Back to Journals » Risk Management and Healthcare Policy » Volume 18
Exploring Challenges and Opportunities in Hospital Disaster Preparedness: A Qualitative Study on the Perspectives of Hospital Incident Command System Members
Authors Singh P ![]() , Sapkota S
, Sapkota S ![]() , Achour N
, Achour N ![]() , Ragazzoni L, Lamine H
, Ragazzoni L, Lamine H ![]()
Received 18 March 2025
Accepted for publication 23 August 2025
Published 30 October 2025 Volume 2025:18 Pages 3499—3515
DOI https://doi.org/10.2147/RMHP.S528810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Prinka Singh,1,2 Sujan Sapkota,3 Nebil Achour,4 Luca Ragazzoni,1,2 Hamdi Lamine1,5
1CRIMEDIM-Center for Research and Training in Disaster Medicine, Humanitarian Aid and Global Health, Università Del Piemonte Orientale, Novara, 28100, Italy; 2Department for Sustainable Development and Ecological Transition, Università Del Piemonte Orientale, Vercelli, 13100, Italy; 3HERD International, Lalitpur, Nepal; 4School of Allied Health and Social Care, Faculty of Health, Education, Medicine and Social Care, Anglia Ruskin University, Cambridge, CB1 1PT, UK; 5Department of Community Health Nursing, College of Nursing, University of Hail, Hail, Saudi Arabia
Correspondence: Prinka Singh, CRIMEDIM-Center for Research and Training in Disaster Medicine, Humanitarian Aid and Global Health, Università Del Piemonte Orientale, Novara, 28100, Italy, Email [email protected]
Purpose: This study aims to explore the perspectives of hospital incident command system (HICS) members to identify key gaps in hospital disaster preparedness and set recommendations to enhance hospital resilience and disaster response capacity in Nepal.
Methods: A qualitative case study method was employed, involving semi-structured in-depth interviews as a sole method of data collection, with HICS members purposively selected based on their active involvement in hospital disaster preparedness. The interviews were conducted in person in Nepali, transcribed verbatim, translated into English, and analyzed using an inductive thematic approach.
Results: Three themes arose from the results. The first theme highlighted the need for policy and systemic reforms, including revising staffing quotas based on an updated organization and management survey, developing standardized national guidelines for hospital nonstructural safety, revising tender policies to allow greater flexibility in emergency resource procurement, and updating hospital disaster preparedness and response plans to adopt a more comprehensive, all-hazards approach. The second theme entailed strategic partnerships and community engagement, demanding formal collaboration with external stakeholders, establishing a local coordination hub to streamline disaster response efforts, and pre-disaster coordination meetings with relevant partners. The third theme was concerned with hospital-level operational reforms, suggesting capacity-building efforts like cross-training and mentoring programs, extending training to alternative HICS focal persons, aligning stockpiling strategies with local hazard risks, and assessing triage areas to ensure their functionality during actual emergencies.
Conclusion: Hospitals in Nepal need a coordinated effort among policymakers, healthcare administrators, frontline hospital personnel, and local stakeholders to bridge existing gaps and build a resilient healthcare system.
Keywords: disaster planning, hospital incident command system, hospital preparedness, healthcare resilience, Nepal
Introduction
Hospitals are vital institutions during disasters, serving as pillars of emergency care and community resilience.1,2 Their ability to maintain functionality during and after disasters is essential for saving lives, reducing injuries, and supporting recovery efforts.3 Globally, hospital disaster preparedness (HDP) has evolved through the adoption of multidisciplinary approaches that integrate structural and nonstructural safety, emergency response protocols, resource management, and staff training.4 International frameworks, such as the Sendai Framework for Disaster Risk Reduction and the World Health Organization (WHO) hospital safety index (HSI) tool, emphasize the necessity of ensuring hospital resilience to protect both healthcare infrastructure and public health during emergencies.5,6
The current global scenario of HDP presents a mixed picture.7–13 Hospitals in many countries have made strides in strengthening their preparedness through structural retrofitting, regular disaster drills, and improved emergency planning.7–9 Nevertheless, there are still challenges, such as inconsistent implementation of disaster preparedness measures, insufficient training for healthcare workers, and weaknesses in coordination among stakeholders.10–13 The Coronavirus disease of 2019 (COVID-19) further demonstrated the necessity for strong HDP, revealing weaknesses in surge capacity, supply chain management, and inter-agency coordination.14–16
In Nepal, HDP challenges are particularly dire.17,18 The country is ranked among the 20 most disaster-prone nations globally, placing 4th in climate vulnerability and 11th in earthquake risk.19 Between 2018 and 2024, Nepal experienced over 32,375 small and large-scale disaster events, including landslides, floods, epidemics, and earthquakes, resulting in 2,996 deaths and 11,752 injuries.20 The 2015 Nepal earthquake alone caused 8,970 deaths, 22,300 injuries, and displaced nearly 2.8 million people.21,22 It also rendered 503 health facilities completely nonfunctional, with another 406 facilities partially damaged, severely disrupting the health system’s ability to provide essential services.23 In response to these challenges, Nepal introduced several post-earthquake innovations, such as formulating hospital disaster preparedness and response plans (HDPRP), establishing a hospital incident command system (HICS), and allocating a budget for simulation exercises and disaster orientation.24,25 However, their implementation remained limited in scope and effectiveness.24,25 A post-earthquake study found that most hospitals still lacked comprehensive disaster plans and functional HICS, and very few conducted regular emergency drills.22,26 Also, epidemic and pandemic preparedness components were absent in most plans, despite Nepal’s recurring dengue outbreaks and influenza surges.24,27 This lack of foresight became evident during the COVID-19 pandemic, when many hospitals faced delays in activating their incident command systems, suffered from inadequate isolation facilities, personal protective equipment (PPE) shortages, oxygen supply constraints, and very limited intensive care unit bed capacity.27–29 These realities expose a critical gap between policy and preparedness, revealing that HDP in Nepal remains fragmented, reactive, and poorly institutionalized. This situation presents a pressing need for in-depth studies and analysis of HDP in Nepal to better understand existing challenges and identify opportunities for strengthening hospital resilience and preparedness for future disasters.
One strategy to improve HDP is the presence of a well-functioning HICS.30 Multidisciplinary HICS is an international standard practice.31 They serve a vital role in disaster preparedness and response by integrating expertise from various departments.30,32 Such committees include senior leadership representatives, nursing services, medical staff, pharmacy services, infection prevention and control team, facilities engineering, security, and information technology.32 Collecting their suggestions is essential for identifying gaps in current plans, tailoring solutions to specific departmental needs, and enhancing coordination across all levels of the organization.33 However, research capturing the perspectives of HICS, the personnel directly involved in disaster planning and response, remains limited in Nepal. Therefore, this study seeks to fill this gap by exploring the perspectives of HICS members to uncover existing challenges and ways to strengthen HDP in Nepal.
Materials and Methods
Study Design
A qualitative exploratory case study approach was employed to explore the perceptions and suggestions of HICS members from three district hospitals in Nepal. These hospitals were purposively selected because they were severely affected by the 2015 Nepal earthquake and have since experienced frequent disaster incidents, including road traffic accidents (RTA), epidemics, floods, and landslides.34 As government-run facilities, they serve as the first point of care during emergencies.17 This selection, therefore, allows for an in-depth understanding of HDP challenges in settings with recurrent and varied disaster exposures. To maintain confidentiality, the selected hospitals were randomly coded as Hospital A, Hospital B, and Hospital C. Hospitals A and B are 50-bedded facilities, while Hospital C is a 15-bedded institution.
