Back to Journals » International Journal of Women's Health » Volume 17
Exploring Theoretical Models and Frameworks Used to Explain Factors Influencing Breast Cancer Screening Participation: A Scoping Review
Authors Zheng D ![]() , Lekdamrongkul P, Gao X, Sriyuktasuth A
, Lekdamrongkul P, Gao X, Sriyuktasuth A
Received 11 July 2025
Accepted for publication 4 November 2025
Published 26 December 2025 Volume 2025:17 Pages 5639—5656
DOI https://doi.org/10.2147/IJWH.S553089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Dandan Zheng,1 Pichitra Lekdamrongkul,1 Xiaofen Gao,2 Aurawamon Sriyuktasuth1
1Faculty of Nursing, Mahidol University, Bangkok, Thailand; 2Department of Adult and Geriatric Nursing, School of Nursing, Hangzhou Medical College, Hangzhou, People’s Republic of China
Correspondence: Aurawamon Sriyuktasuth, Faculty of Nursing, Mahidol University, 2 Wanglang Road, Bangkoknoi, Bangkok, 10700, Thailand, Tel +66 24197479-80 ext 1950-1, Email [email protected]
Objective: The purpose of this study was to explore theoretical models and frameworks used to guide research studies that explain factors influencing participation in breast cancer screening (BCS).
Methods: This study was conducted according to the framework developed by Arksey and O’Malley and reported in line with the PRISMA-ScR guidelines. A comprehensive search was performed across six databases: PubMed, Embase, CNKI, Scopus, EBSCO, and the Cochrane Library. Two researchers independently screened titles and abstracts. Data extraction and cross-checking were conducted on included studies, with a third researcher facilitating consensus in cases of disagreement. Extracted information included author, publication year, country, research methods, sample size, age, theoretical framework, and outcomes. A pre-designed form ensured consistency and accuracy in data extraction.
Results: A total of 70 studies were included. The studies were primarily cross-sectional (66/70, 94.29%), with the largest geographical locations being the United States (16/70, 22.86%), Iran (15/70, 21.43%), and China (9/70, 12.86%). The review identified 13 models, with Health Belief Model being the most commonly used (21/70, 30.0%), followed by Andersen’s Behavioral Model (11/70, 15.71%) and Theory of Planned Behavior (8/70, 11.43%). The Health Belief Model emerged as the most empirically supported framework across all studies, particularly effective in identifying economic barriers and trust issues within healthcare systems among low-income and low-health literacy populations. This model has also been incorporated into more comprehensive frameworks, demonstrating strong predictive power and practical applicability with additional variables. All models offer distinct strengths, but their predictive power largely depends on research contexts and target populations. These variations may result in an incomplete or unreliable understanding of factors influencing BCS behavior.
Conclusion: The findings provide a comprehensive summary of the models and frameworks employed to investigate factors influencing BCS over the past decade. These insights have significant implications for designing targeted healthcare interventions and informing policy changes to enhance global BCS participation and reduce disparities. Future refinements of these models are expected to improve their applicability and effectiveness across diverse populations and settings.
Keywords: breast cancer screening, theories, models, frameworks, factors
Introduction
Breast cancer (BC) represents the most common cancer among women in 86% of countries.1 In 2022, BC mortality was ranked fourth worldwide, as reported by the International Agency for Research on Cancer.2 Annually, around 1.7 million new cases of BC are diagnosed. Projections suggest that by 2040, this figure may increase to 3.19 million new cases each year, accompanied by an estimated 1.04 million deaths.3 Early detection and regular screening are essential for identifying cases prior to the advanced stage of disease.4,5
Existing research indicated that approximately 40% of cancer-related deaths are preventable through early screening.6 Evidence consistently shows that breast cancer screening (BCS) significantly reduces the incidence of late-stage diagnosis and associated mortality rates of BC.7–10 According to BCS, women can engage in many methods,11 including breast self-examination (BSE),12 mammography (MMG),13 clinical breast examination (CBE),14 MRI,15 and ultrasound.16 Available evidence indicates that the participation rate of women in BCS remains low worldwide.17 This low participation has been linked to multiple factors, including cultural beliefs and social norms that influence health-seeking behaviors, limited health literacy, socioeconomic constraints, and inadequate access to screening services—particularly among women in developing countries and vulnerable populations.18
To comprehend the low participation rate in BCS, it is essential to establish a theoretical framework to guide research on factors influencing BCS involvement. Therefore, theoretical models are essential for explaining and predicting the complex factors that influence individuals’ decisions to participate in BCS.18 Theoretical models, along with their “metaphoric structures”,19 provide a framework for linking observed phenomena with conceptual insights.20 These frameworks or models enable researchers to understand the relationships between variables, formulate hypotheses, interpret findings, and draw meaningful conclusions.20 Nilsen’s Taxonomy classifies different theories and models according to various dimensions of their function and application.21 This taxonomy is commonly used in health behavior research to identify which theories are more effective in explaining mechanisms of behavior change, including Process models, Determinant frameworks, Classic theories, Implementation theories, and Evaluation frameworks.22
The BCS theoretical model offers a framework for understanding and predicting factors influencing participation in BCS,23 examining personal, environmental, social, and health-related aspects. It serves as a tool for policymakers, healthcare providers, and educators to promote screening behaviors.24 Various theoretical models have been employed to address the numerous factors affecting screening participation, but challenges such as inadequate knowledge dissemination, patient willingness, and insufficient decision support hinder their implementation.25 Additionally, issues like poor local adaptation and practical application barriers further limit the success of these models.26 Despite the theoretical models proposed, their practical application often faces difficulties in feasibility and effectiveness, often due to a disconnect between theory and real-world practice. Common challenges, such as inappropriate model selection and insufficient rigor, can undermine their effectiveness.27 Although numerous theoretical models have been developed to explain BCS behavior, many fail to fully address contextual factors such as cultural norms, differences in health literacy, and socioeconomic barriers that influence participation, particularly among disadvantaged populations.
This study reviews theoretical models applied to BCS participation over the past decade. It emphasizes an integrated approach across diverse populations and healthcare systems and examines which theoretical frameworks most effective in explaining the factors influencing BCS participation rates. It also accesses their applicability, identifies, challenges in implementation, and their potential to bridge the gap between theory and practice in promoting BCS uptake.
Materials and Methods
This study is based on the scoping review framework proposed by Arksey and O’Malley,28 with procedural guidance derived from the specific methodology outlined by Canadian scholars Danielle Levac.29 Additionally, the study adheres to the PRISMA-ScR guidelines for reporting.30 To ensure transparency in the research process, the study protocol for this scoping review has been registered with the Open Science Framework (https://osf.io/gujm7/).
Identifying the Research Question
This study aims to address the following research questions:
1) Which theoretical models and frameworks have been utilized in the past decade to examine the factors influencing BCS?
2) How effective in explaining the determinants of BCS participation?
3) What are the similarities and differences among these models and frameworks in the context of BCS research?
Identifying Relevant Studies
For the search strategy of this study, we constructed the search terms based on the components of the PICO(T)/PICo framework (Table 1), focusing on the key concepts relevant to the research question: “breast cancer screening, participation, and ‘factors’”, as well as “theories/models/frameworks”. We employed free-text terms, subject headings, MeSH Terms, Boolean operators (“AND” and “OR”), and truncation to ensure a comprehensive search (Tables 2–7). The final search strategy was tested on Ovid and subsequently adapted for other databases. We searched six major electronic databases: PubMed, Embase, CNKI, Scopus, EBSCO, and the Cochrane Library, for studies published between January 1, 2014, and December 31, 2024.
