Back to Archived Journals » Adolescent Health, Medicine and Therapeutics » Volume 15
Exploring Predictors of HPV Vaccination Decisions: A Stage-Based Study on Chinese Parents of Girls
Authors Li D ![]() , Stinson J
, Stinson J ![]() , Zhang W, Wu F, Wang J, Shen B
, Zhang W, Wu F, Wang J, Shen B ![]() , Wu F, Yuan C
, Wu F, Yuan C
Received 12 October 2024
Accepted for publication 16 April 2025
Published 25 April 2025 Volume 2024:15 Pages 119—131
DOI https://doi.org/10.2147/AHMT.S500527
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Danyu Li,1,2 Jennifer Stinson,3,4 Wen Zhang,2 Fulei Wu,2 Jingting Wang,5 Biyu Shen,6 Fan Wu,1,* Changrong Yuan2,*
1Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, Shanghai, People’s Republic of China; 2School of Nursing, Fudan University, Shanghai, People’s Republic of China; 3Child Health Evaluation Sciences, Research Institute, The Hospital for Sick Children, Toronto, Ontario, Canada; 4Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, Toronto, Ontario, Canada; 5School of Nursing, Naval Medical University, Shanghai, People’s Republic of China; 6Shanghai Children’s Medical Center Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fan Wu, Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, 130 Dong’an Road, Shanghai, 200032, People’s Republic of China, Email [email protected] Changrong Yuan, School of Nursing, Fudan University, 305 Fenglin Road, Shanghai, 200032, People’s Republic of China, Email [email protected]
Purpose: To assess the predictors of Chinese parents of girls’ decision stage about the Human Papillomavirus (HPV) vaccination.
Patients and Methods: Two hundred and seventy-three parents of girls aged 9– 17 with no HPV vaccination history were recruited to complete an online survey between September–December 2023. We assessed factors thought to influence decisions about HPV vaccination, including sociodemographics, HPV general knowledge, HPV vaccination knowledge, attitudes, and decisional conflict. Parents were asked to choose the decision stages among Stage 1 (have not thought), Stage 2 (considering), and Stage 3 (decided). Predictors of the decision stage were assessed with univariate and multivariate multinomial logistic regression.
Results: The parents of the three decision stages accounted for 48.4%, 29.7%, and 22.0%, respectively. Parents of older girls were more likely to be in the “considering” stage (OR = 1.29) than the “haven’t thought” stage. A higher sense of being uninformed was associated with lower odds of being in the “considering” stage (OR = 0.97). Additionally, greater feelings of uncertainty were linked to lower odds of being in the “decided” stage (OR = 0.95) than the “haven’t thought” stage.
Conclusion: This study highlights the importance of understanding the various stages of decision-making in HPV vaccination among Chinese parents. Parents’ subjective feelings of being informed and certainty appear to be significant factors in advancing through the decision-making stages. Future research should develop and explore the impact of specific knowledge and valued based tools and decision aids.
Keywords: decision stage, decisional conflict, human papillomavirus, China, papillomavirus vaccination
Introduction
Human Papillomavirus (HPV) can cause a wide range of health issues, with low-risk strains causing benign warts while high-risk types, notably HPV 16 and 18, elevate the risk of cervical, anal, and other cancers.1 According to the World Health Organization (WHO), HPV can cause cancer in approximately 625,600 women and 68,400 men each year globally, which is 5% of all cancers.2 HPV exerts a huge burden on financial and healthcare burden with billions of lifetime direct medical costs.3,4
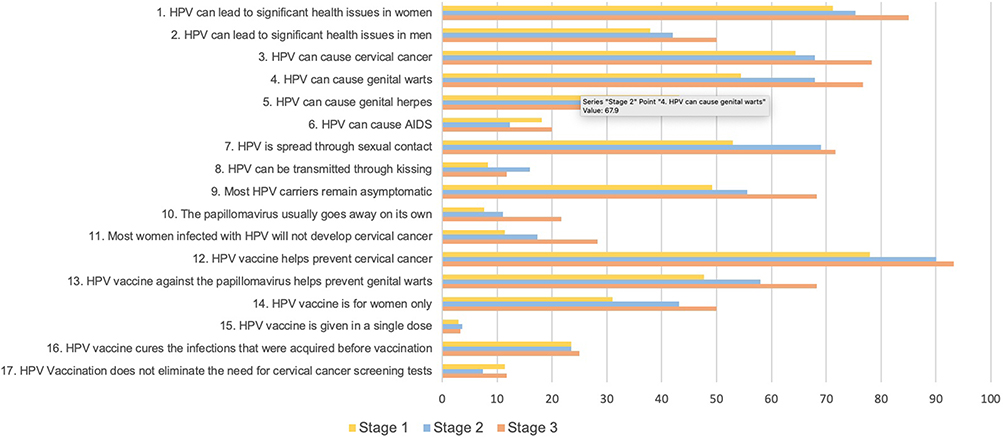 |
Figure 1 The correct (%) of HPV knowledge by item among parents of girls in different decision stages of HPV vaccination. |
In China, the prevalence of HPV among women is estimated at 18.4%, with the rate of high-risk HPV infections exceeding 15%.5 Cervical cancer continues to be a major public health issue, with approximately 106,000 new cases and 48,000 deaths each year.6 These statistics highlight the pressing need for effective preventive measures.
