Back to Journals » Psychology Research and Behavior Management » Volume 18
Exploring Risky Decision-Making in Depressed Patients with High Aggression: An Event-Related Potential Study
Authors Huang L, Zhang Q, Pan W ![]() , Li Q, Wang Z, Liu Y, Geng F, Wang K, Zhang M, Zhu C
, Li Q, Wang Z, Liu Y, Geng F, Wang K, Zhang M, Zhu C
Received 3 June 2025
Accepted for publication 21 August 2025
Published 16 September 2025 Volume 2025:18 Pages 1993—2008
DOI https://doi.org/10.2147/PRBM.S538756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Lei Huang,1,* Qingqing Zhang,1,* Woxin Pan,1 Qianqian Li,2 Zixu Wang,1 Yiming Liu,1 Feng Geng,2 Kai Wang,1,3– 6 Mengzhu Zhang,7 Chunyan Zhu1– 5
1School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, 230032, People’s Republic of China; 2Department of Psychology and Sleep Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, 230601, People’s Republic of China; 3Anhui Province Key Laboratory of Cognition and Neuropsychiatric Disorders, Hefei, 230032, People’s Republic of China; 4Collaborative Innovation Center of Neuropsychiatric Disorders and Mental Health, Hefei, 230032, People’s Republic of China; 5Institute of Artificial Intelligence, Hefei Comprehensive National Science Center, Hefei, 230032, People’s Republic of China; 6Department of Neurology, The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China; 7Affiliated Psychological Hospital of Anhui Medical University, Anhui Mental Health Center, Hefei Fourth People’s Hospital, Hefei, 230032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mengzhu Zhang, Email [email protected] Chunyan Zhu, Email [email protected]
Background: Beyond self-injurious and suicidal behaviors, depressed patients may show outward aggression. However, it remains unclear whether high levels of aggression in depressed patients are associated with abnormalities in decision-making processes and altered sensitivity to feedback.
Methods: Ninety-six depressed patients were recruited and divided into two groups (n = 48 patients each) based on aggression. Patients completed psychological tests (Balloon Analog Risk Task and Iowa Gambling Task [IGT]), with event-related potentials recorded during the IGT to measure neural responses to feedback.
Results: Depressed patients with high aggression showed stronger risk aversion on the IGT compared to those with low aggression. Electrophysiological findings indicated that depressed patients with high aggression generate larger feedback-related negativity (FRN) components in response to losses, as well as greater FRN amplitude differences between loss and win. The FRN difference wave (loss–win) was significantly correlated with higher scores on the anger dimension of the Buss-Perry Aggression Questionnaire, trait anger scale, emotion regulation difficulties, and depression severity, supporting heightened feedback sensitivity as a mechanism underlying aggression in depression.
Limitations: The cross-sectional design limits causal inference, and the relatively small ERP subsample may affect generalizability of electrophysiological findings.
Conclusion: Depressed patients with high aggression exhibited stronger electrophysiologic responses to negative feedback during risky decision-making. This hypersensitivity may contribute to aggression in depression, highlighting a potential clinical target for interventions that modulate feedback sensitivity or emotional reactivity.
Keywords: depressed patients, high aggression, risky decision-making, iowa gambling task, event-related potentials, ERPs
Introduction
The lifetime prevalence of depressive disorders in China is 6.8% with a 12-month prevalence of 3.6%.1 Depression is not only highly prevalent but is frequently accompanied by self-harm, and in some cases, violent suicide attempts.2,3 While most research has focused on self-injurious suicidal behaviors in depressed patients, outward expressions of violent tendencies may also pose significant risks to others and society. Depressed patients are more likely to exhibit hostile attributional biases,4,5 respond with angry outbursts,6 and demonstrate greater impulsivity compared to the general population,7 which are also risk factors for aggressive behavior. Previous studies identified a link between depressive symptoms and aggression in non-clinical populations.8 This relationship is even more pronounced in clinical populations. Fazel et al9 reported that depressed patients are three times more likely to commit violent offenses compared to general population controls. Additionally, adolescents with depression in low- and middle-income countries are more likely to engage in risky behaviors, including delinquency and self-injurious suicidal actions.10
Executive dysfunction is a well-established risk factor for violent behavior11 with abnormalities in decision-making (a critical executive function), which often contributes to negative behavioral outcomes. Studies investigating risky decision-making in violent offenders have shown that violent offenders tend to exhibit greater risk-seeking biases compared to non-violent offenders.12 Findings on risky decision-making are inconsistent among depressed patients. For example, while some studies using the Iowa Gambling Task (IGT) indicate a greater propensity for risk-taking among depressed patients compared to healthy controls,13 other studies have reported reduced risk-taking14 or no significant differences.15 These differences make it challenging to determine whether the heightened aggression observed in depressed patients is associated with abnormalities in decision-making processes. Additionally, suicidal behaviors, which can be conceptualized as a form of inward aggression (self-directed violent impulses), may share underlying mechanisms with outward aggression. However, the relationship between decision-making and suicidal tendencies in depressed patients is also inconsistent. Some studies have found no association between suicide attempts and impaired performance on the IGT,16 while other studies have reported significantly impaired decision-making abilities in patients with unipolar depression who have attempted suicide.17 Taken together, these inconsistent findings suggest that examining aggression from a decision-making perspective may provide important insight for uncovering its underlying mechanisms.
Most studies on decision-making in depressed patients have focused on behavioral outcomes, with limited attention given to the intrinsic mechanisms underlying these processes. Loss aversion, a central aspect of value-based decision-making,18 has received increasing attention in aggression research. Some studies suggest that violent offenders with psychiatric disorders, such as schizophrenia,19 intermittent explosive disorder,20 and borderline personality disorder,21 exhibit reduced sensitivity to negative feedback, indicating weaker loss aversion. This diminished sensitivity may cause violent offenders to disregard the potential punishments of unfavorable decisions. Conversely, other studies have proposed the opposite, showing that heightened sensitivity to negative feedback is associated with increased aggression.22,23 For example, adolescents with antisocial behavior exhibit significantly heightened blood oxygen level-dependent responses in anatomic regions, such as the dorsolateral prefrontal cortex and orbital frontal cortex, during risky decision-making involving loss feedback.24 This hypersensitivity to negative feedback may also correlate with intensified negative emotions, such as anger25 and rumination.26 In fact, negative emotional experiences are often key contributors to maladaptive behaviors.
In the context of depression, heightened sensitivity to negative feedback has been consistently observed.27,28 For example, Rygula et al29 reviewed animal studies showing that “pessimistic” traits are associated with increased responsiveness to negative feedback compared to “optimistic” traits. Similarly, Fan et al30 demonstrated a positive correlation between sensitivity to negative feedback and psychological distress in patients with major depressive disorder using the Balloon Analog Risk Task (BART) and event-related potentials (ERPs). Furthermore, enhanced loss aversion may drive suicidal behaviors in depressed patients because depressed patients seek to escape the psychological pain associated with negative feedback.31 Therefore, we hypothesize that heightened sensitivity to negative feedback in depressed patients, contrasting with patterns seen in other psychiatric disorders, may increase psychological distress and elevate risk for outward aggression.
Despite these findings, most studies on risky decision-making in depressed patients have relied on single tasks and lacked an in-depth examination of the reward and punishment mechanisms or the neurophysiologic underpinnings. ERP studies on decision-making have identified two key components that reflect the brain’s response to feedback (feedback-related negativity [FRN] and P3 [a positive waveform occurring 300–600 ms after feedback]). FRN, originating in the anterior cingulate cortex,32 typically occurs 200–300 ms after feedback onset and reflects sensitivity to discrepancies between expected and actual outcomes,33 error detection,34 and conflict monitoring.35 Additionally, FRN reflects appraisal of the motivational or affective impact of the error.36 Negative feedback elicits a more negative FRN amplitude compared to positive feedback.37 P3 reflects parietal cortex activity38 and is associated with the allocation of attentional resources to salient environmental information.39,40 Studies on decision-making have shown that the P3 component responds more strongly to negative feedback than to positive feedback.30,41
Although depression is strongly associated with aggression, the mechanisms underlying risky decision-making and sensitivity to reward and punishment have not been established. To address this gap in knowledge, depressed patients were categorized into high- and low-aggression groups, which was determined through the BART and IGT while recording ERP data during the IGT. We hypothesized that depressed patients with high aggression will exhibit heightened sensitivity to loss feedback and a greater tendency toward risk aversion in decision-making compared to depressed patients with low aggression. We further hypothesized that depressed patients with high aggression will exhibit larger FRN and P3 amplitudes under loss feedback conditions, reflecting enhanced neural sensitivity to punishment compared to low aggression counterparts.
