Back to Journals » Patient Preference and Adherence » Volume 19
Exploring Patient Preference Information in Clinical Research and Decision Models: An Investigative Survey
Authors Di Blasio M, Bami Z, Bracco M, Fava C, Visconti A ![]() , Baldi I
, Baldi I ![]() , Berchialla P
, Berchialla P ![]()
Received 11 June 2025
Accepted for publication 10 September 2025
Published 12 November 2025 Volume 2025:19 Pages 3541—3547
DOI https://doi.org/10.2147/PPA.S541040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Martina Di Blasio,1 Zahra Bami,1 Matteo Bracco,1 Carmen Fava,2 Alessia Visconti,1 Ileana Baldi,3,* Paola Berchialla1,*
1Center for Biostatistics, Epidemiology, and Public Health, Department of Clinical and Biological Sciences, University of Turin, Turin, Italy; 2Department of Clinical and Biological Sciences, University of Turin, Turin, Italy; 3Department of Cardiac Thoracic Vascular Sciences and Public Health, University of Padua, Padua, Italy
*These authors contributed equally to this work
Correspondence: Alessia Visconti, Center for Biostatistics, Epidemiology, and Public Health, Department of Clinical and Biological Sciences, University of Turin, Regione Gonzole 10, Orbassano, Turin, 10043, Italy, Email [email protected]
Purpose: Patient preferences are playing an increasingly pivotal role in defining care pathways, assessing care quality, and advancing healthcare technologies, but their current use remains unclear.
Patients and Methods: We conducted an online survey collecting data from 46 experts in clinical research, pharmaceutical industry, regulatory affairs, and health technology assessment.
Results: About 30% of our respondents are using patient preference information routinely, and 90% are willing to prioritize its integration in the future. This is despite challenges such as limited patient engagement, difficulty in obtaining reliable data, and reluctance to deviate from traditional practices.
Conclusion: Here, we show a growing recognition of the potential benefits of integrating patient preference information, and that concerted efforts and investments are necessary to support wider adoption.
Plain Language Summary: In this work, we observed that while experts in clinical research, pharmaceutical industry, regulatory affairs, and health technology assessment recognize the importance of integrating patient preference information in clinical research and decision-making processes, its use is currently suboptimal. Following these observations, and to increase the use of patient preference information, we suggest concerted efforts and investments to establish reliable data repositories, make patient preference information readily accessible, and challenge the resistance to deviating from traditional practices.
Keywords: patient preference information, survey, evidence synthesis, decision-making
Introduction
Patients are increasingly recognized as key stakeholders in healthcare decision-making.1–3 Hence, the integration of patient preference information (PPI) is becoming critical,4,5 particularly when multiple therapeutic options lack clear distinctions in efficacy. In such scenarios, the patient’s perspective on side effect profiles, treatment administration methods, and/or impact on daily life can be the deciding factor in treatment selection.6 This ensures that medical decisions align with clinical best practices and consider individual patients’ values and lifestyle, likely enhancing treatment adherence, health outcomes, and patient satisfaction.7 This is in line with the concept of value-based healthcare, which focuses on delivering the care that matters most to patients while ensuring efficient resource utilization.8
To ensure medical products are developed and evaluated to effectively meet patient needs from conception to market and beyond, and to inform regulatory decisions to ensure approved treatments align with patient needs and desires,9–11 PPI must be considered in decision-making throughout the entire medical product life cycle, from early research and development to clinical trials, regulatory decisions, and post-market surveillance.12–14 However, there is limited knowledge on the extent to which healthcare professionals understand and apply findings from patient preference studies.10,11,15 To investigate the integration of PPI into clinical research and the development of new treatments as well as to explore the awareness, understanding, and interests related to PPI, we present here the results of a comprehensive online survey targeting experts in clinical research, pharmaceutical industry, regulatory affairs, and health technology assessment, providing readers with suggestions for improving PPI use in healthcare decision-making.
