Back to Journals » Patient Preference and Adherence » Volume 9
Exploring older adults’ perceptions of a patient-centered education manual for hip fracture recovery: “everything in one place”
Authors Tsui K, Fleig L, Langford D, Guy P, MacDonald V, Ashe M
Received 6 April 2015
Accepted for publication 11 June 2015
Published 17 November 2015 Volume 2015:9 Pages 1637—1645
DOI https://doi.org/10.2147/PPA.S86148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Karen Tsui,1,2,* Lena Fleig,1,3,4,* Dolores P Langford,2,5 Pierre Guy,1,2,6 Valerie MacDonald,7,8 Maureen C Ashe1,3
1Centre for Hip Health and Mobility, The University of British Columbia, 2Vancouver Coastal Health, 3Department of Family Practice, The University of British Columbia, Vancouver, BC, Canada; 4Health Psychology, Freie Universität Berlin, Berlin, Germany; 5Department of Physical Therapy, The University of British Columbia, 6Department of Orthopaedics, 7School of Nursing, The University of British Columbia, Vancouver, 8Fraser Health Authority, Surrey, BC, Canada
*These authors contributed equally to this work
Purpose: To describe older adults’ perspectives on a new patient education manual for the recovery process after hip fracture.
Materials and methods: The Fracture Recovery for Seniors at Home (FReSH) Start manual is an evidence-based manual for older adults with fall-related hip fracture. The manual aims to support the transition from hospital to home by facilitating self-management of the recovery process. We enrolled 31 community-dwelling older adults with previous fall-related hip fracture and one family member. We collected data using a telephone-based questionnaire with eight five-point Likert items and four semi-structured open-ended questions to explore participants’ perceptions on the structure, content, and illustration of the manual. The questionnaire also asked participants to rate the overall utility (out of 10 points) and length of the manual. We used content analysis to describe main themes from responses to the open-ended interview questions.
Results: Participants’ ratings for structure, content, and illustrations ranged from 4 to 5 (agree to highly agree), and the median usefulness rating was 9 (10th percentile: 7, 90th percentile: 10). Main themes from the content analysis included: ease of use and presentation; health literacy; illustration utility; health care team delivery; general impression, information support from hospital to home; emotional and decision-making support; and the novelty of the manual.
Conclusion: The FReSH Start manual was perceived as comprehensive in content and acceptable for use with older adults post-fall-related hip fracture. Participants expressed a need for delivery and explanation of the manual by a health care team member.
Keywords: falls, patient education, health literacy, self-management, discharge planning
Introduction
Education is vital to enable patients to take an active role in their health care and recovery. Evidence suggests that interventions promoting health literacy also improve patient engagement, resulting in positive health outcomes as measured by health behavior, decreased use of health services, and health status.1 Health professionals often provide verbal education to patients; however, the addition of well-designed printed materials can supplement and reinforce this information to: maximize patients’ knowledge of their condition; support uptake and adherence to preventive health behaviors; and provide self-management tools for the recovery process.1,2 The creation of such evidence-based, printed patient education materials is a desired knowledge translation product for tailoring knowledge to the intended group.3
When developing new and tailored patient education materials, research evidence is ideally synthesized with perspectives and experience from end users, ie, patients, their families, and health care providers.3 Health literacy is fundamental to the application and comprehension of patient health education materials;4 as such, health care providers need to tailor health information for the unique needs and perspectives of the target population.5 Despite this, patient education materials are often created solely by health care professionals or researchers, without participation from consumers.6 Individuals who experience serious health events requiring hospitalization, such as hip fracture, can offer valuable insight to others undergoing the same experience based on their own recovery process.7 A participatory approach that involves iterative consultation and feedback on written health education materials from patients and their caregivers is thus essential to optimize information for informed decision making and successful knowledge translation: it is a cornerstone of patient-centered care.7 A recent meta-analysis, on quality improvement strategies involving coordination of care to reduce health care utilization, noted that patient education reduced hospital admissions by approximately 20%.8
In our previous work,9 older adults who experienced hip fracture and their family members, expressed the need to know more about the recovery process. This was the starting point for the development and implementation of a novel patient education manual. Fall-related hip fractures in older adults are traumatic life events that can catalyze functional decline. Over half of older adults do not regain their former level of mobility after fall-related hip fracture,10–13 and falls and their associated injuries are a predictor of admission to higher level care facilities such as nursing homes.14 The reasons why many patients do not regain their former mobility and functional levels are multifactorial,15 but a contributing factor may be that patients and/or caregivers are uncertain of how to maximize their post-acute hospital recovery process, particularly to prevent subsequent falls and hospital readmission.
