Back to Journals » Risk Management and Healthcare Policy » Volume 14
Exploring Barriers to Effective Implementation of Public Health Measures for Prevention and Control of COVID-19 Pandemic in Gamo Zone of Southern Ethiopia: Using a Modified Tanahashi Model
Authors Boti Sidamo N ![]() , Hussen S
, Hussen S ![]() , Shibiru T
, Shibiru T ![]() , Girma M, Shegaze M
, Girma M, Shegaze M ![]() , Mersha A
, Mersha A ![]() , Fikadu T
, Fikadu T ![]() , Gebru Z, Andarge E
, Gebru Z, Andarge E ![]() , Glagn M
, Glagn M ![]() , Gebeyehu S, Oumer B
, Gebeyehu S, Oumer B ![]() , Temesgen G
, Temesgen G
Received 6 January 2021
Accepted for publication 6 March 2021
Published 19 March 2021 Volume 2021:14 Pages 1219—1232
DOI https://doi.org/10.2147/RMHP.S297114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Negussie Boti Sidamo,1 Sultan Hussen,1 Tamiru Shibiru,2 Meseret Girma,1 Mulugeta Shegaze,1 Abera Mersha,3 Teshale Fikadu,1 Zeleke Gebru,1 Eshetu Andarge,1 Mustefa Glagn,1 Selamawit Gebeyehu,1 Bilcha Oumer,4 Gebremaryam Temesgen5
1School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 2School of Medicine, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3School of Nursing, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 4Department of Midwifery, College of Health Sciences, Arba Minch, Ethiopia; 5Department of Midwifery, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Negussie Boti Sidamo
School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Email [email protected]
Background: Since the occurrence of the COVID-19 pandemic, different public health measures have been implemented to prevent and control the further spread of the disease. However, barriers that influence the effective implementation of public health measures were not explore in Ethiopia especially in study Area. Therefore, this study tried to fill this gap by exploring the barriers to effective implementation of public health measures for prevention and control of the COVID-19 pandemic in the Gamo Zone of southern Ethiopia.
Methods: The study employed a qualitative study with a phenomenology approach among purposely selected 30 individuals in the community and selected institutions. Key informant interview was used to collect the data. The data were transcribed verbatim and translated into the English language. The transcribed data were read several times to clearly understand the content for further analysis. The analysis of the data was conducted based on the modified Tanahashi framework.
Results: The study identified different barriers under five main themes: accessibility, acceptability, availability, contact and use, and effective implementation of public health measures related to barriers. The main barriers to effective implementation of public health measures were resistance to change, negligence, lack of community engagement, insufficient training for front line workers, poor supportive supervision, poor law enforcement, and lack of continuous community awareness creation. Beside, acceptability related barriers like cultural and religious norms and availability related barriers like shortage of personal protective equipment and shortage of skilled health professional have also lion share barriers for implementation of the public health measures.
Conclusion: The study identified different personal, institutional, and societal level barriers for effective implementation of public health measures for the COVID-19 pandemic. Therefore, proper and targeted continuous community awareness creation with further mandatory law enforcement activities should be implemented by the concerned bodies to mitigate individual and societal level barriers. In addition, the government with relevant stakeholders should give due attention to equip and protect the frontline professionals by availing the necessary logistic and provision of continuous capacity-building activities.
Keywords: COVID-19, effective implementation, public health measures, modified Tanahashi model, barriers, Gamo zone
Background
World Health Organization (WHO), declared the COVID-19 outbreak as a global pandemic on March 11, 2020.1,2 COVID-19 has rapidly spread all over the world.3 In Ethiopia, COVID-19 cases continue to increase exponentially with a rapid epidemic doubling time.4 Till the study period there are no specific therapeutics and vaccines available for the disease, the epidemic of COVID-19 is posing a great threat to global public health.5 It disrupts health systems and affects human health globally, it is crucial to protect those most impacted by COVID-19, sustain gains made to address other infectious diseases, and maintain people’s access to life-saving health services.6 The public health systems in Africa are coming under severe strain as the unprecedented COVID-19 pandemic persists.7,8
WHO develop different mitigation and suppression strategies to prevent and control COVID 19 pandemic.9 Among mitigation approaches quarantine, social distancing, and isolation were strategies used to slow the spread of the pandemic. However, implementing Non-Pharmaceutical Interventions (NPI) such as strict lockdowns, social distancing, and closing of schools, community places, businesses, and other interventions were strategies used to suppress the transmission rate of COVID19.10 As evidences show that suppression strategies were more effective than mitigation strategies.10–12
Different countries have adopted different strategies to prevent and control COVID 19 pandemic.10 Ethiopia also Ethiopia Government adopted the basic public health measures recommend by WHO since the first COVID19 case report in Ethiopia on March 13, 2020.13 These include banning large meetings, closing schools/colleges, limiting use of public transportation, suspending sporting and religious gatherings, quarantine, isolation, and lockdowns.4 However, appropriately implementing public health and social (PHS) measures ranging from individuals to large societal level practices are the only available means to control the spread of the virus and minimize its impacts.12,14 The term “public health measures” refers to means to decrease or interrupt transmission of COVID-19 by practicing hand washing, social distancing, wearing the face mask and stay-at-home lockdown measures were means to prevent and control COVID-19 transmission.15–21 A study showed non-pharmaceutical interventions like physical distancing measures were effective in the reduction of infections.22
Despite the recommendations to proper implementation of PHS measures hamper by different barriers.5,23,24 An approach to explore obstacles/challenges faced during implementation of PHS measures for an appropriate decision making technique is Modified Tanahashi Model.25 The Tanahashi model developed in 1978 and subsequently modified is one model that has been adapted to several countries to identify gaps and barriers.13 This modified Tanahashi model is referred to as the Bottleneck Analysis instrument for health systems delivery and highlights five determinants of effective implementation of PHS measures.25 This include availability of essential commodities and human resources for effective implementation (availability coverage), followed by health intervention accessibility (accessibility coverage). Once availability and accessibility coverage are in place, to increase a population’s willingness to use an intervention (acceptability of coverage). Sequential to increase a population’s initial contact and use, and effective implementation of public there will be contact coverage, and effectiveness coverage).13
Most previous studies have published exploring the knowledge, attitudes, and practices towards COVID-19, epidemiology, causes, clinical manifestation, diagnosis, and prevention and control of the novel coronavirus.23,24,26 Some studies exploring the practice of public health measures to prevention and control measures COVID-19.5,17,27 Therefore, this study intended to explore the barriers to effective implementation of public health measures for prevention and control of COVID-19 pandemic in Gamo Zone of southern Ethiopia by using the Modified Tanahashi Model. The study would assist in providing explicit information on the barriers to effective implementation of public health measures, and could suggest solutions to improve the preventive behaviors to prevent and control COVID-19 pandemic. Moreover, the finding of this study would help for future interventions which focus on infectious disease because the prevention and control of those diseases require the community adherence to the recommendation. The responsible body also should consider availability, accessibility, acceptability and effectiveness of the any prevention and control of infectious disease.
