Back to Journals » Patient Preference and Adherence » Volume 16
Exploring Parent’s Satisfaction and the Effectiveness of Preformed Metal Crowns Fitting by Hall Technique for Carious Primary Molars in Jeddah Region, Saudi Arabia: Findings of a Prospective Cohort Study
Authors Almaghrabi MA ![]() , Albadawi EA, Dahlan MA, Aljohani HR, Ahmed NM, Showlag RA
, Albadawi EA, Dahlan MA, Aljohani HR, Ahmed NM, Showlag RA
Received 14 April 2022
Accepted for publication 25 August 2022
Published 8 September 2022 Volume 2022:16 Pages 2497—2507
DOI https://doi.org/10.2147/PPA.S370159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Manal A Almaghrabi, Emad A Albadawi, Mohammad A Dahlan, Hanan R Aljohani, Neveen M Ahmed, Riham A Showlag
Pediatric Dental Department, Specialty Dental Center, Ministry of Health, Jeddah, Saudi Arabia
Correspondence: Manal A Almaghrabi, Pediatric Dental Department, Specialty Dental Center, Ministry of Health, J56+49R, King Fahd Br Rd, An Nuzhah, Jeddah 23532, Saudi Arabia, Tel +699503002376, Fax +966 126205570, Email [email protected]
Purpose: The Hall technique (HT) is a non-invasive approach to treating carious primary teeth. Its acceptability by parents and effectiveness is not widely known in the Middle East. Therefore, we aimed to conduct this study to explore the effectiveness of preformed metal crowns (PMCs) fitting by HT and to what extent the parent’s satisfaction for their children in Jeddah region.
Materials and Methods: A prospective cohort study was conducted in the outpatient pediatric dental clinic at Jeddah Specialty Dental Center, in 2018. The cohort of children was exposed to the HT and was recalled 3 months to two years later to examine present or absence of: crown loss, open margin, signs or symptoms of reversible or irreversible pulpitis, and if the tooth exfoliated naturally. Parents who agreed to undergo the HT for their children completed a 5-point Likert questionnaire after treatment and after three months.
Results: A total of 48 children (72 teeth) were initially enrolled, but only 25 children (49 teeth) completed two years of follow-up. At 2 years follow-up, one PMC was lost (2.04%) while no teeth fitted with the HT required any further intervention. Around 96% of parents were satisfied with this procedure and 92% wanted other carious teeth to be treated similarly. All parents were satisfied with this technique because it did not include local anesthesia and no drilling. It was found that parents of girls were satisfied more than parents of boys and on average their satisfaction score at the time of treatment was 3.04 units higher than parents of boys with a significant p-value of 0.02 and 95% CI for the beta coefficient to be 0.46 to 5.62.
Conclusion: The HT is effective as a treatment of dental caries and it was generally accepted by parents initially and during their follow-up visits.
Keywords: Hall technique, dental caries, parent’s satisfaction, Saudi Arabia
Introduction
Dental caries, a neglected and serious global concern, is the most common chronic condition affecting dental health in children worldwide.1,2 There are significant consequences to tooth loss in terms of chewing, talking, and socializing with other children.3 There are several non-invasive treatment approaches for dental caries, such as fluoride application, oral hygiene, and diet management, but these non-invasive approaches are dependent on children’s compliance. Therefore, these approaches may not be found to be effective in the long term.3,4 Traditionally, infected dental tissues were surgically removed, followed by a different type of restorable material used for the same purpose.5 The majority of methods for treating carious primary molars in children include traditional tooth preparation and restoration with amalgam, composite, glass ionomer, and stain steel crown (SSC).1 However, such methods have some potential drawbacks, such as the destruction of a significant amount of surrounding tissue in order to gain access to dental caries. Another difficulty in restoring teeth in pediatric patients is patient cooperation, which is required for successful outcomes.6
To address these issues, the Hall technique is a long-lasting method of treating dental caries. Over the last decade, it has been regarded as a breakthrough in pediatric dentistry research,7 and it is now highly used in developed countries such as the UK, USA, and Germany.8–10 The HT is one of the methods used nowadays for sealing caries in primary molars.7–10 The HT has been advocated as a less invasive biological approach using PMCs to restore carious teeth.11 A Hall technique is one in which the tooth has not been prepared and caries has been sealed in, and it is used on primary molars as an alternative to conventional restoration.12 Dr. Hall, a general dental practitioner (GDP) in Scotland, developed this technique in 2006 to allow the use of preformed metal crowns without the need for tooth preparation or local anesthesia.13
The HT has very simple biological principles, such as opposing microorganisms from their source of dietary nutrition, which can prevent caries progression. This allows the dental pulp to regenerate reparative dentin.13 Because the HT does not necessitate carious excavation, teeth with clinical suspicion of pulpal involvement should be avoided. For the patient, HT can be used to improve patient cooperation and assist clinicians in reducing patient anxiety. In general, regardless of the technique used or the type of study conducted, PMCs have demonstrated high success rates.14 Although this technique has been used in various parts of the world, it is not widely accepted by parents. Unremoved caries was a common concern expressed by parents or legal guardians in clinical practice about HT. Before promoting this technique to a larger pediatric population, it is critical to understand how parents perceive this technique and how satisfied they are with the procedure. Few studies have been conducted in developed countries to investigate how satisfied parents are with this technique. Because the context of one country may differ from that of another, it is critical to assess parental satisfaction in countries such as Saudi Arabia.
Materials and Methods
A prospective cohort study was carried out in a pediatric dental department outpatient clinic at Jeddah Specialty Dental Center in Saudi Arabia. The study began in 2018, and the children were followed for two years after PMCs were implanted using the HT. The children were exposed to the Hall technique and were tracked over time.
The eligibility criteria of the potential children were contingent on general health classified as ASA I or ASA II, placement of PMCs using the conventional technique was not feasible due to lack of cooperative behaviors, Symptomless teeth that had occlusal or/and proximal caries lesions limited to dentine, and no clinical signs and symptoms of pulpal pathology. Uncooperative children, children with caries involving more than two surfaces with no sound tooth structure left to retain the crown, irreversible pulpal pathology or abscess, history of spontaneous pain, and teeth with mobility were excluded from the study. Since the same children could not tolerate pre-operatively X-ray (bitewing) due to uncooperative behavior, the clinician had to visually judge the depth and extension of the caries lesion to decide if the teeth fit the inclusion criteria of this study.
