Back to Journals » International Journal of Women's Health » Volume 18
Exploring Intergenerational Dialogues as a Strategy to Reduce Rejection of Young Single Mothers in Rwanda: A Qualitative Study
Authors Dusabe A, Habimana S ![]() , Kubwimana I, Khanyola JN, Mhlanga M, Yohannes T, Ndaimani A
, Kubwimana I, Khanyola JN, Mhlanga M, Yohannes T, Ndaimani A ![]()
Received 19 March 2026
Accepted for publication 11 July 2026
Published 15 July 2026 Volume 2026:18 610545
DOI https://doi.org/10.2147/IJWH.S610545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Marta Barba
Anna Dusabe,1,* Samuel Habimana,1,* Isabelle Kubwimana,2 Judy N Khanyola,3 Maxwell Mhlanga,1 Tsion Yohannes,1 Augustine Ndaimani4
1Centre of Gender Equity, University of Global Health Equity, Kigali, Rwanda; 2Programs Department, Haguruka, Kigali, Rwanda; 3Governing Council, African Forum for Research and Education in Health (AFREhealth), Nairobi, Kenya; 4Centre for Nursing and Midwifery, University of Global Health Equity, Kigali, Rwanda
*These authors contributed equally to this work
Correspondence: Augustine Ndaimani, Centre for Nursing and Midwifery, University of Global Health Equity, Kigali Heights, KG 7 Avenue, 5th Floor, P.O. Box 6955, Kigali, Rwanda, Email [email protected]
Introduction: Teenage pregnancy is a major global public health concern, with an estimated 21 million adolescent girls giving birth each year globally. Despite the growing implementation of dialogue-based interventions, limited evidence exists regarding how participants perceive their effectiveness within family and community systems in Rwanda. This study explored participants’ perceptions of the effectiveness of the Ingo z’amahoro intergenerational dialogue programme in resolving intergenerational conflicts, responding to GBV, and improving family and community support for young single mothers.
Methods: An exploratory qualitative study using purposive sampling and reflexive thematic analysis was conducted across four sectors in Musanze and Gasabo Districts, Rwanda. Thirty-two participants were recruited: 12 young single mothers (aged 15– 24 years), 12 parents or guardians, and 8 key informants (community facilitators, local leaders, and programme representatives). Eligible participants had engaged with the programme for at least two years. Data were collected through 24 in-depth interviews and 8 key informant interviews, conducted between May and June 2024. Trustworthiness was enhanced through member checking, reflexive journaling, peer debriefing, and audit trails. The study was conducted in compliance with the Declaration of Helsinki.
Results: Three themes emerged: (1) perceived personal, familial, and community benefits of intergenerational dialogues, including family reconciliation, enhanced GBV and sexual and reproductive health (SRH) awareness, improved community attitudes, and increased self-confidence; (2) socioeconomic and structural barriers to effective participation, including poverty, absent male stakeholders, and persistent social stigma; and (3) strategies for sustaining impact through service integration and economic empowerment.
Conclusion: Intergenerational dialogues hold meaningful potential for family reconciliation and GBV awareness among young single mothers in Rwanda. However, dialogue alone is insufficient without addressing broader structural inequalities, underscoring the need for integrated psychosocial, economic, and male-engagement interventions.
Keywords: gender-based violence, intergenerational dialogues, qualitative study, Rwanda, sexual and reproductive health and rights, teenage pregnancy, young single mothers
Introduction
Teenage pregnancy is a major global public health concern, with an estimated 21 million girls aged 15–19, mostly from low- and middle-income countries, giving birth each year.1 Sub-Saharan Africa bears a disproportionate share of this burden, with the highest regional rate at 97.9 births per 1,000 women and the slowest rate of decline globally.1 Within the African context, a growing body of scholarship has explored the structural drivers and social consequences of adolescent pregnancy, including school dropout, child marriage, poverty, and family breakdown.2 Beyond its demographic dimensions, teenage pregnancy carries serious health consequences: more than half of affected adolescents in Rwanda experience unsafe abortions, placing their lives at risk of severe complications.3
Rwanda offers a particularly salient case: although the national teenage pregnancy rate had declined steadily to around 5% by 2019–20,4 a sharp reversal occurred following the COVID-19 pandemic, with reported cases rising from 17,337 in 2017 to 19,832 in 2020 and 33,423 in 2022.5 This resurgence demands urgent, evidence-grounded, programmatic responses. Young single mothers frequently face gender-based violence (GBV), intergenerational family conflict, social stigmatisation, and economic marginalisation as they navigate the demands of early parenthood alongside disrupted education and limited livelihood options.6,7 These challenges intersect in ways that compound vulnerability: family rejection and abandonment weaken social cohesion, heighten the risk of further violence, and push young mothers into economic dependency on abusive partners. The Rwanda Investigation Bureau documented 12,715 GBV cases in 2020 alone,8 and national data show that the proportion of girls under 18 subjected to sexual violence rose from 27.3% to 38.5% between 2014 and 2020.8 Globally, 1 in 8 girls experiences sexual violence before the age of 18, and 1 in 20 girls aged 15–19 reports having been forced into sexual intercourse during their lifetime.3 In districts such as Musanze, Gasabo, and Nyagatare, the number of teenage mothers rejected by their families is notably high, with 1,465, 1,064, and 1,452 teenage pregnancies recorded per year, respectively,9 indicating that these districts are high-burden sites particularly relevant for studying intergenerational conflict and dialogue-based responses.
