivudine (3TC) + DTG (Dolutegravir) to avoid different side effects experienced from the regime he was using. His viral load was undetectable and remained undetectable in all subsequent viral load tests in 2018, 2020, and 2021 (Table 1).
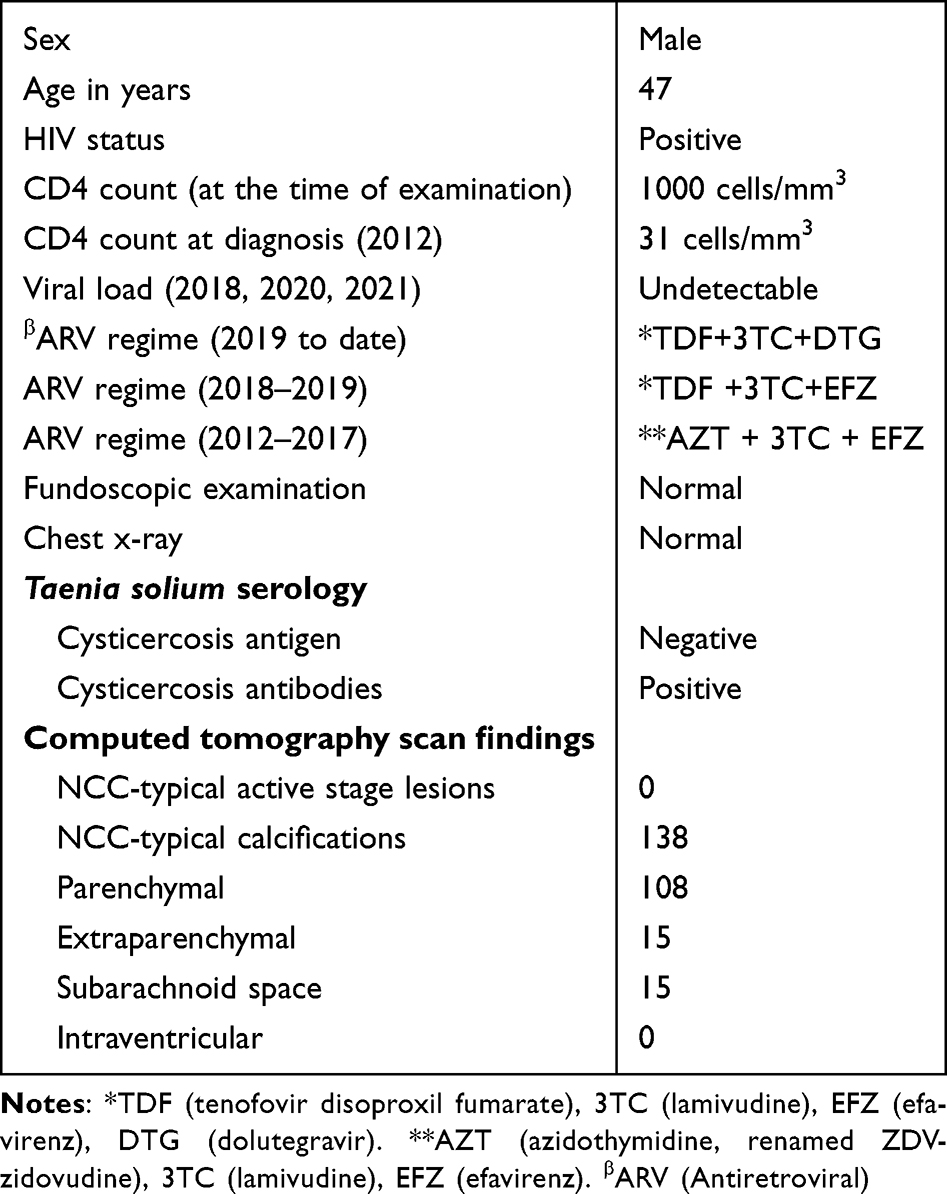 |
Table 1 Summarized patient's clinical, antiretroviral treatmetreatment, and neuroimaging informationn |
Serological testing for T. solium was positive for cysticercosis antibodies using the LDBIO Cysticercosis IgG Western Blot test, but negative for cysticercosis antigen by the apDia Cysticercosis Antigen (Ag) ELISA test. The cerebral CT scan examination was performed at Mbeya consultant hospital on 5 November 2021. The patient was examined neurologically on the day of the CT scan, and an in-depth history was taken.