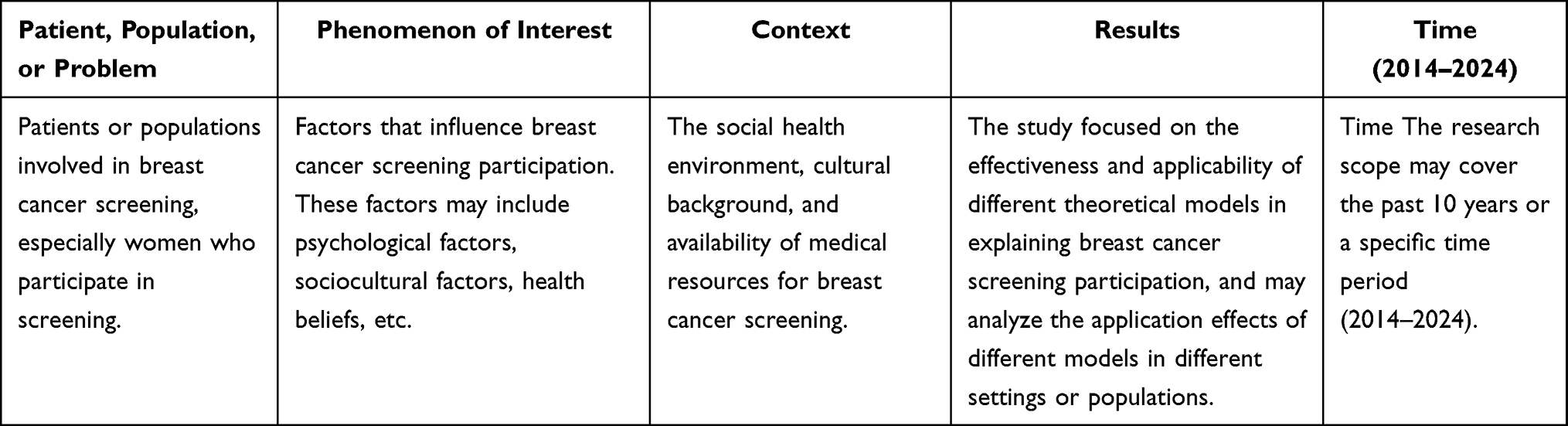 |
Table 1 Database Search Terms Using the PICO(T)/PICO Framework |
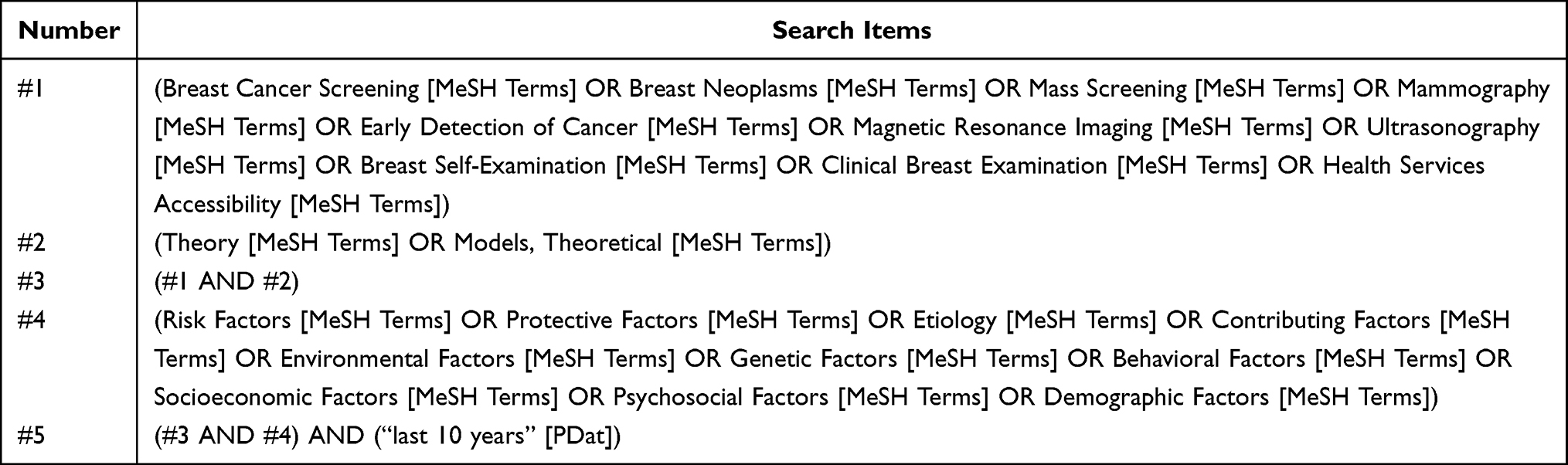 |
Table 2 Search Strategies (PubMed Database) |
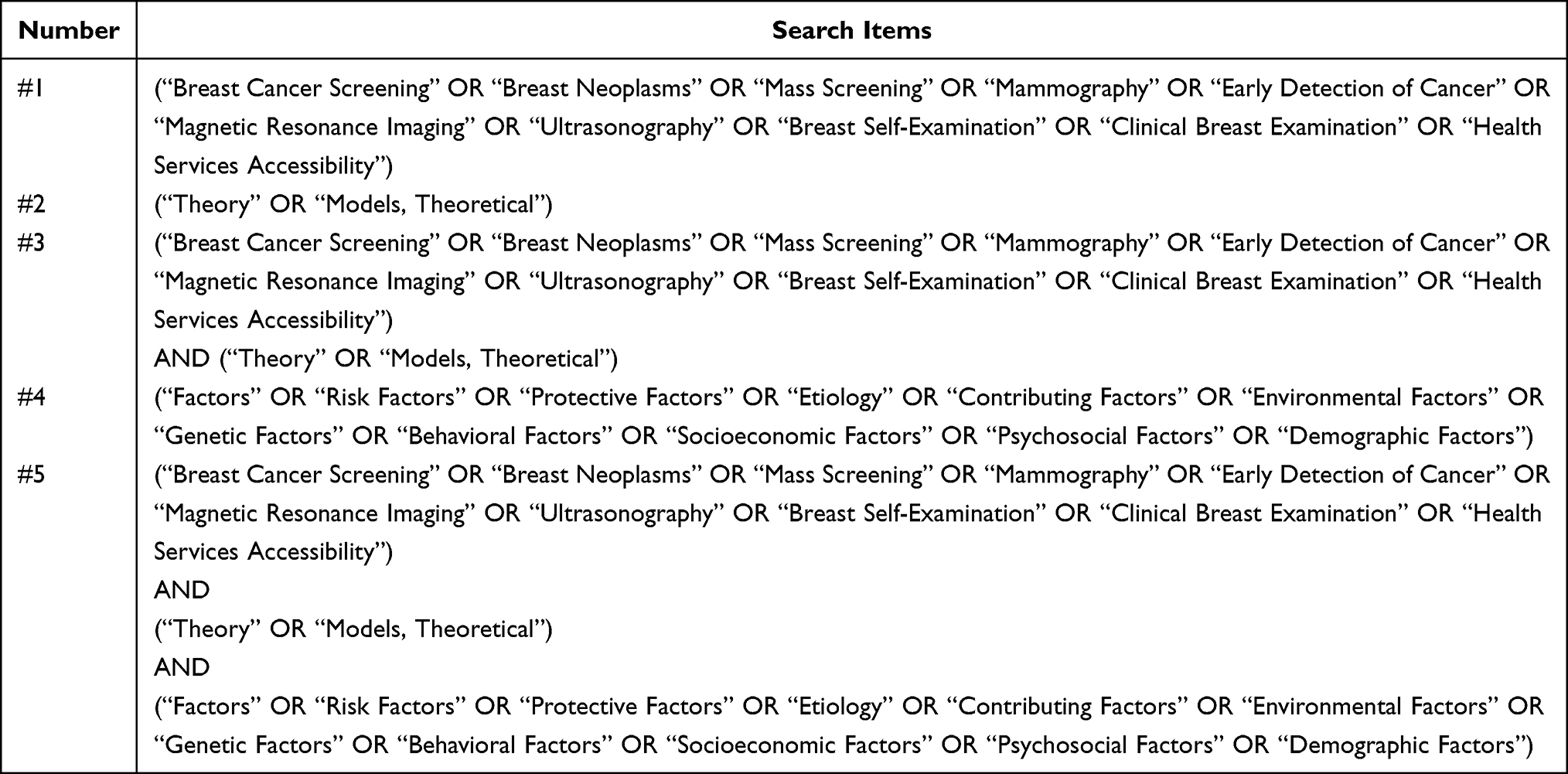 |
Table 3 Search Strategy (Cochrane Library) |
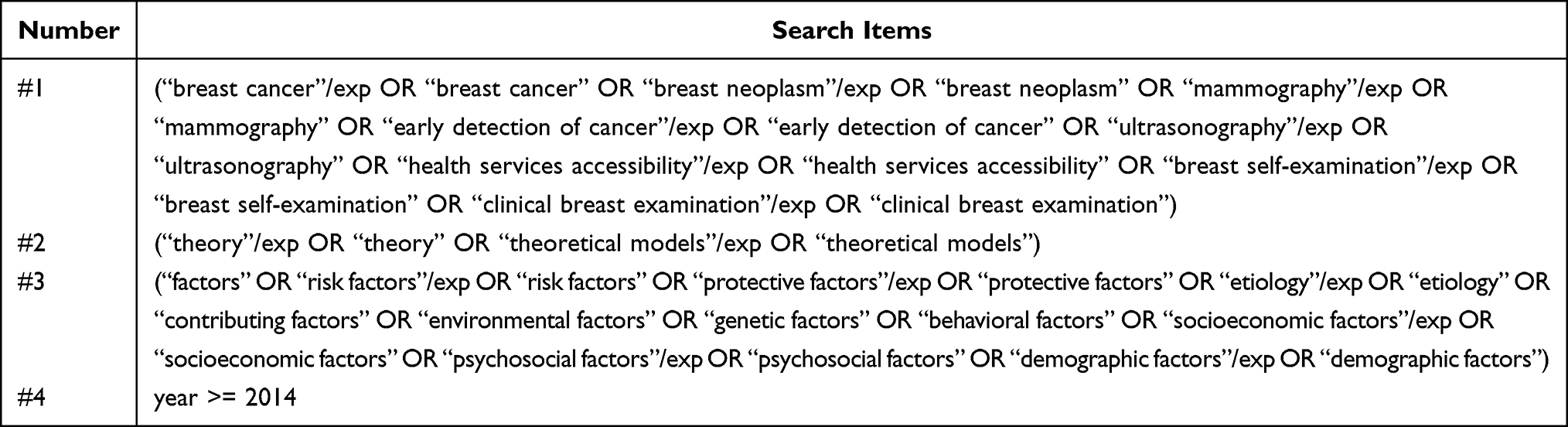 |
Table 4 Search Strategy (Embase) |
 |
Table 5 Search Strategy (CNKI) |
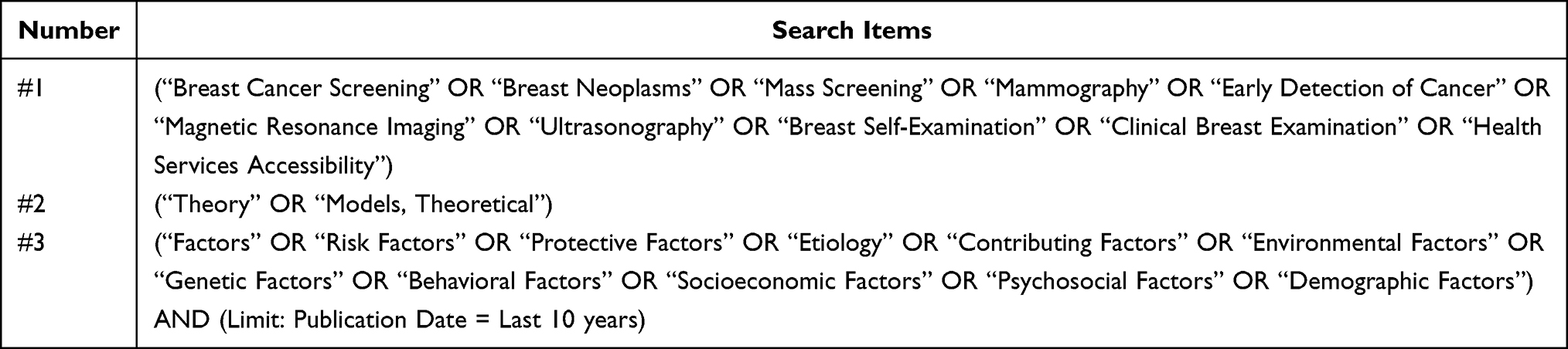 |
Table 6 Search Strategy (EBSCO) |
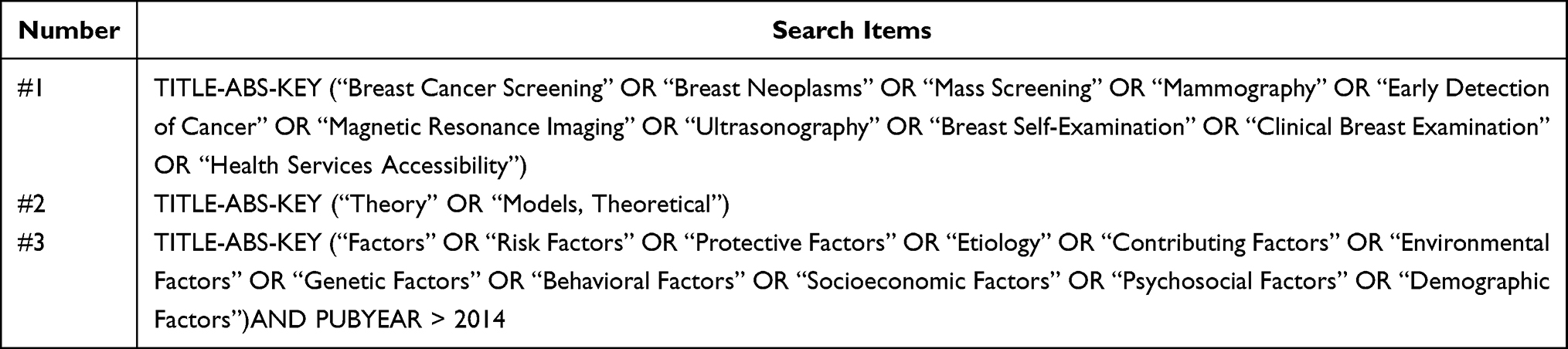 |
Table 7 Search Strategy (Scopus) |
Study Selection
Articles imported into EndNote 21 underwent independent dual screening by two researchers. Initially, titles and abstracts were assessed, followed by full-text evaluation, according to predefined inclusion and exclusion criteria. The inclusion criteria were: 1) Studies published in English or Chinese investigating factors influencing breast cancer screening, employing established theoretical models; 2) Women participants; 3) Quantitative, qualitative, or mixed-method research designs. The following studies were excluded: (1) systematic reviews, meta-analyses, review articles, case reports, expert opinions, conference proceedings, and book chapters; and (2) intervention-based research.
Charting the Data
The research team utilized a collaboratively developed data chart and table to examine the application of theories or models within the studies. Weekly meetings were held to refine, supplement, and adjust the table in order to determine which variables should be extracted to address the primary research questions. The data extraction fields were adapted from the Joanna Briggs Institute (JBI) template in the JBI Evidence Synthesis Handbook.31 The reviewers conducted a trial run and refinement of data extraction forms for 17.14% (12/70) of the included studies to ensure consistency and clarity in the extracted data. The types of theories, models, or frameworks described in the studies were classified according to the categorization system proposed by Nilsen (2015). The figures were completed using ggplot 2 in the R language.
Collating, Summarizing and Reporting the Results (Analysis)
We conducted descriptive statistics to identify the theoretical models influencing BCS, including the number of indexed publications from which data were extracted. Additionally, we reported the counts and/or frequencies and proportions of the characteristics of the theoretical models from which data were extracted. An iterative process was employed by the research team during the organization and synthesis of the results to ensure consensus was reached. The results were synthesized and reported through a narrative summary of the extracted data from all full-text publications, with graphical displays used to present the extracted information. A theme classification system was used to differentiate between the various theories, models, and frameworks related to factors influencing BCS. The similar components of each theoretical model were identified as one theme. Studies utilizing more than one theory, model, or framework were categorized as employing a “UN-category of model” approach.
