Back to Journals » Clinical Ophthalmology » Volume 14
Excisional Goniotomy in Latino Patients with Open-Angle Glaucoma: Outcomes Through 24 Months
Authors Porter M, Garza A ![]() , Gallardo M
, Gallardo M ![]()
Received 16 July 2020
Accepted for publication 8 September 2020
Published 30 October 2020 Volume 2020:14 Pages 3619—3625
DOI https://doi.org/10.2147/OPTH.S271923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Matthew Porter,1,2 Arnulfo Garza,3 Mark Gallardo1
1Private Practice, El Paso Eye Surgeons, P.A., El Paso, Texas, USA; 2Texas Tech University Health Sciences Center School of Medicine-Lubbock, Lubbock, TX, USA; 3Texas Tech University Paul L. Foster School of Medicine, Lubbock, TX, USA
Correspondence: Mark Gallardo Private Practice, El Paso Eye Surgeons, P.A., 1201 N. Mesa, Ste G, El Paso, TX 79902, USA
Email [email protected]
Purpose: To characterize the efficacy of combined phacoemulsification and excisional goniotomy with the Kahook Dual Blade (KDB-phaco) in eyes of Latino adults with cataract and open-angle glaucoma (OAG).
Methods: Health records of consecutive Latino patients undergoing KDB-phaco were retrospectively reviewed. Intraocular pressure (IOP) and IOP-lowering medication use were recorded at baseline and each postoperative visit through up to 24 months. Primary outcomes were reductions in IOP and medication use from baseline; secondary outcomes were the proportions of eyes achieving IOP reductions of ≥ 20% and medication reductions ≥ 1 medication from baseline. Subgroup analysis was conducted in eyes with high and low baseline IOP.
Results: Data from 44 eyes of 32 Latino patients with OAG were analyzed. Mean IOP was 17.8 (0.7) mmHg at baseline and postoperatively ranged from 12.4 to 13.8 mmHg (p≥ 0.0003), representing mean IOP reductions of 4.2– 4.6 mmHg (19.7– 23.1%). Mean medication was 1.5 (0.2) medications per eye at baseline and postoperatively ranged from 0.2 to 1.0 (p≥ 0.0061), representing mean medication reductions of 0.7– 1.2 medications per eye (47.1– 87.2%). In the low baseline IOP group (< 18 mmHg), mean IOP was significantly reduced through Month 24 and medications through Month 12; in the high baseline IOP group (≥ 18 mmHg), IOP and medications were significantly reduced through Month 24. From Months 1– 24, IOP reductions of ≥ 20% were achieved by 48.4– 56.2% of eyes in the full cohort, by 20.0– 33.3% in the low IOP group, and by 66.7– 100% in the high IOP group; medication reductions of ≥ 1 medication were achieved by 72.0– 95.6%, 64.7– 94.2%, and 87.5– 100% of eyes, respectively.
Conclusion: Combined KDB-phaco in eyes of Latino patients with glaucoma and cataract significantly lowers IOP and the need for IOP-lowering medications for up to 24 months and should be considered for such patients who warrant IOP reduction, medication reduction, or both.
Keywords: glaucoma, intraocular pressure, excisional goniotomy, Kahook Dual Blade, Latino
Introduction
The prevalence of primary open-angle glaucoma (POAG) in Latino adults is approximately twice that of white adults in every decade of life, and its prevalence increases faster with age in Latinos than in any other ethnic group.1 Among Latinos aged 40 years or older in the Los Angeles Latino Eye Study, 4.74% were found to have POAG overall, increasing from 1.32% in those aged 40–49 years to 21.76% in those 80 years or older.2 Further, the 4-year incidence of newly-diagnosed POAG is 2.3% and of ocular hypertension (OHTN) is 3.5%.3 Glaucoma is also a leading cause of blindness in Latinos.4
Little is known regarding treatment patterns or responses to therapy in Latinos with glaucoma. Overall, Latinos with glaucoma are less likely to be treated than whites,5 and are less likely to undergo visual field or ocular imaging assessments than other ethnicities.6 The Registry in Glaucoma Outcomes Research (RiGOR) study, no ethnicity-based differences were observed in responses to medical, laser, or surgical interventions for glaucoma.7 An uncontrolled series of Latinos with glaucoma undergoing phacoemulsification, trabeculectomy, or phacotrabeculectomy demonstrated intraocular pressure (IOP) and IOP-lowering medication reductions consistent with those reported in white patients,8 while several other studies have found Latino ethnicity to be a risk factor for surgical success following trabeculectomy9,10 and tube-shunt implantation.11 Regarding minimally invasive glaucoma surgeries, a series of Latinos undergoing combined phacoemulsification and trabecular microbypass implantation manifested IOP and medication reductions consistent with those reported in studies with primarily white patient samples,12 and Latino ethnicity was a positive prognostic factor for success of trabecular ablation.13
In this paper, we report the outcomes of excisional goniotomy using the Kahook Dual Blade (KDB, New World Medical, Rancho Cucamonga, CA) combined with phacoemulsification in Latino patients with glaucoma and visually significant cataract.