Personal History, Risk Factors, and History of the Risk Factors for the Taenia Solium Infection
This patient has been an artisanal miner (small-scale gold mining worker) since 2010, with a history of keeping pigs from 2009 to 2019. He has been married with 4 children; screening of the family members for T. solium infection was done, and the patient denied anyone in the family having neurological signs and symptoms of NCC (ie severe progressive headache and epileptic seizures). The patient reported known risk factors for T. solium infection, such as eating pork and never boiling water. He reported always using the pit latrine at his home and regular handwashing after the toilet and before eating.
Medical History of Taenia Solium Infection and Neurological Examination
The patient denied having experienced any loss of consciousnessor involuntary movements of limbs or having been diagnosed with epilepsy. Any episodes of severe progressive headache, mental state alterations, or other signs/symptoms that could be associated with NCC (or taeniasis) were also denied. The overall physical examination was normal, the patient looked healthy, not pale, not jaundiced and there were no palpable nodules (head/neck, trunk, and extremities). The examination did not reveal any focal neurological deficit.
Fundoscopic Examination
The patient’s red reflex was normal, blood vessels were normal, and macular reflex was normal. The optic nerve and disc appeared normal, vitreous body, and choroid. No floaters were detected.
Chest X-Ray Examinations
Cardiac shadow was normal in size and configuration, and both lung fields and costophrenic angles were clear. No focal pulmonary lesion was seen with the intact bony thorax. Therefore, the chest radiograph was classified as normal.
Computerized Tomographic (CT) Scan Examination of the Brain
Technique
Continuous axial cuts were obtained through the skull with intravenous contrast. Multiple calcifications typical for neurocysticercosis were seen in the cerebral parenchyma, basal ganglia, and cerebellum (Figures 1–3). Bilateral orbital calcifications and calcifications involving the skin, soft palate, oropharynx, and skull base soft tissue were noted. No midline shift was observed. The features were suggestive of diffuse inyracranial and extracranial calcifications.
 |
Figure 1 (A) Multiple NCC-typical calcifications were found in the cerebral parenchyma. (B) Calcification is also found in the cerebellum. |
 |
Figure 2 (A) In addition to multiple NCC typical calcifications in the cerebral parenchyma, there are also two calcifications in the orbitae. (B) Calcification involving the skin, soft palate, oropharynx, and skull base soft tissue are seen. |
 |
Figure 3 (A and B) Multiple NCC typical calcifications are noted throughout the brain parenchyma including the basal ganglia. |
Impression
Features were suggestive of diffuse intracranial and extracranial calcification.
Discussion
We present a case of extensive calcified neurocysticercosis in a patient living with HIV. Despite a massive lesion load, he had never experienced any typical symptoms associated with neurocysticercosis (NCC). It is well known that the manifestations of NCC vary concerning the location, size, number of cysts, virulence of the agent, and immunity of the host.16 Calcified NCC has been associated with migraine in several studies, but this patient did not complain of any kind of headache.17,18 Little is known about how HIV co-infection modifies clinical NCC presentation. It is hypothesized that HIV co-infection might contribute to a high lesion load and/or to less severe clinical signs/symptoms due to modulation of the immune system since the presence or absence of signs/symptoms largely depends on the host’s inflammatory response. Moreover, serological tests can be affected if the patient is immune-compromised.19,20 This is speculated to be one of the reasons for asymptomatic neurocysticercosis in some individuals with advanced HIV. Calcified lesions captured by neuroimaging in people living with HIV are hard to define due to the possibility of mass lesions secondary to other opportunistic infections like toxoplasmosis and tuberculosis. Cysticercosis serological tests are also relatively affected by the host’s immune. In a highly compromised immunity, such as with very low CD4 counts, there is a likelihood of a negative cysticercosis serological test.20 These possibilities might explain the asymptomatic neurocysticercosis in this patient, irrespective of the extensive calcific lesions.