Intergenerational conflict, defined as incompatibility between the ideals, needs, interests, or behaviours of people from different age groups,10 is exacerbated by poor communication, divergent generational expectations, and financial stress.11 Left unaddressed, family rejection and abandonment compound gender inequality, weaken social cohesion, and heighten the risk of further violence. The political economy of teenage pregnancy is also relevant here: young single mothers in Rwanda frequently lack access to education, formal employment, and social protection, making economic dependency a key driver of continued vulnerability, including vulnerability to abusive relationships.12 Addressing intergenerational conflict, therefore, requires a combination of relational and material interventions.
Intergenerational dialogues, structured conversations through which people of different generations exchange ideas, values, experiences, and knowledge, have been used in several settings to foster mutual respect, support policy contributions by young people, and mend family fractures.13 Such dialogues can be formal or informal and are often integrated with empowering interventions such as vocational training, financial literacy, and Sexual and Reproductive Health and Rights (SRHR) education. Despite increasing implementation of dialogue-based interventions for adolescent mothers in Africa, limited evidence exists regarding how participants themselves perceive the effectiveness of these interventions within family and community systems in Rwanda. The literature has tended to focus on programmatic outcomes while marginalising the voices of stigmatised groups such as pregnant teenagers and young mothers, and has not systematically examined the dynamics of parent-child relationships in depth.
The Ingo z’amahoro project, a vernacular Kinyarwanda phrase meaning “peaceful homes”, is implemented by the Haguruka organisation in Rwanda to promote intergenerational dialogue between parents and their estranged pregnant or single-parent teenage daughters. The project aims to prevent teenage pregnancies, reduce mistreatment of young single mothers, and enhance parental, family, and community support through SRHR education, structured dialogue sessions, and the provision of safe spaces for abused young mothers.14 Despite these efforts, the effectiveness of the dialogue component remains underexplored. This study sought to address that gap by exploring participants’ perceptions of the effectiveness of intergenerational dialogues in resolving intergenerational conflicts, preventing and responding to GBV, and identifying strengths, challenges, and preferences for programme delivery.
Theoretical Framework
This study was informed by two complementary theoretical perspectives that together shaped interview guide development, coding, and interpretation. First, dialogue-based approaches to conflict resolution posit that structured, facilitated conversation can interrupt cycles of misunderstanding, build empathy, and create shared commitments to changed behaviour.15,16 This framework informed the focus on communication processes and guided the development of interview questions exploring how dialogue sessions altered relational dynamics between young mothers and their parents.
Second, an intersectional feminist framework situates young single mothers’ experiences at the confluence of age, gender, class, and cultural norms, drawing attention to how structural inequalities shape both the occurrence of teenage pregnancy and the social responses to it.12 This framework guided the deductive coding of data related to power, stigma, economic exclusion, and gendered barriers. Together, these perspectives foreground the importance of attending not only to individual attitude change but also to the socioeconomic and gendered conditions that constrain or enable the transformative potential of dialogue-based interventions. The linkage between the frameworks and the research questions, which explicitly address both relational change and structural barriers, was therefore intentional and analytically productive.
Materials and Methods
Setting
The study was conducted in the Muhoza and Cyuve sectors of Musanze District and the Kinyinya and Remera sectors of Gasabo District, Rwanda. These four sectors were selected purposively because they are active implementation sites for the Ingo z’amahoro programme, representing typical high-burden settings for teenage pregnancy and associated family conflict. Gasabo recorded 1,064 teenage pregnancies attributable to sexual assault, while Musanze reported that 75% of teenage pregnancies in the district were associated with sexual assault.8,17 Participants were recruited across all four sectors, ensuring geographic and contextual variation.
Design
An exploratory qualitative design was used to generate an in-depth understanding of participants’ subjective experiences and perceptions of the intergenerational dialogue programme. Reflexive thematic analysis, following the framework of Braun and Clarke,18 served as the analytic approach. Qualitative methods are well-suited to capturing the nuanced processes of relational change that are unlikely to be visible through quantitative measures alone. The study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Sample and Recruitment
Using purposive sampling, 32 participants were recruited across the four sectors: 12 young single mothers, 12 parents or guardians, and 8 key informants, comprising two local leaders, four community facilitators, and two Haguruka district representatives. In-depth interviews (IDIs) were conducted with 12 young mothers and their 12 parents or guardians; key informant interviews (KIIs) were conducted with eight participants. The IDI sample size was guided by the principle of thematic sufficiency, with coding continuing until no new codes emerged within each participant group (young mothers and parents assessed separately). Empirical evidence indicates that saturation typically occurs within 5–24 interviews,19 the sample of 24 IDI participants allowed adequate representation across both districts and both participant groups. The slightly larger overall sample of 32 reflected the purposive inclusion of key informants to ensure representation of all major programme stakeholders. The number of KIIs (n = 8) was determined a priori to ensure at least two participants per stakeholder category (community facilitators, local leaders, and programme representatives), consistent with expert consensus on stakeholder coverage in qualitative programme evaluations.
Participant diversity was operationalised across age, socioeconomic status, relationship dynamics (mother-daughter and parent-guardian), and geographic variation (two districts, four sectors). Young mothers were eligible if they: were aged 15–24 years (an age range that extends beyond typical adolescence to capture the broader population of young single mothers engaged by the programme, as defined by Rwanda’s national youth policy); resided in one of the four study sectors; and had participated in Ingo z’amahoro dialogues for at least two years. This minimum engagement period was selected to ensure participants had sufficient exposure to the programme to reflect meaningfully on its impact; it is acknowledged as a potential positive selection limitation. Those who had lost their infants were excluded to minimise the risk of acute grief affecting disclosure and to protect participant wellbeing. Parents were eligible if they had participated in the dialogues for at least two years and were excluded if they had been incarcerated for GBV or had received other behavioural interventions that might confound behaviour change; the latter criterion was verified through programme records maintained by Haguruka. Key informants were included if they had direct involvement with programme participants or the sector executive committee for at least one year. Terminology for participants is standardised throughout as ‘young single mothers”, “parents”, and “key informants”.
