Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Exploring the Immunological Implications of Insoluble Particulate Impurities in Hyaluronic Acid Fillers: Integrated Physicochemical and Histological Analyses of the Cohesive Polydensified Matrix Range
Authors Lee S, Tay CM, Martin MU, Seo J ![]()
Received 27 November 2025
Accepted for publication 28 December 2025
Published 7 January 2026 Volume 2026:19 584595
DOI https://doi.org/10.2147/CCID.S584595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Solam Lee,1,2 Clifton Ming Tay,3 Michael Uwe Martin,4 Jimyung Seo1
1Galleria Dermatology Clinic, Seoul, Republic of Korea; 2Department of Dermatology, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea; 3Merz Asia Pacific Pte. Ltd., Singapore, Singapore; 4Independent Researcher, Springe, Germany
Correspondence: Jimyung Seo, Galleria Dermatology Clinic, 34, Seolleung-ro, Gangnam-gu, Seoul, Republic of Korea, Tel +82-2-573-9839, Fax +82-2-578-9839, Email [email protected]
Background: Emerging research has identified insoluble particulate impurities in hyaluronic acid (HA) fillers as a potential factor in modulating inflammatory responses to HA fillers. This integrated study aims to characterize insoluble particles and assess the tissue integration and inflammatory potential of the cohesive polydensified matrix hyaluronic acid (CPM-HA) range of fillers.
Materials and Methods: Samples were prepared by degrading five CPM-HA fillers of varying concentration and rheology using hyaluronidase. An insoluble particle counter was employed to quantify the number of particles of size ≥ 10 μm and ≥ 25 μm present. Scanning electron microscopy (SEM) and energy-dispersive X-ray spectroscopy (EDS) were used to characterize insoluble particles. In vivo evaluation of CPM-HA fillers containing 20 mg/mL HA (CPM-HA S and CPM-HA R) in two healthy volunteers was performed at 1-week and 4-weeks after intradermal injection, via punch biopsy and histological assessments.
Results: The absolute number of insoluble particles in the CPM-HA fillers were low and beneath established pharmacopeial thresholds for injectables. SEM/EDS analysis determined the presence of expected manufacturing-related constituents including sodium (Na), chloride (Cl) and sulfur (S), while confirming the absence of immunologically relevant particulate matter such as silicon (Si), iron (Fe) and aluminum (Al). Hematoxylin and eosin staining of biopsy specimens revealed good tissue integration and no significant inflammatory response following injection of CPM-HA S and CPM-HA R.
Conclusion: CPM-HA fillers exhibited high purity with low levels of insoluble particulate matter and no potential immunologic adjuvants, with preliminary in vivo analyses indicating an absence of inflammatory responses.
Keywords: filler impurity, cohesive polydensified matrix technology, scanning electron microscopy, energy-dispersive X-ray spectrometry, delayed inflammatory reactions, tissue integration
Introduction
Hyaluronic acid (HA) dermal fillers are widely utilized for facial rejuvenation, volumization, and skin quality enhancements in non-invasive aesthetic procedures, owing to their favorable biocompatibility and reversibility.1 As a naturally occurring glycosaminoglycan, HA is generally well-tolerated by the human immune system.2–4 However, despite their widespread use and proven safety, rare but significant complications can arise.5
Among these, delayed inflammatory reactions (DIRs), which are characterized by erythema, swelling, or firm nodules, present a unique clinical challenge.6 DIRs can occur weeks to months after injection, unlike immediate hypersensitivity reactions which were more commonly observed with earlier generations of HA fillers. Their unpredictable onset, heterogeneous presentation, and resistance to treatments make them concerning to physicians and consequently a focus of ongoing research.7 The precise etiology of DIRs is considered to be multifactorial; potential triggers include patient factors such as viral or bacterial infections, immune stimulation following vaccination, as well as procedure-related factors (eg, suboptimal aseptic technique).8 Beyond these, the intrinsic properties of the filler material itself also play an important role.8
Prior literature has focused on the role of low-molecular-weight HA fragments for their potential to activate pro-inflammatory pathways.9–11 Notably, late inflammatory reactions have been associated with HA gels using a high composition of low-molecular weight HAs as starting ingredients in cross-linking, such as those produced with Vycross technology.9,12 In contrast, less attention has been given to non-HA-related particulate matter. These impurities, which can originate from manufacturing processes, crosslinking procedures, or even the container and syringe components, may act as immune adjuvants.13 When injected into dermal or subdermal tissue, they can stimulate innate and adaptive immune responses, potentially contributing to DIRs. This risk is amplified with the growing use of HA skin boosters administered intradermally,14,15 considering the proximity and abundance of immune surveillance cells in the dermis.14 Substandard purification processes can increase complication risk via immune pathways mediated by Langerhans and dermal dendritic cells,16 underscoring the need for more stringent purity standards.
Previously, one investigation detected significant quantities of insoluble particles (size >10 μm and >25 μm) in several commercial HA fillers beyond pharmacopeial thresholds established for standard injectable drugs.17 Various elemental impurities, including potential immunologic adjuvants such as silicon (Si), iron (Fe) and aluminum (Al), were identified. The potential sources of these impurities and the mechanisms underlying their immunological effects are reviewed and summarized in Table 1. However, to date, product specific safety evaluations remain limited as samples were anonymized. Moreover, previous analyses relied solely on physicochemical methods, without biological or histological evaluations to assess tissue responses in human subjects.
