Back to Journals » Patient Preference and Adherence » Volume 12
Exploring strategies to support medication adherence in patients with inflammatory arthritis: a patient-oriented qualitative study using an interactive focus group activity
Authors Rai SK, Howren A, Wilcox ES, Townsend AF, Marra CA ![]() , Aviña-Zubieta JA, De Vera MA
, Aviña-Zubieta JA, De Vera MA ![]()
Received 19 May 2018
Accepted for publication 17 July 2018
Published 5 October 2018 Volume 2018:12 Pages 2015—2025
DOI https://doi.org/10.2147/PPA.S174672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract presented by Mary A De Vera.
Views: 557
Sharan K Rai,1 Alyssa Howren,1,2 Elizabeth S Wilcox,3 Anne F Townsend,1,4 Carlo A Marra,1,5 J Antonio Aviña-Zubieta,1,6 Mary A De Vera1,2
1Arthritis Research Canada, Vancouver, BC, Canada; 2Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada; 3School of Population and Public Health, University of British Columbia, Vancouver, BC, Canada; 4University of Exeter Medical School, Exeter, UK; 5School of Pharmacy, Otago University, Dunedin, New Zealand; 6Division of Rheumatology, Department of Medicine, University of British Columbia, Vancouver, BC, Canada
Objective: Medication non-adherence is a substantial problem among patients with inflammatory arthritis (IA). Our aim was to explore IA patients’ perspectives on strategies to support medication adherence.
Methods: We collaborated with a leading arthritis patient group and conducted a qualitative study on individuals with IA who were taking at least one medication for their IA. An experienced facilitator led participants through a focus group exercise where participants were asked to design, and then discuss, strategies and/or tools supporting medication use. We applied thematic analysis using an iterative, constant comparative approach.
Results: We studied six focus groups with 27 participants diagnosed with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and comparatively under-represented conditions in this research area such as Sjögren’s syndrome. Five themes emerged throughout the analysis. Two themes – 1) adapting to life with IA and 2) the complexities and dynamic nature of taking medications – describe learning to live with a chronic condition and the challenges encountered when using long-term medications. Three themes – 3) developing lifestyle strategies for medication use (eg, having physical reminders and prompts), 4) becoming informed about medications (eg, information at time of diagnosis, means of receiving information) and 5) receiving support (eg, from health care team members, from family) – offer perspectives on facilitators to medication use. From the relationship between the latter themes, a framework was developed that encompasses means of receiving information and support as actionable targets for patient-oriented adherence interventions for IA.
Conclusion: This patient-oriented study highlights the importance of developing timely adherence interventions for IA. Our findings also led to a framework describing means of receiving information, such as through digital media and support, including from health care team members and family, as actionable targets for patient-oriented adherence interventions for IA.
Keywords: inflammatory arthritis, medication adherence, concordance, facilitators, barriers, qualitative research, synthetic DMARDs, biologic DMARDs
Introduction
Long-term pharmacotherapy is paramount to the successful management of inflammatory arthritis (IA), as patients rely on medications to relieve symptoms, perform daily life activities and prevent irreversible joint and organ damage.1 Systematic reviews synthesizing adherence rates as low as 10% in gout,2 25% in systemic lupus erythematosus (SLE)3 and 30% in rheumatoid arthritis (RA)4 are alarming, given the association between non-adherence and adverse outcomes, including increased health care utilization,5,6 costs7–9 and decreased ability to work.10 Given this substantial burden of non-adherence among patients with IA, there is an urgent need for work in designing and evaluating interventions that promote and support treatment adherence. However, to date, such research has been disappointing, with less than half of published interventions reporting a significant impact on medication adherence or clinical outcomes.11 These data support the importance of soliciting patient input to inform the development of successful adherence strategies and interventions.
Patient-oriented research, defined as meaningful and active collaboration in priority setting, conducting and translating research,12 may provide an ideal opportunity to address the burden of non-adherence in IA. To illuminate practical strategies and solutions that may be operationalized into effective adherence interventions through a patient-centered lens, we conducted a patient-oriented qualitative study in partnership with a leading national arthritis patient group based in British Columbia (BC), Canada. Our objective was to explore IA patients’ perspectives on tools and strategies to support chronic medication use using an interactive focus group activity.
Methods
Patient partnership
We partnered with the Arthritis Patient Advisory Board (APAB) of Arthritis Research Canada, a leading national consumer group of individuals living with IA who regularly collaborate in arthritis research.13 As we describe in further detail below, APAB members were engaged throughout the research process, including grant preparation (with one member appointed as a co-investigator on the study team), participant recruitment, focus group activity design and refinement, data analysis and interpretation and manuscript writing.
