Back to Journals » Patient Preference and Adherence » Volume 20
Exploring the Effect of Doctor-Nurse Collaboration on Overall Satisfaction Among the Older Patients: A Moderated Mediation Model of Responsiveness and Environment
Authors Wang H, Wang H, Guan SN, Li J
Received 6 November 2025
Accepted for publication 14 January 2026
Published 1 February 2026 Volume 2026:20 577575
DOI https://doi.org/10.2147/PPA.S577575
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Huilin Wang,1,2 Hao Wang,1 Si nan Guan,2 Jing Li1
1Outpatient Department of Peking University First Hospital, Beijing, People’s Republic of China; 2School of Nursing, Peking University, Beijing, People’s Republic of China
Correspondence: Jing Li, Outpatient Department of Peking University First Hospital, Xishiku Road, Xicheng District, Beijing, 100034, People’s Republic of China, Tel/Fax +86 010-83572020, Email [email protected]
Objective: Older patients often encounter challenges during outpatient visits that adversely affect their overall satisfaction. This study tested a moderated mediation model to examine how doctor-nurse collaboration influences satisfaction through responsiveness to patient needs, and how the outpatient environment moderates this process within geriatric care settings.
Methods: An online cross-sectional survey utilizing a 5-point Likert scale was conducted to assess patient satisfaction by recruiting 9133 older patients (51.6% male). Descriptive statistics were used to analyze the factors associated with satisfaction. After controlling for confounders such as title of registered doctor, gender, and educational status, a moderated mediation analysis was performed using Stata 18.0.
Results: Both dimensions of doctor-nurse collaboration, interprofessional collaboration (X1) and attitudinal alignment (X2), directly enhanced patient satisfaction (β = 0.065, p < 0.001). Responsiveness to patient needs mediated this relationship (β = 0.253, p < 0.001). The outpatient environment significantly moderated the effect of collaboration on responsiveness in both the model1 (β = 0.288, p < 0.001) and the model2 (β = 0.289, p < 0.001).
Conclusion: Effective collaboration between doctors and nurses is essential for addressing the professional and emotional needs of older patients, thereby improving their overall satisfaction. Moreover, integrating the outpatient environment into the doctor-patient collaboration model highlights the importance of considering physical settings and interpersonal dynamics as interrelated components to comprehensively understand patient satisfaction and its determinants.
Keywords: older patients, doctor-nurse collaboration, responsiveness to patient needs, outpatient environment, overall satisfaction, moderated mediation model
Introduction
The World Social Report 2023 indicates that the global population of older adults continues to grow, and the number of people aged 65 and over is projected to increase from 761 million in 2021 to 1.6 billion by the mid-century.1 Alongside the increasing elderly population, multimorbidity and comorbidity will become more prevalent, and age-related declines in sensory perception will often impede older adults’ ability to access healthcare, leading to greater difficulties in interacting with medical staff.2 These challenges underscore the growing demand for professional care and emotional support for older patients.
Outpatients constitute a critical component of the healthcare system worldwide.3 In China, outpatient visits reached an estimated 9.55 billion in 2023, reflecting a year-on-year increase of 13.5%, with older patients accounting for a substantial proportion of these visits.4 Given the specific characteristics of older patients mentioned above, to enhance the efficiency of outpatient visits, satisfaction, referring to patient assessments of care quality and the clinical encounter, serves as a critical indicator of patient experience and a driver of continuous service improvement.5 Prior studies suggest that the overall satisfaction of older patients is influenced by the service provided by doctors and nurses, and may also vary with their mood within the healthcare environment.6,7 Additionally, from the patient’s perspective, whether their needs are met responsively is an important consideration as well.8 Understanding these interconnected factors is therefore crucial for improving overall satisfaction among older patients.
Doctor-nurse collaboration facilitates effective healthcare delivery for older patients.9 It comprises two key elements.9 Involving joint development of diagnosis, treatment, and nursing plans to promote patient recovery, interprofessional collaboration as “doctor explained why and how to use medicine” and “nurses answer the questions correctly” is a key component of doctor-nurse collaboration centered on patient-focused analysis of conditions.10 Substantial evidence underscores the role of effective interprofessional collaboration and clear explanations in delivering high-quality care, which in turn promotes patient safety and enhances satisfaction.11 Encompassing “communication of diagnosis” and “behavior of nurses”, attitudinal alignment constitutes another fundamental dimension of doctor-nurse collaboration. Studies indicate that mutual respect, trust, and efficient communication between doctors and nurses improve responsibility sharing and therapeutic decision making, which entails the ability to communicate with patients in a clear and patient manner.12,13 Additionally, research from a psychological perspective further corroborates the finding that positive communication behaviors and attitudes directly increase patient satisfaction.14 Therefore, this study examined the hypothesis that doctor-nurse collaboration (including interprofessional collaboration and attitudinal alignment) directly affects the overall satisfaction of older patients.
Responsiveness to patient needs refers to the capability of healthcare providers to address patients’ requests or complaints in a timely and effective manner, thereby achieving expected treatment goals.15 Drawing on the SERVQUAL model proposed by Parasuraman, the dimension of “responsiveness” is defined as the willingness of service providers to understand and fulfill individual needs, ultimately contributing to higher patient satisfaction.16 Within this framework, Kashfi17 found that clinical service such as doctors’ behavior, attitude of medical staff play a critical role in shaping the dimensions of “responsiveness” and “empathy”. Similar findings were reported in a study conducted in Africa.18 Furthermore, guided by the 4M framework, the internationally recognized Age-Friendly Health System encourages health care providers to identify the priorities of older patients and focus on addressing their core needs, which has been demonstrated to improve both patient experience and satisfaction.19 Consequently, based on insights from existing research, as the delivery of responsive care is largely dependent on healthcare providers, this study aimed to investigate the mediating role of responsiveness to patient needs in the relationship between doctor-nurse collaboration and overall satisfaction.
The outpatient environment encompasses multiple dimensions such as ventilation, temperature, cleanliness, and maintenance of medical order, representing a comprehensive physical and humanistic environment that integrates space, processes, facilities, services, and management.20 A comfortable environment has been shown to improve the patient experience, increase tolerance for waiting times, and positively influence emotional responses and satisfaction.21,22 A study based on the annual National Public Hospital Patient Satisfaction Survey (NPHPSS) indicated that outpatient satisfaction lags behind inpatient satisfaction, with environmental quality being identified as a significant moderating factor.23 Research from Jiangxi Province found that the environment and facilities positively affect patient satisfaction, exhibiting a positive synergistic effect with quality-of-care indicators such as communication regarding diagnosis, explanation of examination reports, and respect for privacy.24 This relationship is also corroborated by a study from the United States, which emphasizes that collaborative healthcare teams depend on an effective care environment to support patient health and satisfaction.25 Accordingly, this study explored the moderating role of the outpatient environment. In this study, although the outpatient environment is conceptually multidimensional, this study employed a single-item global measure (eg, “satisfaction with the outpatient environment”) to represent the broader construct. This approach is supported by prior studies,23,26 which indicate that global assessments adequately represent overall environmental quality and enable a holistic examination of its role in patient satisfaction.
Although previous studies have examined the independent effects of doctor-nurse collaboration, responsiveness to patient needs, and outpatient environment on patient satisfaction, there remains a scarcity of research on the interactions between these three factors.24 Additionally, the synergistic effects of interpersonal interactions (ie, between doctors and nurses) and the influence of environmental factors during this period have been mentioned less frequently.27 Moreover, moderated mediation analyses targeting older patients, a group potentially facing healthcare access challenges for outpatients, have not been fully explored. Accordingly, this study innovatively integrated both mediating and moderating variables to conduct an in-depth analysis of the impact of doctor-patient collaboration on satisfaction among older patients into a path model. Based on the above, this study examines the following hypotheses:
Hypothesis 1: Doctor-nurse collaboration (interprofessional collaboration and attitudinal alignment) directly affects overall satisfaction. Hypothesis 2: Responsiveness to patient needs significantly mediates the effects of doctor-nurse collaboration (interprofessional collaboration and attitudinal alignment) on overall satisfaction. Hypothesis 3: The outpatient environment significantly moderates the effect of doctor-nurse collaboration (interprofessional collaboration and attitudinal alignment) and overall satisfaction.
