Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Exploring the Comprehensive Treatment of Hashimoto’s Thyroiditis with Traditional Chinese Medicine from the Perspective of Modern Medicine
Received 17 October 2025
Accepted for publication 26 January 2026
Published 6 February 2026 Volume 2026:22 575059
DOI https://doi.org/10.2147/TCRM.S575059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Jing Zhang, Guiling Huang
Jiangsu Medical College, Yancheng, Jiangsu Province, 224005, People’s Republic of China
Correspondence: Guiling Huang, Jiangsu Medical College, No. 283, Jiefang South Road, Yancheng City, Jiangsu Province, 224005, People’s Republic of China, Email [email protected]
Abstract: Hashimoto’s thyroiditis (HT) is a common autoimmune disorder characterized by the presence of thyroid-specific autoantibodies and lymphocytic infiltration within the thyroid gland. Although its etiology is multifactorial and complex—encompassing genetic susceptibility, environmental influences, and epigenetic modifications—HT primarily presents as primary hypothyroidism. Conventional management predominantly involves hormone replacement therapy; however, Traditional Chinese Medicine (TCM) has demonstrated promising efficacy and safety in the treatment of HT. This review critically examines the application of TCM in HT management, contextualized within contemporary understandings of the disease’s pathophysiology. TCM exerts therapeutic effects through multiple mechanisms, including immunomodulation, attenuation of oxidative stress, and inhibition of thyroid cell apoptosis. Clinical studies indicate that TCM interventions, such as herbal formulations and acupuncture, can effectively enhance thyroid function, decrease autoantibody levels, and improve patients’ quality of life. The integration of TCM with standard Western medical treatments offers a valuable complementary strategy for HT, addressing both symptomatic relief and underlying immune dysregulation. Nonetheless, there remains a need for large-scale, multicenter randomized controlled trials to establish standardized treatment protocols and to confirm the long-term safety and efficacy of TCM approaches. Overall, TCM represents a promising adjunctive therapeutic option for HT, expanding the range of treatment modalities beyond conventional hormone replacement. Future investigations should aim to elucidate the molecular mechanisms underlying TCM’s effects and to optimize therapeutic regimens to maximize clinical benefits.
Keywords: Hashimoto’s thyroiditis, cellular immunity, hypothyroidism, traditional Chinese medicine
Introduction
Hashimoto’s thyroiditis (HT), first described by Haraku Hashimoto in 1912, is characterized by “struma lymphoma-tosa,” which refers to an enlarged thyroid gland infiltrated by lymphocytes.1 The condition exhibits a racial predisposition, with a higher incidence observed among Caucasians than among African Americans and Asians, while Pacific Islanders are infrequently affected.2 The prevalence of HT tends to increase with advancing age,3 particularly among individuals diagnosed with other autoimmune disorders such as myasthenia gravis,4 systemic sclerosis,5 and various connective tissue diseases,6 including Sjögren’s syndrome and pernicious anemia.7,8 The coexistence of multiple autoimmune diseases may be related to the interaction of multiple factors, including immune dysregulation, genetic susceptibility, hormonal levels, and environmental influences.9 Furthermore, Hashimoto’s thyroiditis can coexist with other autoimmune endocrine diseases, thereby constituting autoimmune polyendocrine syndromes (APS). These include type 1 APS (HT in conjunction with Addison’s disease, hypoparathyroidism, and chronic mucocutaneous candidiasis), type 2 APS (HT with Addison’s disease and type 1 diabetes), and IPEX syndrome (HT associated with neonatal type 1 diabetes, autoimmune enteropathy, and eczema).8–10 The diagnosis of HT is primarily clinical, relying on the assessment of clinical manifestations, presence of serum antibodies against thyroid antigens, and observation of lymphocytic infiltration through cytological examination. Currently, hormone replacement therapy is the predominant treatment approach for hypothyroidism. In this context, Traditional Chinese Medicine (TCM) has become a promising complementary and alternative therapy. TCM provides a holistic framework for HT management, not only aimed at relieving clinical symptoms, but also committed to regulating immune function and possibly delaying disease progression. More and more clinical and experimental studies have shown that TCM interventions including TCM compound, acupuncture and comprehensive therapy may bring benefits in improving thyroid function, reducing autoantibody titers and improving quality of life. However, the existing body of evidence is substantially constrained by methodological limitations, including small study scales, predominantly single-center designs, and a lack of standardized protocols. Notably, there remains a significant scarcity of large-scale, multicenter randomized controlled trials with sufficient statistical power to definitively confirm the efficacy, safety, and long-term outcomes of such interventions. This narrative review synthesizes contemporary understanding of the pathophysiology of HT and critically evaluates the scientific evidence supporting TCM interventions. It aims to provide a balanced perspective on the potential role of TCM within comprehensive HT management strategies, while highlighting the urgent need for more robust clinical research to translate promise into practice.
Pathophysiology
Recent investigations into the genetic predisposition to autoimmune thyroid disease have predominantly concentrated on Graves’, with comparatively less emphasis on HT. However, one study evaluated the extent to which established or potential polymorphisms linked to HT contribute to this condition. In a relatively small cohort of 142 Polish patients, only seven polymorphisms were confirmed to be associated with HT, accounting for 5.5% of the overall variability. Furthermore, no common environmental factors were found to correlate with susceptibility, likely because of the limited sample size.11 In another study involving 405 patients from Croatia, supplemented by a confirmation cohort of additional 303 patients, three novel variants were identified, representing 4.8% of the genetic variants associated with HT.Nevertheless, the authors were unable to validate associations previously established by conventional genetic association studies, which was attributed to constraints in their analytical capacity.12 A recent study identified a novel splice site variant in the thyroglobulin gene (TG C. 1076–1G > C) that may be implicated in HT. This variant, which is associated with exon skipping and the production of thyroglobulin (TG), was observed in an affected individual from a family exhibiting apparent autosomal dominant inheritance of HT as well as in an unaffected child.13 It is well established that certain polymorphisms in the TG gene are linked to HT and Graves’ disease, albeit at relatively low risk. The precise mechanism by which this new variant may influence the production of thyroglobulin, potentially leading to thyroid cell loss, autoimmunity, or an alternative immune response, remains unclear. However, it is important that affected individuals exhibit autoantibodies against both Tg and TPO. Additionally, another family with autosomal dominant HT has been documented to present mutations that result in haploinsufficiency of the gene encoding tumor necrosis factor A-inducible protein 3.14 A20 haploinsufficiency is known to potentially contribute to inflammatory and autoimmune disorders, likely because of its role in modulating T helper 17 (Th17) cell activity and other immune responses. Furthermore, a case of HT associated with Behçet’s syndrome and vitiligo has recently been reported.15 In a study involving 298 Jordanian patients with HT, consanguinity was found to correlate with a 3.3-fold increased relative risk of HT compared to healthy controls.16 This association suggests a heightened expression of autosomal recessive conditions while not affecting autosomal dominant or X-linked disorders, indicating that further exploration of these cases may yield valuable insights.
A growing body of literature indicates that various environmental factors significantly affect the susceptibility to HT. Over the past decade, considerable focus has been directed towards selenium, particularly regarding its potential as a therapeutic agent, as well as its relationship with intestinal microbiota and medical treatment. Research examining the correlation between selenium intake and autoimmune thyroiditis markers, as well as the impact of selenium supplementation on these markers, has yielded inconsistent results. Nevertheless, a survey conducted among 881 members of the Italian Society of Medical Endocrinology revealed that nearly 80% of respondents prescribed selenium for HT in patients with euthyroid function, despite approximately half expressing skepticism regarding supporting evidence for its use.17 Furthermore, approximately two-thirds of the participants endorsed selenium supplementation in cases of subclinical hypothyroidism associated with TPO antibodies, presumably to mitigate disease progression. A meta-analysis indicated that selenium supplementation led to a reduction in serum TPO antibody levels after 3, 6, and 12 months in HT patients receiving levothyroxine treatment; however, this effect was only observed at the 3-month mark in untreated HT patients, with no significant changes at 6 and 12 months.18 The likelihood of a decrease in thyroglobulin antibody levels remains low, and the overall quality of evidence is deemed insufficient. Furthermore, the ambiguous effects on antibody levels should not be interpreted as indicative of any tangible clinical benefit, particularly in light of increasing reports of adverse effects.
Epigenetics
Current research demonstrates that both genetic and environmental influences interact to influence HT19–22 by modulating epigenetic factors. These epigenetic factors have the potential to regulate gene expression and phenotypic outcomes, which may contribute to the development of diseases without necessitating alterations in the DNA sequence.23 The autoimmune manifestation of HT is influenced by the interplay between environmental factors and genetic predispositions, including specific genes such as human leukocyte antigen (HLA), cytotoxic T lymphocyte-associated protein 4 (CTLA-4), protein tyrosine kinases, and non-receptor type 22 (PTPN22), as well as patterns of X-chromosome inactivation. This interaction leads to a disruption in the self-tolerance mechanisms that are typically regulated by T and B lymphocytes.8,24–26 Furthermore, various autoantigens, cytokines and their receptors, estrogen receptors, genetic polymorphisms of adhesion molecules, promoter region of selenoprotein S, and products related to apoptosis have been associated with thyroid-related autoimmunity.8,27–29 These genetic vulnerabilities may also be subject to epigenetic modifications, including methylation, histone alterations, and RNA interference involving ncRNAs.23
The factors related to epigenetics that contribute to the onset of diseases are extensive; however, the most prevalent include DNA methylation, histone modifications, and RNA interference mediated by non-coding RNAs.23 HT is characterized by the infiltration of lymphocytes into the thyroid gland, which is subsequently followed by the infiltration of T and B cells. It has been suggested that the presence of autoantibodies and B cell dysfunction constitute the primary immune responses in autoimmune thyroid disorders. Furthermore, aberrant functioning of T-cell subsets is believed to significantly disrupt immune homeostasis and initiate autoimmune responses against thyroid tissue.21,30 DNA methylation plays a crucial role in the silencing of certain genes, whereas histone modifications can promote the activation of other genes. Nonetheless, the impact of these epigenetic mechanisms may vary and are subject to modulation by environmental factors.30 Furthermore, non-coding RNAs, such as microRNAs, have also been implicated in the regulation of gene expression.31,32 Research indicates that the observed female predominance in HT may be attributed to X-chromosome inactivation, which is recognized as a significant epigenetic mechanism involved in silencing X-chromosome genes.21 This finding implies that gene functionality can be modified through epigenetic processes, potentially contributing to the development of autoimmune diseases. Consequently, epigenetic factors may play a crucial role in the etiology of autoimmune disorders along with genetic and environmental factors.20,21,33 Furthermore, an increasing body of evidence suggests that environmental factors can trigger epigenetic changes that may lead to autoimmune thyroid diseases such as HT, particularly in individuals with a genetic predisposition.34,35 (See Figure 1).
