Back to Journals » Patient Preference and Adherence » Volume 15
Exploring Culture, Religiosity and Spirituality Influence on Antihypertensive Medication Adherence Among Specialised Population: A Qualitative Ethnographic Approach
Authors Abdul Wahab NA, Makmor Bakry M ![]() , Ahmad M, Mohamad Noor Z, Mhd Ali A
, Ahmad M, Mohamad Noor Z, Mhd Ali A ![]()
Received 21 May 2021
Accepted for publication 21 August 2021
Published 5 October 2021 Volume 2021:15 Pages 2249—2265
DOI https://doi.org/10.2147/PPA.S319469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Noor Azizah Abdul Wahab,1,2 Mohd Makmor Bakry,1 Mahadir Ahmad,3 Zaswiza Mohamad Noor,2 Adliah Mhd Ali1
1Centre of Quality Management of Medicines, Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Kuala Lumpur, 50300, Malaysia; 2Faculty of Pharmacy and Health Sciences, Universiti Kuala Lumpur Royal College of Medicine Perak, Perak, 30450, Malaysia; 3Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, 50300, Malaysia
Correspondence: Adliah Mhd Ali
Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia
Tel +603-9289 7964
Fax +603-2698 3271
Email [email protected]
Background: Hypertension is one of the major risk factors of stroke and leading risk factors for global death. Inadequate control of blood pressure due to medication non-adherence remains a challenge and identifying the underlying causes will provide useful information to formulate suitable interventions.
Purpose: This study aimed to explore the roles of culture, religiosity, and spirituality on adherence to anti-hypertensive medications.
Methodology: A semi-structured qualitative interview was used to explore promoters and barriers to medication adherence among hypertensive individuals residing in urban and rural areas of Perak State, West Malaysia. Study participants were individuals who are able to comprehend either in Malay or English, above 18 years old and on antihypertensive medications. Interview transcriptions from 23 participants were coded inductively and analyzed thematically. Codes generated were verified by three co-investigators who were not involved in transcribing process. The codes were matched with quotations and categorized using three levels of themes named as organizing, classifying and general themes.
Results: Cultural aspects categorized as societal and communication norms were related to non-adherence. The societal norms related to ignorance, belief in testimony and anything “natural is safe” affected medication adherence negatively. Communication norms manifested as superficiality, indirectness and non-confrontational were also linked to medication non-adherence. Internal and organizational religiosity was linked to increased motivation to take medication. In contrast, religious misconception about healing and treatment contributed towards medication non-adherence. The role of spirituality remains unclear and seemed to be understood as related to religiosity.
Conclusion: Culture and religiosity (C/R) are highly regarded in many societies and shaped people’s health belief and behaviour. Identifying the elements and mechanism through which C/R impacted adherence would be useful to provide essential information for linking adherence assessment to the interventions that specifically address causes of medication non-adherence.
Keywords: hypertension, medication adherence, cultural, religiosity, spirituality
Introduction
Hypertension as Risk Factors for Non-communicable Diseases
Non-communicable diseases (NCDs) have posed a significant challenge to society. An estimation of 32% of 17.9 million deaths yearly were due to non-communicable diseases .1 Uncontrolled hypertension (systolic BP greater or equal to 140mmHg and diastolic BP greater or equal to 90mmHg) increases the risk of cardiovascular diseases (CVDs) and being one of the risk factors of NCDs causes high mortality and morbidity.2 Studies confirmed that risk of death due to CVDs and cerebrovascular disease was higher among patients with uncontrolled hypertension compared with normotensive patients.3 Raised blood pressure is one of the major cardiovascular risk factors and leading risk factor for global death. Globally, ischemic heart disease and stroke were among the top leading causes of death in 2019.4 Approximately half of the deaths due to heart disease and stroke were associated with hypertension.5 In Malaysia, the total number of reported deaths due to NCDs were 113,400 (74%) and the probability of premature death from NCDs was 17%.6
Medication Adherence Among Hypertensive Patients
Studies suggested that non-adherence behaviour could be predicted based on its’ association with sociodemographic variables such as gender, age, ethnicity, religious affiliation, marital status, household, education background, employment status, and income.7–10 Other predictors included comorbidity,7,9,10 polypharmacy,11,12 health belief13 and health literacy.14 Knowledge associated with these predictors would facilitate formulation of various interventions to improve medication adherence. The challenges lie upon the ability of healthcare providers to adapt to these findings and utilize them in a suitable way to their context.
In recently published National Health and Morbidity Surveys (NHMS 2019), 3 in 10 or 6.4 million people have hypertension. However, only half of them were aware of having hypertension. Among those that received treatments only 45% had their blood pressure controlled.15 Overall prevalence of hypertension among adults aged 18 years old and above was 30%.15 In Malaysia, uncontrolled hypertension remains a challenge despite free access to consultation and treatment in any public health facilities managed by the Ministry of Health (MOH), which are heavily funded by the government and had the highest spending compared with other sectors.16
Numerous studies have shown that among patients prescribed with antihypertensive medications between 10–55% failed to take their medications diligently.7,17–22 Non-adherence to antihypertensive medication causes uncontrolled blood pressure and increased risk of cardiovascular complications.18
Various interventions were tested and among those is counselling which has been proven effective for the targeted population.23 Intervention that took into account the uniqueness of the targeted population often resulted in improvement of blood pressure control and adherence.24,25 A recent study comparing the effect of educational intervention by healthcare practitioners with and without communication training also showed improvement in hypertension outcomes and also medication adherence.26 A systematic review of qualitative studies indicated that healthcare providers and educational interventions should engage with patients’ concerns and experience of side effects and symptoms of their illness as well as their ideas about causes of hypertension.27
As knowledge about illness is influenced by culture and traditions,28 understanding of the elements in culture that affect patients’ views of illness and treatment would be beneficial to improve the adherence intervention outcome.
Culture, Religiosity and Spirituality
Other important social determinants which have long been associated with certain health behaviour are culture, spirituality29 and religiosity.30–33 Studies related to culture have proposed multiple definitions which differ and often are inconsistent between various disciplines. Nevertheless, culture consists of ideas, values and assumptions about life which are shared and transmitted by people especially those living in the same geographic location and who communicate using the same language.34 Culture is often passed down between generations either explicitly or implicitly35 and people adopt common behaviour within the family unit and the society. Over time, the definition of culture has changed across disciplines.36
Religiosity and spirituality are often used to describe experience of connection with the transcendent, sacred or divine.37 Additionally, religiosity involves affirmation and commitment in organized religion and is often seen as a formal or outward expression of the relationship with the sacred. Whereas, spirituality is often referred to as an individual search for connection with the sacred or an experience that may lead anyone to examine their existence.37 The definition of spirituality itself allows people to define it according to what it means to them.38 Religiosity and spirituality have also been described as overlapping constructs.39 The terms pertaining to religiosity and spirituality are used and understood differently across cultures.39
People who associate themselves with some religious traditions and practices were reported to engage in more healthier choices.33 Positive impact of religiosity related to religious belief was reported to reduce resistance to treatment.40 Organizational religious activities (ORA) had both positive41,42 and negative impacts43 on medication adherence. The effect of religiosity and spirituality (R/S) varies between different study populations in which positive correlation was seen in one population but in others R/S correlated negatively.44 The relationship remains unclear and requires further exploration. The contradicting impacts of ORA were anticipated as these studies were conducted in different cultural and religious settings in which the societal norms and their religious practices could differ significantly. Similarly, prayer had both positive45 and negative impacts46 on medication adherence. A recent study on resilience, religiosity and treatment adherence suggested that negative religious coping (NRC) by some patients was not related to their commitment to religion.47 Patients may encounter other problems related to discrimination or deprivation of healthcare services that force them to have inappropriate reliance in God or divine power as their coping mechanism.48
In relation to spirituality, studies have shown that having fewer symptoms of anxiety, stress and depression was associated with greater spiritual well-being. As stress was also found to increase the odds of non-adherence,49 improving symptoms of stress could also improve adherence. Other studies have reported negative association29 or no association between spiritual or religious belief with medication adherence.50
Cultural factors has been linked to the positive51 and negative impacts52 on medication adherence. Additionally, studies have also highlighted racial disparities53,54 in medication adherence. A negative influence of culture was linked to lower perceived susceptibility to the disease52 while the positive influence was significantly linked to health literacy.51
In Malaysia, the majority of Malaysians across the ethnic groups identified themselves with religious belief including Islam (66.1%), Buddhist (15.7%), Christians (9.4%) or Hinduism (5.5%) and unaffiliated are less than 1%.55 Islam being the religion of Bumiputera Malays is the basis of Malay identity56 and plays a significant role in their cultures and values. The flow of either culture or religious elements into each other could have contributed towards promotion or inhibition of medication adherence. Malaysia being part of the Malay Archipelago has unique cultural characteristics which are more collectivist in nature57 and people naturally align themselves with societal norms and expectations.58 The Malays, for example, embrace self-effacement and conflict avoidance59 in daily interaction and value the role of kinship, family, and community in decision making.