The findings of this study not only provide a novel perspective for outpatient satisfaction but also offer practical guidance for understanding the healthcare needs of older patients. The results will assist hospital managers in considering that doctor-nurse collaboration enhances patient satisfaction by promptly addressing the needs of older patients, while a favorable clinical environment helps strengthen this effect. The hypothesized path model is depicted in Figure 1: “a1” and “a2” denote the hypothesized paths from the independent variables (X1, X2) to the mediator (responsiveness of patient needs); “b” signifies the path from the mediator to the dependent variable (overall satisfaction), while “c1” and “c2” represent the direct paths from the independent variables to the dependent variable; “w1” and “w2” correspond to the hypothesized moderating effects of the outpatient environment on the “a1” and “a2” paths, respectively.
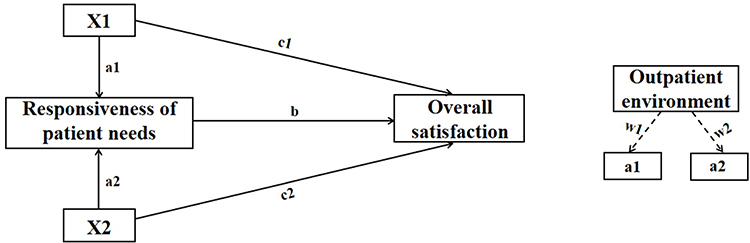 |
Figure 1 Research hypothesis model diagram. Notes: X1 represents interprofessional collaboration, and X2 represents attitudinal alignment. Paths a1 and a2 denote the hypothesized effects from the independent variables (X1, X2) to the mediator (responsiveness to patient needs). Path b signifies the effect from the mediator to the dependent variable (overall satisfaction), while c1 and c2 represent the direct effects from the independent variables to the dependent variable. Labels w1 and w2 correspond to the hypothesized moderating effects of the outpatient environment on paths a1 and a2, respectively. |
Methods
Study Sample
This study utilized a simple random sampling method based on Wenjuanxing, a prominent online questionnaire service in China, to conduct a cross-sectional study from June to July 2025 in the outpatient department of a tertiary hospital to assess patient satisfaction among older patients. Collected data were retrieved from an online analysis system. Altogether 9520 patients consented to participate in this study, and we successfully collected 9133, yielding a high response rate of 95.93%. According to the inclusion criteria, each patient (1) was 60 years or older, (2) was cognitively able to complete the questionnaire, (3) was admitted to the outpatient department, and (4) provided informed consent and willing to participate in the investigation. We excluded patients with severe conditions and/or infectious diseases that may cause danger to themselves or others.
This study has certain limitations. Self-reported measures may introduce bias, as participants could overstate positive experiences. Furthermore, the online survey design may have excluded older patients without internet access, limiting the generalizability of the findings. Future research should aim to incorporate objective measures and employ broader recruitment strategies.
Measures
Instrument and Scaling
Building on prior validated instruments in this field,27,28 the questionnaire was not newly devised; its items were refined by incorporating expert feedback and aligning with the established questionnaires (Supplementary Material 2). And the original Chinese version is available in Supplementary Material 1. This questionnaire includes 33 items grouped into three sections: (1) demographic characteristics; (2) core healthcare process; (3) satisfaction evaluation system of medical experience. Patient satisfaction was rated on a 5-point Likert scale (1 = “very dissatisfied”, 5 = “very satisfied”) with higher scores indicating higher level of satisfaction. The duration of filling out this online questionnaire was approximately five – eight minutes. In this study, Cronbach’s alpha was 0.969, the KMO measure was 0.963, and the χ2 value of Bartlett’s test of sphericity was 6,717,92.782 (p < 0.001), indicating excellent internal consistency.
Data Coding
Gender was a binary variable and categorized into two groups: 1 = female and 0 = male. Respondents aged 60 years and above: 60–80 = 0, > 80 = 1. Education status was an ordinal variable and was delineated as follows: 0 = high school and below, 1 = undergraduate/junior college, and 2 = postgraduate and above. Registered physician’s title had three categories: senior resident = 0; associate chief physician = 1; and chief physician = 2. Patient source: non-local patients = 0; local patients = 1. Payment method: 0 = no medical insurance; 1 = medical insurance. Type of outpatient registration had two categories: general outpatient = 0; VIP outpatient = 1. Satisfaction items, for example, doctor explained why and how to use medicine, doctor diagnosed diseases, responsiveness of patient needs, outpatient environment, behaviour of nurses, and nurses answer the questions correctly were all measured on the 5-point Likert scale.
Variable Definitions
To test the hypotheses proposed in our moderated mediation model, key variables were operationalized as follows. Specifically, the interaction terms were constructed by multiplying the corresponding items derived from the questionnaire (eg, doctor explained why and how to use medicine, nurses answer the questions correctly).
- Independent Variables (X): it is represented by two distinct latent interaction terms, X1 and X2.
- X1 (interprofessional collaboration): doctor explained why and how to use medicine × nurses answer the questions correctly. This pairing captures the dynamic interaction inherent in interprofessional collaboration, where effective professional service arises from doctor’s clear explanations and nurse’s accurate responses to clinical inquiries, thereby serving as a metric for the synergistic effect of the professional level delivered by healthcare providers.
- X2 (attitudinal alignment): how doctors communicate a diagnosis × satisfaction with behaviour of nurses. It reflects the attitudinal dimension, shaped by the doctor’s communication style and the nurse’s etiquette norms, thereby capturing the synergistic effect of healthcare providers’ communication skills and overall demeanor.
- Mediator (M): responsiveness to patient needs. This term indicates whether patient needs are acknowledged and addressed in a timely manner by the healthcare staff.
- Moderator: outpatient environment. It mainly refers to the physical facilities and service environment experienced by patients in the hospital. In this study, outpatient environment functions as a moderator between doctor-nurse collaboration (X1, X2) and patient satisfaction (Y). Specifically, a supportive environment is likely to strengthen this positive relationship, whereas a poor environment may weaken it.
- Dependent Variable (Y): overall satisfaction. This term captures the patient’s overall assessment of the outpatient visit.
Control Variables
The control variables in this study included gender, educational status, and registered physician’s title.
Statistical Analyses
Descriptive statistics using SPSS (version 27.0) were applied to present the characteristics of the 9133 respondents. Data analysis was conducted using Stata 18.0, with a significance level set at 0.05. We employed path analysis with maximum likelihood estimation to test the hypothesized moderated mediation model. The significance of indirect effects was evaluated using bias-corrected bootstrap confidence intervals based on 5000 samples. We also assessed potential multicollinearity by examining variance inflation factors (VIFs). Finally, robustness tests were conducted to examine the stability of the model when the sample size was reduced to 8000 or when additional control variables were included.
Quality Control
In this study, data were collected by a team of six researchers, all of whom had received standardized training before conducting the survey. To verify the reliability and stability of the results, this study examined the robustness of the model by reducing the sample size to 8000 and incorporating additional moderating variables. Prior to the questionnaire, participants were informed of the research objectives and completed the informed consent process to assure data confidentiality.