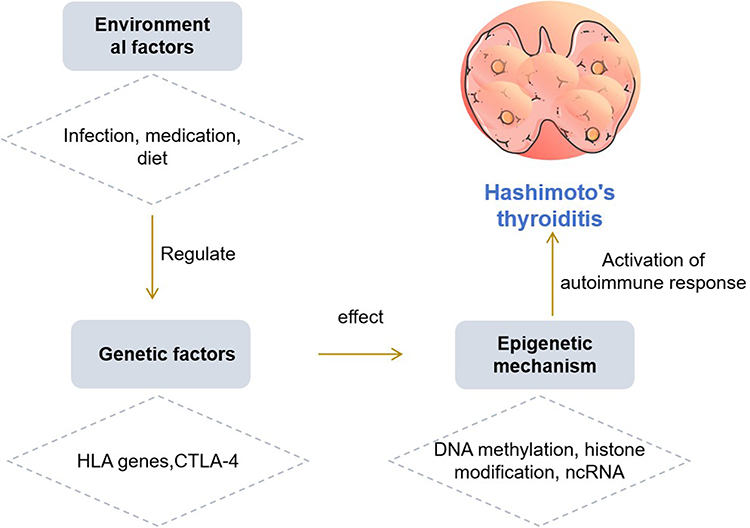 |
Figure 1 Epigenetic regulation of HT. |
Morbidity Mechanism
The association between goiter and atrophic autoimmune thyroiditis has been a subject of considerable debate, particularly regarding whether goiter merely progresses into atrophic autoimmune thyroiditis or whether they represent distinct pathological entities. Recently, IgG4-related diseases (IgG4-BD) have emerged as recognized conditions that affect various tissues and are characterized by the infiltration of IgG4-positive plasma cells, stromal fibrosis, and elevated serum IgG4 levels. In Japan and the United States, approximately 30% of patients with HT exhibit thyroid-affecting IgG4-BD, which correlates with early onset hypothyroidism and thyroid atrophy. In contrast, the prevalence of this association appears to be significantly lower in Europe (approximately 12%.36 The reasons for this discrepancy remain unclear and may be attributed to methodological differences, iodine deficiency in the specific European populations studied, or unidentified factors. Nonetheless, these findings support the notion that thyroid atrophy in HT frequently results from the disease progression.
Regulatory T cells (Tregs) have been firmly established as playing a pivotal role in the prevention of autoimmunity. Various subsets of Tregs have been identified and can be broadly categorized into native or thymic Tregs (characterized by the expression of CD4, CD25, and Foxp3). Previous studies have indicated that these cells exhibit HT abnormalities and are capable of inducing a peripherally differentiated Treg subset in response to specific antigens. In HT, there is an observed elevation of CD4+ CD69+ Foxp3- Tregs; however, their functional capacity is compromised.37 Additionally, the quantity and functionality of Treg type 1 cells, identified as CD4+ CD49+ LAG-3+ IL-10+, are diminished under these conditions.38 These alterations have been documented through analyses of peripheral blood samples and are similarly observed in Graves’.The relationship between Tregs and HT appears intricate, particularly when the disease is fully characterized. Cytokines produced by lymphocyte infiltration are pivotal in the damage to thyroid cells, particularly because of their capacity to induce thyroid cells to release pro-inflammatory mediators autonomously, thereby exacerbating and sustaining the autoimmune response.39 Prior research has indicated that, similar to other autoimmune disorders, there is an increase in Th17 cells secreting the cytokine IL-17 in both the blood and thyroid tissues of patients with HT. However, a recent investigation identified an additional source of IL-17 within thyroid follicular cells in cases of HT.40 While there is currently no evidence to suggest a direct involvement of IL-17 in the dysfunction of tight junctions, its expression has been associated with the presence of CD68+ macrophages within follicles. In addition to IL-17, Th17 cells produce IL-22, a cytokine that targets epithelial cells and is similarly secreted by Th22 cells. Recent studies have reported elevated levels of Th22 cells41 in the blood and thyroid of HT patients, warranting further exploration of the effects of IL-22 on thyroid cells. IL-21, a pleiotropic cytokine essential for the development of Th17 cells, has also been found to be increased in the thyroid and blood of individuals with HT. Furthermore, thyroid lymphocytes in HT patients exhibit higher expression of the IL-21 receptor42 than those with Graves’ disease or healthy controls (see Figure 2).
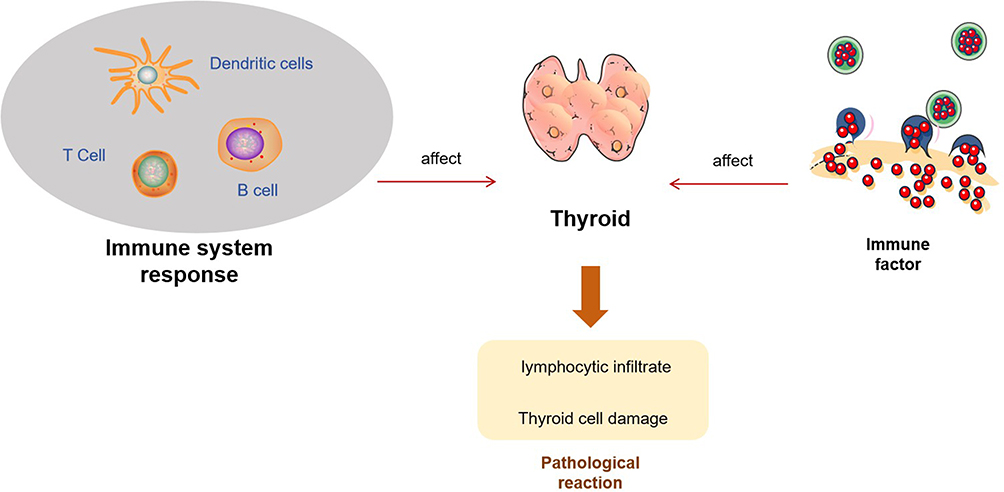 |
Figure 2 Pathological mechanism of HT. |
Symptoms and Diagnosis
Hashimoto’s thyroiditis typically begins in genetically predisposed individuals and is triggered by environmental factors, leading to the production of thyroid autoantibodies, most commonly thyroid peroxidase antibodies (TPOAb). The progression of the disease generally involves two functional stages. The first is subclinical hypothyroidism, characterized by elevated levels of thyroid-stimulating hormone (TSH), while free thyroxine (FT4) and free triiodothyronine (FT3) concentrations remain within the normal reference range.43,44 The second stage is overt hypothyroidism, marked by significantly elevated TSH levels accompanied by a decrease in FT4 levels as thyroid destruction worsens.43,44 The definition of the TSH reference range must account for factors such as age, sex, and pregnancy status, and there is currently a lack of globally unified diagnostic cutoff standards.45 The clinical manifestations of overt hypothyroidism result from thyroid hormone deficiency in various tissues and organs throughout the body, with severity ranging widely and symptoms being broad and non-specific. These may include fatigue, cold intolerance, weight gain, dry skin, bradycardia, memory impairment, constipation, and in severe cases, myxedema coma.46–48
The diagnosis of HT relies on a combination of clinical, serological, and imaging evidence. Serological testing: TPOAb positivity is a key serological marker for diagnosis and is observed in approximately 95% of patients, while thyroglobulin antibody (TgAb) positivity occurs in about 60–80% of cases.48–50 TPOAb serves not only as a diagnostic marker but also as an important risk factor for predicting the progression from subclinical to overt hypothyroidism, and it is associated with adverse pregnancy outcomes.50,51 Thyroid function assessment: TSH and FT4 levels are measured to determine functional status (euthyroidism, subclinical hypothyroidism, or overt hypothyroidism). Thyroid ultrasound: This is particularly valuable for diagnosis, especially in seronegative patients (accounting for approximately 5–10% of cases). Typical ultrasound features include diffusely reduced and heterogeneous echogenicity of the thyroid parenchyma, often accompanied by a grid-like hyperechoic pattern and abnormal vascular distribution.44,49 Clinical evaluation: A detailed history and physical examination are essential to identify symptoms and signs related to hypothyroidism. (See Figure 3).
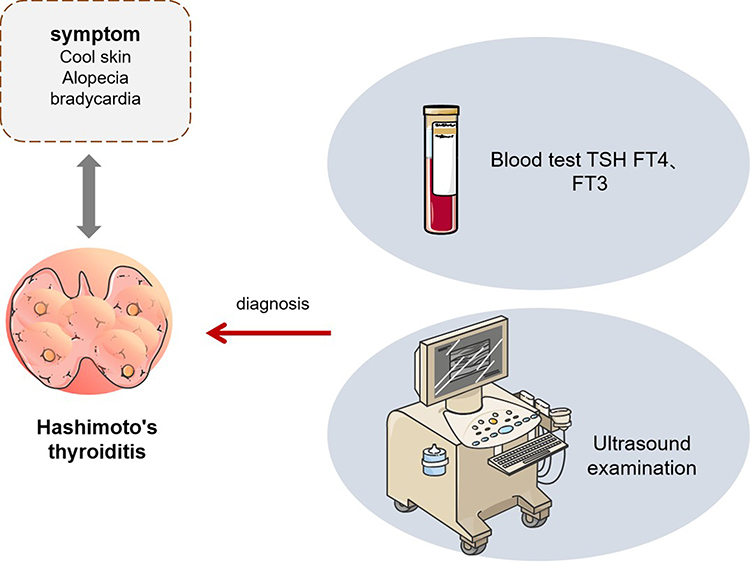 |
Figure 3 Symptoms and diagnosis of HT. |
Diagnostic Criteria and Patient Selection for TCM in HT
The identification of patients with HT who may benefit from TCM interventions requires the application of standardized diagnostic criteria and appropriate clinical staging. Both the Beijing Expert Consensus on the Diagnosis and Treatment of HT with Integrated Traditional Chinese and Western Medicine (2021, Beijing) and the Guidelines for Diagnosis and Treatment of HT with Integrated Traditional Chinese and Western Medicine (2025) emphasize that the diagnosis of HT should rely on a comprehensive assessment that integrates clinical manifestations, serological markers, imaging features, and, when necessary, pathological examination.52,53
Clinically, the presentation is typically characterized by a diffuse, firm, and often symmetrical thyroid enlargement that moves with swallowing. Patients may also experience compressive symptoms like throat discomfort or difficulty swallowing.54 Early-stage Hashimoto’s thyroiditis is typically asymptomatic or presents with non-specific symptoms. As the disease progresses, characteristic manifestations of hypothyroidism may emerge, including fatigue, cold intolerance, bradycardia, myxedema, and neuropsychiatric symptoms. A minority of patients may experience fluctuations in thyroid function, presenting with transient thyrotoxicosis features such as palpitations, sweating, and weight loss.55 In terms of laboratory findings, elevated serum levels of thyroid peroxidase antibody (TPOAb) and/or thyroglobulin antibody (TgAb) are the most distinctive immunological markers of HT, with their titers correlating with the degree of thyroid lymphocytic infiltration.56,57 Thyroid function can vary from normal to subclinical or overt hypothyroidism, with occasional fluctuations.58 Imaging-wise, thyroid ultrasonography typically reveals diffuse hypoechogenicity, heterogeneous texture, and a coarse reticular pattern, which may be accompanied by nodules requiring careful differentiation.59,60 For diagnostically ambiguous cases, fine-needle aspiration or histopathological examination can confirm the diagnosis by revealing features such as lymphocytic and plasma cell infiltration, follicular atrophy, and fibrosis.61
Based on these diagnostic parameters, we focus on two patient subgroups with clear pathophysiological and clinical therapeutic relevance. The first subgroup comprises patients who remain symptomatic despite adequate and stable thyroid hormone replacement therapy, continuing to experience neck discomfort, throat foreign body sensation, fatigue, or emotional disturbances.62 While modern medicine’s replacement therapy effectively corrects hormone levels, it struggles to address these persistent immune abnormalities and systemic dysregulation. In contrast, Traditional Chinese Medicine (TCM), through its multi-target actions and holistic integrative regulation, precisely targets the root causes of these residual symptoms, offering benefits beyond symptomatic relief. Additionally, patients in the early stages of the disease, when thyroid function remains preserved, also represent suitable candidates for intervention.63 This phase constitutes a critical window for intervening in the immune process and slowing disease progression. Conventional Western medicine often adopts a watchful waiting strategy at this stage, whereas TCM, guided by its preventive concept of “treating the pre-disease state”, can achieve early immunomodulation such as reducing thyroid autoantibody (TPOAb, TgAb) titers and improving thyroid ultrasound morphology, thereby delaying or preventing progression to clinical hypothyroidism. In summary, both consensus documents and guidelines emphasize that TCM can contribute to reducing antibody titers, improving thyroid morphology, and alleviating systemic symptoms, thereby providing complementary benefits to conventional management strategies.