Methods
This was a retrospective analysis of data drawn from the medical records of Latino patients undergoing excisional goniotomy using the Kahook Dual Blade (KDB, New World Medical, Rancho Cucamonga, CA) combined with phacoemulsification (KDB-phaco) by a single surgeon in the United States. The study protocol was reviewed and approved by the Surgical Center of El Paso Executive Committee (El Paso, TX) in February 2019 (and revised to permit longer term data collection in June 2020) and a waiver of consent was granted and all data accessed complied with relevant patient data protection and privacy regulations. Reasonable requests for data sharing submitted to the authors will be considered.
Data from the medical records of consecutive adult self-identified Latino subjects with open-angle glaucoma and visually significant cataract undergoing elective KDB-phaco between 9 June 2016 and 8 May 2019 were included. Subjects were included with all stages of glaucoma severity, on any number of topical IOP-lowering medications (including none), and irrespective of any prior laser or incisional glaucoma procedures.
The KDB-phaco procedure has been described in detail.14–25 Phacoemulsification and intraocular lens implantation were performed in standard fashion. The KDB was then introduced into the anterior chamber through the phacoemulsification incision and advanced to the nasal angle. Its tip was used to pierce the trabecular meshwork, and advanced to position the instrument’s heel against the anterior (outer) wall of Schlemm canal and the ramp and blades approximating the posterior (inner) wall. The instrument was then advanced along the canal to excise a strip of TM extended through 3–4 clock hours, which was removed using forceps. Standard antimicrobial and anti-inflammatory therapy were prescribed for postoperative use.
In addition to demographic and baseline glaucoma characteristics, data extracted from the records included best-corrected visual acuity (BCVA), IOP, and the number of IOP-lowering medications at every postoperative visit. Intraoperative and postoperative adverse events were also recorded. Visual acuity was measured using the Snellen chart and converted to logMAR for analysis. Goldmann tonometry was used for IOP measurement. Medications were counted by the number of active ingredients in the formulation.
The primary outcomes of this analysis were the reductions from baseline in IOP and IOP medications at each postoperative time point (IOP beginning on postoperative Day 1 to reflect acute extremes of IOP, and medications beginning at Month 1 once variable postoperative medication use stabilized). These outcomes were assessed using two-sided paired t-tests, with the level of significance taken as p=0.05. Secondary outcomes included the proportion of eyes achieving IOP reductions of ≥20% and medication reductions ≥1 medication (the latter evaluated only in eyes on ≥1 medication at baseline) at each time point from Month 1 onward, after postoperative stabilization; these outcomes were evaluated using descriptive statistics. Subgroup analysis was undertaken in patients with high and low baseline IOP; the groups were defined by baseline IOP above or below the full cohort’s mean baseline IOP. The purpose of this analysis was to evaluate outcomes based on likely individual surgical goals, with the assumption that eyes with lower baseline IOP underwent surgery primarily to reduce the medication burden and eyes with higher baseline IOP primarily to reduce IOP. Safety analysis consisted of descriptive analysis of the nature and incidence of adverse events. Means are reported with standard errors. As no specific hypotheses were being tested, formal power/sample size analysis was not undertaken.
Results
Data from 44 eyes of 32 patients were included in this analysis. Demographic and baseline glaucoma status data are given in Table 1. All subjects were Latino, their average age was 69.8 (2.6) years, and most (65.6%) were female. Most (84.1%) had primary open-angle glaucoma, with the balance having pseudoexfoliation glaucoma. Mild, moderate, and severe cases of glaucoma were roughly equally represented, roughly one-third were using 2 or more IOP-lowering medications, and 15.9% had undergone prior laser or incisional glaucoma procedures. Mean follow-up was 19.6 (7.5) months; 72.7% of eyes (32/44) were seen at Month 24.