Results
Demographic Characteristics of Older Patients in Outpatient
In total, 9133 older patients were included in this study (Table 1). Of the participants, 51.6% were male. Nearly half of the respondents had an undergraduate or junior college degree (56.7%). A total of 38.3% sought care from an associate-chief physician. Most of the participants (86.5%) had health insurance.
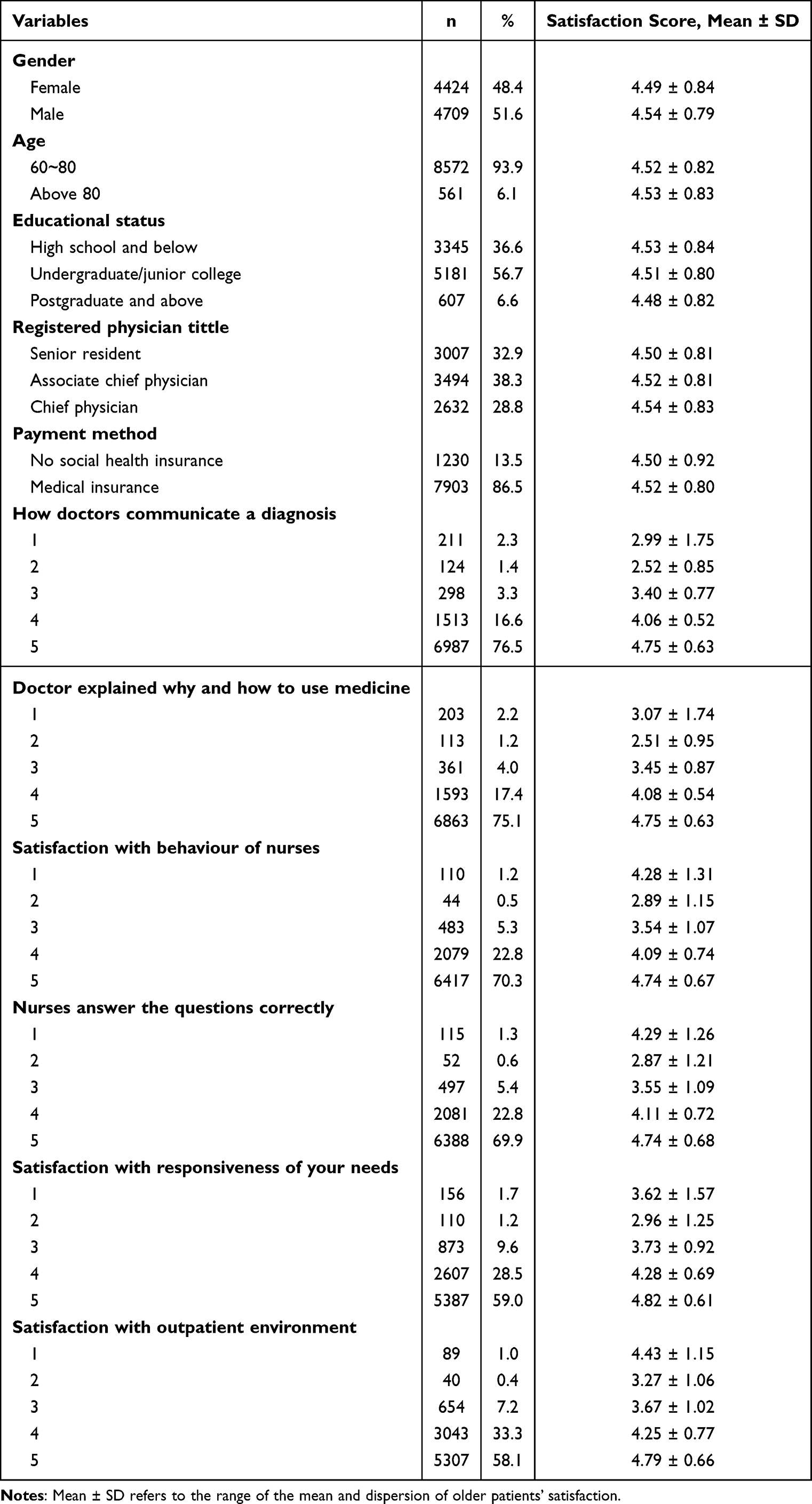 |
Table 1 Descriptive Characteristics of the Respondents (n = 9133) |
Correlation Analysis
Before conducting the moderated mediation analysis, we assessed the Pearson correlation coefficients among the variables to examine their interrelationships. This preliminary step focused on the key variables (defined in Section “2.2.3 Variable Definitions”) outlined in the proposed model. Specifically, we tested the correlations between: (1) interprofessional collaboration and responsiveness to patient needs; (2) attitudinal alignment and responsiveness to patient needs; (3) responsiveness to patient needs and overall satisfaction; (4) outpatient environment and responsiveness to patient needs; (5) outpatient environment and overall satisfaction.
As shown in Table 2, all core variables demonstrated significant positive correlations, detailed as follows: (1) interprofessional collaboration was significantly positively correlated with responsiveness to patient needs (r = 0.689, p < 0.01); (2) attitudinal alignment was strongly correlated with responsiveness to patient needs (r = 0.688, p < 0.01); (3) responsiveness to patient needs exhibited a strong positive correlation with overall satisfaction (r = 0.486, p < 0.01); (4) outpatient environment was also positively correlated with both responsiveness to patient needs (r = 0.745, p < 0.01) and overall satisfaction (r = 0.384, p < 0.01).
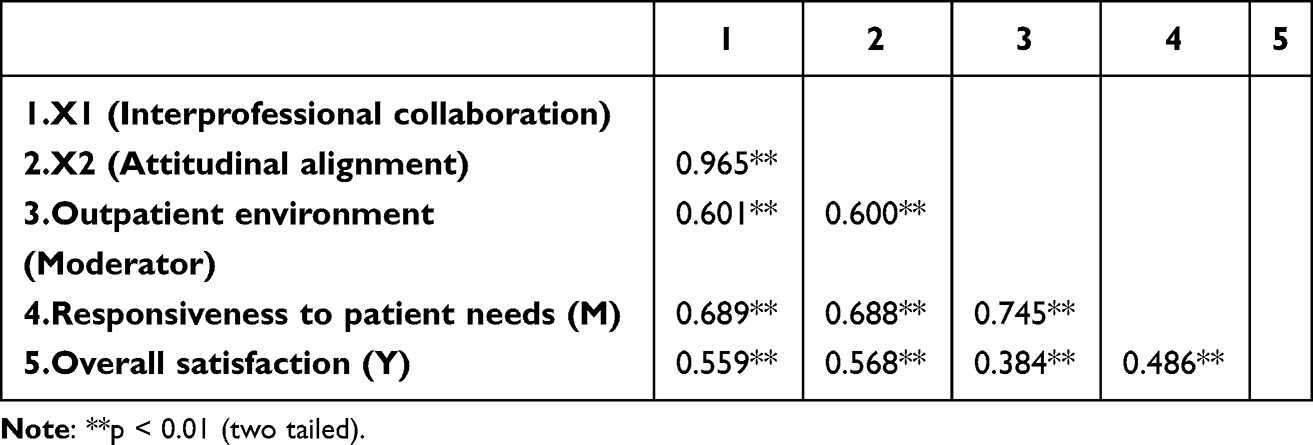 |
Table 2 Spearman Rank-Order Correlations Among Key Variables |
Testing the Direct Effect of X1 and X2 on Overall Satisfaction
The first research question aimed to establish a direct-effect model for X1 and X2 on overall satisfaction. After controlling for gender, educational status, and title of registered doctor, the results (Table 3) indicated that the path coefficients of X1 and X2 were 0.647 (p < 0.001) and 0.648 (p < 0.001), respectively, demonstrating that the direct effects of X1 and X2 on overall satisfaction were statistically significant and suitable for the mediating effect analysis. This finding supports Hypothesis 1.