Study sample
Eligible participants were those who met the following criteria: 1) rheumatologist-confirmed diagnosis of IA, 2) 19 years of age or older, 3) currently taking medication (eg, disease modifying anti-rheumatic drugs [DMARD]) for their IA and 4) able to communicate in English. Participants were recruited from rheumatology clinics in the lower mainland of BC. APAB supported study recruitment through their various social media channels, including their quarterly electronic newsletter, members’ Twitter feeds and word-of-mouth advertising. Although we originally intended to include only patients with RA, APAB members recommended including a broader range of inflammatory arthritis, given that many conditions share similar treatments, and to ensure capture of rarer conditions that were less represented in prior qualitative research of medication use. As such, we purposively sampled participants on age, sex, type and duration of IA diagnosis and IA medication(s) prescribed to obtain diverse perspectives and experiences.
Study design and methodology
We used a qualitative approach for data gathering, specifically focus group methodology, as processes and interactions within focus groups more readily facilitate people’s exploration and clarification of views than one-on-one interviews and can enhance the depth and breadth of the information obtained.14,15 We used a relatively novel technique of incorporating a group activity to focus the attention of the group on the core topic of the study.16 Specifically, a trained facilitator asked participants to describe or design at least one strategy and/or tool (whether hypothetical or currently available) that would support their medication use on color-coded labels and corresponding activity sheets provided. Participants were then invited to share their strategies/tools with the group and the facilitator used open-ended questions to promote discussion. To allow sufficient time for the activity and subsequent discussion, focus groups were formed with four to six participants. Each focus group interaction lasted approximately two hours and was audio recorded and transcribed verbatim for analysis. At least one study team member attended all focus group interactions as an observer, noting elements of participants’ actions and interactions. APAB inputs for the focus group design included providing feedback on the topic guide to ensure the use of appropriate and accessible language that would effectively engage participants; furthermore, we conducted a pilot focus group interaction with six APAB members to identify areas for improvement in execution of the group activity. The uses of color-coded labels and activity sheets were a direct result of this pilot focus group with APAB, as we had originally proposed the uses of poster boards and cards attached with velcro, which were found cumbersome and potentially challenging for the target patient population.
Data analysis
Analysis of the focus group data was guided by thematic analysis informed by aspects of grounded theory17 and used an iterative, constant comparative approach.18 The first step in this approach was open coding, whereby each line of the transcript was ascribed individual codes that represented its main concept or phenomenon. This was an iterative process, since information from previous decisions helped to inform subsequent ones and vice versa. Constant comparison helped to identify patterns and similarities between data from different transcripts and notes were made to help inform subsequent steps in the analysis. The second step was axial coding, where codes were condensed and sorted; similar phenomena were grouped together and relationships between codes were explored and mapped. Finally, selective coding resulted in a final list of five higher-level themes and associated categories that captured the main ideas discussed by participants in relation to their experiences with the disease and medication use. This list was reviewed in relation to existing literature and theories on this topic and additional themes or categories were added. All six transcripts were subsequently reviewed and recoded according to these themes. Furthermore, APAB members provided input on study results during interim and final presentations on elucidated themes.
Results
We held six focus group interactions with a total of 27 participants, including 17 women and 10 men. As shown in Table 1, our sampling strategy achieved a broad representation of diagnoses, including RA, psoriatic arthritis (PsA) and ankylosing spondylitis (AS), as well as comparatively under-represented conditions in this research area (eg, Sjögren’s syndrome and granulomatosis with polyangiitis). Nine participants had been living with IA for 5 years or less and 18 participants for over 5 years. Table 1 also shows current IA medications taken by participants; methotrexate was the most common medication taken by participants (n=15), either alone or in combination with another DMARD. A total of 13 participants were taking biologic therapy.
