Back to Journals » Patient Preference and Adherence » Volume 14
Exploring Patient’s Perspectives and Experiences After Start with Inhalation Maintenance Therapy: A Qualitative Theory-Based Study
Authors Kuipers E ![]() , Wensing M
, Wensing M ![]() , De Smet PAGM, Teichert M
, De Smet PAGM, Teichert M ![]()
Received 9 October 2019
Accepted for publication 3 January 2020
Published 29 January 2020 Volume 2020:14 Pages 203—212
DOI https://doi.org/10.2147/PPA.S234094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Esther Kuipers, 1, 2 Michel Wensing, 1, 3 Peter AGM De Smet, 1, 4 Martina Teichert 5
1Radboud University Medical Centre, Radboud Institute for Health Sciences, Department of IQ Healthcare, Nijmegen 6500 HB, The Netherlands; 2BENU Apotheek Zeist West, Zeist, The Netherlands; 3University Hospital Heidelberg, Department of General Practice and Health Services Research, Heidelberg, Germany; 4Radboud University Medical Centre, Radboud Institute for Health Sciences, Department of Clinical Pharmacy, Nijmegen, The Netherlands; 5Leiden University Medical Centre, Department of Clinical Pharmacy and Toxicology, Leiden, The Netherlands
Correspondence: Esther Kuipers
Radboud University Medical Centre, Radboud Institute for Health Sciences, Department of IQ Healthcare, PO Box 9101, Nijmegen 6500 HB, The Netherlands
Tel +31 24 361 0591
Fax +31 24 354 0166
Email [email protected]
Background: Treatment of obstructive lung disease with inhalation therapy needs changes in patient behavior. Shortly after the start with inhaled corticosteroids (ICS) maintenance therapy, patients might be in need of additional pharmaceutical care, tailored to their individual needs. This study aimed to provide insight into patient behavior, goals and perceptions regarding their medical treatment at start with ICS therapy, by telephone interviews with ICS starters. Besides, this study investigated pharmacists’ and patients’ experiences with these interviews and opinions on the utility of this type of consultation for daily practice.
Methods: Semi-structured telephone interviews were conducted by pharmacists with adult patients 2– 3 weeks after starting ICS. The Theoretical Domain Framework (TDF) was used for data analysis and coding. Afterward, the patients and pharmacists were questioned about their experiences with the interview.
Results: Five pharmacists conducted interviews with 23 ICS starters. Except the domains “environmental context and resources”, “optimism”, and “reinforcement”, the remaining 11 domains in the TDF were addressed in the interviews. The majority of patients defined personal goals, which mainly addressed disease or symptom control (clinical goals). Some patients showed a lack of knowledge regarding the clinical indication or therapy duration. Views on beneficial medication effects differed between patients. Some patients specifically mentioned concerns or anxiety about side effects. The interviewees described different perceptions on the necessity of a personalized routine for regular medication use. Patients and pharmacists both felt positive about an added value of these interviews for daily practice.
Conclusion: Patient interviews shortly after start with ICS therapy revealed various perceptions and beliefs that might influence medication use and achievement of individual treatment goals. The patients appreciated the opportunity to ask questions and share their perspectives and needs with their pharmacist, and the pharmacists experienced that the interviews had added value.
Keywords: inhalation therapy, asthma, COPD, pharmaceutical care, pharmacy practice research, consultation, patient perspective
Introduction
Daily use of inhaled corticosteroids (ICS) is effective for patients with obstructive lung diseases in the reduction of symptoms and the frequency of exacerbations.1,2 The behavior of taking medication for a chronic disease is a complex and dynamic process,3 and inhaled therapy has additional challenges for patients in daily practice.4 Both the inhaler device technique and patient adherence to ICS are crucial in the effectiveness of the medical treatment.5–8 However, patient adherence to ICS is shown to be generally poor,9–12 and many patients experience problems in achieving and maintaining the correct inhaler device technique.5,6,13–15
Patient support programs, such as medication management and counseling, have the potential to improve patient’s disease control and medication adherence.16,17 A previous pharmacist intervention study has shown a positive impact on patients’ knowledge about asthma and medication.18 Other studies have shown that pharmacist interventions were effective in improving the inhaler device technique skills,19,20 and a randomized controlled trial demonstrated that pharmacist interventions improved both medication adherence and inhaler device technique in patients with chronic obstructive pulmonary disease (COPD).14 However, pharmacists’ interventions in these studies mainly focused on improving patients’ knowledge or practical skills by providing protocol-defined information or education, rather than being tailored on patients’ individual needs or goals.