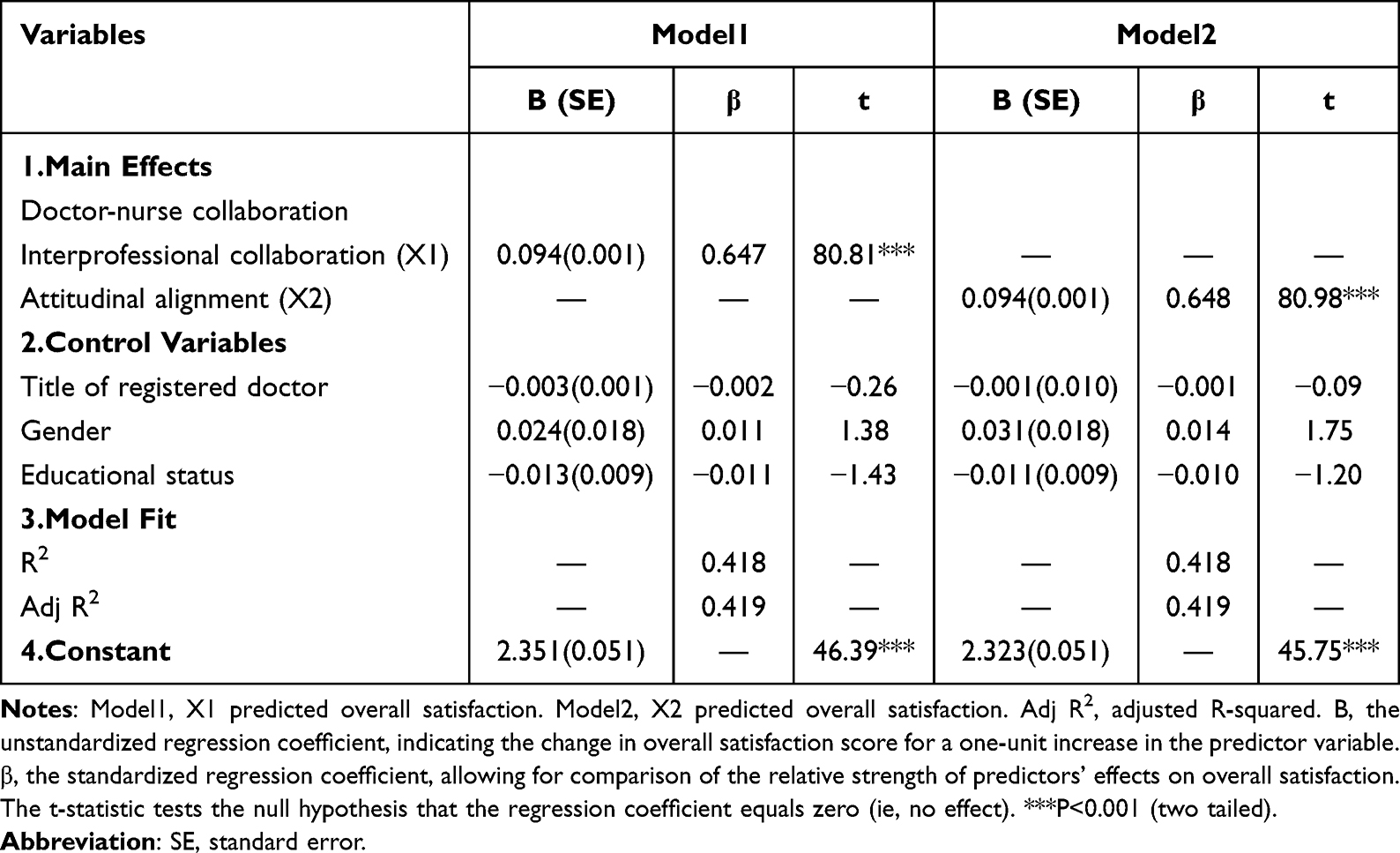 |
Table 3 The Regression Analyses Predicting Overall Satisfaction (n = 9133) |
Mediating Role of Responsiveness to Patient Needs
Table 4 indicates that X1 is significantly relationship to overall satisfaction (β = 0.065, p < 0.001), and responsiveness to patient needs partially mediates a positive relationship between X1 and overall satisfaction (β = 0.029, p = 0.005), indicating that professional collaboration between doctors and nurses leads to higher patient satisfaction, both directly and indirectly, through the mediating pathway of response to patient needs. The direct influence of X2 on overall satisfaction, coupled with its indirect influence mediated through responsiveness to patient needs, was assessed using bootstrap 95% confidence intervals, which were (0.063 and 0.068) for the direct effect, and (0.027 and 0.031) for the indirect effect, respectively. Significantly, both intervals notably exclude 0, thereby confirming that X2 impacts overall satisfaction not only in a direct manner but also indirectly through responsiveness to patient needs. These results are consistent with Hypothesis 2. X1 and X2 were positively related to responsiveness to patient needs (Î 2 = 0.114, p < 0.001). Responsiveness to patient needs was positive associated with overall satisfaction (Î 2 = 0.253, p < 0.001).
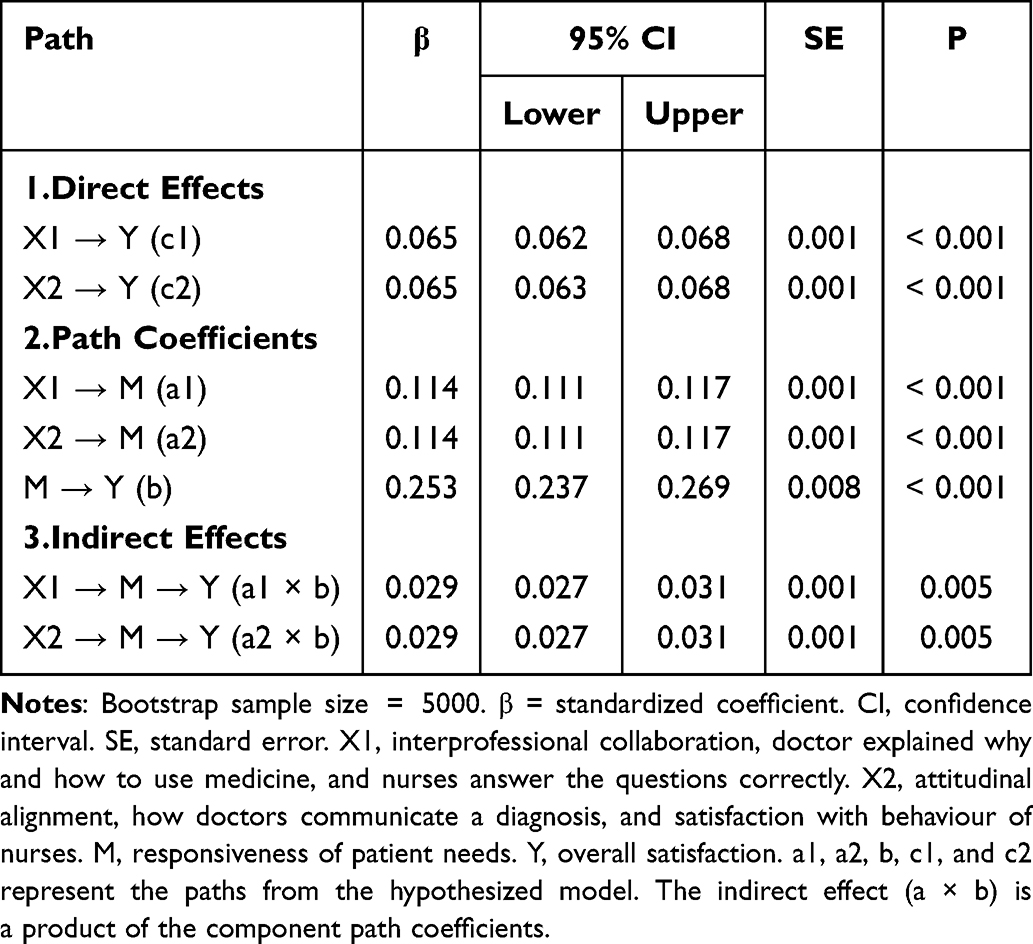 |
Table 4 Multilevel Path Analysis Results of Responsiveness to Patient Needs |
Testing the Moderated Effects of Outpatient Environment
To test this hypothesis, overall satisfaction was used as a dependent variable, whereas X1 and X2 were treated as independent variables. As shown in Table 5, after controlling for gender, educational status, and title of registered doctor, none of the interactions were significant except in the outpatient environment. Although educational status did not show statistically significant effects on overall satisfaction (p > 0.05), we retained it in the model based on the absence of new evidence demonstrating a lack of correlation between them. The analysis demonstrated that the outpatient environment had a significant and positive (β = 0.288, p < 0.001, X1; β = 0.289, p < 0.001, X2) moderating effect on the relationship between X1/X2 and outcome. Thus, Hypothesis 3 is supported. The model also showed a good fit for each moderated independent variable.