This study aims to explore the roles of culture, religiosity, and spirituality on patients’ adherence behaviour using a qualitative ethnographic approach. Understanding the underlying reasons for this behaviour could provide valuable insights and direct future development of non-adherence risk assessment and intervention.
Methods
Study Design
A qualitative ethnographic approach was used to gain an in-depth understanding of CRS influence on patients’ experience related to medication taking. Ethical approval was obtained from the National University of Malaysia (UKM) Research Ethics Committee (UKM/PPI/111/8/JEP-2019-138).
Study Setting
This study explores the influence of cultural, religiosity and spirituality (CRS) on medication adherence among individuals diagnosed with hypertension in the state of Perak, which is one of the top three states with the highest incidence of hypertension in Malaysia. Participants were selected from both rural and urban areas.
The majority of study participants are Malay Muslims, who make up the largest ethnicity in Malaysia. The main communicative language is Malay and English is the second language. A small number of study participants are Chinese, Indians and Indigenous people (Orang Asli).
The interview questionnaire guide used in the study was developed based on recently published research,29,40,41,46,51,60,61 opinions of experts and guided by objectives of this study (Figure 1: Interview Questionnaire Guide Development Process). Exploration of the CRS role on medication adherence were done inductively without attachment to any existing theory to facilitate generation of new perspectives to the existing role.
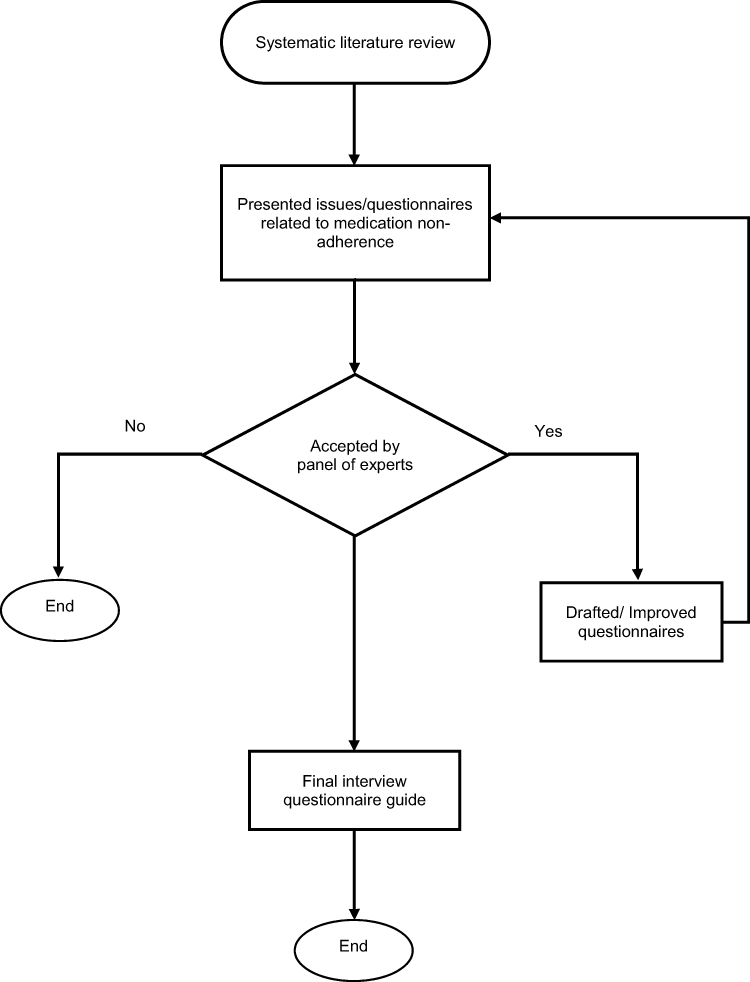 |
Figure 1 Interview questionnaire development process. |
Participant Recruitment
The study was conducted between April and August 2019. Study participants were patients diagnosed with hypertension and prescribed with antihypertensive medications. During the interviews, probing was done until the researcher was satisfied that participants’ perspectives were thoroughly explored. The number of participants recruited was also based on data saturation which is signalled by no new issues or themes identified during the interviews and data analysis.62,63 In general the number of participants considered to be sufficient would depend on the context of the study and based upon whether the data have satisfactorily explained the scope of research.63 Potential participants were identified through screening of blood pressure at various community pharmacies, community centres and shopping complexes. Some of them were identified through personal contacts of study participants. Potential study participants were then invited to take part in the study and appointments were set for the face-to-face interviews. Confirmation of the diagnosis were made by the pharmacist through checking of the prescriptions and appointment cards with patient details during a visit at their home or workplace. The process of identifying potential study participants is illustrated in Figure 2 (Recruitment process).
 |
Figure 2 Recruitment process flowchart. |
Individuals who were able to comprehend either in Malay or English, above 18 years old, diagnosed with hypertension and willing to participate were included in the study.
Arrangement for the face-to-face interview were made according to participants’ convenience and availability. Interviews were conducted either at participants’ home, their working place or community pharmacies and public facilities suitable for private conversations. Interview sessions lasted between 30 minutes to more than an hour depending on participants’ responses. Semi-structured interview questionnaires guide (Table 1: Semi-structured Interview Guide) was used to facilitate the discussion. Recruitment of participants was finalised at the point when no new data were identified and similar codes were generated from the transcriptions of the last few interviews. At this point, data saturation were decided based on the judgement that there is diminishing return and little need for further recruitment.64
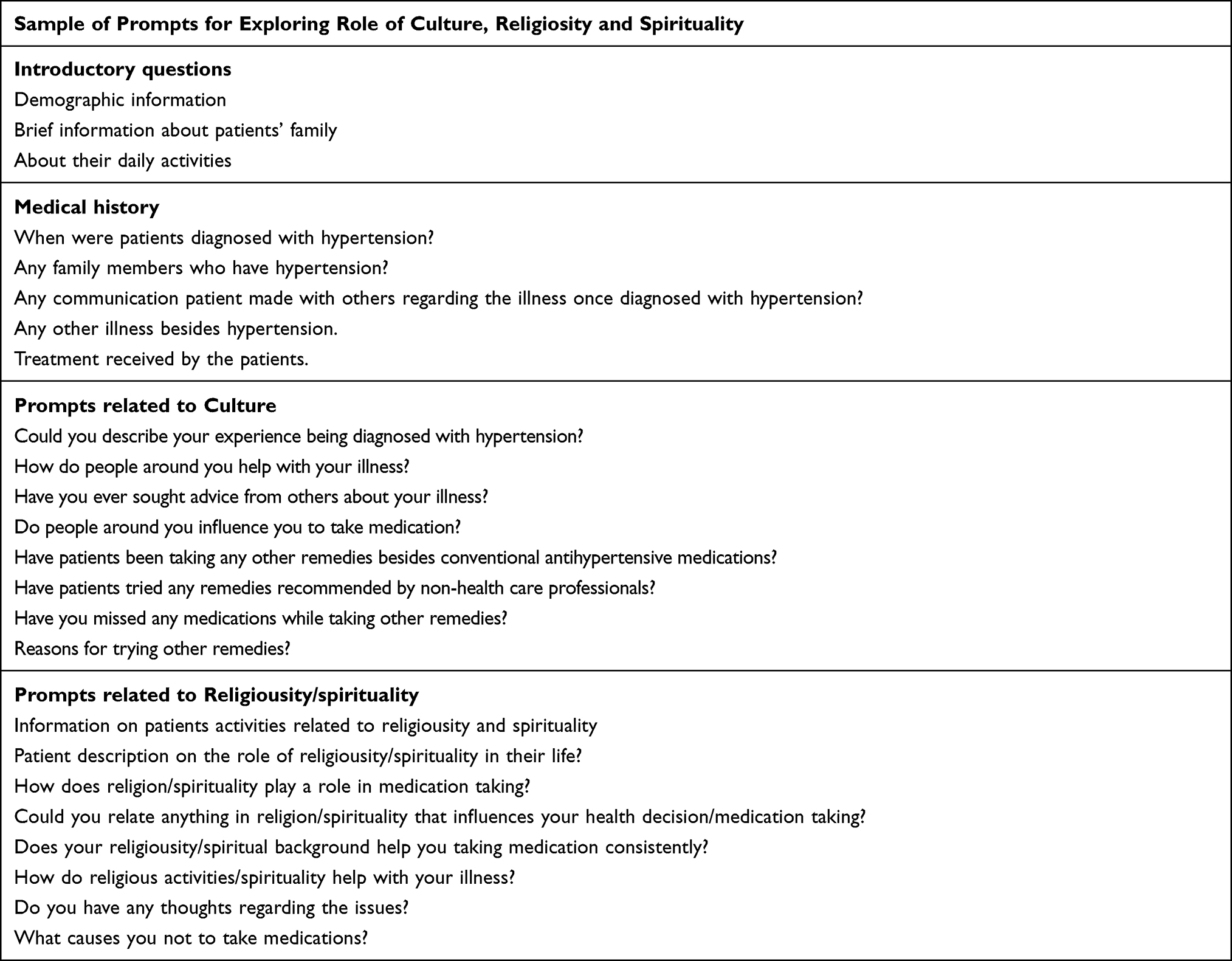 |
Table 1 Summary of Semi-Structured Interview Guide |
Data Collection
Prior to the interviews, both verbal (face to face or phone calls) and written consents which included publication of anonymized responses from the participants were obtained. The study was conducted in accordance with the Declaration of Helsinki. Individual interviews were conducted in the form of discussion either at participants’ homes, community pharmacies or public places, as agreed by both participants and interviewer. All interviews were conducted in Malay as our study participants were able to understand and also respond meaningfully. English was only used to elaborate some of the queries from a few participants who preferred to communicate in this language and some of them used both languages in communicating. The interview sessions were audio-taped and notes were taken to ensure important points were recorded. Study participants were given general information about the purpose of the study, potential contribution to improve medication adherence and potential risk to them. The participants were briefed on the voluntary basis of their participation and the right to withdraw from the study at any time.