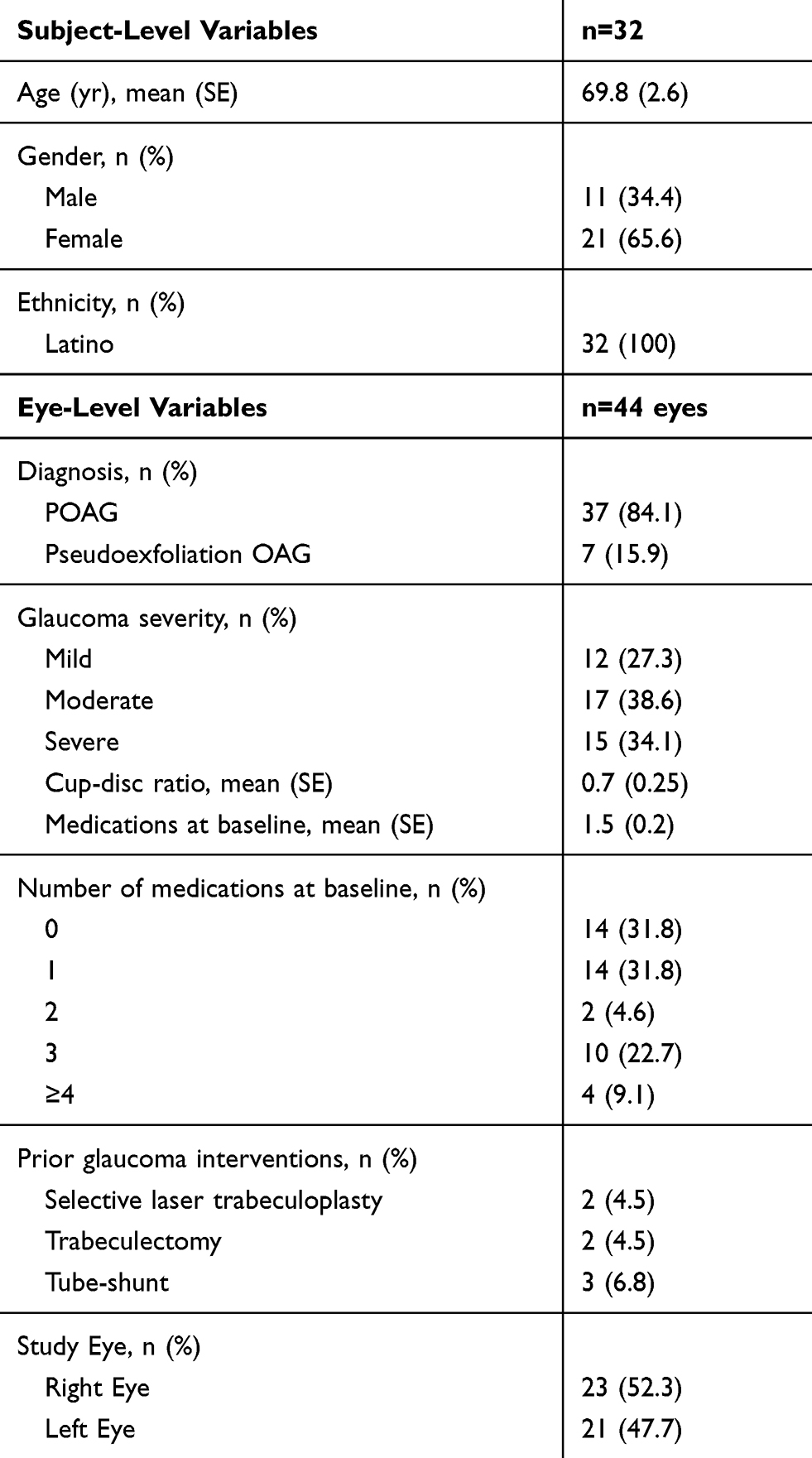 |
Table 1 Demographic and Baseline Glaucoma Status of the Study Participants |
Mean IOP for the full cohort (Table 2) was 17.8 (0.7) mmHg at baseline and from Month 1 through up to Month 24 ranged from 12.4 to 13.8 mmHg (p≥0.0003), representing mean IOP reductions of 4.2–4.6 mmHg (19.7–23.1%). In the low IOP group (baseline IOP <18 mmHg), mean IOP was reduced from 14.8 (0.4) at baseline to 12.5–14.0 mmHg from Months 1–24 (mean IOP reductions of 0.9–2.4 mmHg [4.5–15.3%]); these reductions were significant at Months 1, 3, and 24 (p≤0.03) but not at Months 6 or 12. In the high IOP group (baseline IOP ≥18 mmHg), mean IOP was reduced from 21.3 (0.9) mmHg to 11.8–14.6 mmHg at Months 1–24 (mean IOP reductions of 6.8–8.9 mmHg [28.7–42.3%]); these reductions were significant (p≤0.0023) at every time point. From Months 1–24, IOP reductions of ≥20% were achieved by 48.4–56.2% of eyes in the full cohort, by 20.0–33.3% in the low IOP group, and by 66.7–100% in the high IOP group (Table 4).