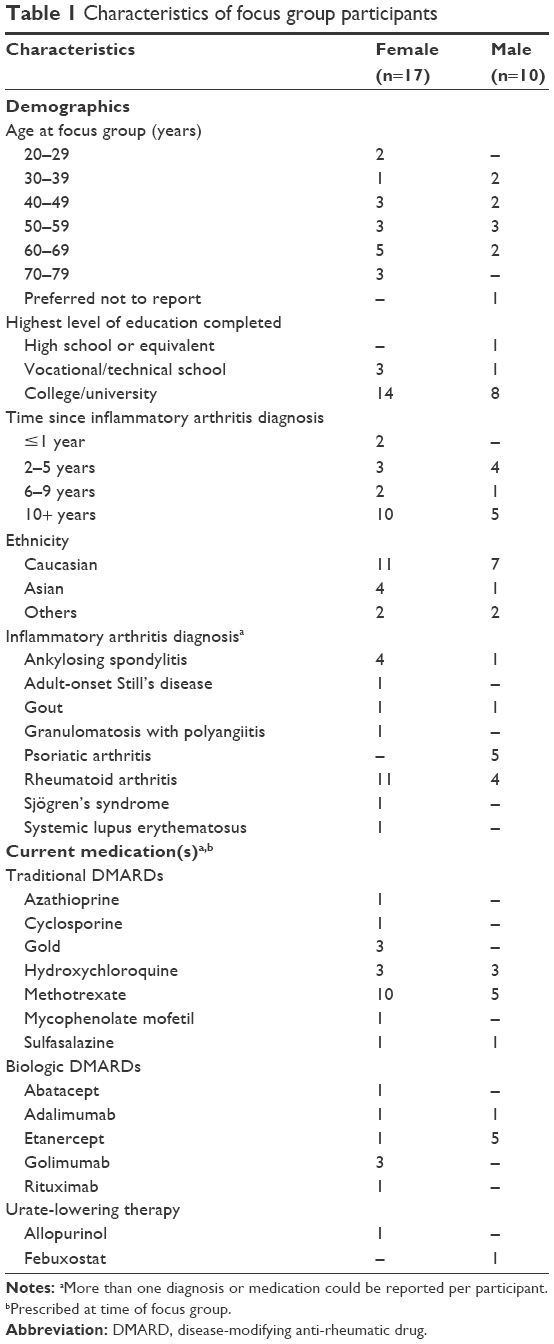 | Table 1 Characteristics of focus group participants |
Five themes emerged from the analyses. The first two themes of 1) adapting to life with IA and 2) the complexities and dynamic nature of taking medications described the interrelated experiences of living with and taking medications for IA, with illustrative quotes for each theme and category provided in Table 2. Then three overlapping and interlocking themes of 3) developing lifestyle strategies for medication use, 4) becoming informed about medications and 5) receiving support collectively capture participants’ perspectives on facilitators to medication use, as illustrated in quotes in Table 3.
 | Table 2 Illustrative quotes for themes on living with and taking medications for inflammatory arthritis |
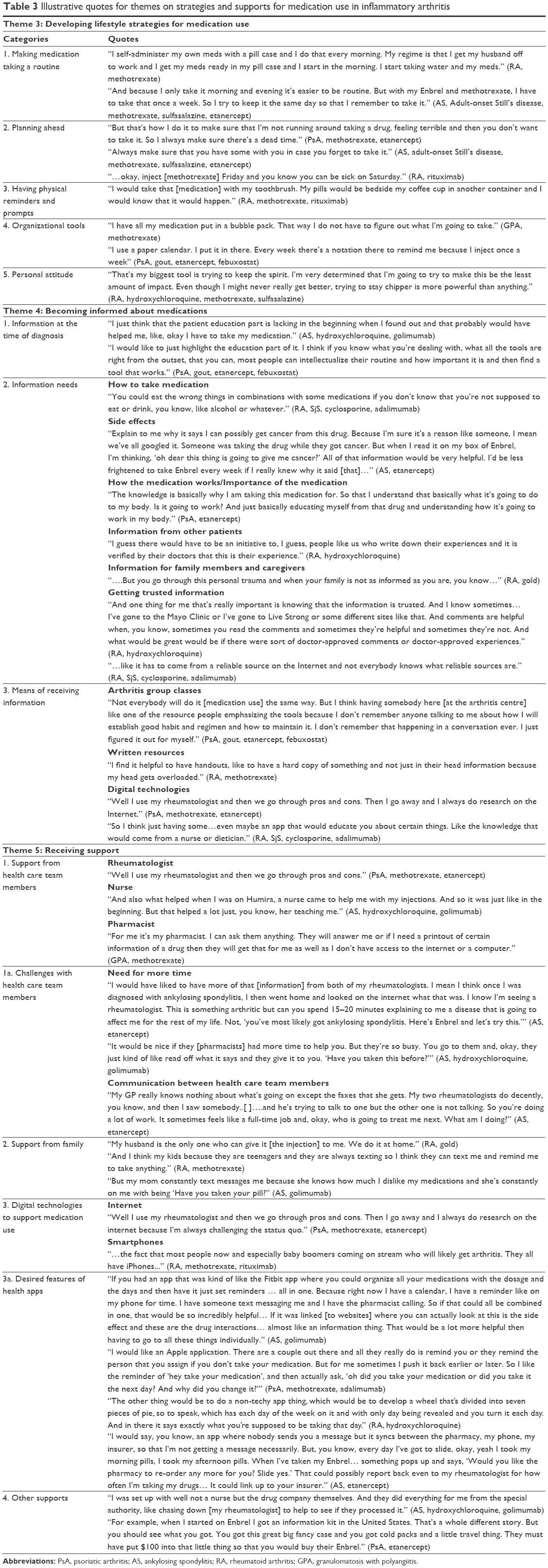 | Table 3 Illustrative quotes for themes on strategies and supports for medication use in inflammatory arthritis |
Theme 1: Adapting to life with inflammatory arthritis
The theme of adapting to life with IA was captured in four categories: 1) being diagnosed, 2) losing identity, 3) accepting the disease and 4) experiencing personal, social and career impacts. At the outset of each focus group interaction, participants detailed receiving their diagnosis, including struggling to deal with their diagnoses and searching for reasons for the onset of their condition – “I mean why did this happen to me? Is it genetic? Is it something that I ate?” (RA, methotrexate). Many also described the adjustment – both initially from being a healthy individual to having a diagnosis and the associated loss of identity, as well as with respect to long-term acceptance of living with a chronic condition. Through these, participants touched on “…big restrictions…” (RA, gold) imposed on them by their diseases, with impacts on families: “I’ve got a young kid and another one coming. So it’s tough for me to do things at home with them” (AS, etanercept), on friendships: “…I think I’ve lost friends over it…” (RA, gold) and on careers: “[Doctor] had said a while ago to apply for disability and I didn’t want to. I wanted to keep working” (AS, adult-onset Still’s disease, methotrexate, sulfasalazine, etanercept).
Theme 2: Complexities and dynamic nature of taking medications for inflammatory arthritis