All the interviews were conducted by the same individual and the data were verified by three other researchers to minimize any bias. The interview sessions were conducted by one interviewer (abbreviated as NAAW) from April to early August 2019, and a total of 23 participants were included in the study. Nine participants were from urban and 14 were from rural areas.
Data Analysis
The recorded interviews were transcribed verbatim and compared with the audio-tapes. Transcriptions of the interviews were coded inductively using Atlas-ti and the codes generated from relevant quotations were presented and checked by the principal investigator (abbreviated as AMA) and another two co-investigators (abbreviated as MM and MA) multiple times. The six-step framework for conducting thematic analysis was used to ensure rigour in synthesizing the results.65,66
Analysis of the codes generated from interviews was conducted multiple times. Three levels of themes were used to explore and define CRS related factors from participants’ perspectives. At the first level of thematic analysis, all of the codes generated and the transcripts were read and presented to the other three investigators who were not involved in the transcribing process. In the second stage of analysis, the codes were matched with quotations and grouped using three level of themes i.e. organizing, classifying and general themes. The process of checking and matching of the codes, quotation and themes were repeated several times and the codes which represented participants’ views and experience were finalized by consensus. Table 1 shows a sample of semi-structured interview prompts used in the interviews. However, these prompts were non-exhaustive and were adapted based on participants’ responses and comprehension.
Results
General Characteristics of Study Participants
Out of 40 individuals who were invited to participate in the study, 23 participants consented. The response rate was 57.5%. Table 2 (General characteristics of study participants) shows that more than half of the participants were from a rural area. The majority of them are Malays, while Chinese, Indians and indigenous people (Orang Asli) constitute less than one third of the total participants. Less than 20% of the participants had normal BP (systolic BP: 120–129 mmHg, diastolic BP: 80–84 mmHg).
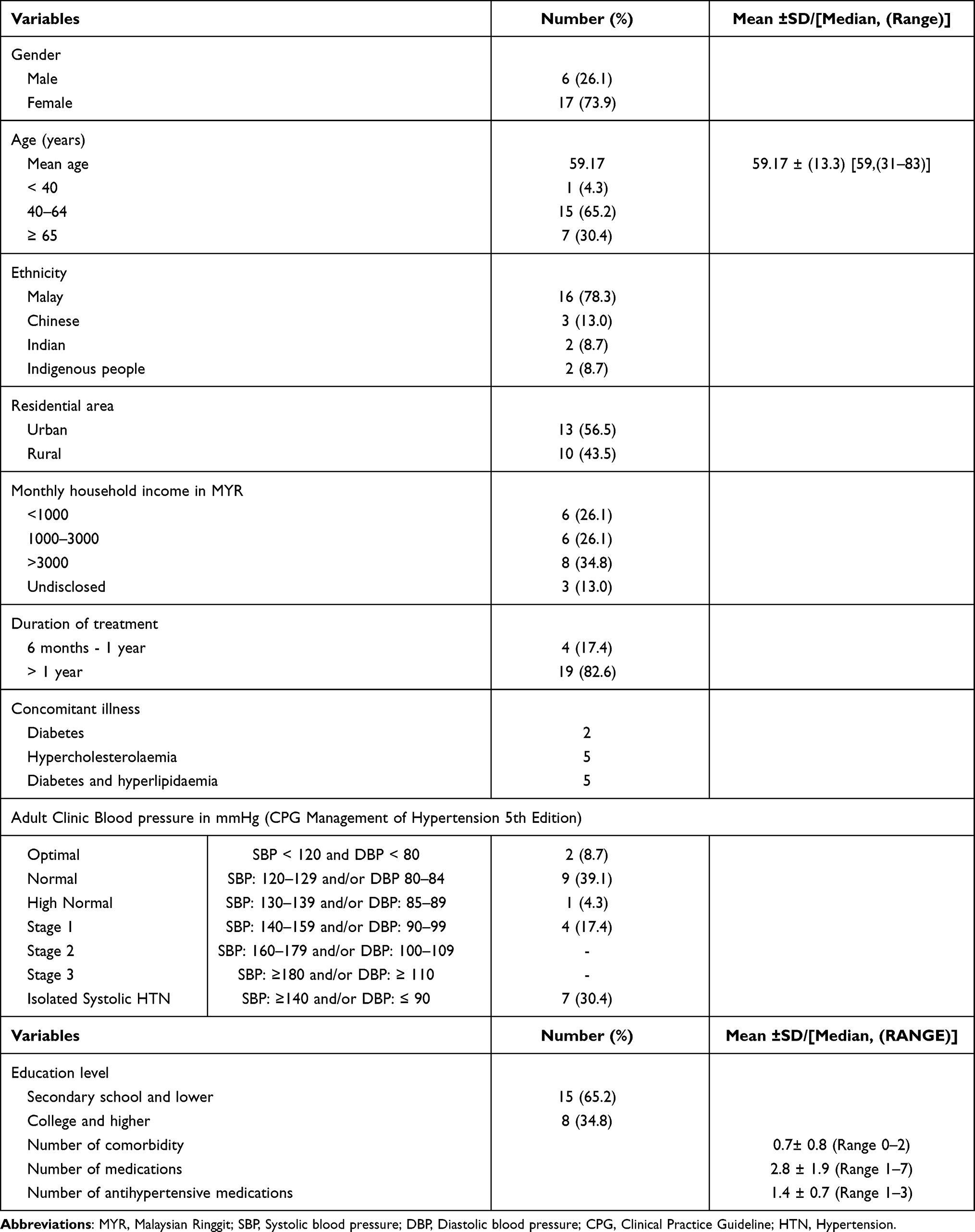 |
Table 2 General Characteristics of Study Participants (n = 23) |
More than half of the study participants either had secondary school education or lower, reside in rural areas and most of them are of Malay ethnic. A low number of Chinese and Indian participants was mainly due to the language barrier. Correlation analysis revealed no significant correlation between patients’ characteristics with BP control (<140/90 mmHg) as depicted in Table 3 (Table 3: Correlation of selected variables with BP control).
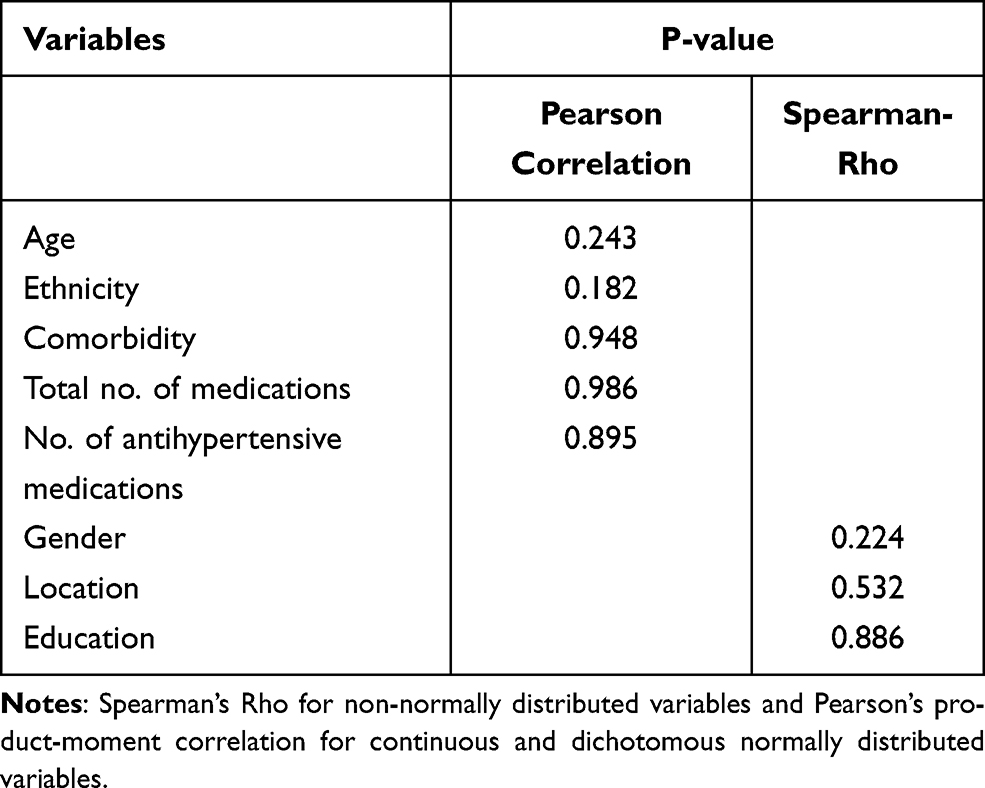 |
Table 3 Correlation of Selected Variables with BP Control |
Coding and Thematic Analysis
A total of 104 codes were generated inductively from the transcriptions of which 17 codes were categorized as cultural related themes, 8 religiosity or spirituality related themes and the remainder were classified as others.