Results
Study Characteristics
The database search yielded 9,633 citations. After removing duplicates, records flagged as ineligible by automated tools, and those excluded for other reasons, 1,934 citations remained for the abstract screening process. The inter-rater agreement for the title/abstract screening phase was 89%, with all discrepancies resolved through consensus. The remaining 889 studies underwent full-text review, following the same procedures as the title/abstract screening. The inter-rater agreement during the full-text screening phase was 87%. The reasons for exclusion at this stage were also recorded. A total of 70 articles passed the full-text screening and were included in this scoping review. The study selection process is illustrated in the PRISMA flowchart (Figure 1).
 |
Figure 1 PRISMA flowchart. This diagram illustrates the process of identifying and screening studies through database searches. From the initial 9,633 records, studies were ultimately selected for analysis after deduplication, screening, and eligibility assessment. |
These studies employed diverse research methods, with cross-sectional studies being the most prevalent (66/70, 94.29%), followed by qualitative studies (3/70, 4.29%) and mixed-methods study (1/70, 1.43%). Geographically, the studies were conducted in various countries worldwide, with the highest number of studies originating from the United States (16/70, 22.86%), Iran (15/70, 21.43%), and China (9/70, 12.86%). The age of participants varied, with the majority falling between 40 and 70 years old, thereby targeting predominantly middle-aged and older populations. The sample sizes varied considerably across studies, with some involving thousands of participants such as the study by Narcisse,32 with a sample size of 5,484, while others were small-scale case studies, such as Sarmah’s studies with around 22 participants.33
Research on Applying BCS Theoretical Model
The scoping review identified 13 theoretical models, each used independently as a framework to examine factors influencing BCS participation. The three most frequently used models were the Health Belief Model (HBM) (21 studies, 30.0%), followed by Andersen’s Behavioral Model (ABM) (11 studies, 15.71%), and the Theory of Planned Behavior (TPB) (8 studies, 11.43%). Additionally, some studies employed a combination of models, such as HBM and TPB, to provide a more comprehensive explanation of the factors influencing BCS participation. Details of these models are presented in Table 8.