The qualitative method was chosen because it allows for an in-depth understanding of complex, context-specific issues related to HDP.35 Similarly, an exploratory case study approach was selected because it enables a detailed examination of each hospital as a bounded system, capturing the unique organizational context, local challenges, and practices in HDP that a descriptive approach might not fully address.36 The exploratory nature of the approach is appropriate given the limited prior research on HDP in these settings, facilitating the generation of new insights and practical recommendations.36
Study Population
According to the Ministry of Health and Population (MoHP) Nepal, every government hospital is required to establish HICS as part of its HDPRP. The composition of HICS is outlined in Table 1. HICS is a standardized management framework activated during disasters, designed to support hospitals and healthcare facilities in preparing for, responding to, and recovering from emergencies.37,38 It provides a clear organizational structure with defined roles, responsibilities, and communication channels to ensure the efficient coordination of resources and personnel throughout an incident.37,38
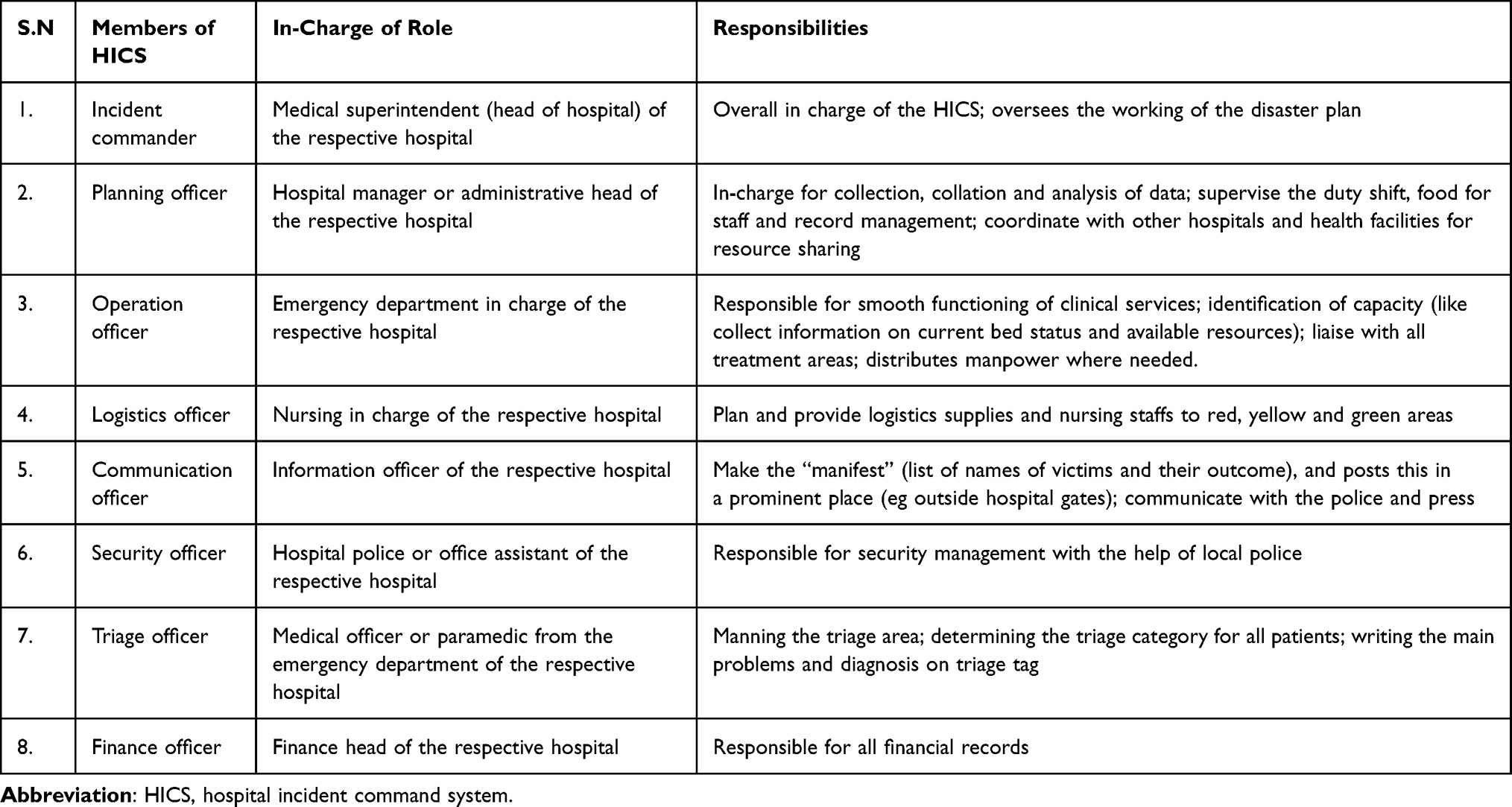 |
Table 1 Structure of Hospital Incident Command System |
For this study, purposive sampling was done, and all members of HICS, except the finance officer, participated. These individuals hold key roles in disaster preparedness and response. Their selection aimed to capture diverse perspectives from those directly involved in disaster management within the hospital setting. The finance officer was excluded due to their limited involvement in direct operational and decision-making activities related to HDP.
Data Collection
Data was collected through semi-structured in-depth interviews conducted between March and August 2024. A semi-structured interview guide was developed based on existing literature, including the 2015 version of the HSI tool and the WHO hospital emergency response checklist.6,39 The guide covered key areas, including demographic information, participants’ experience in managing disasters and mass casualty incidents, focusing on hospital structural, nonstructural, and functional safety aspects, and recommendations for strengthening HDP (interview guide is provided in the Supplementary Material).
Interviews were conducted in person at the respective hospitals, depending on participants’ availability. Each session lasted approximately 30 to 60 minutes. Core questions were asked to all participants, but follow-up questions were adapted based on each participant’s specific role, responsibilities, and the natural flow of the conversation. This flexibility allowed the interviewer to explore areas most relevant to each participant, while still ensuring that the main research objectives were addressed.
To ensure clear communication and comfort for the participants, interviews were conducted in the Nepali language. The principal investigator (PS), a Nepalese female with relevant academic and professional experience, facilitated the interviews. The interviews were conducted confidentially, with only the interviewer and the interviewee present. All interviews were audio recorded with prior consent, and handwritten notes were also taken to help probe discussions.
Data Analysis
Data analysis was conducted by two researchers (PS and SS). Initially, all audio recordings were transcribed verbatim in Nepali and subsequently translated into English. To ensure the accuracy of the translations, the English transcripts were shared with participants for their review and validation. The verified English versions were then used for the analysis. Both researchers (PS and SS) are native Nepali speakers, fluent in both Nepali and English, and had access to both the original Nepali transcripts and the translated versions. Data analysis was performed manually using Microsoft Excel version 2507.
An inductive thematic analysis was conducted, allowing themes to emerge directly from the data. Therefore, the approach was grounded in a constructivist view, which means it assumes that knowledge is created through people’s experiences and interactions. The study recognizes that multiple realities exist, shaped by individual perspectives. This theoretical stance guided the interpretation of the data, helping to understand participants’ views on HDP. This approach follows the framework described by Braun and Clarke (2006).40
An inductive thematic approach was employed following the six phases outlined by Braun and Clarke (2006):40
- Familiarization with the data: Both researchers read the transcripts several times to familiarize themselves with the content, developing a thorough understanding and observing preliminary patterns.
- Generating initial codes: Each researcher independently developed individual codebook using participants’ exact words. Individual codebooks were then compared, and a final codebook was created through consensus.
- Searching for themes: Using the finalized codebook, researchers collaboratively reviewed transcripts to extract relevant quotes, assign codes, organize them into broader categories, and identify preliminary themes.
- Reviewing themes: Themes were checked and refined for internal consistency and fit with the data. Each theme was corroborated by several excerpts, and no important data was excluded.
- Defining and naming themes: Each theme was clearly defined and named to reflect its scope and essence.
- Writing the report: Key findings were organized under each theme, supported by illustrative quotes to provide depth and insight.
Reflexivity
Reflexivity was maintained to ensure the credibility and ethical integrity of the study. Nepalese researchers, who conducted data collection and analysis, regularly engaged in reflective journaling to acknowledge and examine their own perspectives, assumptions, and potential biases. Regular team discussions, including both Nepalese and international members, provided opportunities to challenge interpretations and consider alternative viewpoints. Furthermore, the English transcripts were shared with participants for their review and confirmation, allowing for participant validation of the data.
Results
A total of 21 participants were interviewed, with seven participants from each hospital. The average duration of the interview was 38 minutes. A total of 298 quotes were identified and systematically categorized into 42 distinct codes. These codes were further grouped into 11 broader categories, which in turn were consolidated into three overarching themes, as detailed in Table 2.