Hall Technique Procedure
A pediatric dentistry consultant or specialist performed the procedure. A spoon excavator or low-speed handpiece was used to remove obvious food debris and/or gross caries from the cavity. The gauze was placed behind the tooth while the child was in a semi-sitting position to reduce the possibility of non-fitting PMC being swallowed or aspirated. The correct size PMC was partially fitted by hand, giving the impression of “spring-back” when placed up and past the contact point, ensuring that the PMC covered all cusps and mesial and distal marginal ridges of the primary teeth. When proximal contacts were extremely tight, interproximal slicing from the mesial and distal surfaces was performed with a pointed taper diamond bur. Glass ionomer luting cement was used to secure the PMC. The child was told to bite down on the PMC firmly until the crown was pushed down over the tooth. If the child was unable to bite down on the PMC, the crown was seated using finger pressure or a band pusher.
Data Collection
Following the procedure, the parents/legal guardians were given a questionnaire to assess their satisfaction with the HT. Parents/legal guardians were asked to complete another set of questionnaires at the 3-month recall visit to assess their long-term satisfaction. Clinical examination of treated teeth was performed at three-month intervals to assess the presence or absence of crown loss, open margin, dental abscess, signs and symptoms of reversible or irreversible pulpitis, and if the tooth exfoliated naturally. Each tooth had its own set of data collection forms, including a 3-month and a 2-year follow-up form. A single trained examiner performed and recorded all clinical assessments. If the PMCs was in place with no clinical signs or symptoms of pulp pathology during the two-year follow-up period, the Hall technique was considered successful.
Parent Satisfaction Questionnaires
Parents who agreed to undergo the HT for their children completed a 5-point Likert (Strongly agree, agree, do not know, disagree, and strongly disagree) questionnaire comprised of 10 questions. A validated questionnaire was used in the current study that attempted to capture different domains of satisfaction. The questionnaire covered various constructs such as a proper explanation of the Hall technique, perception of pain, acceptance of the treatment by the patient, preference to use the Hall technique for other carious teeth, satisfaction with the Hall technique, and reason for preferring the Hall technique.
Throughout the treatment, the parent or legal guardian was present with their children. Each questionnaire was given to a different study participant. After three months, the parents were asked to complete a follow-up questionnaire consisting of eight items formulated on a 5-point Likert scale to determine if they are still satisfied with the treatment procedure and if their children experienced any pain or discomfort while eating or brushing their teeth. We also asked if they were concerned about unremoved caries and if they would return to repeat the procedure.
The questionnaire was translated into English for publication purposes using Behling and Law’s technique. The Ethics Committee of Medical Research and Studies Department, Directorate of Health Affairs in Jeddah, Ministry of Health, Saudi Arabia, granted ethical approval for the study, IRB approval number A01256. Parents/legal guardians were informed about the study’s procedure and purpose, and informed consent was obtained. All procedures were carried out in accordance with the institutional and national research committee’s ethical standards, as well as the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards.
Statistical Analysis
The Statistical Package for Social Sciences version 25 was used to analyze the data (SPSS; IBM Corporation, Armonk, NY, USA). The information was gathered and tabulated. The Chi-square test was used. If the P-value was less than 0.05, the difference was considered significant. Furthermore, using the Likert scale questions, a satisfaction score on a continuous scale was created at the time of treatment and follow-up. A higher satisfaction level was demonstrated by a higher score at both time points, and vice versa. An independent t-test was used to assess the difference in mean score, and F-statistics were also calculated. This was followed by doing a linear regression analysis to assess the predictors of the satisfaction score mainly the age and sex of the child. Both standardized and unstandardized beta coefficients were computed for the satisfaction scores and their respective 95% confidence intervals were also reported. The p-value of < 0.05 was considered statistically significant for all findings and mean differences.
Results
A total of 48 children (72 teeth) were initially enrolled, but only 25 children (49 teeth) complete two years of follow-up. Around 30.6% of the children were 5 years old, while only 2% were 10 years old (Figure 1). Around three fourth of the participants (73.5%) were girls and 26.5% were boys. The mean age of the participants was 5.34 ± 1.73 years with no significant difference between boys (mean = 5.54±2.26 years) and girls (mean = 5.28 ±1.52 years), P=0.705. There were no significant differences in the distribution between boys and girls for the studied teeth (Table 1).