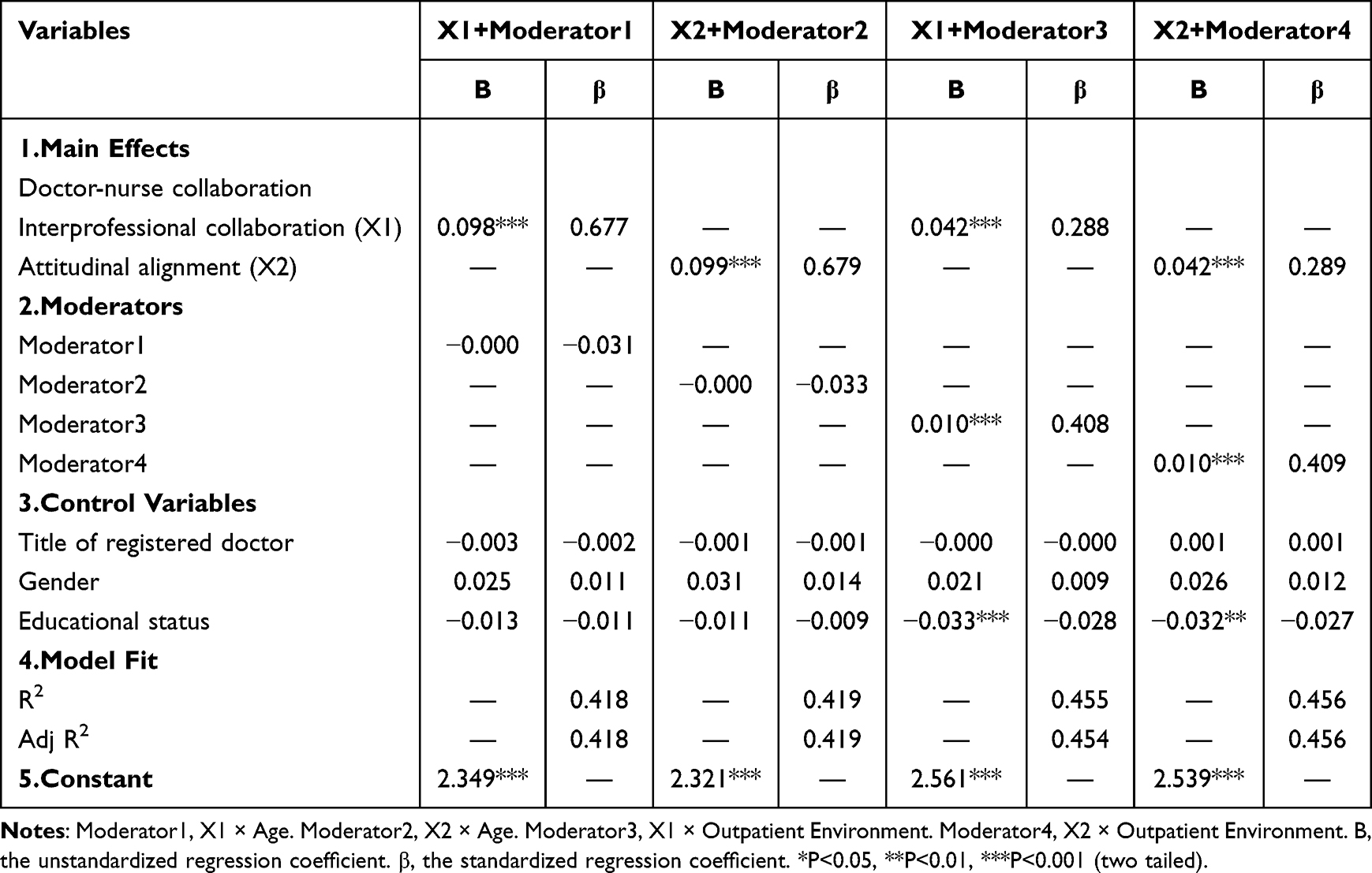 |
Table 5 Moderating Effects of Outpatient Environment on the Outcome |
Multicollinearity Analysis Among the Independent Variables
Multicollinearity is used to identify excessive intercorrelations among independent variables within a multiple linear regression framework, thereby avoiding estimator perturbations and instability. Prevalent scholarly conventions posit that a VIF exceeding five necessitates caution, and a VIF exceeding 10 is diagnostic of pronounced multicollinearity, mandating rectifying actions. A tolerance statistic falling below 0.1 is conventionally interpreted as evidence of substantial collinearity, prompting the elimination or consolidation of the affected variables. A mean VIF value of 2.08 is significantly lower than the threshold of 5, is typically used to indicate substantial multicollinearity concerns. Similarly, the calculated tolerance level of 0.48 is considerably higher than the conventional minimum standard of 0.10. These results suggest that there are no multicollinearity issues in our model.
Testing the Robustness of the Moderated Mediation Model
The robustness of the moderated mediation model employed in this study was substantiated by the following aspects; the results are shown in Table 6:
- Regarding the main effects, the coefficients remain statistically significant at the 1% level (B = 0.095, p < 0.001, after sample reduction to 8000; B = 0.094, p < 0.001, after incorporating additional control variables), demonstrating consistency with original Model1 and Model2.
- For the mediator, the effect estimates exhibited remarkable stability across the altered model specifications, with variations not exceeding 0.004 (p < 0.001).
- For the control variables, all variables showed consistently small and statistically insignificant coefficients in all models, indicating a negligible influence on the dependent variable.
