Back to Journals » Clinical Interventions in Aging » Volume 14
Exercise Training Induced Changes In Nuclear Magnetic Resonance-Measured Lipid Particles In Mild Cognitively Impaired Elderly African American Volunteers: A Pilot Study
Authors Fungwe TV ![]() , Ngwa JS, Ntekim OE, Allard JS, Nadarajah S
, Ngwa JS, Ntekim OE, Allard JS, Nadarajah S ![]() , Wolday S, Ogunlana OO, Johnson SP
, Wolday S, Ogunlana OO, Johnson SP ![]() , Hughes K, Larbi D, Gillum RF, Obisesan TO
, Hughes K, Larbi D, Gillum RF, Obisesan TO ![]()
Received 5 December 2018
Accepted for publication 2 March 2019
Published 5 December 2019 Volume 2019:14 Pages 2115—2123
DOI https://doi.org/10.2147/CIA.S195878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Thomas V Fungwe,1 Julius S Ngwa,2 Oyonumo E Ntekim,1 Joanne S Allard,3 Sheeba Nadarajah,4 Saba Wolday,5 Oludolapo O Ogunlana,5 Steven P Johnson,5 Kakra Hughes,6 Daniel Larbi,5 Richard F Gillum,7 Thomas O Obisesan5
1Department of Nutritional Sciences, School of Nursing and Allied Health Sciences, Howard University, Washington, DC, USA; 2Division of Cardiology, Department of Medicine, Howard University, Washington, DC, USA; 3Division of Cardiology, Department of Physiology and Biophysics, Howard University, Washington, DC, USA; 4Division of Nursing, College of Nursing and Allied Health Sciences, Howard University, Washington, DC, USA; 5Division of Geriatrics, Department of Medicine and Clinical, Howard University Hospital, Washington, DC, USA; 6Department of Surgery, Howard University College of Medicine, Washington, DC, USA; 7Department of Internal Medicine, Howard University Hospital, Washington, DC, USA
Correspondence: Thomas O Obisesan
Division of Geriatrics, Department of Medicine and Clinical/Translational Science Program, Howard University Hospital, 2041 Georgia Ave NW, Washington, DC 20060, USA
Tel +1 202 865 3397
Fax +1 202 865 3777
Email [email protected]
Purpose: Poor cardiorespiratory fitness (CRF) is linked to cognitive deterioration, but its effects on lipid heterogeneity and functional properties in older African American (AA) subjects with mild cognitive impairment (MCI) need elucidation. This study determined whether exercise training-induced changes in blood lipid particle sizes (LPS) were associated with CRF determined by VO2Max in elderly AAs with MCI. Given the pivotal role of brain-derived neurotrophic factor (BDNF) on glucose metabolism, and therefore, “diabetic dyslipidemia”, we also determined whether changes in LPS were associated with the levels of serum BDNF.
Methods: This analysis included 17 of the 29 randomized elderly AAs with MCI who had NMR data at baseline and after a 6-month training. We used Generalized Linear Regression (GLM) models to examine cardiorespiratory fitness (VO2Max) effects on training-induced change in LPS in the stretch and aerobic groups. Additionally, we determined whether the level of BDNF influenced change in LPS.
Results: Collectively, mean VO2Max (23.81±6.17) did not differ significantly between aerobic and stretch groups (difference=3.17±3.56, P=0.495). Training-related changes in very low-density lipoprotein, chylomicrons, and total low-density lipoprotein (LDL) particle sizes correlated significantly with VO2Max, but not after adjustment for age and gender. However, increased VO2Max significantly associated with reduced total LDL particle size after similar adjustments (P = 0.046). While stretch exercise associated with increased protective large high-density lipoprotein particle size, the overall effect was not sustained following adjustments for gender and age. However, changes in serum BDNF were associated with changes in triglyceride and cholesterol transport particle sizes (P < 0.051).
Conclusion: Promotion of stretch and aerobic exercise to increase CRF in elderly AA volunteers with MCI may also promote beneficial changes in lipoprotein particle profile. Because high BDNF concentration may reduce CVD risk, training-related improvements in BDNF levels are likely advantageous. Large randomized studies are needed to confirm our observations and to further elucidate the role for exercise therapy in reducing CVD risk in elderly AAs with MCI.
Keywords: lipoprotein, elderly, exercise, cardiovascular disease, Alzheimer’s disease, brain-derived neurotrophic factor, cardiovascular fitness
Introduction
Cardiovascular disease (CVD) risk is associated with elevated risk of mild cognitive impairment (MCI), with the potential of progressing to Alzheimer’s disease (AD) dementia1–3 which is 10 times that in normal populations.4 It is also increasingly recognized that systemic metabolites such as blood lipid concentration in AAs with MCI may associate more with the conversion from MCI to AD dementia than previously conceived.5,6 As shown in disorders of endogenous lipid metabolism and neurodegenerative diseases,7 individuals with subclinical CVD are at a higher risk for dementia and AD.8 Indeed, several conditions known to increase CVD risks such as high blood pressure, diabetes, and high cholesterol levels are also associated with increased risk of cognitive deterioration, neurodegeneration, and Alzheimer’s disease.9,10 However, it is unknown whether higher rates of cognitive loss among elderly AAs are related to the relatively high burden of CVD.
Growing evidence suggests that chronic renal failure (CRF) can influence serum BDNF known to promote decreased CVD risk and mortality, but this relationship needs more nuanced understanding, particularly in AA with MCI. In fact, Mendelian randomization suggests a causal protective role of BDNF in the pathogenesis of CVD.11 However, possible interactions among exercise, serum BDNF, and cardiovascular disease risk have not been examined in AAs who suffer significantly higher rates of CVD and cognitive loss. Notably, regular physical exercise may increase BDNF level and reduce CVD risks by increasing brain perfusion and oxygen flow to the brain, with simultaneous reductions in blood lipids12 and increased BDNF levels.13 Though older AAs suffer higher rates of CVD and concomitant memory loss, it not known if exercise can promote improvements in the heterogenous Nuclear Magnetic Resonance Spectroscopy (NMR)-measured lipids in older AA MCI subjects.