As patients differ fundamentally in coping with their chronic disease, there might be more individual barriers that hamper optimal medication use, which need different techniques to change behavior. For example, beside knowledge of their disease, asthma patients reported different beliefs about the consequences of their condition and the necessity of the medication prescribed.21 Additionally, fear and worries about short- and long-term side effects of treatment, including safety of the medication and addiction to it, were related to poorer adherence.22 In patients with COPD, the knowledge of ICS and potential side effects was shown to be limited.23 Besides, patients’ beliefs and expectations about therapy, and the complexity of the dose regimen (eg, frequency of administration) influenced medication use.24,25 The Theoretical Domains Framework (TDF) has been developed to summarize possible determinants to address factors that influence behavior, from a behavior change psychology perspective.26,27 This framework can be used as a theoretical basis to identify and develop theory-informed behavior change interventions.26,28,29
Taking medication is a complex behavioral process, and a previous study has shown that non-adherence to medicines for chronic conditions may develop shortly after the start of medication.30 So this period is an important time window for pharmacist interventions; patients may be in need of counseling and support, while being highly focused on their health and new therapy.31 Earlier studies have shown that questioning patients during the first refill of a medicine could encourage patients to report how they experienced their medication use and if they had drug-related problems.32,33 At present, the pharmacy staff mainly plays a role in organizing the logistics of repeat prescriptions,34,35 but exploring patients’ experiences with the medication is not yet routine in daily practice.36 However, especially with inhaled medication, the recognition of (adherence) problems could be delayed, as refills with inhalers containing a large number of doses (eg, 200 doses in some pMDIs) could take some time.
Consequently, consultations shortly after the start of inhaled maintenance medication may be useful to explore patients’ personal goals, discuss medication experiences, concerns, questions and problems. However, such care is not yet part of daily practice, and little is known about the utility and feasibility of these consultations, and the best way to conduct them.
This study aimed to provide insight into personal goals, patient perceptions and beliefs regarding the medical treatment for their obstructive lung disease in patients who just started their drug therapy, by a telephone interview with their pharmacist. Furthermore, this study aimed to evaluate the experiences of patients and pharmacists on the utility of these interviews.
Methods
Design
This was a qualitative study based on telephone interviews performed by five pharmacists from five community pharmacies in the Netherlands between July and December 2018. Reporting of the study follows the relevant sections of the consolidated criteria for reporting qualitative research (COREQ).37
Setting
The participating pharmacists were recruited by convenience sampling in the researchers’ network. They had a special interest in pharmacy practice research and lung diseases (eg, as member of the special interest group “lung diseases” of the Royal Dutch Association for the advancement of Pharmacy (KNMP)). In the Netherlands, pharmacists have a professional and legal responsibility to enhance the safety and efficacy of their patients’ drug treatment. As most patients in the Netherlands adhere to one community pharmacy, pharmacists usually dispose of complete prescription histories of their patients.38,39
In community pharmacies in the Netherlands, patient counseling is usually linked to the moment of the first dispensing and first refill (ie, second dispensing) of the medication. The pharmacy staff generally consists of pharmacists (educated in 6-year university programs) and pharmacy assistants, who were educated in 3-year vocational programs.40 In contrast to the first dispensing consultations, which mainly aim to provide practical information and technical instruction to the patient, during the second and subsequent dispensing encounters, the pharmacy staff ideally ask for patients’ experiences with the medication.41
Ethical Approval
The study protocol was approved by the Ethical Committee of the Radboudumc Nijmegen (approval number, 2018–4381). All the procedures were in accordance with the requirements for studies involving human participants, with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Prior written informed consent was obtained from all individual participants included in this study.
Patient Inclusion
Patients were screened and selected during the first dispensing by the prescription checks of the pharmacists or by a search strategy in the pharmacy information system. The pharmacists invited all patients >18 years of age who received a first dispensing of ICS or the combination of an ICS and a long-acting beta-agonist (LABA); Anatomic Therapeutic Chemical (ATC)-codes: R03BA, R03AK06, R03AK07 and R03AK08.42 A first dispensing was defined as a dispensing of a new prescription in the absence of a dispensing for ICS during the previous 12 months. Patients were included if they spoke, read, and wrote Dutch sufficiently well.
Patients fulfilling the inclusion criteria were informed of the study personally at the moment of the first dispensing encounter or by telephone within one to two weeks afterward. The patients also received written information and an informed consent form. If the patient was willing to participate and provided informed consent, the pharmacist made an appointment for a telephone interview. Anonymized data about gender, age, type and dose of medication were obtained from the pharmacy information system.
Patient Interview
The interviews were performed by the five community pharmacists (including one of the researchers (EK)) in their pharmacy. The telephone interview was semi-structured, allowing interviewees to respond in their own words. The content of the telephone interview guide (Appendix A) was based on the existing literature and recommendations from national pharmaceutical guidelines regarding the dispensing encounters.41,43,44 The information collected was about symptoms and disease control, the experiences with medication use in daily practice, patients’ personal goals, and disease and treatment-related concerns and personal questions (eg, side effects, concerns). Each interview took about 10–15 mins.
Estimation of the Utility of the Interviews
At the end of the interview, patients were asked how they felt about the interview. Besides, all pharmacists were questioned about their experiences with the patient interviews, regarding the feasibility in daily practice (time investment, organizational factors), and their ideas about the utility and opportunities for providing additional care (for the topic list: see Appendix A). All interviews were conducted in Dutch.