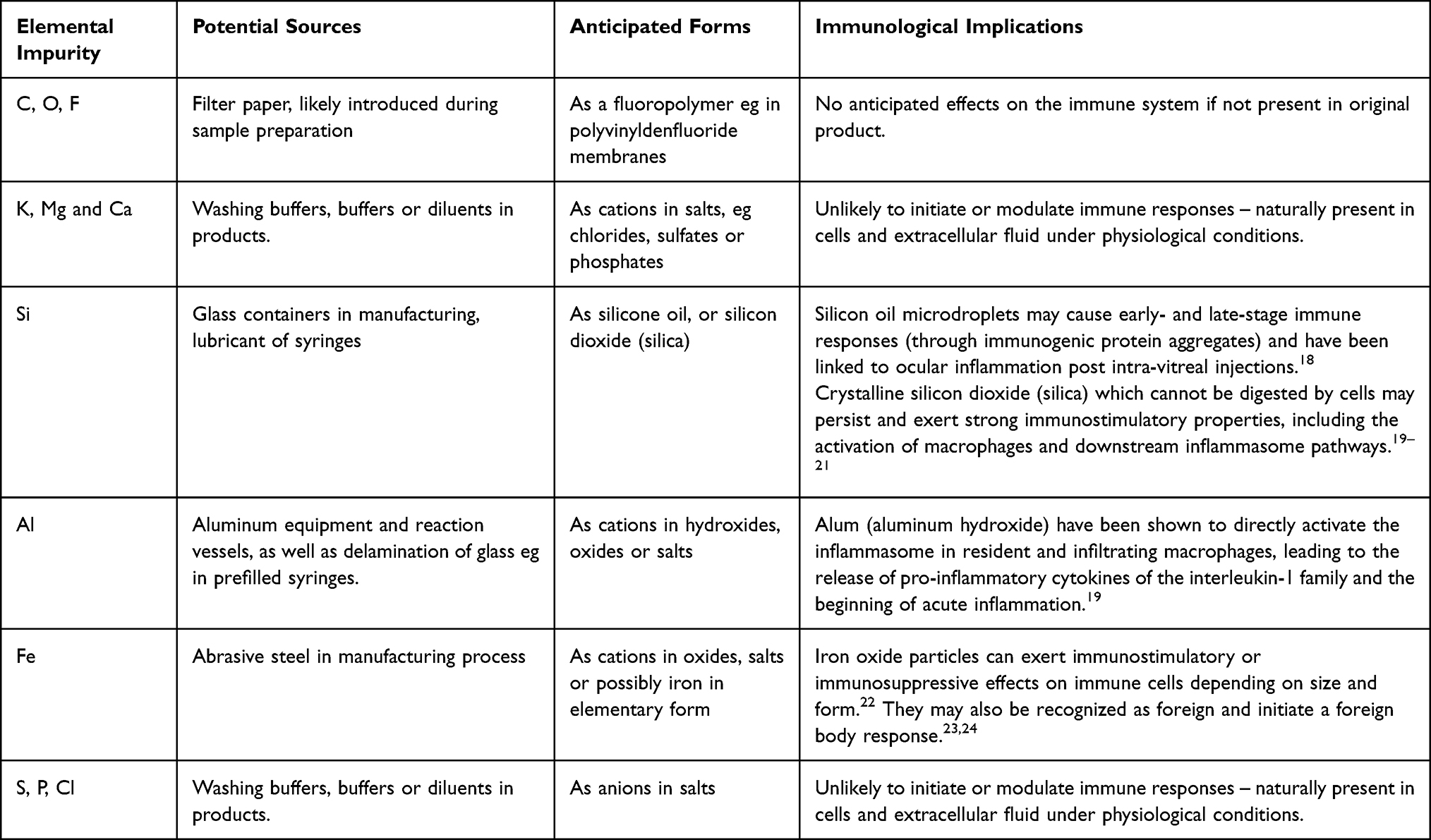 |
Table 1 Proposed Sources and Immunological Implications of Filler Impurities |
Cohesive polydensified matrix (CPM) HA fillers have an established safety profile based on extensive clinical use in aesthetic medicine, however, product-specific data in relation to insoluble particulate impurities are not yet available. An integrated approach would provide deeper insight into potential links between specific filler impurities and inflammatory reactions, with the goal of informing clinical practice and future product development. As such, this study aims to bridge this critical gap by characterizing the quantity and the composition of insoluble particles within the CPM range of HA fillers using scanning electron microscopy (SEM) and energy-dispersive X-ray spectroscopy (EDS). These physicochemical findings are complemented by histological assessments of human skin after HA filler injection to evaluate tissue integration and inflammatory potential.
Materials and Methods
Sample Preparation of HA Dermal Fillers and Hyaluronidase
A total of five CPM-HA fillers, including: CPM-HA R, (Anteis S.A., a company of the Merz Aesthetics® group, Belotero® Revive, Plan-les-Ouates, Switzerland; 20.0 mg/mL HA with 17.5 mg/mL glycerol), CPM-HA S (Belotero® Soft; 20.0 mg/mL HA), CPM-HA B (Belotero® Balance; 22.5 mg/mL HA), CPM-HA I (Belotero® Intense; 25.5 mg/mL HA) and CPM-HA V (Belotero® Volume; 26.0 mg/mL HA) were prepared for analysis. Hyaluronidase at 10,000 IU/mL (Sigma-Aldrich, St. Louis, MO, USA) was prepared by mixing 13.36 mg of hyaluronidase powder with 20 mL of ultrapure (Milli-Q) water. The mixture was filtered with a 0.22 µm syringe filter to remove any insoluble particles of hyaluronidase powder. The use of normal saline as a solvent can introduce additional insoluble particles, and it can be difficult to differentiate these from particles originally present in the filler. To eliminate potential confounding, the hyaluronidase solution was prepared using triple-filtered ultra-pure water.
In each 50 mL conical tube, 2 mL of hyaluronidase was mixed with 1 mL of each CPM-HA filler. Ultrapure water was added in place of CPM-HA filler and used as a negative control. To make up to a total volume of 20 mL, 17 mL of ultrapure water was further added to the tube. All conical tubes were incubated in a 37°C water tank and shaken for 36 hours for complete degradation of the CPM-HA filler and hyaluronidase powder. A schematic diagram of the workflow is provided in Figure 1A.