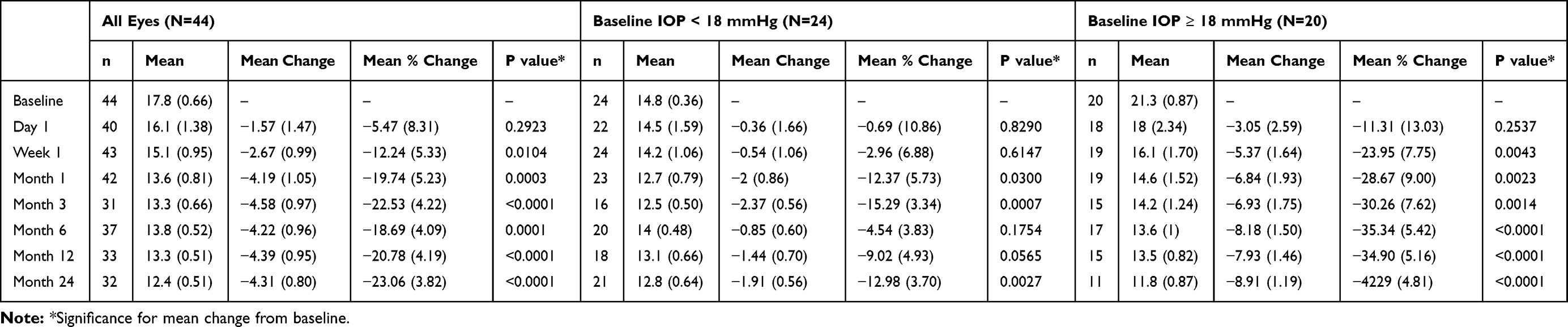 |
Table 2 Mean IOP and Changes from Baseline at Each Study Time Point |
 |
Table 3 Mean Medications and Changes from Baseline at Each Study Time Point |
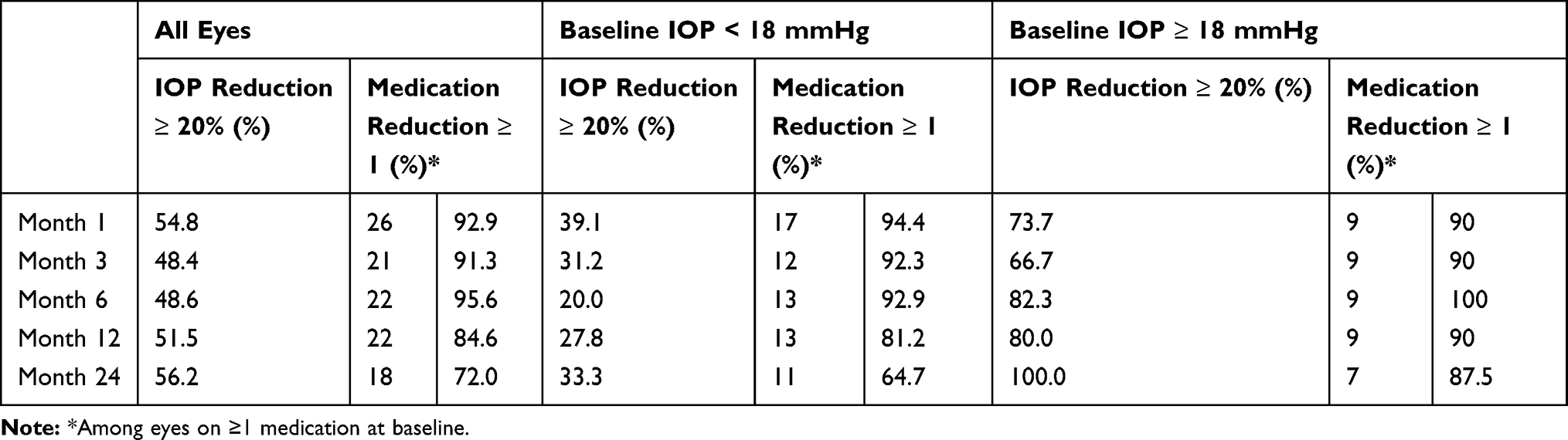 |
Table 4 Treatment Success at Each Study Time Point |
Mean medication use for the full cohort (Table 3) was 1.5 (0.2) medications per eye at baseline and from Month 1 through up to Month 24 ranged from 0.2 to 1.0 (p≥0.0061), representing mean medication reductions of 0.7–1.2 medications per eye (47.1–87.2%). In the low IOP group, mean medication use was reduced from 1.1 (0.2) at baseline to 0.2–0.8 from Months 1–24 (mean reductions of 0.4–1.0 [46.1–90.7%]); these reductions were significant (p≤0.0047) at all time points except Month 24. In the high IOP group, mean medication use was reduced from 2.0 (0.4) to 0.3–1.3 at Months 1–24 (mean reductions of 1.1–1.6 [49.4–85.9%]); these reductions were significant (p≤0.0379) at every time point. From Months 1–24, medication reductions of ≥1 medication were achieved by 72.0–95.6% of eyes in the full cohort, by 64.7–94.2% in the low IOP group, and by 87.5–100% in the high IOP group (Table 4).
Safety outcomes are given in Table 5. The most common adverse events were transient IOP elevation seen in 8 eyes (18.2%) and corneal edema in 4 eyes (9.1%), the latter of which resolved within a one month in 3 cases. The one patient with persistent corneal edema through month 24 was absent from scheduled clinical exams following his one-month postoperative visit and