Based on the initial requests for more information from older adults with hip fracture, we extended our previous qualitative work with older adults after hip fracture9 to develop, in consultation with clinical partners, a comprehensive manual (or roadmap) for the recovery process. In the present phase of our “knowledge-to-action cycle” (Figure 1), our goal was to invite community-dwelling older adults who experienced a previous hip fracture, and their family members, to evaluate a patient-centered education manual. We wanted to explore their overall perceptions of our manual; more specifically the content, structure, and pictures. A priori, we sought feedback on the acceptability (which we defined as the comments from participants identifying missing or inadequate information in the booklet) and utility (a subjective scoring of usefulness by participants) of our newly developed clinical tool.
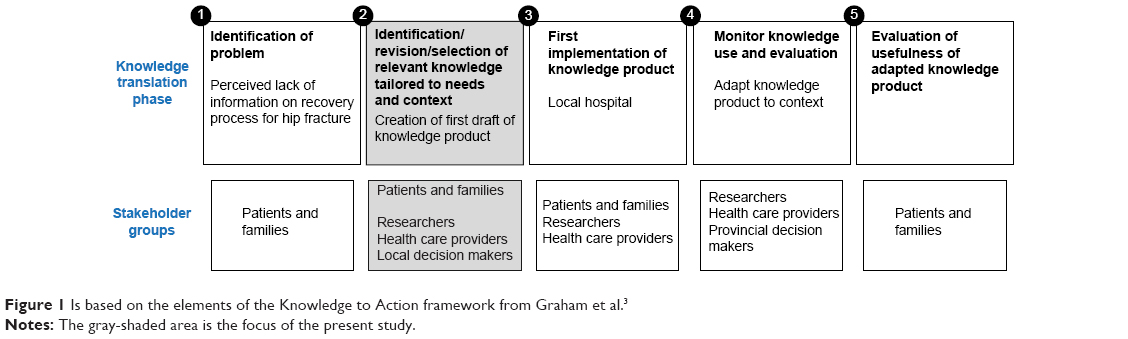 | Figure 1 Is based on the elements of the Knowledge to Action framework from Graham et al.3 |
Materials and methods
Design
We conducted telephone interviews with older adults, who had previously sustained a fall-related hip fracture, to evaluate the new manual designed to provide education about hip fracture recovery across the care continuum (from hospital to home). The manual and accompanying videos collectively make up the Fracture Recovery for Seniors at Home (FReSH) Start Toolkit, but in this phase, we requested feedback exclusively on the print manual component. All participants provided written informed consent to participate. This study was approved by the University of British Columbia and Vancouver Coastal Health Research Institute ethics review boards.
Sample
We contacted participants from a list of relevant individuals (older adults with hip fracture and/or family members involved in the care following hip fracture) who previously consented to communication about future research. We included community-dwelling adults aged 65 years or older who had previously sustained a fall-related hip fracture or who were a family member (with no age restrictions). We excluded older adults who had profound hearing loss which precluded telephone conversations and/or who were unable to converse or read in English.