Data Analysis
All interviews were digitally recorded and transcribed verbatim. Data analysis was facilitated by Microsoft Office Excel. Data were analyzed using an iteration of inductive and deductive steps in a thematic approach.45 In the first phase of the analysis process, two members of the research team (EK and MT) started with an inductive approach by several readings of the transcripts to become familiar with the data and check the appropriateness of the 14 domains Theoretical Domains Framework (TDF)27 for analysis. During the deductive second phase, themes regarding the perceptions and beliefs regarding medication used were defined and organized into the TDF domains. Each theme was reviewed for content and allocated into relevant domains of the TDF or recorded as not fitting into any of the TDF domains. One member of the research team (EK) read and coded the transcripts. A second member (MT) independently coded a sample of the transcripts (approximately 40%). Discrepancies were discussed until consensus was reached. Illustrative citations were selected for each of the domains. After 23 interviews no new themes were derived from analysis and data saturation was achieved.46,47 In the final phase, it was checked whether there were text fragments that could not be categorized within the TDF, but this was not the case.
Results
Participants
In five pharmacies, 223 ICS-users were initially selected and screened for eligibility (Figure 1). A total of 164 patients did not meet the inclusion criteria, for example, concerning their age, or because they switched from an ICS to a combination of ICS/LABA. Fifty-nine patients were eligible. From those pharmacists contacted a first group of 33 patients, of whom 10 did not participate. This was due to refusal from the beginning or due to later drop out. For example, one patient initially agreed to participate, but did not answer the phone at the moment of the appointment and was not available anymore. In total 23 patients were interviewed for the study (Table 1) within 2–3 weeks after starting the ICS. The mean duration of the interviews was about 11 mins (range 4 to 29 mins).
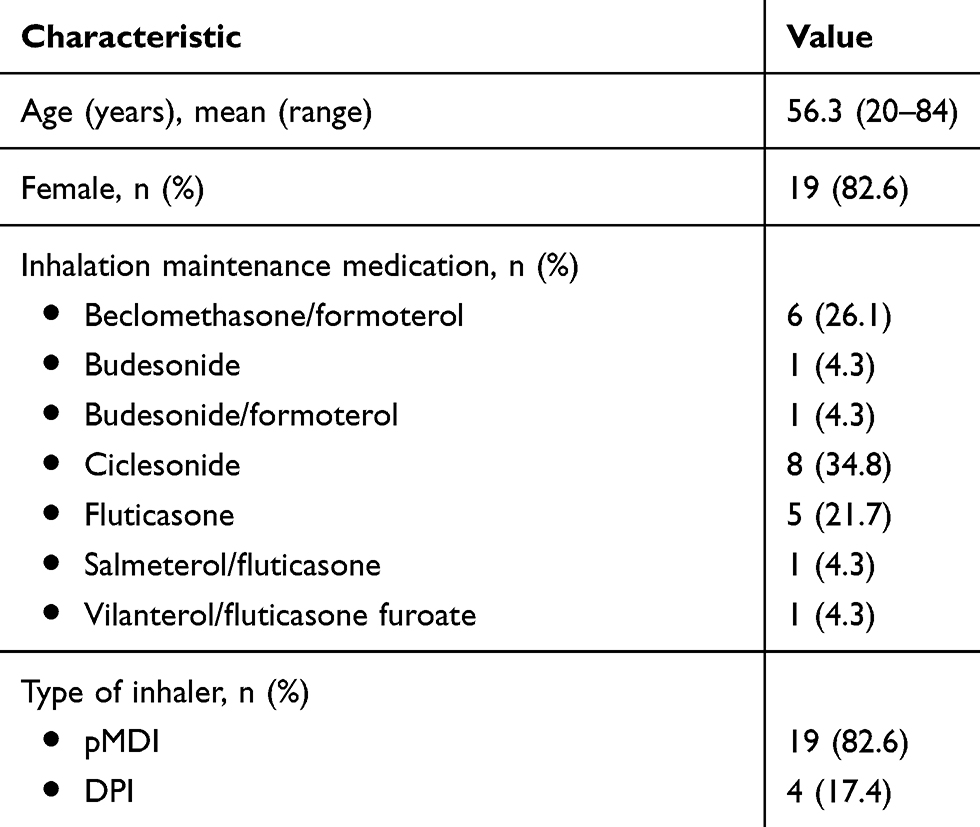 |
Table 1 Patient Characteristics (n=23) |
All five interviewers were female and they were practicing pharmacists, with working experience in the community pharmacy between 1 and 15 years.
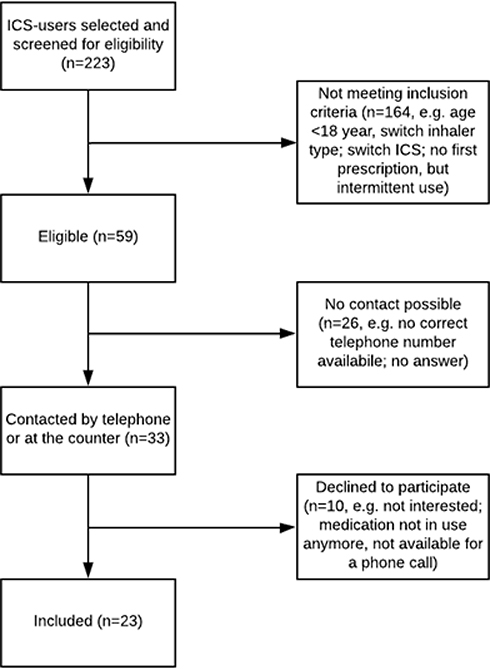 |
Figure 1 Flowchart patient inclusion. Abbreviation: ICS, inhaled corticosteroids. |
TDF Domains
Of the 14 TDF domains, 11 domains with possible influence on patients’ medication use behavior were covered, except the domains “reinforcement”, “optimism”, and “environmental context and resources”. The domains with illustrative quotes are presented in Table 2.