Pathophysiological Mechanisms of TCM in the Treatment of HT
The evidence base for the use of TCM in the management of HT has expanded over the past decade, although much of the available literature remains constrained by modest sample sizes and variable study design quality. Nevertheless, both herbal and integrative approaches have been systematically evaluated in clinical trials, with outcomes suggesting meaningful improvements in thyroid function, autoantibody levels, and quality of life indices. Conventional management largely focuses on levothyroxine replacement to correct hypothyroidism; however, this approach does not directly address the underlying autoimmune or inflammatory milieu. In this context, TCM has been proposed as a complementary option to modulate immunity, temper oxidative damage, and ameliorate symptoms beyond what hormone replacement alone can achieve.In TCM theory, HT is often conceptualized as arising from imbalances such as “liver qi stagnation,” “spleen deficiency,” or “phlegm-damp accumulation,” which correspond to systemic dysregulation rather than isolated thyroid dysfunction. On a mechanistic level, recent reviews suggest that many active constituents in TCM formulations exert antioxidant, anti-inflammatory, or immunoregulatory actions—effects that may intersect with known HT pathogenic pathways. Huang et al (2024) summarized that components of TCM recipes frequently act via suppression of pro-inflammatory cytokines and attenuation of oxidative stress (eg via Nrf2/ROS pathways).64 In parallel, network-medicine frameworks have begun to map herb–target–symptom proximity in human protein interactomes, offering a systems-level justification for multiherb TCM prescriptions in chronic autoimmune conditions.65
Emerging evidence suggests that TCM exerts its therapeutic effects in HT through the modulation of multiple immune and cellular pathways, involving alterations in gene expression, protein synthesis, and intracellular signaling within thyroid and immune cells.Studies have demonstrated that Th17 and Treg cells collaborate to sustain immune homeostasis, and alterations in their relative proportions significantly influence the onset and progression of HT. In recent years, TCM has carried out extensive foundational research on the Th17/Treg axis. Wu Wenping et al66 reported that treatment with Shenqi Fuzheng Decoction in HT models led to decreased expression of miR-17 and increased expression of the long non-coding RNA MEG3, changes that restored the balance between Th17 and Treg cells and reduced thyroidal immune injury. Similarly, Zhou et al67 found that Buzhong Yiqi Decoction corrected Th17/Treg imbalance in HT mice through modulation of the transcription factors Foxp3 and RORγt, thereby protecting thyroid tissue. Acupuncture interventions in HT rats have likewise been shown to alter Foxp3 and RORγt expression in thyroid cells, reinforcing Treg differentiation and suppressing Th17-driven inflammation.68 Beyond these examples, additional studies indicate that TCM formulas may downregulate pro-inflammatory cytokines such as IL-17A and IL-23, while enhancing anti-inflammatory pathways mediated by TGF-β and IL-10, thereby stabilizing the Treg phenotype and maintaining immune tolerance.69 Numerous studies have also established a strong correlation between oxidative stress and the immune dysregulation that underlies HT pathogenesis. Excessive generation of reactive oxygen species (ROS) contributes to follicular cell injury and enhances antigen presentation, fueling autoantibody production. TCM therapies have demonstrated the capacity to mitigate oxidative damage and reduce thyroid autoantibody levels. Zhang Jie et al70 showed that administration of Sanjie Xiaoying Granules to HT rats decreased the mRNA and protein expression of NADPH oxidase subunits p22phox and gp91phox, leading to lower titers of TgAb and TPOAb in both high- and low-dose groups. Similarly, Zhao et al71 demonstrated that Qijian Xiaozheng Fang increased expression of the antioxidant enzyme GPX4 while reducing levels of lipid peroxidation markers such as LPO and inflammatory mediators such as COX-2. These effects exceeded those seen in the control group, suggesting that the prescription enhances antioxidant capacity, attenuates inflammatory cascades, and alleviates symptoms. Recent mechanistic work further indicates that TCM compounds may activate the Nrf2/ARE signaling pathway, upregulate downstream antioxidant enzymes including superoxide dismutase and catalase, and thereby strengthen cellular defenses against ROS.72 Collectively, these findings support the view that TCM formulas exert antioxidant and immunomodulatory effects at the transcriptional and post-translational level, contributing to reduced antibody production and improved thyroid microenvironment stability.
Apoptosis of thyroid follicular cells is another well-recognized mechanism underlying tissue destruction in HT, and TCM has been reported to counteract this process through multiple molecular pathways. Ting et al73 observed that Buzhong Yiqi Granules inhibited activation of the Akt/mTOR signaling pathway, promoted autophagic body formation, and decreased apoptosis in thyroid follicular epithelial cells, resulting in partial restoration of thyroid morphology. Liu Guangxia et al74 demonstrated that astragaloside suppressed activation of the RhoA/ROCK2 pathway, reducing apoptosis in thyroid tissues of HT rats. Additional reports show that TCM interventions can modulate the intrinsic apoptosis pathway by downregulating pro-apoptotic proteins such as Bax and caspase-3, while upregulating anti-apoptotic factors including Bcl-2, thereby protecting follicular cells from programmed death.75 Certain herbal compounds have also been shown to influence mitochondrial membrane potential and cytochrome c release, further interfering with the execution phase of apoptosis and preserving thyroid architecture.76 Taken together, these mechanistic insights indicate that TCM exerts multifaceted effects in HT through modulation of immune balance, reduction of oxidative stress, and inhibition of apoptotic signaling. By regulating transcription factors such as Foxp3 and RORγt, altering non-coding RNA expression, suppressing NADPH oxidase activity, activating the Nrf2 antioxidant pathway, and modulating pro- and anti-apoptotic proteins, TCM therapies provide a coherent mechanistic rationale for their observed benefits. While these findings highlight promising molecular targets, further integrative research is required to confirm how these molecular effects translate into consistent clinical outcomes in human populations.
Herbal Formulations in the Management of HT
Herbal prescriptions constitute one of the most extensively studied components of TCM in the treatment of HT. Based on the principle of syndrome differentiation, these formulations are designed to address specific diagnostic patterns such as qi deficiency, yin deficiency, or toxin stagnation, which are regarded within TCM as important contributors to the onset and progression of HT. In recent years, a growing number of clinical investigations, including randomized controlled trials (RCTs), have evaluated the therapeutic value of these prescriptions, frequently in combination with standard Western medical therapies. The results of these studies generally suggest that herbal interventions can provide symptomatic relief while also producing measurable biochemical improvements.One representative study was conducted by Liu Shaowei et al,77 who evaluated the effects of a modified Buzhong Yiqi Decoction administered together with selenium supplementation in patients with HT characterized by concurrent qi and yin deficiencies. Forty participants were randomized to either a control group, which received selenium alone, or an observation group, which received selenium in combination with the herbal decoction. Patients in the integrative treatment group exhibited significant improvements in thyroid function parameters, marked reductions in thyroid autoantibody titers, decreases in thyroid volume, and improved TCM syndrome scores compared with the control group, and importantly, these benefits were achieved without an increase in adverse reactions. These findings suggest that the integration of herbal decoctions with conventional therapy may enhance overall clinical efficacy, particularly for patients with specific TCM syndromes.Additional evidence was provided by Meixin et al,78 who investigated the use of a modified Erxian Decoction in patients with HT complicated by hypothyroidism. Sixty patients were randomly assigned to receive either standard therapy alone or standard therapy in combination with the herbal decoction. The integrative group demonstrated significant improvements across a range of endpoints, including thyroid hormone indices (TSH, FT3, and FT4), autoantibody levels (TPOAb and TGAb), and immunologic markers, with increased interleukin-10 (IL-10) and decreased interferon-γ (IFN-γ). In addition to these biochemical and immunological improvements, patients also reported better symptom control, reflecting the clinical significance of the intervention. This study underscores the capacity of TCM formulas not only to improve thyroid function but also to restore immune balance, which is particularly relevant in autoimmune thyroid disorders such as HT. Further support for the potential benefits of herbal therapies were reported by Chunping et al,79 who assessed the efficacy of Yiqi Qingjie Decoction in 80 patients with HT characterized by qi deficiency and toxin stagnation. After 12 weeks of treatment, patients receiving the herbal prescription exhibited significant reductions in thyroid autoantibody titers, improvements in thyroid function tests, better TCM syndrome scores, and favorable changes in immune cell subsets when compared with controls treated with selenium preparations. These results emphasize the potential immunomodulatory effects of herbal medicine in HT, particularly through the regulation of T lymphocyte subsets, which are central to autoimmune mechanisms underlying the disease.
Recent clinical investigations have provided additional evidence supporting the therapeutic potential of various herbal formulations in HT management. A 2025 meta-analysis by Wang et al examined seven randomized controlled trials (n=612) evaluating Xiaoyao-San preparations, demonstrating that these formulations, particularly when combined with levothyroxine, significantly reduced TPOAb (SMD = −0.77, 95% CI [−1.06, −0.47], p < 0.00001) and TgAb levels while improving TSH normalization (SMD = −0.76, 95% CI [−0.98, −0.54], p < 0.00001) compared to standard therapy alone.80 Similarly, Meng et al81 conducted a double-blind, placebo-controlled trial (n=48) investigating Bupleurum inula flower soup as an adjunct to levothyroxine therapy, revealing significant reductions in both TPOAb (275.77 ± 132.98 vs 441.78 ± 195.50, p < 0.01) and TgAb levels, alongside improvements in depression and anxiety scores and enhanced quality of life measures at 8 and 24-week follow-ups. Furthermore, a systematic review and meta-analysis by Wei et al evaluated 14 trials (n=1014) examining Ophiocordyceps sinensis preparations, showing substantial decreases in thyroid autoantibodies (TPOAb: SMD = −2.04, TgAb: SMD = −2.01, both p < 0.00001) and pro-inflammatory cytokines including TNF-α, IL-2, and IL-6, while improving FT4 levels in hypothyroid patients.82 The content mentioned above has been summarized in Table 1.