Methods
Participants
Ninety-six patients with depression (male, n = 27; female, n = 69; mean age = 23.1 ± 7 years) were recruited from the Outpatient Psychiatric Clinic and the Inpatient Ward of the Department of Psychology and Sleep Medicine (Second Affiliated Hospital of Anhui Medical University, Anhui, China). All patients were diagnosed by a psychiatrist. The inclusion criteria were as follows: (i) met the diagnostic criteria for depressive disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5); (ii) 15–45 years of age; (iii) right-handed; (iv) normal or corrected-to-normal visual acuity; (v) no physical interventions, such as transcranial magnetic stimulation or convulsion-free electroconvulsive therapy, in the last 6 months; (vi) no intellectual deficits or history of severe physical illness or brain injury; (vii) no history of alcohol or psychoactive substance abuse; and (viii) Patient Health Questionnaire (PHQ)-9 score > 4.
Participants aged 18 years and above provided written informed consent. For participants under the age of 18, written informed consent was obtained from a parent or legal guardian in accordance with the requirements of the Ethics Committee of Anhui Medical University (approval number: 82240127). The study was conducted in accordance with the Declaration of Helsinki. Based on the study objectives, patients were categorized into high- and low-aggression groups according to their scores on the Buss-Perry Aggression Questionnaire (BP-AQ). Patients with BP-AQ scores above the median (69.5) were assigned to the high-aggression group (n = 48), while patients with BP-AQ scores below the median were assigned to the low-aggression group (n = 48). Median split has been widely used in psychiatric research involving clinical populations, including major depressive disorder samples.42 All participants completed self-report questionnaires and two behavioral tasks (BART and IGT), with the order of task administration counterbalanced across participants to control for potential order effects. To ensure statistical robustness of ERP analyses, an a priori power analysis was conducted using G*Power 3.1. Assuming a conventional medium effect size (Cohen’s f = 0.25) for group-by-condition interactions, with 80% power and α = 0.05 in a 2×2×2×2 repeated-measures ANOVA (within-subject factors: electrode position, feedback type, feedback strength; between-subject factor: group), the analysis indicated a minimum requirement of 28 participants (14 per group). Not all participants completed ERP recording during the IGT due to individual preferences and logistical constraints (eg, scheduling conflicts and willingness to undergo ERP recording). The final ERP subsample comprised 40 participants, which exceeded the minimum requirement by 43% (high-aggression: n = 21; low-aggression: n = 19). The differences in demographic and clinical characteristics between the two patient groups participating in ERP recordings were consistent with the difference in demographics and clinical characteristics observed in the overall sample. A detailed comparison of the demographic and clinical characteristics of the overall sample is presented in Table 1.
 |
Table 1 Demographic, Clinical, and BART Behavioral Characteristics of Depressed Patients with High and Low Aggression (Mean ± SD) |
Measures
The PHQ-9
The PHQ-9 is a nine-item self-report measure developed by Spitzer et al43 to assess the severity of depressive symptoms. Each item corresponds to one of the nine diagnostic criteria for major depressive disorder outlined in DSM-IV. Participants rate the frequency of each symptom on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day) with higher total scores indicating greater levels of depression. In a Chinese psychiatric sample, the Cronbach’s α for the internal consistency reliability of the PHQ-9 was 0.86, and the 2-week test–retest reliability was 0.86.44
BP-AQ
The BP-AQ is a 29-item self-report measure designed to assess four dimensions of aggression (physical aggression, verbal aggression, anger, and hostility). Responses were recorded on a 5-point Likert scale ranging from 1 (extremely uncharacteristic of me) to 5 (extremely characteristic of me) with higher scores indicating greater aggression levels. In a Chinese validation study, the Cronbach’s α for the total scale was 0.90, indicating excellent internal consistency.45
The Trait Anger Scale
The Trait Anger Scale (TAS), a subscale of the State-Trait Anger Expression Inventory-2, consists of 10 items assessing dispositional anger. The scale is further divided into two subscales (anger temperament and anger reaction). Participants rate items on a 4-point Likert scale with higher scores reflecting stronger trait anger tendencies. In Chinese populations, the TAS has demonstrated good reliability, with Cronbach’s α for the total scale reported as 0.81 in validation studies.46
Difficulties in the Emotion Regulation Scale (DERS)
The DERS is a 36-item self-report instrument designed to evaluate difficulties in regulating emotions across six dimensions (lack of emotional awareness, lack of emotional clarity, non-acceptance of emotional responses, difficulties in impulse control, difficulties engaging in goal-directed behaviors, and limited access to emotion regulation strategies). Responses are rated on a 5-point Likert scale with higher scores indicating greater emotion regulation difficulties. In Chinese validation studies, the DERS demonstrated good internal consistency (Cronbach’s α = 0.90 for the total scale; α = 0.68–0.89 for subscales) and adequate test–retest reliability (r = 0.84 for the total scale), supporting its reliability and cultural applicability.47
Behavioral Task
BART
The classic BART paradigm48 was used to examine the decision-making processes of participants. In this task, a balloon is displayed on the screen (Figure 1) and participants are instructed to press the “F” key to inflate the balloon. Each incremental inflation increases the potential earnings, which are temporarily stored in a “temporary bank”. The participants may press the “J” key to stop inflating the balloon at any time, transferring the accumulated earnings for that balloon to a “permanent bank”. The participants are instructed to maximize their total earnings during the task. Each inflation carries a risk of the balloon bursting. If the balloon bursts, all earnings for that balloon are lost and no amount is transferred to the permanent bank. The probability of the balloon bursting increases incrementally with each inflation. Balloons can be inflated up to 128 times with an average bursting point at 64 inflations. The task includes 30 balloons that are presented sequentially.
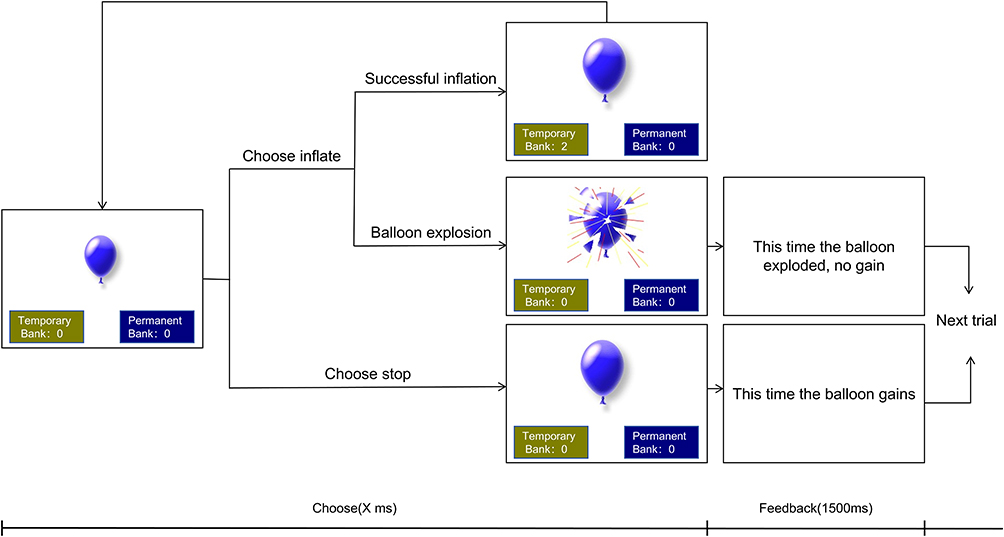 |
Figure 1 Schematic of the Balloon Analog Risk Task (BART). Notes: Participants choose to inflate or stop inflating the balloon in each trial. If the balloon is successfully inflated, a bonus is deposited into the “permanent bank” according to the number of times the balloon was inflated and the round continues. If the balloon explodes, the balloon earnings are zeroed out and the game continues to the next round. |
IGT
A modified version of the IGT,49 a reward-based learning paradigm that utilizes monetary feedback, was used. The participants were presented with two chip options, valued at 50 and 100, displayed on the screen (Figure 2) in this task. The “F” key represents the choice of 50 and the “J” key represents the choice of 100. Participants can either win or lose the selected amount by starting the task with an initial fund of ¥1000 and aiming to maximize the total earnings. The 50-chip option was designated as the favorable choice in this study and the 100-chip option was unfavorable. The probability of winning or losing varied. Specifically, the 50-chip option had a 60% probability of winning and a 40% probability of losing, whereas the probabilities were reversed for the 100-chip option. Importantly, these probabilities were not explicitly disclosed to participants at the start of the task. Instead, the participants were required to learn and adapt their decision-making strategies through feedback provided during the task. Each trial began with the presentation of the two-chip options on the screen, followed by a fixation cross displayed for 200–400 ms. After the participant made their selection by pressing a key, feedback was displayed for 1000 ms, consisting of a smiling face (indicating a win) or a crying face (indicating a loss). Subsequently, the monetary outcome of the trial (eg, the amount gained or lost) was shown for an additional 1000 ms. The modified IGT comprised a total of 300 trials divided into 6 blocks of 50 trials each.