Extensive Calcific Lesions Without Any Clinical Manifestations
Although the patient has a very large number of lesions, he had never had any neurological signs or signs/symptoms. The calcified stage of T. solium cysts is an inactive form and the end stage of the degeneration process. The fully developed initial viable stages (vesicular stage) then degenerate into the colloidal and granular stages and end in the calcified (inactive) stage. Whilst most patients are symptomatic in degenerative stages, they can also be symptomatic in the viable and calcified stages. Although possible, it is uncommon for patients to develop signs/symptoms for the first time in the calcified stage if they were asymptomatic in viable and degenerative stages.21 Studies show that patients with only calcified lesions are often not as symptomatic as before reaching the calcified stage.22 The Infectious Disease Society of America (IDSA) and the American Society of Tropical Medicine & Hygiene (ASHTM) guidelines recommend a gradual withdrawal of seizure suppressant medication in patients with epileptic seizures six months after the establishment of calcifications or resolution of all lesions if patients do not present with epileptic seizures anymore.23 Some patients with the inactive calcified NCC lesions may be free from any neurological signs/symptoms, but some of them are left with persistent sequelae, especially epileptic seizures, focal neurological deficits, or other manifestations of neurological deficits.24
The lack of any clinical manifestations in this patient evidences the symptomatic variability of neuro/cysticercosis. Extensive lesions have been observed previously among immunosuppressed individuals, and this has led to the hypothesis that immunosuppression secondary to HIV might modify the clinical presentation of neuro/cysticercosis. Other case studies have presented differing uncommon clinical manifestations related to HIV immunosuppression including Immune Reconstitution Inflammatory Syndrome (IRIS) for those who were recently initiated with antiretroviral (ARV) drugs.25 One case report described a 4-year-old Tanzanian child living with HIV and presenting with disseminated cysticercosis as well as a case of disseminated NCC in the contexts of IRIS after initiation of antiretroviral treament.26 There is a paucity of reliable information on the possible association between HIV and outcomes of T. solium, including the posited relationship with neurocysticercosis. Case reports are not well suited to address this, and more robust epidemiological study designs, with sufficient sample sizes are needed.7
Conclusion
Neurological signs/symptoms vary considerably in patients with NCC and some patients remain asymptomatic. The more NCC lesions patients have, the more likely they are to have neurological signs/symptoms. However, some patients with few lesions are highly symptomatic, and others with many disseminated lesions may not show any neurological signs/symptoms. Whether HIV alters the presentation of NCC in terms of neurological signs/symptoms or radiological characteristics is plausible, but this still needs to be evaluated reliably.
Abbreviation
3TC, Lamivudine; AIDS, Acquired Immunodeficiency Syndrome; ARV, Antiretroviral; AZT, Azidothymidine, renamed ZDV-zidovudine; CC, Cysticercosis; CD4, Cluster of differentiation 4; DTG, Dolutegravir; CNS, Central nervous system; CT, Computed tomography; EFZ, Efavirenz; HIV, Human immunodeficiency virus; IRIS, Immune Reconstitution Inflammatory Syndrome; MRI, Magnetic resonance imaging; NCC, Neurocysticercosis; PLHIV, person/people living with HIV; TDF, Tenofovir disoproxil fumarate; WHO, World Health Organization.