Illustration of the influence of culture, religiosity and spirituality on medication adherence is as shown in Figure 3 (CRS influence on medication adherence).
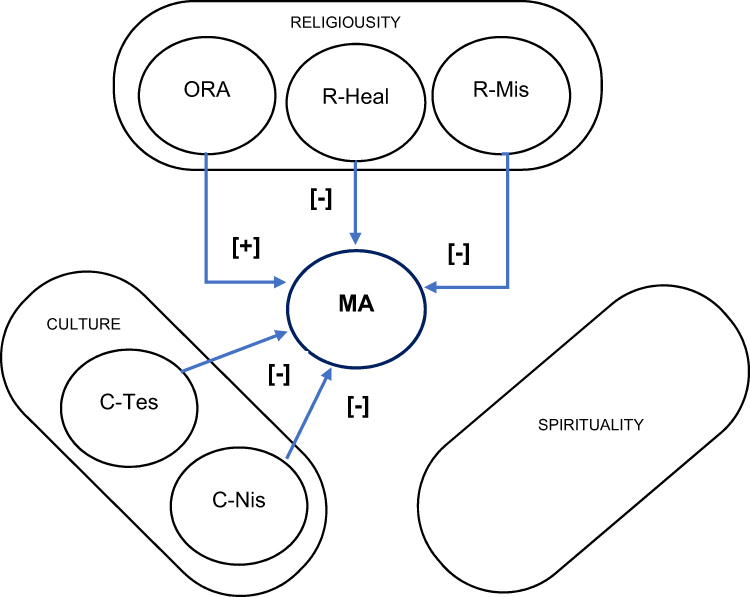 |
Figure 3 CRS Influence on medication adherence. Abbreviations: MA, Medication adherence; ORA, Organised Religious Activity; R-Heal, Religious Related Healing; R-Mis, Religious Misconception; C-Tes, Culture-Testimony; C-NiS, Culture-Natural is Safe; [+], Positive effect; [-], Negative effect. |
Influence of Culture on Medication Adherence
Cultural elements, identified through responses related to pattern of behaviour grouped as societal norms and communication norms, exhibited a negative influence on medication adherence. For societal norms, the pattern of responses identified as “trust non-healthcare professionals”, “guide decision making” and “natural is safe” referred to verbal information, advice or experience from non-healthcare professionals. Information, advice or an account of personal experience were classified as “testimony”.
Some of the study participants exhibited specific patterns of communication when dealing with healthcare professionals, family members and acquaintances in relation to their illness. These patterns were identified as “superficiality”, “non-confrontational” and “indirectness” and grouped as communication norms.
Societal Norms: Testimony (Trust Non-Expert, Guide Decision Making, Natural is Safe)
Trust Non-Expert
The study findings suggested that verbal and written statements by non-experts were accepted as testimony and used to guide participants’ decisions related to treatment adherence. Some of them reported to have consulted family members and friends before initiating their medications. Others admitted that the information or advice from people known to them without formal medical training are important in helping them to decide on following the treatment. It was often observed that when participants mentioned “other people said … ”, it has a connotation of referring to non-expert advice.
“Seek others’ opinion. Asked friends, to find out how to deal with it (illness).” (P04: 72-year-old Malay woman).
Experience of others in relation to the effects and effectiveness of treatment is widely practiced by the participants and were regarded as important to aid the decision on starting medications.
“I asked others experience. I asked them and we talked about whether it is good to take the medications”. (P07: 60-year-old Malay woman).
One of the male participants mentioned that he believes that the dose should be adjusted by patients. He would reduce the dose when he feels healthy and he also advised his friends to do the same.
“You don’t have to take the medicine three times a day, you just take once or twice”. (P05: 74-year-old Malay man).
He argued that those who have the illness know themselves better and they should be able to decide and adjust their medications as they believe appropriate.
Another advice from non-HCP was related to the need to be cautious in starting medications as it would cause one to be dependent on it for life. Being on medications was associated with being dependent on it and not good for the participants.
… because other people said if you start taking the medications you cannot stop and that is what the doctor described as well. Once you start, you cannot skip the medications. (P015: 31-year-old Malay man)
Advice from others was valued as they provide living examples of how they manage their own illness and are experiencing the effect of medications.
Natural is Safe
Besides sharing experience related to illness and medications, some participants reported that they received recommendations on alternative and natural remedies from families and friends. For some participants, they have ingrained ideas that anything natural is free from “drugs” and their side effects. Medications are often equated as “drugs” which carries negative connotations. Natural remedies were perceived as safer than medications because of the belief that it does not contain “drugs”. For them, anything associated with drugs have potential side effects and perceived as less safe compared with natural remedies. Alternative treatments or natural remedies were perceived as free from harmful effects and able to delay and even prevent them from depending on medications for hypertension as described in the following statement.
… if possible I would opt for natural way. I would take herbs as others said it is good. I would take it once a week … I do not want to end up taking medications. (P07: 60-year-old Malay woman)
One study participant reported that she adjusted her medication time while taking alternative treatment. She admitted to delaying administration of medications while on homeopathy remedies and took alternative remedies because she believes it is effective.
“I took the medication but I delay it. If it supposed to be taken in the morning, I will take it mid-day … ”. (P04: 72-year-old Malay woman).
Among the study participants, unverified information was well accepted, as described by one participant who sees herself as being well-informed and admitted to obtaining information through internet search.
“… I already knew. I know a lot of things related to this … I read about effects of medication consumption.” (P07).
In contrast, participants with higher education level were more sceptical of any information obtained from non-healthcare professionals. They would rather rely on doctors or pharmacists for health-related advice or information. This is well expressed by one of the participants.
Actually some Chinese medicines they are quite good in certain ways, but to me what I believe is Chinese medicines are for those acute cases. There might be ways to work with it. All the chronic ones no, like hypertension, high cholesterol or some other chronic cases. … I don’t really believe that because there may be no clinical study, we don’t have any evidence to prove it really lower down your BP or cholesterol or diabetes. (P22: 44-year-old Chinese man)
Communication Norms: Communication Styles (Superficiality, Non-Confrontational and Indirectness)
There were three communication styles identified as superficiality, non-confrontational and indirectness. Superficiality refers to lack of thoroughness and depth in communicating which often led to misunderstanding of the messages conveyed and causes unwanted reaction from the recipients. In this context, for example, information about diseases and complications was conveyed in a simplified manner which was often understood inaccurately.
Non-confrontational refers to a diplomatic approach mainly aimed to avoid hostility and to deal with situations calmly. Non-confrontational approach was often followed by indirectness in conveying messages as not to offend the recipients. Indirectness in communication could also be described as being subtle, delicate and in a polite manner.
Superficiality
One of our study participants admitted to refusing to take medication due to numerous bad stories related to long-term effects of hypertensive medications. She was very concerned about potential kidney dysfunction due to consumption of medications over a long period of time. Lack of thorough understanding related to the disease and treatment leaves the participants with limited options but to accept unverified information.
I do not want to take medications. I heard a lot of things. People said taking medications is dangerous. They said if you took it for ten or fifteen years, it would eventually damage your kidney. (P11: 44-year-old Malay woman)
In contrast, another participant admitted that she felt obliged to take her medications diligently when the doctor advised her concerning the potential effect of organ dysfunction due to non-adherence.
My doctor always said if we frequently missed taking our medications, blood pressure would be high and causes damage to kidney. I got scared … I am scared of the effect. (P02: 59-year-old Malay woman)
A few participants perceived taking medications as a threat to their health that outweighs the benefit of slowing down disease progression. Dependency on medications was perceived as a bigger threat than controlling the disease itself. Fear of being dependent on medications and the presence of distorted understanding related to the treatment and disease could possibly lead them to neglect professional advice. In addition, lack of thoroughness and in-depth understanding related to illness and treatment were observed. There is alarming evidence of shallowness and superficiality in making sense of the communicated information.