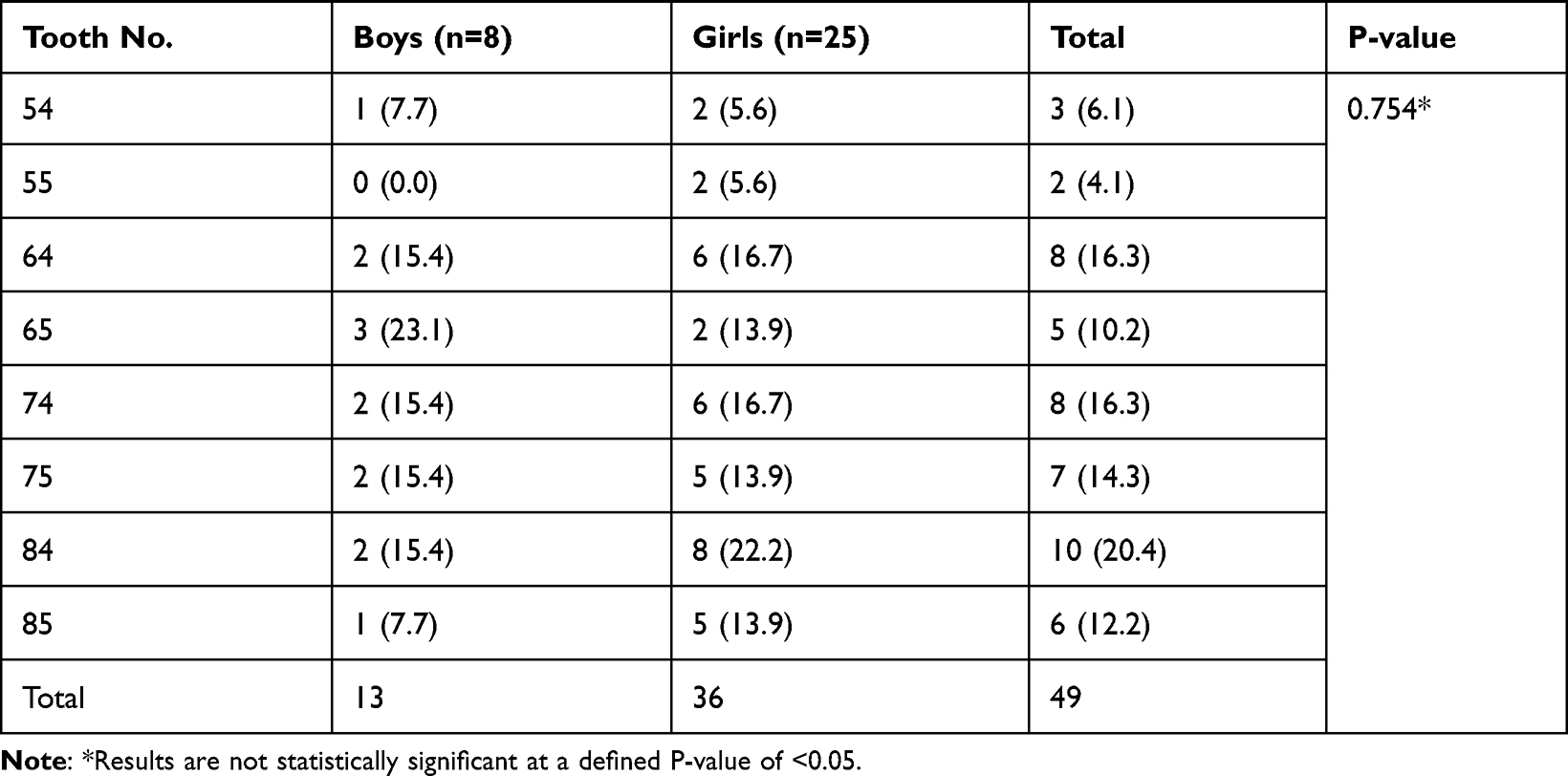 |
Table 1 Frequency and Percentages of Teeth Receiving Hall Technique Among the Study Sample |
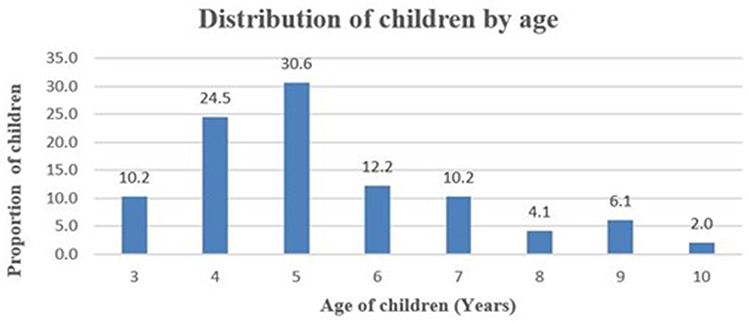 |
Figure 1 Distribution of study participants by age (in years). |
Table 2 shows the response of 25 parents/legal guardians to the questionnaires immediately post Hall technique. The study findings revealed no significant differences in the answers to specific questions by gender. Almost 62.5% of boys and 47.1% of the girls strongly agreed that there was no pain or discomfort during the procedure and 75% of boys and 64.5% strongly agreed while responding to whether they accepted the treatment or not. Also, 62.5% of the boys’ parents and 0.1% of the girls’ parents strongly agreed that their kids did not complain to them about their bites after treatment. Around 75% of boys’ parents and 58.8% strongly agreed that they were satisfied with this procedure and almost three-fourths of the girl’s and boys’ parents strongly agreed that they wanted other carious teeth to be treated similarly. All parents of boys showed strong agreement to be satisfied with this technique because it did not include local anesthesia using a syringe and no drilling. Whereas, 75.5% of boys’ parents and 52.9% of girls’ parents strongly agreed that they were satisfied with the technique because this technique avoided general anesthesia.
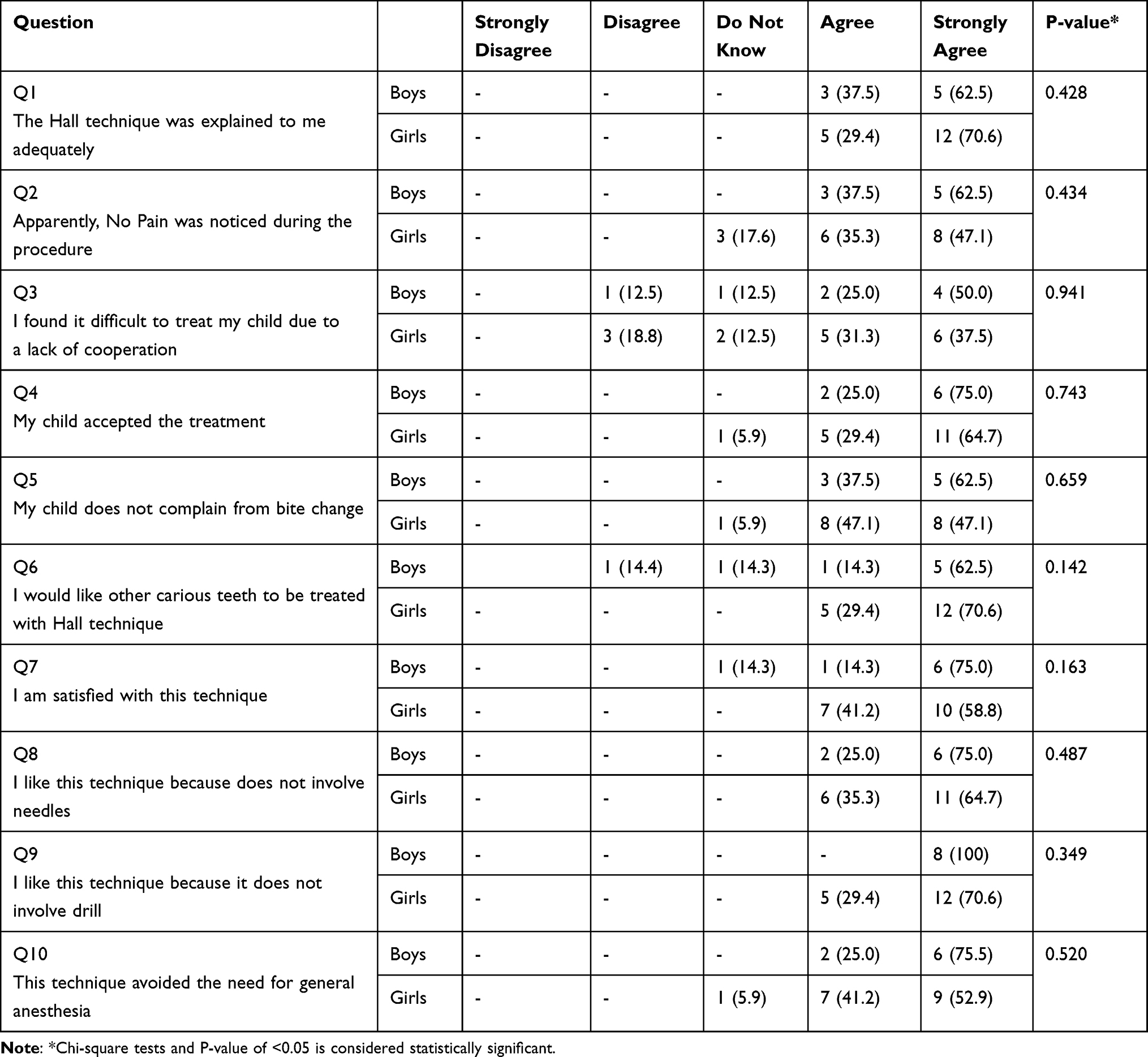 |
Table 2 Responses of the Parents to the Questionnaires Immediately Post Hall Technique |