Materials and Methods
The Survey
The survey, available as Supplementary Data 1, was designed to investigate how patient preferences are perceived, utilized and valued. To this aim, we first conducted a literature search to identify the main domains in which preference studies are applied, i.e., clinical trial design, treatment decision-making, and drug development. Then, we used these domains to directly inform the wording of our survey items. In particular, our questionnaire was informed by a published systematic review which explored the potential use of PPI and the connected motivation, expectations, and concerns.16
The survey was administered via Typeform and was open from April 1, 2023, to June 30, 2023. It included 16 questions divided into six key areas: Frequency of Use: respondents were asked to indicate how often they incorporate patient preference information in their work, ranging from “never” to “always”; Perceived Benefits: the survey explored the perceived advantages of integrating patient preferences, such as improved trial design, enhanced patient recruitment and retention, and more patient-centric outcomes; Implementation Challenges: participants were prompted to identify and rate the significance of various obstacles to integrating patient preferences, including methodological complexities, resource constraints, and regulatory uncertainties; Organizational Readiness: questions assessed the availability and accessibility of patient preference data within respondents’ organizations, as well as the existence of processes for incorporating this information; Current Practices: the survey inquired about specific ways in which patient preference information is currently being used in respondents’ work, such as in protocol design, endpoint selection, or benefit-risk assessments; and Future Outlook: respondents were asked about their expectations for the future role of patient preferences in clinical research and treatment development.
Survey Respondents
We used a snowball sampling approach, starting from members of the Italian Society of Pharmaceutical Medicine (SIMeF, https://www.simef.it/; Supplementary Data 2). They were invited to forward the invitation to any colleague who might be interested in taking part, and those colleagues were asked to do the same, resulting in a total of 47 respondents. We did not collect any personal information (e.g., age, sex, geographical location), so we cannot confirm whether the respondents were all Italian and/or worked in Italy. To increase the response rate,17 respondents were remunerated with €10, which they could either receive as an Amazon voucher (n = 24) or donate to the Red Cross (n = 21). Two respondents decided not to receive or donate any remuneration.
We included one question to verify that users were paying attention to the questionnaire (i.e., “We want to verify that you are paying attention to the questions in the questionnaire, so we ask you to select the option ‘three’”) which disqualified one respondent.
Statistical Analysis
Descriptive statistics (i.e., absolute and relative frequencies) were generated using base R (v 4.4.2). Figures were generated using ggplot2 (v 2.3.5, bar plots in Figure 1 and 2), ggsankey (v 0.0.99999, Sankey plot in Figure 1), and ggsunburst (v 0.3.0, Sunburst plot in Supplementary Figure 1).
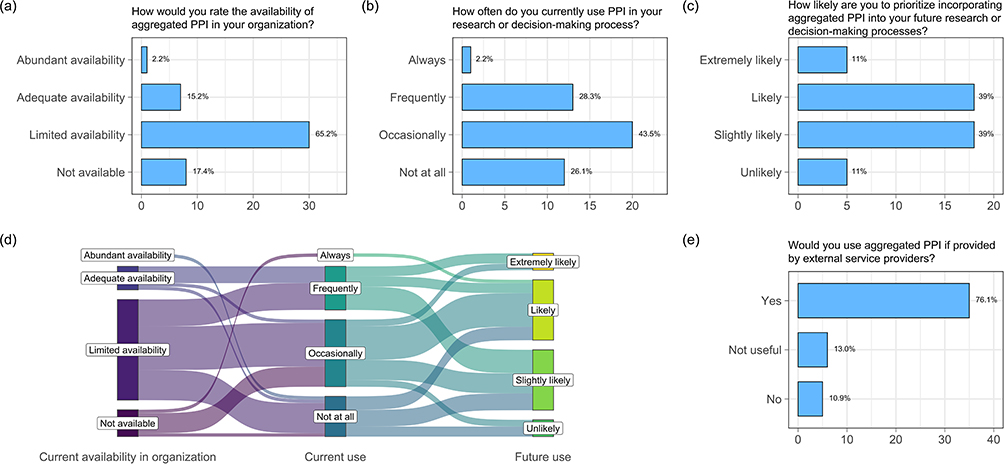 |
Figure 1 Patient Preference Information: Use in Research and Development. The bar plots in the upper panel show the distribution of responses regarding the (a) current availability and (b) use of PPI as well as (c) the likelihood of future use, with the (d) Sankey plot showing the flow of answers between these three topics. The bar plot in the bottom panel (e) shows the distribution of responses regarding the desire for external service providers supplying PPI. In each bar plot, the actual text of the question is reported as the title. The x-axes show absolute frequencies; relative frequencies are reported beside each bar. All questions allowed a single answer. Abbreviation: PPI, patient preference information. |
 |