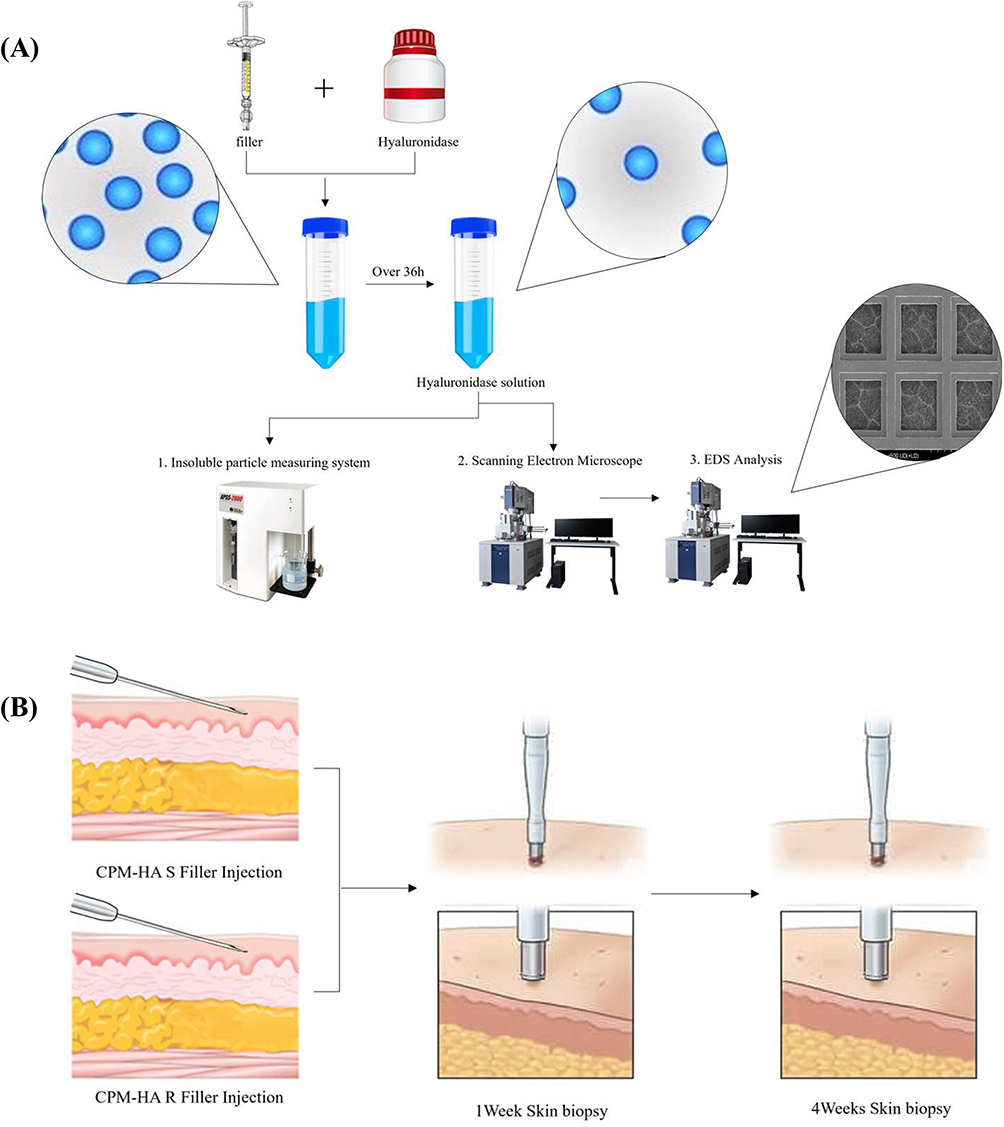 |
Figure 1 Study Flowchart. (A) Diagram of the workflow for insoluble particulate matter analyses. Each hyaluronic acid (HA) dermal filler from a syringe is mixed with hyaluronidase to enzymatically degrade the HA matrix. After the incubation period, the resulting solution is subjected to three main analyses: insoluble particle count, and SEM in conjunction with EDS analysis. (B) Diagram of procedures taken for the in vivo histological study. CPM-HA S and CPM-HA R fillers are injected intradermally into the forearm skin of human subjects. Punch biopsies samples collected at baseline (pre-injection), 1 week, and 4 weeks post-injection are processed for histological analysis to assess the tissue’s response and filler integration. Abbreviations: EDS, Energy-Dispersive X-ray Spectroscopy; HA, hyaluronic acid; SEM, scanning electron microscopy. |
Insoluble Particle Count
Prior to analysis, each HA filler sample was subjected to enzymatic degradation to liquify the cross-linked gel matrix, as described above. A 5 mL aliquot of the degraded sample was then placed into an automated light obscuration particulate counter (Particle Measuring Systems, APSS-2000 Automated Parenteral Sampling System, Boulder, CO, USA). The instrument was calibrated according to the manufacturer’s protocol, and a flushing cycle with particle-free water was performed before each sample run. Particles of sizes ≥10 μm and ≥25 μm were counted and evaluated according to the criteria in the United States Pharmacopeia (USP)25 for particulate matter in injections. Three independent measurements were performed for each sample, and the average particle count per milliliter with its standard deviation (SD) was calculated and reported.