While safe sexual practices and a healthy lifestyle are crucial for preventing HPV, HPV vaccines offer broader protection when administered at an early age. HPV vaccines can prevent persistent infections with high-risk HPV strains and significantly reduce the incidence of cervical cancer and precancerous lesions.7 Therefore, countries worldwide have been promoting HPV vaccination since 2006, with the World Health Organization recommending it starting in 2009.8 Countries around the world have different target populations (eg, vaccination only for girls or for both boys and girls) and recommended age groups, as well as varying delivery strategies.9 As for China, HPV vaccines were introduced in 2016, and currently, women aged 9 to 45 are eligible for vaccination.10 More importantly, HPV vaccines are not included in the national immunization program and must be self-funded, with the three-dose series costing over $400.11,12
Unfortunately, global HPV vaccination coverage was only 12.2% in 2018, and in China, the rate was even lower, with 10.15% of the first-dose cumulative coverage in 2022.13,14 There is a significant body of research identifying factors that contribute to parents’ refusal or hesitancy to agree to HPV vaccination, including inadequate knowledge, negative attitudes toward the vaccine, and the absence of publicly funded vaccination programs in certain countries.15,16 Most studies to date have approached this issue as a binary outcome—vaccinated or not vaccinated.17 While some research has explored the stages of HPV vaccine decision-making and the predictors of these stages among Canadian parents, no study has yet compared the decision-making processes of parents of girls regarding HPV vaccination in China.18,19 In East Asian cultures, the patriarchal family structure often means that parents play a crucial role in making decisions for their children, with children relying heavily on their parents’ advice.20,21 Moreover, previous studies have confirmed that parents tend to prioritize different factors when making decisions for themselves compared to their children.22 Therefore, examining parents’ decision-making regarding their children’s vaccination is especially important in this cultural context.
Materials and Methods
Study Design and Population
This was a cross-sectional study conducted between September to December 2023. All mainland China jurisdictions at this time provided self-paid HPV vaccines.
This study targeted parents and/or guardians (hereafter referred to as parents) of girls aged 9–17 years. The inclusion criteria for parents were having a daughter aged 9 to 17 years who had not received the HPV vaccine. The exclusion criteria included parents whose daughters were ineligible for HPV vaccination, specifically: 1) girls who had experienced a severe allergic reaction to any component of the HPV vaccine, such as yeast, amorphous aluminum hydroxyphosphate sulfate, or Polysorbate 80; 2) girls who were in a critical or terminal condition (with a life expectancy of 6 weeks or less). Parents with multiple daughters who met the inclusion criteria were asked to complete the questionnaire based on the daughter they selected, to ensure randomization.
This study was implemented by Wenjuanxing (a Chinese online survey service provider), and the first page of the online questionnaire showed the aim of the study and outlined that participants could quit the survey anytime they wanted. If the participants clicked the “yes and continue”, the questionnaire would then be presented to ensure informed consent.
Study Instruments
We combined the questionnaire containing 52 items for parents covering 5 parts: sociodemographics, decision stage, knowledge, attitudes toward HPV vaccine, and decisional conflict scale.
Sociodemographics (14 Variables)
There were two parts for the sociodemographics questions with one part reporting parents’ information (age, number of children, ethnicity, religion, educational background, area of residence, marital status, healthcare-related major learning experience, healthcare-related job doing experience, monthly family income) and another part for their daughter’s information (age, ethnicity, religion, overall health condition).
Decision Stage (1 Item)
The primary outcome variable in our study was parents’ self-reported HPV vaccine decision stage. We made the item and its three-stage response level according to the Ottawa Decision Support Framework (ODSF) User Manual-Stage of Decision Making.23 Parents were asked: “How far along are you with your daughter’s HPV vaccine decision?” Three response options were provided: Stage 1 (not yet considered: I have not begun to think about the choices); Stage 2 (considering: I am considering the options now); Stage 3 (decided: I have already made a decision).
Knowledge (17 Items)
In the part of knowledge, we included two aspects of measures concerning the study of Yulia Gendler,24 containing the first aspect of 11 items of HPV general knowledge (eg, “The papillomavirus is transmitted through sexual contact”) and the second aspect of 6 items of HPV vaccine knowledge (eg, “The vaccine against the papillomavirus is intended for women only”). For each item, the respondents answered “Yes”, “No” or “Unclear”, for which a score was calculated based on correct answers (True-1, False-0, Unclear-0), and thus higher scores indicate greater knowledge on both aspects.