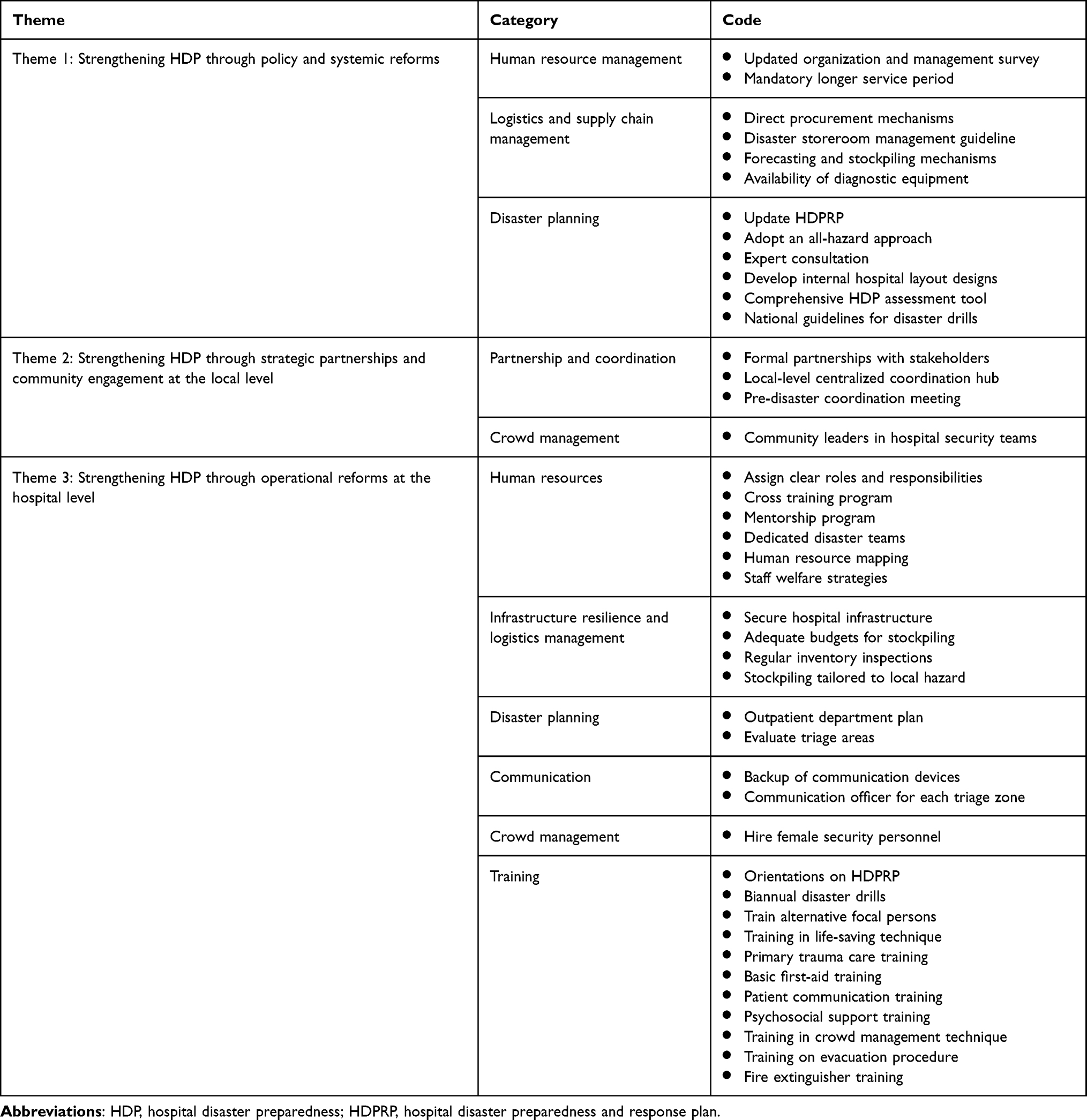 |
Table 2 Results of Data Analysis |
Demographic Information of Participants
To ensure anonymity, each participant was assigned a unique code, ranging from P1 to P21. Table 3 provides a detailed summary of the respondents’ demographic information.
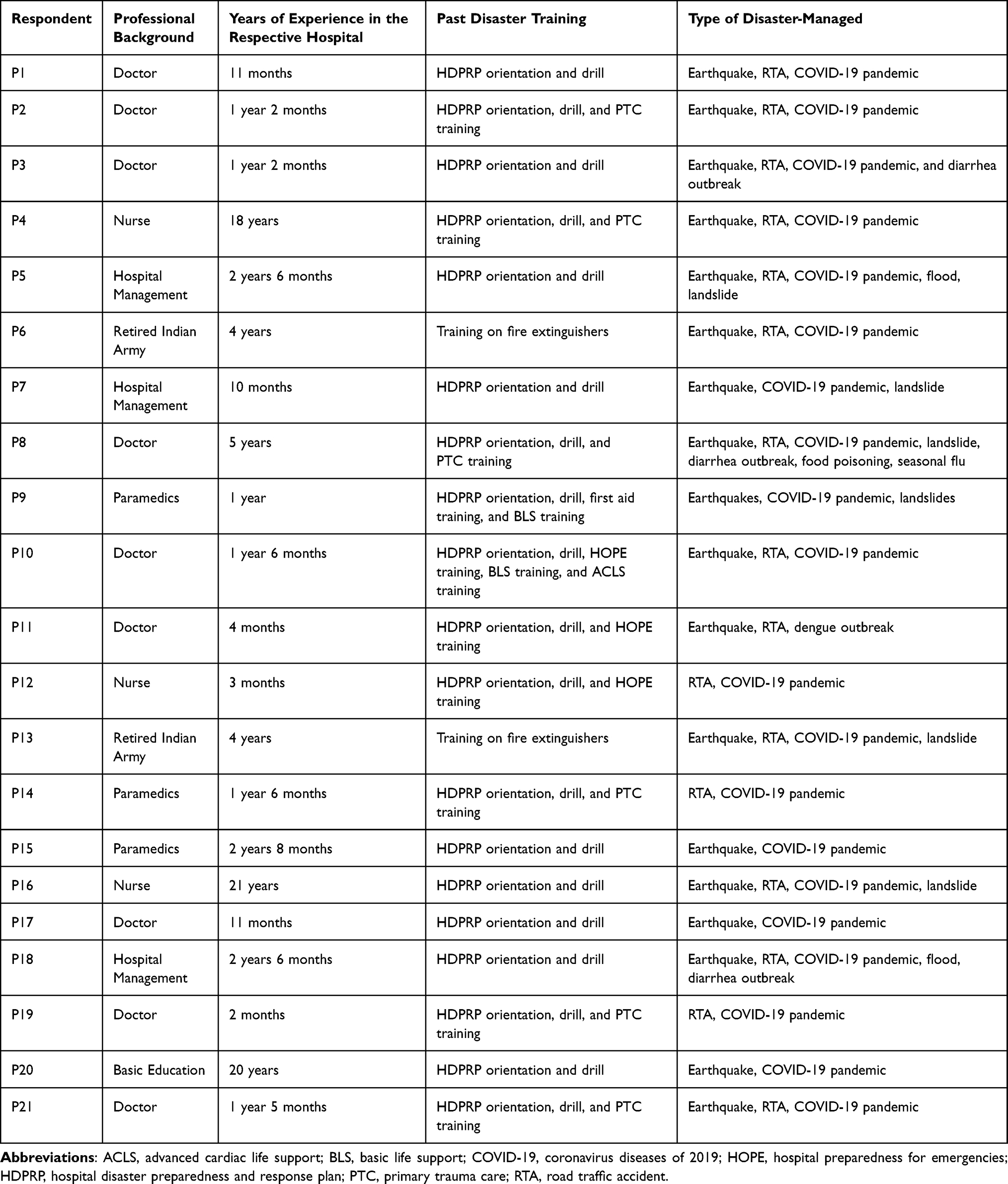 |
Table 3 Demographic Characteristics of Participants |
The majority of participants were doctors, with most having less than three years of experience working in their respective hospitals. Nearly all participants reported receiving orientation on HDPRP and participating in hospital disaster drills. However, only a small number had undergone specialized training, such as primary trauma care, basic first aid, fire extinguisher training, basic life support training, training on hospital preparedness for emergencies, and advanced cardiac life support training (Table 3).
In terms of disaster management experience, most participants had been involved in responding to the 2015 Nepal earthquake, road traffic accidents (RTAs), and the COVID-19 pandemic. Fewer respondents reported managing other disasters, including landslides, floods, diarrhea outbreaks, seasonal flu, and dengue (Table 3).
Themes
Three themes emerged from the findings, which are listed below.
Theme 1: Strengthening HDP Through Policy and Systemic Reforms
The theme encompasses strategic suggestions for shaping decision-making frameworks and influencing governance at higher governmental levels, including federal and provincial authorities.