Intertwined with participants’ experiences of their IA diagnoses were their experiences with medications, which were summed across six categories as complex and dynamic: “Every single drug they tried me on I have either a physical reaction or worse. So it’s been a very long frustrating journey” (RA, gold). Four categories – 1) taking medications, 2) trying different medications, 3) being able to afford medications/accessing expensive medications and 4) experiencing unwanted effects of medications – capture the challenges experienced by participants in taking medications for their IA. For example, the first category included issues on managing multiple medications and administering medications, particularly the use of needles with the sentiment “…I hate needles…” (AS, hydroxychloroquine, golimumab) echoed across focus groups. Being able to afford medications or the process of accessing medications (particularly biologics) was also identified as a challenge, as well as experiencing unwanted side effects of medications such as injection site inflammation, allergic reactions, nausea, infections and complications associated with other organs (eg, neurological complications) and worrying about long-term effects of chronic medication use. The fifth category, not taking medications, captures both intentional – “…I was very anti-drug. So when I was diagnosed, I was actually given a prescription for methotrexate, which I did not use” (RA, SjS, cyclosporine, adalimumab) – and non-intentional – “Because if I’m out with friends or if I’m really tired after a long week, I will forget” (RA, hydroxychloroquine, methotrexate, tocilizumab) reasons why participants did not take IA medications. Finally, despite challenges, we also identified a sixth category of feeling better with medications and how medications had positively impacted their IA: “It’s like a cloud has been lifted and I can function” (PsA, methotrexate, adalimumab).
Theme 3: Developing lifestyle strategies for medication use
The third theme captures lifestyle strategies, both already implemented and suggested, by participants that support medication use. Consistent across focus groups was making a routine of taking medication, for example, at the same time each day or each week, or combining it with other daily activities that can serve as a reminder: “make that medicine so much part of your life that you do not think about it. It’s like eating.” (RA, methotrexate, rituximab). Facilitating the development of routines was planning ahead, for example, injecting methotrexate on weekends and having medications on hand at all times, as well as having physical reminders and prompts, such as placing medications with routine household items (eg, beside a toothbrush). Organizational tools such as blister packs obtained from pharmacies as well as pill cases were also found to be useful, along with calendars.