Table 3 shows the 25 parents’ responses during the follow-up visit after three months of follow-up. Almost three-fourths (75.0%) of the boy’s parents and 62.5% of the girl’s parents strongly agreed that they were satisfied with the procedure. However, 50.0% of the boys’ parents and 56.3% of the girl’s parents strongly agreed that their kids did not report any pain or discomfort. Further, 62.5% of the boys’ parents and 56.3% of the girl’s parents strongly agreed that no issues were reported during teeth brushing. During the follow-up appointment, 75% of the boys’ parents and 50% of the girl’s parents disagreed (both disagree and strongly disagreed) on complaining of bite change. Whereas, 62.5% of the boy’s parents and 50.0% of the girl’s parents strongly agreed that there was no discomfort in the Temporomandibular joint (TMJ) area. Almost one-third of the boy’s and girls’ parents strongly agreed that their kids’ appetite had improved. Around 50% of the boy’s and girls’ parents strongly agreed to get other carious teeth to be treated with this technique.
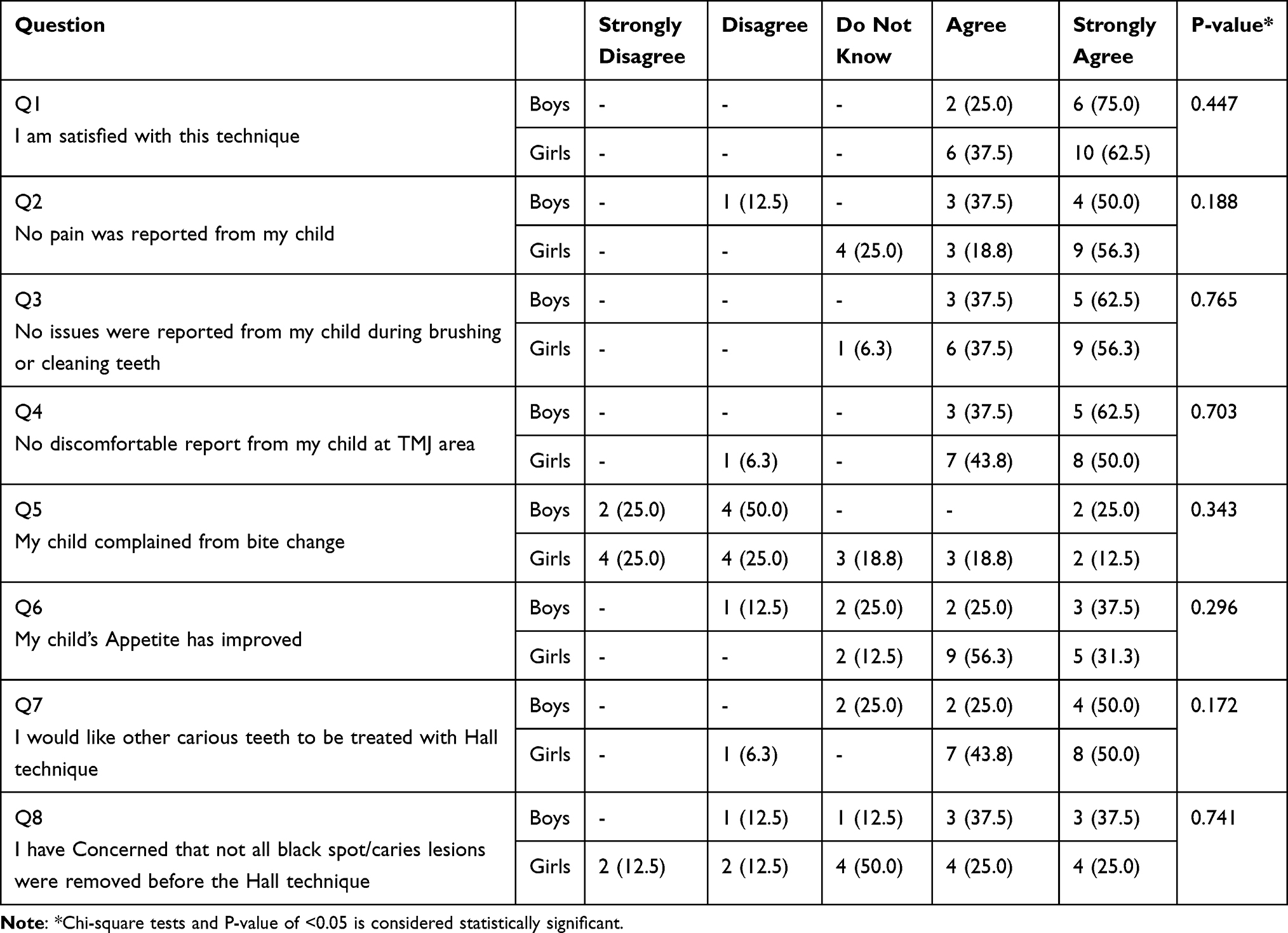 |
Table 3 Responses of the Parents to the Questionnaires 3-Month Post Hall Technique |
Table 4 describes the basic descriptive including mean and standard deviation for the satisfaction score at the time of treatment and follow-up. The mean satisfaction score at the time of treatment was higher (49) with a standard deviation (SD) of 4.077 than the mean score at the time of follow-up (40) with an SD of 5.98. The satisfaction score at the time of treatment ranges from 36 to 49 with a range of 13, whereas it ranged from 0 to 40 at the time of follow-up as shown in Table 4.