did not return for two years. The eye was hypotonous but associated with the self administration of four topical anti-glauocma medications. Once mediations were discontinued, his intraocular pressure rose to target levels but the coreal edema persisted. Aside from the hypotony, most of the other ocular adverse events were not directly correlated to the surgery. Rather, predisposing co-morbidities were present in these subjects, which included uncontrolled diabetes mellitus and systemic hypertension. The subject with macular edema presenting at postoperative month 1 also had proliferative diabetic retinopathy. The vein occlusion occurred at postoperative year 1 and was not a manifestation of the surgery. The single case of persistent hypotony resolved without surgical intervention. Gonioscopic evaluation of the angle did not reveal iatrogenic cleft formation in this eye.
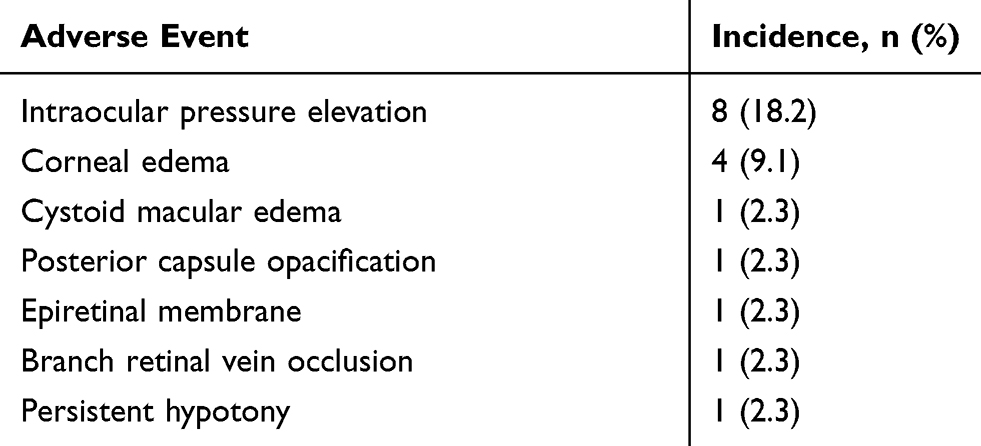 |
Table 5 Adverse Events |
Three eyes required secondary glaucoma surgery: one eye failed at Month 3 and underwent diode cyclophotocoagulation, another developed a branch retinal vein occlusion and subsequent neovascular glaucoma unrelated to the procedure between Months 12–24 requiring a Baerveldt shunt, and one eye underwent selective laser trabeculoplasty at Month 24. Mean BCVA improved from 0.69 (0.10) at baseline to 0.45 (0.13) at Month 24 (p=0.0165); 13 eyes (29.5%) had BCVA of 20/200 or worse (including 6 with BCVA of counting fingers or worse) at baseline, of which 9 had BCVA of 20/200 or worse at last follow-up.