Figure 2 Patient Preference Information: Importance and Challenges in Research and Development. The bar plots show the distribution of responses regarding the importance of PPI in (a) the design and outcomes of clinical trials and (b) development and commercialization of new treatments and therapies, as well as the challenges that researchers predict facing by including them in (c) clinical trial design and (d) decision-making. In each bar plot, the actual text of the question is reported as the title. The x-axes show absolute frequencies. The questions presented in the upper panels allowed a single answer, and their relative frequencies are reported beside each bar. The questions presented in the bottom panel allowed multiple answers, and their total absolute frequencies are reported beside each bar. The entry “Others” in (c) includes additional work, lack of time, and costs. Abbreviation: PPI, patient preference information. |
Due to the exploratory nature of this study, the sample size was not pre-determined, and all the received questionnaires were analyzed with no inclusion or exclusion criteria. Answers were processed anonymously in aggregate, and in compliance with GDPR regulations.
Results
Participant Characteristics
We elicited valid responses from 46 participants hailing from various sectors, including pharmaceutical and biotechnology companies (n = 27, 58.7%), academic and research institutions (n = 6, 13.0%), hospitals and clinics (n = 5, 10.9%), government agencies (n = 2, 4.3%), consulting firms (n = 1, 2.2%) and vendors (n = 1, 2.2%), with respondents also at the intersection between multiple roles (i.e., academic and research institutions, and hospitals and clinics, n = 4, 8.7%). The primary occupational domains encompassed researchers (n = 10, 21.7%), healthcare professionals (n = 9, 19.6%), statisticians (n = 8, 17.4%), quality assurance (n = 3, 6.5%), policy or decision analysts (n = 2, 4.3%), pharmacovigilance experts (n = 2, 4.3%), as well as various management and consultancy roles (n = 11, 23.9%), and a patient advocate (2.2%).
About half of the respondents researched more than one disease (n = 21, 45.7%), with slightly less than one quarter of them researching more than three areas (n = 11, 23.9%). Neurological, cardiovascular and oncological diseases were the most active research areas, with at least 10 respondents mentioning them, followed by endocrine, respiratory, gastrointestinal and renal diseases, infectious diseases and vaccines, and chronic pain (number of respondents ≥ 5, Supplementary Figure 1).
Patient Preference Information: Current and Future Use
The availability of PPI within organizations is at best limited, with only 8 respondents reporting it as at least adequate (17.5%; Figure 1a). In line with this observation, most respondents reported using PPI only occasionally or not at all (n = 32, 69.6%; Figure 1b), though future usage is likely (n = 41, 89.1%; Figure 1c). Notably, the lack of availability of PPI within one’s organization is not a clear indicator of its actual use: 7 out of the 8 respondents whose organizations did not provide any patient preference information still use it at least occasionally (Figure 1d), confirming the inclination to use such data when provided by external services (n = 35, 76.1%; Figure 1e). We also noted that the current use of PPI in research or decision-making processes positively influences future use (Figure 1d), highlighting the significance of such data.
Patient Preference Information: Importance and Challenges
Respondents agree that PPI could improve the identification of innovative clinical trial endpoints, at least moderately (n = 38, 82.0%, Figure 2a) and play a crucial role in the development and commercialization of new treatments and therapies (n = 36, 73.8%, Figure 2b), and would always have an impact, even if limited. However, significant ideological and practical challenges remain in effectively incorporating these preferences into practice, mostly due to the resistance to innovation and limited patient engagement, with the consequent difficulty in obtaining preference data (Figure 2c and d). Interestingly, while lack of time and/or budget and the necessity of additional work (“Others”, in Figure 2c and d) represent a minor challenge for the use of PPI in clinical trial design (Figure 2c), none of these issues are reported when PPI is used in the decision-making process (Figure 2d).