Attitudes Toward HPV Vaccine (4 Items)
For this part, we included four main important factors of HPV vaccination decisions in people’s value system. The two main benefits are: HPV vaccination protects against all types of HPV-related cancers, and HPV vaccination prevents genital warts caused by HPV. The two main barriers are: the various side effects that can be caused by HPV vaccination, and the cost of the vaccine, with responses ranging from 0 (not important at all) to 10 (extremely important).
Decisional Conflict Scale (16 Items)
Decisional conflict scale (DCS) was developed by O’Connor in 1995 and revised in 2005,25 measuring a person’s perceptions of their uncertainty in health care options, the modifiable factors contributing to uncertainty, and the quality of the decision made.26 DCS consists of 16 items with a Likert 5-point scoring method across 5 dimensions, including feeling uncertain (3 items), feeling uninformed (3 items), feeling unclear about values (3 items), and feeling unsupported (3 items), as well as ineffective decision making (4 items). The items were rated using a 5-point Likert scale, with scores ranging from 0 (Strongly Agree) to 4 (Strongly Disagree). The total score of each dimension was obtained by multiplying the mean of the dimension by 25; the total scale score is equal to the sum of the item scores divided by 16 and multiplied by 25 and the score ranges from 0 to 100. A higher score of DCS means a greater decisional conflict or uncertainty. The validation study of the Chinese version of the DCS shows its good criteria validity and satisfactory internal consistency.27 To be specific, the Cronbach’s α for DCS total score was 0.963 and that for each subscale ranged from 0.784 to 0.93.27
Ethics
This study was approved by the IRB of Shanghai Children’s Medical Center Affiliated to Shanghai Jiao Tong University School of Medicine (No. SCMCIRB-K2024271-1) and was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Data Analysis
This study reports parents’ HPV vaccination decisions across three stages, presented as percentages. To assess significant differences in decision stages based on sociodemographic factors, knowledge, attitudes, and decisional conflict, chi-square tests, Fisher’s exact tests, and one-way ANOVA were applied, depending on the suitability of the data. When appropriate, post hoc analyses using Bonferroni or Tamhane’s T2 tests were performed.
Multinomial logistic regression analyses were used to calculate the odds ratios (OR) of being in Stage 2 (considering) and Stage 3 (decided) compared to Stage 1 (have not thought). The decision stage was the dependent variable. First, we conducted univariate multinomial logistic regression analyses and estimated the associations for each independent variable individually. Subsequently, we performed multivariate multinomial logistic regression analyses by including 11 independent variables in a single model. To select variables that would ensure the most parsimonious multivariate model, variables were included based on significant modifying factors in univariate analysis. OR and 95% confidence intervals (CI) were calculated. To assess the multicollinearity of the multivariate multinomial logistic regression models, the Variation Inflation Factor (VIF) was calculated for all predictors. A VIF < 5 was obtained for all predictors, which indicates that multicollinearity is not an issue. Model fit diagnostics were reported based on the following criteria: (a) Cox-Snell R2, (b) Cragg-Uhler R2, and (c) McFadden R2. Statistical analyses were performed using SPSS version 26.
Results
Sociodemographics Characteristics
A total of 273 parents of girls participated in the survey. The sociodemographic characteristics of parents and girls are reported in Table 1. Most parents reported being at Stage 1 (48.4%), 29.7% were at Stage 2, and 22.0% were at Stage 3. The stage of HPV vaccination decision-making significantly differed by the age of the girls (p = 0.001). According to the post hoc analysis (Bonferroni), parents in Stage 2 (considering) regarding their daughters’ HPV vaccination are significantly older than girls of parents in Stage 1 (have not thought). There were no other differences in sociodemographic variables across the decision stages.