Theme 4: Becoming informed about medications
In the fourth theme, participants discussed various aspects of becoming informed about IA medications across three categories of: 1) receiving information at the time of diagnosis, 2) information needs and 3) means of receiving information. Participants touched on the importance of receiving sufficient information about medication at the time of IA diagnosis which some felt was lacking when they were diagnosed. Various information needs were captured in the second category including how to take the medication, side effects, as well as how the medication works and placing an emphasis on its importance: “I think the big one is impressing on a lot of people how important it is to take your medication and that missing a dose can be pretty disastrous for some people” (PsA, etanercept). Hearing about other patients’ experiences of living with IA and using prescribed medications was viewed mostly positively: “…and then from people who experience it. Just say, ‘Hey this is my experience and, you know, how it could progress. You can do this” (AS, hydroxychloroquine, golimumab). In addition to their own information needs, some felt that education of family members would also be helpful:
And if I could add I think the education of your spouse or caregiver to know that having the medications needed to be done pretty well at the same time is going to make it easier for you to be able to make the commitments for social activities and things and for that to be part of the education process. It helps to just keep the whole thing on course, right? (RA, methotrexate, sulfasalazine).
Aside from the type of information, participants also emphasized the importance of being able to recognize whether information was credible or trustworthy; this was particularly important for information collected from the Internet. The final category identified means of receiving information about medications, including group classes, written resources and in particular, digital technologies.
Theme 5: Receiving support
This theme describes a number of means by which patients receive support, including functional and emotional, from individuals such as health care providers and family members as well as other tangible supports. The first category captures the importance of education from participants’ health care providers, including rheumatologists and nurses as well as pharmacists. However, participants also noted challenges with health encounters, particularly the need for more time, especially when explaining their conditions and medications. The second category captures the importance of support from family, whether it is reminding participants to take their medications or helping administer medications. The third category captures the role of digital technologies in supporting medication use. Participants identified two main technologies – the Internet and smartphones – that they used, as well as anticipate other patients with IA using. Health apps were also discussed and within this subcategory participants described desired features and functions of medication taking apps, such as setting more detailed reminders for multiple medications (eg, including dosage information), cataloging information about missed or altered doses, recording side effects and synchronizing with the pharmacy and insurance company. Finally, within the fourth category, some participants also noted other supports, including patient support programs provided by drug companies for the use of biologics:
I was set up with, well not a nurse but the drug company themselves. And they did everything for me from the special authority, like chasing down [my rheumatologist] to help to see if they processed it (AS, hydroxychloroquine, golimumab).
Relationship between themes
From our analyses, there are two essential considerations for adherence – information (as captured in Theme 4) and support (as captured in Theme 5) and we outline a framework for patient-oriented adherence interventions for IA. In the framework shown in Figure 1, actionable targets for adherence interventions for IA represent potential areas for designing patient-oriented adherence interventions. These areas may be in the form of receiving support as captured by Theme 5. For example, an adherence intervention may be designed to facilitate encounters with health care team members to optimize patient support. Another target area for an adherence intervention for IA is through means of receiving support as captured by Theme 4, category 3. With this, an adherence intervention may be designed around arthritis group classes, written resources, or digital technologies as means to deliver information. Outside of the actionable targets but also key to this framework is Theme 4’s category 1 of “information needs” which represents inputs for these actionable targets in terms of patient-identified knowledge gaps that could be readily addressed by the interventions.