Discussion
Understanding and incorporating patients’ values, priorities, and trade-offs in healthcare decision-making, thus recognizing that truly effective personalized care goes beyond clinical outcomes, has become a crucial aspect of developing and evaluating medical products.5,7,9 However, data on the integration of PPI in clinical research and in the development of new treatments is lacking.
Here, by using data collected across various stakeholder groups, we observed that, while half of the respondents expressed an inclination to prioritize the integration of PPI in their future research projects, the overall current utilization rates are suboptimal, with 26% of respondents reporting that they never employ PPI, and an additional 44% doing so only occasionally. This is partially due to the inadequate availability of aggregated patient preference, with 65% of respondents reporting limited availability, and 17% indicating a complete lack of such data. Therefore, we advocate here for concerted efforts and investments to establish reliable data repositories, as 76% of participants expressed interest in using them, if provided.
Further challenges hinder the effective incorporation of PPI into healthcare delivery and product development, as already observed by previous literature.15,16,18 Respondents mentioned the lack of standardized data collection methodologies as one of the main problems. This highlights the need to enhance awareness regarding past and current efforts in data collection and standardization, such as the Patient-Centered Outcomes Research Institute’s (PCORI) methodology standards,19 and the IMI-PREFER project.5 IMI-PREFER, which was mentioned only by one of our respondents, developed a robust framework that outlines the methodology for conducting patient preference studies,20 including guidelines for study design,21,22 and stakeholder interaction.11 Two of its key aspects are the standardization of the methods used to collect and analyze PPI, including defining quantitative (e.g., discrete choice experiments, best-worst scaling, and conjoint analysis), and qualitative (e.g., in-depth interviews, focus groups, and Delphi method) techniques, and creating templates and guidelines for conducting studies in diverse disease areas.19,20
Respondents further reported limited patient engagement, difficulty in obtaining reliable preference data, and concerns regarding the potential introduction of bias as important challenges. This builds on stereotypes, with, for instance, many professionals perceiving patient preferences as subjective or less relevant compared to clinical data and scientific evidence.16 We believe that creating direct communication channels (e.g., round-table discussions, transparent reporting, feedback loops) between pharmaceutical companies and disease-specific patient advocacy groups and/or global patient networks, which already have strong connections and trust within the patient community, will challenge these stereotypes, and foster a more collaborative environment. Additionally, we believe that providing patients with educational materials about the relevance of their input in healthcare decision-making can further strengthen their willingness to participate actively in shaping research and regulatory priorities.
More worrisomely, about half of the respondents cited as a major obstacle the resistance to deviating from traditional practices. Shifting mindset is not trivial, and much effort will be needed. For instance, it has already been recognized that traditional evaluation methods prioritize quantitative data and economic metrics, especially when resources are limited, and financial considerations may overshadow the need for a patient-centered approach.18 We advocate here for regulatory bodies, such as the US Food and Drug Administration and the European Medicines Agency, to encourage industry stakeholders to adopt PPI systematically. For instance, they could allow expedited pathways, particularly in cases where patient preferences highlight unmet medical needs or shape clinically meaningful endpoints. Additionally, we believe that companies should establish dedicated roles, thus ensuring that patient preference data are appropriately collected, analyzed, and applied to decision-making. An increasing exposure to best practices will contribute to a cultural shift, encouraging a more receptive and informed approach.
Despite these challenges, about 90% of the respondents expressed at least a mild inclination to prioritize integrating patient preference information in their future research or decision-making processes. This positive outlook reflects a growing recognition of the potential benefits of adopting a more patient-centric approach in future research or decision-making processes.