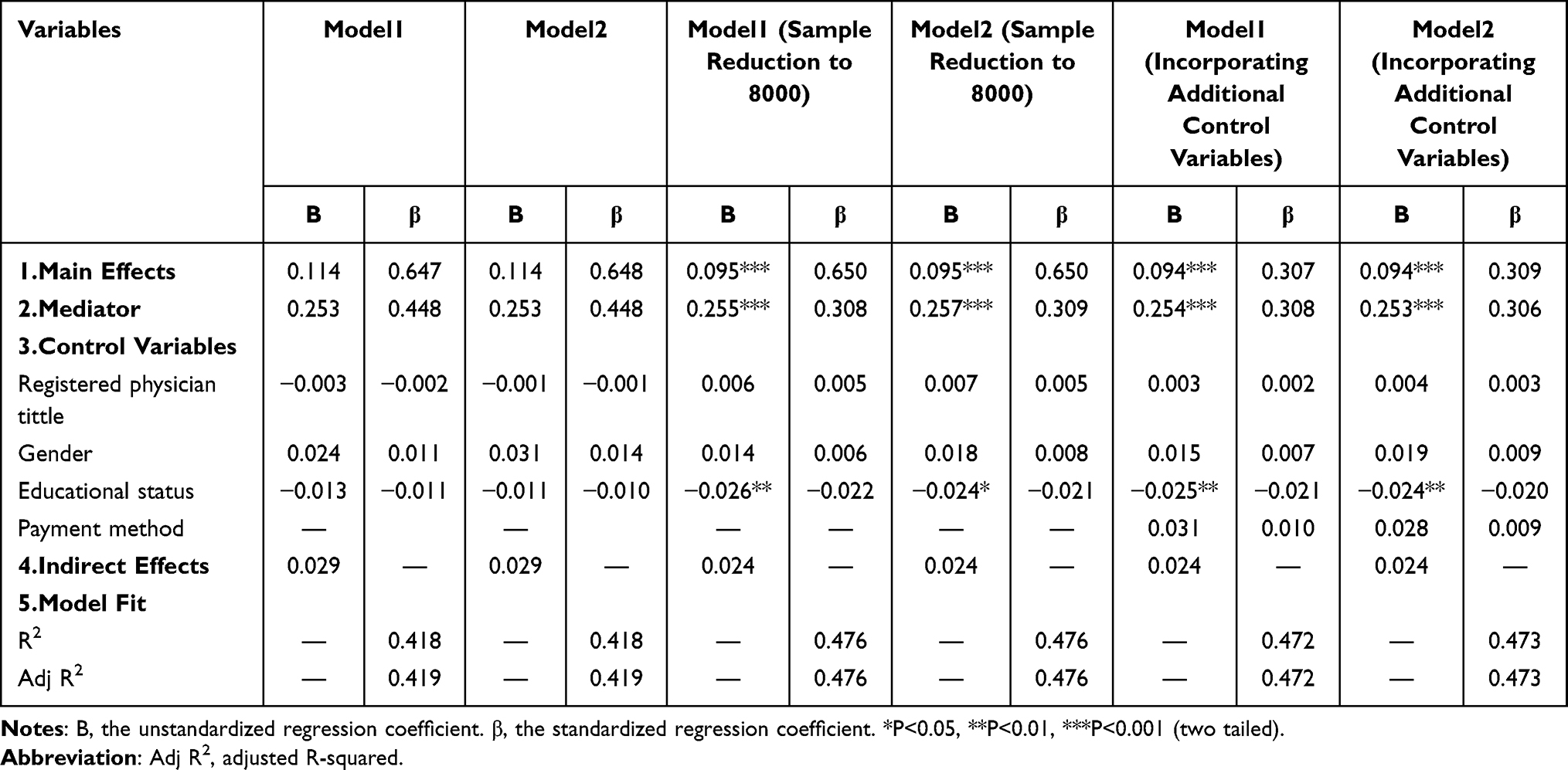 |
Table 6 Robustness Tests (Sample Reduction to 8000 or Incorporating Additional Control Variables) |
(4) The indirect effect remains highly stable, with the point estimate changing from 0.029 in the baseline model to 0.024 under robustness tests, a variation of approximately 17%, which is below the 20% threshold commonly adopted to indicate robustness in mediation analyses.
The Confirmed Moderated Mediation Model
Figure 2 illustrating the proposed mediating and moderating relationships between the independent variables and the dependent variables. The detailed statistical testing of direct and indirect effects was conducted through regression analysis and bootstrap procedures, consequently, this diagram provides a visual representation of this relationship.
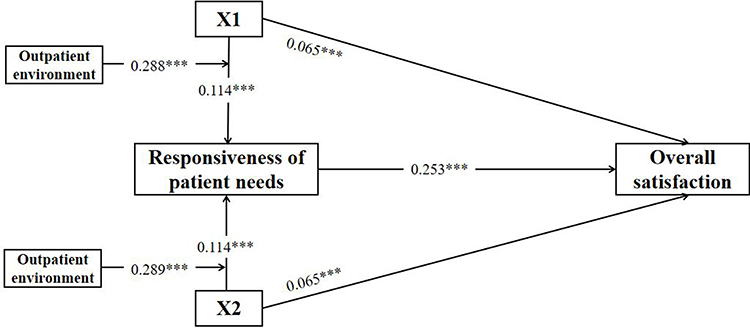 |
Figure 2 Confirmed moderated mediation model linking X1, X2, responsiveness of patient needs, outpatient environment, and overall satisfaction. Note: X1, interprofessional collaboration. X2, attitudinal alignment. ***P<0.001 (two tailed). |
Discussion
This study constructs a moderated mediation model to validate how doctor-nurse collaboration enhances older patients’ overall satisfaction both directly and indirectly through improved responsiveness to their needs, while the outpatient environment critically moderates this indirect pathway. This study transcends previous research that primarily focused on interpersonal interactions by integrating the outpatient environment into the model, revealing its critical role as a moderator in the satisfaction pathway. This underscores the need to study these factors in relation to one another to fully understand patient satisfaction, identify their medical needs, and ultimately mitigate barriers to healthcare access among older patients. Based on cross-sectional survey data, this study offers several important implications for both policy and clinical practice aimed at older patients.
First, the results confirmed a direct positive effect of doctor-nurse collaboration on overall satisfaction. In both models, interprofessional collaboration and attitudinal alignment significantly and positively predicted satisfaction among older adults. Facing complex conditions and often experiencing negative emotions (eg, anxiety, depression), these patients heavily rely on healthcare professionals for support.29,30 Therefore, when doctors and nurses respond accurately to patients’ professional inquiries, such as medication usage and precautions, their collaborative synergy helps patients to better understand their health status and treatment plans. They are more likely to perceive the medical environment as safe and trustworthy, which fosters equitable communication and enhances treatment adherence. These findings align with Maslow’s hierarchy of needs, suggesting that only when such basic needs of patients as a sense of security during medical visits are met can higher-level needs be satisfied throughout the treatment process, ultimately improving overall satisfaction.31 By contrast, the model proposed in this study suggests that such positive interactive effects may be compromised by inappropriate behavior by doctors or nurses. Only when patients simultaneously receive consistent and collaborative support from doctors and nurses in terms of professionalism and attitudes can they perceive the overall effectiveness of the service, leading to increased satisfaction. Consistent with the findings of Gu,32 effective interprofessional communication is crucial for accurately identifying older patients’ needs and ensuring holistic care. This finding also accords with a Greek study.33 In summary, in addition to considering this collaborative dynamic, the positive attitude and emotional coordination of information conveyors are equally critical factors influencing healthcare services and overall satisfaction among older patients. Evidence from Portugal suggests that interprofessional and team communication is an imperative component of clinical education, in order to optimally address the diverse needs of older patients.34
Second, the study confirms that responsiveness to patient needs plays a crucial mediating role in the transition from doctor-patient collaboration to overall satisfaction. Specifically, inter-professional collaboration and attitudinal alignment significantly enhanced responsiveness to patient needs, which in turn predicted satisfaction among older patients. This indicates that doctor-nurse collaboration is not merely communication and coordination between healthcare workers, but also an operational and patient-centered approach that delivers tangible benefits to patients by responding to patient needs in a timely manner, thereby elevating satisfaction levels. Previous studies have consistently identified timely and actionable responsiveness as one of the strongest predictors of patient satisfaction.35 Additionally, the SERVQUAL model further emphasizes that responsiveness is a manifestation of service efficiency and quality.36 This conclusion is further corroborated by a Nepalese study of outpatient satisfaction.37 Waiting time is another critical indicator of operational efficiency, and has been widely studied in relation to patient satisfaction.38 This aligns with the conclusions drawn by researchers from Africa.39,40 In summary, responsiveness to patient needs constitutes concrete and actionable behavior that must be systematically implemented. Studies suggest that key performance indicators (KPIs), such as door-to-doctor time, request fulfillment rate, and response rates, can serve as specific and quantifiable metrics for monitoring clinical responsiveness and healthcare service quality.41–43 Therefore, to genuinely enhance patient satisfaction, healthcare institutions should move beyond superficial gestures, such as explanations, communication, and smiles, and establishing mechanisms for doctors and nurses to collaboratively and rapidly respond to patient needs through team collaboration training is crucial.