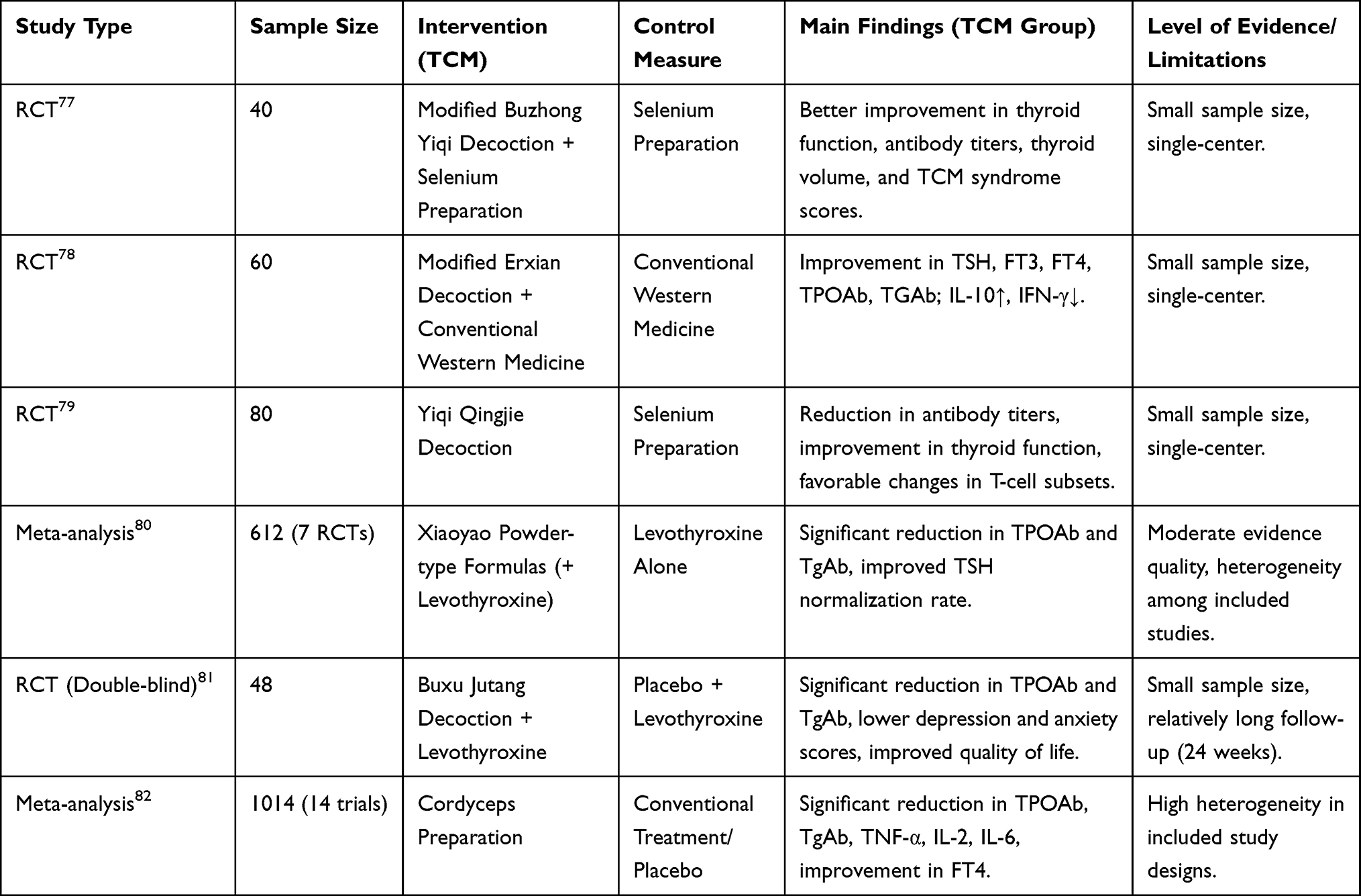 |
Table 1 Efficacy of TCM Herbal Formulations in Hashimoto’s Thyroiditis |
Currently, most clinical evidence is based on multi-herb compound formulations rather than single compounds or standardized extracts. This approach to polyherbal therapy embodies the essence of TCM principles such as “treatment based on syndrome differentiation” and the “sovereign-minister-assistant-courier” (compatibility) strategy, aiming to achieve multi-target regulation through the synergistic effects of multiple components. However, this also presents unique challenges for modern pharmacological research: it is difficult to isolate and identify a single, decisive “target active ingredient”. In a compound formula, various compounds—such as alkaloids, flavonoids, saponins, and polysaccharides—may collectively act on pathways related to immunity, oxidative stress, and apoptosis. Their overall effect is far more complex than the simple sum of individual components. Consequently, while we observe downstream biological effects—such as Th17/Treg balance modulation and downregulation of inflammatory factors—the precise upstream molecular target map remains incompletely elucidated. Future research needs to employ methodologies such as systems pharmacology, metabolomics, and network pharmacology to systematically analyze the material basis and integrative mechanisms of TCM compound formulations from a “drug-target-pathway-disease” network perspective. This will help address the limitations of the single-active-ingredient research paradigm in this field.
Taken together, these studies suggest that TCM herbal formulas may serve as valuable complementary interventions in the management of HT, particularly when individualized to specific syndrome patterns and used alongside conventional medical therapies. Although the findings consistently indicate improvements in thyroid function, reductions in autoantibody titers, and beneficial effects on immune regulation, it is important to recognize the limitations inherent in these studies, including the overall quality of evidence remains limited by small sample sizes, methodological heterogeneity, and predominantly single-center designs conducted in China. Consequently, there remains a pressing need for larger, multicenter, and longer-term trials to confirm the efficacy of these interventions, establish reproducibility, and evaluate their safety profiles in greater depth. Nonetheless, the currently available evidence provides a compelling rationale for further exploration of herbal formulations as an integral component of an integrative treatment strategy for HT.
Acupuncture and Related Modalities in the Management of HT
In addition to herbal prescriptions, acupuncture and related therapeutic modalities have also been explored as potential strategies for the management of HT and findings from these studies provide insights into both symptomatic relief and underlying immunological mechanisms, thereby expanding the scope of TCM-based approaches to HT.Ren Haitao et al83 conducted an RCT to investigate the relationship between HT and localized temperature variations in the thyroid gland, aiming to elucidate novel mechanistic links relevant to the disease. A total of 68 patients who met strict inclusion criteria were enrolled and randomized into two groups: one receiving selenium yeast tablets as standard Western medicine treatment (n=34), and the other receiving a combined regimen of massage and acupuncture (n=34). The investigators assessed changes in TCM symptom scores, thyroid antibody levels (TPOAb and TGAb), inflammatory markers (IL-6 and IL-12), and local heat metabolism of both the thyroid gland and related acupuncture points before and after the intervention. Using Pearson’s linear correlation analysis, the study revealed a significant association between local thyroid temperature variations and autoantibody production, suggesting a thermodynamic mechanism underlying the autoimmune process. Furthermore, patients in the combined treatment group showed enhanced local thyroid temperature, decreased antibody titers, and improved clinical indicators, indicating that acupuncture combined with massage could serve as an effective therapeutic modality in HT by influencing immune and inflammatory pathways.Further evidence was provided by Wenli et al,84 who performed an RCT to assess the clinical efficacy of the “Yi Qi Zhou Liu” acupuncture technique in HT patients with liver depression and qi stagnation syndromes. Sixty patients were randomized by a number table into two groups of equal size, with one group receiving levothyroxine sodium tablets alone for 8 weeks, and the other receiving acupuncture in addition to levothyroxine therapy. Acupuncture was performed at a combination of general acupoints (Baihui, Neiguan, Hegu, Taichong, Zusanli, Yinlingquan, and Taixi) and local points (Tiantu, Futu, and Renying), tailored according to individual symptoms. Each treatment session lasted 20 minutes and was delivered twice weekly for two courses, each of four weeks. After treatment, the acupuncture plus medication group showed superior improvements compared with medication alone, including reductions in TSH and TgAb levels, relief of emotional depression and chest distress, and overall better symptom scores. These findings suggest that the Yi Qi Zhou Liu acupuncture technique can potentiate the effects of levothyroxine in HT patients, especially those with specific TCM syndrome patterns, by simultaneously addressing emotional, biochemical, and symptomatic dimensions of the disease. Moreover, Xue et al,85 who evaluated the clinical efficacy and safety of acupoint application in HT patients diagnosed with liver qi stagnation, randomized 150 patients into two groups: an intervention group (n=75, with 11 exclusions and 5 dropouts) receiving acupoint application, and a placebo group (n=75, with 12 exclusions and 3 dropouts) receiving sham treatment. Both groups were also provided with health education and conventional Western medical management. The selected acupoints included Shenque, bilateral Yongquan, Xishi, and Ashi points, with Xishi treated once weekly and the others every other day over four weeks. The outcomes evaluated included serum levels of TgAb, TPOAb, FT3, FT4, and TSH, as well as thyroid morphology (thickness of the left and right lobes and isthmus). In addition, TCM symptom scores, the Hospital Anxiety and Depression Scale (HADS), and the Short Form 36 Health Survey (SF-36) were used to measure clinical efficacy and adverse reactions. The intervention group demonstrated significant reductions in autoantibody titers, alleviation of goiter severity, improvement in TCM symptom scores, and better psychological outcomes, with enhanced quality of life compared with the placebo group. Importantly, the therapy was reported to be safe and well tolerated, further supporting the use of acupoint application as an adjunctive modality in HT.
Recent clinical investigations have also provided systematic evidence on the role of acupuncture and related modalities in the management of HT. A meta-analysis by Wang et al that included 14 randomized controlled trials with a total of 1020 patients showed that acupuncture achieved better outcomes than levothyroxine monotherapy. The results demonstrated significant reductions in thyroid autoantibody levels (TPOAb: MD = −63.18, 95% CI [−91.73, −34.62]; TgAb: MD = −68.56, 95% CI [−101.55, −35.57]) and improvements in thyroid hormone profiles, with increases in FT3 (MD = 0.74, 95% CI [0.20, 1.27]) and FT4 (MD = 1.10, 95% CI [0.29, 1.92]), as well as normalization of TSH concentrations (MD = −2.16, 95% CI [−3.14, −1.19], all p < 0.00001).86 In addition, Li et al conducted a large-scale randomized controlled trial with 284 women of childbearing age diagnosed with HT. The study applied a standardized 12-week acupuncture protocol at eight main acupoints (RN23, ST9, RN17, RN4, RN6, ST36, SP6, KI6) and evaluated thyroid autoantibody reduction as the primary endpoint, with secondary outcomes including ovarian function markers and fertility parameters assessed over a one-year follow-up.87 In addition, other modalities related to TCM have been investigated. Obeid et al performed a controlled pilot study on wet cupping therapy and found significant decreases in anti-TPO and anti-TG antibody titers, reductions in inflammatory markers such as ESR, and lower prolactin and TSH levels, while T4 concentrations remained unchanged. These findings indicate that wet cupping may influence immunological pathways distinct from those of acupuncture, suggesting potential complementary effects.88 The content mentioned above has been summarized in Table 2.