Particle Characterization by SEM/EDS
After degradation with hyaluronidase, a small amount of the solution was drop-casted onto a transmission electron microscopy (TEM) grid under clean room conditions. This method was used to prevent contamination from standard filter paper. Any material or particles found on the reverse side of the grid were excluded from the analysis because they were likely contaminants from the underlying paper. The samples were then visualized using a cold-field emission SEM (Hitachi, SU8600, Tokyo, Japan), and the elemental composition of the impurities was determined by EDS. Each sample was analyzed at a minimum of five different locations and all detected elements from these analyses were then recorded. Signals corresponding to copper (Cu), palladium (Pd), and platinum (Pt) were excluded from the analysis as these elements are the primary constituents of the TEM grid, which was used as the main sample support for the particle analysis.
In vivo Histological Evaluation in Human Subjects
To complement our physicochemical analysis, we conducted a histological study to evaluate the in vivo tissue response to the HA fillers. Two healthy subjects (1 male, 1 female) each received an intradermal injection of 0.1 mL of CPM-HA R and CPM-HA S, administered into the forearm skin on either side (Figure 1B). At 1 week and 4-weeks post-injection, 2mm punch biopsies were performed for each side. For histological evaluations, samples were prepared and stained using hematoxylin and eosin. Further evaluation was performed by immunohistochemical (IHC) staining for CD68 which is used as a histochemical marker of inflammation associated with the involvement of monocytes and macrophages.
Results
Insoluble Particle Count
The counts for insoluble particles of size ≥10 µm and ≥25 µm were quantified for each filler sample and control group, with results summarized in Figure 2. For particles of size ≥10 µm, CPM-HA I had the highest mean particle count at 3,435.0 (SD 43.3). This was followed by CPM-HA S (1,833.3, SD 186.2), CPM-HA B (1,498.3, SD 113.4), CPM-HA R (1,476.7, SD 163.1), and CPM-HA V (938.3, SD 35.1). For particles of size ≥25 µm, CPM-HA I showed the highest mean count at 171.7 (SD 47.3), followed by CPM-HA S (131.7, SD 28.9), CPM-HA B (96.7, SD 29.3), and CPM-HA V (50.0, SD 13.2). CPM-HA R had the lowest mean count at 13.3 (SD 5.8). The observed particle counts for all tested samples were below the established USP thresholds for injectable drugs, in which thresholds are set at a maximum of 6,000 particles per container for sizes ≥10 µm and 600 particles per container for sizes ≥25 µm.
 |
Figure 2 Quantitative analysis of insoluble particles in CPM-HA fillers. Bar graphs showing the mean number of insoluble particles per syringe for each sample, error bars representing the standard deviation. The dotted lines represent the USP threshold for injectable drugs for respective corresponding particle sizes. (A) Graph (left) showing the number of insoluble particles ≥10 µm in size. (B) Graph (right) showing the number of insoluble particles ≥25 µm in size. Abbreviation: UPW, Ultrapure water; USP: United States Pharmacopeia. |
Visualization of Insoluble Particles by SEM
SEM images visualizing the morphology and size of insoluble particles within the degraded samples are presented in Figure 3. Across all CPM-HA filler samples, a porous network of degraded HA matrix, with particulate matter embedded within or resting upon the degraded HA scaffold, was observed. The particles varied in shape and size across the different filler types. The particles generally appeared to have a non-uniform, crystalline or aggregated morphology. In the higher magnification images, CPM-HA S, CPM-HA B, and CPM-HA I each presented discrete, irregularly shaped particles of varying sizes. CPM-HA V showed a larger agglomerate of particles, while CPM-HA R revealed a singular and smaller particle.
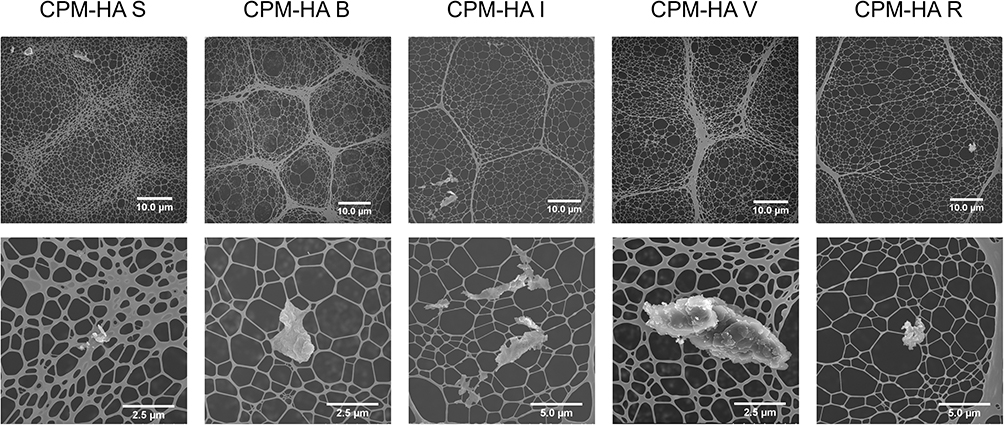 |
Figure 3 SEM images of insoluble particles within HA fillers. Top row: Low-magnification SEM images (at 1,000 X), illustrating the porous network of the degraded HA matrix. Bottom row: High-magnification SEM images (at 5,000 X to 20,000 X), showing the insoluble particles with varying sizes and irregular, aggregated morphologies embedded within or resting on the degraded HA scaffold. Abbreviations: HA, hyaluronic acid; SEM, scanning electron microscopy. |
Elemental Determination of Insoluble Particles by EDS Analysis
The elemental composition of insoluble particles based on EDS analysis, as well as their potential sources, are described in Table 2. Across all samples, including the control, the primary elements detected were carbon (C), oxygen (O), and nitrogen (N). These signals are considered to originate from adventitious contamination, an unavoidable consequence of sample handling (eg from laboratory equipment and environment) or exposure to air. Additional elements were also identified in specific samples. Sulfur (S) was detected in the CPM-HA S sample. In the CPM-HA V sample, sodium (Na) and chlorine (Cl) were present. The CPM-HA R sample also showed the presence of sodium (Na). The remaining samples (CPM-HA B, CPM-HA I) did not show any additional elemental signals beyond C, O, and N. Notably, silicon (Si), iron (Fe) and aluminum (Al) were not detected in any of the analyses.