To inform the effects of physical activity on lipids and lipoprotein metabolism on CVD, we evaluated blood lipids using NMR-measured lipoprotein (NMR-lipid) subclass analysis in AAs with MCI. In this pilot study, training-induced change in lipid particles was examined in elderly AAs with MCI following 6-month of aerobic or stretch exercise program. Also, we examined the relationship between change in serum BDNF and changes in lipid particle sizes as it relates to CVD risk.
Methods
The methods used for this study have been previously reported.13 Briefly, the protocol was approved by the Howard University Institutional Review Board, and informed consent was obtained from all participants prior to the sample collection and intervention. Volunteers were recruited through a newspaper advertisement, direct mailing, health fairs, and hospital clinics. Of those who completed the intervention, seventeen older AA volunteers confirmed to be MCI randomly assigned into a six-month program of either aerobic or stretch exercise had NMR data. Participants underwent 40 mins of supervised training three times/week. VO2Max was determined at baseline and repeated after subjects completed the 6-month exercise program.
Screening Phase I And II
The inclusion criteria were age >55 years, ability to perform vigorous exercise without causing harm to self, meeting study criteria for MCI, having a study partner, in general good health, willing to exercise for study duration, and being able to undergo all required assessments. Diagnosis of MCI was made using the following criteria: memory complaints, education adjusted Mini-Mental State Examination (MMSE) scores, where the Adjusted MMSE=Raw MMSE–(0.471 x [education-12]) + (0.131 x [age – 70]) with a score of 24–30 being inclusive,14 objective memory loss, ascertained by performance on education-adjusted scores on the Wechsler Memory Scale Logical Memory II, Clinical Dementia Rating Scale (CDR) of ≤0.5, modified Hachinski score <4, Geriatrics Depression Scale (GDS) <6. Monitoring was carried out for probable dementia according to National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and Related Disorders Association criteria, medical, neurological, psychiatric assessments, and medication effects or delirium.
MMSE and logical memory scores, vital signs and anthropometric measurements were obtained, including performing a detailed general physical and neurological examination after obtaining informed consent. Fasting blood was drawn for determining plasma NMR-lipids and BDNF as previously reported.13,14 Participants were screened using prespecified inclusion/exclusion criteria, and a qualifying treadmill test to determine ability to exercise safely. The maximal treadmill exercise test used the Bruce protocol15,16 to screen to ascertain CVD safety and the threshold for inclusion. Tests were terminated when the subject could no longer continue, or CV signs or symptoms occurred. Blood pressure, heart rate, and ECG were recorded before the test, at the end of every exercise stage, and every 2 min for 6 min after discontinuing the test as reported.17 VO2Max was determined using a validated customized online system (Kb4 by Cosmed, Chicago Illinois). Prior to treadmill screening tests, all participants had brain MRI to exclude significant intracranial pathology. Before randomization, study partners and subjects maintained regular caloric intake during the study period, while on an American Heart Association Step 1 diet: (<30% of energy from fat, ~55% from carbohydrate, ~15% from protein, and cholesterol intake <300 mg/day).
Randomization, Blinding, And Baseline Testing
After randomizing volunteers into exercise intervention (n = 14) and control (n = 15) groups, baseline tests were performed. All staff, except those directly monitoring exercise training, were blinded to group assignments. The data were de-identified using assigned unique identifiers for labeling and tracking.
After dietary stabilization, randomization, and familiarization with screening treadmill tests, additional treadmill tests were performed to determine baseline VO2Max and endurance capacity, using a modified Bruce protocol. Discontinuation criteria for these tests were similar to those used for the screening tests. Twelve hours prior to drawing blood for baseline tests, participants were instructed not to eat or use alcohol, use anti-inflammatory medication, smoke or perform any exercise in 72 hrs before testing. Participants who had an infection in the week before testing were excluded from the study.
Aerobic Exercise Training And Stretch Protocol
Details of this protocol have been previously described. Both the intervention (aerobic exercise) and control (stretch exercise) groups underwent supervised exercise training three times/week lasting 6 months. Initial training sessions lasted 20 min at 50% VO2Max, as previously reported.15 During each session, training duration increased by 5 min/week until subjects completed 40 min of exercise at 50% VO2Max. Then, training intensity increased by 5% VO2Max weekly until achieving 70% VO2Max. Participants were instructed to add an unsupervised 45–60 min lower intensity walk on the weekend after the first 4–6 weeks of exercise.
Stretch activity consisted of exercise positions that produced a slight pull on the muscle but not to the point of pain while maintaining stretch positions for 15–30 s. Because static but not a dynamic stretch of joints increases flexibility, joint range without motion loss have minimal impact on VO2Max.18 Each stretch was directed at often tight muscles (hamstrings, hip flexors, calves, and chest), and repeated slowly 3–5 times on each body side three days/week using different positions for about 40 mins.19
After a 6-month aerobic and stretch exercise program, all baseline tests including VO2Max, lipid particles were repeated under similar standardized conditions and processes.
BDNF And Blood Lipid Analyses
Blood lipid particle sizes were measured using NMR spectroscopy,20 a technique that simultaneously quantifies the number and sizes of very low-density lipoprotein (VLDLNMR), low-density lipoprotein (LDLNMR), and high-density lipoprotein (HDLNMR) particles, expressing each as a lipoprotein particle concentration (particles/L), or as an average particle size measured in nanometers, [lipoScience, Chicago Illinois].21 Serum BDNF levels were quantitatively determined using the human BDNF ELISA kit (Abcam, Cambridge, MA USA) as reported previously.13
Statistical Methods
We used descriptive statistics to assess patient baseline clinical and demographic characteristics associated with the exercise testing groups (aerobic vs stretch). For categorical variables, the counts (proportions) were obtained and evaluated for significant differences using chi-square and Fisher’s exact tests. To test for differences in baseline characteristics in aerobic versus stretch groups, we performed an analysis of variance (ANOVA) for continuous variables to assess significant differences in means. Wilcoxon’s rank-sum test was applied for comparisons of non-normal continuously distributed data. The association between exercise and change (baseline vs 6-month) in particle size was tested using GLM models. Potential confounders of the association between change in particle size and exercise were included in a multivariable logistic regression analysis (variables are presented as estimates, standard errors and p-values). P-values less than 0.05 were considered statistically significant and confidence intervals (CI) calculated at the 95% level. All analyses were conducted using the Statistical Analysis System software 9.3 (SAS Institute, Cary, NC).