Methods
Study Setting
This study was conducted in the Gamo zone, one of the 14 Zones in the Southern Nations, Nationalities, and People’s Regional State (SNNPR) of Ethiopia. The administrative center of Gamo Zone is Arba Minch town. Arba Minch town is located 435 km southwest of Addis Ababa, the capital city of Ethiopia, and 275 km southwest of Hawassa, the capital city of southern nations and nationalities regional state. Currently, in Gamo zone, there is 14 woreda and 4 town administrator.
Study Design
A phenomenological qualitative study approach was carried out to explore barriers for the adherence to public health measures for prevention and control of the COVID-19 pandemic, Gamo zone, Southern Ethiopia.
Selection of Study Sample
A purposive sampling method was employed to recruit key informants. Zonal health manager, district health manager, health center head, health professional, Health development armies (HDA), Health extension workers (HEW), Youth representative, religious leader, community leader, and police leaders were involved in the key Informants’ interview (KII). They are a key source of information because they are directly involved in COVID 19 prevention task force. The task force leader assisted in the selection of the study.
Data Collection and Procedures
We conducted data collection from August 1 to 15, 2020. Data were collected through the key informant interview method. Key Informants Interviews (KII) Guide was prepared by the research team (see the Supporting Information). KII was an important technique to get in-depth information. A semi-structured interview guide was adapted from the modified Tanahashi framework model. All interview information was an audio tape recorder, and keynotes took. Furthermore, to reduce the risk of COVID-19 infection both interviewer and interviewer were used to face mask during the data collection period. Besides this, after each interview, the recorder was clean with a sanitizer. Also, we used a phone call for the interviewee as necessary. The interviewee was conducted in the Amharic language since it is the national language of Ethiopia. The interview was conducted in comfortable environment in a private room. The duration of each KII was between 30 minutes and 60 minutes.
Data Quality Control
Data was collected by experienced public health professionals with a Master’s degree qualification and who had experience in conducting qualitative studies. On-site supervision was being carried out during the whole period of data collection daily by senior qualitative research expertise. To maintain the quality of Intensive training was given for both data collector and supervisor on how to conduct KII. In addition, training on the major sign of Covid-19 was given by senior qualitative research expertise before fieldwork. To establish trustworthiness data were collected by a researcher who was already familiar with the culture of the local organization understudy and who in the current research assumed a neutral role. To achieve data credibility, we used a maximum variation of sampling to get a vast range of views and experiences. Also during the development of the theme, we re-checked original audio and written transcripts. To achieve conformability standards, we used ATLAS Ti7/Open code V4 software to enhance the maintenance of connections between participant descriptions and the interpretation the researcher made. We also present the finding alongside direct quotes from participants. To achieve the dependability of standards, we maintain a record of interview transcripts, translations, and a demographic summary of participants. Also, we write notes during and after interviews.
Data Analysis
An audio recorder was used to record the interviewee. This record was transcribed verbatim in the Amharic language. The transcription was checked independently by the supervisors for verification for accuracy with simultaneous audio playing. After validation of the Amharic transcript, it was translated the text into the English language. The data were analysed through thematic content analysis. Major themes were derived based on the research questions. However, subthemes were induced from the text itself through repeated reading. After reading the transcripts, the research team was identified emergent themes, and then coded each theme to delineate individual topics identified during the discussions. A transcript was coded using ATLAS Ti7/Open code V4 software. The finding was presented in narratives by thematic areas based on the research questions. The unit of analysis for this study was a meaningful statement, ranging in length from a word to one or two complete sentences. The first phase of the analysis was the line by line coding; key phrases of the transcripts, in participants’ own words, were identified and underlined. The underlined codes were rephrased into a shorter code phrase in the second phase of the analysis. Subsequently, that phrase with similar meanings was brought to the most useful unit of content analysis. In the final stage of analysis named, categories were generated through further abstraction and grouping of subcategory themes.
Ethical Consideration
Ethical clearance was obtained from the Institutional Research Ethics Review Board (IRB) of Arba Minch University with the reference number of IRB/411/12. Before the fieldwork, necessary communications about the overall purpose of the study was made with the zone, woreda/town, and kebeles/community level administrative bodies. Written informed consent was secured from study participants after explaining the objective and purpose of the study to each study participant. They also agree for the publication of their response to journals. To maintain confidentiality, no personal identifiers were used on data collection forms and the recorded data were not accessed by a third person, except the principal investigators. All recommended COVID-19 preventions measures were applied to protect the data. The suspected cases were linked with the nearby health facility COVID-19 task forces. Besides, this study was conducted in accordance with the Declaration of Helsinki, and all ethical and professional considerations were followed throughout the study to keep participants’ data strictly confidential.
Results
Socio-Demography Characteristics of Participants
Interviews were conducted with a total of 30 key informants from zonal health managers, district health managers, Health center heads, Health professionals, HEW, HDA, Youth representatives, Religious leaders, community leaders, and a representative from law enforcement bodies. The interviews lasted between 25 and 60 minutes (on average 40 minute) (Table 1).