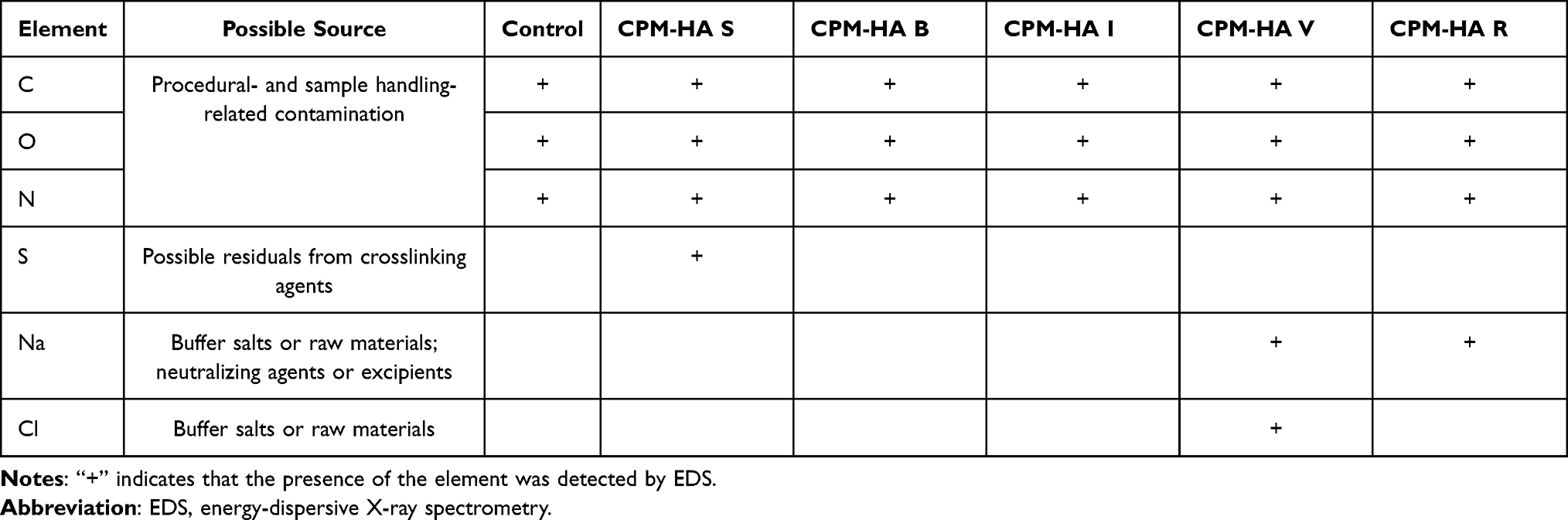 |
Table 2 Elemental Composition of Particles in CPM-HA Fillers Analyzed by Energy-Dispersive X-Ray Spectrometry (EDS) |
Histological Findings in Human Subjects
Histological evaluation of tissue samples from human subjects before and after the injection of CPM-HA S and CPM-HA R are presented in Figure 4. At baseline, both subjects exhibited normal dermal tissue architecture. Following the injection of both CPM-HA S and CPM-HA R, the HA fillers were observed to be homogenously integrated into the dermal layer. Examination of the 1-week and 4-week post-injection samples from both subjects revealed no significant inflammatory cell infiltration. There was an absence of notable lymphocytes, macrophages, or other inflammatory cell infiltrates around the injection sites. This was further confirmed by IHC analyses which revealed minimal CD68-positive staining around the implantation sites (Supplementary Figure 1). Overall, the findings were consistent with good tissue integration and a lack of significant inflammatory response over the 4-week observation period for both filler types.
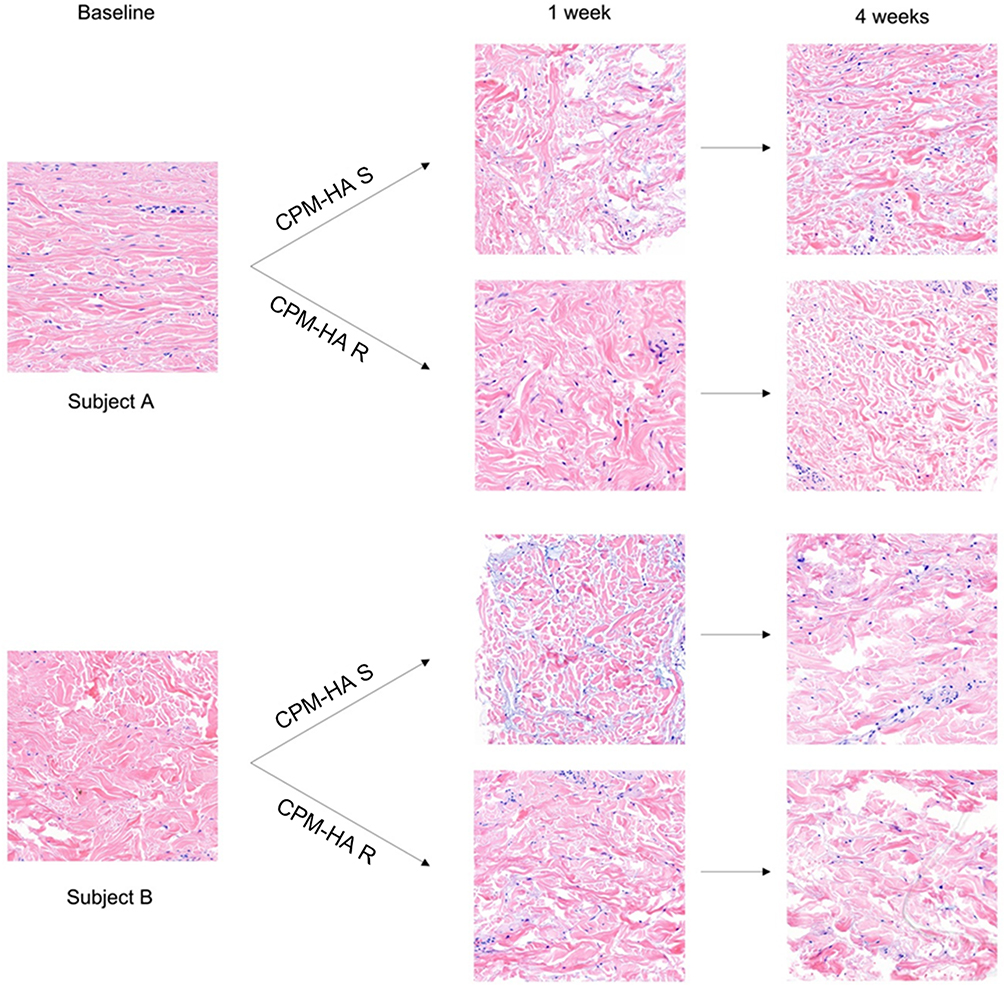 |
Figure 4 Histological evaluation of CPM-HA S and CPM-HA R fillers in human skin at baseline, 1-week and 4-weeks post-injection. Hematoxylin and eosin staining of skin biopsy specimens revealed no significant inflammatory response following intradermal injection of CPM-HA S and CPM-HA R. |
Discussion
This study provides a comprehensive investigation into the safety and biocompatibility profile of the CPM range of HA fillers by integrating physicochemical analysis with in vivo histological evaluation in human subjects. One key finding from our analysis was that the number of insoluble particles in the CPM-HA fillers fell well below the established pharmacopeial thresholds for injectable drugs (ie, <6000 particles of size ≥10 μm and <600 particles of size ≥25 μm per container). SEM/EDS analysis revealed the presence of expected manufacturing-related constituents, including sodium (Na), chloride (Cl) and sulfur (S).
Importantly, the study confirmed the absence of silicon (Si), iron (Fe), and aluminum (Al), which are associated with immunologically relevant particulate matter, and previously detected in other commercially available HA fillers.17 Literature suggests that contaminants encompassing such elements can act as danger signals, triggering local immune responses and inflammasome activation, contributing to the onset of DIRs. Downstream immunological effects may depend on the size, form or composition of these impurities, as previously summarized in Table 1. Silicon-based impurities may have distinct implications when present as silicone oil or silicon dioxide (silica). Silicone oil impurities are shown to induce proinflammatory cytokines (IL-6, IL-8, TNF-α) in human peripheral blood monocytes, and can adsorb proteins to form silicone-protein complexes enhancing immunogenicity.26 Notably, inflammatory reactions including foreign body granulomas in response to soft silicone gel or free silicone oil have been well documented in literature.27–29 Silicone oil, which is more likely to be present as droplets, is less likely to be detected by SEM-EDS as compared to silicon dioxide (silica). The uptake of crystalline silica by macrophages or