 |
Table 1 The Sociodemographic Characteristics of Participants by HPV Vaccination Decision Stage (N=273) |
 |
Table 2 The Knowledge of Parents by HPV Vaccination Decision Stage (N=273) |
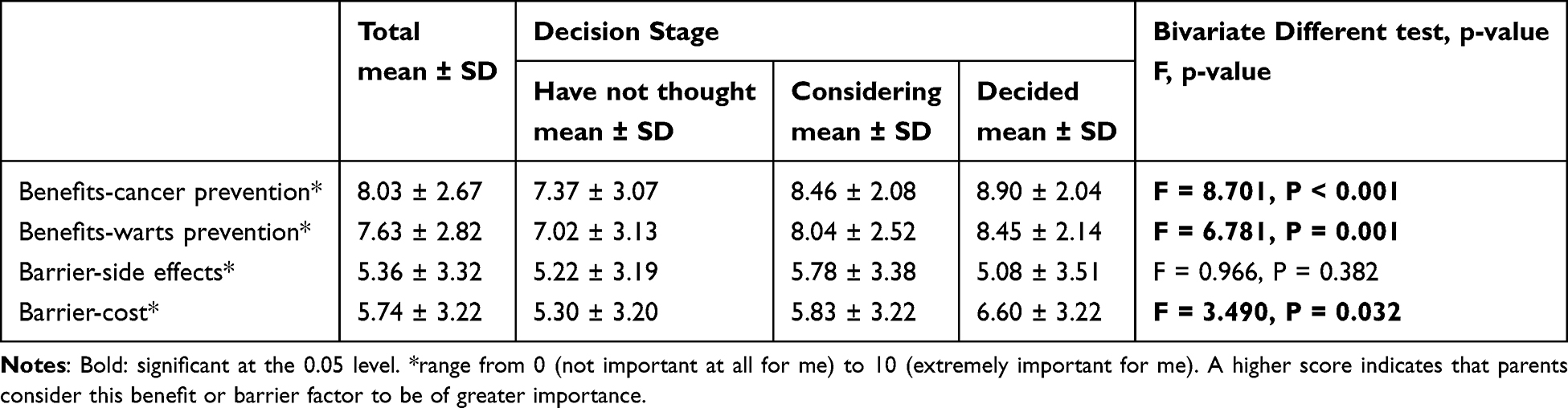 |
Table 3 The Attitudes of Parents by HPV Vaccination Decision Stage (N=273) |
 |
Table 4 The Decisional Conflict of Parents by HPV Vaccination Decision Stage (N=273) |
Knowledge of HPV and HPV Vaccination
Figure 1 shows the HPV general knowledge and HPV vaccination knowledge by item among parents at the three different decision stages. Among the 17 items, 7 items (2nd, 6th, 8th, 10th, 15th, 16th, and 17th) had an overall accuracy rate lower than 50%. The three items with the lowest accuracy rates were item 8th (regarding transmission routes of HPV), item 15th (regarding the dosage regimen of the HPV vaccine), and item 17th (regarding the need for cervical cancer screening after vaccination).
Table 2 presents the mean scores for parents’ knowledge of HPV and the HPV vaccination. Statistically significant differences were found across the different decision stages in both HPV general knowledge and HPV vaccine knowledge. Post hoc analysis (Bonferroni) revealed that parents in Stage 3 (decided) scored significantly higher in both HPV general knowledge and HPV vaccine knowledge compared to those in Stage 1 (have not thought).
Attitudes to HPV Vaccination
Table 3 presents the HPV vaccine attitudes of parents across the three decision stages. Overall, respondents emphasized that the benefits of vaccination outweighed the barriers, with two benefit items—cancer prevention and warts prevention—scoring higher than 7. Statistically significant differences were observed among parents at different decision stages regarding the benefits of cancer prevention, the benefits of warts prevention, and the barrier of cost. Post hoc analyses revealed that, for cancer prevention and cost barriers, parents in Stage 3 (decided) scored significantly higher than those in Stage 1 (have not thought). For warts prevention, both Stage 3 (decided) and Stage 2 (considering) parents scored significantly higher than those in Stage 1 (have not thought).
Decisional Conflict Toward HPV Vaccination
Table 4 presents the HPV vaccine attitudes of parents at different decision stages. Statistically significant differences were observed among parents in various decision stages regarding the total decisional conflict score and scores across five subscales. Post hoc tests indicated that parents in Stage 1 (have not thought) reported higher total and subscale scores compared to parents in Stage 2 (considering) and Stage 3 (decided).
Factors Associated with the Decision Stage
In the univariate multinomial logistic regression analyses, several predictors were significantly associated with being in at least one decision stage (compared to being in Stage 1) (Table 5). Parents of older age were significantly more likely to be in Stage 2 (considering) compared to Stage 1 (have not thought), with an OR of 1.24 [95% CI: 1.10, 1.39]. Parents with higher HPV general knowledge and HPV vaccination knowledge were significantly more likely to be in Stage 3 (decided) compared to Stage 1 (have not thought), with OR of 1.21 [95% CI: 1.08, 1.36] and 1.44 [95% CI: 1.12, 1.85], respectively. Parents who placed higher importance on the benefits of cancer prevention were significantly more likely to be in Stage 2 (considering) and Stage 3 (decided) compared to Stage 1 (have not thought), with OR of 1.17 [95% CI: 1.04, 1.30] and 1.29 [95% CI: 1.11, 1.50], respectively. Parents who placed higher importance on the benefits of warts prevention were significantly more likely to be in Stage 2 (considering) and Stage 3 (decided) compared to Stage 1 (have not thought), with OR of 1.14 [95% CI: 1.03, 1.26] and 1.22 [95% CI: 1.08, 1.39], respectively. Parents who placed higher importance on the barrier of cost were significantly more likely to be in Stage 3 (decided) compared to Stage 1 (have not thought), with an OR of 1.14 [95% CI: 1.03, 1.26]. Parents who felt more uninformed and unclear about their values were significantly less likely to be in Stage 2 (considering) compared to Stage 1 (have not thought), with an odds ratio (OR) of 0.98. Additionally, parents who felt more uninformed, unclear about their values, unsupported, uncertain, and ineffective in decision-making were significantly less likely to be in Stage 3 (decided) compared to Stage 1 (have not thought), with odds ratios (OR) of 0.95, 0.95, 0.96, 0.94, and 0.95, respectively. Further analysis by other predictors indicated that this effect was not significant in the model examining parents of girls.
