Back to Journals » Nursing: Research and Reviews » Volume 12
Exploring Occupational Stress Among Intensive Care Units Nurses in Saudi Arabia Using the Health and Safety Executive Management Standards Indicator Tool
Received 20 August 2022
Accepted for publication 9 December 2022
Published 19 December 2022 Volume 2022:12 Pages 247—258
DOI https://doi.org/10.2147/NRR.S386670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Mohammed Ageel, Abdullah Shbeer
College of Medicine, Jazan University, Jazan, 45142, Saudi Arabia
Correspondence: Abdullah Shbeer, College of Medicine, Jazan University, Jazan, 45142, Saudi Arabia, Tel +966505769570, Email [email protected]
Background: Work in intensive care units (ICU) is associated with high levels of stress, which can result in reduced productivity and compromised health care quality, if not managed appropriately. The Health and Safety Executive (HSE) has developed the Management Standards Indicator Tool (IT) that includes the six HSE Management Standards; demands (workload, work patterns and environment), control (how much say a person has in the way they work), manager support (encouragement, sponsorship, resources provided by organization/line management) and peer support (encouragement and resources from colleagues), workplace relationships (promoting positive working to avoid conflict and deal with unacceptable behavior), roles (whether people understood their role), and change (how organizational change is managed). This study aimed to assess occupational stress and identify the major management standards indicators of organizational psychosocial hazard exposure among ICU nurses in public hospitals in Jazan, Saudi Arabia, using the HSE-IT for occupational stress.
Methods: The survey population included all full-time ICU nurses affiliated with the Jazan Region Health Administration. This study used a cross-sectional online survey based on the HSE-IT, which assesses the six HSE Management Standards representing potential stress hazards. The mean scores were interpreted in relation to the HSE benchmarks. It also included a qualitative component in the form of narrative comments regarding the most common sources of occupational stress and recommendations to reduce this stress. The data were analyzed to obtain descriptive and inferential statistics. The demographic variables examined for their association with the HSE-IT Standards.
Results: A total of 120 responses were collected from ICU nurses, with a response rate of 66%. The nurses were primarily female (53.3%) and aged between 25 and 34 years (60.0%). They had bachelor’s degrees (61.7%) and between 6 and 10 years of experience (55.0%). Most of them lived in urban settings (75.0%), were married (60.0%), and earned between 10,000 and 15,000 Saudi riyals per month (41.7%). In terms of weekly overtime, 66.7% of them did fewer than 5 hours. The results show that in relation to the HSE benchmarks, “good but needs improvement” was indicated in the change standard, “clear need for improvement” was indicated in the demands, peer support and relationships standards, “urgent action needed” was indicated in the control, manager support and roles standards. The qualitative data revealed that the most cited source of occupational stress was unsupportive management. Consequently, the most commonly proposed recommendation to reduce such stress was better management. The associations between sociodemographic characteristics, place of residence and overtime working hours, and the HSE Management Standards were commonly observed.
Conclusion: The findings of this study indicate that the risks associated with occupational stress for ICU nurses are not being optimally managed and that the standards are not being achieved. The study suggests that a psychologist-designed and -led staff stress management intervention should be adopted in ICUs, with regular evaluations being undertaken to track the implemented changes and identify any shortcomings.
Keywords: occupational stress, nursing practice, intensive care, nurses
Introduction
According to the United Kingdom National Institute for Occupational Safety and Health, occupational stress consists of “harmful physical and emotional responses which occur when job requirements do not match the capabilities, resources, or needs of the worker”.1 High levels of stress among intensive care workers have a negative impact on their health and productivity. Workplace anxiety, depression, and burnout have all been related to excessive stress (defined as emotional exhaustion, cynicism, and inefficacy).2,3 These issues might exacerbate the ongoing problem of frequent employee turnover in intensive care units (ICUs).4 Several studies have evaluated occupational stress among ICU staff and found that 33% and 31% and 29% of ICU nurses suffered burnout in France, Portugal and the United Kingdom, respectively.5,6 The United Kingdom Intensive Care Society has broadened its focus to promote workplace well-being as well as reduce occupational stress among ICU workers. Furthermore, critical care societies in the United States have recently called for measures to diminish the detrimental effects of occupational stress.7,8
Occupational stressors, including long hours, intense workloads, time constraints, difficult or complex tasks, and lack of breaks or variety, can all lead to health problems among ICU nurses. Moreover, interaction with patients, with their associated psychological, physical, and social problems, can potentially expose health care professionals to more stress than is endured by members of other professions.9 The impact of stress can also manifest as physical effects on the body, such as fatigue, changes in sex drive, upset stomach, and sleep problems, and/or as emotional effects, such as anxiety, restlessness, lack of motivation or focus, irritability, sadness, and depression.10
ICU nurses are frequently subjected to high demands to fulfill the duties assigned to them.11 Working in a field that involves complex multitasking, high workloads, and providing specialized care to critically ill and reliant patients can be overwhelming for nurses,12 especially during the coronavirus disease (COVID-19) pandemic. In addition, maintaining healthy lifestyle behaviors such as participating in regular physical activity, obtaining adequate sleep and engaging in social activities was disrupted by COVID-19. Reduced levels of physical activity during the COVID-19 pandemic have been extensively reported.13,14 Physical activity can lead to positive health benefits and can be considered as a stress management tool.15,16 Poor sleep quality and decreased sleep duration are associated with higher levels of perceived stress.13 Healthcare professionals, including ICU nurses, are considered to be a high-risk population for experiencing occupational stress.17,18 Several recent studies from different countries have reported an elevated risk of occupational stress due to the impact of the COVID-19.19–25