Intervention: FReSH Start manual
The FReSH Start manual covers key milestones of hip fracture recovery across care transitions from hospital to home (please see the full pdf online version of the manual: FReSH Start manual http://www.hiphealth.ca/blog/FReSHStart). It was designed for delivery in hospital, immediately post-hip fracture repair surgery. The manual provides information on essential factors related to the recovery process. For example: what is a hip fracture and how is it repaired; what to expect in hospital; how to prepare for home; community resources; and specific instructions on mobility and exercises to decrease the risk of falls, etc. Certain sections in the manual are personalized to the patient, with individual information written by the health care team regarding the type of fracture and surgical procedure, postoperative weight-bearing status and hip precautions, space to write down equipment required, and checklists for discharge.
Specifically, the manual addresses core principles of Safer Health Care Now! (www.saferhealthcarenow.ca), and guides patients and their families to play an active role in preventing foreseeable risks, such as pneumonia, urinary tract infections, pain, and medication adverse events. This model, that provides communication tools and coaching for the transition period, reduced re-hospitalization rates in community-dwelling older adults; it encourages people to be active participants in their care.16 FReSH Start follows these principles to provide the patient/family with a navigation aid to identify and communicate their care needs across the continuum and request support and services from health care providers. It is grounded in Coleman et al’s care transitions model17 to promote a successful return home, and includes important information such as: identifying red flags, a personal patient health record, timely follow-up, safe medication use, and actions to take at home.
The toolkit was created following discussions from older adults involved in a randomized controlled trial18 who commented on the challenges experienced after hip fracture and the perceived lack of knowledge of the recovery process. This feedback prompted us to work with older adults and clinical partners to develop a toolkit to clarify the recovery process. The six key steps involved in the manual development included: 1) a qualitative study requesting information from older adults on their “words of wisdom” for recovery and perceptions on how to deliver educational materials;9 2) reviewing existing educational materials for older adults after hip fracture; 3) development of a draft manual based on the two previous steps; 4) three in-depth meetings with a provincial interdisciplinary health care team of expert orthopedic clinicians. There was representation from orthopedic surgery, physiotherapy, occupational therapy, nursing, and a patient representative. They reviewed the manual as a possible tool for inclusion in standardized clinical care pathways and to ensure consistency with best available evidence for falls prevention;19,20 5) evaluation of the revised manual with older adults (this current study); and 6) revision of the draft manual based on the feedback from the older adults.
Procedures
We mailed out an initial package to potential participants containing a letter of introduction and consent form. We followed up with a telephone call within 2 weeks, and asked individuals who agreed to participate to sign and mail back the consent form. Following receipt of the participant’s consent form, we mailed out a second package containing the FReSH Start manual and the questionnaire.
The questionnaire asked participants to rank the manual’s utility (usefulness) on a scale of 1 (not useful) to 10 (highly useful), and to choose whether they thought the manual length was: 1) too short; 2) just right; or 3) too long. We asked participants to locate a specific section in the manual to evaluate ease of navigation through the manual’s contents. The questionnaire also included eight five-point Likert items, and open-ended questions on: 1) structure and organization of the manual; 2) content; and 3) illustrations. The five-point Likert scale items were ranked from strongly disagree (1) to strongly agree (5). Each of the four open-ended questions included two to three probing questions, and provided space for the participant to write their response. The questions were: “1. Do you have any other comments regarding the structure and organization of the manual?” (Probing questions: “What would make the manual easier to read?” “How would you order the information?” “What would make the information easier to find?”); “2. Do you have any other comments regarding the content of the manual?” (Probing questions: “Was the information confusing in any way?” “Are there any parts or words that were hard to read or hard to understand?” “How could those parts be improved?”); “3. Do you have any other comments about the pictures?” (Probing questions: “Which pictures were not helpful?” “Which pictures are not clear?” “How can they be improved?”); and “4. Do you have any other comments or suggestions about the manual?”
We sent the questionnaire to participants in advance to give participants time to read the manual, to allow them to gauge the scope and length of the questions in the interview, and to provide the opportunity to reflect on responses prior to the telephone call. We also collected basic demographic information from participants, including their age, length of time since their hip fracture, and their highest education level obtained, categorized as primary school or some secondary school; completed secondary school; some trade/technical school, college, or university; completed trade/technical school, college, or university; or graduate level university.