Results
Baseline Characteristics
The baseline characteristics (Table 1) were limited to participants who completed the study and had data for VO2Max. Overall, the sample mean age was 71 ± 6.90 years, 70.59% women and BMI of 29.11±4.47. However, the stretch group had significantly higher BMI than the aerobic group (31.64±4.36 vs 27.34±3.46; p = 0.051) at baseline. Whereas, mean years of education (16.18 ± 3.59) did not differ significantly between the two groups, the stretch group performed significantly better than the exercise group on the adjusted MMSE (mean = 27.02±2.41 vs 24.47±1.62; p = 0.040) at baseline. Although the stretch group also performed slightly better than the aerobic group on the test of endurance at baseline (mean relative VO2Max 25.39±2.72 vs 22.78±9.15; p = 0.495), the differences were not significant.
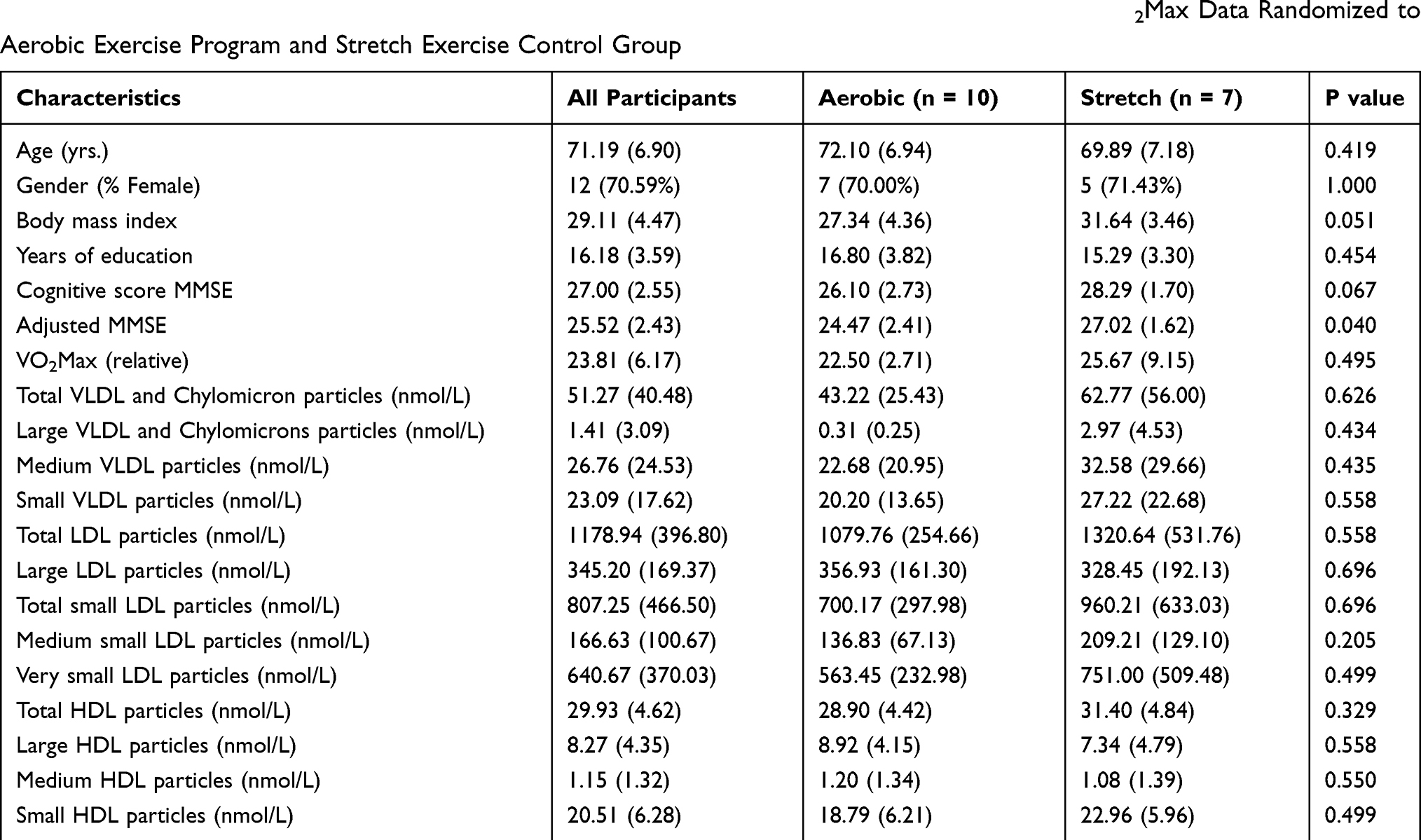 |
Table 1 Baseline Characteristics of Study Participants by Exercise Group. Participants With Baseline VO2Max Data Randomized to Aerobic Exercise Program and Stretch Exercise Control Group |
Training-Related Change In BDNF And Lipid Particle Size
Table 2 represents the correlations between change in BDNF and change in lipid particle size for all study participants. Total VLDL and Chylomicron (triglyceride carrying lipoproteins) particle sizes were significantly reduced in both aerobic and stretch groups. Both correlated with change in VO2Max (p < 0.007), but not with change in BDNF (p < 0.0127), compared to change in large VLDL and chylomicron particles (p < 0.456; P > 0.109). Exercise training-related change in VO2Max was associated with a significant reduction in the levels of medium size VLDL (p = 0.050) and small VLDL particle sizes (p=0.023), suggesting that increased VO2Max resulted in decreased production of VLDL particles. Only medium VLDL particle size (Table 3) correlated with BDNF (p < 0.038). Among the different HDL particles, change in small HDL particles correlated with change in VO2Max (p > 0.014), but not with change in BDNF (p > 0.0896).