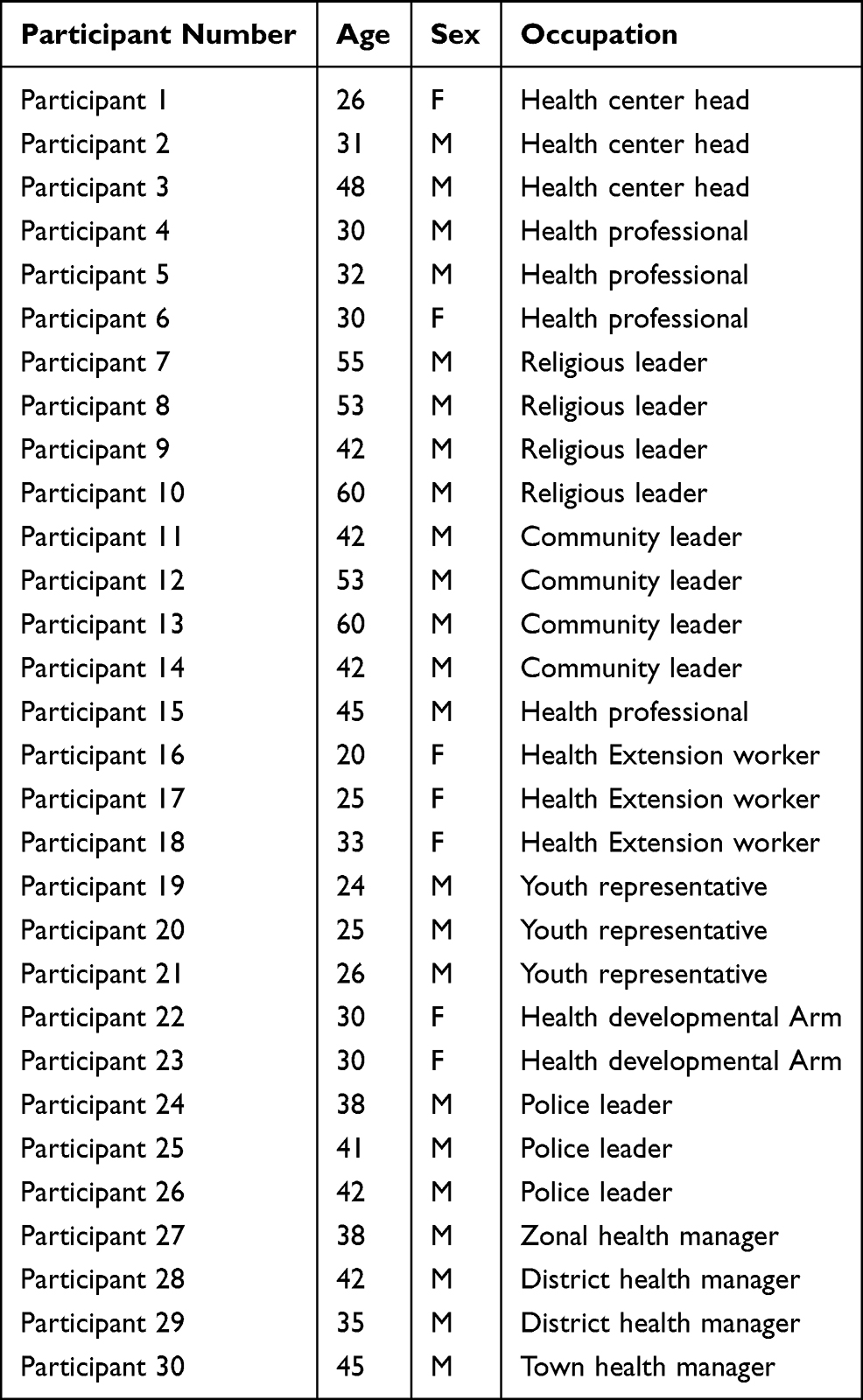 |
Table 1 Socio-Demography Characteristics of Participants of the Barriers for Effective Implementations of Public Health Measures Towards COVID-19 Pandemic in Gamo Zone, Southern Ethiopia, 2020 |
Barriers of the Effective Implementations of Public Health Measures for COVID-19
This study identified several individuals, institutional, and societal level barriers for effective implementations of public health measures for prevention and control of COVID-19 as subthemes under the predetermined five main themes (Availability, Accessibility, Acceptability, Contact and use, and effectiveness of public health measures) (Table 2).
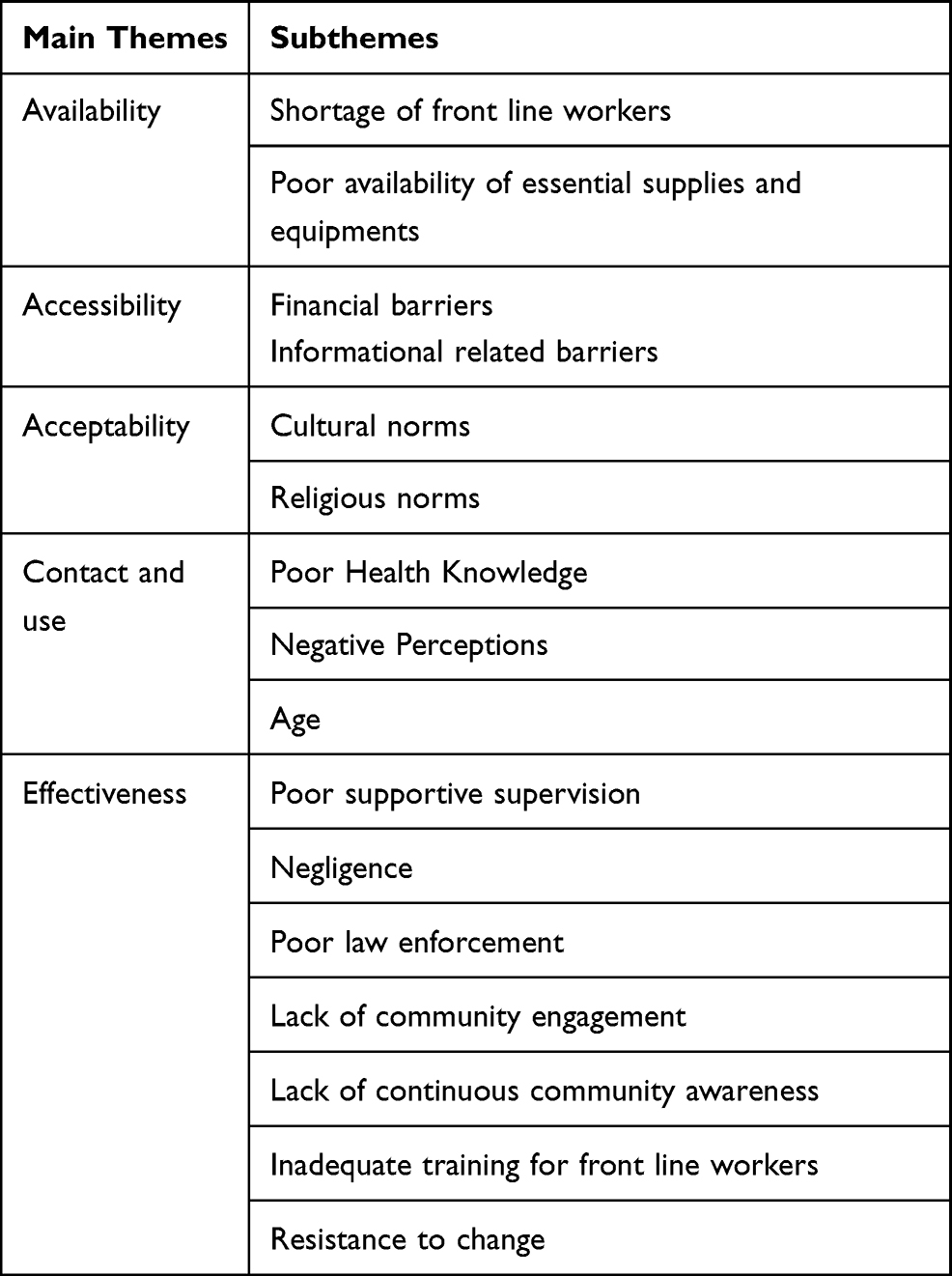 |
Table 2 The Main and Subthemes of the Barriers for Effective Implementations of Public Health Measures Towards COVID-19 Pandemic in Gamo Zone, Southern Ethiopia, 2020 |
Theme One: Availability
The availability dimension of effective implementation of an intervention is used to measure the availability of sufficient recourses like adequate supply and appropriately equipped frontline workers and materials for effective implementation of the program. The shortage and in-adequately prepared and equipped frontline workers were identified as the main barriers for effective implementation of public health measures for prevention and control of COVID-19.