Data Collection
Data were collected in May and June 2024 using three semi-structured interview guides developed for young mothers, their parents, and key informants. The guides were informed by the study’s theoretical frameworks and by existing instruments from the adolescent SRH and intergenerational dialogue literature. Each guide included biographical items and questions on perceived effectiveness, strengths, challenges, limitations, and preferences. The young mother guide comprised eight items with 16 probes; the parent guide comprised seven items with 14 probes; and the key informant guide comprised five items with nine probes. The guides were pre-tested with five global health students fluent in both Kinyarwanda and English. Pre-testing feedback was used to refine question wording and probe sequencing, and to culturally adapt phrasing to ensure contextual relevance.
A trained team of data collectors with backgrounds in public health and social sciences, and with training in ethical research conduct, interview technique, psychological first aid, and the study objectives, conducted all interviews. Data collectors were independent of the Haguruka programme and had no prior relationship with participants, thereby minimising the risk of coercion. Interviews lasted 40 to 55 minutes and were conducted in participants’ preferred language (Kinyarwanda or English) in private rooms at Haguruka offices, with the research data kept confidential. Data collectors were trained to provide on-site psychological first aid and refer participants who disclosed psychological distress during interviews for further management.
The study was approved by the UGHE Institutional Review Board (UGHE-IRB/2024/301) and was conducted in compliance with the Declaration of Helsinki. Signed informed consent was obtained from all participants prior to interview commencement; informed consent explicitly covered the publication of anonymised responses and direct quotes. The one participant aged under 18 years provided voluntary assent alongside parental consent. Interviews were audio-recorded, transcribed verbatim, de-identified, and translated into English by bilingual researchers using a back-translation process to verify accuracy and consistency. Following quality checks, audio files were permanently deleted, and transcripts were password-protected.
Data Analysis
Data were analysed using reflexive thematic analysis following Braun and Clarke’s six-phase framework:18 (1) familiarisation with data; (2) generating initial codes; (3) searching for themes; (4) reviewing themes; (5) defining and naming themes; and (6) producing the final report. Analysis was conducted via Dedoose software, which facilitated systematic code management; the analytical interpretations were generated by the research team rather than by the software itself. The codebook was developed both inductively (from participant narratives) and deductively (from study objectives). Initial coding was conducted independently by two members of the research team; codes were subsequently reviewed in team discussions, and themes were refined iteratively through consensus. Prior to coding, investigators recorded their positionality in a reflexive journal to minimise interpretive bias.
Member checking was conducted with a sub-sample of participants following thematic analysis: emerging themes were shared with six participants (three young mothers and three parents, selected for diversity of district and age), and their feedback was incorporated into final theme descriptions. Additional trustworthiness measures included independent back-translation, audio recording, use of open-ended questions and probes, thick description of findings, peer debriefing, and maintenance of an audit trail of field notes.
Results
Participant Characteristics
Thirty-two participants were recruited: 12 young single mothers, 12 parents or guardians, and 8 key informants. Sixteen participants were recruited from each of Musanze and Gasabo (Kigali) Districts. All young single mothers and their parents had participated in the Ingo z’amahoro programme since 2018. Eleven young mothers were aged 18–24 years; one was 17. All young mothers had a primary-level education; a characteristic that reflects both the socioeconomic profile of programme participants and the educational disruption commonly associated with early pregnancy. Parents ranged in age from 36 to 64 years and included 11 women and one man, reflecting the predominantly female uptake of the programme among parents and a potential limitation for the gendered perspectives captured. The demographic profiles of participants are summarised in Table 1.