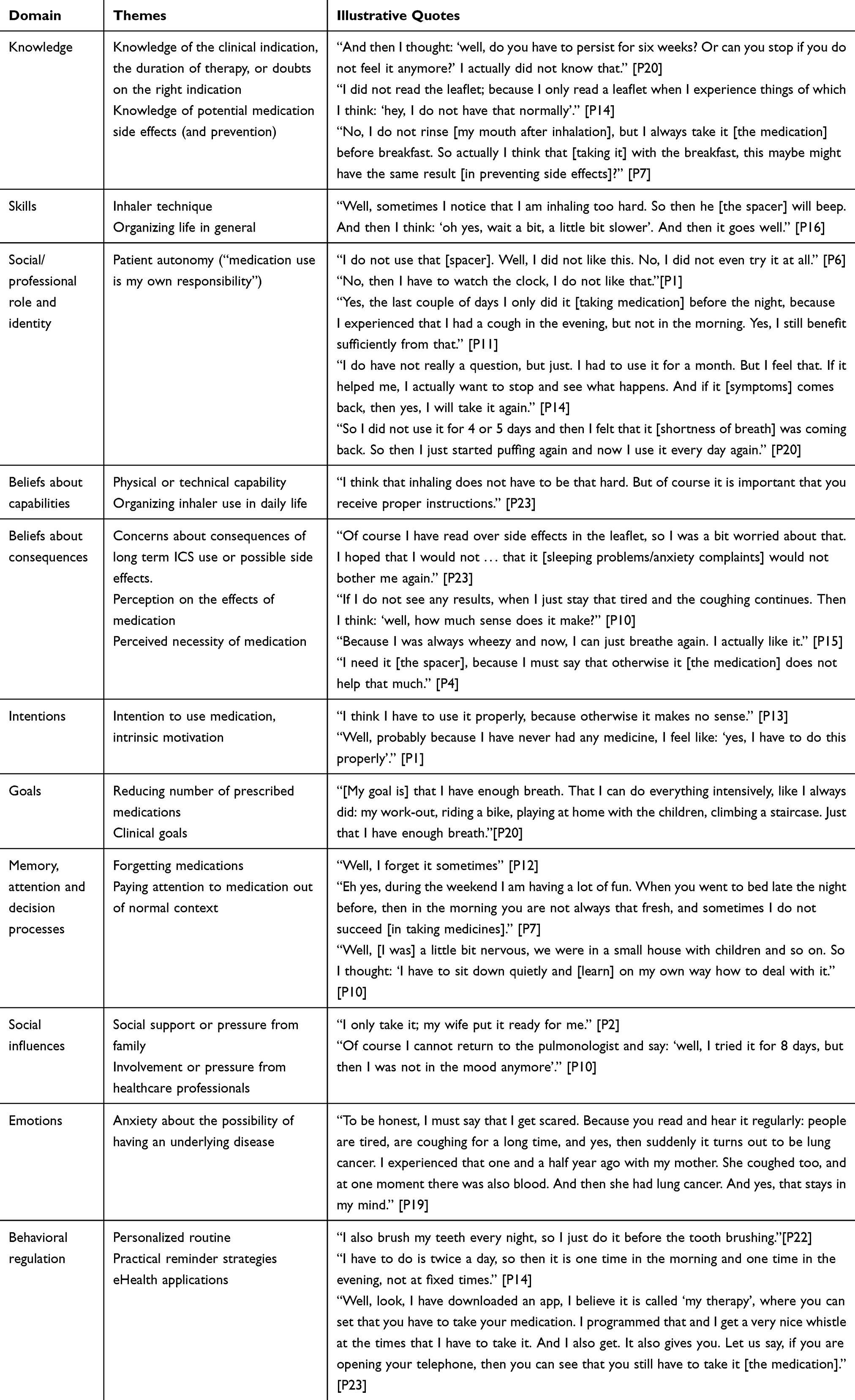 |
Table 2 TDF Domains and Illustrative Quotes |
Some patients reported a lack of knowledge of the clinical indication, the duration of therapy, or doubts on the right indication. The extent of knowledge on potential medication side effects and prevention differed strongly between the patients. Some patients reported that they were well informed, while one patient specifically mentioned that she did not know anything regarding the possible side effects, but that she would possibly be more interested in the side effects when experiencing unexpected effects.
Patients had different perceptions on the effect of medication; some patients doubted an effect, while others were convinced of a beneficial effect. The perceived necessity of the medication was higher when patients experienced a reduction in symptoms.
Some patients reported that using their pMDI with a spacer was easy and that they never experienced any problems, while others described some difficulties with the inhaler technique. Patients’ beliefs about capabilities included their beliefs about their physical or technical capability and skills to use their inhaler, but also beliefs about the capability to organize using the inhaler in daily life.