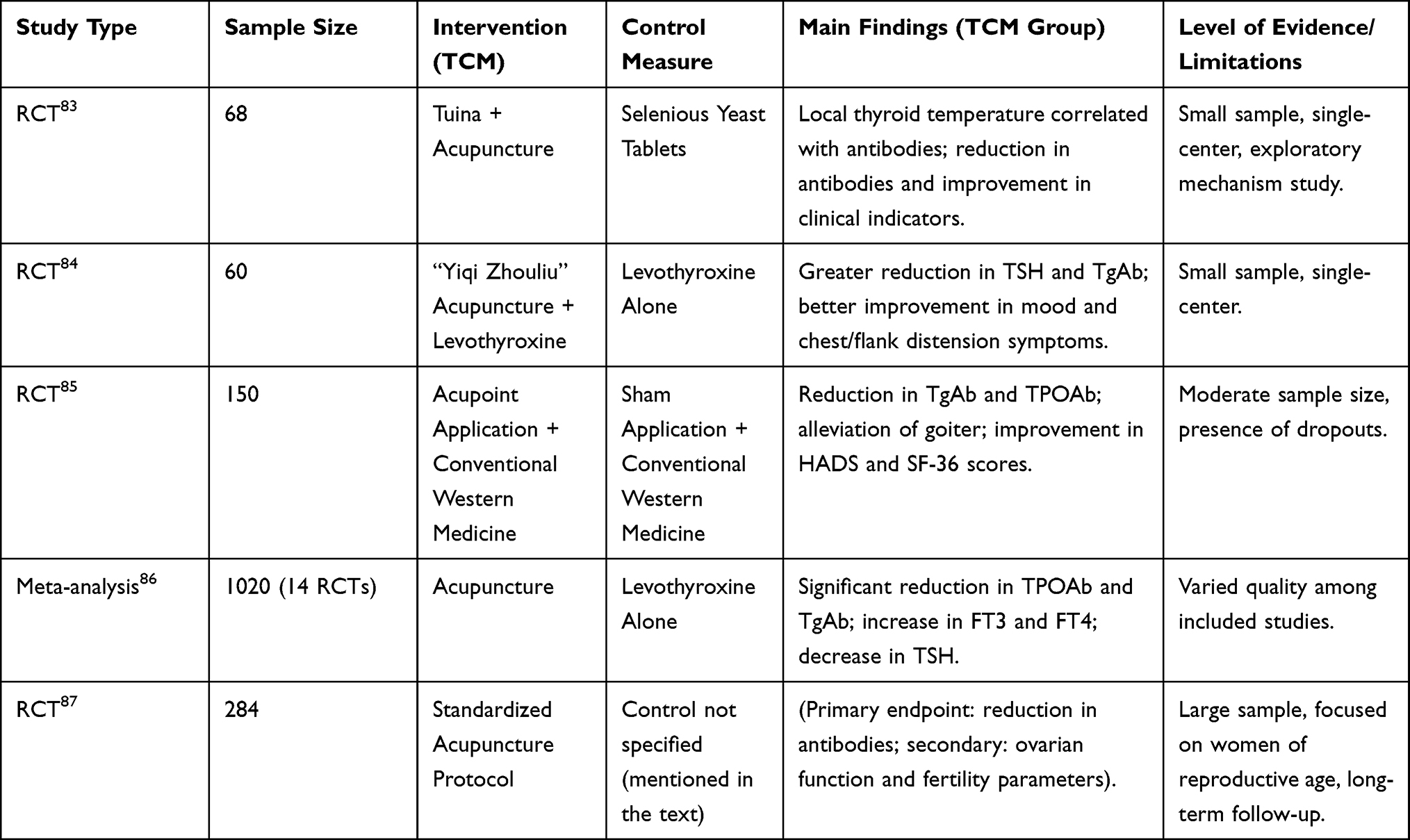 |
Table 2 Efficacy of TCM Non-Pharmacological Therapies in Hashimoto’s Thyroiditis |
Taken together, these studies support the potential benefits of acupuncture and related interventions in reducing thyroid autoantibodies, improving thyroid function, and extending treatment outcomes to include psychological, endocrine, and reproductive parameters. At the same time, the predominance of single-center studies from specific regions emphasizes the need for large, multicenter, and standardized clinical trials to confirm reproducibility and to provide reliable evidence for clinical guidelines.
Integrated TCM-Based Therapies in the Management of HT
In addition to single herbal prescriptions or acupuncture alone, several studies have explored integrated treatment strategies that combine herbal medicine, external applications, moxibustion, and acupuncture with conventional Western therapies for HT. The rationale behind these combined approaches is that they may simultaneously improve thyroid function, reduce autoimmune activity, and relieve symptoms, while also addressing syndrome patterns described in TCM.Wang et al89 conducted an RCT to evaluate the clinical efficacy of Xiaoyaosan Jiawei granules combined with external application of TCM. Sixty-six HT patients were randomized into two groups: the control group (n=33), which received selenium yeast tablets, and the observation group (n=33), which received oral Xiaoyaosan Jiawei granules in addition to external TCM application. The study compared thyroid function indicators, antibody levels, and TCM syndrome scores before and after treatment. Results showed that the combined therapy significantly improved thyroid hormone levels, lowered thyroid antibody titers, and relieved clinical symptoms. These findings suggest that combining oral and external TCM treatment with standard therapy may provide more comprehensive benefits than selenium supplementation alone. This study aimed to evaluate the clinical efficacy90 of Chaifu Xiaoying Fang in conjunction with moxibustion for the Another RCT investigated Chaifu Xiaoying Fang combined with moxibustion in patients with hypothyroidism due to HT and accompanied by liver depression and spleen deficiency.90 Eighty-seven patients were enrolled, with 43 in the control group and 44 in the treatment group. In the control group, 41 patients completed levothyroxine treatment, while in the treatment group, 41 patients (after three exclusions) received levothyroxine plus Chaifu Xiaoying Fang and moxibustion. After 12 weeks, the treatment group demonstrated significant improvements, including reduced thyroid gland size on ultrasound, lower levels of TPOAb and TGAb, and improved clinical symptoms. Blood tests also showed decreased IL-17 and IL-23 levels and increased levels of Resolvin E1 (RVE1), suggesting that this combined therapy may improve thyroid function and reduce autoimmune inflammation.Further support for integrated therapy was provided by Huang et al,91 who evaluated Xiaochaihu Decoction and Danggui Shaoyao Powder combined with acupuncture. Eighty patients with HT were randomized into a control group (n=40) receiving levothyroxine alone and a treatment group (n=40) receiving levothyroxine together with the two decoctions and acupuncture. The outcomes measured included TCM syndrome scores, thyroid function markers (FT3, FT4, TSH, TPOAb, TGAb), peripheral blood T cell subsets, and thyroid volume. Compared with the control group, the treatment group showed significant improvements in thyroid hormone levels, reductions in autoantibody titers, and favorable changes in T cell subsets. Clinically, patients also reported relief of symptoms, reflecting benefits for both thyroid and immune function (Figure 4).
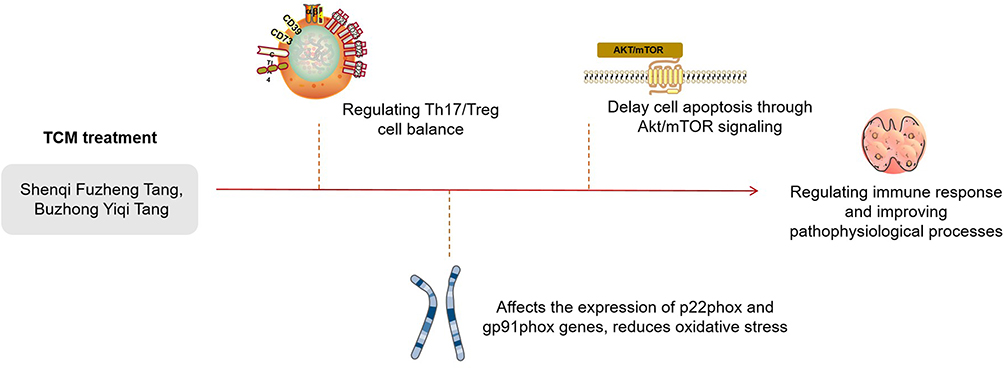 |
Figure 4 The mechanism of action of traditional Chinese medicine in the treatment of Hashimoto’s thyroiditis. |
Moreover, recent systematic evidence has further substantiated the therapeutic potential of integrated TCM approaches in HT management, with expanding research demonstrating synergistic benefits of multimodal interventions. Building upon conventional acupuncture and herbal combinations, emerging research has explored specialized moxibustion techniques, with multiple clinical investigations demonstrating that herbal cake-partitioned moxibustion, often combined with levothyroxine, produces measurable improvements in thyroid autoantibody profiles and clinical symptom scores in patients with chronic lymphocytic thyroiditis and HT, particularly those classified with spleen-kidney yang deficiency patterns according to TCM differentiation.92 Additionally, mechanistic studies using experimental autoimmune thyroiditis models have elucidated that integrated moxibustion therapies exert their therapeutic effects through modulation of inflammatory cytokine networks, regulation of microRNA expression profiles involved in immune responses, and potential influence on thyroid cellular autophagy pathways, providing biological rationale for the clinical observations.93 The content mentioned above has been summarized in Table 3.