There is currently no single questionnaire that can assess all the risks associated with occupational stress.26 However, at an organizational level, a broad indication of how adequately management handles potential sources of occupational stress can help evaluate this problem. Therefore, the United Kingdom Health and Safety Executive (HSE) has developed the Management Standards Indicator Tool (IT), which consists of a 35-item questionnaire related to six primary stressors, to assess occupational stress. Based on the best available evidence linking work design to health outcomes, the HSE-IT was developed to indicate how well workers rate their organizations’ performance in managing the risks associated with occupational stress. The HSE identifies six management standards—demands, control, manager and peer support, workplace relationships, roles, and change—which represent potential stress hazards if optimal levels are not achieved.27
Despite the extensive research in this area, very little has been written on the factors causing stress among ICU nurses in Saudi Arabia. Interventions to prevent both the organizational and individual effects of occupational stress may only be implemented once the stressors in an occupational group have been identified, hence the need for the current study. Therefore, this study aimed to assess occupational stress among ICU nurses in Saudi Arabia using the HSE-IT and identify the major management standards indicators of organizational psychosocial hazard exposure in ICUs. The results of this study can provide baseline data to enable hospital management to benchmark their status based on established standards and may be useful for identifying HSE management standards that require improvement.
Methods
Study Design and Sampling
This convergent study design was conducted at public and private hospitals affiliated with the Jazan Region Health Administration in Saudi Arabia, between June 2021 and June 2022. The survey population included all full-time ICU nurses (n = 180). The questionnaire was distributed online to minimize costs and time requirements and maximize geographical coverage;28 it was developed using Qualtrics Research Core (Qualtrics, Provo, UT). The survey link was emailed to nurse supervisors, who were asked to forward it to the nurses in their teams. The sample size in this study included the whole population with a total of 180 invitations were sent to ICU nurses. This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Jazan University. Participant confidentiality was protected by deidentifying all responses.
Survey
The data were collected using a self-administered and structured questionnaire with quantitative (HSE-IT) and qualitative (narrative comments) components. The questionnaire items were in English language. The demographic data included gender, age, education, experience, place of residence, marital status, monthly income, and weekly overtime working hours. The HSE-IT consists of six standards (demands, control, manager and peer support, workplace relationships, roles, and change) representing potential stress hazards, which contain 35 close-ended questions rated on a 5-point Likert scale:29
- The first standard focuses on eight items used for assessing work demands (workload, work patterns, and the work environment).
- The second standard concentrates on six items related to work control and how much say the ICU nurses have in the way they do their work.
- The third standard is concerned with five items linked to manager support (encouragement, sponsorship, resources provided by the organization, and line management) and four elements associated with peer support.
- The fourth standard focuses on four items related to workplace relationships (eg, promotion of positive work to avoid conflict and dealing with unacceptable behavior).
- The fifth standard contains five items associated with the organization’s roles (eg, understanding roles and ensuring that roles do not conflict with each other).
- The sixth standard has three items linked to change (eg, management and communication of change).
Cronbach’s alpha was obtained for the six standards; work demands (0.801), work control (0.825), managers’ support (0.862), peer support (0.762), workplace relationship (C0.820), organizational roles (0.854), organizational change (0.829). The reliability of the survey was found to be consistent with what was obtained in similar studies in the literature (17–20).
The qualitative section of the survey was dedicated to narrative comments. It contained two questions regarding the three most common sources of occupational stress and the respondents’ recommendations to diminish stress in the ICU. Content analyses were conducted to develop exhaustive category sets of sources of occupational stress and recommendations to mitigate occupational stress. The responses to the two questions were counted based on matching categories to find frequencies.
The cover page of the survey included an introduction sheet that contained the study’s objective, duration, and the option to withdraw at any time, as well as privacy and confidentiality statements. The first page of the questionnaire included the consent form, which participants had to sign to access the survey.
Statistical Analyses
The Statistical Package for Social Sciences (SPSS) Version 27 (IBM Corp., Armonk, NY) was used for the statistical analyses. Descriptive statistics were calculated for the continuous variables (mean, standard deviation [SD]) and the categorical variables (n, %). Participant responses were aggregated and averaged to obtain the mean scores for each standard. A lower score indicates poor performance, or a potential problem area.29 The mean scores were interpreted in relation to the HSE benchmarks obtained from 136 organizations that have completed the survey as categorical thresholds (Table 1).29 The normality of distribution of the quantitative variables was evaluated using the Kolmogorov–Smirnov test. In addition, Mann–Whitney U and Kruskal–Wallis tests were conducted to compare the sociodemographic variables with the mean scores for each standard. Spearman’s rank correlation was used to measure the degree of association between the HSE management standards. A p-value of < 0.05 was adopted to determine the statistical significance.