Third, the mediating effect of a favorable outpatient environment offers a novel perspective for understanding the mechanisms through which doctor-nurse collaboration influences responsiveness to patient needs. Recent European research indicates that the outpatient environment shapes patient satisfaction indirectly, exerting its influence through a moderating effect on other key variables.44 A well-designed environment (eg, clear signage, adequate seating) mitigates age-related burdens, enabling older patients to better concentrate on understanding medical information and, thus, more effectively establish trust and rapport with doctors and nurses.45,46 Consequently, a favorable outpatient environment acts as both “lubricants” and “amplifiers” in enhancing the positive impact of doctor-nurse collaboration on responsiveness to patient needs, thereby improving overall satisfaction. Conversely, a poor environment can undermine even effective collaboration by increasing patient distress. Thus, this study suggests that improving patient satisfaction requires not only promoting doctor-nurse collaboration but also systematically enhancing healthcare services through environmental optimization to elevate overall satisfaction and quality of service. Tailoring environmental improvements to the needs and characteristics of older patients is referred to as age-friendly environmental design that significantly shapes their healthcare experience, and some studies indicate that the outpatient environment is one of the primary criteria influencing hospital selection among older patients.47 For example, a study from Australia showed that bright, modern settings with clear signage and well-placed seating evoke warm and positive feelings, improve visit efficiency, and reduce discomfort, thereby supporting effective communication.48 Finally, integrating safety features such as non-slip flooring, wheelchair ramps, and handrails in toilets constitutes a fundamental aspect of age-friendly design, facilitating responsiveness to patient needs and ultimately enhancing the satisfaction of older patients.47
Limitation
This study had several limitations. First, this cross-sectional study constrained our capacity to establish strict causal inferences, allowing only the identification of associations among multiple variables. Therefore, future longitudinal or experimental studies could provide more robust evidence regarding the relationship between doctor-patient collaboration and satisfaction. Further exploration of other potential moderating variables, such as educational status and health literacy, and mediating variables, such as anxiety, depression, and socioeconomic status, will contribute to a more comprehensive and in-depth understanding of the underlying mechanisms. Furthermore, as the sample was drawn exclusively from Beijing, the results may not be generalizable to other regions. Consequently, future studies should seek to expand the survey coverage to a national scale to enhance the robustness and general applicability of the conclusions.
Conclusion
This study tested a hypothesized moderated mediation model. The results demonstrate that doctor-nurse collaboration not only directly improves older patients’ overall satisfaction but also exerts an indirect effect through enhanced responsiveness to their needs. Moreover, the outpatient environment positively moderates this indirect pathway. Compared to traditional studies that often examine each variable independently, we incorporated the frequently overlooked variable of the outpatient environment into the doctor-nurse collaboration on a moderated mediation model, emphasizing the necessity of treating the physical environment and interpersonal interactions as an integrated concept for a comprehensive analysis of satisfaction and its influencing factors. Through these validation analyses, we aimed to reduce the difficulties faced by older outpatients and enhance their overall satisfaction.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethics approval was granted by the Ethics Committee of the Peking University First Hospital. (NO. 2025R0051-0002). Informed consent was obtained in written form from all participants. Specifically, after reviewing an online information sheet, participants provided their consent by clicking an “I agree” button to proceed to the main questionnaire. Participation was entirely voluntary, and respondents retained the right to withdraw at any time without penalty.
Acknowledgment
The study acknowledges all the authors cited in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Peking University First Hospital Scientific Research Project Fund (grant number 2025SF124).
Disclosure
The authors declare that they have no competing interest.
References
1. World Health Organization. World Social Report 2023: leaving No One Behind In An Ageing World. Available from: https://social.desa.un.org/development/desa/dspd/world-social-report/2023-2.html.
2. Chowdhury SR, Das DC, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClin Med. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
3. Akin T. Assessing quality of health care in the context of patient satisfaction from patients’ perspective among a physical therapy and rehabilitation unit. BMC Health Serv Res. 2025;25. doi:10.1186/s12913-025-12214-w
4. National Health Commission. Statistical Bulletin on the Development of Health Care in China in 2023. Available from: https://www.nhc.gov.cn/guihuaxxs/c100133/202408/0c53d04ede9e4079afff912d71b5131c/files/1734002454304_67772.pdf.
5. Ai HL, Shensa A, Linkov F. Outpatient pooling policy and healthcare satisfaction among middle-aged and older adults: evidence from China. BMC Health Serv Res. 2025;25. doi:10.1186/s12913-025-12769-8
6. Lu LY, Harris MB, Chiodo C, Chen AF. Surgeon age, years in practice, and location of training are associated with patient satisfaction. J Am Acad Orthop Surg. 2025;33(6):275–14. doi:10.5435/JAAOS-D-24-00941
7. Liu TT, Kuo LC, Liao SJ. Evaluating older adults’ satisfaction with age-friendly hospitals services: insights from an Eastern Taiwan regional teaching hospital. BMC Geriatr. 2025;25. doi:10.1186/s12877-025-06286-w
8. Dibba Y, Boima F, Jerome JG, et al. Patient satisfaction and its associated factors in selected primary healthcare facilities in Kono District, Sierra Leone: a cross-sectional study. BMJ Open. 2025:15. doi:10.1136/bmjopen-2024-093501
9. Ilic VO, Tasic L, Marinkovic V. Research on the attitudes of the elderly towards interprofessional cooperation and collaborative pharmacy practices: cross-sectional Study in Serbia. Indian J Pharm Educ. 2021;55(1):276–287. doi:10.5530/ijper.55.1.31
10. R B. Families of the deceased in the hospital: a multi-disciplinary approach to intervention. J Prim Prev. 1993;13(4):281–298.
11. Messmer PR. Enhancing nurse-physician collaboration using pediatric simulation. J Contin Educ Nurs. 2008;39(7):319–327. doi:10.3928/00220124-20080701-07
12. Berduzco-Torres N, Choquenaira-Callañaupa B, Medina P, et al. Factors related to the differential development of inter-professional collaboration abilities in medicine and nursing students. Front Psychol. 2020;11:432. doi:10.3389/fpsyg.2020.00432
13. Chen XY, Liu C, Yan PP, Wang HL, Xu JJ, Yao K. The impact of doctor-patient communication on patient satisfaction in outpatient settings: implications for medical training and practice. BMC Med Educ. 2025. doi:10.1186/s12909-025-07433-y
14. Wang Y, Liu CC, Wang P. Patient satisfaction impact indicators from a psychosocial perspective. Front Public Health. 2023;11:1103819. doi:10.3389/fpubh.2023.1103819
15. Reid RJ, Greene SM. Gathering speed and countering tensions in the rapid learning health system. Learn Health Syst. 2023;7(2):e10358. doi:10.1002/lrh2.10358
16. Parasuraman A, Zeithaml VA, Berry LL. A conceptual model of service quality and its implications for future research. J Mark. 1985;49(4):41–50. doi:10.1177/002224298504900403
17. Kashfi SM, Karimian E, Ravangard R, Mehralian G, Bastani P. Service quality in outpatient teaching hospital pharmacies based on the SERVQUAL model: an assessment in the south of Iran. Int J Pharm Pract. 2022;30(2):153–159. doi:10.1093/ijpp/riac004
18. Asiamah N, Opuni FF, Aggrey M, Adu-Gyamfi K. ADAPTED SERVQUAL: a health service quality scale incorporating indicators of sanitation and hygiene. Qual Manag Health Care. 2021;30(3):184–193. doi:10.1097/QMH.0000000000000269
19. Nahabedian A, Bullock LM, Fitzpatrick S, Resnick B, Brandt N. Discovering “What Matters” to patients: a quality improvement project. Geriatr Nurs. 2024;55:237–241. doi:10.1016/j.gerinurse.2023.11.007
20. National Health Commission. Notice on the Interim Provisions on Outpatient Quality Management of Medical Institutions. Available from: https://www.nhc.gov.cn/yzygj/c100068/202206/778aca5d2be74894a5626202154359b4.shtml.