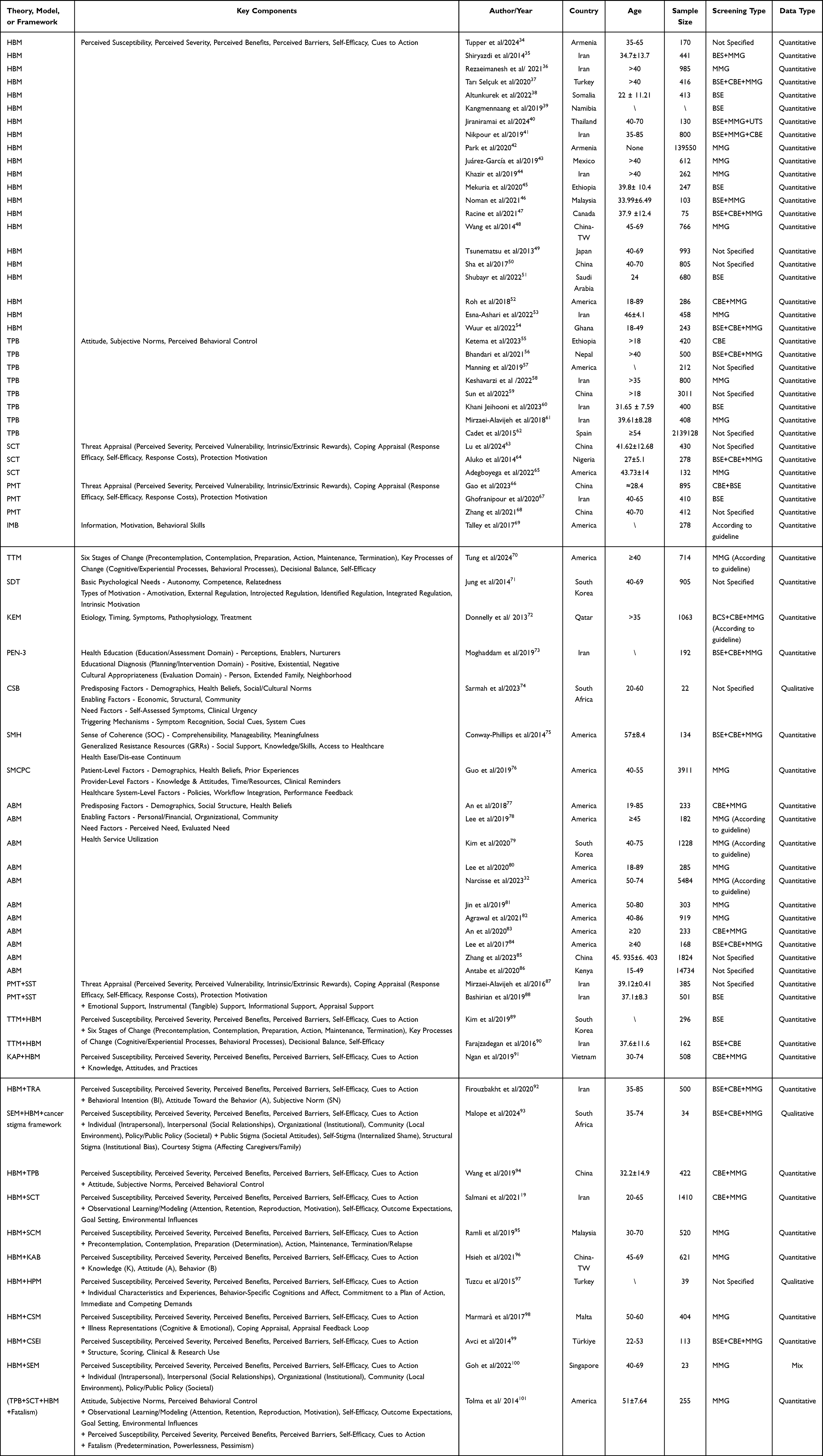 |
Table 8 Basic Characteristics of Included Studies (N = 70) |
These 13 models can be categorized into three themes based on the characteristics they address. The first theme, Behavioral and Cognitive factors, includes six models: the HBM, the TPB, the Social Cognitive Theory (SCT), the Protection Motivation Theory (PMT), the Information-Motivation-Behavioral Skills Model (IMB), and the Transtheoretical Model (TTM). The second theme, Health and Social Determinants, includes the Self-Determinant Theory (SDT), the PEN-3 Cultural Model (PEN-3), the Kleinman’s Explanatory Model (KEM), and the Theory of Care Seeking Behavior (CSB). The final theme, Systems and Contextual Factors, includes the ABM, the Salutogenic Model of Health (SMH) and the Systems Model of Clinical Preventive Care (SMCPC), which focus on the impact of healthcare delivery systems (Table 9). Although these models are categorized separately, they intersect conceptually across themes to explain their impact on health behaviors and other components related to health outcomes.
 |
Table 9 Classification According to the Theme of Theoretical Models |
Discussion
Variability in Predictive Ability of Models for BCS Behavior
Among all studies analyzing BCS factors using theoretical models. The HBM ranks first. It focuses on individual perceptions,97,102 and performs well in identifying economic barriers and health system trust issues, especially among low-income populations in urban settings of developing countries, such as India.35 However, it shows limitations in addressing perceived severity, barriers, and social/psychological factors including depression and smoking behavior.34,36–51,77,102–104 ABM’s key advantage is identifying health insurance and cultural beliefs factors,32,53,54 emphasizing regular checkups and health education.82,86 However, psychological factors is limited.32,50,53,54,78–80,82,84–86 TPB effectively captures the influence of attitudes and subjective norms.81 But its predictive power for actual behavior is limited in complex social contexts.55–60,83,87,105 PMT lacks support for emotional factors such as fear and requires further cross-cultural validation, particularly in African and Southeast Asian cohorts, where fear responses vary due to local stigma.59,62,66,101 SCT integrates multidimensional factors to explain screening decisions, though it overlooks the role of cultural/social support.63,67,68 The PEN-3 model highlights beliefs and family support,64 studies reported higher screening rates among women with a history of breast disease.65 The KEM model emphasizes physician recommendations, health status and cancer prevention beliefs, while barriers include fear and lack of recommendations.73 The IMB model identifies barriers,72 such as lack of information, behavioral skills, and practical issues such as financial constraints and transportation.69 TTM associates age, health cognition, biopsy history, and self-efficacy with mammography stages, particularly in Asian Americans.106 The SMCPC model identification barriers such as time constraints, distrust in doctors, and smoking.70 The SMH model shows that spirituality and participation in free screening programs improve screening rates.76 The SDT model focuses on perceived effort, choice, and stress as screening influences.75 The CSB model emphasizes the role of entrenched cultural norms in shaping health behaviors.33 While these models offer strong predictive power in certain contexts, their practical application is often hindered by resource limitations, insufficient healthcare infrastructure, and cultural barriers that prevent effective implementation, especially in low-income and rural areas of sub-Saharan Africa and rural Latin America.71
Complexity of Integrated Models
Integrated models’ complexity arises from combining multiple theoretical frameworks, each with its own distinct concepts and structures. Combining HBM with TPB allows simultaneously consider the influence of individual beliefs and social norms.74 Combining HBM with TPB also reveals occupational differences, with higher screening intentions among teachers and medical staff.[74] The HBM-SCT combination emphasizes perceived barriers, benefits, and susceptibility across BSE stages,19 while the HBM-TTM model suggests stage-specific strategies for better BSE acceptance,89,94 highlighting the impact of perceived barriers, especially for women with a family history. The HBM-TRA combined model showed that the TRA model had a better model fit than the HBM.90 The HBM-CSEI found that women scholars who participated in BSE reported higher perceived benefits and self-efficacy.92 The HBM-CSM believes that lack of trust in the medical team and concerns about procedural pain affect BCS.99 The HBM-SCM found that women in the action and maintenance stages were more likely to adopt MMG.98 The HBM-KAB model links health beliefs with screening behaviors,95 considering factors like age, marital status, and motivation, thereby supporting personalized interventions. The HBM-KAP offers a different view, suggesting that sociodemographic characteristics affect the use of MMG but not the adoption of CBE.96 The PMT-SST suggests that women who believe in the effectiveness of BSE and have self-confidence are more likely to undergo BSE.91 The TPB+CDT combination shows that women’s decisions are more influenced by family and friends’ attitudes than by screening invitations.88 The HBM+HPM model highlights that lack of information, indifference, and cultural factors are key barriers to screening participation.100 The SEM, HBM,[93] and cancer stigma framework together reveal that sociocultural misunderstandings, health literacy gaps, and limited healthcare resources contribute to women to seek treatment only when symptoms are severe.107 For instance, in low-resource settings in Southeast Asia, integrating HBM with local cultural models has shown promise in addressing socioeconomic disparities, though challenges persist in rural vs urban implementations.108 Integrating social media52 and digital health tools into these models may help examine how they enhance access to healthcare services and social support, thereby promoting participation in health screenings.61
Model Intersections and Hybrid Framework Implications
Our analyses (Figures 2–4) reveal systematic theoretical convergence patterns that inform hybrid framework development for BCS. Hybrid frameworks integrate complementary constructs by addressing multilevel determinants individual cognition, social context, and structural factors that single models are unable to capture adequately. Evidence demonstrates that multilevel interventions based on integrated theories achieve 1.5–2.3 times higher screening rates than single-theory approaches.109
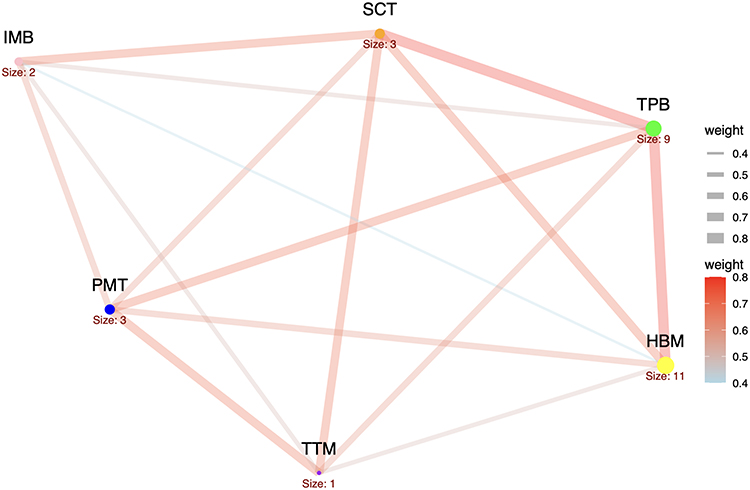 |
Figure 2 Behavioral and Cognitive Models. This diagram illustrates the relationships between major health behavior theoretical models, including the IMB, TPB, PMT, HBM, SCT and TTM. Node size indicates influence, and line thickness indicates the strength of the association between models. |