The majority of respondents mentioned that they already had developed a personalized routine for using the medication, for example, by linking the inhalation to meal times, the moment of tooth brushing, or bed time. Almost one-third of the patients used practical reminder strategies: they placed the medication in a visually prominent place (eg, on the kitchen table or near the sink). One patient used an eHealth application on her mobile phone, which contained a reminder function.
Patient autonomy was considered an important identity factor; respondents regarded medication use as their own responsibility. This was expressed in different situations; for example, one patient had never used the inhaler with the spacer because she did not want to. Another patient tried to use the inhaler without a spacer but experienced that the medication was less effective and decided that the spacer was really necessary for her.
One patient mentioned that she used her medication according to the frequency prescribed, but she wanted to choose her own time during the day to use the medication. A few patients decided or doubted about reducing their daily dose or stop the medication without consulting any healthcare professional, when they felt that there was no need to continue.
Although some patients reported that they never forgot to take their medications as prescribed, there were also people admitting that this happened sometimes. It seemed more difficult to pay attention to medication specifically when patients were out of normal context, for example, during weekends or on holidays.
The majority of patients (20 of the 23) described personal goals. Two patients described goals to reduce the total number of prescribed medications. However, most patients mentioned that their condition had impacted their lives and they aimed clinical goals, like the improvement of symptoms and disease control.
During one of the conversations, there were several signals that the patient (male, 84 years old) experienced difficulties in organizing his life in general. During the conversation, the patient seemed to be a little bit confused and he could not answer all questions clearly (“I don’t know where my inhaler is”, or “I think I have to use it twice a day, but to be honest: I don’t know.”). There were signs of impairment in both mental and physical skills to use all medication as prescribed and the patient received help from his wife. However, during an additional interview with his wife, she reported that she found it difficult to support her husband with the use of the inhalation medication:
“The inhaler that he received from the doctor, he actually didn’t use it at all. It is completely new. I don’t know why. The inhaler is actually the only medicine that I’m not involved with very much”.
Experiences with the Interviews
Eighteen patients were asked for their opinion regarding the interview with the pharmacist. All of them felt positive and some patients specifically mentioned that they have liked sharing their experiences with the pharmacist or asking their questions:
“It was a good conversation, nice and smooth. And I always feel when talking with a doctor: ‘you may not lie about medication use’. But yes, I am busy and then I do not succeed [in taking medicines] and then I feel embarrassed [to tell]. But I did not get that idea now, and I really like that.” [P7]
“Well, I am glad that I was able to tell briefly my concerns.”[P19]
Patients regarded an additional telephone consult with the pharmacist to be useful, even when they personally did not have problems or questions at that moment:
“It is good to ask those questions, because there are people who have troubles. Not me, but it is good that those questions are being asked.” [P5]
All pharmacists felt positive about the interviews. Conducting the interviews was reported to be feasible in daily practice; the time investment of the patient interviews was manageable and acceptable for all pharmacists. Two of the pharmacists reported to have experienced difficulties with the selection of patients and they initially found a lot of patients who were not eligible. All pharmacists felt that these telephone consultations, shortly after the start of ICS, could potentially have an added value to the patient (eg, the opportunity to share their experiences and ask questions shortly after the start), but also to themselves (eg, the opportunity to obtain early insights in patients’ thoughts and motivation regarding their medication use).
“One patient said to me: ‘I actually do not notice any effect. I don’t know if I should continue, what should I do?’ At the moment it felt good to provide appropriate information.”[A4]
Discussion
This study provided insights into the perceptions and beliefs regarding medication use of patients shortly after their start with ICS maintenance therapy in obstructive lung diseases. Telephone interviews in this study revealed various perceptions that might influence the achievement of individual treatment goals and showed opportunities for additional pharmaceutical care after starting with ICS.
Patients shared much personal information during the interviews. They revealed various factors influencing the perspectives regarding their medication and condition, which might have hampered optimal medication use (now or later). Eleven of the 14 TDF domains were covered by the information from 23 interviews. Patients reported different perceptions and beliefs on the effect of medication, and although some reported that they had always taken their medications as prescribed, others admitted that they did not (either intentional or unintentional). Some patients reported that they already had developed a routine for using the medication daily, while others were still searching for such a routine. In earlier studies, building a habit was stated to be useful for overcoming forgetfulness, and also lengthen medication persistence (ie, the length of time between initiation and discontinuation).48
Separating pharmaceutical care from the medication delivery process might provide more timely insights in patients’ needs and wants. Some important information that patients reported during the interviews would not have been emerged during standard counseling at the pharmacy’s counter. Pharmacists’ interventions in earlier studies focused on the domains of knowledge and skills.14,18–20 Our study showed additional individual barriers or facilitators, that might influence the behavior of medication use. Personal goals, concerns about side effects or emotional factors would probably not have been asked and discussed during the regular encounters. Earlier studies have shown that the pharmacy staff is generally used to provide practical information and technical instruction, but do not often discuss patient’s preferences and perceptions about prescribed medications,49,50 or stimulate patients to ask questions.50–55
All responding patients in this study felt positive about the interview and although not all patients reported to be in need of additional care, they appreciated the moment of personal attention and often reported that this evaluation moment was of added value for them. Also all pharmacists experienced the interviews generally as beneficial for the patients and for themselves. Although this type of counseling is not routine, all of them were positive about the interview and they regarded this type of consultation as feasible in daily practice. They felt that additional telephone pharmacist consultations in daily practice gave them opportunities to grow in applying a patient-tailored approach, and to focus on exploring patients’ individual needs and wants, rather than only providing practical information. Both patients and pharmacists reported that they saw an added value of the pharmacists’ consultations and that these could possibly provide information for future tailored interventions related to personal goals, side effects and behavior for medication use.