Ethics Approval and Consent to Participate
Ethical clearance for conducting this study was granted by all participating institutions in Tanzania. These included the Kilimanjaro Christian Medical College Research Ethics and Review Committee (CRERC); Certificate No 2450. National Health Research Ethics Committee (NatHREC) under the National Institute for Medical Research (NIMR) (Reference No. NIMR/HQ/R.8a/Vol. IX/2529). This was followed by a request for permission for study conduct from other appropriate authorities, including regional and district health authorities. Health facility in-charges were also asked for permission for a research permit. Individual written Informed consent was obtained from all the participants involved in the study.
The publication of this Case report is covered by the above-mentioned two approvals from the NatHREC and CRERCC provided that the study participant gives individual consent for this purpose. Therefore, the participant gave individual consent for publication.
Consent for Publication
The patient consented to participate in the CYSTINET Africa study and also consented to his data and any accompanying images to be published in this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Acknowledgments
The study was fully funded by the German Federal Ministry of Education and Research under Tanzania II contract number 81203616 of CYSTINET-Africa project number 01KA1618. The funder played no role in the design and conduct of the study or the interpretation of the results. I would like to express my deepest appreciation to the Kilimanjaro Christian Medical University College; for registering me to pursue my PhD at the institute and to all CYSTINET-Africa members and staff at Chunya District Hospital for caring for this patient reported in this publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or, in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work” has been replaced by the existing paragraph at the section of the author’s contribution.
Funding
The research project was funded by the Bundesministerium für Bildung und Forschung (Germany Federal Ministry of Education and Research) (BMBF), under the Cysticercosis Network of Sub-Saharan Africa (CYSTINET-Africa).
Disclosure
We confirm that all authors of this article have no conflicts of interest to declare.
References
1. Rodrigues A, Neves D, Maury I, Sargento D, Pereira A. A classic neurocysticercosis case with an unusual complication. Eur J Case Rep Intern Med. 2018;5(1):000762. doi:10.12890/2017_000762
2. Gonzales I, Rivera JT, Garcia HH. Pathogenesis of taenia solium taeniasis and cysticercosis. Parasite Immunol. 2016;38(3):136–146. doi:10.1111/pim.12307
3. Raibagkar P, Berkowitz AL. The many faces of neurocysticercosis. J Neurol Sci. 2018;390:75–76. doi:10.1016/j.jns.2018.04.018
4. Garcia HH. Antiparasitic drugs in neurocysticercosis: albendazole or praziquantel? Exp Rev Anti-Infective Ther. 2008;6(3):295–298. doi:10.1586/14787210.6.3.295
5. Monk EJM, Abba K, Ranganathan LN. Anthelmintics for people with neurocysticercosis. Cochrane Database Syst Rev. 2021;6(6):Cd000215. doi:10.1002/14651858.CD000215.pub5
6. Coyle CM. Neurocysticerosis: an individualized approach. Infect Dis Clin North Am. 2019;33(1):153–168. doi:10.1016/j.idc.2018.10.007
7. Jewell PD, Abraham A, Schmidt V, et al. Neurocysticercosis and hiv/aids co-infection: a scoping review. Tropical Med Int Health. 2021;26(10):1140–1152. doi:10.1111/tmi.13652
8. Ndimubanzi PC, Carabin H, Budke CM, et al. A systematic review of the frequency of neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis. 2010;4(11):e870. doi:10.1371/journal.pntd.0000870
9. Siddiqua T, Habeeb A. Neurocysticercosis. Saudi J Kidney Dis Transpl. 2020;31(1):254–258. doi:10.4103/1319-2442.279948