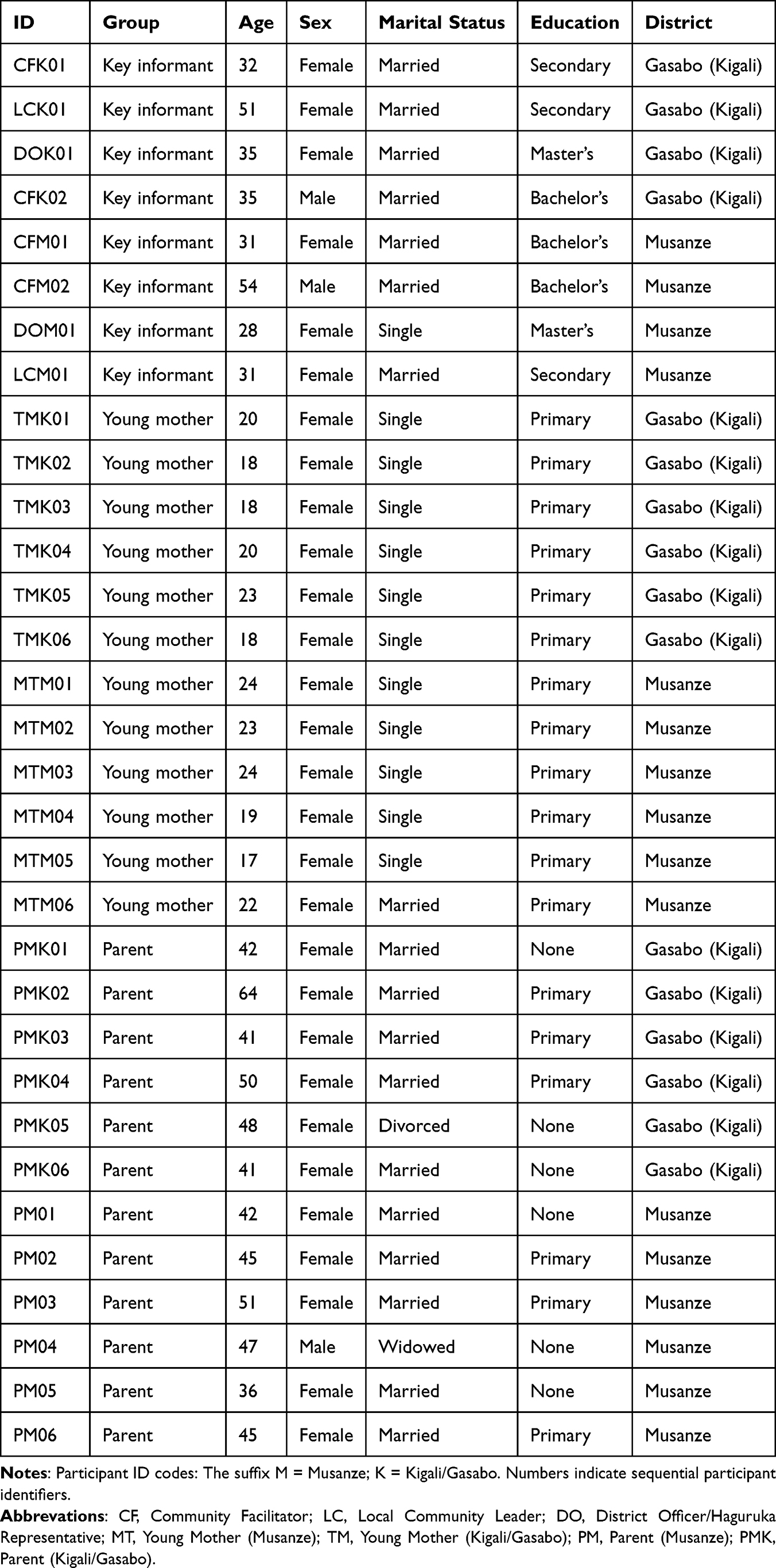 |
Table 1 Sociodemographic Characteristics of Participants |
Three themes were identified, as summarised in Table 2: (1) perceived personal, familial, and community benefits of intergenerational dialogues; (2) socioeconomic and structural barriers to effective participation; and (3) strategies for sustaining impact through service integration and economic empowerment. These themes emerged through iterative coding and thematic refinement across the full dataset. Participant quotes are identified by their participant codes; a legend explaining the code structure appears below, Table 2.
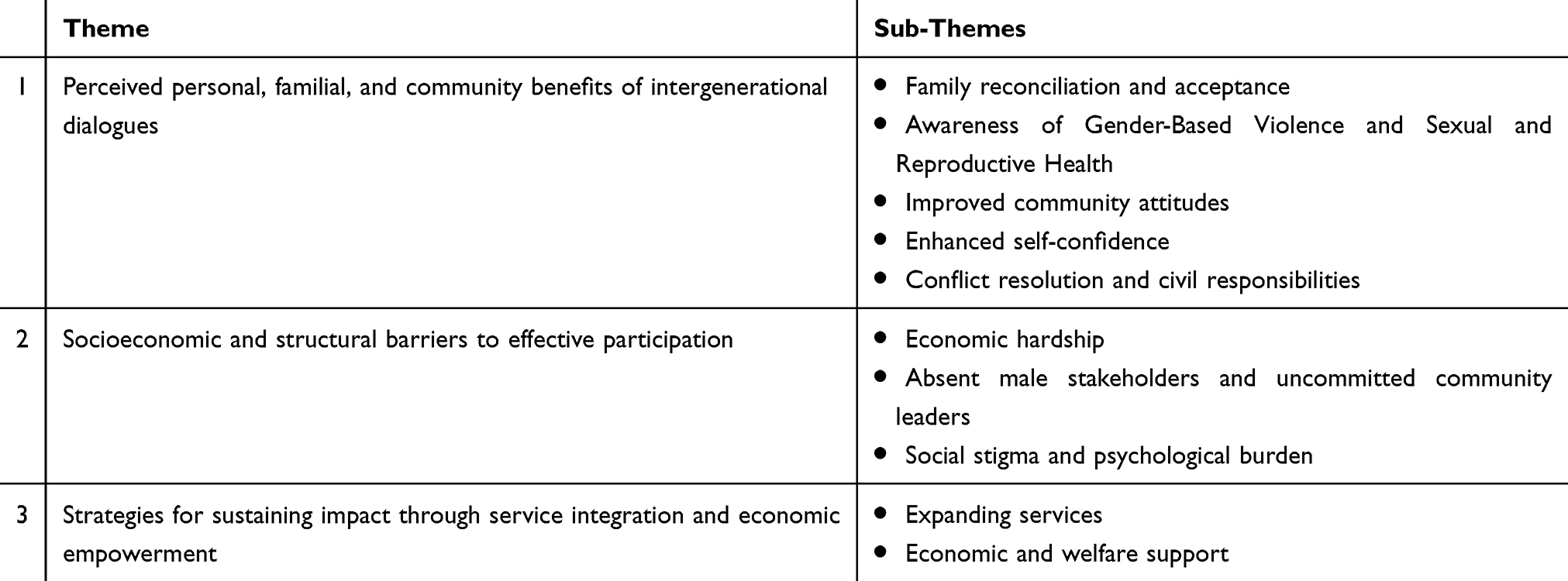 |
Table 2 Summary of Themes and Sub-Themes |
Theme 1: Perceived Personal, Familial, and Community Benefits of Intergenerational Dialogues
This theme captures five categories of benefit reported by participants: family reconciliation and acceptance; awareness of GBV and sexual and reproductive health (SRH); improved community attitudes; enhanced self-confidence; and conflict resolution and civil responsibilities.