A trained research assistant telephoned participants 1–2 weeks after their receipt of the information package. Each call lasted approximately 20 minutes, and the interviewer transcribed participants’ responses during the interview onto an identical questionnaire form.
Data analysis
All data were entered into a database by a trained research assistant, independent of the study. Once quantitative and qualitative data were entered, a different research assistant independent of the study confirmed data accuracy through comparison with the interview notes. We provided pseudonyms for all participants to maintain anonymity. We summarized demographic information using means (standard deviations). For each rating response, we calculated the median score with 10th and 90th percentiles.
Two authors (KT, LF) from different perspectives (physiotherapy and health psychology) conducted the content analysis to reduce the risk of bias. Each author independently read several times through the participants’ responses and annotated extracted items of interest. These points were then grouped into categories of similar information (subthemes) that were further consolidated into main themes. Following independent content analysis, these authors convened to compare their coding to assess analysis credibility and dependability (based on the similarity in their subthemes and main themes), and decided on a final list of main themes.
Results
Participant demographics
There were 32 participants (31 older adults with a prior hip fracture plus one family member) who enrolled in the study (Table 1). The average age of our participant group was 78 (SD 7.8) years, and ages ranged from 65 to 89 years. The majority (90%) of participants were women, and most participants had received postsecondary training or education, with 75% having completed trade school, college, or university. All participants but one reported a hip fracture, with a median time since fracture of 3 years. One participant reported being a caregiver, while another participant reported being a caregiver for an older adult with hip fracture and had also sustained a hip fracture.
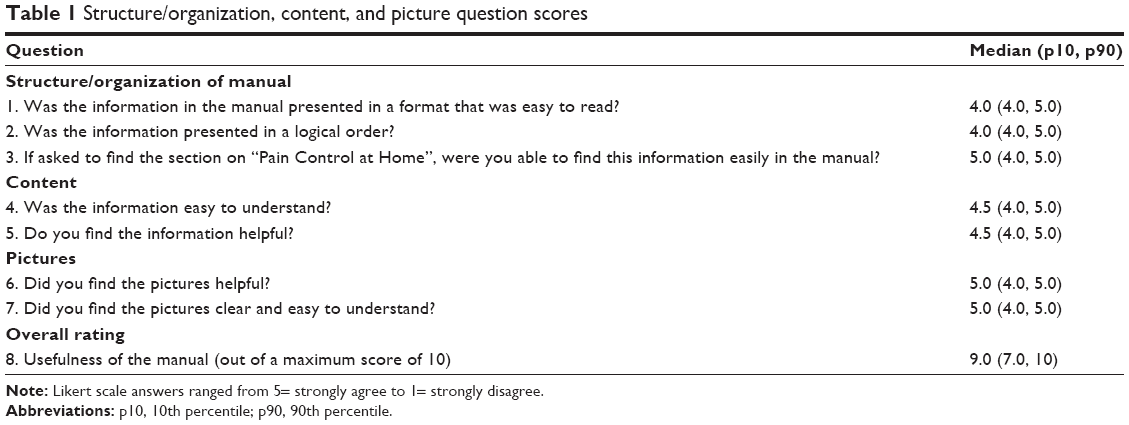 | Table 1 Structure/organization, content, and picture question scores |
Likert scale questions and usefulness rating
All participants chose “agree” or “strongly agree” to all questions, with no individual responses in the “disagree” or “strongly disagree” categories. As presented in Table 1, participants’ ratings across all three content domains were high. When participants were asked to find a section located in the middle of the manual, 30 out of 32 participants were able to find the correct page number without assistance. All 32 participants rated the utility of the manual as 7 or higher, and rated the length of the manual “just right”; however, two participants later noted that “some parts were a little long”.