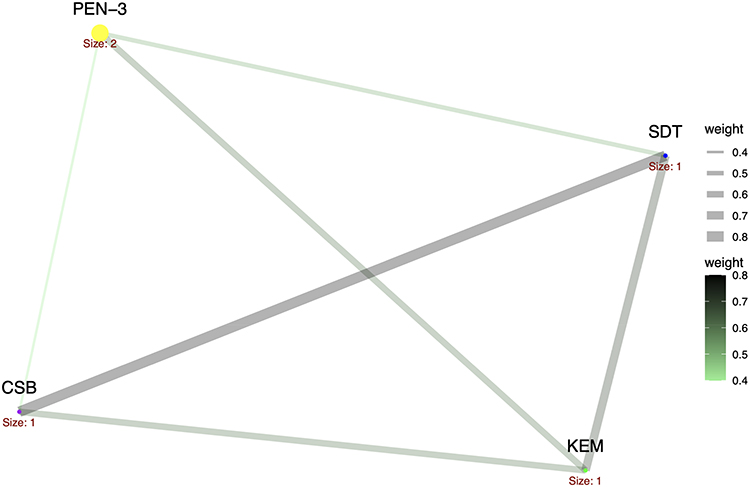 |
Figure 3 Health and Social Determinants Models. This diagram illustrates a network of models focusing on the relationship between sociocultural factors and health, including the PEN-3, CSB, SDT, and KEM. This model highlights the central role of cultural background and individual motivation in health interventions. |
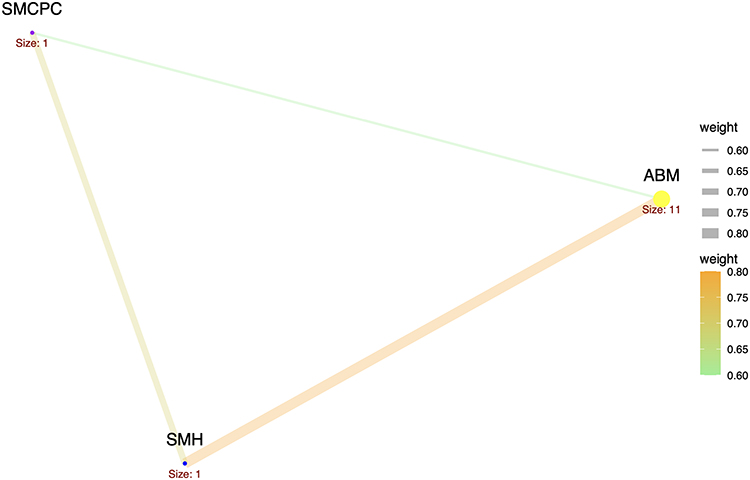 |
Figure 4 Systems and Contextual Models. This diagram illustrates the synergistic relationship between systems models, including the ABM, SMCPC, and SMH. The strong synergy between the ABM and SMCPC can be used to proactively optimize intervention strategies, reduce costs, and improve efficiency. |
Behavioral and Cognitive Models (Figure 2) show strong HBM-TPB correlation (r = 0.72), indicating complementary mechanisms: HBM addresses threat appraisal and outcome expectations,110 while the TPB captures normative influences and perceived behavioral control. SCT bridges both through reciprocal determinism, linking individual cognition with social factors and environmental influences.111 Community-based programs integrating HBM-TPB-SCT increased mammography rates from 42% to 67% in underserved populations. Weak IMB-TTM correlations (r = 0.31) reflect theoretical incompatibility; however, stage-matched interventions applying these models sequentially achieved 68% versus 41% screening completion over 12 months.
Health and Social Determinants Models (Figure 3) demonstrate PEN-3 and SDT alignment (r = 0.68), both prioritizing cultural context and autonomous agency across minority populations.112 PEN-3 identifies culturally relevant enablers while SDT provides motivational pathways respecting cultural autonomy.113 Faith-based screening programs integrating both models achieved 73% participation among African American women versus 48% in culturally non-tailored programs. SDT exhibits minimal overlap with KEM (r<0.25), reflecting distinct intrinsic-motivation versus knowledge-based orientation.
Systems and Contextual Models (Figure 4) reveal ABM-SMCPC synergy (r = 0.74): ABM simulates behavioral dynamics while SMCPC operationalizes communication strategies.114 This integration enables prospective intervention testing, with simulated pre-testing identifying optimal intervention components that reduced implementation costs by 34% while improving reach by 28%. SMH shows weak ABM convergence (r = 0.29), indicating complementary rather than overlapping application.
These hybrid frameworks provide nurses with more precise assessment tools to identify whether non-adherence stems from knowledge gaps, social barriers, or self-efficacy deficits, enabling targeted interventions. For policy, computational modeling enables evidence-based resource allocation across diverse contexts.115 Future research should empirically test these theoretical synergies through randomized controlled trials examining both screening outcomes and the feasibility of implementation across diverse populations.
Conclusion
Over the past decade, various theoretical frameworks have been used to explore the complex factors influencing BCS behaviors. However, the evolving nature of health behaviors has led researchers to increasingly adopt mixed methods, integrating multiple theoretical models for a more comprehensive understanding of BCS determinants. These multidimensional perspectives, when combined, offer a more robust and nuanced predictive framework. Future refinements to these models are expected to enhance their applicability and validity across diverse populations and contexts. Predictions generated from these models emphasize the importance of incorporating contextual and personal factors to improve accuracy. Future research should focus on developing hybrid models and validating these frameworks in real-world settings. These findings not only demonstrate that refining theoretical models is crucial to improving their applicability but also highlight the importance of translating these theoretical insights into actionable public health strategies, such as community interventions, targeted education campaigns, and policy changes aimed at reducing barriers to screening. A potential limitation of this review is the inclusion of studies from diverse methodologies and settings, which may limit the comparability and generalizability of the findings. In addition, this review may have introduced biases. Language restrictions could have led to the exclusion of relevant studies published in other languages. The geographical distribution of included studies is concentrated in specific countries, which may limit the global applicability of the findings. Furthermore, the limited inclusion of indigenous or ethnic minority populations may have overlooked the impact of cultural diversity on screening behavior.
Abbreviation
HBM, Health Belief model; TPB, Theory of Planned Behavior; SCT, Social Cognitive Theory; PMT, Protection motivation Theory; IMB, Information-motivation-Behavioral Skills model; TTM, Transtheoretical model; SDT, Self-determinant theory; KEM, Kleinman’s Explanatory model; PEN-3, PEN-3 model; CSB, Theory of Care Seeking Behavior; SMH, Salutogenic model of health; SMCPC, Systems model of Clinical Preventive Care; ABM, Andersen’s Behavioral model; PMT+SST, Protection motivation Theory+Social Support Theory; TTM+HBM, Transtheoretical model+Health Belief model; KAP+HBM, Knowledge, Attitudes, and Practices+Health Belief model; HBM+TRA, Health Belief model + Theory of Reasoned Action; SEM+HBM+cancer stigma framework, Social Ecological model+Health Belief model+Cancer Stigma Framework; HBM+TPB, Health Belief model + Theory of Planned Behavior; HBM+SCT, Health Belief model + Social Cognitive Theory; HBM+SCM, Health Belief model+Stages of Change model; HBM+KAB, Health Belief model+Knowledge-Attitude-Behavior model; HBM+HPM, Health Belief model+Health Promotion model; HBM+CSM, Health Belief model;del+Common-Sense model; HBM+CSEI, Health Belief model + Coopersmith Self-Esteem Inventory; HBM+SEM, Health Belief model+Social Ecological model; TPB+SCT+HBM+Fatalism, Theory of Planned Behavior + Social Cognitive Theory + Health Belief model + Fatalism.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149(4):778–789. doi:10.1002/ijc.33588
2. International Agency for Research on Cancer. Cancer today. Available from: https://gco.iarc.fr/today/en.
3. Koc G, Gulen-Savas H, Ergol S, Yildirim-Cetinkaya M, Aydin N. Female university students’ knowledge and practice of breast self-examination in Turkey. Niger J Clin Pract. 2019;22(3):410–415. doi:10.4103/njcp.njcp_341_18
4. Chung KP, Lai MS, Cheng SH, et al. Organization-based performance measures of cancer care quality: core measure development for breast cancer in Taiwan. Eur J Cancer Care. 2008;17(1):5–18. doi:10.1111/j.1365-2354.2007.00796.x
5. National Department of Medical and Health Policy and Management. Breast cancer treatment guidelines(2022 edition). Zhonghua Zhong Liu Za Zhi. 2023;45(10):803–833. doi:10.3760/cma.j.cn112152-20230706-00281