Subtheme: Shortage of Front Line Workers
According to the key informants from the frontline community health workers, the implementation of the public health measures to control and prevent COVID-19 in the community was challenged by the limited number of community health workers.
“One health extension is scheduled to reach twenty houses per day. When we do home-to-home visits we educate them to practice frequent hand washing and avoid going to a place where people gather in mass and keep distance in public gatherings and main ways of transmission. Doing all those activities was difficult for one health extension”. (Participant 16)
The shortage of health care workers further compromises the routine delivery of health care provision. Since the majority of the health professionals were focusing on prevention and control of COVID-19 at the community level. COVID-19.
“There is a shortage of health workers and in fact, only one health officer & nurse were performing all tasks in the health center. All other health workers were assigned to the field for community work. This does not mean that community activities are valueless, but the problem in the health center is not less than that of the communities”. (Participant 3)
Subtheme: Poor Availability of Essential Supplies and Equipments
The availability of adequate and proper supplies and equipment like personal protective equipment (PPE) is vital to effectively implement the lifesaving public health measures to control and prevent the COVID-19 pandemic. According to most key informants from COVID-19 task forces and frontline workers (health care professionals and Police), even these essential equipment were not adequately available for people at the frontline of the war against the pandemic. The shortage of supplies and equipment put the life of front line workers at risk and further compromise the effectiveness of implementation essential public health measures.
“The task force members do not have facemask. For instance, if one case is identified, we do not have PPE to wear. I have this one facemask and reserved it to use in case a suspected case comes. Otherwise, it would be challenging to initiate management right away in case one comes”. (Participant 1)
“As you can see the mask that I wear now must be used only for 4–6 hours. Surgical mask can only be used for a maximum of 4 to 6 hours. There are big problems with supplies where we are only provided once in two months. Even I have been using this mask for over two weeks”. (Participant 3)
“First the Officials need to protect themselves but the lack of gloves, sanitizer and alcohol were very challenging … ”. (Participant 26)
Furthermore, the participants of the study from the health care sector reported that the basic recourses for the implementation of public health measures were inadequately available for the community to properly practice the measures.
“Sanitizer is not available. Even the community members have asked us challenging questions like ‘In the absence of adequate water how would you tell us to prevent the virus with water and soap? “. (Participant 1)
Theme Two: Accessibility
According to the modified Tanahashi model, accessibility-related barriers are also influencing the effective implementation of any intervention. The direct out-of-pocket expenditure and indirect opportunistic cost and information related barriers were mainly identified as the barriers for accessing the public health measures to effectively prevent and control the COVID-19 pandemic.
Subtheme: Financial Barriers
The opportunistic cost was mainly impacting the implementation of the public health measures in the study area. Almost all informants responded that majority of the community members could not be at home due to the large segment of the population support the family based on the income from daily activities.
“those people with low economic status will not be able to stay home because they must go to work every day to meet the needs of their daily livelihood”. (Participant 8)
“With regard to the economy, people are poor they don’t have anything to eat so that they are forced to move to different places because food is the basic need. Poor people don’t have reserves or anything saved”. (Participant 4)
“Let corona kill me rather than hunger kills me. Many of the town people’s livelihood is based on jobs of daily laborers, wood collection, & making cloths. He couldn’t stay home without providing his family necessities for daily livelihood. These things identified our basic necessities of life. If they stayed home they couldn’t be able to get it”. (Participant 12)
“In order to do this (stay at home), our income decreasing. Everyone must move from place to place to meet for his lunch & dinner. They eat their lunch from their morning earning & their dinner from their late afternoon earning. The rule that advocates staying at home needs to be revised because people are saying that they rather die of COVID-19 than hunger”. (Participant 28)
The effect of the pandemic on the economy also affects the income of only the poor nation but also the developed nations. This scenario further exacerbates the ability of the poor nation to access essential public health measures. The majority of the informants from the key population confirmed that the community member was challenged to access the measures due to their low economic status.
“They (the community members) do not have the capability to buy a mask. Corona is posing a difficulty. As a result of the corona, many job options have been closed & people are losing everything they would get for their daily livelihood. There are so many people working as a car driver in banana carrying cars & daily laborers. What would they if you tell them to stay at home? What he will provide his children to eat because they have lost all of their income. Peoples are saying that they rather die of corona than hunger”. (Participant 22)
Subtheme: Informational Related Barriers
The poor access to public health intervention is further exacerbated by the lack of community awareness about public health measures. Most of the respondents said that there are peoples who have no access to information about the intervention to effective prevent and control the pandemic.
“I think especially the daily laborer section of the population lack awareness. There are people who do not own radio & television. They have many challenges with practicing many issues. Those who are economically capable and literate wear masks because they are well aware and are better at staying at home. If you see children’s of a daily laborer they most of the time they spent outdoor and weak in practicing measures”. (Participant 3)
Theme Three: Acceptability of Public Health Measures
The availability and accessibility of public health interventions are not exclusively guaranteed the effective utilization of the services without accepting the service. The acceptability of health interventions is perceived to be limited by the religious, cultural, and gender norms of the community. The finding of this study showed that the acceptability of public health interventions mainly affected by cultural and religious norms.
Subtheme: Cultural Norms
What became clear during all of the interviews conducted in this qualitative study is that Ethiopian culture, which is deeply patriarchal, presents the greatest barrier to accept public health interventions during the era of COVID 19. The fear of isolation from the community was mostly identified as the barriers to accepting the measures that promote social distancing.
“It is not unto your will to attend mourning services because family the deceased will stigmatize you if you didn’t accompany them & you might lose your beloved one someday. If I didn’t attend to his mourning & might lose someone. As a result of this no one of his family members would come to me and it so difficult. In order to stop this, I think it would be better to hang a robe so that family members will situate on the other side while people attending them will socially distance themselves & return back”. (Participant 8)
The long-standing culture of practicing social gathering during the occurrence of vital events, compromise the acceptance of the public health measures by the community which further challenge the effective implementation of the measures against the COVID-19 pandemic.