Strengths and Limitations
This study emphasized the added value of an early evaluation of patient’s beliefs and perceptions, shortly after the start with ICS; patients mentioned several issues that were judged to need additional pharmaceutical or medical care. Although it is practically impossible to check patients’ inhaler technique during a telephone interview, patients were invited for a check in the pharmacy if there was a signal that they were in need of that. Judging from these consultations, the pharmacists could not have estimated in advance which patients were in need of additional pharmaceutical or medical care. It could not be deduced from a person’s pharmacy record whether additional care was needed. So, pharmacists can gather relevant information from and about their patients if they practice this kind of consultation.
There are some limitations to this study. First, in this convenience sample, the majority of the participants was female, which might hamper extrapolation of the findings to other individuals. Based on the general data of ICS users in the pharmacy population, we had expected that a lower percentage (55–60%) of the participants would be female. During the inclusion, the women appeared to be more willing to participate. Although there was a broad age range (20–84 years), younger people were also underrepresented in the sample. There were less starters with ICS in the age group 18–50 than in the group aged >50 years. This may be explained by the fact that it is likely that younger patients had been diagnosed with asthma during childhood. However, although the proportion of male – and younger participants was lower than expected, the research team remains confident that the patients illustrated a broad range of experiences and that interviewing was continued until data saturation had been met. This is also reflected in the broad range of identified TDF domains. Besides, this study only included patients who started with ICS: the patients that had switched their medication or inhaler device were excluded. However, this latter population could also comprise patients in need of additional care, as switching could indicate suboptimal therapy. Second, although the TDF covered most of the data, some of the identified themes were strongly related, and therefore could be coded to more than one domain, depending on the patients’ context. For example, the wife’s role in the situation of the earlier described case (ie, the confused man, possibly demented), is related to the domain of social support, but also interfaces with the domains of skills (mental and physical skills to organize life in general) and memory, attention and decision processes. Third, it appeared to be difficult for the pharmacists to enter the selection criteria completely in the searching module of the pharmacy information system. It was not possible to select the age and the system did not recognize immediately whether patients had switched between different inhaler types or ICS and ICS/LABA combinations. Consequently, the selection had to be checked manually and the majority of people from the initial selection seemed not eligible. This was also mentioned by the pharmacists; the selection of patients took more time than expected.
Conclusion
Telephone interviews conducted by community pharmacists shortly after start with ICS maintenance therapy revealed various behavioral barriers that might influence the achievement of individual treatment goals. Patients shared important information, which probably would not or incompletely have emerged during encounters in regular daily practice. Both patients and pharmacists were positive about the interviews. Pharmacists felt that telephone consultation gives them an opportunity to grow in applying a patient-tailored approach and they experienced that they were of added value. The patients appreciated the opportunity to ask their questions and share their perspectives and needs with a healthcare professional.
In several patients, problems were detected that were judged to need additional pharmaceutical or medical care. Further research is needed to explore the potential benefit of the pharmacists’ consultation and the effects of this type of early intervention.
Acknowledgments
We thank all patients and community pharmacists who participated in this study. This work was supported by unconditional research grants from the Royal Dutch Pharmacists Association (KNMP) [grant number PR16_1410]; and AstraZeneca [grant number 2603949255].
Disclosure
Mrs Esther Kuipers and Dr Martina Teichert report grants from Royal Dutch Pharmacists Association and AstraZeneca, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Sin DD, McAlister FA, Man SF, Anthonisen NR. Contemporary management of chronic obstructive pulmonary disease: scientific review. JAMA. 2003;290(17):2301–2312. doi:10.1001/jama.290.17.2301
2. Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA). Available from: http://www.ginasthma.org. Archived by WebCite® at http://www.webcitation.org/75oQTDICX.
3. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
4. George M, Bender B. New insights to improve treatment adherence in asthma and COPD. Patient Prefer Adherence. 2019;13:1325–1334. doi:10.2147/PPA.S209532
5. Hesso I, Gebara SN, Kayyali R. Impact of community pharmacists in COPD management: inhalation technique and medication adherence. Respir Med. 2016;118:22–30. doi:10.1016/j.rmed.2016.07.010
6. Garcia-Cardenas V, Sabater-Hernandez D, Kenny P, Martinez-Martinez F, Faus MJ, Benrimoj SI. Effect of a pharmacist intervention on asthma control. A cluster randomised trial. Respir Med. 2013;107(9):1346–1355. doi:10.1016/j.rmed.2013.05.014
7. Haughney J, Price D, Barnes NC, Virchow JC, Roche N, Chrystyn H. Choosing inhaler devices for people with asthma: current knowledge and outstanding research needs. Respir Med. 2010;104(9):1237–1245. doi:10.1016/j.rmed.2010.04.012
8. Mannan H, Foo SW, Cochrane B. Does device matter for inhaled therapies in advanced chronic obstructive pulmonary disease (COPD)? A comparative trial of two devices. BMC Res Notes. 2019;12(1):94. doi:10.1186/s13104-019-4123-5
9. Charles T, Quinn D, Weatherall M, Aldington S, Beasley R, Holt S. An audiovisual reminder function improves adherence with inhaled corticosteroid therapy in asthma. J Allergy Clin Immunol. 2007;119(4):811–816. doi:10.1016/j.jaci.2006.11.700
10. Burgess SW, Sly PD, Devadason SG. Providing feedback on adherence increases use of preventive medication by asthmatic children. J Asthma. 2010;47(2):198–201. doi:10.3109/02770900903483840
11. Foster JM, Usherwood T, Smith L, et al. Inhaler reminders improve adherence with controller treatment in primary care patients with asthma. J Allergy Clin Immunol. 2014;134(6):1260–1268.e1263. doi:10.1016/j.jaci.2014.05.041
12. Gonzalez-Martin G, Joo I, Sanchez I. Evaluation of the impact of a pharmaceutical care program in children with asthma. Patient Educ Couns. 2003;49(1):13–18. doi:10.1016/S0738-3991(02)00027-7
13. Basheti IA, Qunaibi EA, Hamadi SA, Reddel HK. Inhaler technique training and health-care professionals: effective long-term solution for a current problem. Respir Care. 2014;59(11):1716–1725. doi:10.4187/respcare.02671
14. Tommelein E, Mehuys E, Van Hees T, et al. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled trial. Br J Clin Pharmacol. 2014;77(5):756–766. doi:10.1111/bcp.2014.77.issue-5
15. Price D, Bosnic-Anticevich S, Briggs A, et al. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107(1):37–46. doi:10.1016/j.rmed.2012.09.017
16. Shanmugam S, Varughese J, Nair MA, et al. Pharmaceutical care for asthma patients: a developing country’s experience. J Res Pharm Pract. 2012;1(2):66–71. doi:10.4103/2279-042X.108373
17. Ganguli A, Clewell J, Shillington AC. The impact of patient support programs on adherence, clinical, humanistic, and economic patient outcomes: a targeted systematic review. Patient Prefer Adherence. 2016;10:711–725. doi:10.2147/PPA.S101175
18. Narhi U, Airaksinen M, Tanskanen P, Enlund H. The effects of a pharmacy-based intervention on the knowledge and attitudes of asthma patients. Patient Educ Couns. 2001;43(2):171–177. doi:10.1016/S0738-3991(00)00158-0
19. Hammerlein A, Muller U, Schulz M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Pract. 2011;17(1):61–70. doi:10.1111/j.1365-2753.2010.01369.x
20. Bosnic-Anticevich SZ, Sinha H, So S, Reddel HK. Metered-dose inhaler technique: the effect of two educational interventions delivered in community pharmacy over time. J Asthma. 2010;47(3):251–256. doi:10.3109/02770900903580843
21. Adams S, Pill R, Jones A. Medication, chronic illness and identity: the perspective of people with asthma. Soc Sci Med. 1997;45(2):189–201. doi:10.1016/S0277-9536(96)00333-4
22. Lycett H, Wildman E, Raebel EM, Sherlock JP, Kenny T, Chan AHY. Treatment perceptions in patients with asthma: synthesis of factors influencing adherence. Respir Med. 2018;141:180–189. doi:10.1016/j.rmed.2018.06.032
23. Gilworth G, Harries T, Corrigan C, Thomas M, White P. Perceptions of COPD patients of the proposed withdrawal of inhaled corticosteroids prescribed outside guidelines: a qualitative study. Chron Respir Dis. 2019;16:1479973119855880. doi:10.1177/1479973119855880
24. Rand CS. Patient adherence with COPD therapy. Eur Respir Rev. 2005;14(96):97–101. doi:10.1183/09059180.05.00009604
25. Koehorst-Ter Huurne K, Brusse-Keizer M, van der Valk P, Movig K, van der Palen J, Bode C. Patients with underuse or overuse of inhaled corticosteroids have different perceptions and beliefs regarding COPD and inhaled medication. Patient Prefer Adherence. 2018;12:1777–1783. doi:10.2147/PPA.S167002
26. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implementation Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
27. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Sci. 2012;7:37. doi:10.1186/1748-5908-7-37
28. Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
29. French SD, Green SE, O’Connor DA, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implementation Sci. 2012;7:38. doi:10.1186/1748-5908-7-38
30. Barber N, Parsons J, Clifford S, Darracott R, Horne R. Patients’ problems with new medication for chronic conditions. Qual Saf Health Care. 2004;13(3):172–175. doi:10.1136/qshc.2003.005926
31. Feifer RA, Greenberg L, Rosenberg-Brandl S, Franzblau-Isaac E. Pharmacist counseling at the start of therapy: patient receptivity to offers of in-person and subsequent telephonic clinical support. Popul Health Manag. 2010;13(4):189–193. doi:10.1089/pop.2009.0064
32. Hugtenburg JG, Blom AT, Gopie CT, Beckeringh JJ. Communicating with patients the second time they present their prescription at the pharmacy. Discovering patients’ drug-related problems. Pharm World Sci. 2004;26(6):328–332. doi:10.1007/s11096-004-0560-9
33. Hugtenburg JGB, Gopie CTW. Zinvolle actie aan de balie, Eerste en tweede uitgifte van geneesmiddelen. Pharm Weekbl. 2001;136(43):1612–1613.