6. W. H. Organization. Cancer. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/cancer.
7. Molassiotis A, Tyrovolas S, Giné-Vázquez I, Yeo W, Aapro M, Herrstedt J. Organized breast cancer screening not only reduces mortality from breast cancer but also significantly decreases disability-adjusted life years: analysis of the Global Burden of Disease Study and screening programme availability in 130 countries. ESMO Open. 2021;6(3):100111. doi:10.1016/j.esmoop.2021.100111
8. Pataki J, Dombrádi V, Sárváry A, Szőllősi GJ. Breast cancer screening and its associating factors among Hungarian women aged 45-65: a cross-sectional study based on the European health interview surveys from 2009 to 2019. BMC Public Health. 2023;23(1):1679. doi:10.1186/s12889-023-16608-5
9. Ingman WV, Richards B, Street JM, et al. Breast density notification: an Australian perspective. J Clin Med. 2020;9(3):681. doi:10.3390/jcm9030681
10. Blay L, Louro J, Barata T, et al. Variability of breast surgery in women participating in breast cancer screening programs. Cir Esp. 2019;97(2):89–96. Variabilidad en la práctica de la cirugía mamaria en mujeres participantes en el programa de cribado poblacional de cáncer de mama. doi:10.1016/j.ciresp.2018.11.001
11. Warrier S, Tapia G, Goltsman D, Beith J. An update in breast cancer screening and management. Womens Health. 2016;12(2):229–239. doi:10.2217/whe.15.105
12. Miller AB, Baines CJ. The role of clinical breast examination and breast self-examination. Prev Med. 2011;53(3):118–120. doi:10.1016/j.ypmed.2011.05.001
13. Zhang X, Yang L, Liu S, et al. Evaluation of different breast cancer screening strategies for high-risk women in Beijing, China: a real-world population-based study. Front Oncol. 2021;11:776848. doi:10.3389/fonc.2021.776848
14. Qaseem A, Lin JS, Mustafa RA, et al. Screening for breast cancer in average-risk women: a guidance statement from the American College of Physicians. Ann Intern Med. 2019;170(8):547–560. doi:10.7326/m18-2147
15. Ren W, Chen M, Qiao Y, Zhao F. Global guidelines for breast cancer screening: a systematic review. Breast. 2022;64:85–99. doi:10.1016/j.breast.2022.04.003
16. Wang Y, Chen H, Li N, et al. Ultrasound for breast cancer screening in high-risk women: results from a population-based cancer screening program in China. Front Oncol. 2019;9:286. doi:10.3389/fonc.2019.00286
17. M. Mascara and C. Constantinou. Global perceptions of women on breast cancer and barriers to screening. Current Oncol Rep. 2021;23:1–9.
18. Tavakoli B, Feizi A, Zamani-Alavijeh F, Shahnazi H. Factors influencing breast cancer screening practices among women worldwide: a systematic review of observational and qualitative studies. BMC Womens Health. 2024;24(1):268. doi:10.1186/s12905-024-03096-x
19. Salmani F, Moodi M, Yousefi A, Norozi E. Healthy beliefs regarding breast cancer screening in Iranian women health volunteers: a path analysis. Korean J Fam Med. 2021;42(2):132–139. doi:10.4082/kjfm.20.0001
20. Shaw DR, Allen TF. Observational decisions and metaphors in the theory construction process: the business ecosystem metaphor. in
21. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. doi:10.1186/s13012-015-0242-0
22. Nilsen P, Ingvarsson S, Hasson H, von Thiele Schwarz U, Augustsson H. Theories, models, and frameworks for de-implementation of low-value care: a scoping review of the literature. Implement Res Pract. 2020;1:2633489520953762. doi:10.1177/2633489520953762
23. Liao Y, Hairon SM, Yaacob NM, Luo L, Ismail TAT. A comprehensive model for understanding breast cancer screening hesitancy: integrating the health belief model and the confidence, convenience, complacency, constraints, and risk and responsibility calculations (5C) model. Cureus. 2024;16(10):e71583. doi:10.7759/cureus.71583
24. Lemmo D, Martino ML, Vallone F, et al. Clinical and psychosocial constructs for breast, cervical, and colorectal cancer screening participation: a systematic review. Int J Clin Health Psychol. 2023;23(2):100354. doi:10.1016/j.ijchp.2022.100354
25. Pitsillidou M, Roupa Z, Farmakas A, Noula M. Factors affecting the application and implementation of evidence-based practice in nursing. Acta Inform Med. 2021;29(4):281–287. doi:10.5455/aim.2021.29.281-287
26. Moullin JC, Dickson KS, Stadnick NA, et al. Ten recommendations for using implementation frameworks in research and practice. Implementation Sci Commun. 2020;1(1):42. doi:10.1186/s43058-020-00023-7
27. Strifler L, Barnsley JM, Hillmer M, Straus SE. Identifying and selecting implementation theories, models and frameworks: a qualitative study to inform the development of a decision support tool. BMC Med Inform Decis Mak. 2020;20(1):91. doi:10.1186/s12911-020-01128-8
28. Arksey H, O’malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
29. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. doi:10.1186/1748-5908-5-69
30. Tricco AC, Lillie E, Zarin W, PRISMA-ScR. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473
31. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/jbies-20-00167
32. Narcisse M-R, Shah SK, Hallgren E, Felix HC, Schootman M, McElfish PA. Factors associated with breast cancer screening services use among women in the United States: an application of the andersen’s behavioral model of health services use. Preventive Med. 2023;173:107545. doi:10.1016/j.ypmed.2023.107545
33. Sarmah N, Sibiya MN, Khoza TE. The sociocultural influences on breast cancer screening among Rural African Women in South Africa. Int J Environ Res Public Health. 2023;20(21):7005. doi:10.3390/ijerph20217005
34. Tarı Selçuk K, Avcı D, Yılmaz Dündar G, Mercan Y. Breast cancer screening behaviors in women aged 40 years and over in a semi-urban region in Turkey: relationships with health beliefs. Healthcare. 2020;8(2):171. doi:10.3390/healthcare8020171
35. Ritchie D, Van den Broucke S, Van Hal G. The health belief model and theory of planned behavior applied to mammography screening: a systematic review and meta-analysis. Public Health Nurs. 2021;38(3):482–492. doi:10.1111/phn.12842
36. Altunkurek ŞZ, Mohamed SH. Determine knowledge and belief of Somalian young women about breast cancer and breast self-examination with champion health belief model: a cross-sectional study. BMC Med Inf Decis Making. 2022;22(1):326. doi:10.1186/s12911-022-02065-4
37. Kangmennaang J, Mkandawire P, Luginaah I. Breast cancer screening among women in Namibia: explaining the effect of health insurance coverage and access to information on screening behaviours. Global Health Promotion. 2019;26(3):50–61. doi:10.1177/1757975917727017
38. Jiraniramai S, Pinyopornpanish K, Wongpakaran N, et al. Association between sociodemographic factors and health beliefs related to breast cancer screening behavior among Northern Thai women: a hospital-based study. Sci Rep. 2024;14(1):7596. doi:10.1038/s41598-024-58155-y
39. Nikpour M, Hajian-Tilaki K, Bakhtiari A. Risk assessment for breast cancer development and its clinical impact on screening performance in Iranian women. Cancer Manage Res. 2019;Volume 11:10073–10082. doi:10.2147/CMAR.S229585
40. Park C, Ma X, Park SK, Lawson KA. Association of depression with adherence to breast cancer screening among women aged 50 to 74 years in the United States. J Eval Clin Pract. 2020;26(6):1677–1688. doi:10.1111/jep.13356
41. Juárez-García DM, Valenciano-Salas IA, de Jesús García-Solís M, Téllez A. Development and validation of a Mexican version of the champion’s health belief model scale for breast cancer screening. J Cancer Educ. 2021;36:100–105. doi:10.1007/s13187-019-01603-5
42. Khazir Z, Sharifabad MAM, Vaezi AA, Enjezab B, Fallahzadeh H, Yari F. Predictors of mammography based on Health Belief Model in Khorramabad women. J Educ Health Promotion. 2019;8(1):180. doi:10.4103/jehp.jehp_63_19
43. Mekuria M, Nigusse A, Tadele A. Breast self-examination practice and associated factors among secondary school female teachers in Gammo Gofa Zone, southern, Ethiopia. Breast Cancer: Target Therapy. 2020;2020:1–10.