While our survey was grounded in the existing literature on patient preference studies, it is important to note that we did not perform any formal validation and/or reliability testing. Additionally, our findings may have underlying bias due to the relatively small sample size, and the use of a snowball sampling strategy. However, such a number of respondents is not uncommon, with other similar studies on multiple stakeholders involving between 12 and 143 individuals.12,15,23 Finally, we did not collect any demographic information, further limiting the generalizability of our findings. Further research involving larger and more diverse populations is necessary to validate and generalize our findings.
Conclusion
Our study provides a much-needed overview of the current use of PPI in clinical research and decision-making processes in a sample of 46 respondents encompassing researchers, healthcare professionals, statisticians, quality assurance, policy or decision analysts, pharmacovigilance experts, consultants, and a patient advocate.
We observed that, while the adoption of PPI remains limited, there is a growing recognition of its potential benefits and increasing interest in integrating it into future processes, despite existing challenges and disparities in the utilization rates across organizations and stakeholder groups. Concerted efforts are, however, needed to overcome identified challenges, such as resistance to change, limited patient participation, lack of standardization and the availability of high-quality data. A patient-centered approach is essential for promoting a more effective, equitable and patient-focused healthcare system.
Data Sharing Statement
Data collected during the study are available to bona fide researchers under managed access due to governance constraints and can be requested from the corresponding author.
Ethical Review Board Statement
We confirm that the procedures comply with national and EU legislation. Research was performed in accordance with the Declaration of Helsinki. The Ethics Committee of the University of Turin (Comitato di Bioetica d’Ateneo) waived ethical approval as well as the need to obtain informed consent for this work (Protocol number: 0722874) since we used data that were anonymized before the analysis, and did not collect any sensitive information. By returning a completed questionnaire, respondents consented to be included in the study.
Author Contributions
All authors made a significant contribution to the work reported. Specifically, MdB, IB, and PB contributed in the conception, MdB, CF, IB, and PB in the study design, MdB, CF, IB, and PB in the execution, MdB, CF, IB, and PB in the acquisition of data, MdB, ZB, MB, AV, and PB in the analysis and interpretation. MdB, AV, and PB drafted the manuscript. All authors took part in revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by “NODES Spoke 5 project” no ECS00000036, which has received funding from MUR-M4C2 1.5 of PNRR (code BERP_PNRR_EI_23_01_F). This work was partially supported by the “Proof of Value Instrument 2022 Initiative” (S1921_POV_D218) funded by Compagnia San Paolo and University of Turin.
Disclosure
The authors declare no competing interests. This manuscript has been uploaded to medRxiv as a preprint: https://www.medrxiv.org/content/10.1101/2024.12.25.24319624v2.
References
1. Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017;19:e367. doi:10.2196/jmir.8775
2. Coulter A. Measuring what matters to patients. BMJ. 2017;356:j816. doi:10.1136/bmj.j816
3. Bombard Y, Baker GR, Orlando E, et al. Engaging patients to improve quality of care: a systematic review. Implement Sci IS. 2018;13:98 doi:10.1186/s13012-018-0784-z
4. US Food and Drug Administration. Patient preference information - voluntary submission, review in premarket approval applications, humanitarian device exemption applications, and De Novo requests, and inclusion in decision summaries and device labeling; 2016. Available from: https://www.federalregister.gov/d/2016-20221.