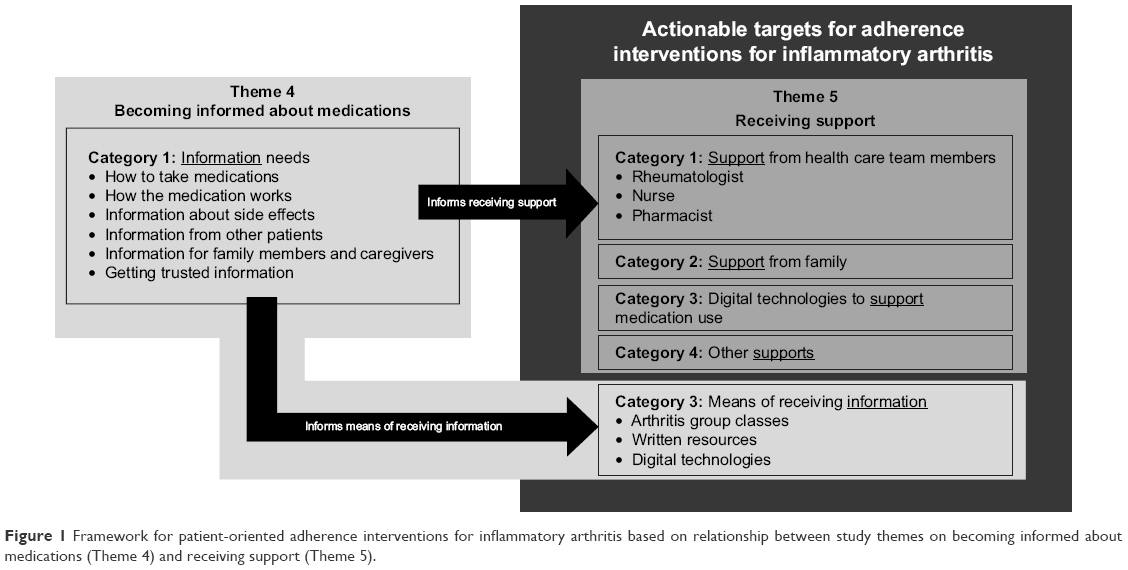 | Figure 1 Framework for patient-oriented adherence interventions for inflammatory arthritis based on relationship between study themes on becoming informed about medications (Theme 4) and receiving support (Theme 5). |
Discussion
We conducted a patient-oriented qualitative study using an interactive focus group activity to better understand IA patients’ perspectives on and experiences with chronic medication use. Findings of this study conducted in partnership with a national arthritis consumer group include participant accounts of the complexities and dynamic nature of living with and taking medications for IA. Our study also confirms the importance of having information and receiving support as key facilitators of taking medication and has expanded on these with categories describing when information should be delivered, what type of information is needed and the means of receiving information. Aside from identifying individuals who provide functional and emotional support (eg, health care team and family members), participants also identified other tangible supports for medication use including digital technologies. Taking these together lends itself to a framework for patient-oriented adherence interventions for IA that encompasses means of receiving information and support as actionable targets for patient-oriented adherence interventions for IA.
Aside from confirming recommendations, including those from the European League Against Rheumatism on patient education for people with IA as priority care,19 our finding on the importance of becoming informed about medications supports results from our prior systematic review of medication adherence interventions in IA, that those shown to have an impact on adherence outcomes included an educational component.11 Perhaps more valuable, the current qualitative study identifies tangible areas for education development drawn directly from patients with IA such as when information should be delivered (ie, at the time of diagnosis) and what information is desired. With respect to the latter, our findings suggest that educational tools that effectively present how to take medications, how medications work, including potential benefits in addition to the risks may be helpful to individuals with IA. Furthermore, patients with IA emphasized the need for information to be drawn from the experiences of other patients, which has been echoed in studies in RA20 and SLE21 populations. For example, utilizing other patients’ experiences may help to alleviate apprehensions about medication side effects, as identified in prior studies.22,23 Lastly, patient preferences for information delivery extended beyond the typical health care setting to patient groups, written resources and digital technologies, thereby highlighting future avenues for intervention development. Such informational tools and resources may be further bolstered by behavioral strategies that support daily medication use. Indeed, participants in the current study described specific strategies used to overcome the daily logistical challenges encountered with long-term medication use.
Study participants with IA indicated multiple opportunities to optimize medication adherence through functional and/or emotional support, namely by means of health care professionals, family and digital technologies. Indeed, the important role of health care providers in supporting medication use has been shown in recent qualitative syntheses among patients with RA,20 systemic autoimmune rheumatic diseases,24 and gout.25 Importantly, our study adds a collective perspective from IA patients, including those living with less common forms of IA, on some of the challenges with health care providers, including the need for more time during encounters as well as improved communication, particularly when multiple providers are involved in a patient’s care. Also, similar to prior qualitative inquiry in IA,22,23 our focus groups articulated how family can provide reminders and assist with administering injections, all while having a deeper insight into the personal experiences and needs of the individual with IA. Aside from identifying the supporting role of family members, participants in our study also identified the need for information to be delivered to family members themselves.
In terms of other tangible supports, study participants identified the role of digital technologies which have indeed gained traction in supporting care in rheumatology, with implications for medication use.26 With health apps forming a sub-category within this theme, participants identified a number of desired features such as the ability to organize medications or serve as a means to communicate a patient’s medication taking to their rheumatologist or pharmacist. Indeed, the ubiquitous and accessible nature of digital technologies makes for potential adherence support tools. However, there remains need for work in this area. We conducted a scoping review and quality assessment and identified 704 smartphone medication adherence apps in Apple and Android platforms and noted that the primary function of the majority of apps was sending a reminder or alert to users to take their medication.27 Apps specific to rheumatic diseases, such as SLE28 and RA,29 however focus on monitoring disease activity rather than medication use. As such, subsequent directions to optimize medication adherence may include building apps specific to IA that incorporate patient preferences such as dynamic follow-up after the initial dose reminder, access to reliable drug information and synchronization with pharmacies and insurance companies.