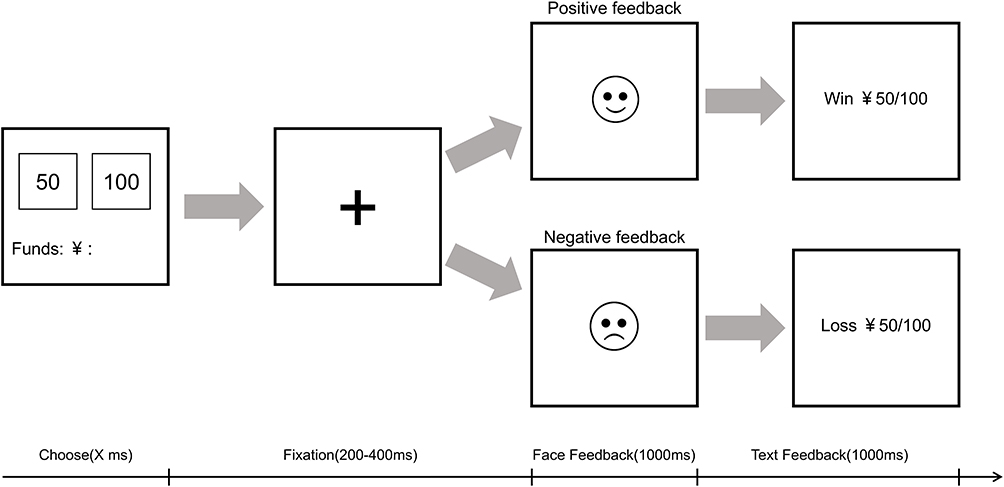 |
Figure 2 Schematic of the Iowa Gambling Task (IGT). Notes: At the beginning of each trial, two chips (valued at 50 and 100) were presented and participants were asked to make a choice. This was followed by a fixation point displayed for 200–400 ms. Based on the participant keypress responses, a feedback stimulus (either a smiling or crying face) was shown for 1000 ms. Finally, the amount of money won or lost during the trial was displayed on the screen for 1000 ms before proceeding to the next trial. |
Electroencephalogram (EEG) Recording and Pre-Processing
EEG signals were recorded using a Neuracle 32-channel portable EEG device (Changzhou, China) following the 10–20 international electrode placement system, with 32 electrodes evenly distributed across the scalp of the participant. The sampling rate was set to 1000 Hz and electrode impedance was maintained below 5 kΩ during data acquisition. The reference electrode was placed at the prefrontal location. For offline analysis, whole-brain averaging was applied for re-referencing. A low-pass filter with a cut-off of 40 Hz (24 dB/octave) was used to eliminate high-frequency noise, while a high-pass filter with a cut-off of 0.1 Hz was applied to remove baseline drift.
Data were segmented around the onset of the cued stimulus with 200 ms of pre-stimulus and 1000 ms of post-stimulus epochs. Artifacts were identified and rejected using a combination of SASICA plug-ins and visual inspection to ensure the reliability of the independent component analysis results. EEG preprocessing was conducted in EEGLAB running on MATLAB. The analysis time windows were set to 200 ms prior to stimulus onset and 1000 ms following stimulus presentation for ERPs with the 200 ms pre-stimulus period serving as the baseline. The time windows for analyzing specific ERP components were as follows: the FRN wave was analyzed within the 250–350 ms window; and the P3 wave was examined within the 410–460 ms window. Fz and Cz were selected a priori, consistent with previous ERP studies and our scalp topography results showing maximal FRN and P3 amplitudes at fronto-central sites during feedback processing.50,51
Data Analysis
The behavioral metrics for the BART included the adjusted mean number of inflations, which is defined as the mean number of inflations for unexploded balloons, the number of exploded balloons, and the number of unexploded balloons. Group membership (high- vs low-aggression group) for the IGT was treated as a between-subjects factor, while net scores across six blocks were analyzed as a within-subjects factor using repeated-measures ANOVA. The net scores were calculated by subtracting the number of unfavorable selections (100-point cards) from the number of favorable selections (50-point cards) within each block.
Repeated-measures ANOVA was performed on the raw mean wave amplitudes of the FRN and P3 components for the ERP results. Electrode position (Fz and Cz), feedback type (loss vs win) and feedback strength (50- vs 100-point feedback) were treated as within-subjects factors, while group (high vs low aggression) was included as a between-subjects factor. To further investigate the impact of feedback type, a repeated-measures ANOVA was performed on the FRN difference wave (loss-minus-win) under loss and win conditions with electrode position (Fz and Cz) and feedback strength (50- vs 100-point) as within-subjects factors and group membership as a between-subjects factor. Additionally, Pearson correlation analysis was used to determine the relationship between self-reported psychological measurement scales and the FRN difference wave. To control for false positive results arising from multiple comparisons, post-hoc pairwise comparisons following significant ANOVA effects were adjusted using the Bonferroni correction. In addition, all correlation analyses were subjected to false discovery rate (FDR) correction using the Benjamini–Hochberg procedure with α = 0.05. All statistical analyses were conducted in SPSS Statistics.
Results
Descriptive Statistics and BART Behavioral Results
A comparison of demographic and clinical characteristics (Table 1) showed that depressed patients with high aggression and depressed patients with low aggression have no significant differences in gender, age, years of education, place of residence, hospitalization rate, antidepressant use, and depression severity. However, depressed patients with high aggression scored significantly higher on the BP-AQ than depressed patients with low aggression and had a notably higher percentage of property damage or physical aggression in the past year. Additionally, depressed patients with high aggression scored significantly higher on trait anger and difficulties in emotion regulation compared to depressed patients with low aggression. There were no significant differences between the two groups in the BART behavioral results.
IGT Behavioral Results
The results of the repeated measures ANOVA revealed a significant interaction effect between block and group (F(5,470) = 3.87, P = 0.005, partial η² = 0.04). Simple effect analyses indicated no significant differences across blocks in the depressed patients with low aggression, suggesting that patients in this group consistently preferred disadvantageous options. In contrast, significant differences were detected across blocks in the depressed patients with high aggression (F(5,90) = 3.65, P = 0.005, partial η² = 0.169). Specifically, post hoc comparisons (Bonferroni-corrected) indicated that net scores in blocks 4–6 were significantly higher than in block 1 (all P values < 0.05), suggesting that individuals in this group gradually shifted to more advantageous choices over time. These findings are depicted in Figure 3.