 |
Table 4 Descriptive Statistics for the Satisfaction Score at the Time of Treatment and Follow-Up |
Table 5 illustrates the differences in the mean satisfaction score at the time of treatment and follow-up by age and sex groups. The mean satisfaction score at the time of treatment for the parents of boy’s children was slightly lower (40.46) in comparison to the girls (43.33) with an SD of 4.25 and 3.78 respectively. This difference was found to be statistically significant with a p-value of 0.028 (95% CI: −5.42 to −0.32) (Table 5). Likewise, we found that the mean satisfaction score at the time of treatment for the parents of ≤ 5years older children was slightly lower (42.34) in comparison to the >5 years old children (43.33) with an SD of 4.52 and 3.16 respectively. However, this difference was not found to be statistically significant with a p-value of 0.597 (95% CI: 3.14 to 1.82). Similarly, for the satisfaction score at the time of follow-up, it was found that the mean satisfaction score at the time of follow-up for the parents of boys was slightly higher (33.38) in comparison to the girls (31.44) with an SD of 3.99 and 6.53 respectively. However, this difference was not found to be statistically significant with a p-value of 0. 322 (95% CI: −1.96 to 5.84). Similarly, the mean satisfaction score at the time of follow-up for the parents of ≤ 5years older children was slightly higher (32.50) in comparison to the >5 years old children (30.94) with an SD of 3.46 and 90.9 respectively. This difference in the mean score was not statistically significant with a p-value of 0.39 (95% CI: −2.06 and 5.18) as shown in Table 5.
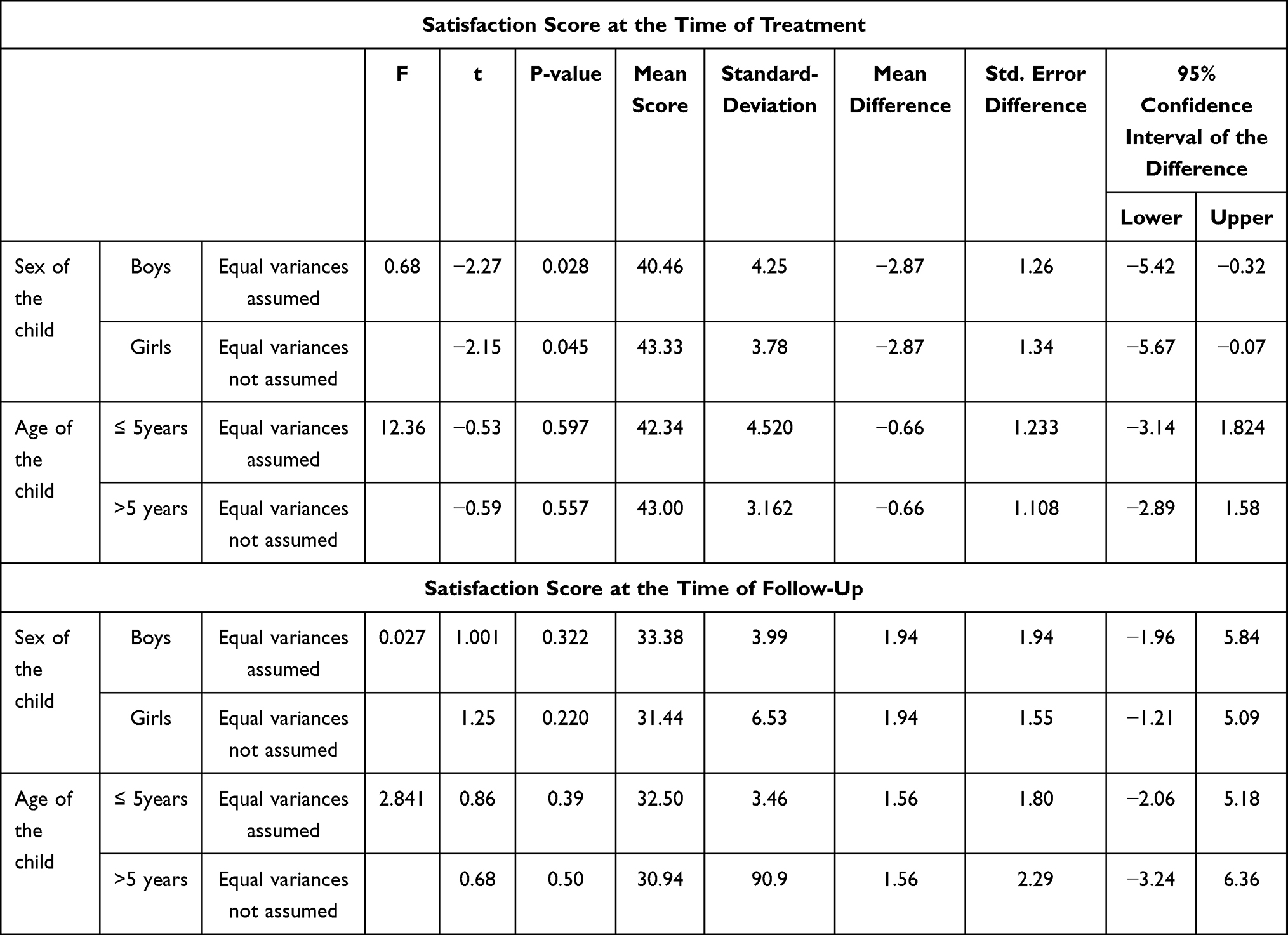 |
Table 5 Differences in the Mean Satisfaction Score at the Time of Treatment and Follow-Up by Age and Sex Groups |
Table 6 shows the findings of advanced regression analysis where we looked at the predictors of satisfaction scores at the time of treatment and follow-up. The results revealed that on average the satisfaction score at the time of treatment was 1.064 units higher for the parents of more than 5 years old children than parents of less than 5 years old children. However, these findings were statistically non-significant with a p-value of 0.37 (95% CI: −1.33 to 3.46). However, it was found that parents of girls were satisfied more than parents of boys and on average their satisfaction score at the time of treatment was 3.04 units higher than parents of boys with a significant p-value of 0.02 (95% CI: 0.46 to 5.62).