“I think the culture they have grown up with is challenging. They celebrate together all their rituals including mourning, marriage & birthdays. The social gathering was strong … ”. (Participant 14)
“ In our area mourning & marriage is similar. It is difficult if you didn’t involve in the marriage ceremony & mourning service. It is challenging to make tell them to stop doing this”. (Participant 9)
The acceptance of the intervention is further compromised by falsely perceived long-standing cultures that relate social distance with being handicapped in the community.
“According to our culture staying home is equivalent to being handicapped. When a person stays at home they thought of him as a disabled one” Staying home is the main way to prevent covid 19 diseases. Staying home means stopping a relationship with others … ”. (Participant 3)
Some study participants said that handshake is a way to show special respect.
“Even though I decided not to shake hands others will force me to shake hands. Our elders give their hands to shake my hands. If I refuse to shake their hand, they will not accept me. Unless the community act in a similar way it would be meaningless because all my family members were practicing handshaking”. (Participant 22)
Subtheme: Religious Norms
Religious related norms in the community were identified as the major barriers to effectively implement public health measures against the COVID-19 pandemic. The information from most of the respondents indicating that the pandemic is happened due to the evil act of the human race and the solution is only from God than the public health measures.
“There is a misunderstanding that GOD will protect us, but this is men’s doing. Some advocate prayer to GOD & there is a think that mask is not the solution to this disease. But the need to take precaution is indicated in GOD’S words. Besides this, we do have a gap. There is a problem of inaction with the executive branch”. (Participant 10)
“they (the community members) believe that this is God works so that it would be lifted when its time come though they wonder outdoor and indoor as usual” (. (Participant 7)
Personal religious beliefs about the public health measures were further exacerbated by the teaching of the religious leaders about the pandemic.
“As a member of this community, what I repeatedly witnessed is influence from religion where religious fathers say that the disease will not occur in this area as far as they are praying. It is a perception that the disease will not reach them & GOD will protect them … ”. (Participant 2)
Theme Four: Initial Contact and Use
The fourth dimension of the modified Tanahashi model’s initial utilization of public health measures is characterized by the actual utilization of the service. The effective implementation of the public health measures might be affected by the absence of the actual utilization of the measures while the measures are available, accessible, and acceptable In this study, the major barriers that hamper the actual implementation of the public health measures against the COVID-19 pandemic were poor health knowledge, age, and negative perception about the pandemic and the public health measures.
Subtheme: Poor Health Knowledge
The findings from this study showed that most of the community members have poor literacy levels about the general health-related issues and the pandemic.
“The reason that made the community rejects the information provided by the government and/or health workers is that they think the disease is similar to other communicable diseases that they know of before. But if they understand it all such matters wouldn’t be an issue. Even now we need to strengthen our effort and educate the community until they become fully aware”. (Participant 7)
“Most people perceive the disease as simple as cold which will immediately pass if they get infected & think that they will not die if they have no history of HIV, DM, HIV, and Cardiac comorbid disease”. (Participant 2)
Some of the study key informants mentioned that rumors and misconceptions about the diseases and public health measures can lead to the ineffective implementation of public health measures.
“some people think that this is just a rumor and the disease will not kill us & some of them consider it us a common cold & it will disappear by itself. Why they exaggerate it”. (Participant 6)
“so much false information happens to circulate within the community at the beginning. I think it would take too long for this community to be liberated from the false information once they hear. It has been said that the disease will not occur in Africa & Ethiopia, but it did & counted in thousands. But there is a misconception within the community”. (Participant 3)
Subtheme: Negative Perception
The insufficient understanding of the diseases and the value of seeking the public measures results from the community to have an improper perception about the disease and the public health measures for controlling and preventing the COVID-19 pandemic.
“some people have a thinking that because this area is hot & the virus couldn’t tolerate heat & this all made the community to be reluctant”. (Participant 25)
“Considering themself as wise, we are a believer of GOD & it will not infect us, our prophet has told us so that the disease didn’t really exist”. (Participant 18)
The negative perceptions were further exacerbated by the teaching of the religious leaders about the disease is happened from the GOD and no need of implementing the public health measures despite the teaching of religious scriptures.
“Some advocates prayer to GOD & there is a think that mask is not the solution to this disease. But the need to take precaution is indicated in GOD’S words. Beside this we do have a gap”. (Participant 13)
“Even religious leaders say that ‘it is GOD who brought it & let him resolve it, our caution will not save us’. So that, don’t get us in conflict with GOD, & you are making the disease to spread more clash & they protest against”. (Participant 25)
Subtheme: Age
The majority of study participants said the most challenging section of the population not implementing public health measures were adolescents. However, elders were very cautious to practice public health measures because most of the elders perceive themselves as more vulnerable to the infection and a small chance of recovery.
“Most of the time adolescents are the challenging population segments. They are the one who organizes & participate in spiritual programs. They go out together to enjoy themselves. Together they chew chat & enjoy”. (Participant 17)
“Those aged 50 years old and above were very cautious where they perceive themselves as more vulnerable to the infection & small chance of recovery” In fact, the adolescent group is the one with higher problems. They are adolescents who are seen in a team of two or more people in chat chewing areas, bars, & hotels. We frighten that adolescent might endanger us”. (Participant 7)
Theme Five: Effectiveness
The fifth dimension of the modified Tanahashi model is the effective utilization of public health measures. This dimension explores the extent of the intended aims of the intervention achieved by effective implementation of the intervention. The ultimate goal of implementing public health measures could be affected by the adherence level of the community and provider compliance. The finding of this study showed that the main barriers that affect the community to effectively implement the public health measures were resistance to change, negligence, lack of community engagement, insufficient training for front line workers, poor supportive supervision, poor law enforcement, and lack of continuous community awareness creation.
Subtheme: Resistance to Change
According to the responses from most of the study participants, the continuous implementation of the measures was mainly affected by the difficulty of the community to get out of the long-standing habits and adopt the public health measures.
“Muslim experts said that ‘abandoning a habit is more difficult than crushed velvet’ which means it is better to be crushed velvet. Rather than ordering them to abandon their habit, it would be better for him to be beaten by a stick. And this wearing mask or distancing is the newly coming practice & also people are innocent that he give due consideration for what other thought of him but it is not issued acceptance. A religious leader condemns nonbelievers and those who do know but reject to stay at home”. (Participant 8)
“It is not because they lack knowledge but it is because they lack the motivation to change. People not only literate but illiterate one has awareness about corona especially town residents. But there is a limitation with regard to implementing it”. (Participant 29)
The lack of adopting the new habits of using public health measures were influenced by the lack of experience and difficulties of adopting the measures.