Discussion
In this analysis of Latino patients with cataract and glaucoma undergoing combined phacoemulsification and excisional goniotomy with the KDB, clinically and statistically significant reductions in both IOP (19–23%) and the need for IOP-lowering medications (47–87%) were achieved through up to 24 months of postoperative follow-up. The procedure was safe with few adverse events, most of which were self-limited.
This study demonstrates that KDB-phaco can provide long-term reductions in both IOP and medication use across the spectrum of baseline IOP. In eyes with low baseline IOP—many of which underwent surgery primarily to reduce the medication burden—mean IOP was significantly reduced at 24 months, and medications were significantly reduced at 12 but not 24 months. This group had a very low baseline IOP (14.8 mmHg), offering a narrow therapeutic window for IOP reduction; despite this, 33.3% achieved a ≥20% IOP reduction from baseline at Month 24, accomplished with concurrent reduction of the medication burden by ≥1 medication in 64.7%. In the high baseline IOP group, both IOP and medications were significantly reduced at all time points through Month 24; 100% of these eyes achieved a ≥20% IOP reduction and 87.5% a ≥1 medication reduction by Month 24.
These outcomes in Latino patients compare favorably to outcomes of similar studies in other populations, in which combined KDB-phaco lowered IOP 12–27% and medications by 21–71% in studies of 6–12 months in duration.14–26 Of these studies, one is a randomized clinical trial comparing excisional goniotomy with the KDB to trabecular microbypass implantation (iStent, Glaukos, San Clemente, CA) in combination with phacoemulsification in which 12-month IOP reductions were 15% and 11%, respectively (p=0.2903), and medication reductions were 79% and 71%, respectively (p=0.2707).26 The safety profile characterized in the current study is also similar to that described in prior studies, with the exception of corneal edema, which occurred in 4 eyes (9.1%). Of note, 2 of these eyes had low vision (counting fingers and light perception) at baseline due both to advanced glaucoma and dense cataract requiring higher than typical ultrasound energy for extraction.
Outcomes of glaucoma surgery in Latinos—particularly in comparison to outcomes in other ethnicities—are incompletely characterized in the literature. Gallardo and Supnet reported IOP and medication outcomes 1 year following combined phacoemulsification and trabecular micro-bypass (iStent, Glaukos, San Clemente, CA) in a predominantly (76%) Latino population12 that were similar to those reported in the device’s first- and second-generation registry trials27,28 and persisted through 3 years of follow-up.29 Interestingly, Latino ethnicity was associated with lower failure rates than other ethnicities following trabecular ablation (Trabectome, Microsurgical Technology, Redmond, WA)13 but higher failure rates for trabeculectomy.30
Strengths of this study include its focus on Latino patients, a group in whom glaucoma and blindness are highly prevalent and yet little is known about the efficacy and safety of modern glaucoma therapies. Also, the duration of follow-up—up to 24 months in the majority (73%) of eyes—is beneficial in characterizing longer-term outcomes given the chronic nature of glaucoma. The retrospective nature of data collection is a limitation of the study; the risk of selection bias was mitigated by including data from all Latino subjects undergoing the procedure within the data collection window. The lack of a control group is also a limitation that precludes benchmarking these outcomes against other procedures, although the similarity of the results in this series to published results of other studies—including comparative studies16,18,20,21,25,26 supports the representative nature of these data. Also, as this was a retrospective study, there was no specific protocol for the addition or withdrawal of medications; instead, these decisions were made by the investigator on a case by case basis determined by clinical status, as reflects clinical practice.