dendritic cells can activate the inflammasome. If the silica particles are too large to be ingested (eg small glass fibres), resident macrophages will try to extend their membranes in an attempt to engulf the particles – these attempts of phagocytosis without result lead to a phenomena known as “frustrated phagocytosis”.30 Such conditions can keep resident macrophages in a permanently activated state, resulting in the constant release of reactive oxygen species and proinflammatory mediators and chronic inflammation.20
Iron, present in its elemental form (eg in steel abrasive) is not digestible, but may oxidize within the body to form iron oxide particles which can behave like a foreign body and initiate a foreign body response.22–24 Aluminum, in contrast, is rarely found in pure form in nature and typically exists as compounds with potent immunologic adjuvant properties. These compounds can enhance humoral immune responses and contributing to granulomatous inflammation upon persistent tissue exposure.31 Similar to silicon, aluminum hydroxides have been shown to directly activate the inflammasome not only in dendritic cells32 but also in resident and infiltrating macrophages.19 This is aligned with broader immunology literature wherein aluminum hydroxides are well-established as vaccine adjuvants due to their ability to induce inflammasome activation and robust Th2 immune responses.33
Considering the above immunological implications, it is conceivable that persistent adjuvant exposure in HA fillers could play a role in autoimmune/inflammatory syndrome induced by adjuvants (ASIA), which has previously been reported with aesthetic HA injections.34 Notably, ASIA was first described by Shoenfeld et al35 as a mechanism of adverse immune reactions after vaccination using aluminum compounds as an adjuvant.
Overall, the absence of potentially immunogenic particles in the CPM-HA range is a notable finding, which points toward an immunologically favorable profile. The encouraging physicochemical data were corroborated by our in vivo histological assessments. Examination of skin biopsies at 1- and 4-weeks post-injection with CPM-HA S and CPM-HA R demonstrated excellent tissue integration, with no evidence of significant inflammatory cell infiltrates, foreign body reactions, or granuloma formation. These data add evidence for the fillers’ biocompatibility in human tissue. Our findings are consistent with earlier reviews6 noting that foreign body reactions are unlikely to occur when optimal tissue integration is achieved, highlighting the biomimetic design of the CPM-HA fillers. Further, our data align with the real-world safety profile of the CPM-HA filler range. In a literature review examining the safety of 15 HA fillers, CPM-HA fillers were found to have no reports of delayed adverse reactions.36 Ultimately, safety should be considered as an underlying tenet to the achievement of desired natural results with HA fillers, as complications can impact underlying elements (eg visual, tactile, sensory and expressive elements) to defining such outcomes. Taken together, our results highlight the importance of greater scrutiny when evaluating fillers, underscoring the clinician’s role to consider not only HA composition, but also the purity of the formulation when evaluating risk of immune-mediated complications.