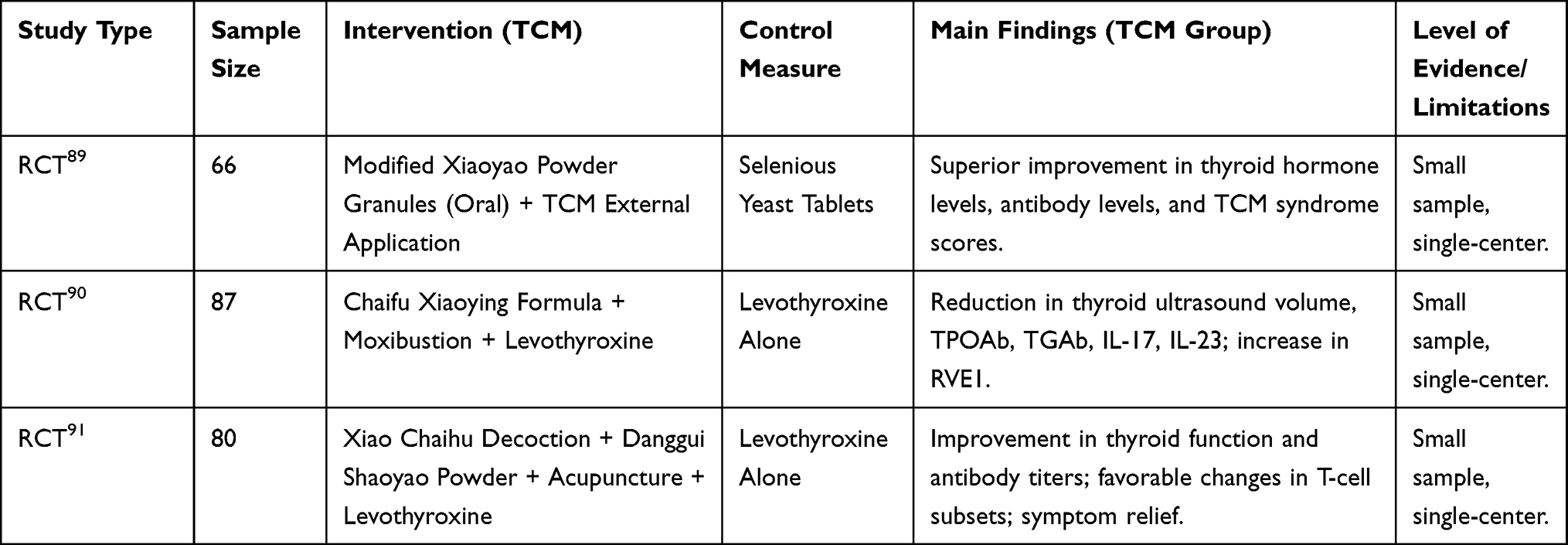 |
Table 3 Efficacy of Integrated TCM Therapies in Hashimoto’s Thyroiditis |
In summary, studies on integrated TCM-based therapies indicate that combining herbal medicine, external application, moxibustion, or acupuncture with conventional treatment may enhance therapeutic outcomes in HT. These regimens appear to improve thyroid function, lower antibody titers, modulate immune responses, and relieve clinical symptoms more effectively than Western medicine alone. However, the trials conducted so far are limited in scale, often single-center, and of short duration. Larger multicenter RCTs with longer follow-up are necessary to confirm these findings and to better define their role in clinical practice. Current evidence nevertheless supports the use of integrated TCM as a promising complementary approach in the management of HT. (See Figure 5).
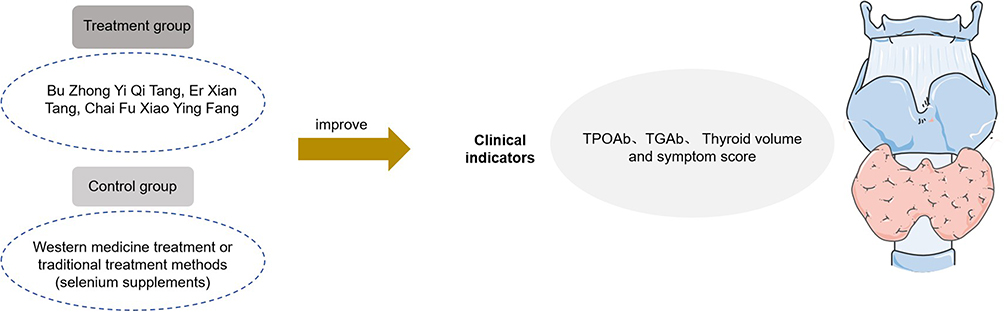 |
Figure 5 The efficacy and clinical research of TCM comprehensive treatment for HT. |
Long-Term Follow-Up and Durability of Effects
HT is a chronic autoimmune condition that requires ongoing monitoring. National integrated-care guidance recommends regular follow-up every 6–12 months with thyroid function testing, and ultrasound when indicated, as part of long-term management; these recommendations apply whether patients receive Western therapy alone or integrated TCM–Western care.53 These documents also emphasize staged management and the need for continued review over time, underscoring that patients “require long-term follow-up and management”.52 Evidence on the persistence of TCM-associated benefits remains limited. A recent survey of randomized trials in HT found that long-term outcomes are rarely reported, with “far-term prognosis” endpoints representing <1% of all outcome frequency, whereas laboratory measures dominate; the authors call for core outcome sets that include longer follow-up and quality-of-life measures.94 Multiple cited clinical trials have incorporated patient-reported outcome measures to assess improvements in symptoms and quality of life. For example, in the trial investigating Buxu Jutang combined with levothyroxine treatment, Meng et al (2022) reported significant reductions in depression and anxiety scores, measured using validated scales, during follow-up assessments, alongside improvements in overall quality of life.81 Similarly, studies on acupuncture and acupoint application consistently utilized tools such as the Hospital Anxiety and Depression Scale (HADS) and the 36-Item Short Form Health Survey (SF-36), confirming significant alleviation of emotional distress, fatigue, and physical discomfort, as well as enhanced overall health perception.84,85,87 Additionally, a Traditional Chinese Medicine syndrome element efficacy scale, specifically developed for patients with Hashimoto’s thyroiditis who maintain normal thyroid function, provides a validated and purpose-built tool for quantifying symptom changes across dimensions such as energy, mood, and local neck discomfort, and has been applied in recent clinical evaluations.62 These data indicate that the clinical benefits of Traditional Chinese Medicine interventions for HT extend beyond reductions in antibody levels to include meaningful improvements in patients’ daily functioning and quality of life.
Challenges and Opportunities
Despite encouraging findings, the evidence base for TCM in HT remains constrained by several important limitations. Many of the available clinical trials are single-center in nature, include relatively small sample sizes, and employ short follow-up periods, thereby limiting their ability to capture long-term efficacy and safety. Methodological weaknesses, such as inadequate blinding and heterogeneous control interventions, further restrict the reliability of reported outcomes.
A particularly important issue concerns the impact of TCM on thyroid hormone levels and thyroid autoantibodies, which represent the primary biomarkers of disease activity. Although several trials and meta-analyses have reported reductions in TPOAb and TgAb titers and improvements in thyroid function indices, these effects are frequently modest, inconsistently documented across studies, or not sustained during extended follow-up. Furthermore, inconsistencies in laboratory thresholds, outcome definitions, and reporting standards complicate cross-trial comparisons and make it difficult to determine the true clinical significance of the observed changes. Beyond these outcome-related concerns, the heterogeneity of TCM diagnostic frameworks and the variation in formula composition hinder reproducibility and standardization. Mechanistic studies have increased in recent years, but most still focus on single herbs or isolated compounds rather than the integrative prescriptions commonly used in practice, limiting their translational value.
Future advancement in this field depends on multicenter, well-designed randomized controlled trials with adequate sample sizes, extended follow-up, and uniform assessment of thyroid hormone and antibody outcomes, combined with standardized TCM syndrome definitions to enhance reproducibility. Parallel mechanistic investigations employing integrative approaches, supported by omics and systems biology, are also required to delineate underlying pathways and refine therapeutic strategies, thereby providing a stronger scientific basis for the application of TCM in HT.
Conclusion
HT is a multifactorial autoimmune disorder in which genetic, environmental, and epigenetic factors interact to drive chronic immune-mediated destruction of the thyroid gland. Conventional management with levothyroxine replacement corrects hypothyroidism but does not adequately address the underlying autoimmune mechanisms or the persistence of symptoms in many patients. Evidence from clinical and mechanistic studies indicates that TCM, including herbal formulations, acupuncture, and integrated approaches, can improve thyroid function, reduce autoantibody titers, and alleviate clinical symptoms by modulating immune balance, reducing oxidative stress, and protecting thyroid follicular cells from apoptosis. From a clinical perspective, TCM offers a complementary option for patients who remain symptomatic despite biochemical euthyroidism, particularly when tailored to individual syndrome patterns and combined with standard therapy. At the same time, challenges remain, including heterogeneity in syndrome differentiation, variability in herbal formulations, and limited long-term follow-up data. To enhance clinical applicability, future research should prioritize large, multicenter randomized controlled trials with standardized protocols, longer follow-up periods, and consistent evaluation of thyroid hormone and antibody outcomes. Parallel mechanistic investigations using omics and systems biology are also essential to better define the biological pathways affected by TCM interventions and to establish reproducibility across populations.
In summary, TCM provides a promising adjunctive strategy for the management of Hashimoto’s thyroiditis. Its integration into routine clinical practice requires standardization of diagnostic criteria, rigorous evaluation of efficacy and safety, and incorporation of patient-centered outcomes, including quality of life and health economics. Addressing these areas will facilitate the translation of TCM from complementary use to evidence-based, integrative management of autoimmune thyroid disease.
Abbreviations
HT, Hashimoto’s thyroiditis; APS, autoimmune polyendocrine syndromes; TCM, Traditional Chinese Medicine; TPO, thyroid peroxidase; MG, myasthenia gravis; TPOAb, thyroid peroxidase antibodies; TSH, thyroid-stimulating hormone; FT4, free thyroxine; FT3, free triiodothyronine; MRI, magnetic resonance imaging; anti-TGAb, anti-thyroglobulin antibodies; HLA, human leukocyte antigen; CTLA-4, cytotoxic T lymphocyte-associated protein 4; PTPN22, protein tyrosine kinases, and non-receptor type 22; TG, thyroglobulin; Th17, T helper 17; IgG4-BD, IgG4-related diseases; Tregs, Regulatory T cells; RCT, randomized controlled trial; TGAb, thyroglobulin antibody (TGAb); IFN-γ, interferon-γ; IL-10, interleukin-10; HADS, Hospital Anxiety and Depression Scale; SF-36, Short Form 36 Health Survey; RVE1, Resolvin E1.
Funding
The Scientific Research Project for High-level Talents of Jiangsu Medical College (20216105).
Disclosure
The authors declare that they have no affiliation with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
1. Hashimoto H. Zur Kenntnis der lymphomatösen Veränderung der Schilddrüse (Struma lymphomatosa). Arch Klin Chir. 1912;97:219–18.