Human Resource Management
One of the major issues identified was the outdated staffing quotas that directly affect the effectiveness of HDP efforts. Many participants emphasized the urgent need for a revised organization and management (O&M) survey to reassess staffing requirements and implement necessary adjustments (n = 13, 61.90%). Moreover, frequent staff rotations were highlighted as another challenge, with participants noting that personnel are often reassigned every one to two years, which disrupts institutional memory and expertise, a key component in HDP (n = 8, 38.10%). As P15 explained:
Staff are reassigned every one to two years, leaving before they gain sufficient experience. The constant turnover necessitates the creation of a new HDPRP each year, and new staff members require time to acclimate. This inconsistency is a major factor in why our disaster management efforts have not achieved their full potential.
To address this issue, participants recommended implementing longer mandatory service periods for hospital staff to enhance continuity in disaster planning.
Logistics and Supply Chain Management
The procurement process for acquiring necessary supplies during a disaster was recognized as a major barrier to effective disaster management (n = 6, 28.57%). P12 remarked:
The government procurement procedures are quite complex in Nepal. These procedures, which involve lengthy tendering and bid submission processes, often prevent hospitals from having pre-arranged agreements with vendors.
Participants expressed that this delay in procurement is especially problematic during emergencies when time is of the essence. Hospitals are often forced to either request the provincial or federal government to send necessary supplies or navigate through the lengthy procurement process, both of which consume substantial time. Participants, therefore, suggested revising the existing procurement system to allow for more flexibility and quicker access to resources during disasters.
Concerns were also raised about the lack of essential diagnostic equipment, such as computed tomography (CT) scans and magnetic resonance imaging (MRI) machines (n = 9, 42.86%). P4 shared the importance of such equipment, stating:
Equipping hospitals with CT scans and MRI machines is not just an upgrade. It is a lifeline. However, the lack of such equipment often forces hospitals to refer patients elsewhere during disasters, delaying critical care when every second counts.
Further recommendations included developing disaster-specific storeroom management guidelines (n = 3, 14.28%) and establishing forecasting and stockpiling mechanisms to ensure that hospitals are well-stocked with essential supplies and resources (n = 2, 9.52%).
Disaster Planning
Participants widely agreed on the need for updated and more comprehensive disaster planning guidelines (n = 17, 80.95%). The current HDPRP, although helpful, was deemed insufficient to handle a range of potential disaster scenarios. In this regard, P7 elaborated:
Our HDPRP has proven effective in managing disasters, but there is still room for improvement. For example, it currently lacks components on post-disaster planning, planning for vulnerable groups such as pregnant women, postpartum mothers, children, the elderly, and persons with disabilities, and preparedness for other disasters like floods, landslides, and seasonal epidemics, which leaves our healthcare system vulnerable to recurring and diverse threats.
To address these gaps, participants recommended that MoHP Nepal adopt an all-hazards approach to HDP. This would ensure that hospital disaster plans are comprehensive, covering a wide range of disaster scenarios and the unique needs of vulnerable populations. Additionally, expert consultation during the revision of the HDPRP guidelines was considered necessary to incorporate and integrate the best practices and lessons learned from past disasters (n = 7, 33.33%).
Another suggested area was the design and layout of hospital infrastructure. Participants recommended that national guidelines on hospital internal layout would greatly enhance operational efficiency and disaster preparedness (n = 7, 33.33%). P21 noted:
The government should not only provide a structural design but also define internal spaces, such as where the OPD (meaning outpatient department) should be, where the wards should be, where the elevator systems should be, and how the evacuation routes should be designed.
Including engineering expert consultation in drafting these guidelines was also seen as essential for ensuring that infrastructure plans are both technically sound and disaster resilient (n = 6, 28.57%). Furthermore, some respondents proposed developing an exhaustive assessment tool for evaluating HDP (n = 13, 61.90%). Although the existing minimum service standards (MSS) offer a baseline, they were generally considered inadequate to address the complexities of disaster scenarios. P1 clarified:
Hospitals are currently working in a restricted framework that does not address the diverse challenges presented by disasters. A refined evaluation index would enable hospitals to systematically evaluate their readiness, determine weak points, and implement focused improvements. This would provide hospitals with a better understanding of their areas of strength and weakness in disaster readiness and, ultimately, guide additional improvement.
Finally, participants emphasized the need for standardized national guidelines for disaster drills (n = 4, 19.05%). They noted that, in the absence of clear directives, individuals often relied on their own interpretations, resulting in uncoordinated and inconsistent response practices. A well-structured set of guidelines, they suggested, would ensure a more systematic and organized approach, ensuring that drills are conducted effectively rather than being treated as mere formalities.
Theme 2: Strengthening HDP Through Strategic Partnerships and Community Engagement at Local Level
The theme emphasizes strategic collaborations with key stakeholders and active community involvement at the local level.
Partnership and Coordination
The participants emphasized the need to promote partnerships and improve coordination to aid in HDP and disaster response (n = 16, 76.19%). One of the key issues was resource management, more particularly pinpointing the need for formal coordination with external stakeholders, including neighboring hospitals, local health facilities (like primary healthcare centers and local clinics), municipalities, and health offices. Such partnerships, according to the participants, would contribute to the sharing of essential resources, especially human resources, in times of disaster. Still, the failure to formally integrate local authorities, local health facilities, and private hospitals into the HDPRP was identified as a missed opportunity.
Beyond partnerships, participants stressed the necessity of a local-level coordination hub to streamline disaster response efforts (n = 11, 52.38%). Hospitals, particularly in the aftermath of disasters, often bear the overwhelming responsibility of patient care, coordination, and communication. Participants emphasized that this overwhelming burden frequently leads to delays, miscommunication, and inefficiencies, specifically when resources are strained and demand surges. To address these challenges, a centralized hub, similar to a telemedicine setup, was proposed to serve as a liaison between federal and provincial authorities, hospitals, and local stakeholders, preventing duplication of efforts and improving coordination. Further, the participants conveyed that the establishment of such a hub would consolidate response efforts to bring all concerned stakeholders together to deliver the best and well-coordinated disaster response.
Participants further underlined that coordination should not be limited to disaster events alone (n = 4, 19.05%). They viewed pre-disaster coordination meetings among hospitals and local actors on a regular basis as an imperative to anticipate risks and establish response measures in advance. P8 highlighted proactive planning, stating:
Disaster preparedness should not be reactive. For instance, when the rainy season is approaching in April, we should recognize weather patterns and plan for possible disasters. Waiting until a disaster happens to act is not effective.
Crowd Management
Community engagement was acknowledged as a key strategy for maintaining order during disasters, particularly in managing huge crowds that often gather in and around hospitals during emergencies (n = 6, 28.57%). Participants suggested leveraging the leadership and influence of community leaders to assist in crowd management and security efforts. P6 indicated:
Community leaders have strong connections with the local population, which enables them to control crowds, diffuse tensions, and maintain order. Working together with such leaders and incorporating them within hospital disaster security teams could improve security management in the event of disasters.
Theme 3: Strengthening HDP Through Operational Reforms at Hospital Level
The theme includes suggestions or actions proposed for implementation within hospitals to improve practices, policies, or systems.
Human Resource Management
One of the recommendations was the need for clearly defined roles for hospital staff during emergencies (n = 7, 33.33%). For example, P11 related an experience illustrating how, in times of stressful events, role confusion tends to create chaos and inappropriate management of patients.
When a patient arrives in the resuscitation area, everyone rushes there, leaving green and yellow patients unattended. This ambiguity surrounding roles presents considerable challenges, as green patients need supervision, and yellow patients can deteriorate into critical cases.
To mitigate this challenge, participants suggested the establishment of a well-defined job description and a structured response framework, ensuring that all patients receive the necessary care while preventing resource misallocation and treatment delays.
Cross-training emerged as another strategy to strengthen human resources, enabling staff to perform multiple roles during emergencies (n = 5, 23.81%). Mentorship programs were also recommended to foster staff development, where experienced personnel mentor newer staff to build their confidence and increase their ability to handle emergencies (n = 2, 9.52%). Furthermore, participants suggested having a separate hospital disaster team solely for pre and post-disaster management activities (n = 2, 9.52%).
Additional recommendations included human resource mapping to ensure that hospitals maintain an updated record of personnel skills (n = 4, 19.04%), as well as the implementation of staff welfare schemes (n = 4, 19.04%). Such schemes could be in the form of financial incentives, psychosocial counseling, and adequate shift rotations to avoid burnout and minimize the physical and emotional toll of disaster response.
Infrastructure Resilience and Logistic Management
Securing hospital infrastructure and managing logistics were both recognized as essential areas for strengthening HDP. Many participants highlighted the importance of safeguarding hospital infrastructure to minimize damage during disasters (n = 14, 66.66%). Yet, a key concern was the absence of necessary preventive measures to protect such structures. For instance, P10 illustrated:
Heavy furniture and equipment like X-ray machines should be anchored using straps or brackets to prevent them from toppling during earthquakes. Similarly, electronic devices like computers and printers should be secured with safety cables or mounting brackets. Unfortunately, these measures are absent from our hospital due to budget constraints.