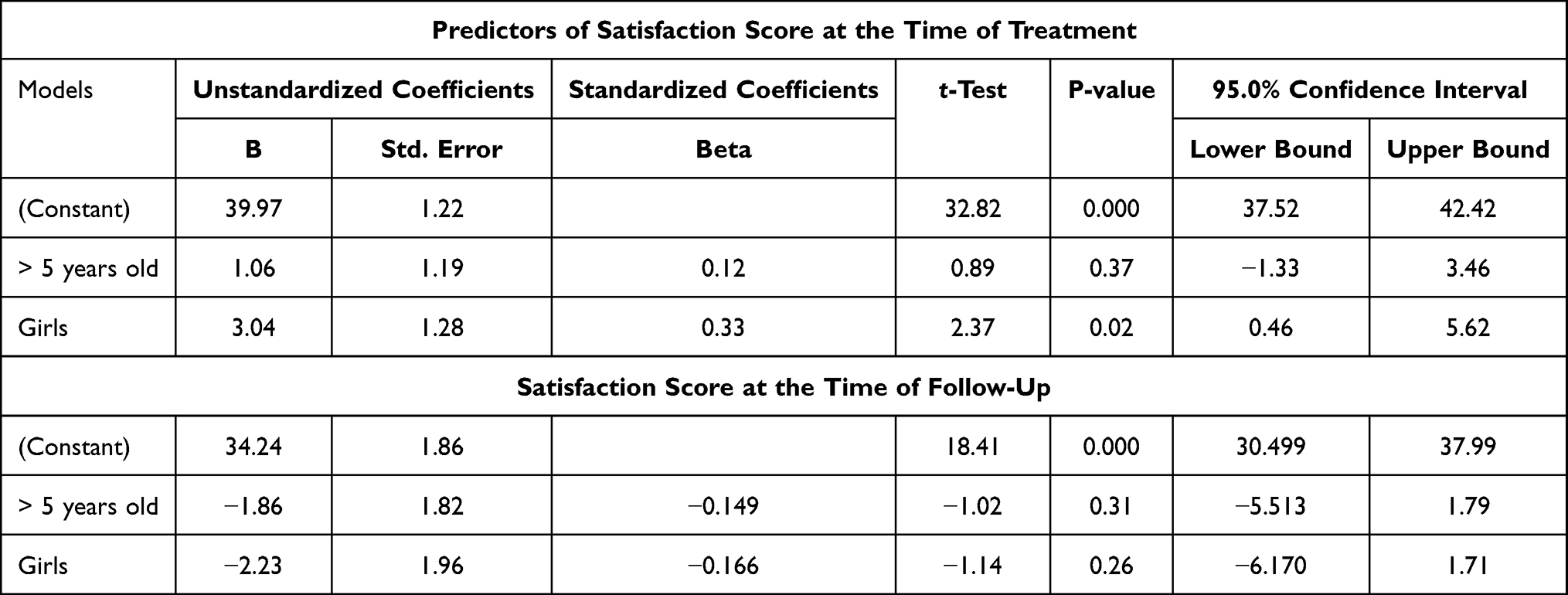 |
Table 6 Sex and Age of the Child as Predictors of Satisfaction Score at the Time of Treatment and Follow-Up |
In contrast, the results revealed that on average the satisfaction score at the time of follow-up was 1.86 units lower for the parents of more than 5 years old children than parents of less than 5 years old children. However, these findings were statistically non-significant with a p-value of 0.31 (95% CI: −5.51 to 1.79). Parents of girls were satisfied less than parents of boys and on average their satisfaction score at the time of treatment was 2.230 units lower than parents of boys with a significant p-value of 0.26 (95% CI: −6.170 to 1.71) as illustrated in Table 6.
Discussion
Due to behavioral limitations, dental practitioners treating early childhood caries (ECC) had few options for conventional restorative treatments in young children, which frequently required conscious sedation and general anesthesia. Newer materials and techniques have been introduced as a result of a paradigm shift in caries management. Biological methodologies are prioritized over the traditional drill and fill philosophy.14 “Although operative dentistry may be perfect, the appointment is a failure if a child departs in tears” this statement was eloquently put by McElroy (1895), emphasizing the importance of behavior management over technical excellence in Pediatric Dentistry.
We conducted this study to assess the effectiveness and satisfaction of parents with the Hall technique that their children were undergoing. We discovered that nearly 96% of the children accepted the treatment and that a similar proportion did not complain afterward. A nearly similar proportion of parents were found to be satisfied with this procedure, and nearly 100% were satisfied because it did not require anesthesia exposure. We discovered a significant difference in the mean satisfaction score at the time of treatment between parents of boys and parents of girls, with girls scoring slightly higher than boys. However, we did not find any difference by age. While investigating the age and gender of children as predictors of parental satisfaction, it was discovered that, unlike the gender of the child, the age of a child was not a predictor of the parent’s satisfaction score at the time of treatment. However, neither the child’s age nor gender were found to be predictors of the parent’s satisfaction score at the time of the follow-up.