2. McLeod DS, Caturegli P, Cooper DS, Matos PG, Hutfless S. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. JAMA. 2014;311(15):1563–1565. doi:10.1001/jama.2013.285606
3. Ralli M, Angeletti D, Fiore M, et al. Hashimoto’s thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev. 2020;19(10):102649. doi:10.1016/j.autrev.2020.102649
4. Song R-H, Yao Q-M, Wang B, Li Q, Jia X, Zhang J-A. Thyroid disorders in patients with myasthenia gravis: a systematic review and meta-analysis. Autoimmun Rev. 2019;18(10):102368. doi:10.1016/j.autrev.2019.102368
5. Yao Q, Song Z, Wang B, Jia X, Li Q, Zhang J-A. Thyroid disorders in patients with systemic sclerosis: a systematic review and meta-analysis. Autoimmun Rev. 2019;18(6):634–636. doi:10.1016/j.autrev.2019.01.003
6. Nakamura H, Usa T, Motomura M, et al. Prevalence of interrelated autoantibodies in thyroid diseases and autoimmune disorders. J Endocrinol Invest. 2008;31:861–865. doi:10.1007/BF03346432
7. Feldt-Rasmussen U, Høier-Madsen M, Bech K, Bliddal H, Date J. Anti-thyroid peroxidase antibodies in thyroid disorders and non-thyroid autoimmune diseases. Autoimmunity. 1991;9(3):245–254. doi:10.3109/08916939109007650
8. Bliddal S, Nielsen CH, Feldt-Rasmussen U. Recent advances in understanding autoimmune thyroid disease: the tallest tree in the forest of polyautoimmunity. F1000Res. 2017;6:1776. doi:10.12688/f1000research.11535.1
9. Lazúrová I, Benhatchi K. Autoimmune thyroid diseases and non-organ-specific autoimmunity. Pol Arch Med Wewn. 2012;122:55–59. doi:10.20452/pamw.1499
10. Eisenbarth GS, Gottlieb PA. Autoimmune polyendocrine syndromes. N Engl J Med. 2004;350(20):2068–2079. doi:10.1056/NEJMra030158
11. Jabrocka-Hybel A, Skalniak A, Piątkowski J, Twardowska K, Pach D, Hubalewska-Dydejczyk A. How much of the predisposition to Hashimoto’s thyroiditis can be explained based on previously reported associations? J Endocrinol Invest. 2018;41:1409–1416. doi:10.1007/s40618-018-0910-4
12. Brčić L, Barić A, Gračan S, et al. Genome-wide association analysis suggests novel loci for Hashimoto’s thyroiditis. J Endocrinol Invest. 2019;42:567–576. doi:10.1007/s40618-018-0955-4
13. Lo MS, Towne M, Vannoy GE, et al. Monogenic Hashimoto thyroiditis associated with a variant in the thyroglobulin (TG) gene. J Autoimmun. 2018;86:116–119. doi:10.1016/j.jaut.2017.09.003
14. Aeschlimann FA, Batu ED, Canna SW, et al. A20 haploinsufficiency (HA20): clinical phenotypes and disease course of patients with a newly recognised NF-κB-mediated autoinflammatory disease. Ann Rheum Dis. 2018;77(5):728–735. doi:10.1136/annrheumdis-2017-212403
15. Raja YZ, Alireza H, Motasem MA, et al. Consanguinity and the risk of Hashimoto’s thyroiditis. Thyroid. 2017;27(3):341–348.
16. Hori T, Ohnishi H, Kadowaki T, et al. Autosomal dominant Hashimoto’s thyroiditis with a mutation. Clin Pediatr Endocrinol. 2019;28(3):91–96. doi:10.1297/cpe.28.91
17. Negro R, Attanasio R, Grimaldi F, et al. A 2016 Italian survey about the clinical use of selenium in thyroid disease. Eur Thyroid J. 2016;5(3):164–170. doi:10.1159/000447667
18. Wichman J, Winther KH, Bonnema SJ, Hegedüs L. Selenium supplementation significantly reduces thyroid autoantibody levels in patients with chronic autoimmune thyroiditis: a systematic review and meta-analysis. Thyroid. 2016;26(12):1681–1692. doi:10.1089/thy.2016.0256
19. Marsit CJ. Influence of environmental exposure on human epigenetic regulation. J Exp Biol. 2015;218(1):71–79. doi:10.1242/jeb.106971
20. Cañas CA, Cañas F, Bonilla-Abadía F, Tobón GJ, Montoya-Ortiz G. Epigenetic changes associated to environmental triggers in autoimmunity. Autoimmunity. 2016;49(1):1–11. doi:10.3109/08916934.2015.1086996
21. Wang B, Shao X, Song R, Xu D, Zhang JA. The emerging role of epigenetics in autoimmune thyroid diseases. Front Immunol. 2017;8:396. doi:10.3389/fimmu.2017.00396
22. Mazzone R, Zwergel C, Artico M, et al. The emerging role of epigenetics in human autoimmune disorders. Clin Clin Epigenet. 2019;11:34. doi:10.1186/s13148-019-0632-2
23. Feil R, Fraga MF. Epigenetics and the environment: emerging patterns and implications. Nat Rev Genet. 2012;13(2):97–109. doi:10.1038/nrg3142
24. Brix TH, Hegedüs L. Twin studies as a model for exploring the aetiology of autoimmune thyroid disease. Clin Endocrinol. 2012;76(4):457–464. doi:10.1111/j.1365-2265.2011.04318.x
25. Gleicher N, Barad DH. Gender as risk factor for autoimmune diseases. J Autoimmun. 2007;28(1):1–6. doi:10.1016/j.jaut.2006.12.004
26. Brand O, Gough S, Heward J. CTLA-4 and PTPN22: the shared genetic master-key to autoimmunity? Expert Rev Mol Med. 2005;7(23):1–15. doi:10.1017/S1462399405009981
27. Weetman AP. The immunopathogenesis of chronic autoimmune thyroiditis one century after Hashimoto. Eur Thyroid J. 2013;1(4):243–250. doi:10.1159/000343834
28. Johar A, Sarmiento-Monroy JC, Rojas-Villarraga A, Cañas C, Tobón GJ, Anaya JM. Definition of mutations in polyautoimmunity. J Autoimmun. 2016;72:65–72. doi:10.1016/j.jaut.2016.05.003
29. Santos LR, Durães C, Mendes A, et al. A polymorphism in the promoter region of the selenoprotein S gene (SEPS1) contributes to Hashimoto’s thyroiditis susceptibility. J Clin Endocrinol Metab. 2014;99(4):E719–23. doi:10.1210/jc.2013-3539
30. Dik S, Scheepers PT, Godderis L. Effects of environmental stressors on histone modifications and their relevance to carcinogenesis: a systematic review. Crit Rev Toxicol. 2012;42(6):491–500. doi:10.3109/10408444.2012.684146
31. Turner M, Galloway A, Vigorito E. Noncoding RNA and its associated proteins as regulatory elements of the immune system. Nat Immunol. 2014;15(6):484–491. doi:10.1038/ni.2887
32. Ranzani V, Rossetti G, Panzeri I, Arrigoni A, Abrignani S, Pagani M. The long intergenic noncoding RNA landscape of human lymphocytes highlights the regulation of T cell differentiation by linc-MAF-4. Nat Immunol. 2015;16(3):318–325. doi:10.1038/ni.3093
33. Hewagama A, Richardson B. The genetics and epigenetics of autoimmune diseases. J Autoimmun. 2009;33(1):3–11. doi:10.1016/j.jaut.2009.03.007
34. Tomer Y. Mechanisms of autoimmune thyroid diseases: from genetics to epigenetics. Annu Rev Pathol. 2014;9:147–156. doi:10.1146/annurev-pathol-012513-104713
35. Limbach M, Saare M, Tserel L, et al. Epigenetic profiling in CD4+ and CD8+ T cells from Graves’ disease patients reveals changes in genes associated with T cell receptor signaling. J Autoimmun. 2016;67:46–56. doi:10.1016/j.jaut.2015.09.006
36. Jokisch F, Kleinlein I, Haller B, et al. A small subgroup of Hashimoto’s thyroiditis is associated with IgG4-related disease. Virchows Arch. 2016;468:321–327. doi:10.1007/s00428-015-1893-6
37. Rodriguez-Muñoz A, Vitales-Noyola M, Ramos-Levi A, et al. Levels of regulatory T cells CD69+ NKG2D+ IL-10+ are increased in patients with autoimmune thyroid disorders. Endocrine. 2016;51:478–489. doi:10.1007/s12020-015-0662-2
38. Vitales-Noyola M, Serrano-Somavilla A, Martínez-Hernández R, Sampedro-Núñez M, Ramos-Levi AM, Marazuela M. Patients with autoimmune thyroiditis show diminished levels and defective suppressive function of Tr1 regulatory lymphocytes. J Clin Endocrinol Metab. 2018;103(9):3359–3367. doi:10.1210/jc.2018-00498
39. Ajjan RA, Weetman AP. The pathogenesis of Hashimoto’s thyroiditis: further developments in our understanding. Horm Metab Res. 2015;47(10):702–710. doi:10.1055/s-0035-1548832
40. Zake T, Skuja S, Kalere I, Konrade I, Groma V. Heterogeneity of tissue IL-17 and tight junction proteins expression in patients with autoimmune thyroid diseases. Medicine. 2018;97(25):e11211. doi:10.1097/MD.0000000000011211
41. Vitales-Noyola M, Ramos-Levi AM, Martínez-Hernández R, Serrano-Somavilla A, Sampedro-Núñez M, Marazuela M. Pathogenic Th17 and Th22 cells are increased in patients with autoimmune thyroid disorders. Endocrine. 2017;57:409–417. doi:10.1007/s12020-017-1361-y
42. Guan L-J, Wang X, Meng S, Shi X, Wu Y, Zhang J-A. Increased IL-21/IL-21R expression and its proinflammatory effects in autoimmune thyroid disease. Cytokine. 2015;72(2):160–165. doi:10.1016/j.cyto.2014.11.005
43. Pedersen IB, Knudsen N, Jørgensen T, Perrild H, Ovesen L, Laurberg P. Thyroid peroxidase and thyroglobulin autoantibodies in a large survey of populations with mild and moderate iodine deficiency. Clin Endocrinol. 2003;58(1):36–42. doi:10.1046/j.1365-2265.2003.01633.x
44. Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on thyroid hormone replacement. Thyroid. 2014;24(12):1670–1751. doi:10.1089/thy.2014.0028
45. Boucai L, Hollowell JG, Surks MI. An approach for development of age-, gender-, and ethnicity-specific thyrotropin reference limits. Thyroid. 2011;21(1):5–11. doi:10.1089/thy.2010.0092
46. Klubo-Gwiezdzinska J, Wartofsky L. Hashimoto thyroiditis: an evidence-based guide to etiology, diagnosis and treatment. Pol Arch Intern Med. 2022;132(3):16222. doi:10.20452/pamw.16222
47. Jonklaas J. Optimal thyroid hormone replacement. Endocr Rev. 2022;43(2):366–404. doi:10.1210/endrev/bnab031
48. Caturegli P, De Remigis A, Rose N. Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmun Rev. 2014;13(4–5):391–397. doi:10.1016/j.autrev.2014.01.007
49. Anderson L, Middleton WD, Teefey SA, et al. Hashimoto thyroiditis: part 2, sonographic analysis of benign and malignant nodules in patients with diffuse Hashimoto thyroiditis. AJR Am J Roentgenol. 2010;195(1):216–222. doi:10.2214/AJR.09.3680
50. McLachlan SM, Rapoport B. Why measure thyroglobulin autoantibodies rather than thyroid peroxidase autoantibodies? Thyroid. 2004;14(7):510–520. doi:10.1089/1050725041517057
51. Jonklaas J, Bianco AC, Cappola AR, et al. Evidence-based use of levothyroxine/liothyronine combinations in treating hypothyroidism: a consensus document. Eur Thyroid J. 2021;10(1):10–38. doi:10.1159/000512970
52. Beijing Association for the Integration of Traditional and Western Medicine. Beijing expert consensus on diagnosis and treatment of Hashimoto thyroiditis (2021, Beijing). J Integr Chin West Med. 2022;34(01). doi:10.20047/j.issn1673-7210.2022.34.01
53. China Association of Chinese Medicine. Guidelines for diagnosis and treatment of Hashimoto’s thyroiditis by combining traditional Chinese and Western medicine (2025). J Chin Med Assoc. 2025;08:049. doi:10.13193/j.issn.1673-7717.2025.08.049
54. Cui Z, Wang Z, Liu X, Cai Y, Xu X, Yang T. Establishment of clinical diagnosis model of Graves’ disease and Hashimoto’s thyroiditis. J Transl Med. 2019;17(1):11. doi:10.1186/s12967-018-1765-3
55. Takasu N, Yoshimura Noh J. Hashimoto’s thyroiditis: tGAb, TPOAb, TRAb and recovery from hypothyroidism. Expert Rev Clin Immunol. 2008;4(2):221–237. doi:10.1586/1744666X.4.2.221
56. Vargas-Uricoechea H, Nogueira JP, Pinzón-Fernández MV, Schwarzstein L. The usefulness of thyroid antibodies in the diagnostic approach to autoimmune thyroid disease. Antibodies (Basel). 2023;12(3):48. doi:10.3390/antib12030048
57. Barić A, Brčić L, Gračan S, et al. Thyroglobulin antibodies are associated with symptom burden in patients with Hashimoto’s thyroiditis: a cross-sectional study. Immunol Invest. 2019;48(2):198–209. doi:10.1080/08820139.2018.1529040
58. Iwamoto Y, Kimura T, Itoh T, et al. Structural and functional differences in autoantibody-positive compared to autoantibody-negative hypothyroid patients with chronic thyroiditis. Sci Rep. 2023;13(1):15044. doi:10.1038/s41598-023-42765-z
59. Yamashiro I, Saito OC, Chammas MC, Tessler FN, Hoang JK. Ultrasound findings in thyroiditis. Radiol Bras. 2007;40(1):33–39.