 |
Table 1 Organizational Data Set - Rules Governing Color Coding Cut-Offs for Each Standard. |
Results
Sociodemographic Characteristics
A total of 120 responses were collected from ICU nurses, with a response rate of 66%. Table 2 shows the sociodemographic characteristics of the participants. The nurses were primarily female (53.3%) and aged between 25 and 34 years (60.0%). The majority had bachelor’s degrees (61.7%) and between 6 and 10 years of experience (55.0%). Most of them lived in urban settings (75.0%), were married (60.0%), and earned between 10,000 and 15,000 Saudi Arabian Riyal (SAR) per month (41.7%). In terms of weekly overtime, 66.7% of them did fewer than 5 hours.
 |
Table 2 Sociodemographic Characteristics |
Potential Stress Hazard Standards
Regarding the HSE management standards indicator tool, scores for each factor were calculated and benchmarked against 136 UK organizations is presented in Table 3. The results fall within color-coded percentile ranks requiring follow-up actions: urgent action (<20th percentile, red zone); clear need for improvement (20th–50th percentile, yellow zone); good, but need for improvement (50th–80th percentile, blue zone); or performance to be maintained (>80th percentile, green zone). In this study, “good but needs improvement” was indicated in change standard, “clear need for improvement” was indicated in demands, peer support and relationships standards, and “urgent action needed” was indicated in control, manager support and roles standards.
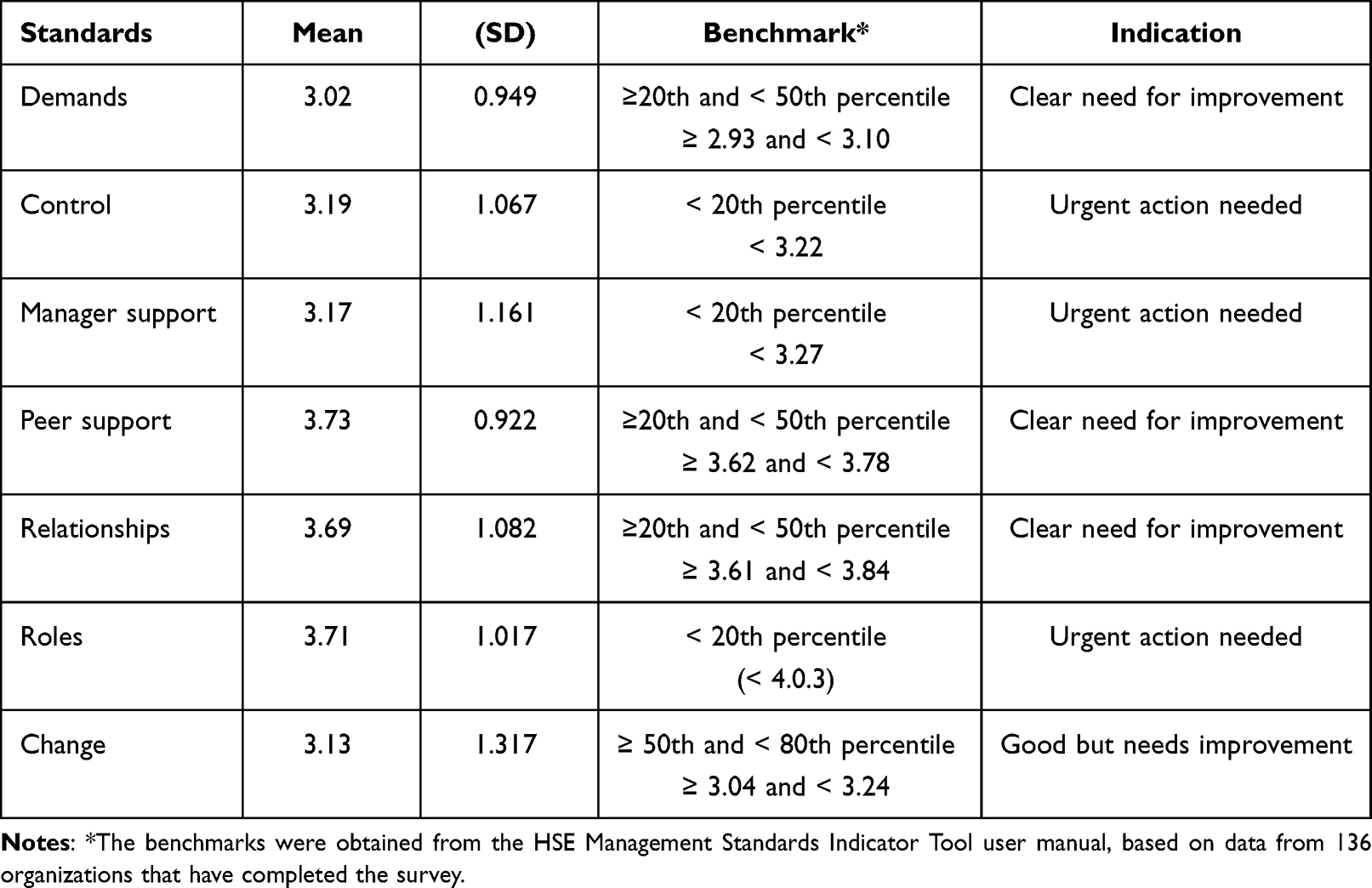 |
Table 3 Summary of the HSE Management Standards |
HSE Management Standards Based on Sociodemographic Characteristics
The mean scores for each standard based on sociodemographic characteristics are presented in Table 4. When the groups in each sociodemographic category were compared, variations in the mean scores of their HSE management standards were observed. A lower mean score indicates poor performance, which commonly was found in the place of residence (lower score for rural residents) and weekly overtime (lower score for >10 hrs) categories with statistically significant differences between ICU nurses for all HSE management standards, except demand and relationship standards. None of the sociodemographic variables for the demand standard showed statistically significant differences among the ICU nurses. There were statistically significant differences between ICU nurses based on gender in the roles and changes standards (lower scores for females), education in the peer support and relationships standards (lower scores for postgraduates), years of experience in the peer support standards (lower score for 6–10 years of experience), marital status in relationships standard (lower scores for married group), monthly income in the control, peer support and the change standards (lower scores for > 20,000 SR).