Content analysis of open-ended questions
There was a high level of agreement between the two content analysts for their independent coding of the interview data. They identified nine main themes (Table 2) including: 1) general impression/attitude toward the manual. All participants spontaneously volunteered very positive impressions of the manual, including satisfaction with how complete, helpful, and useful the manual was as a resource; 2) ease of use/manual structure and presentation. This theme included: the convenience and compactness of information in the manual; text legibility (only one participant said the text could be rendered at a larger font but was still legible as is); appropriate length of the manual (all participants found the length “just right”); and format and presentation of the manual (several participants expressed satisfaction with the color and illustrations). Also included within this theme were comments regarding the ease of navigation for the manual; 3) health literacy. This theme included comments related to the manual’s use of medical terminology. A small number of medical terms were identified as difficult to understand by the layperson; 4) utility of illustrations. The illustrations in the manual garnered positive comments for their clarity, usefulness, and presentation. We received two insightful comments suggesting additions to clarify the movement planes in specific exercise illustrations, and three participants also suggested the addition of illustrations for equipment and how to navigate stairs; 5) health care team delivery of manual. Four participants independently made recommendations regarding the timing of delivery of the manual (soon after the operation) and how the health care team should review and personalize the information contained in the manual for each individual; 6) informational support for the patient from hospital to home. This theme summarized the completeness of information required for transitioning from the hospital back to the participant’s place of residence; participants offered additional practical tips to bridge the hospital-to-home gap; 7) emotional support/psychological reassurance. Participants conveyed the extent to which the manual was perceived as reassuring, and that it provided emotional support (to counter the uncertainty of the recovery process). Participants also reported that they perceived the booklet conveyed realistic expectations for recovery; 8) decision-making support. These were comments in which participants confirmed that the booklet contained information required to assist in their decisions regarding their postoperative care. Participants also made suggestions for areas where they would benefit from more detailed information for exercise and activity, medications, and pain; and 9) the novelty of the manual. Participants commented positively on the current manual compared with their previous experience with print materials (received during their hip fracture recovery).
 | Table 2 Main themes from participants’ comments about the manual |
The majority of responses were practical tips drawn from the participant’s own experience with their hip fracture and positive comments regarding the manual. Of particular interest, four participants indicated that they would like to have the health care team or a health care professional review the manual with them:
It would be helpful to have the healthcare team go over the booklet while in hospital [Nancy, 76 years]
A health care provider should highlight the areas important for each individual. [Sandra, 78 years]
In addition, three other participants indicated that involvement of the health care team around the tasks in the manual was essential; for example
The “before leaving the hospital” (discharge list) is very important, go over what the medications are for so you do not double up on things you are already taking! [Betty, 70 years]
Occupational therapy and physio was VERY helpful, so focus on this … they were really helpful and made me feel supported [Sophie, 79 years]
Discussion
In this study, we aimed to explore the perspectives regarding the FReSH Start patient education manual from older adults who previously experienced hip fracture. Overall, there was strong agreement by all participants that the manual was very useful, and every participant gave positive ratings for the structure, organization, and content of the manual. Many participants believed that the manual was easy and convenient to use; they provided some additional items to include in the manual such as how to use the stairs, which were included in the subsequent version of FReSH Start. In addition, participants expressed that they valued the manual as it gave them information as to what to expect for recovery timeline and milestones, which could alleviate anxiety surrounding the uncertainty after such an unexpected, traumatic event. Thus, the manual provided older adults with practical information (informational support) about the recovery process after hip fracture, and it had the potential to provide a source of emotional support by alleviating the psychological adjustment to the recovery process and their new status postfracture. Overall, the manual was summed up best by one participant who commented that the information was “everything in one place”.