Another participant refused to even start taking the medications because the information from others confirmed her concerns that it would be impossible to be free from medications once started. The fear of being dependent on medications for life seems to be greater than the worry about their own illness.
“We cannot stop once we start taking the medications. So, when my parents advised me … I said, ‘I do not want to start taking it’ … ” (P08: 47-year-old Malay woman).
Another participant shared a similar belief as illustrated through his statement. The participant understood the phrase “cannot skip” as equivalent to “cannot stop” or being dependent on medications for life.
because other people said if you start taking the medications you cannot stop and that is what the doctor described as well. Once you start, you cannot skip the medications. (P015: 31-year-old Malay man)
This evidence suggests that some communication norms may have contributed towards fear of being dependent on drugs and eventually leading towards non-adherence behaviour.
Non-Confrontational and Indirectness
The non-confrontational nature of the Malays is related to their behavioural characteristics of being self-effacing and conflict avoidance.59 In order to avoid conflicts they always resort to being subtle and often use indirect communication.
One participant reported that her communication with the doctor was undesirable. She admitted that she feels uncomfortable being told about the complications of the disease and felt that the doctor was trying to scare her and this has caused her to be more stressed.
He said I would get this and that (referring to disease complications) … Seems like he is trying to scare me. I don’t like that. It makes me feel more stressful. [P07: 60-year-old Malay woman]
Similar responses were also recorded in other participants which suggests the inability to tolerate revelation of facts in an open and direct manner. Participants reacted negatively by rejecting the advice given by healthcare professionals. The advice was seen as a scaremongering and confrontational.
She said (referring to the doctor), ‘Do you know that your veins are small and you are already aged ….’. Then the doctor told me not to take the supplements. He said ‘Do not take anything except medications supplied by the hospital’ … I did not take the medications at all. (P07: 60-year-old Malay woman)
Participants expressed dislikes as some advice or health information directly relate their health condition with disease complications and sounded as threatening. This style of communicating is known as indirectness.
Impact of Religiosity on Medication Adherence
This study found three elements of religiosity classified as organized religious activities (ORA), misinterpretation of religious concept (R-Mis) and religious related healing (R-Heal) that influence medication adherence. Organizational religiosity improved medication adherence while misinterpretation of religious concept and religious related healing caused medication non-adherence.
Religiosity: Organized Religious Activities, Misinterpretation of Religious Concept and Religious Related Healing
Organized Religious Activities
Our findings suggested that organizational religiosity improved medication adherence. Some participants reported that being involved with a religious community improved medication adherence and provided a source of motivation to take medications diligently. A few participants admitted that they took medications as prescribed to stay healthy and be able to join religious activities in their communities.
“I want to stay healthy. As long as I can perform my prayer and go to place of worship. That is what I want.” (P01: 80-year-old Malay woman).
I wanted to try religious product for high blood sugar. There are products that can reduce blood sugar and blood pressure. So I don’t have to continue my medications. (P08: 47-year-old Malay woman)
Misinterpretation of Religious Concept
Misinterpretation of religious concept had a negative impact on medication adherence. Statements by a few of the participants suggested that they view treatment as either religious or non-religious.
Participants who claimed that they have been taking medications diligently seem to relate their understanding of religious concept with illness in a positive way. They understood that taking medications is one of the ways they could act in tandem with their religious principles.
“Prayer is just part of it that helps you overcome certain things. But we just believe that God will … always help those that help themselves. …” (P22: 44-year-old Chinese man).
Another participant viewed that being religious required her to be evidence-based. The participant reported that she would not take any remedy which is not proven even though recommended by somebody with religious authority.
“Yes, but I did not take it (referring to health products recommended by those with religious authority) because it is not proven.” (P03: 52-year-old Malay woman).
Religious Related Healing (RRH)
Belief in the superiority of religious related healing compared with prescribed medicines seems to be the reason for avoiding medications in some participants.
A number of participants literally view religion as the source of solutions for both their spiritual and physical illness. One of the participants described religious related healing as superior than prescribed medications.
“Religious healing focus more on our spiritual. Medication only helps.” [P08: 47-year-old Malay woman].
She resorted to religious healing because of the belief that taking medications could harm her and may cause dependence on medications. She referred to medications as “drugs” which seem to have negative connotations and undesirable effects on the body. The participant also confessed that religious related healing provided hope for healing.
“Dad, I want to try other method, I do not want to depend on these medications. They are drugs and taking it can affect your body. If I use religious healing … ”. My father burst into anger. I just have to listen to him … ” (P08: 47-year-old Malay woman).
Spirituality
None of the findings could be related to dimensions of spirituality as study participants always referred their experience within the context of their religious belief. An example of a participant who admitted to doing some religious rituals only to respect her parents admitted that religion or spirituality do not have any significant role in her life.
“It does not play a role in my life also. I just pray what I want to the God. That’s it. (P20: 60-year-old Chinese woman).
She denied any R/S influence when asked whether her belief had any influence on motivation to take medications.
“Nothing of that sort” (P20: -year-old Chinese woman).
In summary, our study could not trace any influence of spirituality on medication adherence as our study participants always linked their experience either within the realm of religion or none at all.
Discussion
Cultural Related Barriers to Antihypertensive Medication Adherence
This study found that some elements in societal and communication norms impacted medication adherence negatively, which include belief in testimony and having unique communication styles. Previous studies suggested that culture had both positive51 and negative impacts67–69 on health behaviour. Cultural barriers have prevented patients from having adequate understanding of the illness and medications.61 Some cultural factors were linked to lower perception of susceptibility to diseases.52 Recent study had identified some cultural factors believed to have influenced patients’ discontinuation of medication.70 Yet, at least one study reported a positive impact of culture on health literacy and its significant contribution towards improving medication adherence.51 These findings suggest the influence of cultural factors in shaping patients’ perception and belief regarding illness and medications as well as on the necessity of taking medications.
The impact of culture was more obvious among Malay participants and other ethnics who lived among the Malays compared with those living among the same race. Regular interaction between different ethnics allows flow of some traditions and beliefs between them. The situations were different for individuals with higher educational level as they were less affected by the negative influence of culture regardless of their racial background. Higher education level could have improved an individual’s ability to discriminately use advice or passed down health-related practices.
Among the Malays, using verbal and written testimony from non-experts was perceived as normal among participants. This has led them to either withhold or totally neglect taking medications as prescribed. Some of the testimonies were related to their personal experience of medications’ side effects and also news that they have heard from others who were also taking antihypertensive medications. Belief in testimonials was a unique characteristic of our participants which could be traced to the larger population. A study conducted among patients with type 2 diabetes mellitus reported that social influences from family members, friends and peers impacted patients’ choice of treatment.71
Trust in non-expert people who are either well known by the participants, their own family members or relatives suggested that any information or advice from an individual regarded as trustworthy were often accepted as the truth. Hence, the information or advice from trustworthy individuals would naturally be accepted as reliable. Through feedback obtained during the interviews, more than half of the participants emphasized families and friends as source of information and advice that they relied on when making important decisions regarding their health matters. This scenario was common among those with lower education background and could be related to health literacy.
Testimony as defined in most dictionaries is a formal written or spoken statement especially one given in a court of law. It can also refer to evidence or proof of something. In the context of health, testimonials are usually obtained from those who have used the products or services often used to market products, treatment or services. Testimonials were also used to improve perceived severity of illness, perceived vulnerability and to help individuals making informed decisions related to medications and other treatment.72 Studies have shown that testimonials improved health attitudes and outcomes.72
Testimonials which are also known as first-person narratives, first person perspectives, anecdotal evidence and case history have unique appeal to patients and capable of motivating the patients to decide on doing things that benefit themselves.72
Contrastingly, this study suggests that testimonials appeal to patients in a negative way and motivate them to neglect their medications. One of the most plausible explanations for this behaviour could be related to the element of trust that exists between patients and the influencers. People rarely trust others completely, instead trust is related to particular things73 and given as a result of something in exchange either between two individuals or more than that.
Belief in testimonials related to natural remedies appears to be common and linked to the belief that anything natural is safe. Inclination towards using natural remedies has led some of the participants to defer from taking their antihypertensive medications. It was observed that for some of the participants, the use of natural or herbal remedies came about when they realized the need to take medications for life. They tried alternative remedies as they provide some hope of being cured. Previous studies suggested that belief and preference towards traditional and complementary medicines was associated with non-adherence.74,75,76 Use of herbs was often believed as the natural way of treating the illness and acceptable in some communities.75 Preference of CAM could also be motivated by the fear of being dependent on drugs and the concern related to kidney or liver dysfunction.