 |
Table 5 Univariate Multinomial Logistic Regression Analysis Between Decision Stages and the Predictors (N=273) |
Results from multivariate multinomial logistic regression analyses are presented in Table 6. The following predictors were found to be significant: the age of the girls, feeling informed, and feelings of uncertainty about parents’ HPV vaccination decision stages. Parents of older girls were significantly more likely to be in the “considering” stage (OR = 1.29) compared to those in the “haven’t thought” stage. A higher sense of being uninformed was significantly associated with lower odds of being in the “considering” stage (OR = 0.97) compared to the “haven’t thought” stage. Additionally, higher feelings of uncertainty were significantly associated with lower odds of being in the “decided” stage (OR = 0.95) compared to the “haven’t thought” stage.
 |
Table 6 Multivariate Multinomial Logistic Regression Analysis Between Decision Stages and the Predictors (N=273) |
Discussion
Cervical cancer is the third most common cancer in women, primarily caused by persistent HPV infections, with high-risk strains such as HPV 16 and 18 being the main culprits.28 Early detection through screening methods like cervical cytology, HPV testing, and colposcopy plays a critical role in managing precancerous lesions and early-stage cancers.29 In recent years, minimally invasive surgery has become a common treatment for low-risk cervical tumors.30,31 HPV vaccination, particularly during adolescence, has proven effective in reducing HPV infection rates and the incidence of cervical cancer.29 Furthermore, recent studies emphasize the importance of HPV vaccination even after hysterectomy for high-grade cervical lesions or early-stage cancer, as it can still prevent the development of lower genital tract dysplasia.32
HPV vaccination has been globally recognized for its role in preventing cervical cancer, with China introducing the vaccine in 2016.10 Given China’s unique family-based decision-making model, where parents play a central role in children’s health decisions, understanding parental decision-making around vaccines is crucial.20,21 While most existing studies on parents’ HPV decisions focus on vaccination status or intention levels, they do not differentiate between the stages of decision-making or identify predictors for each stage.33,34 This study fills that gap by examining the three distinct stages of HPV vaccine decision-making among Chinese parents of girls aged 9–17, making it a valuable contribution to understanding the decision-making process in this context.
Our study found that only 22% of parents had reached the final decision-making stage (Stage 3 - decided), which is lower than the 30.1% reported in a similar 2018 study in Canada.19 This disparity may be attributed to differences in the cost and availability of the HPV vaccine. Specifically, all Canadian provinces and territories offer free HPV vaccines through school-based immunization programs, whereas China has not yet implemented a national free vaccination program.35,36 Additionally, the limited availability of HPV vaccines in China, where they are frequently out of stock despite high demand, contrasts with the widespread accessibility in Canada.12,37,38
We found a significant association between girls’ age and the decision-making stage, with parents of older girls more likely to be in the “considering” stage. The association between a child’s age and vaccine decision-making is consistent with existing literature, where parents often delay making vaccination decisions until they perceive their children to be at greater risk due to potential exposure to sexual activity.39 Notably, research indicates that sexual activity among adolescents can begin earlier than parents might expect, with over 10% of girls aged 15–19 engaging in sexual activity.40 This underscores the importance of vaccinating girls before the onset of sexual activity, highlighting the need for timely education and intervention. In light of these findings, it is crucial to develop targeted interventions for parents of middle and high school students in China. These interventions could include informational materials, health education during parent meetings, and novel approaches such as creating films or short videos to support vaccine-hesitant parents.41,42
As for knowledge level, though the ANOVA and Post Hoc Tests show that parents at Stage 3 (decided) have a significantly higher score of both HPV general knowledge and HPV vaccine knowledge than those at Stage 1 (have not thought), the multivariate analysis shows the insignificant relationship between knowledge and stage, which is different from previous studies.19,43 Furthermore, our study included the feeling of being informed rated by parents themselves, and it shows that having more sense of being “uninformed” was significantly associated with lower odds of being under thinking than have not thought. This suggests an avenue for interventions: by enhancing parents’ subjective “feeling of being informed”, we may help facilitate their progression to decision-making. Previous research has firmly established the importance of informed choice from an ethical perspective and its beneficial impact on patient health outcomes.44 In this study, the assessment of the participants’ “feeling of being informed” was based solely on one dimension of the DCS self-assessment tool. However, previous research has confirmed that relying exclusively on individuals’ self-reported perceptions is insufficient, as this method often overestimates their actual level of informedness. Therefore, future research and practice must utilize more specific, knowledge-based assessment tools to ensure patients make fully informed decisions.45 Regarding interventions, knowledge and attitudes are the two fundamental components of informed decision-making.44 Therefore, decision aids, which serve as effective tools for delivering knowledge and exploring values, play a crucial role in facilitating decision-making.46 Currently, there are existing decision aids for HPV vaccination,24,47–49 but none have been specifically tailored to the decision-making needs of individuals in mainland China, nor have they been built based on the vaccination policies in the region. A decision aid designed specifically for mainland China’s HPV vaccination policies could better address the unique context and needs of local decision-makers.