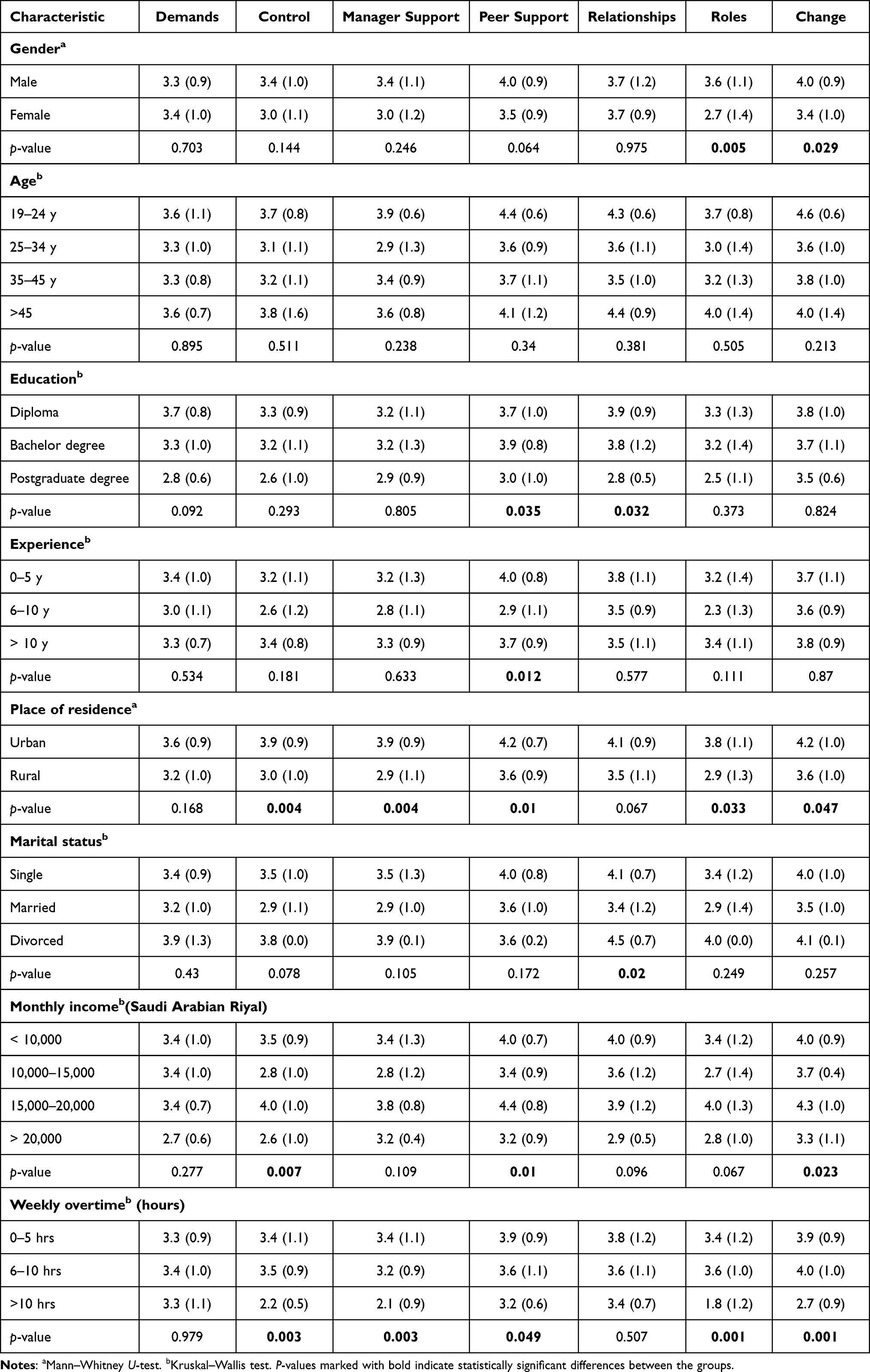 |
Table 4 Mean (SD) Scores for Each Standard Based on Sociodemographic Characteristics |
Spearman’s rank correlation was used to determine the relationship between the HSE management standards (Table 5). There was a significant positive correlation between all HSE management standards, except the correlation between the demand and change standards was non-significant.