Inadequate information can contribute to unsatisfactory post-discharge care21 and increase patient and caregiver anxiety.22 Our participants’ feedback regarding the emotional support from the FReSH Start manual extends previous findings that have similarly reported that the vulnerability of patients can be decreased with the provision of essential and realistic outcome information.23,24 Burton et al25 demonstrated that reassurance incorporated into a print manual for back pain alleviated fear-avoidance of activity. For older adults with hip fracture, decreased activity can inhibit functional recovery post-discharge due to the individual avoiding activity, secondary to a fear of falling.26 Optimism-promoting and reassuring wording is present in the FReSH Start manual; for example: “Think positively! You will become more comfortable and feel better with time”. Meeting the educational needs of patients and their families can also assist in decision making, thereby conferring some ability to regain autonomy, self-esteem, and control (namely, control beliefs) of an unexpected and challenging recovery.27
Poor health literacy is recognized as one of the greatest challenges to effective understanding and application of health education, and4 it is associated with worse health outcomes.28 In the FReSH Start manual, illustrations are provided to communicate important information. Illustrations linked to written text can greatly increase comprehension, retention, and recall of health information, particularly in individuals with low health literacy.29 For patients with low education levels, illustrations can also improve comprehension of hospital discharge information.30 Katz et al reported that by adding illustrations to written instructions, patient understanding and satisfaction with their medication instruction improved.31 Our participants were receptive to the illustrations; however, there was some incomprehension regarding the conveyance of dynamic movement with the exercise figures. Further, a small number of participants requested an explanation of some medical terms and an overall reduction in the number of words in the manual. Despite having illustrations accompany the medical terms, these words were still identified as confusing by some participants. This feedback from the patient perspective was essential to ensure that instructions and information are clear and facilitate understanding, especially for individuals with low health literacy.
Many participants mentioned their experience with pain and pain medications and suggested expansion of the information within the manual. Participants emphasized the need to encourage patients to report pain levels to the health care providers and to seek more information regarding pain medications. These comments supported the qualitative descriptions of experiences by patients with hip fracture documented by Archibald,32 who found the pain experience to be one of the four major themes which emerged.
Surprisingly, several participants independently identified a desire for health care professionals to be involved in the manual delivery. One participant noted that:
The health care provider should highlight the areas important for each individual [Joan, 78 years]
This mode of delivery is consistent with the literature; well-designed health information materials should be supplemented with health professional consultation and advice to improve health knowledge and recall.1 Print patient education materials in conjunction with verbal instruction improved knowledge and satisfaction for patients and caregivers compared with verbal delivery alone.6 Veronovici et al33 reported that individualized education was essential to the delivery of standardized education tools (such as the FReSH Start manual). More specifically, discharge plans (of which patient education constitutes a large component) that are individually tailored for patients can reduce length of stay and hospital readmissions for older adults.34 Our manual was purposely designed with sections of information tailored to patient needs and as a discharge and patient education resource for collaborative, multidisciplinary use by nursing, physiotherapy, and occupational therapy.
Patient characteristics, such as acceptance, motivation, and a positive attitude toward a new intervention, are important facilitators to effective implementation of a tool such as a patient education manual.35 If patients positively perceive a tailored intervention, this is likely to carry over to health care professionals’ implementation behaviors. That is, health care providers may feel more confident and motivated to fulfill their role in delivery of the intervention. Other barriers to patient self-efficacy with care and recovery can be overcome with problem solving by the delivering health care professional, and the manual facilitates patient participation and problem solving by providing writing space for goal setting, recovery timelines, discharge planning, and follow-up appointments.
The FReSH Start manual is unique because the need and development of the toolkit arose at the request of older adults who had previously navigated the hip fracture recovery process. Further, we worked in collaboration with older adults and health care professionals to provide information that was relevant and easy to follow. However, we appreciate that creating patient-centered material is only the beginning. As families and caregivers may have different informational needs, we suggest the manual requires additional evaluation across other populations, such as older adults in residential care. Our experience is that a participatory approach that engages all stakeholders in the creation and evaluation process ensures that these materials are patient centered, tailored to needs, and ultimately address knowledge gaps. Identifying key factors associated with effective implementation at the health care provider level is also required, and will inform successful delivery and uptake of a patient education manual, like FReSH Start.35 Including all stakeholders in this process increases the potential for behaviour change in patients as well as health professionals’ implementation practices, and knowledge uptake and utilization by patients. The FReSH Start manual is now currently being delivered in hospitals and the community by health care professionals (physiotherapists, occupational therapists, nurses) who are involved in the care of patients with hip fracture. There are future plans for an implementation study of the manual to determine health professionals’ perceived barriers and facilitators to toolkit delivery and studies to test if the manual can improve hip fracture outcomes.