Family Reconciliation and Acceptance
For many young mothers, participation in the programme marked the beginning of their reintegration into family life after being abandoned. Prior to the dialogues, mothers described living in isolation and being unable to provide for themselves or their infants. The dialogues created a structured space for parents to reconceptualise their roles and relationships with their daughters. One parent reflected:
The training we received gave us lessons in how to talk to them and show them that life goes on, and every person who is involved should understand that her child is hers and we don’t have anywhere else to put her. (PM02)
For another parent, the change was emotional as well as practical: “The positive effect of those conversations touched my heart … we were in the same mood” (PM01). Young mothers, in turn, described being able to return home and resume some degree of normal family life: “I went back into the family. Now I can leave my child home and search for a job” (MTM04).
Community facilitators noted remarkable transformations:
Before, life was so bad, some children seemed to be cut off from home, their parents failed to accept them … After discussing with them, their parents accepted them, welcomed them, and forgave them; the parents asked for their children’s forgiveness … the children also asked their parents for forgiveness. (CFM02)
These accounts are consistent with evidence that structured communication interventions can enhance family dynamics and reduce tension in high-conflict households.16 However, reconciliation with family does not necessarily eliminate underlying patriarchal norms or economic dependence, and young mothers remained vulnerable to renewed rejection if they became pregnant again or failed to conform to gendered expectations, a tension that the programme must continue to address.
Awareness of Gender-Based Violence and Sexual and Reproductive Health
The dialogues provided participants with what many described as their first formal engagement with GBV and SRH content. Facilitators described teaching parents how to discuss contraception and respond to sexual violence:
Methods that would make them not have another child … showing the existing laws that punish gender-based violence offenders, ways to avoid conflict, [or] sexual violence. (DOK01)
Young mothers who had initially internalised blame, feeling “the guilt of pregnancy, that they deserved to be disrespected”, began to identify violence as such and to open difficult conversations about family planning (DOK01). The Programme facilitators also helped parents recognise subtler forms of GBV: “Even insulting my kid that she’s useless and she will not do anything is also GBV” (DOM01). One community leader observed that “the cause of family conflict is the lack of knowledge people have about reproductive health, and not only for young people, as we mistakenly believe” (DOK01).
These gains are significant given that Rwandan cultural norms have historically made intergenerational discussion of sex, reproduction, and intimate violence taboo, particularly between fathers and their daughters. From an intersectional feminist perspective, this awareness-raising represents a disruption of gendered knowledge hierarchies that have historically silenced young women. However, the limited participation of fathers, discussed under Theme 2, meant this awareness-raising was largely confined to mothers and their daughters, leaving male household heads outside the frame of change.
Improved Community Attitudes
Participants reported meaningful shifts in community attitudes toward young single mothers, moving from ostracism and verbal abuse toward acceptance and support. One young mother recalled: “They used to talk behind my back that ‘see her she got pregnant, see how she is behaving badly dressed and looks bad’” (TMK01). After programme engagement:
When a person was pregnant, they used to bully her, insult or stigmatise her every day, but owing to dialogues brought by Haguruka, the insult stopped; they now treat me and my child as theirs without any problems. (MTM04)
Programme facilitators noted that parents were encouraged to model acceptance publicly “to change and treat the child as usual, so that the neighbours also see … that a girl who got pregnant or gave birth should not be thrown away” (PMK05), thereby extending the normative shift beyond the immediate family. An increase in civil registration of children born to young single mothers was also observed: “The number of children who have started asking for registration in civil status has grown” (LCM01). This is particularly noteworthy because civil registration is a prerequisite for accessing education, healthcare and social services.
While these attitudinal changes are encouraging, they must be understood within Rwanda’s broader landscape of social norms: patriarchal household dynamics and cultural stigma attached to out-of-wedlock childbearing remain deeply entrenched in many communities. Normative change at the community level requires sustained, multi-generational engagement beyond time-limited dialogue sessions.
Enhanced Self-Confidence
Several young mothers described transformative gains in self-confidence and agency. One participant reported: “The dialogues from the training organised by Haguruka have boosted my self-awareness … I dream of achieving more in life despite all I went through” (MTM03). Another described a shift from spiritual despair to active participation:
I can now attend meetings and contribute to discussions … I felt that even God had abandoned me, that it was impossible, and I had no faith, but now Haguruka gave me confidence. (TMK06)
Some participants reported using their newfound confidence to educate other young women in their communities about SRH and GBV, suggesting an informal diffusion of programme benefits that warrants further investigation.
Conflict Resolution and Civil Responsibilities
The dialogues equipped young mothers with skills for de-escalating conflicts. One mother reflected: “Before, I would immediately answer my mother angrily, but after training, I learned to listen and respond calmly” (TMK01). Another described learning to “answer like a child talking to a parent well, without being rude” (TMK03), which enabled genuine reconciliation: “I apologised for my behaviour after giving birth … they were very kind to me, and they forgave me” (TMK05). Conflict resolution also facilitated civil registration of children, a priority for both community leaders and families. Local leaders described active mediation efforts to ensure that fathers acknowledged their children:
We visited them and told some of them that we would take them to jail if they did not register their child … they understood and registered their child; now all the children were registered under their parents. (LCM01)
This finding highlights the intersections between interpersonal conflict, legal accountability, and children’s rights, connecting dialogue-based approaches to broader governance and social protection systems.