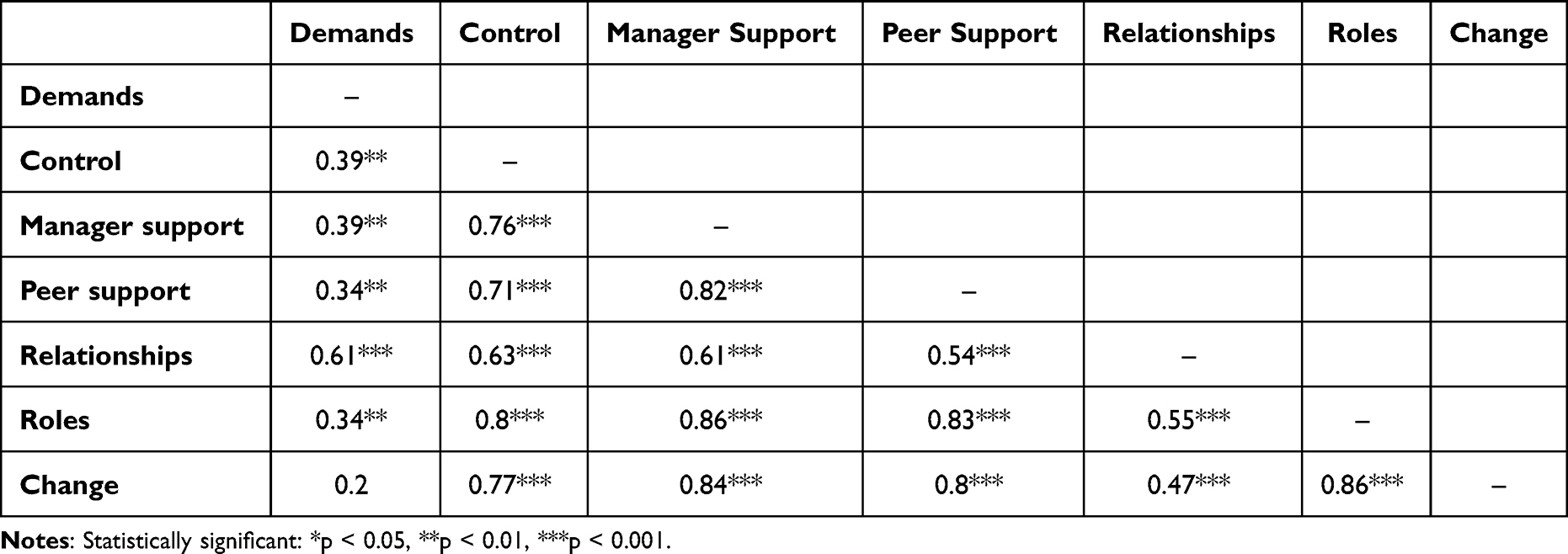 |
Table 5 Correlations Between the Mean Scores of the HSE Management Standards |
Narrative Comments
The qualitative section of the questionnaire ascertained the most common sources of occupational stress and the recommendations to reduce this. The results are shown in Figures 1 and 2, respectively. The most commonly cited source of occupational pressure was unsupportive management. Consequently, the most common recommendation to reduce such pressure was better management.
 |
Figure 1 The most common sources of occupational stress cited by ICU nurses. |
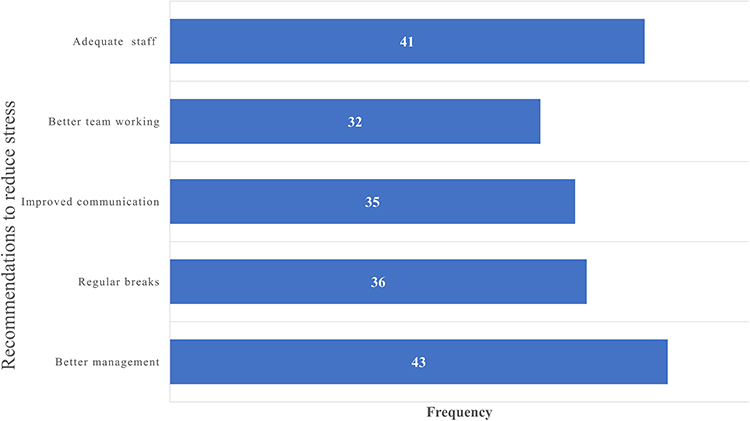 |
Figure 2 The most common recommendations to reduce occupational stress cited by ICU nurses. |
Discussion
Recent studies have reported an elevated risk of occupational stress due to the impact of the COVID-19.19,21,23–25 Studies indicated that the circumstances created by the COVID-19 epidemic have put ICU staff’s mental health at risk.19–25 This study identified the need to manage occupational stress among ICU nurses, which has been previously highlighted by several studies. Once the potential stress hazard standards in a given occupational group have been identified, interventions to mitigate both the organizational and individual effects of occupational stress may be put into place. In this study, none of the HSE Management Standards exhibited satisfactory levels, which indicates the need for interventions. Each HSE standard needs constant attention and should be viewed as a permanent opportunity for improvement.