One strength of our study is the incorporation of in vivo histological analyses to corroborate with physicochemical analysis. While SEM/EDS and insoluble particulate counter provide valuable quantitative and qualitative data (morphology, distribution and elemental identity) relating to insoluble impurities, in vivo histological studies enable further evaluations in a biologically relevant setting that reflects clinical practice. We acknowledge that the duration of our study could be a limitation to capture effects over a longer period of time and may not sufficiently account for delayed presentations of inflammatory reactions which can often take months to occur. The in vivo assessments were performed only in two subjects to obtain descriptive assessments of filler integration, while minimizing the extent of invasive biopsy procedures. Nevertheless, our descriptive findings provide an important preliminary indication of the favorable tissue response and biocompatibility of these formulations. With respect to the SEM/EDS method, while it can identify elemental isotopes present in the filler, it is unable to evaluate the type of compounds that are present, thereby constraining our ability to fully interpret the identity of these elemental impurities. Considering the possible presence of protein aggregates or even carbohydrates, it may be valuable to incorporate other enzymes (eg proteases) to break down such macromolecules for further analysis.
Overall, future efforts could look to examining outcomes over a longer period and employing other physicochemical analytic methods that could differentiate between compounds of a similar elemental composition.
Conclusion
This study confirms that the CPM-HA range dermal fillers possess low levels of insoluble particles that fall far below stringent injectable drug impurity thresholds, and no elemental impurities of concern were identified. In in vivo analyses, the CPM-HA range of fillers demonstrated good tissue biocompatibility at 1-week and 4-weeks after placement, without evidence of inflammatory or granulomatous responses in human skin. The findings from these integrated analyses underscore the critical importance of advanced manufacturing and purification standards. For clinicians and patients, this data provides reassurance regarding the safety of the CPM-HA range and reinforces the principle that selecting high-purity fillers is fundamental to achieving predictable, safe, and natural-looking aesthetic outcomes.
Abbreviations
ASIA, autoimmune/inflammatory syndrome induced by adjuvants; CPM, cohesive polydensified matrix; DIR, delayed inflammatory reactions; HA, hyaluronic acid; SEM, scanning electron microscopy; SD, standard deviation; TEM, Transmission Electron Microscopy; UPW, Ultrapure water; USP, United States Pharmacopeia.
Ethical Statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) of Yonsei University, Republic of Korea (IRB No. CR 325309). All participants provided written informed consent for study participation and data publication.
Acknowledgments
The authors are grateful to the volunteers who have participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a research grant by Merz Asia Pacific Pte Ltd.
Disclosure
Solam Lee has no relevant conflicts of interest to disclose. Clifton Tay is an employee of Merz Asia Pacific Pte. Ltd. Michael Uwe Martin serves as an ad hoc consultant and speaker for Merz Pharma GmbH & Co., KGaA. Jimyung Seo serves as a speaker and consultant for Merz Aesthetics.
References
1. Salih ARC, Farooqi HMU, Amin H, Karn PR, Meghani N, Nagendran S. Hyaluronic acid: comprehensive review of a multifunctional biopolymer. Future J Pharm Sci. 2024;10(1):63. doi:10.1186/s43094-024-00636-y
2. Kogan G, Soltés L, Stern R, et al. Hyaluronic acid: a natural biopolymer with a broad range of biomedical and industrial applications. Biotechnol Lett. 2007;29(1):17–11. doi:10.1007/s10529-006-9219-z
3. Tran C, Carraux P, Micheels P, et al. In vivo bio-integration of three hyaluronic acid fillers in human skin: a histological study. Dermatology. 2014;228(1):47–54. doi:10.1159/000354384
4. Hong GW, Wan J, Park Y, et al. Manufacturing process of hyaluronic acid dermal fillers. Polymers. 2024;16(19):2739. doi:10.3390/polym16192739
5. Corduff N, Juniarti L, Lim TS, et al. Current practices in hyaluronic acid dermal filler treatment in Asia Pacific and practical approaches to achieving safe and natural-looking results. Clin Cosmet Invest Dermatol. 2022;15:1213–1223. doi:10.2147/CCID.S363583
6. Funt DK. Treatment of delayed-onset inflammatory reactions to hyaluronic acid filler: an algorithmic approach. Plast Reconstr Surg Glob Open. 2022;10(6):e4362. doi:10.1097/GOX.0000000000004362
7. Landau M, Silikovich F, Fida M, Cartier H, Kroumpouzos G. Oral methotrexate treatment of delayed-onset inflammatory reactions to dermal fillers. Aesthetic Surg J Open Forum. 2024;6:ojae011. doi:10.1093/asjof/ojae011
8. Lee W, Shah-Desai S, Rho NK, Cho J. Etiology of delayed inflammatory reaction induced by hyaluronic acid filler. Arch Plast Surg. 2024;51(01):020–026. doi:10.1055/a-2184-6554
9. Artzi O, Loizides C, Verner I, Landau M. Resistant and recurrent late reaction to hyaluronic acid–based gel. Dermatol Surg. 2016;42(1):31–37. doi:10.1097/DSS.0000000000000562