34. Bond C, Matheson C, Williams S, Williams P, Donnan P. Repeat prescribing: a role for community pharmacists in controlling and monitoring repeat prescriptions. Br J Gen Pract. 2000;50(453):271–275.
35. De Smet PA, Dautzenberg M. Repeat prescribing: scale, problems and quality management in ambulatory care patients. Drugs. 2004;64(16):1779–1800. doi:10.2165/00003495-200464160-00005
36. van Dijk L, Hendriks M, Zwikker H, de Jong J, Vervloet M Informatiebehoeften van patiënten over geneesmiddelen. Available from: https://www.nivel.nl/sites/default/files/bestanden/Informatiebehoeften_van_patienten_over_geneesmiddelen.pdf. Published 2016.
37. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
38. Buurma H, Bouvy ML, De Smet PA, Floor-Schreudering A, Leufkens HG, Egberts AC. Prevalence and determinants of pharmacy shopping behaviour. J Clin Pharm Ther. 2008;33(1):17–23. doi:10.1111/jcp.2008.33.issue-1
39. Wet op de geneeskundige behandelingsovereenkomst (WGBO). Available from: http://wetten.overheid.nl/BWBR0005290/2016-04-01#Boek7_Titel7_Afdeling5. Published 2018.
40. Koehler TC, Bok H, Westerman M, Jaarsma D. Developing a competency framework for pharmacy technicians: perspectives from the field. Res Social Adm Pharm. 2019;15(5):514–520.
41. KNMP. KNMP-richtlijn Ter hand stellen. Available from: https://www.knmp.nl/praktijkvoering/bekostiging/begeleidingsgesprek-nieuw-geneesmiddel/knmp-richtlijn-ter-hand-stellen/at_download/file_1. Published 2018.
42. World Health Organization Collaborating Centre for Drug Statistics Methodology. ATC classifications system. Oslo: World Health Organization. Available from: https://www.whocc.no/atc_ddd_index/.
43. KNMP. KNMP-richtlijn COPD. Available from: https://www.knmp.nl/praktijkvoering/richtlijnen/knmp-richtlijnen-farmaceutische-zorg/knmp-richtlijn-copd. Published 2014.
44. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
45. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
46. Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. 2017;27(4):591–608. doi:10.1177/1049732316665344
47. Guest G, Bunce A, Johnson L. How many interviews are enough?: An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
48. Vrijens B, Urquhart J, White D. Electronically monitored dosing histories can be used to develop a medication-taking habit and manage patient adherence. Expert Rev Clin Pharmacol. 2014;7(5):633–644. doi:10.1586/17512433.2014.940896
49. Koster ES, van Meeteren MM, van Dijk M, et al. Patient-provider interaction during medication encounters: a study in outpatient pharmacies in the Netherlands. Patient Educ Couns. 2015;98(7):843–848. doi:10.1016/j.pec.2015.03.007
50. van Dijk M, Blom L, Koopman L, et al. Patient-provider communication about medication use at the community pharmacy counter. Int J Pharm Pract. 2016;24(1):13–21. doi:10.1111/ijpp.2016.24.issue-1
51. van Dulmen S. The value of tailored communication for person-centred outcomes. J Eval Clin Pract. 2011;17(2):381–383. doi:10.1111/jep.2011.17.issue-2
52. van Hulten R, Blom L, Mattheusens J, Wolters M, Bouvy M. Communication with patients who are dispensed a first prescription of chronic medication in the community pharmacy. Patient Educ Couns. 2011;83(3):417–422. doi:10.1016/j.pec.2011.05.020
53. Stevenson FA, Cox K, Britten N, Dundar Y. A systematic review of the research on communication between patients and health care professionals about medicines: the consequences for concordance. Health Expect. 2004;7(3):235–245. doi:10.1111/hex.2004.7.issue-3
54. Driesenaar JA, De Smet PA, van Hulten R, Hu L, van Dulmen S. Communication during counseling sessions about inhaled corticosteroids at the community pharmacy. Patient Prefer Adherence. 2016;10:2239–2254. doi:10.2147/PPA.S108006
55. Driesenaar JA, De Smet PA, van Hulten R, Noordman J, van Dulmen S. Cue-responding behaviors during pharmacy counseling sessions with patients with asthma about inhaled corticosteroids: potential relations with medication beliefs and self-reported adherence. Health Commun. 2016;31(10):1266–1275. doi:10.1080/10410236.2015.1062974
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.