In parallel with infrastructure resilience, participants highlighted the need for adequate budgeting to support stockpiling efforts (n = 20, 95.24%). P5 clarified:
While our disaster storeroom maintains stock for 50 victims, disasters are unpredictable, and the number of casualties can exceed this limit. To enhance preparedness, it would be more prudent to stock supplies for 60 or even 100 individuals. However, financial constraints make it difficult to expand our stockpile.
Moreover, regular inventory inspections were suggested to ensure supplies remained functional and intact (n = 10, 47.62%). Tailoring logistics to specific local disaster risks was also considered essential for improving HDP (n = 4, 19.04%). Participants stressed that disaster logistics should align with the unique hazards faced by each region. As P8 remarked:
Hospitals in urban areas frequently manage trauma cases from RTAs, whereas hospitals in flood-prone regions must be equipped to handle waterborne disease outbreaks and large-scale evacuations.
Hence, the respondents suggested that logistical planning should be synchronized with local risk factors so that resources, supplies, and response plans are maximized for the most probable hazards to which each hospital is exposed.
Disaster Planning
Concerns were raised regarding the operational challenges of outpatient department (OPD) services during emergencies (n = 9, 42.86%). One major concern was the evacuation of the OPD in case of disasters, which breaks the continuity of patient care, particularly for patients who travel a long distance to access medical services. Participants thus emphasized the need for an effective contingency plan, which includes alternative sites of OPD and a team that is solely responsible for managing the OPD patients under such emergency circumstances. Currently, the absence of these measures leaves hospitals unprepared to maintain essential OPD services during emergencies.
Triage area functionality was another issue (n = 7, 33.33%). Participants mentioned that while designated triage zones existed on paper, their practicality in real-life emergencies was rarely assessed. As a result, participants stressed the importance of evaluating triage areas to determine whether they could effectively handle patient surges during disasters. P21 elaborated:
For example, a green zone intended for stable patients might require modifications to accommodate unexpected increases in patient volume. Assessing these areas before a disaster strikes would allow hospitals to make necessary adjustments, improving overall response efficiency.
Training
Orientation sessions on HDPRP, along with simulation exercises, were viewed as a crucial component for ensuring staff readiness (n = 21, 100%). While many staff members were aware of disaster response protocols, participants noted that awareness alone was insufficient. Regular simulation exercises and drills were considered essential to ensure that staff could apply their knowledge in high-pressure situations. Many participants advocated conducting these exercises at least twice a year to reinforce preparedness and identify gaps in response strategies.
Beyond general preparedness, participants highlighted gaps in training for alternate focal persons within HICS (n = 9, 42.86%). While primary focal persons receive some training, their alternates are often overlooked, creating a vulnerability in leadership succession. P2 asserted:
Primary focal persons often receive minimal training, while their alternates are entirely neglected. These secondary personnel must be equipped with the skills to step into leadership roles when required. Without the training, we risk operational failure when primary personnel are unavailable.
Clinical training was also identified as a priority, with emphasis on life-saving techniques, trauma management, and first aid training for ambulance drivers (n = 13, 61.90%). However, participants argued that non-technical training is equally necessary in disaster settings (n = 10, 47.62%). For example, P20 pointed out the importance of communication skills:
Communication training for healthcare workers is essential so they can interact professionally and empathetically with patients and their families.
Additionally, training in psychosocial support, crowd management, evacuation procedures, and fire extinguisher use was recommended.
Communication
Reliable communication systems were consistently recognized as a key element of HDP, and thus participants emphasized the need for backup communication devices to ensure no break in information flow during emergencies (n = 12, 57.14%). For instance, P15 highlighted this need by stating:
When the bus accident occurred, there was no mobile network at the site. We were unable to contact the ambulance driver for updates on their estimated arrival time or the number of casualties. Had we possessed backup communication systems such as wireless radios, coordination would have been much more effective.
Another key recommendation was the designation of communication officers for each triage zone (n = 8, 38.10%). Generally, a single communication officer is responsible for managing both internal and external communications during disasters, a workload that becomes overwhelming as the disaster heightens. To synthesize information flow and make coordination more effective, participants recommended assigning dedicated communication officers in each of the triage zones—green, yellow, and red. This approach would enable the main communication officer to concentrate on high-level coordination while making sure that the zone officers effectively coordinated ground-level communication within their zones.
Crowd Management
Another area needing attention was effective crowd management, especially concerning female security personnel (n = 5, 23.81%). The participants narrated that the lack of female security officers made de-escalation challenging. P13 gave their account, stating:
In a recent response to a road accident, female visitors became agitated, and the situation escalated, There is often an assumption that women will not be harmed in such situations, leading to more aggressive behavior. The absence of female security personnel in our hospital made it challenging to manage the crowd, allowing unauthorized individuals to enter the hospital premises.
Consequently, the participants suggested the hiring and training of female security personnel to address such issues. A gender-balanced security team was recognized as essential for maintaining order and effectively managing crowds during emergencies.
Discussion
HICS provides a structured framework that enables hospitals to respond swiftly and effectively during disasters by integrating expertise from multiple departments.38 This study examines the perspectives of HICS members within three district hospitals in Nepal, identifying key challenges and opportunities for strengthening HDP. The findings reveal multiple gaps and potential strategies for HDP improvement at policy, local, and hospital levels.
Nepal has achieved considerable progress in adopting HDPRPs across its healthcare system.24,25,41 The MoHP’s Health Emergency Operation Center has been instrumental in the process, organizing workshops in all seven provinces and establishing HDPRPs in over 100 hospitals.24,25,41 These initiatives have strengthened hospitals’ ability to manage disasters and public health emergencies.24,25,41 However, findings from this study indicate that these plans primarily concentrate on RTAs, failing to adopt the “all-hazards” approach as recommended by the WHO.42 This trend mirrors findings from similar studies conducted in Ethiopia, Saudi Arabia, and Tanzania.43–45 The prevailing emphasis on RTAs is largely due to their high frequency, immediate impact, and measurable burden. Unlike natural disasters, which tend to be sporadic or seasonal, RTAs occur regularly and require urgent trauma care, making them a constant and visible challenge for hospital emergency services.
However, this narrow focus has considerable implications. A lack of all-hazards planning weakens system-wide preparedness and resilience. For example, staff training often centers heavily on trauma care, as highlighted in a study from the United States, which found that healthcare workers were generally less prepared to manage infectious disease outbreaks, chemical hazards, or mass casualties resulting from floods, landslides, or earthquakes.46 Similarly, logistical planning and stockpiling efforts tend to prioritize surgical and trauma-related supplies, often overlooking essential resources such as PPE, ventilators, and isolation beds, as emphasized in several other studies.28,29,47
This limitation became evident during the COVID-19 pandemic, which exposed gaps in the existing HDPRPs, particularly their lack of comprehensiveness.27,48 While the studied hospitals had general disaster response frameworks, they were not adequately equipped to handle the unprecedented scale and complexity of the pandemic. The hospitals struggled with rapidly evolving protocols, inter-agency coordination, and prolonged resource shortages, exposing gaps in flexibility and scalability within existing HDPRPs. Similar shortcomings have been observed in the United States, where existing emergency management and disaster preparedness plans were deemed inadequate for handling the intensity and duration of the COVID-19 crisis.49 Drawing from these lessons, Nepalese hospitals must revise their current HDPRP guidelines and incorporate hazard-specific sub-plans to ensure that the hospital’s responses are tailored to the specific challenges it may encounter from particular hazards, allowing for the efficient allocation of resources, personnel, and medical supplies.50
Structural resilience in Nepalese hospitals has improved following the 2015 earthquake, with revisions to the national building code focusing on seismic safety.51 Nonstructural safety, equally important for hospital functionality during disasters, however, remains a cause for concern, as highlighted by this study.10,52 Nonstructural vulnerabilities, such as unanchored medical equipment, inadequate emergency evacuation routes, and unreliable backup power supplies, have historically led to hospital evacuations in major disasters, including the Kobe earthquake (1995), Chile earthquake (2010), and Japan tsunami (2011).53–55 Despite the importance of nonstructural safety, the present study revealed that only a handful of Nepalese hospitals, often with external support, have implemented necessary safety measures. This clearly indicates the need for stronger national policies and increased resource allocation to address nonstructural vulnerabilities across the country’s healthcare system. A noteworthy model for Nepal to consider is Iran, where national policies mandate high standards for both structural and nonstructural hospital safety.56 Nepal could benefit from adopting a similar national framework, including mandatory anchoring of furniture and equipment, to ensure functional continuity of nonstructural elements during disasters.