It has been proven that the Hall Technique is well tolerated and accepted in children and has excellent outcomes compared with conventional caries management procedures. In our study, at 2 years follow-up, one PMC was lost (2.04%) while no teeth fitted with the HT required any further intervention. Similar results were reported by the authors in a study published in 2019,8 the majority of crowns were successful (92.3%; n = 167), and four presented at least one minor failure (2.2%; reversible pulpitis, crown loss, or secondary caries) and ten were major failures (5.5%; irreversible pulpitis or abscess).8
The Hall technique is being reviewed by multiple authors in randomized controlled trials. For example, there was an analysis done for 12 HT-treated and 4 control teeth with little to no carried observed on x-rays over time. Further, there was a lower mean hardness in HT-treated teeth than in controls.15 Similarly, another study conducted in India found that children are free of any signs and symptoms of mandibular joint dysfunction following this technique, and any changes in the occlusion are settled four weeks after employing the HT.16 Likewise, findings from one systematic review and meta-analysis showed that randomized controlled trials and quasi-experimental studies favored the HT in comparison to other approaches. to be favored as a treatment modality for dental caries than other conventional restorations.17 The results demonstrated that HT is 5 times more likely to be favored as a treatment modality for dental caries than other conventional restorations.17
Findings regarding the degree of acceptance are analogous to the findings from systematic reviews and meta-analyses. For example, a systematic review of 15 studies, published recently in 2021, showed that the rate of acceptance for the HT was 88.3%, 85.7%, and 81.8% among children, their parents, and dentists respectively.18 Another systematic review and meta-analysis, published in 2022 revealed similar findings regarding the acceptance of the HT among children and their parents.18 Likewise, a review of the literature, published in 2020, showed that the Hall technique is considered a promising choice with higher acceptability, longevity, and lower failure rate to manage carious primary molars when compared with other conventional treatment options used by the dentist practitioners in their clinical settings.1
The HT necessitates proper case selection and pulp status determination. A history, clinical examination, mechanical tests such as probing or blowing air, test cavity, percussion, and radiograph should be used to determine pulp status. In certain clinical circumstances, such as in our study, the same children could not cooperate and diagnostic images could not be obtained; thus, the clinician should consider caries extension and pulp vitality (vital or nonvital) when deciding on a treatment modality. A global perspective study show taking pre-HT radiographs was considered acceptable practic by 26% specialist paediatric dentist. .10
The global perspective pediatric dentist questionnaire shows that 17% believed the HT was substandard dentistry.10 In our study, 56% of parents were concerned that not all carious lesions were removed before crown cementation. Parents’ concern could be attributed to the fact that they started contemplating the procedure and expressed this in the follow-up survey. However, once we explained the biological concept, they all accepted the treatment. Twelve HT-treated primary molars and four controls were analyzed in the first study to provide chemical, ultrastructural, and mechanical property data on carious primary teeth treated with the Hall Technique purplish in 2020. Pre- and post-treatment X-rays revealed little to no caries progression over time, and Ca and P values were higher than previously reported for carious lesions in primary molars, implying that remineralization may have occurred in caries in HT-treated teeth.15
Since the Hall technique does not involve occlusal preparation, placing the preformed crown may cause an increase in the occlusal vertical dimension (OVD). In this study, 96% did not complain to their parent about their bite after treatment. During the follow-up appointment, fourteen (56%) of children complained to their parents about bite changes. when they asked if they still have bite changes, they respond “no, it was around the first week after treatment”. only one girl (4%) reported disconformable in the TMJ area. When we asked if she still felt that disconformable, she responds “no” and she provided an explanatory qualitative response “I had it only a few days then it disappears”. The change of occlusion and OVD following the placement of metal crown by HT was studied by the authors in 2020.16 As a secondary goal of the study, the questionnaire was distributed at the end of four weeks to assess the occurrence of TMD. All 44 children had a negative response for signs and symptoms of temporomandibular disorder TMD.16 According to the findings of a randomized controlled trial, the occlusion will balance by the next recall visit, and no patient demonstrated temporomandibular joint problem.14
Despite the growing evidence in favor of HT, a global survey from six continents found that while 92% had heard of it, only 50% had used it. According to a 2021 study on HT knowledge in Saudi Arabia, approximately 73.6% of specialists and 54.9% of graduates were aware of the technique.19 All the guidelines support the use of PMCs For primary molars with extensive multi-surface carious lesions with signs of reversible pulpitis and the clinician’s judgment is the key to success for this biological approach.20 Knowing the effectiveness and acceptability of HT by parents may encourage dental practitioners to use this technique confidently and optimize clinical outcomes in a variety of situations, such as in response to the COVID-19 outbreak, which required minimal aerosol-generating procedure (AGP), or when child cooperation compromised the conventional invasive approach to managing dental caries.
The HT was generally accepted by parents in this prospective cohort study, both initially and during their follow-up visit. Approximately 96% of parents were pleased with the procedure, and 92% desired that other carious teeth be treated similarly. All parents were pleased with this technique because it did not involve local anesthesia with a syringe or drilling, and 96% of parents thought it avoided general anesthesia. However, the Hall technique was widely accepted, and its effectiveness appears to be superior, as the failure rate was only 2% (one out of 49 teeth lost the SSC), with no other reported complications. Our findings are comparable to those of other studies conducted around the world. For instance, a study conducted in New Zealand observed 91% of parents acceptability for PMCs using HT in their children.21 Similarly, another study conducted by authors in Brazil also observed a similar result of 97% parent satisfaction with HT.12
According to the findings of the study, the high acceptance of HT provides clinicians with interesting treatment options to discuss with parents and children, and it may also motivate dental pediatric dental specialists, general practitioners, and students to practice HT with confidence.
Strengths and Limitations
This study on the acceptability of HT could be effort data that can be used to compare to other populations such as Europe, Asian countries, or African countries to deepen our understanding of perceptions of parents’ preferences for treatment. This was the first study of its kind in the Jeddah region that looked at parent satisfaction after HT. Furthermore, we used validated questionnaires that were similar to the questions used in a previous study. 20. However, one limitation is the small sample size, which resulted in less precise estimates. The sample size was reduced because the parent/contact guardian’s information had changed, making it difficult to track them down during the COVID-19 pandemic. Second, we lost children at follow-up and were unable to determine the level of acceptability of HT from 100% of the participants at the follow-up, which may have influenced our study findings. Third, unlike other studies in the literature, this study did not include controls; rather, all children were exposed to HT, making it difficult to draw any firm conclusions in the absence of a comparison group. Due to the observational nature of the study, we did not randomize the children; thus, our study findings may be skewed due to unmeasured confounding. As a result, more experimental studies will be needed in the future to gain a better understanding of the same phenomenon. Lastly, we conducted this study only in one region of Saudi Arabia, therefore, the findings may not be generalizable to other parts of Saudi Arabia.