Strengths and limitations
The strengths of our study deserve comment. Unique to our study is the patient-oriented approach used to explore medication use among individuals with IA. Engaging APAB, a renowned arthritis patient organization in Canada, throughout the research enriched the execution of this study, including input on the use of patient-friendly language in the topic guide, opportunity to pilot and refine the focus group and embedded activity, as well as providing a “patient lens” to the interpretation and reporting of the findings. Further, strengthening our study is the use of focus groups, as group processes and interactions more readily facilitate participants’ exploration and clarification of views and opinions as compared with one-on-one interviews, thereby enhancing the depth and breadth of the information obtained.14,15 Next, while the majority of focus group participants were individuals with RA, we were additionally able to recruit individuals with less common forms of IA that have generally been underrepresented in prior qualitative research in this area. Moreover, our findings across these patient populations suggest largely shared experiences and perspectives on the topic, thereby broadening the applicability of our findings.
Nevertheless, potential limitations of our study also warrant discussion. Participant recruitment primarily took place in the metropolitan city of Vancouver; however, those living in rural communities in BC were also invited to participate through phone or videoconference, thereby broadening the representation of our sample and increasing the generalizability of our findings. Next, those who voluntarily participated in our study may be more likely to use their medications as prescribed and thus might not reflect the perspectives of “non-adherent” individuals. However, this is an inherent limitation of all voluntary research studies and is not limited to the current study.
Conclusion
This patient-oriented qualitative study conducted in the Canadian province of BC has enriched our understanding of the complexities of medication use in IA. Beyond confirming the roles of information and support as facilitators of medication use, we have established a framework that identifies practical and actionable targets for patient-oriented adherence interventions for IA.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available as they contain information that could compromise participant privacy. Nevertheless, these data are available from the corresponding author on reasonable request.
Acknowledgments
This study was funded by the Canadian Rheumatology Association (CRA)’s Canadian Initiative for Outcomes in Rheumatology Care (CIORA) grant program. The study sponsor had no role in the study design, data collection, analysis/interpretation, writing of the manuscript and decision to submit the manuscript for publication. Dr De Vera holds a Canada Research Chair in Medication Adherence, Utilization and Outcomes and is a recipient of a Network Scholar Award from The Arthritis Society/Canadian Arthritis Network and a Scholar Award from the Michael Smith Foundation for Health Research. We gratefully acknowledge members of Arthritis Research Canada’s Patient Advisory Board for their contributions to the design and execution of the study.
Ethical approval
Ethics approval was obtained from the Behavioral Research Ethics Board at the University of British Columbia (protocol #H14-01460). All participants provided written informed consent.
Author contributions
All authors meet the conditions for authorship according to the IMCJE guidelines. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Campbell NKJ, Saadeldin K, De Vera MA. The Duality of Economic Issues With Medication Non-adherence in Patients With Inflammatory Arthritis. Curr Rheumatol Rep. 2017;19(10):66. | ||
De Vera MA, Marcotte G, Rai S, Galo JS, Bhole V. Medication adherence in gout: a systematic review. Arthritis Care Res. 2014;66(10):1551–1559. | ||
Mehat P, Atiquzzaman M, Esdaile JM, Aviña-Zubieta A, De Vera MA. Medication Nonadherence in Systemic Lupus Erythematosus: A Systematic Review. Arthritis Care Res. 2017;69(11):1706–1713. | ||
Salt E, Frazier SK. Adherence to disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a narrative review of the literature. Orthop Nurs. 2010;29(4):260–275. | ||
Feldman CH, Yazdany J, Guan H, Solomon DH, Costenbader KH. Medication Nonadherence Is Associated With Increased Subsequent Acute Care Utilization Among Medicaid Beneficiaries With Systemic Lupus Erythematosus. Arthritis Care Res. 2015;67(12):1712–1721. | ||