10. Litwiniuk M, Krejner A. Hyaluronic acid in inflammation and tissue regeneration. Wounds. 2016;28(3):78–88.
11. Rayahin JE, Buhrman JS, Zhang Y, Koh TJ, Gemeinhart RA. High and low molecular weight hyaluronic acid differentially influence macrophage activation. ACS Biomater Sci Eng. 2015;1(7):481–493. doi:10.1021/acsbiomaterials.5b00181
12. Pérez-Pérez L, García-Gavín J, Wortsman X, Santos-Briz Á. Delayed adverse subcutaneous reaction to a new family of hyaluronic acid dermal fillers with clinical, ultrasound, and histologic correlation. Dermatol Surg. 2017;43(4):605–608. doi:10.1097/DSS.0000000000000945
13. Wollina U, Goldman A, Kocic H, Andjelkovic T, Bogdanovic D, Kokić IK. Impurities in hyaluronic acid dermal fillers? A narrative review on nonanimal cross-linked fillers. Facial Plast Surg Aesthetic Med. 2024;26(2):190–194. doi:10.1089/fpsam.2023.0294
14. Rho NK, HS K, SY K, Lee W. Injectable “skin boosters” in aging skin rejuvenation: a current overview. Arch Plast Surg. 2024;51(06):528–541. doi:10.1055/a-2366-3436
15. La Gatta A, Aschettino M, Stellavato A, et al. Hyaluronan hydrogels for injection in superficial dermal layers: an in vitro characterization to compare performance and unravel the scientific basis of their indication. Int J Mol Sci. 2021;22(11):6005. doi:10.3390/ijms22116005
16. Nguyen AV, Soulika AM. The dynamics of the skin’s immune system. Int J Mol Sci. 2019;20(8):1811. doi:10.3390/ijms20081811
17. Lee W, Rho NK, Yang EJ. Determination of hyaluronic acid dermal filler impurities using SEM/EDS analysis. Polymers. 2023;15(7):1649. doi:10.3390/polym15071649
18. Melo GB, Shoenfeld Y, Rodrigues EB. The risks behind the widespread use of siliconized syringes in the healthcare practice. Int J Retina Vitreous. 2021;7(1). doi:10.1186/s40942-021-00338-0
19. Hornung V, Bauernfeind F, Halle A, et al. Silica crystals and aluminum salts activate the NALP3 inflammasome through phagosomal destabilization. Nat Immunol. 2008;9(8):847–856. doi:10.1038/ni.1631
20. Marrocco A, Ortiz LA. Role of metabolic reprogramming in pro-inflammatory cytokine secretion from LPS or silica-activated macrophages. Front Immunol. 2022;13:936167. doi:10.3389/fimmu.2022.936167
21. Pollard KM. Silica, silicosis, and autoimmunity. Front Immunol. 2016;7. doi:10.3389/fimmu.2016.00097
22. Shah A, Dobrovolskaia MA. Immunological effects of iron oxide nanoparticles and iron-based complex drug formulations: therapeutic benefits, toxicity, mechanistic insights, and translational considerations. Nanomedicine. 2018;14(3):977–990. doi:10.1016/j.nano.2018.01.014
23. Rubianes EI, Sánchez JL. Granulomatous dermatitis to iron oxide after permanent pigmentation of the eyebrows. J Dermatol Surg Oncol. 1993;19(1):14–16. doi:10.1111/j.1524-4725.1993.tb03324.x
24. Vermeij EA, Koenders MI, Bennink MB, et al. The in-vivo use of superparamagnetic iron oxide nanoparticles to detect inflammation elicits a cytokine response but does not aggravate experimental arthritis. Cunha TM, ed. PLoS One. 2015;10(5):e0126687. doi:10.1371/journal.pone.0126687
25. United States Pharmacopeia. USP <788> particulate matter in injections. In: United States Pharmacopeia and National Formulary (USP–NF). Rockville, MD: United States Pharmacoial Convention; 2021.
26. Krayukhina E, Yokoyama M, Hayashihara KK, et al. An assessment of the ability of submicron- and micron-size silicone oil droplets in dropped prefillable syringes to invoke early- and late-stage immune responses. J Pharm Sci. 2019;108(7):2278–2287. doi:10.1016/j.xphs.2019.02.002
27. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241–258. doi:10.1016/j.semarthrit.2013.02.001
28. Lee JM, Kim YJ. Foreign body granulomas after the use of dermal fillers: pathophysiology, clinical appearance, histologic features, and treatment. Arch Plast Surg. 2015;42(02):232–239. doi:10.5999/aps.2015.42.2.232
29. Wang LL, Thomas WW, Friedman O. Granuloma formation secondary to silicone injection for soft-tissue augmentation in facial cosmetics: mechanisms and literature review. Ear Nose Throat J. 2018;97(1–2):E46–E51. doi:10.1177/0145561318097001-211
30. Baranov MV, Kumar M, Sacanna S, Thutupalli S, Van Den Bogaart G. Modulation of immune responses by particle size and shape. Front Immunol. 2021;11:607945. doi:10.3389/fimmu.2020.607945
31. Laera D, HogenEsch H, O’Hagan DT. Aluminum adjuvants—’back to the future. Pharmaceutics. 2023;15(7):1884. doi:10.3390/pharmaceutics15071884
32. Li H, Nookala S, Re F. Aluminum hydroxide adjuvants activate caspase-1 and induce IL-1β and IL-18 release. J Immunol. 2007;178(8):5271–5276. doi:10.4049/jimmunol.178.8.5271
33. HogenEsch H. Mechanisms of stimulation of the immune response by aluminum adjuvants. Vaccine. 2002;20 Suppl 3:S34-39. doi:10.1016/s0264-410x(02)00169-x
34. Owczarczyk-Saczonek A, De Boulle K. Hyaluronic acid fillers and Asia syndrome: case studies. Clin Cosmet Invest Dermatol. 2023;16:2763–2771. doi:10.2147/CCID.S419716
35. Shoenfeld Y, Agmon-Levin N. ‘ASIA’ – autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmune. 2011;36(1):4–8. doi:10.1016/j.jaut.2010.07.003A
36. Kokoska RE, Lima AM, Kingsley MM. Review of delayed reactions to 15 hyaluronic acid fillers. Dermatol Surg. 2022;48(7):752–757. doi:10.1097/DSS.0000000000003473
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.