44. Noman S, Shahar HK, Rahman HA, Ismail S, Aljaberi MA, Abdulrahman MN. Factor structure and internal reliability of breast cancer screening champion’s health belief model scale in Yemeni women in Malaysia: a cross-sectional study. BMC Women’s Health. 2021;21:1–11. doi:10.1186/s12905-021-01543-7
45. Racine L, Andsoy I, Maposa S, Vatanparast H, Fowler-Kerry S. Examination of breast cancer screening knowledge, attitudes, and beliefs among Syrian refugee women in a Western Canadian province. Can J Nurs Res. 2022;54(2):177–189. doi:10.1177/08445621211013200
46. Wang W-L, Hsu S-D, Wang J-H, Huang L-C, Hsu W-L. Survey of breast cancer mammography screening behaviors in Eastern Taiwan based on a health belief model. Kaohsiung J Med Sci. 2014;30(8):422–427. doi:10.1016/j.kjms.2014.04.007
47. Tsunematsu M, Kawasaki H, Masuoka Y, Kakehashi M. Factors affecting breast cancer screening behavior in Japan-assessment using the health belief model and conjoint analysis. Asian Pac J Cancer Prev. 2013;14(10):6041–6048. doi:10.7314/APJCP.2013.14.10.6041
48. Sha R, Zhao T, Feng R. Health beliefs and breast cancer screening behavior and willingness of community residents in Hefei. Acta Universitatis Medicinalis Anhui. 2017;52:993–997.
49. Shubayr N, Khmees R, Alyami A, Majrashi N, Alomairy N, Abdelwahab S. Knowledge and factors associated with breast cancer self-screening intention among Saudi female college students: utilization of the health belief model. Int J Environ Res Public Health. 2022;19(20):13615. doi:10.3390/ijerph192013615
50. An S, Choi YJ, Lee HY, Yoon YJ, Platt M. Predictors of breast cancer screening among Korean American women: is having an annual checkup critical? Asian Pac J Cancer Prev. 2018;19(5):1281. doi:10.22034/APJCP.2018.19.5.1281
51. Esna-Ashari F, Saffari N, Parsapour H, Rezapur-Shahkolai F. Factors associated with breast cancer mammographic screening behavior among Iranian women. Asian Pac J Cancer Prev. 2022;23(12):4073. doi:10.31557/APJCP.2022.23.12.4073
52. Islam KF, Awal A, Mazumder H, et al. Social cognitive theory-based health promotion in primary care practice: a scoping review. Heliyon. 2023;9(4):e14889. doi:10.1016/j.heliyon.2023.e14889
53. Agrawal P, Chen TA, McNeill LH, et al. Factors associated with breast cancer screening adherence among church-going African American women. Int J Environ Res Public Health. 2021;18(16):8494. doi:10.3390/ijerph18168494
54. Antabe R, Kansanga M, Sano Y, Kyeremeh E, Galaa Y. Utilization of breast cancer screening in Kenya: what are the determinants? BMC Health Serv Res. 2020;20:1–9. doi:10.1186/s12913-020-5073-2
55. Manning M, Albrecht TL, Penner L, Purrington K. Between-race differences in processes predicting physician communication for African American and European American recipients of breast density notifications. Ann Behav Med. 2019;53(8):721–731. doi:10.1093/abm/kay079
56. Keshavarzi A, Asadi S, Asadollahi A, Mohammadkhah F, Jeihooni AK. Tendency to breast cancer screening among rural women in southern Iran: a structural equation modeling (SEM) analysis of theory of planned behavior. Breast Cancer. 2022;16:11782234221121001. doi:10.1177/11782234221121001
57. Sun Y, Yuan J, Liu W, et al. Predicting rural women’s breast cancer screening intention in China: a PLS-SEM approach based on the theory of planned behavior. Front Public Health. 2022;10:858788. doi:10.3389/fpubh.2022.858788
58. Jeihooni AK, Moayedi ZS, Momenabadi V, Ghalegolab F, Harsini PA. Effect of educational intervention based on theory of planned behavior (TPB) on doing breast self-examination in a sample of Iranian Women. Breast Cancer. 2023;17:11782234221145417. doi:10.1177/11782234221145417
59. Mirzaei-Alavijeh M, Heydari ST, Ahmadi-Jouybari T, Jalilian F, Gharibnavaz H, Mahboubi M. Socio-demographic and cognitive determinants of breast cancer screening. Int J Adv Biotechnol Res. 2016;7(4):1684–1690.
60. Cadet TJ. The relationship between psychosocial factors and breast cancer screening behaviors of older Hispanic women. Soc Work Public Health. 2015;30(2):207–223. doi:10.1080/19371918.2014.969857
61. Erku D, Khatri R, Endalamaw A, et al. Digital health interventions to improve access to and quality of primary health care services: a scoping review. Int J Environ Res Public Health. 2023;20(19):6854. doi:10.3390/ijerph20196854
62. Gao Y, Yu J, Wang H, Liu B, Zhang S. Predicting breast cancer screening behaviors using protective motivation theory: a structural equation modeling approach. CEOG. 2023;50(8). doi:10.31083/j.ceog5008168
63. Adegboyega A, Wiggins AT, Obielodan O, Dignan M, Schoenberg N. Beliefs associated with cancer screening behaviors among African Americans and Sub-Saharan African immigrant adults: a cross-sectional study. BMC Public Health. 2022;22(1):2219. doi:10.1186/s12889-022-14591-x
64. Elewonibi B, BeLue R. The influence of socio-cultural factors on breast cancer screening behaviors in Lagos, Nigeria. Ethn Health. 2019;24(5):544–559. doi:10.1080/13557858.2017.1348489
65. Moghaddam ES, Shahnazi H, Hassanzadeh A. Predictive power of PEN-3 model constructs in breast cancer screening behaviors among teachers: a cross- sectional study in Central Iran. Eur J Breast Health. 2019;15(2):105–110. doi:10.5152/ejbh.2019.4417
66. Zhang M, Wei W, Li Q, et al. Determinants of intention to participate in breast cancer screening among urban Chinese women: an application of the protection motivation theory. Int J Environ Res Public Health. 2021;18(21). doi:10.3390/ijerph182111093
67. Lu N, Zhang C, You H, Ma Z, Zhu P, Cheng F. Factors affecting breast screening behavior of first-degree relatives of breast cancer patients in China: a cross-sectional study. Cancer Nurs. 2024;47(4):271–280. doi:10.1097/ncc.0000000000001176
68. Aluko JO, Ojelade MF, Sowunmi CO, Oluwatosin OA. Awareness, knowledge and practices of breast cancer screening measures among female postgraduate students of a Nigerian Federal University: a cross-sectional study. Afr J Med Med Sci. 2014;43(Suppl 1):79–86.
69. Wells AA, Shon EJ, McGowan K, James A. Perspectives of low-income African-American women non-adherent to mammography screening: the importance of information, behavioral skills, and motivation. J Cancer Educ. 2017;32(2):328–334. doi:10.1007/s13187-015-0947-4
70. Guo Y, Cheng TC, Lee HY. Factors associated with adherence to preventive breast cancer screenings among middle-aged African American women. Soc Work Public Health. 2019;34(7):646–656. doi:10.1080/19371918.2019.1649226
71. Victor A. Artificial intelligence in global health: an unfair future for health in Sub-Saharan Africa? Health Aff Sch. 2025;3(2):qxaf023. doi:10.1093/haschl/qxaf023
72. Talley CH, Yang L, Williams KP. Breast cancer screening paved with good intentions: application of the information-motivation-behavioral skills model to racial/ethnic minority women. J Immigr Minor Health. 2017;19(6):1362–1371. doi:10.1007/s10903-016-0355-9
73. Donnelly TT, Al Khater A-H, Al-Bader SB, et al. Beliefs and attitudes about breast cancer and screening practices among Arab women living in Qatar: a cross-sectional study. BMC Womens Health. 2013;13(1):49. doi:10.1186/1472-6874-13-49
74. Wang X, Chen D, Xie T, Zhang W. Predicting women’s intentions to screen for breast cancer based on the health belief model and the theory of planned behavior. J Obstet Gynaecol Res. 2019;45(12):2440–2451. doi:10.1111/jog.14109
75. Jung SM, Jo HS. Intrinsic motivation factors based on the self-determinant theory for regular breast cancer screening. Asian Pac J Cancer Prev. 2014;15(23):10101–10106. doi:10.7314/apjcp.2014.15.23.10101
76. Conway-Phillips R, Janusek L. Influence of sense of coherence, spirituality, social support and health perception on breast cancer screening motivation and behaviors in African American women. Abnf J. 2014;25(3):72–79
77. Wuur MM, Duodu DA, Tarkang EE. Factors that influence breast cancer screening among women of reproductive age in the Nandom Municipality, Ghana. BMC Women’s Health. 2022;22(1):359. doi:10.1186/s12905-022-01946-0
78. Lee Y-S, Roh S, Moon H, Lee KH, McKinley C, LaPlante K. Andersen’s behavioral model to identify correlates of breast cancer screening behaviors among indigenous women. J Evidence-Based Soc Work. 2020;17(1):117–135. doi:10.1080/26408066.2019.1650316
79. Jin SW, Lee HY, Lee J. Analyzing factors of breast cancer screening adherence among Korean American women using Andersen’s behavioral model of healthcare services utilization. Ethnicity Dis. 2019;29(Suppl 2):427. doi:10.18865/ed.29.S2.427