Theme 2: Socioeconomic and Structural Barriers to Effective Participation
Alongside these achievements, several structural barriers constrained the effectiveness and reach of the dialogues. This theme addresses economic hardship, absent male stakeholders, and persistent social stigma. These barriers are analytically distinct from the benefits described in Theme 1, even though stigma and vulnerability appear in both themes: Theme 1 captures shifts in attitudes, whereas this theme foregrounds the structural forces that remain resistant to dialogue-based change alone.
Economic Hardship
Poverty was a pervasive barrier to full programme participation. The Programme Facilitators noted that
Families struggle to support their children’s educational journeys or provide necessities such as school supplies; this economic strain sometimes hinders their full participation in our project. (DOK01)
Young mothers, most of whom had only primary education and no formal employment, faced a dual burden of sustaining themselves and their infants while attending monthly sessions. From an intersectional perspective, this economic vulnerability reflects the structural reproduction of gendered poverty: limited access to land, credit, and formal labour markets constrains young mothers’ autonomy and resilience.11,12 Addressing this structural dimension is essential if intergenerational dialogues are to have a lasting impact beyond the session room, as the dialogue-based conflict resolution framework itself recognises that material deprivation constrains the capacity for sustained relational change.
Absent Male Stakeholders and Uncommitted Community Leaders
A significant structural limitation of the programme was the near-absence of fathers and male community leaders. Facilitators noted that leaders’ “busy schedules or reluctance to discuss sensitive topics sometimes limit our outreach to key leaders who could help amplify our message” (DOK01). This finding is consistent with the broader literature on male engagement in SRHR interventions, which identifies cultural norms around masculinity and sexual propriety as key barriers.20 In contrast to similar programmes where fathers were actively involved in intergenerational dialogue,20 the Ingo z’amahoro dialogues engaged predominantly mothers and their daughters. Given that household decision-making authority in many Rwandan communities resides primarily with men, their exclusion limits the transformative scope of the dialogues. It also risks leaving in place the patriarchal norms that render young single mothers vulnerable to violence and rejection. Community leaders’ engagement is strategically important, given their formal and informal authority in dispute resolution and GBV redress. This gap must be addressed through gender-sensitive male engagement strategies that reframe participation as an expression of responsible fatherhood and community leadership rather than a transgression of cultural propriety.
Social Stigma and Psychological Burden
Despite the reported shifts in community attitudes in Theme 1, social stigma remained a significant and sometimes overwhelming burden. One young mother described reaching “the point where she decided to go and lock herself in the house” (PM05). Another recalled:
My classmates ridiculed me, and my parents did not support me. They sometimes doubted the paternity of my child. However, my friend from the training comforted me. (TMK05)
The psychological consequences of stigma, including social isolation, depression, and limited engagement in SRHR services, are well established in the literature.21 Participants consistently identified the absence of formal psychosocial counselling as a gap in the programme, highlighting the need to integrate mental health support into the dialogue model.
Theme 3: Strategies for Sustaining Impact Through Service Integration and Economic Empowerment
Participants expressed a clear desire for the programme to expand in scope, frequency, and ancillary support. Two sub-themes were identified: expanding services and economic and welfare support.
Expanding Services
Many participants felt that the monthly sessions were insufficient to produce effective learning: “Once a month, for me, I feel like you should try twice so that we understand better” (MTM01). This is consistent with evidence that reinforcement sessions enhance learning retention, particularly for participants with limited formal education.22 Participants also called for integration with related services, including “contraceptive methods and HIV testing” (MTM03) and formal “counselling services, because many of us were psychologically traumatised, in addition to giving birth at a young age” (MTM03). These calls reflect the integrated nature of the challenges young mothers face and align with global recommendations for comprehensive, multi-component adolescent health interventions.
Economic and Welfare Support
The most consistently expressed need across participant groups was economic empowerment. Participants called for support with vocational training (“put them in technical schools”, CFM01), business creation (“creating small businesses”, PM01; “sewing machines and materials”, CFK02), and school reintegration (“children who want to go back to school should be helped”, CFM01). Several participants highlighted the material vulnerabilities of infants during session attendance:
Sometimes, a parent brings only one nappy, and when it becomes dirty, she does not have another to change it. I suggest Haguruka sometimes assist with some nappies in case it happens in the chat room, or provide some milk to kids in the chat room. (MTM03)
These demands reflect the fundamental principle that individuals cannot fully engage with psychological and relational development while basic physiological needs remain unmet, and are consistent with broader evidence that livelihood support significantly enhances the durability of dialogue-based programme outcomes.23
Discussion
This study explored the perceived effectiveness of the Ingo z’amahoro intergenerational dialogues with 32 participants across Musanze and Gasabo Districts of Rwanda. The findings demonstrate that structured, facilitated dialogues can create the conditions for meaningful family reconciliation, GBV awareness, and community norm change among young single mothers and their parents. At the same time, analysis of the data reveals that the programme’s impact is substantially constrained by structural inequalities, particularly poverty and male non-participation, which the dialogue model alone is insufficient to address. We engage each of these dimensions in turn.