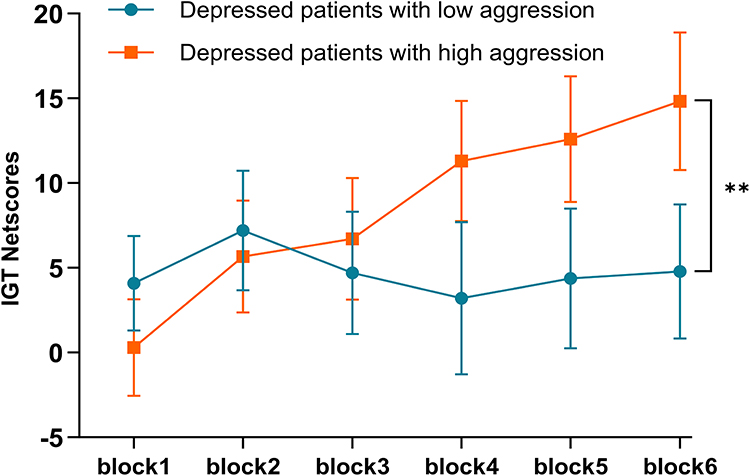 |
Figure 3 IGT Behavioral Performance in Depressed Patients with High and Low Aggression. Notes: The means and standard errors of net scores (calculated as the number of times 50 was chosen minus the number of times 100 was chosen within each interval) across the 6 blocks of the IGT. The blocks were defined as follows: block 1 = trials 1–50; block 2 = trials 51–100; block 3 = trials 101–150; block 4 = trials 151–200; block 5 = trials 201–250; and block 6 = trials 251–300. **p < 0.01. |
ERP Results
FRN
A repeated measures ANOVA on the mean amplitudes of the original FRN waveforms revealed significant main effects of feedback type (F(1,38) = 15.47, P < 0.001, partial η² = 0.289) and feedback magnitude (F(1,38) = 21.47, P < 0.001, partial η² = 0.361). The mean amplitude for loss conditions (2.24 ± 0.33 μV) was significantly larger than win conditions (3.03 ± 0.33 μV) and the mean amplitude for the 50-feedback magnitude (2.33 ± 0.34 μV) was significantly larger than 100-feedback magnitude (2.94 ± 0.31 μV). Additionally, there was a significant interaction effect between feedback type and feedback magnitude (F(1,38) = 7.22, P = 0.011, partial η² = 0.16). Significant differences were observed between loss-50 (2.05 ± 0.36 μV) and loss-100 (2.42 ± 0.32 μV), as well as between win-50 (2.60 ± 0.36 μV) and win-100 (3.46 ± 0.33 μV).
Importantly, a significant interaction effect was found between group and feedback type (F(1,38) = 4.57, P = 0.039, partial η² = 0.107). Further simple effect analyses showed that under loss conditions the mean amplitude for the depressed patients with high aggression (1.51 ± 0.48 μV) was significantly lower than the depressed patients with low aggression (2.97 ± 0.46 μV), indicating a stronger negative deflection. Given that FRN is a negative-going ERP component, a more negative FRN amplitude reflects greater neural sensitivity to negative feedback, while no significant differences were detected between the groups under win conditions. Within the depressed patients with high aggression, the mean amplitude for loss conditions (1.51 ± 0.48 μV) was significantly lower than win conditions (2.73 ± 0.48 μV), whereas no significant differences between loss and win conditions were detected in the depressed patients with low aggression. These results are illustrated in Figure 4A and B. Further analysis of the FRN difference wave (loss-win) revealed a significant main effect of group (F(1,38) = 4.57, P = 0.039, partial η² = 0.107). The depressed patients with high aggression exhibited a significantly larger FRN difference wave (−1.22 ± 0.29 μV) compared to the depressed patients with low aggression (−0.36 ± 0.28 μV), as shown in Figure 4C. Note that the FRN difference wave (loss – win) is more negative when individuals differentiate more strongly between negative and positive outcomes.
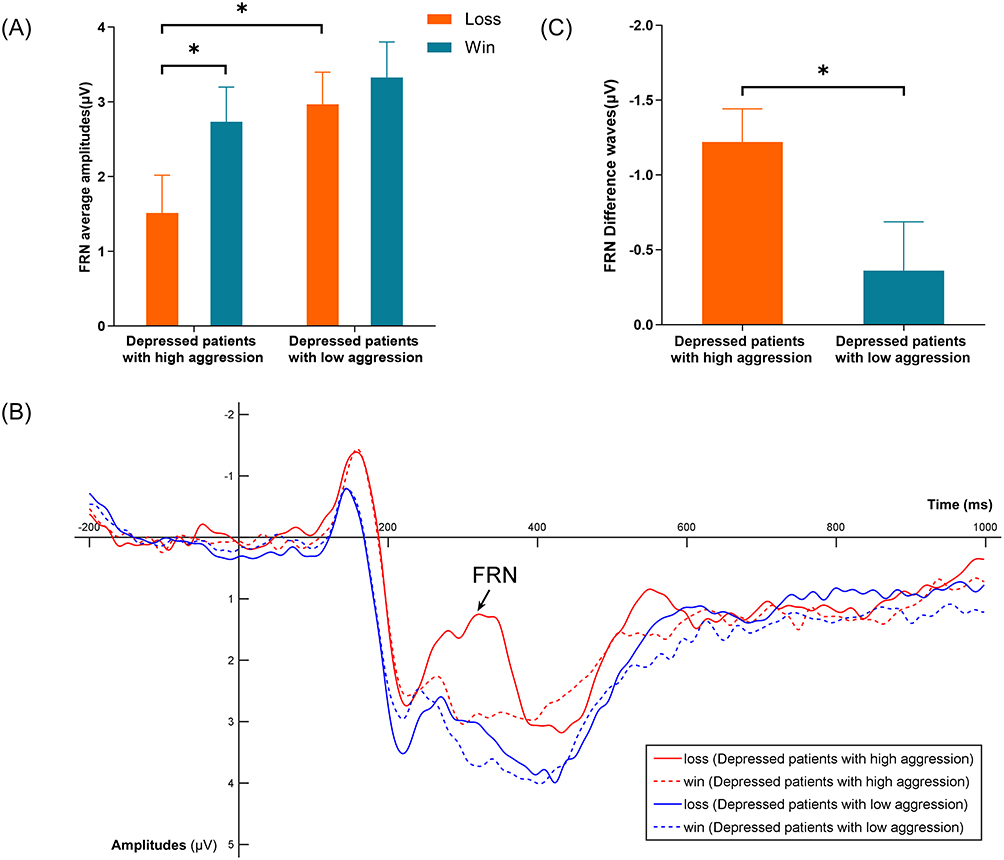 |
Figure 4 FRN Amplitudes and Difference Waves in Depressed Patients with High and Low Aggression. Notes: (A) Bar chart of the mean FRN amplitudes for depressed patients with high aggression and low aggression under win and loss conditions. (B) Waveform chart of mean FRN amplitudes for depressed patients with high aggression and low aggression under win and loss conditions. (C) Bar chart of FRN difference waves (loss - win) for depressed patients with high aggression and low aggression. All charts are averaged across electrode sites (Fz and Cz) and feedback intensities of 50-point vs 100-point. *p<0.05. |
P3
A repeated-measures ANOVA on the mean amplitudes of the P3 component revealed a significant main effect of feedback intensity (F(1,38) = 11.56, P = 0.002, partial η² = 0.233). The mean amplitude for 100-point feedback (3.57 ± 0.39 μV) was significantly greater than 50-point feedback (2.91 ± 0.41 μV). There was also a significant interaction effect of electrode × feedback type (F(1,38) = 5.70, P = 0.022, partial η² = 0.13), which showed that the mean amplitude in the loss condition (3.60 ± 0.52 μV) was significantly greater than the win condition (2.98 ± 0.48 μV) at the Fz electrode site, while no significant difference was detected between loss and win conditions at the Cz electrode site. Additionally, a trend-level interaction effect of electrode × feedback type × group existed (F(1,38) = 3.65, P = 0.064, partial η² = 0.088). Simple effect analysis indicated that the patients with high aggression had significantly greater mean amplitudes in the loss condition at the Fz electrode site (3.36 ± 0.75 μV) compared to the win condition (2.29 ± 0.69 μV), whereas no significant difference existed between loss and win conditions in the patients with low aggression. These findings are illustrated in Figure 5A and B.