“Urgent action needed” was indicated in “control”, “manager support” and “roles” standards. Control, which is how much say a person has in the way they work, was below average performance. For health care workers, a lack of autonomy in their daily practices can significantly reduce job satisfaction. This aspect would be considerably improved if managers changed their approach from authoritative to participative, involving ICU nurses in the decision-making process. Nursing staff should be empowered and provided with opportunities to participate in decision-making processes, which should be paired with equivalent accountability, to encourage them to strive for excellence.30 “Manager support” standard indicated very poor performance. This finding was emphasized in the narrative comments sections, which the respondents highlighted unsupportive management as the most common reason for occupational stress, and the majority of them recommended better management practices. The literature shows that poor support from management has negative stress outcomes. Manager support entails effective communicators, team builders, and collaborators, who can positively impact nurse retention and job satisfaction and play a key role in shaping the health care practice environment for the better.31 Other studies also found poor management regarding communication, staff welfare, planning, and organization.32,33 The “roles” standard was below average performance. Researchers have found that as role ambiguity increases, the level of stress rises.34 The engagement of ICU nurses in organizational goals can foster commitment and contribute to the reduction of burnout. ICU nurses’ perception of their role mainly depends on whether they feel valued and cared for by their managers.32,33 The three standards that warranted an “urgent action needed” are related with improvement in one of them can be reflected on the others.
“Clear need for improvement” was indicated in “demands”, “peer support” and “workplace relationships” standards. The demands standard, which covers workload, work patterns and work environment, has been reported as one of the most significant stressors and can lead to burnout.35 A previous study reported found that 48% of nurses who left their jobs cited poor and inadequate staffing as their reason for quitting.36 Moreover, researchers have indicated that increasing the number of nurse staff assigned to a unit provides better patient care and decreases the incidence of mortality and adverse patient outcomes.37 “Peer support” included guidance and reassurance of worth from colleagues and was linked to positive motivation and reduction in the effects of occupational stress. Peer support is essential to decrease compassion fatigue and leads to positive patient care outcomes.38,39 “Workplace relationships” are important for healthy work environment. The present study found that ICU nurses felt subjected to personal harassment and perceived friction and anger among colleagues, highlighting a largely problematic area in terms of occupational stress. According to Grissinger,
disrespectful behavior chills communication and collaboration, undercuts individual contributions to care, undermines staff morale, increases staff resignations and absenteeism, creates an unhealthy or hostile work environment, causes some to abandon their profession, and ultimately harms patients40.
Several studies have found that such behaviors have been linked to adverse events, medical errors, compromises in patient safety, and even patient mortality.41,42
The overall result for the “change” standard was indicated “Good but needs improvement”. Several studies have reported associations between stress and how organizational change is managed.43,44 One study found that training, effective communication, and consultation indirectly reduce occupational stress and have a positive impact on staff.31 Proper communication of change in a work environment is crucial in providing excellent patient care and job satisfaction.31,45
The associations between sociodemographic characteristics, commonly with the place of residence and overtime working hours, and the HSE management standards were observed. Statistically significant differences between ICU nurses for all HSE management standards, except demand and relationship standards, were found based on the place of residence, with ICU nurses living in rural areas scoring lower than nurses in urban areas, and weekly overtime, with ICU nurses who work overtime more than 10 hours scoring lower than other groups with less overtime working hours. Where one lives and the associated commute can also contribute to occupational stress. In the present study, this evidence can be explained by the fact that most of the hospitals are located in urban areas, so nurses commute to work daily. Studies have shown that commuting stress may have direct links to task performance, task motivation, negative mood upon arrival to work, and aggression in the workplace.46,47 Working long hours will directly increase the ICU nurses’ possibility of coming into contact with sources of occupational stress.48 Along with differences in scores of HSE management standards based on gender, education, years of experience, monthly income and marital status, these major findings suggest an opportunity for developing intervention plans that take into account interpersonal differences. In addition, the positive correlation between the HSE management standards indicates that improving the performance of one of the standards could lead to improvement of the others.
Limitations of the Study
This study has some limitations need to be acknowledged, including the small sample size and that the study population was obtained through a convenience sampling method, which the findings might not statistically generalizable beyond the sample. Larger sample size would serve to confirm aspects of the current study. Also, there was no baseline from before the pandemic against which to compare the occupational stress.
Conclusion
The overall findings of this study indicate that the risks associated with occupational stress for ICU nurses are not being optimally managed and that the standards are not being achieved. The results show that “good but needs improvement” indicated in change, “clear need for improvement” was indicated in demands, peer support and relationships, “urgent action needed” was indicated for and control, manager support and roles. Manager support standard indicated very poor performance, which also was emphasized in the narrative comments by respondents who highlighted unsupportive management as the most common reason for occupational stress, and recommended better management practices. Therefore, the study suggests that a psychologist-designed and -led staff stress management intervention should be adopted in ICUs, with regular evaluations being undertaken to track the implemented changes and identify any shortcomings.