80. An S, Lee HY, Choi YJ, Yoon YJ. Literacy of breast cancer and screening guideline in an immigrant group: importance of health accessibility. J Immigrant Minority Health. 2020;22(3):563–570. doi:10.1007/s10903-020-00973-z
81. Kamyab A, Mohammadkhah F, Asadi S, Ghalehgolab F, Jeihooni AK. The effect of an educational intervention on breast cancer screening of rural women: application of the theory of planned behavior. Cancer Control. 2024;31:10732748241266788. doi:10.1177/10732748241266788
82. Zhang H, Meng Q, Jin X, Ma S, Liu C, Zhang J. Analysis of the influencing factors of preventive healthcare and healthcare utilization for breast cancer patients in Jinan based on the Anderson model of healthcare utilization. Chin J Maternal Child Health Care. 2023;01:142–146. doi:10.19829/j.zgfybj.issn.1001-4411.2023.01.037
83. Ketema B, Kaba M, Negash S, Addissie A, Kantelhardt EJ. Intention to undergo clinical breast examination and its associated factors among women attending rural primary healthcare facilities in South Central Ethiopia. Breast Care. 2023;18(6):464–472. doi:10.1159/000531944
84. Kim SY, Guo Y, Won C, Lee HY. Factors associated with receipt of mammogram among caregivers: a comparison with non-caregivers. BMC Women’s Health. 2020;20:1–8. doi:10.1186/s12905-020-01079-2
85. Lee MH, Merighi JR, Lee HY. Factors associated with mammogram use in Korean American immigrant women. Am J Health Behav. 2019;43(6):1075–1085. doi:10.5993/AJHB.43.6.6
86. Lee HY, Lee MH, Jang YJ, Lee DK. Breast cancer screening disparity among Korean American immigrant women in Midwest. Asian Pac J Cancer Prev. 2017;18(10):2663. doi:10.22034/APJCP.2017.18.10.2663
87. Tolma EL, Stoner JA, Li J, Kim Y, Engelman KK. Predictors of regular mammography use among American Indian women in Oklahoma: a cross-sectional study. BMC Womens Health. 2014;14:101. doi:10.1186/1472-6874-14-101
88. Henriksen MJ, Guassora AD, Brodersen J. Preconceptions influence women’s perceptions of information on breast cancer screening: a qualitative study. BMC Res Notes. 2015;8:404. doi:10.1186/s13104-015-1327-1
89. Farajzadegan Z, Fathollahi-Dehkordi F, Hematti S, Sirous R, Tavakoli N, Rouzbahani R. The transtheoretical model, health belief model, and breast cancer screening among Iranian women with a family history of breast cancer. J Res Med Sci. 2016;21:122. eng. doi:10.4103/1735-1995.193513
90. Firouzbakht M, Hajian-Tilaki K, Bakhtiari A. Comparison of competitive cognitive models in explanation of women breast cancer screening behaviours using structural equation modelling: health belief model and theory of reasoned action. Eur J Cancer Care. 2021;30(1):e13328. doi:10.1111/ecc.13328
91. bashirian S, Barati M, Shoar LM, Mohammadi Y, Dogonchi M. Factors affecting breast self-examination behavior among female healthcare workers in Iran: the role of social support theory. J Preventive Med Public Health. 2019;52(4):224–233. doi:10.3961/jpmph.18.277
92. Avci IA, Kumcagiz H, Altinel B, Caloglu A. Turkish female academician self-esteem and health beliefs for breast cancer screening. Asian Pac J Cancer Prev. 2014;15(1):155–160. doi:10.7314/apjcp.2014.15.1.155
93. Goh SA, Lee JK, Seh WY, et al. Multi-level determinants of breast cancer screening among Malay-Muslim women in Singapore: a sequential mixed-methods study. BMC Womens Health. 2022;22(1):383. doi:10.1186/s12905-022-01972-y
94. Kim EM, Lee H, Kim J-G, et al. Using the stage-based approaches to predict breast self-examination among Rural Vietnamese women. Asia Pac J Public Health. 2019;31(4):325–334. doi:10.1177/1010539519849326
95. Hsieh HM, Chang WC, Shen CT, Liu Y, Chen FM, Kang YT. Mediation effect of health beliefs in the relationship between health knowledge and uptake of mammography in a national breast cancer screening program in Taiwan. J Cancer Educ. 2021;36(4):832–843. doi:10.1007/s13187-020-01711-7
96. Ngan TT, Jenkins C, Minh HV, Donnelly M, O’Neill C. Breast cancer screening practices among Vietnamese women and factors associated with clinical breast examination uptake. PLoS One. 2022;17(5):e0269228. doi:10.1371/journal.pone.0269228
97. Kisiangani J, Baliddawa J, Marinda P, et al. Determinants of breast cancer early detection for cues to expanded control and care: the lived experiences among women from Western Kenya. BMC Womens Health. 2018;18(1):81. doi:10.1186/s12905-018-0571-7
98. Ramli HA, Moey SF, Mutalib AMA. The relationship of health beliefs on the stage of mammography behavior adoption amongst women in Kuantan, Pahang. Asian Pac J Cancer Prev. 2019;20(6):1913–1920. doi:10.31557/apjcp.2019.20.6.1913
99. Marmarà D, Marmarà V, Hubbard G. Health beliefs, illness perceptions and determinants of breast screening uptake in Malta: a cross-sectional survey. BMC Public Health. 2017;17(1):416. doi:10.1186/s12889-017-4324-6
100. Tuzcu A, Bahar Z. Barriers and facilitators to breast cancer screening among migrant women within Turkey. J Transcult Nurs. 2015;26(1):47–56. doi:10.1177/1043659614526245
101. Ghofranipour F, Pourhaji F, Delshad MH, Pourhaji F. Determinants of breast cancer screening: application of protection motivation theory. Int J Cancer Manag. 2020;13(5):e100535. doi:10.5812/ijcm.100535
102. Shiryazdi SM, Kholasehzadeh G, Neamatzadeh H, Kargar S. Health beliefs and breast cancer screening behaviors among Iranian female health workers. Asian Pac J Cancer Prev. 2014;15(22):9817–9822. doi:10.7314/APJCP.2014.15.22.9817
103. Tupper H, Ghukasyan R, Bayburtyan A, Hovhannisyan M, Shekherdimian S. Breast cancer awareness and screening perceptions of women in Yerevan, Armenia. Int J Public Health. 2024;69:1607029. doi:10.3389/ijph.2024.1607029
104. Rezaeimanesh M, Solhi M, Azar FEF, et al. Determinants of mammography screening in Tehranian women in 2018 based on the health belief model: a cross-sectional study. J Educ Health Promotion. 2021;10(1). doi:10.4103/jehp.jehp_339_20
105. Bhandari D, Shibanuma A, Kiriya J, Hirachan S, Ong KIC, Jimba M. Factors associated with breast cancer screening intention in Kathmandu Valley, Nepal. PLoS One. 2021;16(1):e0245856. doi:10.1371/journal.pone.0245856
106. Tung WC, Chen Y. Breast cancer knowledge and mammography use among Asian American women aged 40 and older: using the transtheoretical model approach. J Immigr Minor Health. 2024;26(1):140–147. doi:10.1007/s10903-023-01529-7
107. Malope SD, Norris SA, Joffe M. Culture, community, and cancer: understandings of breast cancer from a non-lived experience among women living in Soweto. BMC Womens Health. 2024;24(1):594. doi:10.1186/s12905-024-03431-2
108. Matthews KA, Spears KS, Anderson-Lewis C. Rural health disparities: contemporary solutions for persistent rural public health challenges. Prev Chronic Dis. 2025;22:E27. doi:10.5888/pcd22.250202
109. Subramanian S, Tangka FKL, Hoover S, DeGroff A. Integrated interventions and supporting activities to increase uptake of multiple cancer screenings: conceptual framework, determinants of implementation success, measurement challenges, and research priorities. Implement Sci Commun. 2022;3(1):105. doi:10.1186/s43058-022-00353-8
110. Pu B, Huang K. Modeling the path to digital health intention: the mediating role of system expectation and health beliefs. Front Public Health. 2025;13:1697273. doi:10.3389/fpubh.2025.1697273
111. Zhai S, Hash J, Ward TM, Yuwen W, Sonney J. Analysis, evaluation, and reformulation of social cognitive theory: toward parent-child shared management in sleep health. J Pediatric Nurs. 2023;73:e65–e74. doi:10.1016/j.pedn.2023.07.011
112. Iwelunmor J, Newsome V, Airhihenbuwa CO. Framing the impact of culture on health: a systematic review of the PEN-3 cultural model and its application in public health research and interventions. Ethn Health. 2014;19(1):20–46. doi:10.1080/13557858.2013.857768
113. Hulen RL. Utilizing the PEN-3 Model to Describe the Cultural Context of Health Literacy for Adult Congolese Refugees Post-Resettlement to Boise, Idaho, United States (US). Idaho State University; 2021.
114. Alkhawaldeh A, ALBashtawy M, Rayan A, et al. Application and use of andersen’s behavioral model as theoretical framework: a systematic literature review from 2012-2021. Iran J Public Health. 2023;52(7):1346–1354. doi:10.18502/ijph.v52i7.13236
115. Prasinos M, Basdekis I, Anisetti M, Spanoudakis G, Koutsouris D, Damiani E. A modelling framework for evidence-based public health policy making. IEEE J Biomed Health Inform. 2022;26(5):2388–2399. doi:10.1109/JBHI.2022.3142503
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.