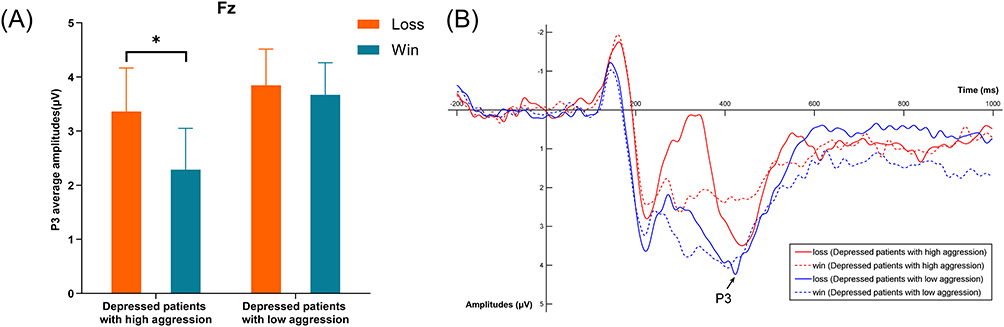 |
Figure 5 P3 Amplitudes in Depressed Patients with High and Low Aggression. Notes: (A) Bar chart of the mean P3 raw wave amplitudes for depressed patients with high aggression and low aggression under win and loss conditions at the Fz electrode point. (B) Waveform chart of mean P3 raw wave amplitudes for depressed patients with high aggression and low aggression under win and loss conditions at the Fz electrode point. Both charts are averaged across feedback intensities of 50-point vs 100-point. *p<0.05. |
Correlation Analysis
Based on Pearson correlation analysis performed on two groups of patients with depression, the FRN difference wave (loss-win) was significantly correlated with the anger subdimension of the BP-AQ (r = −0.66, P_FDR = 0.0004). Additionally, it was negatively correlated with TAS (r = −0.39, P_FDR = 0.0164), the DERS (r = −0.34, P_FDR = 0.0334), and the PHQ-9 (r = −0.56, P_FDR = 0.0004), thus indicating that higher scores on these measures are associated with a larger FRN loss–win difference (see Figure 6).
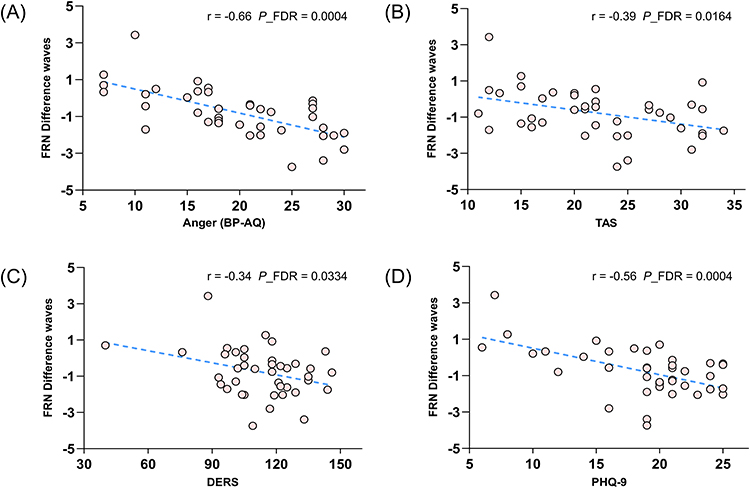 |
Figure 6 Correlations between the FRN Difference Wave (loss-win) and Clinical Symptom Scores. Abbreviations: BP-AQ, Buss-Perry Aggression Questionnaire; TAS, Trait Anger Scale; DERS, Difficulties in Emotion Regulation Scale; PHQ-9, Patient Health Questionnaire-9. Notes: (A) BP-AQ anger dimension. (B) TAS. (C) DERS. (D) PHQ-9. Negative correlations with the BP-AQ anger dimension, TAS, DERS, and PHQ-9 indicate that higher scores on these measures are associated with a larger FRN loss-win difference. |
Discussion
The classic BART paradigm and an adapted IGT task were used to examine the behavioral and electrophysiologic differences in risk decision-making between depressed patients with high and low aggression. Both groups exhibited similar behavioral patterns in the BART task. However, depressed patients with high aggression demonstrated a strong risk-avoidance learning effect on the IGT, increasingly favoring options with higher probabilities of winning. ERP data analysis revealed pronounced FRN and P3 components following negative feedback. The depressed patients with high aggression showed a larger FRN and difference wave (loss-win) compared to the depressed patients with low aggression, with similar trends observed in the P3 component. Moreover, the FRN difference wave was significantly correlated with the anger dimension of the BP-AQ, TAS, DERS, and PHQ-9 scores.
As expected, the FRN showed a significant main effect of feedback type, which was consistent with previous research and indicated that negative feedback elicited a larger FRN amplitude compared to positive feedback.37,52,53 Because the FRN reflects appraisal of the motivational or affective impact of the error36 and a bias in expectations of outcomes,33 depressed patients aimed to maximize winnings and losing money was perceived as error feedback or a deviation from the expected outcomes in the current study. Additionally, the amplitude of the response to smaller magnitude feedback was greater than larger magnitude feedback, which is also consistent with previous findings.49,54 Specifically, the FRN to a loss of 50 was larger than a loss of 100, likely because the probability of losing 50 was lower, which led to a greater expectation violation. These results suggested that the FRN amplitude is not only related to the feedback outcome (win vs loss) and feedback value (feedback intensity), but also to the probability of the outcome. This finding supports the reinforcement learning theory of the FRN,55 which posits that the perception of an outcome as good or bad is relative to deviation from expectations rather than an absolute judgment.
The mean amplitude of the P3 at Fz electrode in the loss condition was significantly greater than the win condition, which is consistent with previous studies, this finding reflects the heightened sensitivity of the P3 component to negative feedback compared to positive feedback.30,41,56 Given that the P3 is associated with the selective allocation of attentional resources to salient environmental information,39,40 negative feedback compared to positive feedback tends to evoke stronger learning and greater cognitive resource allocation. Furthermore, the significantly larger mean amplitude of the P3 in the 100-feedback intensity condition compared to the 50-feedback intensity condition indicates that the P3 is also sensitive to outcome magnitude during the feedback evaluation stage, confirming that larger outcomes elicit more pronounced P3 responses than outcomes ones.57
In our sample, compared with patients with low aggression, those with high aggression not only exhibited greater loss-related FRN amplitudes, but also showed a more pronounced difference between loss and gain conditions. Similar patterns were observed in the P3 component, where the mean amplitude difference between win and loss feedback at the Fz electrode was larger in the high-aggression depression group. These findings suggest that patients with high aggression exhibit abnormally heightened neural responses to negative information. This enhancement reflects not only an increased sensitivity to negative outcomes, but also the recruitment of greater cognitive resources to resolve conflicts between expectations and actual outcomes. The enlarged FRN may indicate amplified signaling of outcome–expectancy mismatches and a state of excessive conflict monitoring, implying that high-aggression patients require greater cognitive effort to adjust their behavior and emotional responses when encountering negative feedback. The increased P3 amplitude reflects subsequent cognitive resource allocation and information integration, with the larger win–loss difference suggesting differential attentional prioritization and processing of feedback types. These electrophysiological findings align with functional neuroimaging evidence showing that abnormalities in the prefrontal–limbic circuitry, particularly in the anterior cingulate cortex and ventromedial prefrontal cortex involved in conflict monitoring and emotion regulation, are associated with depression58,59 and aggressive behaviors.60,61 From a neurobiological perspective, depressed patients with high aggression may exhibit dysfunction in neural networks involved in feedback processing. A “hyper-sensitive, hyper-reactive” response pattern to negative feedback may lower their emotional tolerance threshold,62,63 making them more prone to becoming trapped in cycles of negative affect and triggering aggressive behaviors.