In summary, combined KDB-phaco in eyes of Latino patients with glaucoma and cataract significantly lowers IOP and the need for IOP-lowering medications for up to 24 months. This procedure can be considered for such patients who warrant IOP reduction, medication reduction, or both.
Funding
Assistance with manuscript preparation was provided by Tony Realini, MD, MPH, with support from New World Medical.
Disclosure
Mathew Porter, MD reports data analysis and manuscript preparation by New World Medical. Mark J. Gallardo, MD reports non-financial support from New World Medical, during the conduct of the study; non-financial support from Ivantis and Sight Sciences, grants and non-financial support from Glaukos, Nova Eye, and New World Medical, outside the submitted work.
The authors report no other potential conflicts of interest for this work.
References
1. Kapetanakis VV, Chan MP, Foster PJ, Cook DG, Owen CG, Rudnicka AR. Global variations and time trends in the prevalence of primary open angle glaucoma (POAG): a systematic review and meta-analysis. Br J Ophthalmol. 2016;100(1):86–93. doi:10.1136/bjophthalmol-2015-307223
2. Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles latino eye study. Ophthalmology. 2004;111(8):1439–1448. doi:10.1016/j.ophtha.2004.01.025
3. Varma R, Wang D, Wu C, et al. Four-year incidence of open-angle glaucoma and ocular hypertension: the Los Angeles Latino Eye Study. Am J Ophthalmol. 2012;154(2):315–325 e311. doi:10.1016/j.ajo.2012.02.014
4. Rodriguez J, Sanchez R, Munoz B, et al. Causes of blindness and visual impairment in a population-based sample of U.S. Hispanics. Ophthalmology. 2002;109(4):737–743. doi:10.1016/S0161-6420(01)01008-9
5. Stein JD, Ayyagari P, Sloan FA, Lee PP. Rates of glaucoma medication utilization among persons with primary open-angle glaucoma, 1992 to 2002. Ophthalmology. 2008;115(8):1315–1319, 1319 e1311. doi:10.1016/j.ophtha.2007.12.017
6. Stein JD, Talwar N, Laverne AM, Nan B, Lichter PR. Racial disparities in the use of ancillary testing to evaluate individuals with open-angle glaucoma. Arch Ophthalmol. 2012;130(12):1579–1588. doi:10.1001/archophthalmol.2012.1325
7. Coleman AL, Lum FC, Velentgas P, Su Z, Gliklich RE, Ri GORSG. Impact of treatment strategies for open angle glaucoma on intraocular pressure: the RiGOR study. J Comp Eff Res. 2016;5(1):87–98. doi:10.2217/cer.15.58
8. Jung JL, Isida-Llerandi CG, Lazcano-Gomez G, SooHoo JR, Kahook MY. Intraocular pressure control after trabeculectomy, phacotrabeculectomy and phacoemulsification in a hispanic population. J Curr Glaucoma Pract. 2014;8(2):67–74. doi:10.5005/jp-journals-10008-1164
9. Van Buskirk EM. Five-year follow-up of the fluorouracil filtering surgery study. Am J Ophthalmol. 1996;122(5):751–752. doi:10.1016/S0002-9394(14)70507-0
10. Garris WJ, Le C, Zurakowski D, Ayyala RS. Comparison of surgical outcomes between canaloplasty and trabeculectomy with mitomycin C at 2-year follow-up: A longitudinal cohort study. Indian J Ophthalmol. 2018;66(1):66–70. doi:10.4103/ijo.IJO_543_17
11. Ou Y, Yu F, Law SK, Coleman AL, Caprioli J. Outcomes of Ahmed glaucoma valve implantation in children with primary congenital glaucoma. Arch Ophthalmol. 2009;127(11):1436–1441. doi:10.1001/archophthalmol.2009.267
12. Gallardo MJ, Supnet RA, Giamporcaro JE, Hornbeak DM. Outcomes of combined trabecular micro-bypass and phacoemulsification in a predominantly Hispanic patient population. Clin ophthalmol. 2016;10:1931–1937. doi:10.2147/OPTH.S117403
13. Okeke CO, Miller-Ellis E, Rojas M, Trabectome Study G. Trabectome success factors. Medicine. 2017;96(24):e7061. doi:10.1097/MD.0000000000007061
14. Dorairaj SK, Seibold LK, Radcliffe NM, et al. 12-month outcomes of goniotomy performed using the kahook dual blade combined with cataract surgery in eyes with medically treated glaucoma. Adv Ther. 2018;35(9):1460–1469. doi:10.1007/s12325-018-0755-4
15. Greenwood MD, Seibold LK, Radcliffe NM, et al. Goniotomy with a single-use dual blade: short-term results. J Cataract Refract Surg. 2017;43(9):1197–1201. doi:10.1016/j.jcrs.2017.06.046
16. Dorairaj SK, Kahook MY, Williamson BK, Seibold LK, ElMallah MK, Singh IP. A multicenter retrospective comparison of goniotomy versus trabecular bypass device implantation in glaucoma patients undergoing cataract extraction. Clin Ophthalmol. 2018;12:791–797. doi:10.2147/OPTH.S158403
17. Sieck EG, Epstein RS, Kennedy JB, et al. Outcomes of kahook dual blade goniotomy with and without phacoemulsification cataract extraction. Ophthalmology Glaucoma. 2018;1:75–81. doi:10.1016/j.ogla.2018.06.006
18. ElMallah MK, Seibold LK, Kahook MY, et al. 12-month retrospective comparison of kahook dual blade excisional goniotomy with istent trabecular bypass device implantation in glaucomatous eyes at the time of cataract surgery. Adv Ther. 2019;36(9):2515–2527.