Our participatory approach, combining quantitative ratings of utility with qualitative interviews, highlighted features of the FReSH Start manual that patients and their caregivers perceived as most helpful and valuable for coping with the recovery process; it also provided areas of improvement for the manual. However, we acknowledge limitations to our study. First, to improve precision of the qualitative component of this study, future interviews could be recorded and transcribed verbatim. Second, our questionnaire could be improved by the use of questions with a negative question stem to reduce positive bias. Third, our findings focused primarily on perspectives of individuals with a previous hip fracture, with only a single family member who volunteered for our study. Future studies should aim to further explore the perceptions and needs of a larger sample of family members and caregivers. Fourth, participants included in this study were English speaking, which limits the generalizability of our findings. However, following this study, the manual was translated into Punjabi and Simplified Chinese. In future, we will evaluate the manual within clinical practice to address utility and effectiveness across populations.
Conclusion
In this study, we noted that older adults who experienced a previous hip fracture perceived the FReSH Start manual as useful, convenient, comprehensive, and adequate to support the recovery process. Most patient education packages are created from the view of the health care professional; however, we propose that a more patient-centered approach to the creation of print patient education materials should includes user review and feedback to better meet the needs and concerns of specific populations. Our next knowledge translation phase involves testing: 1) the delivery mode for the manual to determine how it can be most effectively implemented into clinical practice; 2) the short- and long-term effects of the manual for people with low health literacy; and 3) other language versions (translations) of the manual to meet the needs of our culturally diverse community.
Key points for decision makers
- Patients and families from the target population should be involved in the process of creation and evaluation of patient education materials.
- Health care providers should be involved in the delivery and explanation of educational materials to maximize the potential learning opportunity.
Acknowledgments
We extend sincere thanks to our study participants for generously providing feedback on the manual. We also thank members of the BC Hip Fracture Redesign group for their contribution to the manual development. This work was supported by the Vancouver General Hospital and University of British Columbia Hospital Foundation (F14-00436), career award support for Dr Ashe from CIHR, and the Michael Smith Foundation for Health Research. Meetings of the BC Hip Fracture Redesign group were facilitated by a grant from the Doctors of BC and BC Ministry of Health Specialist Services Committee. The sponsors had no role in the study design, analysis, or preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Coulter A, Ellins J. Effectiveness of strategies for informing, educating, and involving patients. BMJ. 2007;335(7609):24–27. | ||
Hoffmann T, Worrall L. Designing effective written health education materials: considerations for health professionals. Disabil Rehabil. 2004;26(19):1166–1173. | ||
Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. | ||
Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259–267. | ||
Nilsen ES, Myrhaug HT, Johansen M, Oliver S, Oxman AD. Methods of consumer involvement in developing healthcare policy and research, clinical practice guidelines and patient information material. Cochrane Database Syst Rev. 2006;(3):CD004563. | ||
Johnson A, Sandford J, Tyndall J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home. Cochrane Database Syst Rev. 2003;(4):CD003716. | ||
Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Health Care. 2006;15(5):307–310. | ||
Tricco AC, Antony J, Ivers NM, et al. Effectiveness of quality improvement strategies for coordination of care to reduce use of health care services: a systematic review and meta-analysis. CMAJ. 2014;186(15):E568–E578. | ||