“So many people claim that lack of experience with mask wearying & type of masks was the challenges determining the practice of mask wearying. Some locally made masks make breathing difficult. Some people say that the communities including them haven’t worn a mask before & currently they wear it because they are obliged to do s” (. (Participant 28)
“Some people claim that wearing a face mask is uncomfortable & cause breathing difficulties. They are unaware & say raise different concerns. If someone is seen wearing a mask it they will be discerned for their use. There are misconceptions that entail individuals who wear a mask are not infected but the others did. Even the claim that sanitizer smells bad and you will be blamed and conspire against you”. (Participant 11)
Subtheme: Negligence
The majority of participants stated that during the early stage of the COVID-19 pandemic most of the community members were implementing public health interventions. However, at the late stage of the COVID-19 pandemic, most of them become careless, negligent and reluctant to implement public health interventions to prevent from COVID-19 pandemic.
“Hand washing is cleanliness by itself & don’t have harm. So those who are don’t implementing this are related to refusal & reluctance related but no other issues. There is no one lacking water but when they told them to wash their hands, they reply with the question of what would happen if they couldn’t wash their hands. The disease seriousness is been told but people tend to disregard it”. (Participant 13)
“Ethiopian is reluctant. I don’t think it is a lack of awareness, but to this day they lack realization & understanding of the thing that will harm or benefit them. Including religious leaders are reluctant. And there is a thinking that GOD himself protects. But GOD himself told us to be cautious. ALLHA says that he did create us with complete body parts. He gave us whole parts so that we better realize things & protect ourselves. And ALLHA also orders us to protect ourselves”. (Participant 8)
Subtheme: Poor Law Enforcement
Lack of uniformity in law enforcement during the implementation of the public health measures was identified as the major barriers that enact the effective continuous utilization of public health measures by the community.
“There is a difference in implementing laws enacted by the government uniformly from place to place. Law is the same for all including legislation in Addis Ababa, SNNPR & that of Arbaminch town is not different for them & you couldn’t ignore it as the context of the town” (. (Participant 30)
“If law enforcement officers didn’t abide by the law others wouldn’t listen to them. I am a health worker and I couldn’t ask others to wear a mask if I serve them without wear a mask. And there are issues like this. I think there will be a change if law enforcement officers enforce the law in collaboration with others”. (Participant 3)
Subtheme: Lack of Community Engagement
The key strategy for successful implementation of any intervention is the active involvement and contribution of the community. However, most of the informants of the study depicted that there were poor utilization and engagement of the community to effectively implement the public health measures against the COVID-19 pandemic. The participants uniformly agreed that there are plenty of locally available effective resources in the community which would have increased the effective implementation of the public health measures by the community members but not actually used by the government.
“In my opinion, the government, religious leaders, tribe leaders, “Abageda”/”Adugawoch” if they educate & condiment at different places, people will listen to them. People will begin to implement if the community condemns & outcast people who didn’t do what they told. For this reason, the government go to cultural places & intensify the integration & it will be good if cultural leaders involve in such tasks in addition to religious leader” . (Participant 25)
“One of the barriers at a local level is not utilizing the available local resource. I think the government isn’t using the already available structures in the community”. (Participant 23)
Subtheme: Lack of Continuous Community Awareness Creation
In addition, some study participants witnessing that the community members did not adhere to public health measures for the COVID-19 pandemic prevention due to a lack of continued community awareness creation and lack of role models.
“At the beginning the task of executing guidelines including awareness creation activities was good but there is a gap in ensuring sustainability”. (Participant 20)
“In our instance, different stakeholders including governmental & non-governmental institutions as well as popular & wealthier persons were involved in community awareness creation tasks. But now when you see the disease is increasing the communities awareness is decreasing”. (Participant 24)
Subtheme: Inadequate Training for Front Line Workers
The majority of study participants from the health facility and health office said that there was a limitation to provide adequate training for the frontline workers.
“It is difficult to claim that the training is adequate. Health professionals could improve one’s knowledge through the use of mass media & the internet in a similar way that the community does, but health workers were not provided with adequate knowledge in order to protect oneself & train and protect others”. (Participant 15)
“In relation to training, there is nothing we have trained on yet … If you are asking me whether we are prepared to prevent if this disease occurred in this Keble, there is no much appraised meant for this disease at the Keble level”. (Participant 13)
It was felt that there was a need for training in how to implement public health interventions; as this is a new pandemic, health professionals are likely to be infected by this pandemic due to their on a regular basis.
“Other than what I have heard from mass media, training was not given to us. As far as this disease is dangerous issues, we have to know something and it is good if some orientation is provided to us because it is better to serve with knowledge than without knowledge. Not only me there are also community volunteers. For example, village & kebele leaders must be provided with the training. If they were not well aware they will bring disease to their family. I think this should not be happening. Even I decided not to go to work. So it is very difficult. It is challenging that if you contract the disease. There is nothing different with regard to supportive supervision”. (Participant 15)
“So far training related to updated issues is not provided even for zone or woreda professionals. We simply update ourselves from what we get from the media. In my view, there is a training gap in reaching all. There will be some improvement if training is given first to zone officials & then reach down all, for example, community influencers including health workers so that they could be made to perform awareness creation activity within the community. Continuous education is necessary to bring behavioral change gradually”. (Participant 27)
There was training on basic concepts of the virus for a limited number of front line workers. The participants claim that the content and number of trainee is inadequate to respond to the pandemic at the expected level.
“Two health officers were trained with the support of Arba Minch University. Other than this there is no training provided for other health workers. Besides what most of us read materials from social media, we are not trained. I believe that every health worker should be trained”. (Participant 2)
Subtheme: Poor Supportive Supervision
The majority of study participants who participate in the COVID 19 prevention and control task force reported that lack of supportive supervision was one of the barriers to the implementation of public health measures.
“There is no supportive supervision even for health care providers in Arba Minch town, the zonal capital town. Even if the zonal office has its own task force delegated to monitor this issue but they have not seen it around. Similarly, no one from woreda office visits these tasks”. (Participant 3)
“I am the leader of a team of six people. There is no one who visited us. There must be monitoring activity on daily basis bout tasks performed, challenges faced & things that are on the right track & the way forward”. (Participant 15)
“There is a task force organized from zone to town level but they aren’t doing monitor activities. Rather than following what work has been done & at what level, it seems task delegation is their responsibility. It is discouraging if there is no supportive supervision while you are working, but it is motivating if there is. And also I think it would be better if there is some form of incentives, but there is no payment made yet & even no one has given a recognition which would bring satisfaction”. (Participant 4)
Discussion
The novel coronavirus is a global pandemic with a highly contagious disease. Until now there is no proven drug and vaccines for this disease. However, effective implementations of public health measures are one strategy for the prevention and control of coronavirus disease (COVID-19) pandemic. Therefore, we apply the modified Tanahashi model to identified barriers for the effective implementation of public health measures for the prevention and control of coronavirus disease (COVID-19) pandemic. The main barriers to effective implementation of public health measures were lack of community engagement, insufficient training for front line workers, poor supportive supervision, poor law enforcement, and lack of continuous community awareness creation. Beside, acceptability related barriers like cultural and religious norms and availability related barriers like shortage of personal protective equipment and shortage of skilled health professional have also lion share barriers for implementation of the public health measures. Moreover, financial barriers and informational related barriers were accessibility-related barriers for implementation of the public health measures.