Different from previous research with a similar topic,18,19 this study also included self-rate certainty feeling as a predictor and found that a higher feeling of uncertainty was significantly associated with lower odds of being decided as compared to have not thought. This result informs us a key intervention strategy to improve the HPV vaccine decision rate is focused on solving parents’ uncertainty. According to ODSF, several practices like clinical counselling, decision tools, and decision coaching are efficient ways can relieve the uncertainty of decision-makers and thus improve decision quality.50–52
The current study has several limitations. First, the convenience sample was collected online, and the parents included in this study were largely well-educated. This introduces potential regional and cultural variability, which may limit the generalizability of the results to the broader Chinese population. We recommend that future research reduce the potential impact of bias by employing multi-channel recruitment or offline surveys. Second, as a cross-sectional survey, we cannot make causal claims regarding the associations described in our findings. Third, some of the measures included in this study are not fully validated and may bring about limitations in the interpretation of results. Besides, we only assessed the decision-making stage and did not ask those in the “decided” stage whether they had chosen to vaccinate or not, which limits the development of targeted interventions that address specific decision outcomes and motivations. Finally, this study was not driven by the theory of the decision-making process, like the Precaution Adoption Process Model (PAPM), bringing potential bias in defining the decision stage. Despite these limitations, the current study provides further description of demographic differences that should be considered when implementing strategies to address HPV vaccination among the age-expanded adult population for which shared clinical decision-making is currently recommended.
Conclusion
HPV vaccine remains unfunded in China and the vaccination rate is low. Using a stage-based model of decision-making, this study found that less than a quarter of parents were in the final stage. Parents having daughters of younger age, feeling more uninformed, and having more uncertainty were more likely to be in the stage of not thinking about getting their daughters vaccinated. This study highlights that the focus of policy development and intervention design (eg, decision aids) should be on enhancing informed decision-making and reducing uncertainty among parents.
Abbreviations
HPV, Human Papillomavirus; ODSF, Ottawa Decision Support Framework; DCS, Decisional conflict scale; OR, Odds Ratios; CI, Confidence Intervals; VIF, Variation Inflation Factor; PAPM, Precaution Adoption Process Model.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burd EM. Human papillomavirus and cervical cancer. Clin Microbiol Rev. 2003;16(1):1–17. doi:10.1128/cmr.16.1.1-17.2003
2. World Health Organization. Human papillomavirus and cancer. Available from: https://www.who.int/news-room/fact-sheets/detail/human-papilloma-virus-and-cancer.
3. Chesson HW, Laprise JF, Brisson M, Martin D, Ekwueme DU, Markowitz LE. The estimated lifetime medical cost of diseases attributable to human papillomavirus infections acquired in 2018. Sex Transm Dis. 2021;48(4):278–284. doi:10.1097/olq.0000000000001379
4. Serrano B, Brotons M, Bosch FX, Bruni L. Epidemiology and burden of HPV-related disease. Best Pract Res Clin Obstet Gynaecol. 2018;47:14–26. doi:10.1016/j.bpobgyn.2017.08.006
5. Yao X, Li Q, Chen Y, et al. Epidemiology of human papillomavirus infection in women from Xiamen, C hina, 2013 to 2023. Front Public Health. 2024;12. doi:10.3389/fpubh.2024.1332696
6. Kamaraju S, Drope J, Sankaranarayanan R, Shastri S. Cancer prevention in low-resource countries: an overview of the opportunity. Am Soc Clin Oncol Educ Book. 2020;40:1–12. doi:10.1200/edbk_280625
7. Yin X, Zhang M, Wang F, et al. A national cross-sectional study on the influencing factors of low HPV vaccination coverage in mainland China. Front Public Health. 2022;10:1064802. doi:10.3389/fpubh.2022.1064802
8. Bruni L, Saura-Lázaro A, Montoliu A, et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prevent Med. 2021;144:106399. doi:10.1016/j.ypmed.2020.106399
9. Tsu VD, LaMontagne DS, Atuhebwe P, Bloem PN, Ndiaye C. National implementation of HPV vaccination programs in low-resource countries: lessons, challenges, and future prospects. Prev Med. 2021;144:106335. doi:10.1016/j.ypmed.2020.106335
10. An J, Liu Y, Ma Y, et al. Real-world data of China: analysis of HPV vaccine coverage and post-vaccination adverse reaction monitoring in Western Chinese provinces from 2018 to 2021. Hum Vaccin Immunother. 2024;20(1):2315653. doi:10.1080/21645515.2024.2315653
11. Zhou L, Wang J, Cheng P, Li Y, Liu G, Zhang X. HPV vaccine hesitancy among medical students in China: a multicenter survey. Front Public Health. 2022;10:774767. doi:10.3389/fpubh.2022.774767
12. Colombara DV, Wang SM. The impact of HPV vaccination delays in China: lessons from HBV control programs. Vaccine. 2013;31(38):4057–4059. doi:10.1016/j.vaccine.2013.06.031
13. Spayne J, Hesketh T. Estimate of global human papillomavirus vaccination coverage: analysis of country-level indicators. BMJ Open. 2021;11(9):e052016. doi:10.1136/bmjopen-2021-052016
14. Chen J, Zhang Z, Pan W, et al. Estimated human papillomavirus vaccine coverage among females 9–45 years of age—China, 2017–2022. China CDC Weekly. 2024;6(19):413.