Other important aspects of culture are communication norms, which are characterized by superficiality, non-confrontational and indirectness. These norms seem to act as barriers to medication adherence. Superficiality in communication was understood as lack of depth in communicating health-related information which could have caused distortion or loss of actual meaning during transmission of the information. The findings were parallel with a study that examined cultural values in communication in which indirect communication was used to deliver certain information considered to be sensitive and offend others.77 Another study has also reported the use of politeness and indirectness in communicating certain messages among this community.78 Indirectness which has both positive and negative effects on communication is known as a cultural identity of the Malays79 and rooted in Islam which is the religion of the Malays. Indirectness is often used to maintain respect and politeness which are characterized by being meticulous and subtle in the choice of words. Additionally, paraphrasing is also commonly used to improve the message and to make it sound less offensive in order to avoid conflict.77 Indirectness in the context of this study refers to a potentially “offensive direct way” of communicating information related to hypertension and its treatment.
The direct way of conveying the information and advice to patients by HCPs as reported by study participants could have caused misunderstanding and rejection of the message.
The unique ways in communicating messages signalled the need to acknowledge the importance of communication norms in delivering the health information to patients. Failure to communicate effectively would be a challenge towards effective implementation of policies and intervention. Finally, it could also cause mutual distrust between patients and healthcare providers.80
On top of that, being superficial and gullible in accepting information or advice from others complicate the matter. Patients with these traits are inevitably at risk of medication non-adherence. Through identifying culturally related risk factors and understanding how they amplify medication non-adherence, the issues of non-adherence could be solved pragmatically.
Religiosity Related Promoters and Barriers to Antihypertensive Medication Adherence
This study revealed both positive and negative impacts of religiosity on medication adherence. Belief that God heals seems to be confused with associating it to anything labelled or promoted with religious-related language. Contrastingly, internal religiosity motivates some participants to be adherent to their medication schedule as it is seen as fulfilling religious duty as adhering to treatment schedules was seen as an act according to what God wanted them to do. A similar notion was also highlighted in previous studies conducted locally41 and abroad.40,45,81,82
Other promoters of adherence were related to organizational religiosity. Involvement in community religious activities provides relief as participants relate it to being a “good religious devotee” and blessed by God. Hence, they look forward to such events. Participants were motivated to take medication as they felt healthy and able to take part in activities organized by religious communities. The findings suggest that involvement in religious activities improved participants’ motivation to take medication diligently. Previous studies have reported negative43 and positive influences41 of organized religious activities (ORA) on adherence. In addition, there are also studies which have reported that religious activities were not unrelated83,84 to medication adherence.
Misunderstanding of religious concepts relating to superiority of religious-related treatment has promoted the views that religious-related healing is superior than modern medicine. In a society in which religion has a central role in their life, it is a common belief that God heals and has the ultimate power. Our findings suggest that those who preferred religious-related healing or products could have misunderstood the concept of God heals. Another possible explanation could be related to religious coping in which participants found refuge in their connection with God and seek alternative solutions for their illness within the realm of religion. Spiritual connection with God could sometimes be an escapism for delegating resolutions to challenges faced to God. Previous studies suggested various mechanisms through which religious coping could be used85–87 when encountering stressful situations related to health.88
The negative impact of religiosity could be related to how the participants understand certain religious teaching instead of the teaching itself. Identification of religiosity elements affecting patients’ perception, belief and attitudes towards treatment would therefore be useful for HCP to overcome non-adherence issues.
Spirituality and Antihypertensive Medication Adherence
Unlike previous studies that suggested both positive89,90 and also negative associations of spirituality with medication adherence,43 none of the findings in this study could be related to spirituality in isolation as our study participants related their experiences to religious belief. Some participants seem to perceive spirituality as related to belief and reliance in God and part of religiosity. This could be related to the tradition of religious belief practiced by this group of people. The situation is rather different from that in western populations whereby the term spirituality is commonly used and understood as different from religiosity.
In the socio-cultural context of this study, it appears that participants are not familiar with the spirituality dimensions outside dogmatic religious belief. This suggests differences in the understanding of certain concepts of belief between people of different ethnicity and demographic background.
Despite the abundance of literature that describe the role of culture, religion and spirituality on medication adherence, no specific measures or solutions were formulated and used in our studied populations. This study proposes new perspectives in understanding the mechanism through which culture and religiosity elements influence patients’ adherence to medications.
Limitation
Our study was conducted in the national language which required certain level of language proficiency. Hence, patients without good proficiency in Malay language had to be excluded because they could not comprehend and provide a meaningful response. As such, we were not able to capture information best explained in some of the participants’ mother tongues.
Additionally, the research intended to explore the influence of culture, religiosity and spirituality within the local context. In relation to generalizability, the findings should only be applied in populations from other locations if they have similar cultural and religious backgrounds.
We only stratified patients into two categories which is rural and urban as the intention was also to understand the difference in the influence of CRS factors between these categories of patients. Hence, the findings is also limited by these categories.
Conclusion
The majority of our study participants are Malay Muslims for whom culture and religion are imbued in their daily life. Cultural elements such as societal norms related to ignorance, belief in testimony and anything “natural is safe” negatively influenced medication adherence. Additionally, communication norms characterized by superficiality, indirectness and non-confrontational were also found to affect adherence negatively. Whereas, elements of religiosity such as internal and organizational religiosity were linked to increased motivation to take medication. Our study has revealed the negative impact of misconception about healing and treatment related to religiosity that reduced participants’ confidence in modern medicine. However, the role of spirituality remains unclear as it seemed to be understood within the realm of religion.
Understanding the mechanism of influence that culture and religiosity had on medication adherence could help healthcare professionals to improve engagement with patients and decide on the appropriate course of intervention.
Future work should consider focusing on extending the exploration of CRS in other ethnic groups to elucidate CRS relationship with health behaviour and medication adherence. A context-based adherence assessment and intervention could be formulated to improve adherence to treatment towards achieving targeted treatment outcomes.
Acknowledgments
This research was supported in part by a grant from Universiti Kebangsaan Malaysia (UKM). We thank all study participants for their willingness to engage with us and provide meaningful insight. We would also like to express our gratitude to the pharmacists and community leaders who have facilitated the process of identifying patients eligible for the study.
Funding
This study was funded by Universiti Kebangsaan Malaysia (UKM) (GUP-2017-107) grant.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. World Health Organization (WHO). Fact sheet: cardiovascular disease. Who.int. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. World Health Organization (WHO). Global NCD target. Reducing premature deaths from NCDs. WHO Int. 2016;31(4):190–215.
3. Zhou D, Xi B, Zhao M, Wang L, Veeranki SP. Uncontrolled hypertension increases risk of all-cause and cardiovascular disease mortality in US adults: the NHANES III linked mortality study. Sci Rep. 2018;8(1):1–7. doi:10.1038/s41598-018-27377-2
4. World Health Organization (WHO). World Health Organization Global Health estimates: life expectancy and leading causes of death and disability. Who.int. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
5. Pinho J, Costa AS, Araújo JM, Amorim JM, Ferreira C. Intracerebral hemorrhage outcome: a comprehensive update. J Neurol Sci. 2019;398:54–66. doi:10.1016/j.jns.2019.01.013
6. World Health Organization (WHO). Noncommunicable diseases progress monitor 2020. Who.int; 2020. Available from: https://www.who.int/publications/i/item/ncd-progress-monitor-2020.
7. Li Y, Jasani F, Su D, et al. Decoding nonadherence to hypertensive medication in New York City: a population segmentation approach. J Prim Care Community Health. 2019;10:1–5. doi:10.1177/2150132719829311
8. Liew SJ, Lee JT, Tan CS, Koh CHG, Van Dam R, Müller-Riemenschneider F. Sociodemographic factors in relation to hypertension prevalence, awareness, treatment and control in a multi-ethnic Asian population: a cross-sectional study. BMJ Open. 2019;9:e025869. doi:10.1136/bmjopen-2018-025869
9. Hussein A, Awad MS, Mahmoud HEM. Patient adherence to antihypertensive medications in upper Egypt: a cross-sectional study. Egypt Heart J. 2020;72(1):1–8. doi:10.1186/s43044-020-00066-0
10. Mahmood S, Jalal Z, Hadi MA, Orooj H, Shah KU. Non-adherence to prescribed antihypertensives in primary, secondary and tertiary healthcare settings in Islamabad, Pakistan: a cross-sectional study. Patient Prefer Adherence. 2020;14:73–85. doi:10.2147/PPA.S235517
11. Kim SJ, Kwon OD, Han EB, et al. Impact of number of medications and age on adherence to antihypertensive medications: a nationwide population-based study. Med (United States). 2019;98(49). doi:10.1097/MD.0000000000017825
12. Akunne OO, Adedapo ADA. Antihypertensive prescription among black patients without compelling indications: prescription, effectiveness, quality and cost of medication. BMC Health Serv Res. 2019;19(1):1–8. doi:10.1186/s12913-019-4202-2
13. Obirikorang Y, Obirikorang C, Acheampong E, et al. Predictors of noncompliance to antihypertensive therapy among hypertensive patients Ghana: application of health belief model. Int J Hypertens. 2018;2018:1–9. doi:10.1155/2018/4701097
14. Mugwano I, Kaddumukasa M, Mugenyi L, et al. Poor drug adherence and lack of awareness of hypertension among hypertensive stroke patients in Kampala, Uganda: a cross sectional study. BMC Res Notes. 2016;9(1):1–8. doi:10.1186/s13104-015-1830-4
15. Institute for Public Health (IPH). National Health and Morbidity Survey (NHMS) 2019: NCDs - non-communicable diseases: risk factors and other health problems. Vol 1; 2019. Available from: https://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2019/Report_NHMS2019-NCD_v2.pdf.