This study reveals that poor supportive supervision and inadequate training for front-line workers were the main barriers to the implementation of public health measures for prevention and control of the COVID 19 pandemic. This finding is supported by a study conducted in Debretabor town, north-central Ethiopia which says insufficient training is perceived as a major barrier for practicing preventive measures during the pandemic.27 Another cross-sectional study conducted in the Amhara region, Ethiopia also supports our finding.28 The implication of this finding may be during the occurrence of any pandemic there should be capacity building activity like training, and information sources available is crucial to prevent ant infection.29,30
Poor law enforcement and lack of community engagement were barriers to the effective implementation of public health measures for COVID-19 pandemic prevention. This finding is supported by a study conducted in North America.31 Another study conducted in the Democratic Republic of the Congo also supports our finding.32 These outcomes call for further attention on improvements of reinforcing preventive measures, and effective engagement of the community for better implementation of public health measures.
Moreover, misinformation and lack of continued community awareness creation were the barriers to the effective implementation of public health measures for COVID-19 pandemic prevention. This finding with a qualitative study Uganda show mentioned that misinformation regarding the intervention mainly from community individuals who did not understand the interventions or had opposing views to public health measure may cause fear among community members that lead the community member to less adhere to the intervention.33
The main barriers for the implementation of public health measures for prevention of COVID 19 were found within the supply side were a shortage of personal protective equipment like facemasks and scarcity of hand cleaning solutions (Water, soap, alcohol, and sanitizer). This finding is similar to the findings of a study conducted among health professionals in public health facilities of southern Ethiopia29 & Debretabor town, north-central Ethiopia.34 Another systematic literature review study also supports this finding which says lack of resources for implementing public health and social measures is the most influential barrier to implement public health and social measures for preventing transmission of COVID-19.12
From the demand-side, the main barrier for the effective implementation of public health measures for the prevention of COVID 19 was the poor health knowledge about the disease. The finding of this study is supported by a study conducted in Riyadh, Saudi Arabia,26 and South-West Saudi Arabia.14 This finding gives hint that public health awareness creation campaigns should continue to improve community awareness about the disease. The outcome of this study highlighted a growing need for the adoption of innovative local strategies to improve awareness in the general population related to COVID-19 and its preventative practices in order to meet its elimination goals.
The findings of this study reveal that informational and financial related barriers were the main barriers to accessing public health measures for the prevention of COVID 19. This finding is supported by World Health Organization (WHO) recommendations which say barriers to implementing basic hygiene measures, such as hand washing (eg hand basins, sinks or water pumps may be physically inaccessible, or a person may have physical difficulty rubbing their hands together thoroughly).35 Finding from rapid evidence review also support this finding.36 The finding of this study shows that cultural norms and religious norms were the main barriers that affect the acceptability of public health measures. Previous studies conducted in Ethiopia and an integrative narrative literature review study conducted on non-pharmaceutical interventions supports the finding of this study.28,29,37 Finding from the Netherlands reveal that culture is one of the barriers to adhere to public health intervention because it affects effective communication to obtain optimal outcomes.38 This can be explained by the fact that prior to the implementation of any interventions the interventions should be not violating cultural and religious norms. Therefore, before the implementation of any interventions, there should have a discussion with a religious leader, community elders, and community leader for better acceptance of the interventions. This main barrier to the effective implementation of any interventions.
Limitations
This study has lots of strength with regards to applying the theoretical models to conceptually identifying the barriers to implement the public health measures against COVID-19. However, it does not immune to different limitations like unable to conduct the focus group discussion (FGD) to generate more collective individual level barrier factors due to the restriction of mass gathering by the government during the earlier phase of the pandemic. Gathering information only from key informant by in-depth interview might affect the transferability of the result.
Conclusion
The finding of this study showed that the main barriers to effective implementation of public health measures based on modified Tanahashi framework model were effectiveness related barriers like community engagement, insufficient training for front-line workers, poor supportive supervision, poor law enforcement, and lack of continuous community awareness creation). Besides this, acceptability related barriers like cultural and religious norms and availability related barriers like shortage of personal protective equipment and shortage of skilled health professional have also lion share barriers for implementation of the public health measures. Moreover, financial barriers and informational related barriers were accessibility-related barriers for implementation of the public health measures. Therefore, proper and targeted continuous community awareness creation with further mandatory law enforcement activities should be implemented by the concerned bodies to mitigate individual and societal level barriers. In addition, the government with relevant stakeholders should give due attention to equip and protect the frontline professionals by availing the necessary logistic and provision of continuous capacity-building activities.
Abbreviations
IP, Infection Prevention; IRB, Institutional Research Board; HDA, Health development armies; HEW, Health extension workers; KII, Key Informants’ interview; PPE, Personal Protective Equipment; PHS, public health and social; SNNPR, Southern Nations, Nationalities, and People’s Region; WHO, World Health Organization.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
The authors would like to thank Arba Minch University for its financial support. The acknowledgment is also forwarded for the study participants for their valuable information and data collectors and supervisors for their commitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Arba Minch University supports this research financially. The university has no role in the design of the study, collection, analysis, and interpretation of the data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organisation. WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
2. Cucinotta D, Vanelli M, WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020;91(1):157-160.
3. World Health Organization. Infections and infectious diseases: a manual for nurses and midwives in the WHO European region. Available from: https://apps.who.int/iris/bitstream/handle/10665/107489/e79822.pdf.
4. Ministry of Health Ethiopia. National Comprehensive COVID19 Management Handbook; 2020. Available from: https://extranet.who.int/goarn/national-comprehensive-covid19-management-handbook.
5. Khan S, Ali A, Shi H, et al. COVID-19: clinical aspects and therapeutics responses. Saudi Pharm J. 2020;28(8):1004–1008. doi:10.1016/j.jsps.2020.06.022
6. USAID, PEPFAR. Strategic Considerations for Mitigating the Impact of COVID-19 on key-population-focused HIV programs; 2020. Available from: https://www.fhi360.org/sites/default/files/media/documents/epic-kp-strategic-considerations-covid-19.pdf.