10. San-juan Orta D. clinical manifestations of neurocysticercosis. Neurologia. 2009;24(5):331–335.
11. Moyano LM, O’Neal SE, Ayvar V, et al. High prevalence of asymptomatic neurocysticercosis in an endemic rural community in Peru. PLoS Negl Trop Dis. 2016;10(12):e0005130–e0005130. doi:10.1371/journal.pntd.0005130
12. Garcia HH, Gonzalez AE, Gilman RH. Taenia solium cysticercosis and its impact in neurological disease. Clin Microbiol Rev. 2020;33(3). doi:10.1128/cmr.00085-19
13. Coyle CM, Tanowitz HB. Diagnosis and treatment of neurocysticercosis. Interdiscipl Perspect Infect Dis. 2009;2009:180742. doi:10.1155/2009/180742
14. Parija SC, Gireesh AR. A serological study of cysticercosis in patients with hiv. Rev Inst Med Trop Sao Paulo. 2009;51(4):185–189. doi:10.1590/s0036-46652009000400002
15. Herrera Vazquez O, Romo ML, Fleury A. Neurocysticercosis and hiv infection: what can we learn from the published literature? Arq Neuropsiquiatr. 2019;77(5):357–365. doi:10.1590/0004-282x20190054
16. Güngör Çağdaş D, Saeed E-A, Luís Manuel Madeira de C. Neurocysticercosis: an overview of pathology and pathogenesis. In: Saeed E-A, Abdulaziz A, Guillermo T-I, et al., editors. Taeniasis and Cycticercosis/Neurocysticercosis. Rijeka: IntechOpen; 2023. Ch. 7.
17. Pradhan S, Das A, Anand S, Deshmukh AR. Clinical characteristics of migraine in patients with calcified neurocysticercosis. Trans R Soc Trop Med Hyg. 2019;113(7):418–423. doi:10.1093/trstmh/trz018
18. Sharma K, Uniyal R, Garg RK, et al. Does calcified neurocysticercosis affect migraine characteristics and treatment responsiveness? A case-control study. Am J Trop Med Hyg. 2022;107(6):1190–1195. doi:10.4269/ajtmh.22-0335
19. Okoye AA, Picker LJ. Cd4(+) t-cell depletion in hiv infection: mechanisms of immunological failure. Immunol Rev. 2013;254(1):54–64. doi:10.1111/imr.12066
20. Anand KS, Wadhwa A, Garg J, Mahajan RK. Hiv-associated neurocysticercosis. J Int Assoc Providers AIDS Care. 2014;14(2):120–122. doi:10.1177/2325957414555232
21. Carpio A, Romo ML, Hauser WA, Kelvin EA. New understanding about the relationship among neurocysticercosis, seizures, and epilepsy. Seizure. 2021;90:123–129. doi:10.1016/j.seizure.2021.02.019
22. Bustos JA, Arroyo G, Del Brutto OH, et al. Calcified neurocysticercosis: demographic, clinical, and radiological characteristics of a large hospital-based patient cohort. Pathogens. 2024;13(1):26. doi:10.3390/pathogens13010026
23. White AC, Coyle CM, Rajshekhar V, et al. Diagnosis and treatment of neurocysticercosis: 2017 clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American society of tropical medicine and hygiene (astmh). Clin Infect Dis. 2018;66(8):1159–1163. doi:10.1093/cid/ciy157
24. Bustos JA, Coyle CM. Brain calcification because of neurocysticercosis: a vast field to be explored. Curr Opin Infect Dis. 2020;33(5):334–338. doi:10.1097/qco.0000000000000673
25. Mukherjee S, Chatterjee P, Datta S, Manna K. A case of disseminated neurocysticercosis as immune reconstitution inflammatory syndrome in an immunocompromised patient. J Health Sci Res. 2016;1(2):34–36. doi:10.18311/jhsr/2016/v1/i2/4608
26. McCormick DW, Bacha JM, El-Mallawany NK, Kovarik CL, Slone JS, Campbell LR. Disseminated cysticercosis and kaposi sarcoma in a child with hiv/aids: a case report. BMC Infect Dis. 2020;20(1):309. doi:10.1186/s12879-020-05039-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.