Another pressing challenge reported in the present study is Nepal’s healthcare workforce shortage. The WHO has identified Nepal as one of 57 nations facing a critical deficit of health workers.57 The current study reveals that staffing quotas in Nepalese hospitals are based on outdated O&M surveys, failing to account for current healthcare demands.58 As a result, many hospitals rely on temporary contract staff, leading to workforce instability as employees seek better opportunities.57 This instability is further compounded by frequent staff turnover, with transfers occurring every one to two years, which disrupts institutional knowledge and continuity. Consequently, repeated training in HDPRPs is required, placing an additional burden on already limited resources. Comparable challenges have been noted in Sri Lanka and the Philippines, where workforce shortages have undermined HDP.59,60 Addressing this issue in Nepal requires updating O&M surveys to align staffing quotas with current healthcare demands. Additionally, adopting workforce retention frameworks, such as the root steam model proposed by Makuku et al, could improve staff retention by addressing key stages in the workforce process, such as academic education, recruitment, job training, remuneration, workforce environment, and investment in skills and resources.61
Stockpile management is another area of concern. Each hospital in the current study adheres to the MSS, which ensures the availability of basic essential healthcare services, including disaster stockpiles.17,62 However, the findings indicate that these stockpiles are only sufficient for handling minor incidents and are inadequate for large-scale disasters such as earthquakes or pandemics. Similar limitations have been documented in studies conducted in Sri Lanka, Egypt, Iran, and Ghana.12,13,63,64 A systematic review by Samei et al identified several key factors influencing hospital functional preparedness, including the supply and storage of PPE, hospital beds, portable laboratories, medical consumables, medicines, and even food and water supplies, and therefore underscores the importance of stockpile planning as an essential component of disaster readiness.65 Countries like New Zealand, which are frequently hit by natural disasters, have established robust stockpiling mechanisms for disasters.66 New Zealand’s national stockpile is stored in various locations, split over several sites to reduce risk and optimize distribution efficiency.66 Nepal can adopt a similar decentralized approach, with multiple reserve inventories at federal, provincial, and local levels. Regular monitoring and a replenishment mechanism would further strengthen this system, building the nation’s capacity to respond effectively to large-scale emergencies.
The study also identifies Nepal’s procurement system as a major barrier to effective HDP. In fact, each hospital in the present study frequently faces delays in receiving essential medicines and medical equipment because of Nepal’s complicated and lengthy tender process. Such procurement delays have been a long-standing issue in the Nepalese health system, leading to perpetual stock-outs and slowing down the response of hospitals to emergencies at a moment’s notice.67,68 While the existing procurement system is designed to be transparent and accountable, its rigidity has a tendency to slow down the procurement of supplies required during emergencies. A potential solution is establishing an emergency procurement mechanism that allows for direct purchases of essential medical supplies, bypassing the lengthy tender process when urgent needs arise. A relevant example is India, where the state procurement board introduced the “Major Emergency Procurement Policy” amidst the COVID-19 pandemic, enabling the public administration to fast-track procurement with some exemption for essential goods and services.69 The same approach in Nepal would render Nepal more disaster-responsive with quick procurements so that hospitals and health centers have uninterrupted access to vital medical supplies.
Since Nepal embraced a federal government system in 2015, a three-level framework, federal, provincial, and local, is practiced by the country.70 Yet, coordination gaps of Nepal’s federal system have become key obstacles for HDP.27,48 Gaps in coordination and role ambiguity at the local level, in congruence with findings reported by Kuikel et al, have been found by the present study.48 The present study also reveals that there are various organizations, such as the Red Cross, municipalities, health offices, and district administration offices, which possess disaster management resources. Nevertheless, their efforts are still disjointed, tending to result in duplication of efforts and ineffective mobilization of resources during crises. Observing the importance of multi-sectoral coordination, the United Nations Office for Disaster Risk Reduction advocates for an all-of-society approach in disaster risk reduction.71 Accordingly, Nepal must have centralized coordination centers at the local level as one-stop points of contact, linking hospitals with municipal governments, local stakeholders, and federal and provincial governments. By streamlining resource allocation, improving communication, and reducing redundancies, this method would enhance Nepal’s emergency response capacity as a whole.
Strengths and Limitations of the Study
This study is one of the first in Nepal to explore the perceptions and recommendations of HICS members, providing valuable insights into Nepal’s HDP context. Nevertheless, several limitations must be taken into account in interpreting the findings. Firstly, the study was carried out in only three hospitals, which might not capture the full range of HDP practices in various health settings. The fact that participants from a variety of academic and professional backgrounds, coupled with their varied disaster experiences, participated in the study, enhances the relevance of the findings to similar contexts; however, generalizing them to other regions or healthcare facilities should be done with caution. Furthermore, the study was based on self-reported data, which is prone to biases like recall bias or social desirability bias, which could compromise the validity of the responses of the participants. To reduce these biases, probing techniques were employed to encourage more detailed and accurate responses. Moreover, the study was limited to government district hospitals with fewer than 100 beds, which restricts the ability to compare findings with other types of healthcare facilities, such as federal or private hospitals, where experiences and disaster preparedness interventions may vary. Additionally, the study focused exclusively on hospital personnel, excluding the views of external stakeholders such as local governments, non-governmental organizations, and community groups. These external actors are equally important in disaster management and could offer valuable insights into HDP efforts. Another potential limitation relates to language. Interviews were conducted in Nepali and subsequently translated into English for analysis. Although careful translation procedures were followed and participants reviewed the English transcripts to ensure accuracy, there remains a possibility that subtle meanings or cultural nuances may have been lost in translation, potentially influencing the interpretation of findings. Lastly, investigator bias is acknowledged as a possible limitation. To minimize this, reflexivity was maintained throughout the research process, and the data analysis was conducted collaboratively by two researchers to enhance analytical rigor and ensure a balanced and credible interpretation of the data.
Conclusion
The study concludes that all three tiers of government in Nepal play distinct yet complementary roles in HDP. The federal government is primarily responsible for formulating national policies, setting standards, and allocating resources. Provincial governments adapt these policies to local contexts and coordinate efforts across districts, while local governments (including hospitals) are chiefly responsible for implementation on the ground. Effective coordination across all government levels is therefore essential for preparing and maintaining a robust HDP.
To move forward, reforms should prioritize updating existing HDPRP guideline and establishing formal coordination mechanisms, such as an integrated planning platform and real-time communication. Strengthening the capacity of local governments, particularly in human resources and logistic supply, appears both urgent and feasible. In addition, establishing minimum infrastructure and supply chain standards tailored to varying geographic and risk profiles would significantly improve hospital resilience.
Future research should explore the long-term effectiveness of HDP interventions in a wider range of hospital types and geographic locations. Additionally, studies should assess how resource disparities, such as staffing levels, infrastructure, and supply chains, impact disaster response outcomes. Lastly, qualitative assessments involving local stakeholders would offer deeper insights into the institutional, political, and infrastructural constraints affecting hospital resilience in Nepal.
Abbreviations
COVID-19, coronavirus disease of 2019; CT scan, computed tomography scan; HDP, hospital disaster preparedness; HDPRP, hospital disaster preparedness and response plan; HICS, hospital incident command system; HSI, hospital safety index; MoHP, Ministry of Health and Population; MRI, magnetic resonance imaging; MSS, minimum service standard; O&M, organization and management; OPD, outpatient department; PPE, personal protective equipment; RTA, road traffic accident; WHO, World Health Organization.
Data Sharing Statement
The datasets are available from the corresponding author upon reasonable request.
Ethical Consideration and Consent
Ethical approval was obtained from the Nepal Health Research Council (reference number 457). Participants were provided with detailed information about the study objectives, procedures, and their rights, including the right to withdraw at any time. Written informed consent was obtained prior to data collection, and participants consented to the use of anonymized responses and quotes for publication. Data confidentiality and anonymity were maintained throughout the research process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the preparation of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lestari F, Paramitasari D, Fatmah, et al. Analysis of hospital’s emergency and disaster preparedness using hospital safety index in Indonesia. Sustainability. 2022;14(5879):1–21.
2. Lestari F, Paramitasari D, Kadir A, et al. The application of hospital safety index for analyzing primary healthcare center (PHC) disaster and emergency preparedness. Sustainability. 2022;14(3):1–19.