15. Beavis AL, Meek K, Moran MB, Fleszar L, Adler S, Rositch AF. Exploring HPV vaccine hesitant parents’ perspectives on decision-making and motivators for vaccination. Vaccine X. 2022;12:100231. doi:10.1016/j.jvacx.2022.100231
16. Štrbac M, Vuković V, Pustahija T, et al. Motives and attitudes of parents toward HPV vaccination: results from the initial period of HPV vaccine rollout in Serbia. PLoS One. 2023;18(7):e0287295. doi:10.1371/journal.pone.0287295
17. Lin Y, Su Z, Chen F, et al. Chinese mothers’ intention to vaccinate daughters against human papill omavirus (HPV), and their vaccine preferences: a study in Fujian Provi nce. Human Vaccines Immunotherapeut. 2021;17(1):304–315. doi:10.1080/21645515.2020.1756152
18. Perez S, Tatar O, Gilca V, et al. Untangling the psychosocial predictors of HPV vaccination decision-making among parents of boys. Vaccine. 2017;35(36):4713–4721. doi:10.1016/j.vaccine.2017.07.043
19. Shapiro GK, Tatar O, Amsel R, et al. Using an integrated conceptual framework to investigate parents’ HPV vaccine decision for their daughters and sons. Prev Med. 2018;116:203–210. doi:10.1016/j.ypmed.2018.09.017
20. Chen A-C-C. Developing and pilot testing a digital storytelling intervention to promote HPV vaccination among Vietnamese American adolescents. GSTF J Nurs Health Care. 2020;4(1):1.
21. Cha C, Kim E. Assessing the role of culture in Korean goose mothers’ lives. J Transcultural Nurs. 2013;24(1):86–93.
22. Highet M, Jessiman-Perreault G, Hilton E, Law G, Allen-Scott L. Understanding the decision to immunize: insights into the information needs and priorities of people who have utilized an online human papillomavirus (HPV) vaccine decision aid tool. Canadian J Public Health. 2021;112(2):191–198. doi:10.17269/s41997-020-00425-z
23. O’Connor AM. Use Manual-Stage of Decision Making. 2003. Available from: https://decisionaid.ohri.ca/docs/develop/User_Manuals/UM_Stage_Decision_Making.pdf.
24. Gendler Y. Development and appraisal of a web-based decision aid for HPV vaccination for young adults and parents of children in Israel-a Quasi-experimental study. Vaccines. 2023;11(6):1038. doi:10.3390/vaccines11061038
25. O’Connor AM. Validation of a decisional conflict scale. Med Dec Making. 1995;15(1):25–30.
26. Garvelink MM, Boland L, Klein K, et al. Decisional conflict scale use over 20 years: the anniversary review. Med Dec Making. 2019;39(4):301–314.
27. Lu C, Mu W, Y-h J, et al. Cross-cultural adaptation and psychometric assessment of the statement format decisional conflict scale for Mandarin version. BMC Health Serv Res. 2019;19(1):873. doi:10.1186/s12913-019-4717-6
28. Jaisamrarn U, Castellsagué X, Garland SM, et al. Natural history of progression of HPV infection to cervical lesion or clearance: analysis of the control arm of the large, randomised PATRICIA study. PLoS One. 2013;8(11):e79260. doi:10.1371/journal.pone.0079260
29. T GD, Cuccu I, Etrusco A, et al. State of the art on HPV-related cervical lesions. Italian J Gynæcol Obstetrics. 2024;36(02):135–137.
30. Di Donato V, Bogani G, Casarin J, et al. Ten-year outcomes following laparoscopic and open abdominal radical hysterectomy for “low-risk” early-stage cervical cancer: a propensity-score based analysis. Gynecol Oncol. 2023;174:49–54. doi:10.1016/j.ygyno.2023.04.030
31. Pecorino B, D’Agate MG, Scibilia G, et al. Evaluation of surgical outcomes of abdominal radical hysterectomy and total laparoscopic radical hysterectomy for cervical cancer: a retrospective analysis of data collected before the LACC trial. Int J Environ Res Public Health. 2022;19(20). doi:10.3390/ijerph192013176
32. Bogani G, Sopracordevole F, Ciavattini A, et al. HPV-related lesions after hysterectomy for high-grade cervical intraepithelial neoplasia and early-stage cervical cancer: a focus on the potential role of vaccination. Tumori. 2024;110(2):139–145. doi:10.1177/03008916231208344
33. Wang -LD-L, Lam WWT, Wu J, Fielding R. Psychosocial determinants of Chinese parental HPV vaccination intention for adolescent girls: preventing cervical cancer. Psycho-Oncol. 2015;24(10):1233–1240. doi:10.1002/pon.3859
34. Wang Z, Wang J, Fang Y, et al. Parental acceptability of HPV vaccination for boys and girls aged 9-13 years in China - A population-based study. Vaccine. 2018;36(19):2657–2665. doi:10.1016/j.vaccine.2018.03.057
35. Awoenam Adedzi K, Dubé E. School-Based Immunization Programs: an Effective Strategy for Achieving High Vaccination Rates? Available from: https://canvax.ca/sites/default/files/2021-03/CPHA_School-BasedImmunizationPrograms_2020_EN.pdf.