21. Leddy KM, Kaldenberg DO, Becker BW. Timeliness in ambulatory care treatment: an examination of patient satisfaction and wait times in medical practices and outpatient test and treatment facilities. J Ambul Care Manage. 2003;26(2):138–149.
22. Younis A, Elmubarak M, Elkhwad H, Baig M, Saeed M, Omer A. Maximizing satisfaction in orthopedic outpatient clinics: evidence from Ireland. Cureus. 2024;16. doi:10.7759/cureus.63104
23. Cui J, Du J, Zhang N, Liang ZM. National patient satisfaction survey as a predictor for quality of care and quality improvement - experience and practice. Patient Prefer Adherence. 2025;19:193–206. doi:10.2147/PPA.S496684
24. Zhou X, He Q, Li Q, Kuang J, Han Y, Chen J. Factors associated with outpatient satisfaction in provincial Tertiary hospitals in Nanchang, China: a structural equation modeling approach. Int J Environ Res Public Health. 2022;19(14):8226–8235. doi:10.3390/ijerph19148226
25. Emanuel EJ, Gudbranson E, Van Parys J, Gørtz M, Helgeland J, Skinner J. Comparing health outcomes of privileged US citizens with those of average residents of other developed countries. JAMA Intern Med. 2021;181(3):339–344. doi:10.1001/jamainternmed.2020.7484
26. Cai ZJ, Wu A, Wang XF, Xie HF. Outpatient process transformation and patient satisfaction under new public service theory. Patient Prefer Adherence. 2025;19:3349–3361. doi:10.2147/PPA.S544684
27. Zhou F, Xu C, Sun Y, Meng X. Influencing factors of outpatients’ satisfaction in China a cross-sectional study of 16 public tertiary hospitals. Patient Prefer Adherence. 2021;15:1243–1258. doi:10.2147/PPA.S305600
28. Zhou X, He Q, Li Q, Kuang J, Han Y, Chen J. Factors associated with outpatient satisfaction in provincial tertiary hospitals in Nanchang, China: a structural equation modeling approach. Int J Environ Res Public Health. 2022;19(14):8226. doi:10.3390/ijerph19148226
29. Bae SH, Kim GY. The association between self-reported sensory impairment and cognitive function among Korean older adults: results from the 2017 national survey of the living conditions and welfare needs of older Koreans. Kor J Gerontol Soc. 2019;39(2):389–404.
30. Mo K, Kim K. Factors related to preoperative anxiety in older patients with sensory impairment: a cross-sectional study. J Clin Nurs. 2024;33(10):4354–4366. doi:10.1111/jocn.17100
31. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50(4):370–396.
32. Gu X, Li X, Deng T, Fan R. Application of multidisciplinary doctor-nurse collaboration team to treat the patients in orthopedic department. Asian J Surg. 2023;46(12):6021–6022. doi:10.1016/j.asjsur.2023.09.069
33. Efthymiou A, Kalaitzaki A, Rovithis M. Validation of the self-efficacy questionnaire (SE-12-Gr) assessing the healthcare professionals’ self-reported communication skills with older healthcare users in Greece. Health Commun. 2025;40(3):481–491. doi:10.1080/10410236.2024.2348841
34. Semedo C, Costa J, de Castro EK. The communication satisfaction of geriatric patients treated by dental students and dentists in a university dental clinic: a cross-sectional study. Geriatrics. 2025;10(4):93. doi:10.3390/geriatrics10040093
35. Alfatafta M, Alsubahi N, Alfatafta H, et al. Assessing service quality and its impact on patient experience and satisfaction in prosthetics and orthotics: a SERVQUAL-based cross-sectional study. BMC Health Serv Res. 2025:25. doi:10.1186/s12913-025-13172-z
36. Elahi M, Enayati R, Keramatpour M. A fuzzy Delphi-SERVQUAL model using degree of belief structure for assessing customer satisfaction in automotive after-sales services. Appl Soft Comput. 2025;184:113770. doi:10.1016/j.asoc.2025.113770
37. Adhikari A, Paneru DP, Pokhrel A. Responsiveness of services rendered at primary healthcare facilities of Bharatpur, Nepal: a cross-sectional study. BMJ Public Health. 2024;2(1):e000546. doi:10.1136/bmjph-2023-000546
38. Morales J, Silva-Aravena F, Saez P. Reducing waiting times to improve patient satisfaction: a hybrid strategy for decision support management. Mathematics. 2024;12(23):3743. doi:10.3390/math12233743
39. Seif S, Shah J, Chandani A, Ali SK. The perception of waiting times on patient satisfaction and patient care: a cross-sectional study at a tertiary health care institution in Kenya. PLoS One. 2025;20. doi:10.1371/journal.pone.0322015
40. Sebera E, Hagenimana C, Twagirumukiza E. Patient satisfaction survey in a public hospital: Remera Rukoma District Hospital, Rwanda, 2023. BMC Health Serv Res. 2024;24. doi:10.1186/s12913-024-11996-9
41. Aljohani AA, Alhazmi JM, Alsaedi OH, Al-Ahmadi AF, Alshammary NS. Impact of urgent care centers on emergency department visits in Al Madina Al Munawara. Saudi Med J. 2025;46(1):65–70. doi:10.15537/smj.2025.46.1.20240537
42. Lan CY, Chu CP, Chen CC. Performance assessment of a rehabilitation transportation reservation matching service with market design mechanisms. J Adv Transp. 2023. doi:10.1155/2023/2604479
43. Duch P, Jorgensen CC, Nedergaard HK. Text message questionnaires for patient-reported outcome measures after cesarean section-A feasibility study. Acta Anaesthesiol Scand. 2024;68(9):1254–1260. doi:10.1111/aas.14477
44. Brajic A, Brajic S. The interaction effect of the work environment on the relationship between quality of health services and user satisfaction of the tertiary level of healthcare. Manag J Contemp Manag Issues. 2025;31(2):3–16. doi:10.30924/mjcmi.30.2.3
45. LaVela SL, Etingen B, Hill JN, Miskevics S. Patient perceptions of the environment of care in which their healthcare is delivered. HERD. 2016;9(3):31–46. doi:10.1177/1937586715610577
46. Li Y, Gong W, Kong X, Mueller O, Lu G. Factors associated with outpatient satisfaction in tertiary hospitals in China: a systematic review. Int J Environ Res Public Health. 2020;17(19):7070. doi:10.3390/ijerph17197070
47. Shih CI, Weng CC, Chen W, Yang HF, Fan SY. Consideration factors of older adults seeking medical treatment at outpatient services in Taiwan. BMC Health Serv Res. 2021;21. doi:10.1186/s12913-021-07251-0
48. Martins BA, Barrie H, Visvanathan R, et al. A multidisciplinary exploratory approach for investigating the experience of older adults attending hospital services. HERD. 2021;14(3):141–163. doi:10.1177/1937586720920858
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.