60. Ushakov AV. Principles and features of ultrasound hypoechogenicity in diffuse thyroid pathology. Quant Imaging Med Surg. 2024;14(3):2655–2668. doi:10.21037/qims-23-1357
61. Höfling DB, Cerri GG, Juliano AG, Marui S, Buchpiguel CA, Chammas MC. Value of thyroid echogenicity in the diagnosis of chronic autoimmune thyroiditis. Radiol Bras. 2008;41(6):409–414. doi:10.1590/S0100-39842008000600012
62. Ma W, Qi S, Shang J, et al. Preliminary development of a TCM syndrome evaluation scale for Hashimoto’s thyroiditis with normal thyroid function: based on expert consultation and clinical investigation. Chin Gen Pract. 2025;28(28):3590–3597.
63. Chinese Committee of Interventional Thyroidology, Chinese Society of Endocrinology, Chinese Medical Association. Expert consensus workshop report: guidelines for thermal ablation of thyroid tumors (2019 edition). J Cancer Res Ther. 2020;16(5):960–966. doi:10.4103/jcrt.JCRT_558_19
64. Huang S, Ziros PG, Chartoumpekis DV, et al. Traditional Chinese medicine for Hashimoto’s thyroiditis: focus on selenium and antioxidant phytochemicals. Antioxidants. 2024;13(7):868. doi:10.3390/antiox13070868
65. Gan X, Shu Z, Wang X, et al. Network medicine framework reveals generic herb-symptom effectiveness of traditional Chinese medicine. arXiv [q-bio.MN]. 2022.
66. Wu W, Zhang W, Wang J, et al. Clinical efficacy and related mechanism of Shenqi Fuzheng Decoction in the treatment of Hashimoto’s thyroiditis with hypothyroidism. Tianjin J Tradit Chin Med. 2024;41(07):835–839.
67. Zhou C. Study on the Mechanism of Buzhong Yiqi Decoction Regulating Key Enzymes of Vitamin D Metabolism and DNA Methylation in AIT mice [dissertation]. 2023.
68. Li H. Study on the Mechanism of Acupuncture Regulating Treg/Th17 Immune Imbalance in Rats with Hashimoto’s Thyroiditis [dissertation]. 2023.
69. Xie F, Xiong Q, Li Y, et al. Traditional Chinese medicine regulates Th17/Treg balance in treating inflammatory bowel disease. Evid Based Complement Alternat Med. 2022;2022:6275136. doi:10.1155/2022/6275136
70. Zhang J, Yu Y, Yu L, et al. Intervention of Sanjie Xiaoying Granule on oxidative stress in rats with experimental autoimmune thyroiditis. Mod Pract Med. 2022;34(08):988–991.
71. Zhao Y, Tan Y, Xia F, et al. Effect of Qijianxiaoying Prescription in treating Hashimoto’s thyroiditis of qi -deficiency and blood -stasis type and its influence on ferroptosis markers GPX4, LPO and COX-2. JLiaoning Univ Tradit Chin Med. 2024;26(04):190–194.
72. Hai YP, Lee AC, Chen K, Kahaly GJ. Traditional Chinese medicine in thyroid-associated orbitopathy. J Endocrinol Invest. 2023;46(6):1103–1113. doi:10.1007/s40618-023-02024-4
73. Yao T, Wan M. Protective effect of Buzhong Yiqi Granule on experimental autoimmune thyroiditis rats via Akt/mTOR pathway. Shaanxi J Tradit Chin Med. 2023;44(02):159–164.
74. Liu GX, Chen F, Gao W, et al. Effects of astragaloside IV on apoptosis of thyroid cells and the RhoA/ROCK2 pathway in rats with Hashimoto’s thyroiditis. Chin J Immunol. 2023;39(12):2517–2522.
75. An W, Lai H, Zhang Y, Liu M, Lin X, Cao S. Apoptotic pathway as the therapeutic target for anticancer traditional Chinese medicines. Front Pharmacol. 2019;10:758. doi:10.3389/fphar.2019.00758
76. Wang YY, Sun YP, Yang BY, Wang QH, Kuang HX. Application of metabolomics and network analysis to reveal the ameliorating effect of four typical “hot” property herbs on hypothyroidism rats. Front Pharmacol. 2022;13:955905. doi:10.3389/fphar.2022.955905
77. Liu S, Shi D, Li P, et al. Modified Buzhong Yiqi Decoction combined with selenium preparation for Hashimoto’s thyroiditis with qi- and yin-deficiency: a clinical observation. Zhonghua Health Care. 2024;42(21):27–30.
78. Zhou M, Wu Q, Li Y, et al. Modified Erxian Decoction for Hashimoto’s thyroiditis with hypothyroidism: a clinical observation. Shanxi J Tradit Chin Med. 2024;40(07):17–19.
79. Hu C, Guan Z, Cao L, et al. Yiqi Qingjie Formula for Hashimoto’s thyroiditis (qi -deficiency, toxin -stagnation type) and its influence on T -cell subsets. Chin J Tradit Chin Med Sci Technol. 2024;31(03):385–8,510.
80. Wang C, Ma W, Qin L, Wu L, Liu T. Efficacy of Xiaoyao-San preparations in treating Hashimoto’s thyroiditis: a meta-analysis and systematic review. Front Pharmacol. 2025;16:1528506. doi:10.3389/fphar.2025.1528506
81. Meng X, Liu S, Deng X, et al. Clinical efficacy of Bupleurum inula flower soup for immune damage intervention in Hashimoto’s thyroiditis: a placebo-controlled randomized trial. Front Pharmacol. 2022;13:1049618. doi:10.3389/fphar.2022.1049618
82. Wei M, Ma W, Zhang W, et al. Efficacy and safety of Ophiocordyceps sinensis in the treatment of Hashimoto’s thyroiditis: a systematic review and meta-analysis. Front Pharmacol. 2023;14:1272124. doi:10.3389/fphar.2023.1272124
83. Ren H, Zhou T, Shao Y, et al. Massage plus acupuncture for Hashimoto’s thyroiditis: effects on neck body -surface temperature. Shizhen Tradit Chin Med Materia Medica. 2024;35(11):2619–2624.
84. Wang WL, Gu JH, Wang J. “Qi-circulation” acupuncture therapy for hypothyroidism of Hashimoto’s thyroiditis (liver-qi stagnation type): a clinical study. J Tradit Chin Med. 2023;29(12):57–61.
85. Qiao X, Liu B, Mou S, et al. Acupoint application for Hashimoto’s thyroiditis of liver-qi stagnation type: a randomized controlled trial. Chin Acupunct Moxibustion. 2024;44(05):513–520.
86. Wang X, Li Y, Xie H, et al. Effect of acupuncture on Hashimoto thyroiditis: a systematic review and meta-analysis. Medicine. 2024;103(9):e37518. doi:10.1097/MD.0000000000037518
87. Li F, Qi Z, Hua L, Wang X, Ling M, Juan D. The efficacy of acupuncture for the treatment and the fertility improvement in child-bearing period female with Hashimoto disease: a randomized controlled study. Medicine. 2020;99(27):e21229. doi:10.1097/MD.0000000000021229
88. Landau MB, Abdelmaksoud A, Hussein MH, et al. Reviving ancient therapeutics in modern medicine: an immunological and biological narrative review of wet cupping in the management of Hashimoto’s thyroiditis. Gland Surg. 2024;13(7):1291–1305. doi:10.21037/gs-24-173
89. Wang F, Li M. Xiaoyaosan Jiawei Granule plus external TCM application for Hashimoto’s thyroiditis: clinical effect. Med Clin Res. 2024;41(02):188–191.
90. Zhou W, Zhang L, WenQ, et al. Chaifu Xiaoying Fang plus moxibustion for Hashimoto’s thyroiditis with hypothyroidism (liver -depression, spleen -deficiency): 41 cases. Global J Tradit Chin Med. 2023;16(12):2575–2578.
91. Huang T, Zhou Y, Zhang M. Xiaochaihu Decoction and Danggui Shaoyao Powder plus acupuncture: effects on thyroid function and immune factors in Hashimoto’s thyroiditis. China Contemp Med. 2022;29(11):49–51.
92. Chen K, Zhao J, Qiao Y, et al. Effects of herbal cake-partitioned moxibustion on the expression of thyroid autophagy-related factors LC3B and Beclin-1 in rats with autoimmune thyroiditis. J Acupunct Tuina Sci. 2022;20(6):429–437. doi:10.1007/s11726-022-1345-1
93. Liu YN. Effect of Herbal Cake-Partitioned Moxibustion on microRNA Expression Profiles and Immunomodulatory Mechanisms in Rats with Experimental Autoimmune Thyroiditis [dissertation]. Shanghai: Shanghai University of Traditional Chinese Medicine; 2019.
94. Qiao X, Li J, Qu J, et al. Study on application of outcome indicators in randomized controlled trials of Hashimoto’s thyroiditis. Acta Chin Med. 2024;39(311):893–900. doi:10.16368/j.issn.1674-8999.2024.04.151
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.