Acknowledgments
The authors thank the nursing department supervisors who facilitated the distribution of the survey questionnaire.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Murphy LR, Sauter SL. Work organization interventions: state of knowledge and future directions. Soz Praventivmed. 2004;49(2):79–86. doi:10.1007/s00038-004-3085-z
2. Edwards M. Research review. Burnout syndrome in critical care nursing staff. Dynamics. 2010;21(1):8–9.
3. Bogue TL, Bogue RL. Extinguish burnout in critical care nursing. Crit Care Nurs Clin North Am. 2020;32(3):451–463. doi:10.1016/j.cnc.2020.05.007
4. Laporta DP, Burns J, Doig CJ. Bench-to-bedside review: dealing with increased intensive care unit staff turnover: a leadership challenge. Crit Care. 2005;9(5):454–458. doi:10.1186/cc3543
5. Teixeira C, Ribeiro O, Fonseca AM, Carvalho AS. Burnout in intensive care units - a consideration of the possible prevalence and frequency of new risk factors: a descriptive correlational multicentre study. BMC Anesthesiol. 2013;13(1):38. doi:10.1186/1471-2253-13-38
6. Poncet MC, Toullic P, Papazian L, et al. Burnout syndrome in critical care nursing staff. Am J Respir Crit Care Med. 2007;175(7):698–704. doi:10.1164/rccm.200606-806OC
7. Moss M, Good VS, Gozal D, Kleinpell R, Sessler CN. An official critical care societies collaborative statement: burnout syndrome in critical care health care professionals: a call for action. Am J Crit Care. 2016;25(4):368–376. doi:10.4037/ajcc2016133
8. Mealer M. Promoting well-being and resilience in critical care nursing. AACN Adv Crit Care. 2020;31(2):139–140. doi:10.4037/aacnacc2020952
9. Rathnayake S, Dasanayake D, Maithreepala S, Ekanayake R, Basnayake P. Nurses’ perspectives of taking care of patients with Coronavirus disease 2019: a phenomenological study. PLoS One. 2021;16:e0257064. doi:10.1371/journal.pone.0257064
10. Sirri L, Fabbri S, Fava GA, Sonino N. New strategies in the assessment of psychological factors affecting medical conditions. J Pers Assess. 2007;89(3):216–228. doi:10.1080/00223890701629649
11. Woodrow P. Intensive Care Nursing: A Framework for Practice. Routledge; 2018.
12. Rosa WE, Ferrell BR, Wiencek C. Increasing critical care nurse engagement of palliative care during the COVID-19 pandemic. Crit Care Nurse. 2020;40(6):e28–e36. doi:10.4037/ccn2020946
13. Stanton R, To QG, Khalesi S, et al. Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int J Environ Res Public Health. 2020;17:11. doi:10.3390/ijerph17114065
14. Maugeri G, Castrogiovanni P, Battaglia G, et al. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon. 2020;6(6):e04315. doi:10.1016/j.heliyon.2020.e04315
15. Engeseth K, Prestgaard EE, Mariampillai JE, et al. Physical fitness is a modifiable predictor of early cardiovascular death: a 35-year follow-up study of 2014 healthy middle-aged men. Eur J Prev Cardiol. 2018;25(15):1655–1663. doi:10.1177/2047487318793459
16. Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. 2014;44(1):81–121.
17. Woon LS-C, Mansor NS, Mohamad MA, Teoh SH. Leong Bin Abdullah MFI. Quality of life and its predictive factors among healthcare workers after the end of a movement lockdown: the salient roles of covid-19 stressors, psychological experience, and social support. Front Psychol. 2021;12:1164. doi:10.3389/fpsyg.2021.652326
18. Iqbal MS. Predictors of health-related quality of life among healthcare professionals. Med Sci. 2020;24:4445–4452.
19. Arpacioglu S, Gurler M, Cakiroglu S. Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int J Soc Psychiatry. 2021;67(1):84–89. doi:10.1177/0020764020940742
20. Buselli R, Corsi M, Baldanzi S, et al. Professional quality of life and mental health outcomes among health care workers exposed to sars-cov-2 (covid-19). Int J Environ Res Public Health. 2020;17(17). doi:10.3390/ijerph17176180
21. Çelmeçe N, Menekay M. The effect of stress, anxiety and burnout levels of healthcare professionals caring for COVID-19 patients on their quality of life. Front Psychol. 2020;11:597624. doi:10.3389/fpsyg.2020.597624
22. Rapisarda F, Vallarino M, Cavallini E, et al. The early impact of the covid-19 emergency on mental health workers: a survey in Lombardy, Italy. Int J Environ Res Public Health. 2020;17(22):8615. doi:10.3390/ijerph17228615
23. Secosan I, Virga D, Crainiceanu ZP, Bratu T. The mediating role of insomnia and exhaustion in the relationship between secondary traumatic stress and mental health complaints among frontline medical staff during the COVID-19 pandemic. Behav Sci. 2020;10(11):11. doi:10.3390/bs10110164
24. Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic’s effect on critical care resources and health-care providers: a global survey. Chest. 2021;159(2):619–633. doi:10.1016/j.chest.2020.09.070
25. Lluch C, Galiana L, Doménech P, Sansó N. The impact of the COVID-19 pandemic on burnout, compassion fatigue, and compassion satisfaction in healthcare personnel: a systematic review of the literature published during the first year of the pandemic. Healthcare. 2022;10(2):364. doi:10.3390/healthcare10020364