16. Ministry of Health Malaysia. Malaysia national health accounts: health expenditure report 1997–2017. Health expenditure report. Available from: https://www.moh.gov.my/moh/resources/Penerbitan/PenerbitanUtama/MNHA/Laporan_MNHA_Health_Expenditure_Report_1997-2017_03122019.pdf.
17. Tong X, Chu EK, Fang J, Wall HK, Ayala C. Nonadherence to antihypertensive medication among hypertensive adults in the United States─HealthStyles, 2010. J Clin Hypertens. 2016;18(9):892–900. doi:10.1111/jch.12786
18. Herttua K, Martikainen P, Batty GD, Kivimäki M. Poor adherence to statin and antihypertensive therapies as risk factors for fatal stroke. J Am Coll Cardiol. 2016;67(13):1507–1515. doi:10.1016/j.jacc.2016.01.044
19. Abegaz TM, Shehab A, Gebreyohannes EA, Bhagavathula AS, Elnour AA. Nonadherence to antihypertensive drugs a systematic review and meta-analysis. Med (United States). 2017;96(4). doi:10.1097/MD.0000000000005641
20. Dillon P, Stewart D, Smith SM, Gallagher P, Cousins G. Models: assessing adherence to antihypertensive medication in older adults in a community pharmacy setting. Clin Pharmacol Ther. 2018;103(6):1052–1060. doi:10.1002/cpt.865
21. Asgedom SW, Atey TM, Desse TA. Antihypertensive medication adherence and associated factors among adult hypertensive patients at Jimma University Specialized Hospital, southwest Ethiopia. BMC Res Notes. 2018;11(1):1–8. doi:10.1186/s13104-018-3139-6
22. Lo SHS, Chau JPC, Woo J, Thompson DR, Choi KC. Adherence to antihypertensive medication in older adults with hypertension. J Cardiovasc Nurs. 2016;31(4):296–303. doi:10.1097/JCN.0000000000000251
23. Aziz H, Hatah E, Makmor-Bakry M, Islahudin F, Hamdi NA, Wan IMP. Qualitative exploration of the modifiable factors for medication adherence among subsidised and self-paying patients in Malaysia. BMC Health Serv Res. 2018;18:605. doi:10.1186/s12913-018-3417-y
24. Beune EJAJ, Moll Van Charante EP, Beem L, et al. Culturally adapted hypertension education (CAHE) to improve blood pressure control and treatment adherence in patients of African Origin with uncontrolled hypertension: cluster-randomized trial. PLoS One. 2014;9(3):e90103. doi:10.1371/journal.pone.0090103
25. De Souza ACC, Moreira TMM, De Oliveira ES, et al. Effectiveness of educational technology in promoting quality of life and treatment adherence in hypertensive people. PLoS One. 2016;11(11):1–10. doi:10.1371/journal.pone.0165311
26. Tavakoly Sany SB, Behzhad F, Ferns G, Peyman N. Communication skills training for physicians improves health literacy and medical outcomes among patients with hypertension: a randomized controlled trial. BMC Health Serv Res. 2020;20(1):1–10. doi:10.1186/s12913-020-4901-8
27. Marshall IJ, Wolfe CDA, McKevitt C. Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ. 2012;345(7867):1–16. doi:10.1136/bmj.e3953
28. Espejo M, Magabo S, Rivera-Castro A, et al. Qualitative study of knowledge, perception, and behavior related to hypertension and cardiovascular disease risk reduction among hypertensive African-Americans in Urban Inner City of South Bronx, New York. J Racial Ethn Health Disparit. 2019;6(1):197–206. doi:10.1007/s40615-018-0514-x
29. Kretchy I, Owusu-Daaku F, Danquah S. Spiritual and religious beliefs: do they matter in the medication adherence behaviour of hypertensive patients? Biopsychosoc Med. 2013;7(1):1. doi:10.1186/1751-0759-7-15
30. Koenig HG. Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatr. 2012;2012:278730. doi:10.5402/2012/278730
31. Al-Noumani H, Wu JR, Barksdale D, Alkhasawneh E, Knafl G, Sherwood G. Relationship between medication adherence and health beliefs among patients with hypertension in Oman: pilot study. Sultan Qaboos Univ Med J. 2017;17(3):e329–e333. doi:10.18295/squmj.2017.17.03.012
32. Sutton AL, Salgado TM, He J, Hurtado-de-mendoza A, Sheppard VB. Sociodemographic, clinical, psychosocial, and healthcare-related factors associated with beliefs about adjuvant endocrine therapy among breast cancer survivors. Support Care Cancer. 2020;28:4147–4154. doi:10.1007/s00520-019-05247-5
33. Svensson NH, Hvidt NC, Nissen SP, et al. Religiosity and health-related risk behaviours in a secular culture—is there a correlation? J Relig Health. 2020;59(5):2381–2396. doi:10.1007/s10943-019-00919-2
34. Kroeber AL, Kluckhohn C. Culture, a Critical Review of Concepts and Definitions. Vol. 20. Cambridge University Press;1954. doi:10.1017/S1373971900104433
35. Hofstede GH. Culture′s consequences: comparing values, behaviors, institutions and organizations across nations. Coll Aviat Rev. 2001;34(2):108.
36. Baldwin JR, Faulkner SL, Hecht ML, Lindsley SL. Redefining Culture: Perspectives Across the Disciplines. Routledge; 2005. doi:10.4324/9781410617002
37. Gall TL, Malette J, Guirguis-Younger M. Spirituality and religiousness: a diversity of definitions. J Spirit Ment Health. 2011;13(3):158–181. doi:10.1080/19349637.2011.593404
38. Koenig H, Koenig HG, King D, Carson VB. Handbook of Religion and Health. USA: Oup; 2012.
39. Miller WR, Thoresen CE. Spirituality, religion, and health: an emerging research field. Am Psychol. 2003;58(1):24–35. doi:10.1037/0003-066X.58.1.24
40. Najimi A, Mostafavi F, Sharifirad G, Golshiri P. Patient’s beliefs about adherence to medication toward hypertension: a qualitative study. Int J Adv Biotechnol Res. 2016;7(3):1555–1561.
41. Hatah E, Lim KP, Ali AM, Shah NM, Islahudin F. The influence of cultural and religious orientations on social support and its potential impact on medication adherence. Patient Prefer Adherence. 2015;9:589–596. doi:10.2147/PPA.S79477
42. Lin CY, Saffari M, Koenig HG, Pakpour AH. Effects of religiosity and religious coping on medication adherence and quality of life among people with epilepsy. Epilepsy Behav. 2018;78:45–51. doi:10.1016/j.yebeh.2017.10.008
43. Wai KC, Raina Elley C, Nosa V, Kennelly J, Mabotuwana T, Warren J. Perspectives on adherence to blood pressure lowering medications among Samoan patients: qualitative interviews. J Prim Health Care. 2010;2(3):217–224. doi:10.1071/HC10217
44. Badanta-Romero B, de Diego-cordero R, Rivilla-Garcı´a E. Influence of religious and spiritual elements on adherence to pharmacological treatment. J Relig Health. 2018;57:1905–1917. doi:10.1007/s10943-018-0606-2
45. Odusola AO, Hendriks M, Schultsz C, et al. Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Serv Res. 2014;14(1):1–16. doi:10.1186/s12913-014-0624-z
46. Pettey CM, McSweeney JC, Stewart KE, et al. African Americans’ perceptions of adherence to medications and lifestyle changes prescribed to treat hypertension. SAGE Open. 2016;6(1):215824401562359. doi:10.1177/2158244015623595
47. Freire de Medeiros CM, Arantes EP, Tajra RD, Santiago HR, Carvalho AF, Libório AB. Resilience, religiosity and treatment adherence in hemodialysis patients: a prospective study. Psychol Health Med. 2016;22(5):570–577. doi:10.1080/13548506.2016.1191658
48. Abrums M. Faith and feminism: how African American women from a storefront church resist oppression in healthcare. ANS Adv Nurs Sci. 2004;27(3):187–201. doi:10.1097/00012272-200407000-00004
49. Kretchy IA, Owusu-daaku FT, Danquah SA. Mental health in hypertension: assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int J Ment Health Syst. 2014;8(1):4–9. doi:10.1186/1752-4458-8-25
50. Abel WM, Greer DB. Spiritual/religious beliefs and medication adherence in black women with hypertension. J Christ Nurs. 2017;34(3):164–169. doi:10.1097/CNJ.0000000000000333
51. Wannasirikul P, Termsirikulchai L, Sujirarat D, Benjakul S, Tanasugarn C. Health literacy, medication adherence, and blood pressure level among hypertensive older adults treated at primary health care centers. Southeast Asian J Trop Med Public Health. 2016;47(1):109–120.