36. Nation plans to launch free HPV vaccinations. National Health Commission of the People’s Republic of China. Available from: http://en.nhc.gov.cn/2022-01/14/c_85612.htm.
37. Wang H, Jiang Y, Wang Q, Lai Y, Holloway A. The status and challenges of HPV vaccine programme in China: an explor ation of the related policy obstacles. BMJ Global Health. 2023;8(8):e012554. doi:10.1136/bmjgh-2023-012554
38. Khan A, Abonyi S, Neudorf C. Barriers and facilitators in uptake of human papillomavirus vaccine across English Canada: a review. Hum Vaccin Immunother. 2023;19(1):2176640. doi:10.1080/21645515.2023.2176640
39. Zhu P, Perez S, Griffin-Mathieu G, Tatar O, Rosberger Z. What influences parents to vaccinate (or not) their sons with the Human Papillomavirus (HPV) vaccine: an examination of HPV vaccine decision-making changes over time. J Psychosoc Oncol Res Pract. 2022;4(1):e068.
40. Zhao FH, Tiggelaar SM, Hu SY, et al. A multi-center survey of age of sexual debut and sexual behavior in Chinese women: suggestions for optimal age of human papillomavirus vaccination in China. Cancer Epidemiol. 2012;36(4):384–390. doi:10.1016/j.canep.2012.01.009
41. Pullyblank K, Brunner W, Strogatz D, Manganello J, Massey P. A participatory method to develop human papillomavirus (HPV) vaccine short video content for rural New York parents. Prev Med Rep. 2024;48:102911. doi:10.1016/j.pmedr.2024.102911
42. Fisher H, Denford S, Chantler T, et al. Developing films to support vaccine-hesitant, ethnically diverse parents’ decision-making about the human papillomavirus (HPV) vaccine: a codesign study. BMJ Open. 2024;14(9):e079539. doi:10.1136/bmjopen-2023-079539
43. Nickel B, Dodd RH, Turner RM, et al. Factors associated with the human papillomavirus (HPV) vaccination acr Oss three countries following vaccination introduction. Prevent Med Rep. 2017;8:169–176. doi:10.1016/j.pmedr.2017.10.005
44. Marteau TM, Dormandy E, Michie S. A measure of informed choice. Health Expect. 2001;4(2):99–108. doi:10.1046/j.1369-6513.2001.00140.x
45. Sepucha KR, Fagerlin A, Couper MP, Levin CA, Singer E, Zikmund-Fisher BJ. How does feeling informed relate to being informed? The Decisions survey. Med Dec Making. 2010;30(5_suppl):77–84. doi:10.1177/0272989X10379647
46. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Systematic Rev. 2017;(4). doi:10.1002/14651858.CD001431.pub5
47. Wang -LD-L, Lam WWT, Fielding R. Development and pre/post testing of a decision aid supporting Chinese parental and young women’s HPV vaccination decision-making. Women Health. 2020;60(3):330–340. doi:10.1080/03630242.2019.1626791
48. Healthwise. (2022) HPV: should My Child Get the Vaccine? Available from: https://www.healthwise.net/ohridecisionaid/Content/StdDocument.aspx?DOCHWID=uz2098.
49. Healthwise. (2022) HPV: should I Get the Vaccine? Available from: https://www.healthwise.net/ohridecisionaid/Content/StdDocument.aspx?DOCHWID=abo9722.
50. Hoefel L, Lewis KB, O’Connor A, Stacey D. 20th anniversary update of the Ottawa decision support framework: part 2 Subanalysis of a systematic review of patient decision aids. Med Decis Making. 2020;40(4):522–539. doi:10.1177/0272989x20924645
51. Hoefel L, O’Connor AM, Lewis KB, et al. 20th anniversary update of the Ottawa decision support framework part 1: A systematic review of the decisional needs of people making health or social decisions. Med Decis Making. 2020;40(5):555–581. doi:10.1177/0272989x20936209
52. Stacey D, Légaré F, Boland L, et al. 20th anniversary Ottawa decision support framework: Part 3 overview of systematic reviews and updated framework. Med Decis Making. 2020;40(3):379–398. doi:10.1177/0272989x20911870
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.