7. World Health Organization (WHO). Coronavirus disease 2019 (COVID-19); Situation Report – 38; 2020. Available from: www.who.int/docs/default-source/coronaviruse/situation-reports/20200227-sitrep-38-covid-19.pdf?sfvrsn=9f98940c_2//.
8. World Health Organization. WHO urges countries not to let COVID-19 eclipse other health issues; 23 April 2020. Available from: https://www.afro.who.int/news/who-urges-countries-not-let-covid-19-eclipse-other-health-issues.
9. World Health Organization. Coronavirus disease 2019 (COVID-19): Situation Report – 82. Available from: https://apps.who.int/iris/bitstream/handle/10665/331780/nCoVsitrep11Apr2020-eng.pdf.
10. Alanezi F, Aljahdali A, Alyousef SM, et al. A comparative study on the strategies adopted by the United Kingdom, India, China, Italy, and Saudi Arabia to contain the spread of the COVID-19 pandemic. J Healthc Leadersh. 2020;12:117. doi:10.2147/JHL.S266491
11. Mersha A, Shibiru S, Girma M, Ayele G, Bante A, Kassa M, Abebe S, Shewangizaw M. Health professionals practice and associated factors towards precautionary measures for COVID-19 pandemic in public health facilities of Gamo zone, southern Ethiopia: a cross-sectional study. Plos one. 2021;16(3):e0248272. Available at: https://doi.org/10.1371/journal.pone.0248272//
12. Maqbool A, Khan NZ. Analyzing barriers for implementation of public health and social measures to prevent the transmission of COVID-19 disease using DEMATEL method. Diabetes Metab Syndr. 2020;14(5):887–892. doi:10.1016/j.dsx.2020.06.024
13. Tanahashi T. Health service coverage and its evaluation. Bull World Health Organ. 1978;56(2):295.
14. Tripathi R, Alqahtani SS, Albarraq AA, et al. Awareness and preparedness of COVID-19 outbreak among healthcare workers and other residents of South-West Saudi Arabia: a cross-sectional survey. Front Public Health. 2020;8:482. doi:10.3389/fpubh.2020.00482
15. World Health Organization. Considerations for implementing and adjusting public health and social measures in the context of COVID-19; 2020. Available from: https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance//.
16. Centers for Disease control for prevention and control (CDC). Information for Clinicians on Investigational Therapeutics for Patients with COVID-19, 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html//.
17. Adhikari SP, Meng S, Wu Y-J, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):29. doi:10.1186/s40249-020-00646-x
18. Wei Q, Ren Z. Disinfection measures for pneumonia foci infected by novel coronavirus in 2019. Chin J Disinfect. 2020;37:59–62.
19. World Health Organization (WHO). Coronavirus disease 2019 (COVID-19) situation Report –72; April 1, 2020.
20. World Health Organisation. Advice on the use of masks in the community, during home care and in health care settings in the context of the novel coronavirus 2019-nCoV outbreak (Interim guidance); 2020. Available from: WHO/nCov/IPC_Masks/2020.
21. National Health Commission of People’s Republic of China. Guidelines for public protection against novel coronavirus infection; 2020. Available from: http://www.nhc.gov.cn/jkj/s7915/202001/bc661e49b5bc487dba182f5c49ac445b.shtml.
22. Prem K, Liu Y, Russell TW, et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 2020;5(5):e261–e270. doi:10.1016/S2468-2667(20)30073-6
23. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1):72. doi:10.1186/s41182-020-00254-3
24. Zhong BL, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
25. Ebhohon E, Utilization of the modified Tanahashi model for assessing universal effective health coverage: the Nigeria bottleneck instrument and its’ implications for planning; 2018.
26. Alahdal H, Basingab F, Alotaibi R. An analytical study on the awareness, attitude and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J Infect Public Health. 2020;13(10):1446–1452. doi:10.1016/j.jiph.2020.06.015
27. Zaman W, Saqib S, Ullah F, et al. COVID −19: phylogenetic approaches may help in finding resources for natural cure. Phytother Res. 2020;34(11):2783–2785. doi:10.1002/ptr.6787
28. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1):1–11.
29. Mersha A, Shibiru S, Girma M, et al. Perceived barriers to the practice of preventive measures for COVID-19 pandemic among health professionals in public health facilities of the Gamo zone, southern Ethiopia: a phenomenological study. BMC Public Health. 2021;21(1):1–10. doi:10.1186/s12889-021-10256-3
30. Shewasinad Yehualashet S, Asefa KK, Mekonnen AG, et al. Predictors of adherence to COVID-19 prevention measure among communities in North Shoa Zone, Ethiopia based on health belief model: a cross-sectional study. PLoS One. 2021;16(1):e0246006. doi:10.1371/journal.pone.0246006
31. Coroiu A, Moran C, Campbell T, et al. Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS One. 2020;15(10):e0239795. doi:10.1371/journal.pone.0239795
32. Kabamba Nzaji M, Ngoie Mwamba G, Mbidi Miema J, et al. Predictors of non-adherence to public health instructions during the COVID-19 pandemic in the Democratic Republic of the Congo. J Multidiscip Healthc. 2020;13:1215–1221. doi:10.2147/JMDH.S274944
33. Wanzira H, Naiga S, Mulebeke R, et al. Community facilitators and barriers to a successful implementation of mass drug administration and indoor residual spraying for malaria prevention in Uganda: a qualitative study. Malar J. 2018;17(1):474. doi:10.1186/s12936-018-2624-7
34. Birihane BM, Bayih WA, Alemu AY, et al. Perceived barriers and preventive measures of COVID-19 among healthcare providers in Debretabor, North Central Ethiopia, 2020. Risk Manag Healthc Policy. 2020;13:2699. doi:10.2147/RMHP.S287772
35. World Health Organization. Disability considerations during the COVID-19 outbreak. World Health Organization; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public.
36. Howard J, Huang A, Li Z, et al. An evidence review of face masks against COVID-19. Proc Natl Acad Sci U S A. 2021;118(4):e2014564118.
37. Seale H, Dyer CEF, Abdi I, et al. Improving the impact of non-pharmaceutical interventions during COVID-19: examining the factors that influence engagement and the impact on individuals. BMC Infect Dis. 2020;20(1):1–13. doi:10.1186/s12879-020-05340-9
38. Backman C, Marck PB, Krogman N, et al. Barriers and bridges to infection prevention and control: results of a qualitative case study of a Netherlands’ surgical unit. BMJ Open. 2012;2(2):e000511. doi:10.1136/bmjopen-2011-000511
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.