52. Chen SL, Lee WL, Liang T, Liao IC. Factors associated with gender differences in medication adherence: a longitudinal study. J Adv Nurs. 2014;70(9):2031–2040. doi:10.1111/jan.12361
53. Kressin NR, Orner MB, Manze M, Glickman ME, Berlowitz D. Understanding contributors to Racial disparities in blood pressure control. Circ Cardiovasc Qual Outcomes. 2010;3(2):173–180. doi:10.1161/CIRCOUTCOMES.109.860841
54. Xie Z, Clair PS, Goldman DP, Joyce G, Ruiz JM. Racial and ethnic disparities in medication adherence among privately insured patients in the United States. PLoS One. 2019;14(2):1–9. doi:10.1371/journal.pone.0212117
55. Mitchell T. Religion’s relationship to happiness, civic engagement and health. Pewforum.org; 2019. Available from: https://www.pewforum.org/2019/01/31/religions-relationship-to-happiness-civic-engagement-and-health-around-the-world/.
56. Federal Constitution. Gov.my. Available from: https://www.jac.gov.my/spk/images/stories/10_akta/perlembagaan_persekutuan/federal_constitution.pdf.
57. McLaughlin LA, Braun KL. Asian and pacific islander cultural values: considerations for health care decision making. Health Soc Work. 1998;23(2):116–126. doi:10.1093/hsw/23.2.116
58. Goddard C. The “social emotions” of Malay (Bahasa Melayu). Ethos. 1996;24(3):426–464. doi:10.1525/eth.1996.24.3.02a00020
59. Goddard C. Cultural values and “cultural scripts” of Malay (Bahasa Melayu). J Pragmat. 1997;27(2):183–201. doi:10.1016/s0378-2166(96)00032-x
60. Atinga RA, Yarney L, Gavu NM, Barengo NC. Factors influencing long-term medication non-adherence among diabetes and hypertensive patients in Ghana: a qualitative investigation. PLoS One. 2018;13(3):1–15. doi:10.1371/journal.pone.0193995
61. Hsu Y-H, Mao C-L, Wey M. Antihypertensive medication adherence among elderly Chinese Americans. J Transcult Nurs. 2010;21(4):297–305. doi:10.1177/1043659609360707
62. Francis JJ, Stockton C, Eccles MP, et al. Evidence-based selection of theories for designing behaviour change interventions: using methods based on theoretical construct domains to understand clinicians’ blood transfusion behaviour. Br J Health Psychol. 2009;14(4):625–646. doi:10.1348/135910708X397025
63. Bowen GA. Naturalistic inquiry and the saturation concept: a research note. Qual Res. 2008;8(1):137–152. doi:10.1177/1468794107085301
64. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
65. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
66. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1–13. doi:10.1177/1609406917733847
67. Ahola S. Human values and non-adherence to doctors’ instructions across Europe. J Appl Soc Psychol. 2015;45(4):214–225. doi:10.1111/jasp.12289
68. Waterworth P, Pescud M, Braham R, Dimmock J, Rosenberg M. Factors influencing the health behaviour of indigenous Australians: perspectives from support people. PLoS One. 2015;10(11):1–17. doi:10.1371/journal.pone.0142323
69. Chen S, Lee W, Liang T, Liao I. Factors associated with gender differences in medication adherence: a longitudinal study. J Adv Nurs. 2014;70(9):2031–2040. doi:10.1111/jan.12361
70. Mohamed NF, Azman Shahadan M, Wahab RKA, Maskon O, Rahim AAA. Exploration of the factors in treatment adherence to coronary heart diseases diagnosis among the multi-ethnic patients: a qualitative study. Malay J Med Health Sci. 2019;15(3):117–125.
71. Low LL, Tong SF, Low WY. Social influences of help-seeking behaviour among patients with type 2 diabetes mellitus in Malaysia. Asia Pac J Public Health. 2016;28(2):17S–25S. doi:10.1177/1010539515596807
72. Lipsey AF, Waterman AD, Wood EH, Balliet W. Evaluation of first-person storytelling on changing health-related attitudes, knowledge, behaviors, and outcomes: a scoping review. Patient Educ Couns. 2020;103(10):1922–1934. doi:10.1016/j.pec.2020.04.014
73. Hardin R. Trust and Trustworthiness. Russell Sage Foundation; 2004. doi:10.4324/9781315542294-2
74. Chiu KC, Boonsawat W, Cho SH, et al. Patients’ beliefs and behaviors related to treatment adherence in patients with asthma requiring maintenance treatment in Asia. J Asthma. 2014;51(6):652–659. doi:10.3109/02770903.2014.898772
75. Owusu S, Gaye YE, Hall S, et al. Factors associated with the use of complementary and alternative therapies among patients with hypertension and type 2 diabetes mellitus in Western Jamaica: a cross-sectional study. BMC Complement Med Ther. 2020;20(1):1–11. doi:10.1186/s12906-020-03109-w
76. Farrukh MJ, Makmor-Bakry M, Hatah E, Jan TH. Impact of complementary and alternative medicines on antiepileptic medication adherence among epilepsy patients. BMC Complement Med Ther. 2021;21(1):50. doi:10.1186/s12906-021-03224-2
77. Awang S, Maros M, Ibrahim N. Malay values in intercultural communication. Int J Soc Sci Human. 2013;2(3):201–205. doi:10.7763/ijssh.2012.v2.96
78. Khalib FM, Tayeh A. Indirectness in English requests among Malay University students. Procedia Soc Behav Sci. 2014;134:44–52. doi:10.1016/j.sbspro.2014.04.223
79. Ali KK. Discourse on malay origin, institutions, values and systems. Platform a J Manag Human. 2020;3(1):15–29.
80. Haji Omar A. Patterns of language communication in Malaysia. Asian J Soc Sci. 1985;13(1):19–28. doi:10.1163/080382485X00039
81. Lewis LM, Askie P, Randleman S, Shelton-Dunston B. Medication adherence beliefs of African Americans. J Cardiovasc Nurs. 2010;25(3):199–206. doi:10.1097/JCN.0b013e3181c7ccde
82. Abel WM, Joyner JS, Cornelius JB, Greer DB. Self-care management strategies used by black women who self-report consistent adherence to antihypertensive medication. Patient Prefer Adherence. 2017;11:1401–1412. doi:10.2147/PPA.S138162
83. Amadi KU, Aguocha CM, Attama MC, et al. The longitudinal influence of social determinants of health on glycemic control in elderly adults with diabetes. Diabetes Care. 2021;43(4):759–766. doi:10.1080/13674676.2020.1826916
84. Ransome Y, Mayer KH, Tsuyuki K, et al. The role of religious service attendance, psychosocial and behavioral determinants of Antiretroviral Therapy (ART) adherence: results from HPTN 063 cohort study. AIDS Behav. 2019;23(2):459–474. doi:10.1007/s10461-018-2206-2
85. Pargament KI, Koenig HG, Tarakeshwar N, Hahn J. Religious coping methods as predictors of psychological, physical and spiritual outcomes among medically ill elderly patients: a two-year longitudinal study. J Health Psychol. 2004;9(6):713–730. doi:10.1177/1359105304045366
86. Holt CL, Roth DL, Huang J, Park CL, Clark EM. Longitudinal effects of religious involvement on religious coping and health behaviors in a national sample of African Americans. Soc Sci Med. 2017;187:11–19. doi:10.1016/j.socscimed.2017.06.014
87. Freitas TH, Hyphantis TN, Andreoulakis E, et al. Religious coping and its influence on psychological distress, medication adherence, and quality of life in inflammatory bowel disease. Rev Bras Psiquiatr. 2015;37(3):219–227. doi:10.1590/1516-4446-2014-1507
88. Schleder LP, Stach Parejo L, Cláudia Puggina A, Silva MJPD, Paes Da Silva MJ. Spirituality of relatives of patients hospitalized in intensive care unit. Acta Paul Enferm. 2013;26(1):71–78. doi:10.1590/S0103-21002013000100012
89. Alvarez JS, Goldraich LA, Nunes AH, et al. Association between spirituality and adherence to management in outpatients with heart failure. Arq Bras Cardiol. 2016;106(6):491–501. doi:10.5935/abc.20160076
90. Vitorino LM, Lucchetti G, Leão FC, Vallada H, Peres MFP. The association between spirituality and religiousness and mental health. Sci Rep. 2018;8(1):1–9. doi:10.1038/s41598-018-35380-w
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.