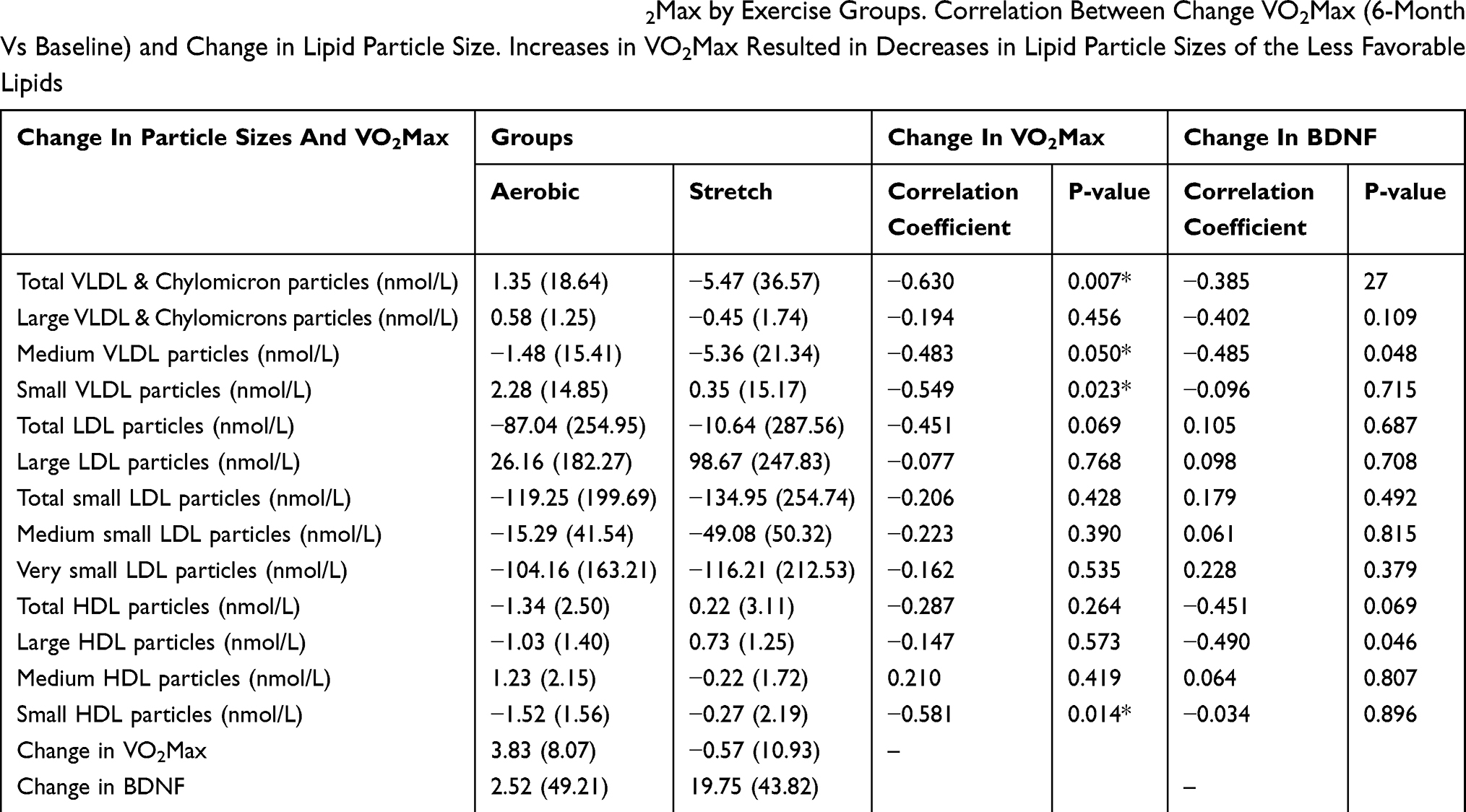 |
Table 2 Mean Change in Lipoprotein Particle Sizes and VO2Max by Exercise Groups. Correlation Between Change VO2Max (6-Month Vs Baseline) and Change in Lipid Particle Size. Increases in VO2Max Resulted in Decreases in Lipid Particle Sizes of the Less Favorable Lipids |
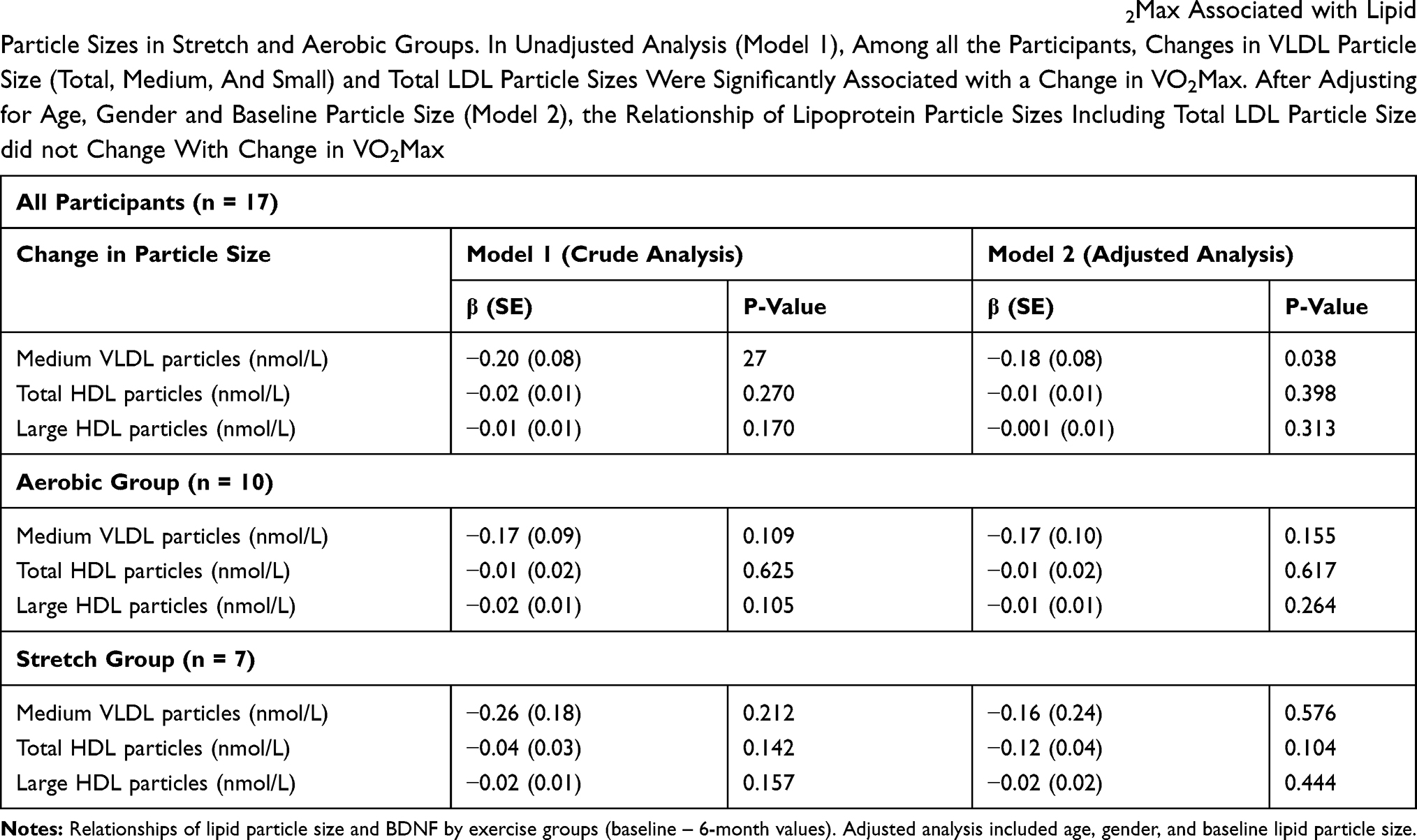 |
Table 3 Linear Regression Coefficients and Standard Errors for the Relationship Between Change in VO2Max Associated with Lipid Particle Sizes in Stretch and Aerobic Groups. In Unadjusted Analysis (Model 1), Among all the Participants, Changes in VLDL Particle Size (Total, Medium, And Small) and Total LDL Particle Sizes Were Significantly Associated with a Change in VO2Max. After Adjusting for Age, Gender and Baseline Particle Size (Model 2), the Relationship of Lipoprotein Particle Sizes Including Total LDL Particle Size did not Change With Change in VO2Max |
These results indicate a moderate negative correlation between the change in small HDL particle size and change in VO2Max (r = −0.581, p = 0.014), suggesting that training-related increases in VO2Max may significantly affect small and less favorable HDL particle size.
Effect Of Stretch And Aerobic Exercise On The Association Of Change In Lipid Particle Size With Change In VO2Max
The association between change in lipid particle sizes with a change in VO2Max in the stretch or aerobic exercise intervention is summarized in Table 4. Unadjusted small VLDL, medium VLDL, and total VLDL and Chylomicron particle sizes were significantly associated with change in VO2Max (β = −1.89 SE = 0.56, p = 0.004; −0.2 SE = 0.43, p = 0.048; −0.96 SE = 0.32, p = 0.009; respectively). However, only small VLDL particle sizes remained significant (p = 0.051) after adjustment. Similarly, unadjusted change in total LDL particle sizes was significantly