3. Farah B, Pavlova M, Groot W. Hospital disaster preparedness in sub-saharan Africa: a systematic review of English literature. BMC Emerg Med. 2023;23(1):71. doi:10.1186/s12873-023-00843-5
4. Khirekar J, Badge A, Bandre GR, Shahu S. Disaster Preparedness in hospitals. Cureus. 2023;15(12):e50073. doi:10.7759/cureus.50073
5. Aitsi-Selmi A, Egawa S, Sasaki H, Wannous C, Murray V. The sendai framework for disaster risk reduction: renewing the global commitment to people’s resilience, health, and well-being. Int J Disaster Risk Sci. 2015;6(2):164–176. doi:10.1007/s13753-015-0050-9
6. World Health Organization, PAN American Health Organization. Hospital safety index: guide for evaluators; 2015. Available from: https://www.who.int/publications/i/item/9789241548984.
7. Luke J, Franklin RC, Dyson J, Aitken P. Building toward a disaster resilient health system: a study of hospital resilience. Disaster Med Public Health Prep. 2022;17(e219):1–8.
8. Raeisi AR, Torabipour A, Karimi L. Evaluating hospital safety index in Susa public hospital: an action research study. Bali Med J. 2018;7(2):457–461. doi:10.15562/bmj.v7i2.845
9. Söderin L, Agri J, Hammarberg E, Lennquist-Montán K, Montán C. Hospital preparedness for major incidents in Sweden: a national survey with focus on mass casualty incidents. Eur J Trauma Emerg Surg. 2023;49(2):635–651. doi:10.1007/s00068-022-02170-z
10. Lamine H, Chebili N, Zedini C. Evaluating the level of disaster preparedness of tunisian university hospitals using the hospital safety index: a nationwide cross-sectional study. Afr Health Sci. 2022;22(3):666–673. doi:10.4314/ahs.v22i3.71
11. Aladhrai SA, Djalali A, Della Corte F, Alsabri M, El-Bakri NK, Ingrassia PL. Impact of the 2011 revolution on hospital disaster preparedness in Yemen. Disaster Med Public Health Prep. 2015;9(4):396–402. doi:10.1017/dmp.2015.30
12. Boateng-Osei EA, Osei I, Diji AKA, et al. Emergency preparedness capacity of a university hospital in Ghana: a cross-sectional study. Afr J Emerg Med. 2023;13(3):152–156. doi:10.1016/j.afjem.2023.05.001
13. Darwish EHB, Ramadan AM, Abdelsalam WN, Ibrahim AG, Foda NMT. Assessment and development of hospital emergency preparedness plan in response to COVID-19 pandemic in Alexandria university hospitals. Alexandria J Med. 2022;58(1):69–77. doi:10.1080/20905068.2022.2075159
14. Gopinathan V, Kunju SA, Krishnan SV, Sirur FM, Balakrishnan JM. Assessment of the preparedness and planning of academic emergency departments in India during the covid-19 pandemic: a multicentric survey. Disaster Med Public Health Prep. 2022;16(5):1910–1915.
15. Dahmash EZ, Madi T, Shatat A, et al. Assessment of hospital readiness to respond to covid-19 pandemic in Jordan-a cross sectional study. Int J Environ Res Public Health. 2023;20(1798):1–20. doi:10.3390/ijerph20031798
16. Tiruneh A, Yetneberk T, Eshetie D, Chekol B, Gellaw M. A cross-sectional survey of covid-19 preparedness in governmental hospitals of north-west Ethiopia. SAGE Open Medicine. 2021;9:1–6. doi:10.1177/2050312121993292
17. Singh P, Lamine H, Sapkota S, Bahattab A, Eriksson A. Management of mass-casualty incidents in Nepal: a qualitative case study of three district hospitals in Nepal. Prehosp Disaster Med. 2023;38(5):606–611. doi:10.1017/S1049023X23006209
18. Parajuli B, Jimee G, Guragain R, editors. Developing and implementing emergency response plan of a zonal hospital in Nepal. In:
19. Government of Nepal, Ministry of Home Affairs. Nepal disaster report 2019; 2019. Available from: https://www.climatenepal.org.np/sites/default/files/doc_resources/NDR%202019_report.pdf.
20. Government of Nepal, Ministry of Home Affairs. Nepal disaster report focus on reconstruction and resilience; 2024. Available from: https://dpnet.org.np/resource-detail/2086.
21. Government of Nepal, National Planning Commission. Nepal earthquake 2015 post disaster needs assessment VoL. A: key findings; 2015. Available from: https://reliefweb.int/report/nepal/nepal-earthquake-2015-post-disaster-needs-assessment-vol-key-findings.
22. Committee on Joint Initiative on Earthquake Preparedness and Disaster Relief in Nepal of the American Society of Nepalese Engineers (ASNEngr), America Nepal Medical Foundation (ANMF), and Computer Association of Nepal – USA (CAN-USA). Earthquake preparedness and disaster relief in nepal a position paper; 2015. Available from: https://www.gnpn.org/wp-content/uploads/2016/07/earthquake_pereparedness.pdf.
23. Government of Nepal, Ministry of Health. Response and beyond: the road to resilience health sector interventions following the Nepal earthquake 2015 and lessons learned; 2017. Available from: https://heoc.mohp.gov.np/uploads/publications/file/64883622568f9.pdf.
24. Phuyal N, Bajracharya S, Adhikari A, Katwal S, Shrestha A. Development and update of hospital disaster preparedness and response plan of 25 hub hospitals of Nepal – process documentation. J General Pract Emerg Med Nepal. 2023;10(15):53–59. doi:10.59284/jgpeman229
25. Bajracharya S, Shrestha A. Implementation of a disaster coordination and communication plan in Nepal: hub and satellite concept. Prehosp Disaster Med. 2019;34(s1):s79. doi:10.1017/S1049023X19001651
26. Shakya YR, Patel JN, Shrestha R, et al. Current understanding of emergency medicine and knowledge, practice, and attitude toward disaster preparedness and management among healthcare workers in Nepal. Kathmandu Univ Med J. 2024;87(3):290–295.
27. Shrestha N, Mishra SR, Ghimire S, et al. Health system preparedness for covid-19 and its impacts on frontline health-care workers in Nepal: a qualitative study among frontline health-care workers and policy-makers. Disaster Med Public Health Prep. 2022;16(6):2560–2568. doi:10.1017/dmp.2021.204
28. Shrestha GS, Paneru HR, Acharya SP, et al. Preparedness for coronavirus disease in hospitals of Nepal: a nation-wide survey. J Nepal Med Assoc. 2020;58(224):248–251. doi:10.31729/jnma.4941
29. Bhattarai S, Neopane AK, Shrestha B, et al. Isolation and intensive care (ICU) service, surge capacity and pandemic training in government designated covid-19 clinics and hospitals of Nepal. Kathmandu Univ Med J. 2022;20(2):224–228. doi:10.3126/kumj.v20i2.51403
30. Borhannejad Z, Madah SBS, Khankeh HR, Falahi Khoshknab M, Rezasoltani P, Ahmadi S. Effect of hospital incident command system establishment on the preparedness level of disaster committee and nursing staff of imam ali hospital, zarand, Iran, 2010. Health Emerg Disasters Q. 2019;4(2):101–108. doi:10.32598/hdq.4.2.101
31. Moyal-Smith R, Barnett DJ, Toner ES, Marsteller JA, Yuan CT. Embedding equity into the hospital incident command system: a narrative review. Jt. Comm J Qual Patient Saf. 2024;50(1):49–58. doi:10.1016/j.jcjq.2023.10.011
32. Murphy JP, Kurland L, Rådestad M, Rüter A. Hospital incident command groups’ performance during major incident simulations: a prospective observational study. Scand J Trauma Resusc Emerg Med. 2020;28(1):73. doi:10.1186/s13049-020-00763-4
33. Kaye AD, Cornett EM, Kallurkar A, et al. Framework for creating an incident command center during crises. Best Pract Res Clin Anaesthesiol. 2021;35(3):377–388. doi:10.1016/j.bpa.2020.11.008
34. Housing Recovery and Reconstruction Platform. 18 moderately affected districts; 2018. Available from: https://www.preventionweb.net/files/63268_18moderatelyaffecteddistrictsovervi.pdf.