Benefits and Mechanisms of Change
The family reconciliation gains reported in this study are consistent with evidence from other African contexts that structured communication interventions can reduce intergenerational tension and strengthen family support for young mothers.16,20 The dialogues appear to function through several mechanisms: creating psychological safety for difficult conversations that cultural norms would otherwise foreclose; promoting parental empathy and responsibility; equipping young mothers with communication and conflict-de-escalation skills; and shifting community norms through public modelling of acceptance. These mechanisms are well captured by the dialogue-based conflict resolution framework,15,16 which predicts that structured facilitation enables empathy-building and shared commitment to behavioural change.
The GBV and SRH awareness gains are particularly significant given the deeply embedded cultural taboos around intergenerational discussion of sexuality and reproduction in Rwanda. School-based and community-based programmes in sub-Saharan Africa that address gender norms alongside reproductive health knowledge have been shown to shift young people’s attitudes and behaviours;2 the Ingo z’amahoro dialogues appear to generate similar dynamics at the family level. From an intersectional feminist perspective, these awareness gains represent an important disruption of gendered knowledge hierarchies. However, the predominantly female composition of dialogue participants means that male norms and authority structures remain largely unchallenged, which poses a critical gap given that household decision-making authority in many Rwandan communities resides primarily with men.
Structural Barriers and Critical Reflections
The absence of fathers and male community leaders from the Ingo z’amahoro dialogues is among the most important structural limitations identified in this study. Cultural norms that render intimate discussions between fathers and daughters taboo are well documented in Rwanda and across sub-Saharan Africa.17,20 These norms are not immutable, and the programme may need to develop gender-sensitive male engagement strategies that reframe participation as an expression of responsible fatherhood and community leadership. Engaging male community leaders is also strategically important, given their formal and informal authority in dispute resolution and GBV redress.
The economic constraints experienced by young single mothers raise important questions about the sustainability of relational change achieved through dialogue when material conditions remain unchanged. The political economy of teenage pregnancy in Rwanda, characterised by gender-based educational exclusion, limited female access to formal labour markets, and inadequate social protection, creates conditions in which young mothers’ vulnerability is structurally reproduced regardless of attitudinal shifts.12 The voices of participants in this study are clear: reconciliation without economic support is incomplete. Similar work in Mozambique demonstrates that dialogue-based interventions for young mothers achieve more durable outcomes when coupled with livelihood support.24 The programme should therefore explore formal partnerships with vocational training institutions, social protection schemes, and microfinance organisations.
Social stigma, while partially attenuated by the programme, remained a persistent and sometimes devastating force in the lives of participants. This is unsurprising: as stigma attached to teenage pregnancy in sub-Saharan Africa was shown to be deeply embedded in cultural and religious norms and unlikely to be durably transformed by community dialogue alone.21 The programme would benefit from integrating formal psychosocial support, including group-based peer counselling and individual psychological first aid, to buffer the mental health consequences of ongoing stigma.
Implications for Programme Design
On the basis of these findings, we recommend the following strategies to the Ingo z’amahoro programme: (1) increase session frequency from monthly to bi-monthly to deepen learning; (2) develop targeted male engagement strategies to include fathers and community leaders, framed around responsible fatherhood; (3) integrate formal psychosocial counselling and mental health screening; (4) establish referral linkages with SRHR services, including contraception, HIV testing, and post-abortion care; (5) partner with economic empowerment organisations to provide vocational training, business development support, and childcare during sessions; and (6) document and formalise the peer education role that empowered participants are already informally playing within their communities. Implementation of these recommendations will require adequate resource allocation and partnership development, which should be acknowledged as real feasibility constraints in programme planning.
Limitations
Some limitations should be noted. The study was conducted in two districts, Musanze and Gasabo, and may not capture the sociocultural diversity of other Rwandan contexts. Because participants were recruited through the implementing organisation and had engaged with the programme for at least two years, they may represent a positively selected group; individuals who discontinued participation, had negative experiences, or did not benefit from the programme were not represented, and the findings may disproportionately reflect positive experiences. The gender distribution among parents (11 women and one man) limits the perspectives captured from male caregivers. Most participants were from low-income households, which may have amplified the salience of economic hardship relative to other barriers. The study did not include currently pregnant teenagers, who might have offered fresher and more acute perspectives on their experiences. Future research employing longitudinal designs, or specifically targeting disengaged participants, would further strengthen understanding of programme impact.
Conclusion
This study demonstrates that the Ingo z’amahoro intergenerational dialogues have generated meaningful gains in family reconciliation, GBV and SRH awareness, community attitude change, and self-confidence among young single mothers and their parents in Rwanda. These gains are not trivial: in a context where teenage pregnancy routinely triggers family rejection, social ostracism, and profound economic precarity, creating the conditions for forgiveness, communication, and renewed parental support represents a significant intervention. Additionally, dialogue-based reconciliation is necessary but insufficient. The programme’s impact is constrained by the structural inequalities, poverty, male non-participation, social stigma, and inadequate psychosocial support that shape young single mothers’ lives. Scaling up intergenerational dialogues in Rwanda and comparable settings will require coupling relational with material interventions: economic empowerment, broader male and community leader engagement, integrated SRHR services, and sustained psychosocial support. Future research should examine the long-term durability of programme gains, the experiences of pregnant teenagers who have not yet participated, and the effectiveness of complementary economic and psychosocial components.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
This study was approved by the UGHE Institutional Review Board (UGHE-IRB/2024/301) and was conducted in full compliance with the Declaration of Helsinki. Signed informed consent was obtained from all participants; informed consent explicitly included permission for the publication of anonymised responses and direct quotes. The one participant aged under 18 years provided voluntary assent alongside parental consent.