associated with a change in VO2Max (p = 0.037) but not after adjustment (p = 0.082). Unadjusted analysis of the entire sample showed that change in total LDL particle size was significantly associated with a change in VO2Max (β = −14.36, SE = 6.29, p = 0.037). Following adjustments for age and gender, the relationship between change in small VLDL, medium VLDL and total VLDL and Chylomicron and total LDL particle size did not correlate with change in VO2Max.
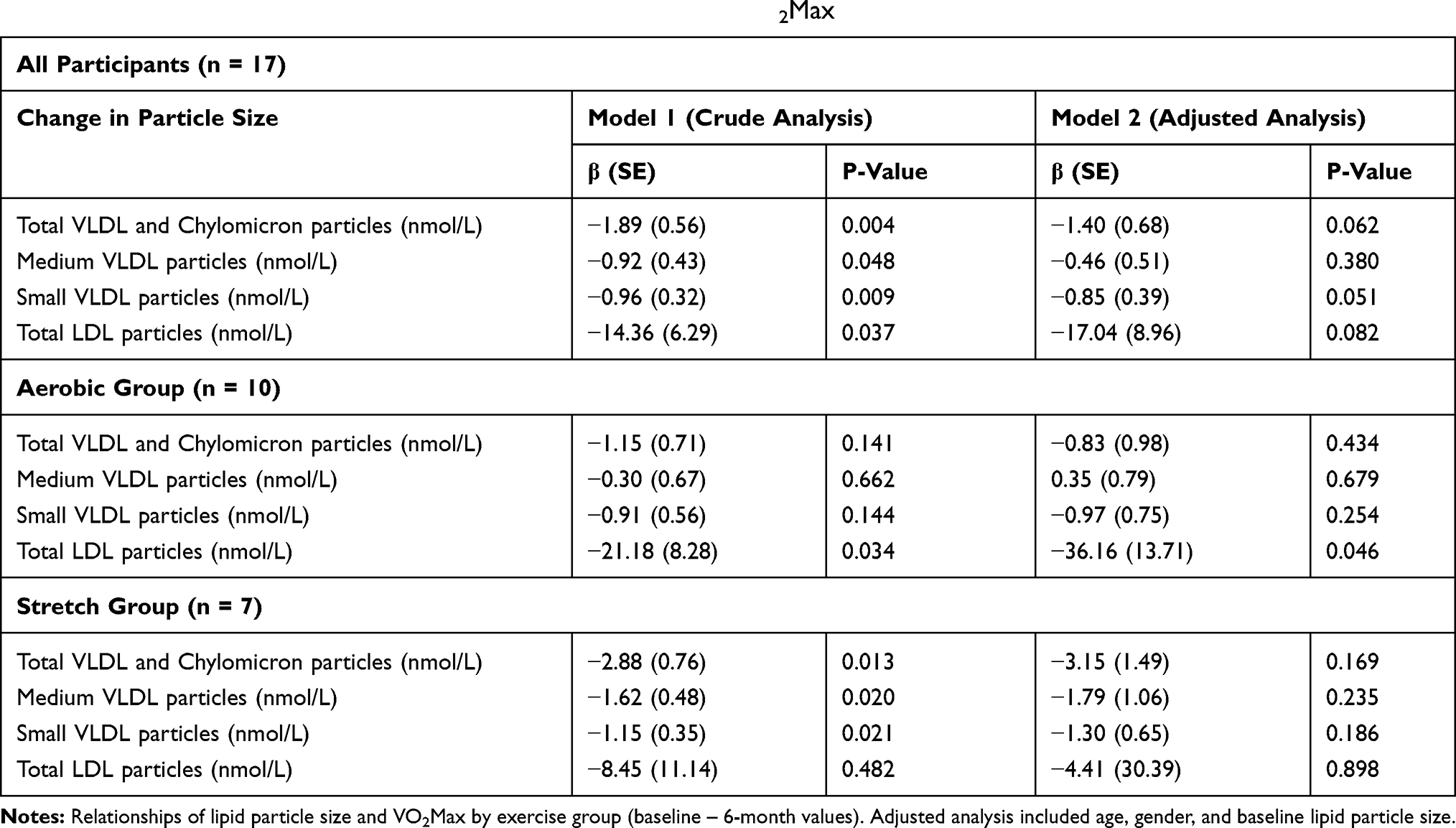 |
Table 4 Training-Related Changes in Particle Size with Changes in VO2Max |
No significant change in total LDL particle size was noted in the stretch group, pre (P = 0.482) and with adjustment for age and gender (p = 0.898). However, the relationship between change in small VLDL particle size with change in VO2Max (p = 0.051) remained significant. Also, change in total LDL particle sizes were significantly associated with a change in VO2Max after discounting the effects of age, gender and baseline particle size (β = −36.16, SE = 13.71, p = 0.046) in the aerobic group. Conversely, total VLDL & Chylomicron, medium VLDL and small VLDL particle sizes were negatively associated with change in VO2Max (VLDL & Chylomicron: p = 0.013; medium VLDL: p = 0.020; p = 0.021) but became nonsignificant after adjusting for age and gender.
The effect of aerobic and stretch exercise on plasma lipid particle size is summarized in Figure 1. Whereas aerobic exercise did not change plasma high-density lipoprotein cholesterol (HDL-C) or motivated a significant decrease in plasma triglyceride, stretch exercise tended to increase HDL-C concentration but showed no effect of triglyceride. Conversely, low-density lipoprotein cholesterol (LDL-C) tended to decrease with aerobic exercise but did not change with stretch exercise, and total cholesterol concentration remains unchanged in both exercise groups.