Conclusion
This study was carried out to evaluate the efficacy and parental satisfaction with the HT that their children were undergoing. It was discovered that approximately 96% of parents were satisfied with this procedure, and 92% desired that other carious teeth be treated similarly. After treatment, 96% of patients did not complain to their parent or legal guardian about their bite. All parents were pleased with this technique because it did not involve local anesthesia with a syringe or drilling, and 96% of parents thought it avoided general anesthesia. Parents accepted the Hall technique initially and during their follow-up visit; however, 56% of parents expressed concern about the remaining carious lesion and staining in their children’s teeth. Before proposing this technique to be used widely, we would recommend conducting more robust experimental studies in a similar context to explore its acceptability in the other parts of Saudi Arabia.
Acknowledgments
The authors would like to thank dr. Khalid Zawawi and dr. Ghadah Malki for their valuable contribution and help.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Altoukhi DH, El-Housseiny AA. Hall technique for carious primary molars: a review of the literature. Dent J. 2020;8(1):11. doi:10.3390/dj8010011
2. Bernabé E, Marcenes W. Can minimal intervention dentistry help in tackling the global burden of untreated dental caries? Br Dent J. 2020;229(7):487–491. doi:10.1038/s41415-020-2155-9
3. Fejerskov O, Nyvad B, Kidd E. Dental Caries: The Disease and Its Clinical Management. John Wiley & Sons; 2015.
4. Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, Eden E. Minimal intervention dentistry for managing dental caries - a review: report of a FDI task group. Int Dent J. 2012;62(5):223–243. doi:10.1111/idj.12007
5. Vila Verde A, Ramos MM, Stoneham AM. Benefits in cost and reduced discomfort of new techniques of minimally invasive cavity treatment. J Dent Res. 2009;88(4):297–299. doi:10.1177/0022034509334157
6. Lygidakis N. Treatment modalities in children with teeth affected by molar-incisor enamel hypomineralisation (MIH): a systematic review. Eur Arch Paediatr Dent. 2010;11(2):65–74. doi:10.1007/BF03262715
7. Ghaith B, Hussein I. The Hall technique in paediatric dentistry: a review of the literature and an “All Hall”case report with a 24 month follow up. Stoma Edu J. 2017;4(3):208–217. doi:10.25241/stomaeduj.2017.4(3).art.6
8. Midani R, Splieth CH, Mustafa Ali M, Schmoeckel J, Mourad SM, Santamaria RM. Success rates of preformed metal crowns placed with the modified and standard hall technique in a paediatric dentistry setting. Int J Paediatr Dent. 2019;29(5):550–556. doi:10.1111/ipd.12495
9. Welbury RR. The Hall Technique 10 years on: its effect and influence. Br Dent J. 2017;222(6):421–422. doi:10.1038/sj.bdj.2017.262
10. Hussein I, Al Halabi M, Kowash M, et al. Use of the Hall technique by specialist paediatric dentists: a global perspective. Br Dent J. 2020;228(1):33–38. doi:10.1038/s41415-019-1100-2
11. Alkilzy M, Santamaria RM, Schmoeckel J, Splieth CH. Treatment of carious lesions using self-assembling peptides. Adv Dent Res. 2018;29(1):42–47. doi:10.1177/0022034517737025
12. Maciel R, Salvador D, Azoubel K, et al. The opinion of children and their parents about four different types of dental restorations in a public health service in Brazil. Eur Arch Paediatr Dent. 2017;18(1):25–29. doi:10.1007/s40368-016-0262-8
13. Innes N, Evans D, Hall N. The Hall Technique for managing carious primary molars. Dent Update. 2009;36(8):
14. Innes NP, Evans DJ, Stirrups DR. The Hall Technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007;7:18. doi:10.1186/1472-6831-7-18
15. Loch C, Jansen van Vuuren L, Duncan WJ, Boyd DH, Foster Page LA. Ultrastructure and properties of primary carious molars treated using the Hall Technique. Int J Paediatr Dent. 2021;31(3):290–298. doi:10.1111/ipd.12681
16. Joseph RM, Rao AP, Srikant N, Karuna YM, Nayak AP. Evaluation of changes in the occlusion and occlusal vertical dimension in children following the placement of preformed metal crowns using the Hall technique. J Clin Pediatr Dent. 2020;44(2):130–134. doi:10.17796/1053-4625-44.2.12
17. Badar SB, Tabassum S, Khan FR, Ghafoor R. Effectiveness of Hall technique for primary carious molars: a systematic review and meta-analysis. Int J Clin Pediatr Dent. 2019;12(5):445–452. doi:10.5005/jp-journals-10005-1666
18. Lin GSS, Cher CY, Cheah KK, et al. Acceptability of atraumatic restorative treatment and Hall technique among children, parents, and general dental practitioners: a systematic review and meta-analysis. Quintessence Int. 2021. doi:10.3290/j.qi.b912685
19. Ezzeldin T, Al-Awasi KA, Bader RM, et al. A Study to assess the awareness and use of silver diammine fluoride and Hall Technique among dental professionals and dental students in the Eastern Province. Saudi Dent J. 2021;33(8):1166–1173. doi:10.1016/j.sdentj.2021.01.005
20. Binladen H, Al Halabi M, Kowash M, Al Salami A, Khamis AH, Hussein I. A 24-month retrospective study of preformed metal crowns: the Hall technique versus the conventional preparation method. Eur Arch Paediatr Dent. 2021;22(1):67–75. doi:10.1007/s40368-020-00528-8
21. Page L, Boyd DH, Davidson SE, McKay SK, Thomson WM, Innes NP. Acceptability of the Hall technique to parents and children. N Z Dent J. 2014;110(1):12–17.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.