Acknowledgments
We are grateful to participants in the Haguruka Ingo z’amahoro programme who shared their life stories, and to the Haguruka team for facilitating access.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Adolescent pregnancy [Fact Sheet]; 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy.
2. Leite L, Yates R, Strigelli GC, et al. Scoping review of social norms interventions to reduce violence and improve SRHR outcomes among adolescents and young people in sub-Saharan Africa. Front Reprod Health. 2025;7(1592696). doi:10.3389/frph.2025.1592696
3. World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): guidance to support country implementation. Geneva: WHO; 2017. Available from: https://iris.who.int/handle/10665/255415.
4. National Institute of Statistics of Rwanda (NISR), Ministry of Health (MOH), and ICF. Rwanda Demographic and Health Survey 2019–20. Kigali, Rwanda and Rockville, MD: NISR/MOH/ICF; 2021. Available from: https://dhsprogram.com/publications/publication-FR370-DHS-Final-Reports.cfm.
5. Kumar R. In Rwanda, teenage pregnancies are rising. The cost is high, analysts say. Al Jazeera; 2023. Available from: https://www.aljazeera.com/features/2023/8/25/in-rwanda-teenage-pregnancies-are-rising-the-cost-is-heavy-analysts-say.
6. Umumararungu CK, Bazubagira AK. Complexity of teen mothers and its implications on family wellbeing in Rwanda. Int J Res Bus Soc Sci. 2023;12(4):392–13. doi:10.20525/ijrbs.v12i4.2604
7. Coast E, Mwali MM, Isimbi R, et al. ‘If she’s pregnant, then that means that her dreams fade away’: exploring experiences of adolescent pregnancy and motherhood in Rwanda. Eur J Develop Res. 2021;33(5):1274–1302. doi:10.1057/s41287-021-00438-5
8. Migeprof. The fight against GBV concerns every Rwandan. Ministry of Gender and Family Promotion; 2021. Available from: https://www.migeprof.gov.rw/news-detail/the-fight-against-gbv-concerns-every-rwandan.
9. Ndahimana R, Umutoni NJ, Nteziryayo JP, et al. Prevalence, trends in and determinants of teenage pregnancies in Rwanda: analysis of Rwanda Demographic and Health Survey (2010 to 2020). J Biomed Res Environ Sci. 2023;4:1425–1434. doi:10.37871/jbres1813
10. Dina TM, Suhendi A. Family conflict in E. Lockhart’s novel we were liars. J Language. 2020;1(2):89–100. doi:10.30743/jol.v1i2.2457
11. Cook SMC, Cameron ST. Social issues of teenage pregnancy. Obstet Gynaecol Reprod Med. 2015;25(9):243–248. doi:10.1016/j.ogrm.2015.06.001
12. United Nations Development Program. Rwanda National Human Development Report 2018: accelerating gender equality and women’s empowerment. Kigali: UNDP Rwanda; 2018. Available from: https://www.rw.undp.org/content/rwanda/en/home/library/poverty/nhdr2018.html.
13. Swanson ZT, Nuño CO, Walker RV, et al. “I will cherish this experience for a lifetime:” A qualitative exploration of the benefits of intergenerational dialogue in college students. J Intergener Relatsh. 2025;23(2):177–192. doi:10.1080/15350770.2024.2324335
14. Kvinna till Kvinna Foundation. The Kvinna till Kvinna Foundation in Rwanda; 2023. Available from: https://kvinnatillkvinna.org/about-us/where-we-work/sub-saharan-africa/rwanda/.
15. Urick MJ, Hollensbe EC, Masterson SS, et al. Understanding and managing intergenerational conflict: an examination of influences and strategies. Work Aging Retir. 2017;3(2):166–185. doi:10.1093/workar/waw009
16. Lloyd A, Broadbent A, Brooks E, et al. The impact of family interventions on communication in the context of anxiety and depression in those aged 14-24 years: systematic review of randomised control trials. BJPsych Open. 2023;9(5). doi:10.1192/bjo.2023.545
17. Uwizeye D, Muhayiteto R, Kantarama E, et al. Prevalence of teenage pregnancy and the associated contextual correlates in Rwanda. Heliyon. 2020;6(10):e05037. doi:10.1016/j.heliyon.2020.e05037
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
19. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292(2):114523. doi:10.1016/j.socscimed.2021.114523
20. Agu CI, Agu IC, Mbachu CO, et al. A qualitative assessment of the impact of a community-embedded intervention on beneficiaries’ attitudes and beliefs about adolescent sexual reproductive health in Ebonyi State, Southeast, Nigeria. Reprod Health. 2024;21(1). doi:10.1186/s12978-024-01738-9
21. Feyissa GT, Tolu LB, Soboka M, et al. Effectiveness of interventions to reduce child marriage and teen pregnancy in sub-Saharan Africa: a systematic review of quantitative evidence. Front Reprod Health. 2023;5:1105390. doi:10.3389/frph.2023.1105390
22. Reschly AL. Interventions to enhance academic engagement. In: Student Engagement: Effective Academic, Behavioral, Cognitive, and Affective Interventions at School. 2020:91–108. doi:10.1007/978-3-030-37285-9_5
23. Cooke P, Hodgkinson K, Manning P. Changing the story: intergenerational dialogue, participatory video and perpetrator memories in Cambodia. Mem Stud. 2023;16(5):1223–1239. doi:10.1177/17506980221108474
24. Salvi F. Teenage pregnancy and education in the Global South: the case of Mozambique; 2019. Available from: https://www.routledge.com/Teenage-Pregnancy-and-Education-in-the-Global-South-The-Case-of-Mozambique/Salvi/p/book/9781032241258.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.