5. Smith IP, DiSantostefano RL, de Bekker-Grob EW, et al. Methodological priorities for patient preferences research: stakeholder input to the PREFER public–private project. Patient - Patient-Centered Outcomes Res. 2021;14:449–453 doi:10.1007/s40271-021-00502-6
6. Losi S, Berra CCF, Fornengo R, et al. The role of patient preferences in adherence to treatment in chronic disease: a narrative review. Drug Target Insights. 2021;15:13–20. doi:10.33393/dti.2021.2342
7. Pauker SG, McNeil BJ. Impact of patient preferences on the selection of therapy. J Chronic Dis. 1981;34:77–86. doi:10.1016/0021-9681(81)90053-9
8. Teisberg E, Wallace S, O’Hara S. Defining and implementing value-based health care: a strategic framework. Acad Med J Assoc Am Med Coll. 2020;95:682–685. doi:10.1097/ACM.0000000000003122
9. Levitan B, Getz K, Eisenstein EL, et al. Assessing the financial value of patient engagement: a quantitative approach from CTTI’s patient groups and clinical trials project. Ther Innov Regul Sci. 2018;52:220–229. doi:10.1177/2168479017716715
10. Janssens R, Barbier L, Muller M, et al. How can patient preferences be used and communicated in the regulatory evaluation of medicinal products? Findings and recommendations from IMI PREFER and call to action. Front Pharmacol. 2023;14:1192770. doi:10.3389/fphar.2023.1192770
11. Hiligsmann M, Liden B, Beaudart C, et al. HTA community perspectives on the use of patient preference information: lessons learned from a survey with members of HTA bodies. Int J Technol Assess Health Care. 2024;40:e17. doi:10.1017/S0266462324000138
12. Whichello C, Bywall KS, Mauer J, et al. An overview of critical decision-points in the medical product lifecycle: where to include patient preference information in the decision-making process? Health Policy. 2020;124:1325–1332. doi:10.1016/j.healthpol.2020.07.007
13. Van Overbeeke E, Vanbinst I, Jimenez-Moreno AC, Huys I. Patient centricity in patient preference studies: the patient perspective. Front Med. 2020;7:93. doi:10.3389/fmed.2020.00093
14. Zhang L, Li D, Li X, Yan J. Patient preferences for generic substitution policies: a discrete choice experiment in China. Front Pharmacol. 2024;15:1400156. doi:10.3389/fphar.2024.1400156
15. Janssens R, Russo S, van Overbeeke E, et al. Patient preferences in the medical product life cycle: what do stakeholders think? Semi-structured qualitative interviews in Europe and the USA. Patient - Patient-Centered Outcomes Res. 2019;12:513–526. doi:10.1007/s40271-019-00367-w
16. Janssens R, Huys I, van Overbeeke E, et al. Opportunities and challenges for the inclusion of patient preferences in the medical product life cycle: a systematic review. BMC Med Inf Decis Mak. 2019;19:189. doi:10.1186/s12911-019-0875-z
17. Abdelazeem B, Hamdallah A, Rizk MA, et al. Does usage of monetary incentive impact the involvement in surveys? A systematic review and meta-analysis of 46 randomized controlled trials. PLoS One. 2023;18:e0279128. doi:10.1371/journal.pone.0279128
18. Huls SPI, Whichello CL, van Exel J, Uyl-de Groot CA, de Bekker-Grob EW. What is next for patient preferences in health technology assessment? A systematic review of the challenges. Value Health J Int Soc PharmacoEcon Outcomes Res. 2019;22:1318–1328. doi:10.1016/j.jval.2019.04.1930
19. Gaglio B, Henton M, Barbeau A, et al. Methodological standards for qualitative and mixed methods patient centered outcomes research. BMJ. 2020:m4435. doi:10.1136/bmj.m4435
20. Soekhai V, Whichello C, Levitan B, et al. Methods for exploring and eliciting patient preferences in the medical product lifecycle: a literature review. Drug Discov Today. 2019;24:1324–1331. doi:10.1016/j.drudis.2019.05.001
21. Whichello C, Levitan B, Juhaeri J, et al. Appraising patient preference methods for decision-making in the medical product lifecycle: an empirical comparison. BMC Med Inf Decis Mak. 2020;20:114. doi:10.1186/s12911-020-01142-w
22. Veldwijk J, de Bekker-Grob E, Juhaeri J, et al. Suitability of preference methods across the medical product lifecycle: a multicriteria decision analysis. Value Health. 2023;26:579–588. doi:10.1016/j.jval.2022.11.019
23. Lansdaal D, Van Nassau F, Van Der Steen M, Bruijne MD, Smeulers M. Lessons learned on the experienced facilitators and barriers of implementing a tailored VBHC model in a Dutch university hospital from a perspective of physicians and nurses. BMJ Open. 2022;12:e051764. doi:10.1136/bmjopen-2021-051764
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.