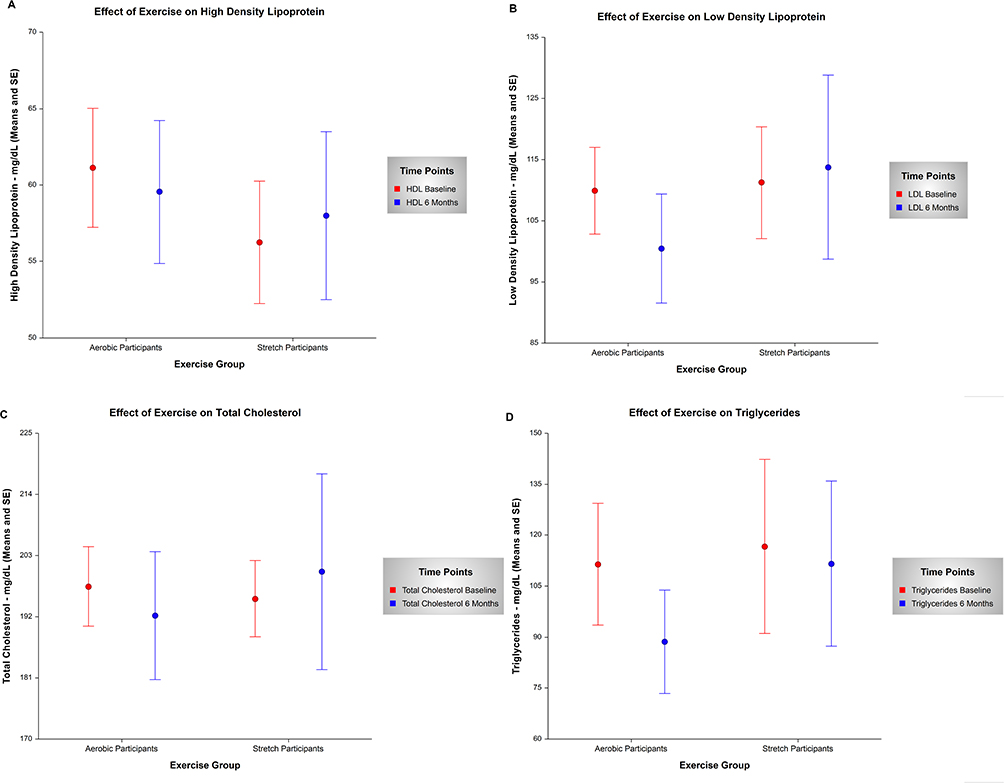 |
Figure 1 Error-bar charts showing the mean estimates and standard errors for HDL concentration (A), LDL concentration (B), total cholesterol (C), and triglycerides (D) by aerobic and stretch groups. Notes: Exercise training-related effects on blood lipid concentration: HDL concentration (A), LDL - C (B), total cholesterol (C), and Triglycerides (D). |
Discussion
This pilot study examined the effects of a 6-month exercise aerobic and stretch exercise program on training-induced changes in blood lipid concentration, particle sizes, and BDNF, in mild-cognitively impaired elderly AA MCI Volunteers. Because NMR-lipids are heterogeneous with respect to particle diameter and size, and therefore, functional property; they better reflect associated CVD risk and potentially lipid-related cognitive risk.21 Although prospective studies have reported an increase in total HDL cholesterol concentration with regular physical exercise training,22,23 low concentrations of HDL are associated with higher serum TG concentrations and an increased number of the small dense LDL particles as observed in the present study. This relationship referred to as the lipid triad or atherogenic dyslipidemia usually appears in persons with typical characteristics such as obesity and elevated BMI(Table 1). It is also known that small HDL and small dense LDL particles tend to correlate with the concentration of VLDL,23 and because VLDL particles are the substrate for HDL, lower levels due to fasting or postprandial VLDL production may contribute to decreases in small HDL particles.24 Aerobic excise, therefore, not only reduced the small HDL particles but also resulted in the reduction of total LDL particle size with increase VO2Max or cardiorespiratory fitness.