26. Rick J, Daniels K, Briner R, Perryman S, Guppy A. A critical review of psychosocial hazard measures; 2001.
27. Kompier M. Does the ‘Management Standards’ approach meet the standard? Work Stress. 2004;18:137–139. doi:10.1080/02678370412331291434
28. Dykema J, Jones NR, Piché T, Stevenson J. Surveying clinicians by web: current issues in design and administration. Eval Health Prof. 2013;36(3):352–381. doi:10.1177/0163278713496630
29. Health, Executive S. HSE management standards indicator tool user manual; 2018.
30. Robertson-Malt S, Chapman Y. Finding the right direction: the importance of open communication in a governance model of nurse management. Contemp Nurse. 2008;29(1):60–66. doi:10.5172/conu.673.29.1.60
31. AACN. AACN standards for establishing and sustaining healthy work environments: a journey to excellence. Am J Crit Care. 2005;14(3):187–197. doi:10.4037/ajcc2005.14.3.187
32. Ray SL, Wong C, White D, Heaslip KJT. Compassion satisfaction, compassion fatigue, work life conditions, and burnout among frontline mental health care professionals. Traumatology. 2013;19(4):255–267. doi:10.1177/1534765612471144
33. Sacco TL, Ciurzynski SM, Harvey ME, Ingersoll GL. Compassion satisfaction and compassion fatigue among critical care nurses. Crit Care Nurse. 2015;35(4):32–43. doi:10.4037/ccn2015392
34. Beauchamp M, Bray S, Eys M, Carron A. The effect of role ambiguity on competitive state anxiety. J Sport Exerc Psychol. 2003;25:77–92.
35. Kohler M. Exploring the relationships among work-related stress; 2010.
36. Ulrich BT, Lavandero R, Woods D, Early S. Critical care nurse work environments 2013: a status report. Crit Care Nurse. 2014;34(4):64–79.
37. Shin S, Park JH, Bae SH. Nurse staffing and nurse outcomes: a systematic review and meta-analysis. Nurs Outlook. 2018;66(3):273–282. doi:10.1016/j.outlook.2017.12.002
38. Boev C, Xia Y. Nurse-physician collaboration and hospital-acquired infections in critical care. Crit Care Nurse. 2015;35(2):66–72. doi:10.4037/ccn2015809
39. Bhutani J, Bhutani S, Balhara YP, Kalra S. Compassion fatigue and burnout amongst clinicians: a medical exploratory study. Indian J Psychol Med. 2012;34(4):332–337. doi:10.4103/0253-7176.108206
40. Grissinger M. Disrespectful behavior in health care: its impact, why it arises and persists, and how to address it-part 2. P T. 2017;42(2):74–77.
41. Rosenstein AH, O’Daniel M. A survey of the impact of disruptive behaviors and communication defects on patient safety. Jt Comm J Qual Patient Saf. 2008;34(8):464–471. doi:10.1016/s1553-7250(08)34058-6
42. McNamara SA. Incivility in nursing: unsafe nurse, unsafe patients. Aorn j. 2012;95(4):535–540. doi:10.1016/j.aorn.2012.01.020
43. Collins M. Taking a lead on stress: rank and relationship awareness in the NHS. J Nurs Manag. 2006;14:310–317. doi:10.1111/j.1365-2934.2006.00593.x
44. MacKay C, Cousins R, Kelly P, Lee S, McCaig R. Management standards’ and work-related stress in the UK: policy background and science. Work Stress. 2004;18:91–112. doi:10.1080/02678370410001727474
45. Henkin S, Chon TY, Christopherson ML, Halvorsen AJ, Worden LM, Ratelle JT. Improving nurse-physician teamwork through interprofessional bedside rounding. J Multidiscip Healthc. 2016;9:201–205. doi:10.2147/JMDH.S106644
46. Novaco R, Stokols D, Campbell J, Stokols J. Transportation, Stress, and Community Psychology. American journal of community psychology. 1979;7:361380.;7:361380.
47. Hennessy D. The Impact of Commuter Stress on Workplace Aggression. Journal of Applied Social Psychology. 2008;38:23152335.;38:23152335.
48. Hong Y, Zhang Y, Xue P, et al. The Influence of Long Working Hours, Occupational Stress, and WellBeing on Depression Among Couriers in Zhejiang, China. Hong Y, Zhang Y, Xue P, et al. The Influence of Long Working Hours, Occupational Stress, and WellBeing on Depression Among Couriers in Zhejiang, China. 2022;13.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of the Critical Care Work Environment of Intensive Care Unit Nurses in Saudi Arabia
Ageel M, Shbeer A
Risk Management and Healthcare Policy 2022, 15:2413-2420
Published Date: 23 December 2022