A correlation between FRN difference waves and depression scores was identified our study. Similarly, previous studies identified a positive correlation between sensitivity to negative feedback and depression,30,41 suggesting that alterations in feedback sensitivity may sustain depressive symptoms.28,64 Additionally, among the four dimensions of the BP-AQ, only anger showed an abnormal correlation with FRN difference waves. Previous studies have also reported a positive correlation between punishment sensitivity and anger, as measured by the BP-AQ,25,65 which aligns with our findings. Although we did not find a relationship between the FRN component and explicit aggression (eg, physical and verbal aggression), we hypothesize that individuals with depression may tend to suppress negative behaviors when coping with negative emotions. This suppression mechanism might lead to the accumulation of anger and other aggressive emotions. Because these unregulated emotions intensify over time, unregulated emotions may contribute to more severe emotional and behavioral regulation issues. This interpretation is consistent with the revised frustration-aggression theory, which posits that frustration, which is defined as an aversive event, triggers aggressive tendencies to the extent that a negative affect is generated.66 Furthermore, the observed correlations between FRN difference waves, trait anger, and difficulties in emotion regulation provide additional evidence for the positive association between sensitivity to negative feedback and negative emotions in individuals with depression. Individuals with heightened sensitivity to punishment often experience difficulties in emotional regulation and rely on maladaptive emotional strategies.67 Depressed patients, in particular, exhibit a lower threshold for reacting to negative emotions and face challenges in regulating these emotions,68 which contributes to an association with higher levels of aggression. This explanation aligns with the hypothesis of dysfunction in the neural circuitry of emotional regulation, which suggests that a predisposition toward aggression is linked to a reduced threshold for activating negative emotions, such as anger, distress, and agitation.69
According to the somatic marker hypothesis, emotions link past experiences with future expectations in decision-making, thereby guiding and facilitating the decision-making process.70 Depressed patients with high aggression often exhibit hypersensitivity to negative feedback on the IGT. When disadvantageous choices lead to negative outcomes and evoke negative somatic signals, the somatic marker system, which is centered in the ventromedial prefrontal cortex, labels these options with negative affective states. Negative emotions, in turn, act as signals for behavioral adjustment.71 Consequently, depressed patients with high aggression may prefer options with higher probabilities of reward, avoiding the negative emotional experiences associated with losses. An alternative perspective, the cognitive-control model, emphasizes the role of higher-order cognitive processes such as working memory, attention, and cognitive flexibility in guiding IGT performance.72,73 From this viewpoint, decision-making is shaped not only by affective biases but also by the capacity to maintain and update explicit knowledge about task contingencies, to inhibit disadvantageous choices, and to flexibly adapt to changing reward–punishment structures. Whereas the somatic marker hypothesis posits that emotional signals precede and facilitate explicit knowledge, cognitive-control accounts suggest that conscious, strategic processing can operate in parallel with or even override affective influences.74 In our study, FRN and P3 exhibited larger differences between win and loss conditions in depressed patients with high aggression, indicating stronger feedback-related learning effects. This pattern may reflect an interplay between rapid, affectively driven feedback evaluation (FRN) and later-stage cognitive integration (P3). Thus, the concurrent enhancement of FRN and P3 could be interpreted as evidence for a dual-process mechanism in which emotion-based and cognition-based systems jointly contribute to behavioral adjustment during risk-related decision-making. Future studies will be needed to explore the dynamic interaction and causal relationships between these components in guiding risk-related decisions.
In our study, we did not detect differences in the BART similar to the difference detected in the IGT, which may be attributable to task-related differences between the paradigms. Individuals must evaluate the gain-loss probabilities underlying different choices on the IGT, with the optimal strategy being to minimize risk-seeking behavior. Conversely, individuals are required to pump balloons enough to maximize rewards without bursting them on the BART, meaning that the optimal strategy involves appropriate risk-seeking.75 From the perspective of the somatic marker hypothesis, hypersensitivity to negative feedback may facilitate the association between choices and emotions. For depressed patients with high aggression, options with higher probabilities of loss may be rapidly linked with aversive emotions, leading to changes in decision-making. This pattern was more pronounced on the IGT. Additionally, the current study used a modified version of the IGT, which was simplified to better suit the study aim of examining sensitivity to feedback during decision-making. In contrast, the BART allowed a maximum of 128 pumps per balloon, introducing greater uncertainty in risk evaluation, which may have contributed to the inconsistent findings. Nevertheless, we also observed that depressed patients with high aggression performed slightly better than depressed patients with low aggression across the three behavioral outcomes on the BART. This may also reflect a stronger learning ability in this group during risk-related decision-making. Due to practical limitations and considerations regarding patient tolerance, we did not record ERP during the BART task. We anticipate corollary studies to address this limitation.
The current study had several notable limitations. First, its cross-sectional design precludes causal inference. Future work employing experimental manipulation of feedback sensitivity could better clarify its causal role in aggression among depressed individuals. Second, the sample of individuals with depression was drawn from a general hospital and included outpatients and inpatients. Patients on antidepressant medication were not excluded, although no significant group differences were detected. Individuals with a history of hospitalization are nearly twice as likely to engage in violent behavior compared to outpatients,9 suggesting that decision-making differences may exist between these groups. While there is no direct evidence linking antidepressants to violent behavior,76 antidepressants may influence sensitivity to negative outcomes.77 Future studies should use multifactorial models to comprehensively assess the complex relationships among pharmacologic treatment, hospitalization history, and risk-related decision-making. Third, ERPs lack high spatial resolution. Future research should integrate high-resolution neuroimaging techniques, such as fMRI, to better localize the brain regions and elucidate the neural mechanisms underlying feedback sensitivity and aggression.78 In addition, the relatively small ERP subsample (n = 40) may limit the generalizability of the findings and reduce statistical power for detecting more subtle subgroup differences. Finally, the majority of the depressed patients in the current study was female, reflecting the gender distribution of clinical populations. Women are more sensitive to losses than to wins during decision-making tasks.79 Future studies should explore the role of gender differences in the relationship between aggression and risk-related decision-making in individuals with depression.
Conclusion
Depressed patients with high aggression exhibited enhanced FRN responses to loss feedback on the IGT, along with greater FRN differences between loss and win conditions compared to those with low aggression. These neural patterns suggest heightened sensitivity to negative feedback and altered cognitive–emotional processing during decision-making. Such hypersensitivity may contribute to the persistence of depressive symptoms and may increase vulnerability to reactive aggression, particularly when emotional reactivity is dysregulated. From a clinical perspective, interventions could incorporate feedback-based cognitive-behavioral strategies and emotion regulation training to reduce sensitivity to punishment and alleviate maladaptive emotional responses. These findings may inform the design of personalized interventions and risk assessment approaches, and they highlight potential avenues for future research, such as integrating neurofeedback protocols or multimodal neuroimaging to target specific neural markers of maladaptive feedback processing in depression.
Data Sharing Statement
The datasets used during the study are available from the corresponding author on reasonable request.
Ethical Compliance
All participants provided written informed consent before participation. For participants under the age of 18, written informed consent was obtained from a parent or legal guardian. The study was approved by the Ethics Committee of Anhui Medical University (approval number: 82240127), and was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to thank all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program (grant number 2021YFC3300500 and 2021YFC3300504), Research Fund of Anhui Institute of translational medicine (grant number 2023zhyx-C76), Anhui Province Clinical Medical Research Transformation Special Project (grant number 202204295107020006 and 202204295107020065).
Disclosure
The authors declare no conflict of interest.