35. Austin Z, Sutton J. Qualitative research: getting started. Can J Hosp Pharm. 2014;67(6):436–440. doi:10.4212/cjhp.v67i6.1406
36. Cassell C, Symon G. Essential Guide to Qualitative Methods in Organizational Research.
37. Bahrami P, Ardalan A, Nejati A, Ostadtaghizadeh A, Yari A. Factors affecting the effectiveness of hospital incident command system; findings from a systematic review. Bull Emerg Trauma. 2020;8(2):62–76. doi:10.30476/BEAT.2020.46445
38. Shooshtari S, Tofighi S, Abbasi S. Benefits, barriers, and limitations on the use of hospital incident command system. J Res Med Sci. 2017;22:36. doi:10.4103/1735-1995.202146
39. World Health Organization. Hospital emergency response checklist. An all-hazards tool for hospital administrators and emergency managers; 2011. Available from: https://www.who.int/docs/default-source/documents/publications/hospital-emergency-response-checklist.pdf.
40. Ahmed SK, Mohammed RA, Nashwan AJ, Ibrahim RH, Abdalla AQ, Ameen BMM. Using thematic analysis in qualitative research. J Med Surg Public Health. 2025;6:100198. doi:10.1016/j.glmedi.2025.100198
41. World Health Organization. Workshops to develop hospital disaster preparedness and response plans in sudurpashchim, karnali and lumbini provinces concludes; 2024. Available from: https://www.who.int/nepal/news-room/item/22-12-2024-workshops-to-develop-hospital-disaster-preparedness-and-response-plans-in-sudurpashchim--karnali-and-lumbini-provinces-concludes.
42. World Health Organization. Key approaches to strengthening emergency preparedness and response. Available from: https://www.who.int/europe/emergencies/our-work-in-emergencies/key-approaches.
43. Alruwaili AS, Islam MS, Usher K. Comparison of the level of disaster preparedness between private and government hospitals in Saudi Arabia: a cross-sectional Study. Disaster Med Public Health Prep. 2023;17(e335):1–10.
44. Koka PM, Sawe HR, Mbaya KR, et al. Disaster preparedness and response capacity of regional hospitals in Tanzania: a descriptive cross-sectional study. BMC Health Serv Res. 2018;18(835):1–7. doi:10.1186/s12913-018-3609-5
45. Ayenew T, Tassew SF, Workneh BS. Level of emergency and disaster preparedness of public hospitals in northwest Ethiopia: a cross-sectional study. Afr J Emerg Med. 2022;12(3):246–251. doi:10.1016/j.afjem.2022.05.007
46. Doucet J, Shatz DV, Kaplan LJ, et al. Are trauma surgeons prepared? A survey of trauma surgeons’ disaster preparedness before and during the covid-19 pandemic. Trauma Surg Acute Care Open. 2023;8(1):e001073. doi:10.1136/tsaco-2022-001073
47. Cordeiro L, Gnatta JR, Ciofi-Silva CL, et al. Personal protective equipment implementation in healthcare: a scoping review. Am J Infect Control. 2022;50(8):898–905. doi:10.1016/j.ajic.2022.01.013
48. Kuikel BS, Shrestha A, Xu DR, et al. A critical analysis of health system in Nepal: perspective’s based on covid-19 response. Dialogues Health. 2023;3:100142. doi:10.1016/j.dialog.2023.100142
49. Proskauer. Lessons from the covid-19 pandemic: planning for disaster preparedness and emergency management in hospitals; 2021. Available from: https://www.healthcarelawbrief.com/2021/10/lessons-from-the-covid-19-pandemic-planning-for-disaster-preparedness-and-emergency-management-in-hospitals.
50. Omer Z, Kahloon OI, Khan MH, Muhammad AI, Arshad F, Iqbal MJ. Level of hospital preparedness for internal disasters in tertiary care hospitals in Pakistan (rawalpindi city). Medforum. 2023;34(1):37–42.
51. The World Organization of Building Officials. Nepal: national building code updated – seismic design of buildings; 2021. Available from: https://wobo-un.org/nepal-national-building-code-updated-seismic-design-of-buildings.
52. Lestari F, Darmawan ES, Modjo R, Dane S. Are indonesian hospitals ready to response to disaster ? Hospital disaster preparedness in west java province. J Res Med Dent Sci. 2020;8(4):89–93.
53. Heidaranlu E, Khankeh H, Ebadi A, Ardalan A. An evaluation of nonstructural vulnerabilities of hospitals involved in the 2012 east Azerbaijan earthquake. Trauma Mon. 2017;22(2):1–6.
54. Kirsch TD, Mitrani-Reiser J, Bissell R, et al. Impact on hospital functions following the 2010 Chilean earthquake. Disaster Med Public Health Prep. 2010;4(2):122–128. doi:10.1001/dmphp.4.2.122
55. Obando Zegarra R, Arévalo-Ipanaqué JM, Aliaga Sánchez RA, Cernuda Martínez JA, Delgado Echevarría JC, Arcos González P. Disaster preparedness and hospital safety in state hospitals in Lima (Peru). Prehosp Disaster Med. 2023;38(5):601–605.
56. Djalali A, Ardalan A, Ohlen G, et al. Nonstructural safety of hospitals for disasters: a comparison between two capital cities. Disaster Med Public Health Prep. 2014;8(2):179–184. doi:10.1017/dmp.2014.21
57. Rokka D, Khanal N. Job satisfaction of health professionals working in governmental tertiary level hospitals of Nepal. Am J Med Sci Innov. 2023;2(1):39–46. doi:10.54536/ajmsi.v2i1.1330
58. Nepal Samaj. Lack of O&M survey in hospitals hampers service delivery: health minister Yadav; 2024. Available from: https://nepalsamaj.com/en/lack-of-om-survey-in-hospitals-hampers-service-delivery-health-minister-yadav.
59. Munasinghe NL, O’Reilly G, Cameron P. Examining the experience and lessons learnt for disaster-preparedness in Sri Lankan hospitals: a scoping review. Int J Disaster Risk Reduct. 2021;64:102494. doi:10.1016/j.ijdrr.2021.102494
60. Robredo JP, Ong B, Eala MA, Naguit RJ. Outmigration and unequal distribution of Filipino physicians and nurses: an urgent call for investment in health human resource and systemic reform. Lancet. Reg Health West Pac. 2022;25:100512.
61. Makuku R, Mosadeghrad AM. Health workforce retention in low-income settings: an application of the root stem model. J Public Health Policy. 2022;43(3):445–455. doi:10.1057/s41271-022-00361-x
62. Government of Nepal, Ministry of Health and Population, Quality Standards and Regulation Division. Checklist to identify the gaps in quality improvement of tertiary hospitals; 2019. Available from: https://msshealth.org.np/UploadDocument/Tertiary%20MSS%20Book.pdf.
63. Munasinghe NL, Matsui K. Examining disaster preparedness at matara district general hospital in Sri Lanka. Int J Disaster Risk Reduct. 2019;40:1–10. doi:10.1016/j.ijdrr.2019.101154
64. Saeid M, Khankeh H, Habibisoola A, Mohammadali M, Hamidkolg G, Dadkhah B. Investigating hospital preparedness in ardabil province against unexpected accidents. Health Emerg Disasters Q. 2019;4(3):127–134. doi:10.32598/hdq.4.3.127
65. Samei B, Babaie J, Sadegh Tabrizi J, et al. Factors affecting the functional preparedness of hospitals in response to disasters: a systematic review. Bull Emerg Trauma. 2023;11(3):109–118. doi:10.30476/BEAT.2023.97841.1414
66. Ministry of Health – Manatū Hauora. National reserve supplies. Available from: https://www.health.govt.nz/strategies-initiatives/programmes-and-initiatives/emergency-management/national-reserve-supplies.
67. Transparency International Nepal. A study of public procurement in the health sector and availability of procurement data; 2020. Available from: https://www.tinepal.org/a-study-of-public.
68. Adhikari B, Ranabhat K, Khanal P, et al. Procurement process and shortages of essential medicines in public health facilities: a qualitative study from Nepal. PLOS Glob Public Health. 2024;4(5):e0003128. doi:10.1371/journal.pgph.0003128
69. Pal R. Procurement for health care service requirements: securing services and maintaining timelines during the covid-19 pandemic. Narayana Med J. 2022;11(1):22–30.
70. Acharya KK, Chandrika A. Federalism practice in Nepal prospects and upshots. J South Asian Stud. 2021;9(1):1–14. doi:10.33687/jsas.009.01.3403
71. United Nations Officer for Disaster Risk Reduction. Engaging with stakeholders. Available from: https://www.undrr.org/engaging-with-stakeholders.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.