Evidence suggests that serum brain-derived neurotrophic factor (serum BDNF) can be influenced by corticotropin-releasing factor (CRF),25 although this relationship is far from clear. In this study, we also examined the association between serum BDNF and lipid particle sizes, as cardiovascular disease risk factors. The results showed a reverse association between serum BDNF and the triacylglycerol carrying lipoproteins, suggesting that increased cardiorespiratory fitness may reduce the risk for CVD. Also, exercise (aerobic or stretch) induced a negative correlation between the change in small HDL particle size and change in VO2Max. This observation agrees with our conclusion that increases in VO2Max resulted in significant decreases in TG carrying lipoproteins (VLDL) and may explain the observed decreases in the level of small less favorable HDL particle size.
Through a pilot study, the strengths of this study were 2-fold. The study population consists of mostly elderly AA MCI subjects on whom there is a paucity of data. In addition, the study employed a very rigorous, supervised, and randomized control trial of a 6-month aerobic and stretch exercise training.
Conclusion And Limitation
Results from this pilot study showed that increased VO2Max (a measure of cardiovascular fitness) positively influenced change in HDL particle sizes and decreased the level of less favorable VLDL & chylomicron (TG carrying particles) in AA subjects with MCI. Further, basal serum BDNF inversely associated with cardiorespiratory fitness and positively associated with cardiovascular disease risk factors such as reduced blood level of VLDL & chylomicron particle sizes. In a recent longitudinal study,26 serum BDNF was positively associated with a composite z-score of cardiovascular risk factors. The association appeared to be mainly driven by the association between TG, HOMA-IR and serum BDNF, and particularly for males. The current pilot study found this temporal relationship between BDNF and cardiovascular risk factors in females following exercise. The reverse association between serum BDNF and the triacylglycerol carrying lipoproteins is associated with increased cardiorespiratory fitness, increased HDL-C and reduction in the risk for cardiovascular disease. However, more research is needed to determine whether the health benefit of increased serum BDNF concentration, and reduced triglyceride and cholesterol carrying particles may be in part, associated with cardiorespiratory fitness. We speculate that the effect of exercise and BDNF may be symbiotic in that, exercise may increase BDNF levels which in turn decreases lipid particle sizes and simultaneously increased brain volume which is beneficial to cognition.
Limitations of this study include small sample size and dropout rates (~30%) which may have resulted in uneven distribution of participants within randomized groups, and perhaps, influenced our observations. It is possible that in the absence of these limitations, aerobic exercise would be more effective in reducing the CVD risks in MCI and/or CVD in this population. Nonetheless, our findings remain a significant contribution to the literature, given that, we are first to preliminarily conduct the most rigorous, supervised and randomized exercise training in older AA MCI subjects. Future studies in the population must address alternative means to bolster enrollment and reduce the dropout rate.
Highlights
- Stretch and aerobic exercises are equally beneficial in changing the lipid profile of elderly subjects with MCI
- Increase in VO2 Max significantly decreases total VLDL and chylomicron particle sizes
- Exercise decreases TG/HDL ratio in elderly subjects with MCI
- One of the few unique studies using minority, elderly participants with MCI
- ClinicalTrials.gov Identifier: NCT01021644; Registered: November 25, 2009
Abbreviations
BMI, body mass index; NMR, nuclear magnetic resonance; VLDL, very low-density lipoprotein; VLDL-P, VLDL particles; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides; VO2Max, maximal oxygen uptake; CVD, cardiovascular disease; MCI, mild cognitive impairment; AD, Alzheimer’s disease; ANOVA, analysis of variance; MMSE, mini-mental state examination; CDR, clinical dementia rating scale; GDS, geriatrics depression scale; BMP, basic metabolic panel; RPR, rapid plasma reagin.
Ethics Approval And Consent To Participate
This study was performed following approval by the Ethics Committee of the Howard University IRB under protocol # IRB-07-MED-41A and was conducted in accordance with the Declaration of Helsinki. All participants signed a consent form.
Availability Of Data And Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Acknowledgment
We thank all our colleagues working at the Division of Geriatrics, Department of Medicine and Clinical/Translational Science Program, Howard University Hospital.