Julian LJ, Yelin E, Yazdany J, et al. Depression, medication adherence, and service utilization in systemic lupus erythematosus. Arthritis Rheum. 2009;61(2):240–246. | ||
Borah BJ, Huang X, Zarotsky V, Globe D. Trends in RA patients’ adherence to subcutaneous anti-TNF therapies and costs. Curr Med Res Opin. 2009;25(6):1365–1377. | ||
Pasma A, Schenk C, Timman R, et al. Does non-adherence to DMARDs influence hospital-related healthcare costs for early arthritis in the first year of treatment? PLoS One. 2017;12(2):e0171070. | ||
Halpern R, Mody RR, Fuldeore MJ, Patel PA, Mikuls TR. Impact of noncompliance with urate-lowering drug on serum urate and gout-related healthcare costs: administrative claims analysis. Curr Med Res Opin. 2009;25(7):1711–1719. | ||
Pavelka K, Forejtova S, Stolfa J, et al. Anti-TNF therapy of ankylosing spondylitis in clinical practice. Results from the Czech national registry ATTRA. Clin Exp Rheumatol. 2009;27(6):958–963. | ||
Galo JS, Mehat P, Rai SK, Avina-Zubieta A, De Vera MA. What are the effects of medication adherence interventions in rheumatic diseases: a systematic review. Ann Rheum Dis. 2016;75(4):667–673. | ||
Canadian Institutes of Health Research. Strategy for Patient-Oriented Research; 2017. Available from: http://www.cihr-irsc.gc.ca/e/41204.html. Accessed December 15, 2017. | ||
Leese J, Kerr S, Mckinnon A, et al. Evolving Patient-Researcher Collaboration: An Illustrative Case Study of a Patient-Led Knowledge Translation Event. J Particip Med. 2017;9(1):e13. | ||
Kitzinger J. Qualitative research. Introducing focus groups. BMJ. 1995;311(7000):299–302. | ||
Kitzinger J. The methodology of Focus Groups: the importance of interaction between research participants. Sociol Health Illn. 1994;16(1):103–121. | ||
Colucci E. “Focus groups can be fun”: the use of activity-oriented questions in focus group discussions. Qual Health Res. 2007;17(10):1422–1433. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
Boeije H. A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual Quant. 2002;36(4):391–409. | ||
Zangi HA, Ndosi M, Adams J, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015;74(6):954–962. | ||
Kelly A, Tymms K, Tunnicliffe DJ, et al. Patients’ Attitudes and Experiences of Disease-Modifying Antirheumatic Drugs in Rheumatoid Arthritis and Spondyloarthritis: A Qualitative Synthesis. Arthritis Care Res. 2018;70(4):525–532. | ||
Sutanto B, Singh-Grewal D, McNeil HP, et al. Experiences and perspectives of adults living with systemic lupus erythematosus: thematic synthesis of qualitative studies. Arthritis Care Res. 2013;65(11):1752–1765. | ||
Brandstetter S, Hertig S, Loss J, Ehrenstein B, Apfelbacher C. ‘The lesser of two evils…’ – views of persons with rheumatoid arthritis on medication adherence: a qualitative study. Psychol Health. 2016;31(6):675–692. | ||
Voshaar M, Vriezekolk J, van Dulmen S, van den Bemt B, van de Laar M. Barriers and facilitators to disease-modifying antirheumatic drug use in patients with inflammatory rheumatic diseases: a qualitative theory-based study. BMC Musculoskelet Disord. 2016;17(1):442. | ||
Haag H, Liang T, Avina-Zubieta JA, de vera MA. How do patients with systemic autoimmune rheumatic disease perceive the use of their medications: a systematic review and thematic synthesis of qualitative research. BMC Rheumatology. 2018;2(1):9. | ||
Rai SK, Choi HK, Choi SHJ, et al. Key barriers to gout care: a systematic review and thematic synthesis of qualitative studies. Rheumatology. 2018;57(7):1282–1292. | ||
Dixon WG, Michaud K. Using technology to support clinical care and research in rheumatoid arthritis. Curr Opin Rheumatol. 2018;30(3):276–281. | ||
Li J, Tsao N, Campbell N, De Vera MA. Smartphone Medication Adherence Mobile Apps: A Scoping Review and Quality Assessment. Vancouver, BC, Canada: University of British Columbia Multidisciplinary Undergraduate Research Conference; 2018. | ||
Pourrahmat M, Zusman EZ, De Vera MA. Patient-targeted smartphone apps for systemic lupus erythematosus: A systematic review and assessment of feature and quality. Amsterdam, Netherlands: European League Against Rheumatism Annual European Congress of Rheumatology; 2018. | ||
Grainger R, Townsley H, White B, Langlotz T, Taylor WJ. Apps for People With Rheumatoid Arthritis to Monitor Their Disease Activity: A Review of Apps for Best Practice and Quality. JMIR Mhealth Uhealth. 2017;5(2):e7. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.