References
1. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
2. Laborderie S, Saint-Martin P, Prat S. 1463 – sociodemographical and psychopathological characteristics to differenciate suicide by burning from accidental and criminal burning: a 11 years retrospective study. Eur Psychiatry. 2013;28(S1):1. doi:10.1016/S0924-9338(13)76491-5
3. Paljärvi T, Tiihonen J, Lähteenvuo M, Tanskanen A, Fazel S, Taipale H. Psychotic depression and deaths due to suicide. J Affect Disord. 2023;321:28–32. doi:10.1016/j.jad.2022.10.035
4. Smith HL, Summers BJ, Dillon KH, Macatee RJ, Cougle JR. Hostile interpretation bias in depression. J Affect Disord. 2016;203:9–13. doi:10.1016/j.jad.2016.05.070
5. Gasse A, Kim WS, Gagnon J. Association between depression and hostile attribution bias in hostile and non-hostile individuals: an ERP study. J Affect Disord. 2020;276:1077–1083. doi:10.1016/j.jad.2020.06.025
6. De Bles NJ, Rius Ottenheim N, Van Hemert AM, et al. Trait anger and anger attacks in relation to depressive and anxiety disorders. J Affect Disord. 2019;259:259–265. doi:10.1016/j.jad.2019.08.023
7. Khemakhem K, Boudabous J, Cherif L, et al. Impulsivity in adolescents with major depressive disorder: a comparative tunisian study. Asian J Psychiatr. 2017;28:183–185. doi:10.1016/j.ajp.2017.06.002
8. Bjork JM, Dougherty DM, Moeller FG. A positive correlation between self-ratings of depression and laboratory-measured aggression. Psychiatry Res. 1997;69(1):33–38. doi:10.1016/s0165-1781(96)03025-9
9. Fazel S, Wolf A, Chang Z, Larsson H, Goodwin GM, Lichtenstein P. Depression and violence: a Swedish population study. Lancet Psychiatry. 2015;2(3):224–232. doi:10.1016/S2215-0366(14)00128-X
10. Pozuelo JR, Desborough L, Stein A, Cipriani A. Systematic review and meta-analysis: depressive symptoms and risky behaviors among adolescents in low- and middle-income countries. J Am Acad Child Adolesc Psychiatry. 2022;61(2):255–276. doi:10.1016/j.jaac.2021.05.005
11. Cruz AR, De Castro-Rodrigues A, Barbosa F. Executive dysfunction, violence and aggression. Aggress Violent Behav. 2020;51:101380. doi:10.1016/j.avb.2020.101380
12. Umbach R, Leonard NR, Luciana M, Ling S, Laitner C. The iowa gambling task in violent and nonviolent incarcerated male adolescents. Crim Justice Behav. 2019;46(11):1611–1629. doi:10.1177/0093854819847707
13. Alacreu-Crespo A, Guillaume S, Sénèque M, Olié E, Courtet P. Cognitive modelling to assess decision-making impairments in patients with current depression and with/without suicide history. Eur Neuropsychopharmacol. 2020;36:50–59. doi:10.1016/j.euroneuro.2020.04.006
14. Smoski MJ, Lynch TR, Rosenthal MZ, Cheavens JS, Chapman AL, Krishnan RR. Decision-making and risk aversion among depressive adults. J Behav Ther Exp Psychiatry. 2008;39(4):567–576. doi:10.1016/j.jbtep.2008.01.004
15. Deisenhammer EA, Schmid SK, Kemmler G, Moser B, Delazer M. Decision making under risk and under ambiguity in depressed suicide attempters, depressed non-attempters and healthy controls. J Affect Disord. 2018;226:261–266. doi:10.1016/j.jad.2017.10.012
16. Gorlyn M, Keilp JG, Oquendo MA, Burke AK, John Mann J. Iowa gambling task performance in currently depressed suicide attempters. Psychiatry Res. 2013;207(3):150–157. doi:10.1016/j.psychres.2013.01.030
17. Richard-Devantoy S, Olié E, Guillaume S, Courtet P. Decision-making in unipolar or bipolar suicide attempters. J Affect Disord. 2016;190:128–136. doi:10.1016/j.jad.2015.10.001
18. Genauck A, Andrejevic M, Brehm K, et al. Cue‐induced effects on decision‐making distinguish subjects with gambling disorder from healthy controls. Addict Biol. 2020;25(6):e12841. doi:10.1111/adb.12841
19. Nishinaka H, Nakane J, Nagata T, et al. Neuropsychological impairment and its association with violence risk in japanese forensic psychiatric patients: a case-control study. PLoS One. 2016;11(1):e0148354. doi:10.1371/journal.pone.0148354
20. Best M, Williams JM, Coccaro EF. Evidence for a dysfunctional prefrontal circuit in patients with an impulsive aggressive disorder. Proc Natl Acad Sci. 2002;99(12):8448–8453. doi:10.1073/pnas.112604099
21. Paret C, Jennen-Steinmetz C, Schmahl C. Disadvantageous decision-making in borderline personality disorder: partial support from a meta-analytic review. Neurosci Biobehav Rev. 2017;72:301–309. doi:10.1016/j.neubiorev.2016.11.019
22. Pederson CA, Fite PJ, Bortolato M. The role of functions of aggression in associations between behavioral inhibition and activation and mental health outcomes. J Aggress Maltreatment Trauma. 2018;27(8):811–830. doi:10.1080/10926771.2017.1370053
23. Parker KEM, Farrell N, Walker BR. The impact of reinforcement sensitivity theory on aggressive behavior. J Interpers Violence. 2022;37(5–6):NP3084–NP3106. doi:10.1177/0886260520948144
24. Crowley TJ, Dalwani MS, Mikulich-Gilbertson SK, et al. Risky decisions and their consequences: neural processing by boys with antisocial substance disorder. PLoS One. 2010;5(9):e12835. doi:10.1371/journal.pone.0012835
25. Megías-Robles A, Gómez-Leal R, Gutiérrez-Cobo MJ, Cabello R, Fernández-Berrocal P. The role of sensitivity to reward and punishment in aggression. J Interpers Violence. 2022;37(13–14):NP12014–NP12039. doi:10.1177/0886260520986275
26. Randles D, Flett GL, Nash KA, McGregor ID, Hewitt PL. Dimensions of perfectionism, behavioral inhibition, and rumination. Personal Individ Differ. 2010;49(2):83–87. doi:10.1016/j.paid.2010.03.002
27. Kasch KL, Rottenberg J, Arnow BA, Gotlib IH. Behavioral activation and inhibition systems and the severity and course of depression. J Abnorm Psychol. 2002;111(4):589–597. doi:10.1037/0021-843X.111.4.589
28. Hevey D, Thomas K, Laureano-Schelten S, Looney K, Booth R. Clinical depression and punishment sensitivity on the BART. Front Psychol. 2017;8:670. doi:10.3389/fpsyg.2017.00670
29. Rygula R, Noworyta-Sokolowska K, Drozd R, Kozub A. Using rodents to model abnormal sensitivity to feedback in depression. Neurosci Biobehav Rev. 2018;95:336–346. doi:10.1016/j.neubiorev.2018.10.008
30. Fan L, Kong X, Zhang P, et al. Hypersensitivity to negative feedback during dynamic risky-decision making in major depressive disorder: an event-related potential study. J Affect Disord. 2021;295:1421–1431. doi:10.1016/j.jad.2021.09.019
31. Liu Q, Zhong R, Ji X, et al. Decision‐making biases in suicide attempters with major depressive disorder: a computational modeling study using the balloon analog risk task (BART). Depress Anxiety. 2022;39(12):845–857. doi:10.1002/da.23291
32. Miltner WHR, Braun CH, Coles MGH. Event-related brain potentials following incorrect feedback in a time-estimation task: evidence for a “generic” neural system for error detection. J Cogn Neurosci. 1997;9(6):788–798. doi:10.1162/jocn.1997.9.6.788
33. Oliveira FTP, McDonald JJ, Goodman D. Performance monitoring in the anterior cingulate is not all error related: expectancy deviation and the representation of action-outcome associations. J Cogn Neurosci. 2007;19(12):1994–2004. doi:10.1162/jocn.2007.19.12.1994
34. Holroyd CB, Coles MGH. The neural basis of human error processing: reinforcement learning, dopamine, and the error-related negativity. Psychol Rev. 2002;109(4):679–709. doi:10.1037/0033-295X.109.4.679
35. Botvinick MM, Cohen JD, Carter CS. Conflict monitoring and anterior cingulate cortex: an update. Trends Cognit Sci. 2004;8(12):539–546. doi:10.1016/j.tics.2004.10.003
36. Gehring WJ, Willoughby AR. The medial frontal cortex and the rapid processing of monetary gains and losses. Science. 2002;295(5563):2279–2282. doi:10.1126/science.1066893
37. Bianchin M, Angrilli A. Decision preceding negativity in the iowa gambling task: an ERP study. Brain Cogn. 2011;75(3):273–280. doi:10.1016/j.bandc.2011.01.005
38. Polich J. Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol. 2007;118(10):2128–2148. doi:10.1016/j.clinph.2007.04.019
39. Sawaki R, Katayama J. Distractor P3 is associated with attentional capture by stimulus deviance. Clin Neurophysiol. 2008;119(6):1300–1309. doi:10.1016/j.clinph.2008.01.107
40. Zhong B, Niu N, Li J, Wu Y, Fan W. Social observation modulates the influence of socioeconomic status on pro-environmental behavior: an event-related potential study. Front Neurosci. 2024;18:1428659. doi:10.3389/fnins.2024.1428659