19. Hirabayashi MT, King JT, Lee D, An JA. Outcome of phacoemulsification combined with excisional goniotomy using the Kahook Dual Blade in severe glaucoma patients at 6 months. Clin Ophthalmol. 2019;13:715–721. doi:10.2147/OPTH.S196105
20. Le C, Kazaryan S, Hubbell M, Zurakowski D, Ayyala RS. Surgical outcomes of phacoemulsification followed by istent implantation versus goniotomy with the kahook dual blade in patients with mild primary open-angle glaucoma with a minimum of 12-month follow-up. Journal of Glaucoma. 2019;28(5):411–414. doi:10.1097/IJG.0000000000001143
21. Hirabayashi MT, Lee D, King JT, Thomsen S, An JA. Comparison of surgical outcomes of 360 degrees circumferential trabeculotomy versus sectoral excisional goniotomy with the kahook dual blade at 6 months. Clin Ophthalmol. 2019;13:2017–2024. doi:10.2147/OPTH.S208468
22. Wakil SM, Birnbaum F, Vu DM, McBurney-Lin S, ElMallah MK, Tseng H. Efficacy and safety of kahook dual blade goniotomy: 18-month results. J Cataract Refract Surg. 2020. doi:10.1097/j.jcrs.0000000000000263
23. Barry M, Alahmadi MW, Alahmadi M, AlMuzaini A, AlMohammadi M. The safety of the kahook dual blade in the surgical treatment of glaucoma. Cureus. 2020;12(1):e6682.
24. Kornmann HL, Fellman RL, Feuer WJ, et al. Early results of goniotomy with the kahook dual blade, a novel device for the treatment of glaucoma. Clin Ophthalmol. 2019;13:2369–2376. doi:10.2147/OPTH.S224643
25. Lee D, King J, Thomsen S, Hirabayashi M, An J. Comparison of surgical outcomes between excisional goniotomy using the kahook dual blade and istent trabecular micro-bypass stent in combination with phacoemulsification. Clin Ophthalmol. 2019;13:2097–2102. doi:10.2147/OPTH.S224109
26. Falkenberry S, Singh IP, Crane CJ, et al. Excisional goniotomy vs trabecular microbypass stent implantation: A prospective randomized clinical trial in eyes with mild to moderate open-angle glaucoma. J Cataract Refract Surg. 2020;46:1165–1171. doi:10.1097/j.jcrs.0000000000000229
27. Samuelson TW, Sarkisian SR
28. Samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro JE. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118(3):459–467. doi:10.1016/j.ophtha.2010.07.007
29. Gallardo MJ, Supnet RA. Three-year outcomes of combined trabecular micro-bypass and phacoemulsification in a predominantly Hispanic population with primary open-angle glaucoma. Clin ophthalmol. 2019;13:869–879. doi:10.2147/OPTH.S189071
30. Five-year follow-up of the Fluorouracil Filtering Surgery Study. The fluorouracil filtering surgery study group. Am J Ophthalmol. 1996;121(4):349–366. doi:10.1016/S0002-9394(14)70431-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.