Schiller C, Franke T, Belle J, Sims-Gould J, Sale J, Ashe MC. Words of wisdom – patient perspectives to guide recovery for older adults after hip fracture: a qualitative study. Patient Prefer Adherence. 2015;9:57–64. | ||
Barnes B. Ambulation outcomes after hip fracture. Phys Ther. 1984;64(3):317–323. | ||
Koval KJ, Skovron ML, Aharonoff GB, Meadows SE, Zuckerman JD. Ambulatory ability after hip fracture. A prospective study in geriatric patients. Clin Orthop Relat Res. 1995;(310):150–159. | ||
Magaziner J, Hawkes W, Hebel JR, et al. Recovery from hip fracture in eight areas of function. J Gerontol A Biol Sci Med Sci. 2000;55(9):M498–M507. | ||
van Balen R, Steyerberg EW, Polder JJ, Ribbers TL, Habbema JD, Cools HJ. Hip fracture in elderly patients: outcomes for function, quality of life, and type of residence. Clin Orthop Relat Res. 2001;(390):232–243. | ||
Tinetti ME, Williams CS. Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337(18):1279–1284. | ||
Zuckerman JD. Hip fracture. N Engl J Med. 1996;334(23):1519–1525. | ||
Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141(7):533–536. | ||
Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828. | ||
Cook WL, Khan KM, Bech MH, et al. Post-discharge management following hip fracture – get you back to B4: a parallel group, randomized controlled trial study protocol. BMC Geriatr. 2011;11:30. | ||
Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;9:CD007146. | ||
Sherrington C, Tiedemann A, Fairhall N, Close JC, Lord SR. Exercise to prevent falls in older adults: an updated meta-analysis and best practice recommendations. N S W Public Health Bull. 2011;22(3–4):78–83. | ||
Tierney AJ, Worth A, Watson N. Meeting patients’ information needs before and after discharge from hospital. J Clin Nurs. 2000;9(6):859–860. | ||
Driscoll A. Managing post-discharge care at home: an analysis of patients’ and their carers’ perceptions of information received during their stay in hospital. J Adv Nurs. 2000;31(5):1165–1173. | ||
Bench SD, Day T, Griffiths P. Involving users in the development of effective critical care discharge information: a focus group study. Am J Crit Care. 2011;20(6):443–452. | ||
McKinley S, Nagy S, Stein-Parbury J, Bramwell M, Hudson J. Vulnerability and security in seriously ill patients in intensive care. Intensive Crit Care Nurs. 2002;18(1):27–36. | ||
Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care. Spine (Phila Pa 1976). 1999;24(23):2484–2491. | ||
Yardley L, Smith H. A prospective study of the relationship between feared consequences of falling and avoidance of activity in community-living older people. Gerontologist. 2002;42(1):17–23. | ||
Warner LM, Schüz B, Wurm S, Ziegelmann JP, Tesch-Römer C. Giving and taking – differential effects of providing, receiving and anticipating emotional support on quality of life in adults with multiple illnesses. J Health Psychol. 2010;15(5):660–670. | ||
Schillinger D, Grumbach K, Piette J, et al. Association of health literacy with diabetes outcomes. JAMA. 2002;288(4):475–482. | ||
Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173–190. | ||
Austin PE, Matlack R 2nd, Dunn KA, Kesler C, Brown CK. Discharge instructions: do illustrations help our patients understand them? Ann Emerg Med. 1995;25(3):317–320. | ||
Katz MG, Kripalani S, Weiss BD. Use of pictorial aids in medication instructions: a review of the literature. Am J Health Syst Pharm. 2006;63(23):2391–2397. | ||
Archibald G. Patients’ experiences of hip fracture. J Adv Nurs. 2003;44(4):385–392. | ||
Veronovici NR, Lasiuk GC, Rempel GR, Norris CM. Discharge education to promote self-management following cardiovascular surgery: an integrative review. Eur J Cardiovasc Nurs. 2014;13(1):22–31. | ||
Shepperd S, Lannin NA, Clemson LM, McCluskey A, Cameron ID, Barras SL. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2013;1:CD000313. | ||
Huijg JM, Gebhardt WA, Dusseldorp E, et al. Measuring determinants of implementation behavior: psychometric properties of a questionnaire based on the theoretical domains framework. Implement Sci. 2014;9:33. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.