Author Contributions
Participated in research design: JSA, OEN, SJ, SW, OOO, RG, and TOO. Conducted research: TVF, JSN, DL, KH and TOO. Performed data analysis: JSN, TVF, and TOO. Wrote or contributed to the writing of the manuscript: TVF, OEN, JSN, SN, JSA, KH, DL, RG, and TOO. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crouse SF, O’Brien BC, Rohack JJ, et al. Changes in serum lipids and apolipoproteins after exercise in men with high cholesterol: influence of intensity. J Appl Physiol. 1995;79(1):279–286. doi:10.1152/jappl.1995.79.1.279
2. Grandjean PW, Crouse SF, Rohack JJ. Influence of cholesterol status on blood lipid and lipoprotein enzyme responses to aerobic exercise. J Appl Physiol. 2000;89(2):472–480. doi:10.1152/jappl.2000.89.2.472
3. Ferguson MA, Alderson NL, Trost SG, Essig DA, Burke JR, Durstine JL. Effects of four different single exercise sessions on lipids, lipoproteins, and lipoprotein lipase. J Appl Physiol. 1998;85(3):1169–1174. doi:10.1152/jappl.1998.85.3.1169
4. Deschaintre Y, Richard F, Leys D, Pasquier F. Treatment of vascular risk factors is associated with slower decline in Alzheimer disease. Neurology. 2009;73(9):674–680. doi:10.1212/WNL.0b013e3181b59bf3
5. Shobab LA, Hsiung G-YR, Feldman HH. Cholesterol in Alzheimer’s disease. Lancet Neurol. 2005;4(12):841–852. doi:10.1016/S1474-4422(05)70248-9
6. Kivipelto M, Solomon A. Cholesterol as a risk factor for Alzheimer’s disease–epidemiological evidence. Acta Neurol Scand. 2006;114:50–57. doi:10.1111/ane.2006.114.issue-s185
7. Cromwell WC, Otvos JD. Low-density lipoprotein particle number and risk for cardiovascular disease. Curr Atheroscler Rep. 2004;6(5):381–387.
8. Stampfer M. Cardiovascular disease and Alzheimer’s disease: common links. J Intern Med. 2006;260(3):211–223. doi:10.1111/j.1365-2796.2006.01687.x
9. van Oijen M, Jan de Jong F, Witteman JC, Hofman A, Koudstaal PJ, Breteler MM. Atherosclerosis and risk for dementia. Ann Neurol. 2007;61(5):403–410. doi:10.1002/ana.21073
10. Dolan H, Crain B, Troncoso J, Resnick SM, Zonderman AB, Obrien RJ. Atherosclerosis, dementia, and Alzheimer disease in the Baltimore longitudinal study of aging cohort. Ann Neurol. 2010;68(2):231–240. doi:10.1002/ana.22055
11. Kaess BM, Preis SR, Lieb W, et al. Circulating brain‐derived neurotrophic factor concentrations and the risk of cardiovascular disease in the community. J Am Heart Assoc. 2015;4(3):e001544. doi:10.1161/JAHA.114.001544
12. Buchman A, Boyle P, Yu L, Shah R, Wilson R, Bennett D. Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology. 2012;78(17):1323–1329. doi:10.1212/WNL.0b013e3182535d35
13. Allard JS, Ntekim O, Johnson SP, et al. APOEε4 impacts up-regulation of brain-derived neurotrophic factor after a six-month stretch and aerobic exercise intervention in mild cognitively impaired elderly African Americans: a pilot study. Exp Gerontol. 2017;87:129–136. doi:10.1016/j.exger.2016.11.001
14. Mungas D, Marshall SC, Weldon M, Haan M, Reed BR. Age and education correction of mini-mental state examination for English and Spanish-speaking elderly. Neurology. 1996;46(3):700–706. doi:10.1212/wnl.46.3.700
15. Iyalomhe O, Chen Y, Allard J, et al. A standardized randomized 6-month aerobic exercise-training down-regulated pro-inflammatory genes, but up-regulated anti-inflammatory, neuron survival and axon growth-related genes. Exp Gerontol. 2015;69:159–169. doi:10.1016/j.exger.2015.05.005
16. Bruce RA, Hornsten TR. Exercise stress testing in evaluation of patients with ischemic heart disease. Prog Cardiovasc Dis. 1969;11(5):371–390. doi:10.1016/0033-0620(69)90027-9
17. Medicine A. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc. 1998;30:975–991. doi:10.1097/00005768-199806000-00032
18. Medicine A. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness in healthy adults. Med Sci Sports Exerc. 1990;22:265–274.
19. Cavanagh P, Evans J, Fiatarone M, Hagberg J, McAuley E, Startzell J. Exercise and physical activity for older adults. Med Sci Sports Exerc. 1998;30:1–29.
20. Jeyarajah EJ, Cromwell WC, Otvos JD. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin Lab Med. 2006;26(4):847–870. doi:10.1016/j.cll.2006.07.006
21. Arvanitakis Z, Bennett DA, Wilson RS, Barnes LL. Diabetes and cognitive systems in older black and white persons. Alzheimer Dis Assoc Disord. 2010;24(1):37. doi:10.1097/WAD.0b013e3181a6bed5
22. Dutheil F, Walther G, Chapier R, et al. Atherogenic subfractions of lipoproteins in the treatment of metabolic syndrome by physical activity and diet–the RESOLVE trial. Lipids Health Dis. 2014;13(1):112. doi:10.1186/1476-511X-13-112
23. Kodama S, Tanaka S, Saito K, et al. Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: a meta-analysis. Arch Intern Med. 2007;167(10):999–1008. doi:10.1001/archinte.167.10.999
24. Tian L, Long S, Li C, et al. High-density lipoprotein subclass and particle size in coronary heart disease patients with or without diabetes. Lipids Health Dis. 2012;11(1):54. doi:10.1186/1476-511X-11-54
25. Gotoh K, Masaki T, Chiba S, et al. Brain‐derived neurotrophic factor, corticotropin‐releasing factor, and hypothalamic neuronal histamine interact to regulate feeding behavior. J Neurochem. 2013;125(4):588–598. doi:10.1111/jnc.12213
26. Pedersen NH, Tarp J, Andersen LB, et al. The association between serum brain-derived neurotrophic factor and a cluster of cardiovascular risk factors in adolescents: the CHAMPS-study DK. PLoS One. 2017;12(10):e0186384. doi:10.1371/journal.pone.0186384
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.