41. Kong X, Zhang P, Xiao F, et al. State-independent and -dependent behavioral and neuroelectrophysiological characteristics during dynamic decision-making in patients with current and remitted depression. J Affect Disord. 2022;309:85–94. doi:10.1016/j.jad.2022.04.120
42. Park H, Sanchez SM, Kuplicki R, et al. Attenuated interoceptive processing in individuals with major depressive disorder and high repetitive negative thinking. J Psychiatr Res. 2022;156:237–244. doi:10.1016/j.jpsychires.2022.10.020
43. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
44. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the patient health questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
45. Li J, Du Q, Gao X. Adolescent aggression and violent video games: the role of moral disengagement and parental rearing patterns. Child Youth Serv Rev. 2020;118:105370. doi:10.1016/j.childyouth.2020.105370
46. Maxwell JP, Sukhodolsky DG, Sit CHP. Preliminary validation of a Chinese version of the state-trait anger expression inventory-2. Asian J Soc Psychol. 2009;12(1):1–11. doi:10.1111/j.1467-839X.2008.01264.x
47. Li J, Han ZR, Gao MM, Sun X, Ahemaitijiang N. Psychometric properties of the Chinese version of the difficulties in emotion regulation scale (DERS): factor structure, reliability, and validity. Psychol Assess. 2018;30(5):e1–e9. doi:10.1037/pas0000582
48. Lejuez CW, Read JP, Kahler CW, et al. Evaluation of a behavioral measure of risk taking: the balloon analogue risk task (BART). J Exp Psychol Appl. 2002;8(2):75–84. doi:10.1037/1076-898X.8.2.75
49. Zhu C, Yu F, Ye R, et al. External error monitoring in subclinical obsessive-compulsive subjects: electrophysiological evidence from a gambling task. PLoS One. 2014;9(3):e90874. doi:10.1371/journal.pone.0090874
50. Guo H, Song H, Liu Y, Xu K, Shen H. Social distance modulates the process of uncertain decision-making: evidence from event-related potentials. Psychol Res Behav Manag. 2019;12:701–714. doi:10.2147/prbm.s210910
51. Li S, Zhang T, Sawyer BD, Zhang W, Hancock PA. Angry drivers take risky decisions: evidence from neurophysiological assessment. Int J Environ Res Public Health. 2019;16(10):1701. doi:10.3390/ijerph16101701
52. Cui JF, Chen YH, Wang Y, Shum DHK, Chan RCK. Neural correlates of uncertain decision making: ERP evidence from the iowa gambling task. Front Hum Neurosci. 2013;7:776. doi:10.3389/fnhum.2013.00776
53. San Martín R. Event-related potential studies of outcome processing and feedback-guided learning. Front Hum Neurosci. 2012;6:304. doi:10.3389/fnhum.2012.00304
54. Luo Q, Qu C. Comparison enhances size sensitivity: neural correlates of outcome magnitude processing. PLoS One. 2013;8(8):e71186. doi:10.1371/journal.pone.0071186
55. Joel D, Niv Y, Ruppin E. Actor–critic models of the basal ganglia: new anatomical and computational perspectives. Neural Netwk. 2002;15(4–6):535–547. doi:10.1016/S0893-6080(02)00047-3
56. Martínez-Selva JM, Muñoz MA, Sánchez-Navarro JP, Walteros C, Montoya P. Time course of the neural activity related to behavioral decision-making as revealed by event-related potentials. Front Behav Neurosci. 2019;13:191. doi:10.3389/fnbeh.2019.00191
57. Kreussel L, Hewig J, Kretschmer N, Hecht H, Coles MGH, Miltner WHR. The influence of the magnitude, probability, and valence of potential wins and losses on the amplitude of the feedback negativity. Psychophysiology. 2012;49(2):207–219. doi:10.1111/j.1469-8986.2011.01291.x
58. Davey CG, Harrison BJ, Yücel M, Allen NB. Regionally specific alterations in functional connectivity of the anterior cingulate cortex in major depressive disorder. Psychol Med. 2012;42(10):2071–2081. doi:10.1017/s0033291712000323
59. Marrus N, Belden A, Nishino T, et al. Ventromedial prefrontal cortex thinning in preschool-onset depression. J Affect Disord. 2015;180:79–86. doi:10.1016/j.jad.2015.03.033
60. Chaibi I, Bouchatta O, Bennis M, Ba-M’hamed S. The role of the anterior cingulate cortex in aggression and impulsivity. Behav Neurosci. 2023;137(3):155–169. doi:10.1037/bne0000552
61. Chester DS, Lynam DR, Milich R, DeWall CN. Physical aggressiveness and gray matter deficits in ventromedial prefrontal cortex. Cortex. 2017;97:17–22. doi:10.1016/j.cortex.2017.09.024
62. Chiu PH, Deldin PJ. Neural evidence for enhanced error detection in major depressive disorder. Am J Psychiatry. 2007;164(4):608–616. doi:10.1176/ajp.2007.164.4.608
63. Tang Y, Zhang X, Simmonite M, et al. Hyperactivity within an extensive cortical distribution associated with excessive sensitivity in error processing in unmedicated depression: a combined event-related potential and sLORETA study. Int J Psychophysiol. 2013;90(2):282–289. doi:10.1016/j.ijpsycho.2013.09.001
64. Kim D, Lam J, Kutz A, Yoon KL. Punishment sensitivity and risk taking in depressed mood. Motiv Emot. 2021;45(1):122–130. doi:10.1007/s11031-020-09860-4
65. Smits DJM, Kuppens P. The relations between anger, coping with anger, and aggression, and the BIS/BAS system. Personal Individ Differ. 2005;39(4):783–793. doi:10.1016/j.paid.2005.02.023
66. Berkowitz L. Frustration-aggression hypothesis: examination and reformulation. Psychol Bull. 1989;106(1):59–73. doi:10.1037/0033-2909.106.1.59
67. Katz BA, Yovel I. Reinforcement sensitivity predicts affective psychopathology via emotion regulation: cross-sectional, longitudinal and quasi-experimental evidence. J Affect Disord. 2022;301:117–129. doi:10.1016/j.jad.2022.01.017
68. Park C, Rosenblat JD, Lee Y, et al. The neural systems of emotion regulation and abnormalities in major depressive disorder. Behav Brain Res. 2019;367:181–188. doi:10.1016/j.bbr.2019.04.002
69. Navas-Casado ML, García-Sancho E, Salguero JM. Associations between maladaptive and adaptive emotion regulation strategies and aggressive behavior: a systematic review. Aggress Violent Behav. 2023;71:101845. doi:10.1016/j.avb.2023.101845
70. Poppa T, Bechara A. The somatic marker hypothesis: revisiting the role of the ‘body-loop’ in decision-making. Curr Opin Behav Sci. 2018;19:61–66. doi:10.1016/j.cobeha.2017.10.007
71. Luu P, Tucker DM, Derryberry D, Reed M, Poulsen C. Electrophysiological responses to errors and feedback in the process of action regulation. Psychol Sci. 2003;14(1):47–53. doi:10.1111/1467-9280.01417
72. Bagneux V, Thomassin N, Gonthier C, Roulin JL. Working memory in the processing of the iowa gambling task: an individual differences approach. PLoS One. 2013;8(11):e81498. doi:10.1371/journal.pone.0081498
73. Toplak ME, Sorge GB, Benoit A, West RF, Stanovich KE. Decision-making and cognitive abilities: a review of associations between Iowa Gambling Task performance, executive functions, and intelligence. Clin Psychol Rev. 2010;30(5):562–581. doi:10.1016/j.cpr.2010.04.002
74. Dong X, Du X, Qi B. Conceptual knowledge influences decision making differently in individuals with high or low cognitive flexibility: an ERP study. PLoS One. 2016;11(8):e0158875. doi:10.1371/journal.pone.0158875
75. Lu J, Zhao X, Wei X, He G. Risky decision-making in major depressive disorder: a three-level meta-analysis. Int J Clin Health Psychol. 2024;24(1):100417. doi:10.1016/j.ijchp.2023.100417
76. Healy D, Herxheimer A, Menkes DB. Antidepressants and violence: problems at the interface of medicine and law. PLoS Med. 2006;3(9):e372. doi:10.1371/journal.pmed.0030372
77. Dalgleish T, Yiend J, Bramham J, et al. Neuropsychological processing associated with recovery from depression after stereotactic subcaudate tractotomy. Am J Psychiatry. 2004;161(10):1913–1916. doi:10.1176/ajp.161.10.1913
78. Alacreu-Crespo A, Olié E, Le Bars E, Cyprien F, Deverdun J, Courtet P. Prefrontal activation in suicide attempters during decision making with emotional feedback. Transl Psychiatry. 2020;10(1):313. doi:10.1038/s41398-020-00995-z
79. Garrido‐Chaves R, Perez‐Alarcón M, Perez V, Hidalgo V, Pulopulos MM, Salvador A. FRN and P3 during the Iowa gambling task: the importance of gender. Psychophysiology. 2021;58(3):e13734. doi:10.1111/psyp.13734
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.