Back to Journals » Patient Preference and Adherence » Volume 20
Examining Sex and Age Differences in Information Needs and Patient-Provider Communication Preferences for Genetic Counseling Among US Adults
Authors Brown LA, Signorelli J, Cotter JD, Baker A
Received 8 July 2025
Accepted for publication 29 October 2025
Published 30 June 2026 Volume 2026:20 552212
DOI https://doi.org/10.2147/PPA.S552212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Emma Veale
Leigh Anna Brown,1,2 Jordan Signorelli,1 Jennifer D Cotter,1 Anna Baker1
1Department of Psychology, Clemson University, Clemson, SC, USA; 2Department of Genetics and Biochemistry, Clemson University, Clemson, SC, USA
Correspondence: Anna Baker, Clemson University, 321-C Brackett Hall, Clemson, SC, 29631, USA, Tel +1-864-656-856, Email [email protected]
Background: Healthcare communication between patient and provider is important to enhance patient experience and ensure quality of care. Demographic differences, specifically sex and age, likely influence patient-provider interactions. The current study aims to examine how sex and age influence preferences for communication behaviors exhibited by their provider.
Methods: Participants who were at least 18 years of age, U.S. residents, fluent in English, completed an online Qualtrics survey (N = 986, Mage=47). A multivariate analysis of variance was conducted in RStudio (Version 2025.05.1+513) to examine differences in informational needs and communication preferences.
Results: Females (MANOVA: F = 2.06, p < 0.001) and older adults (F = 5.83, p < 0.001) found it more important to have sufficient information and clear and open communication with the provider compared to males and emerging, younger, and middle-aged adults.
Conclusion: These findings highlight the importance of tailoring communication to socio-cultural factors including sex and age, which may enhance healthcare experiences.
Keywords: genetic counseling, health communication, health personnel, age groups, sex
Introduction
A pillar of healthcare is communication between the provider and patient. To communicate effectively, a provider must speak with language that is understandable to the specific patient, only covering relevant information, and allow for questioning or discussion to ensure the patient fully understands what is presented to them.1 Communication must be tailored to specific patient needs.2 These needs span across health literacy, cognitive understanding, as well as individual communication preferences.2–4 Health literacy encompasses reading and oral literacy (understanding printed information and conversations) as well as numeracy (basic numerical skills).3 Health literacy is also impacted by background knowledge from the patient’s culture and prior knowledge.3 Patients specifically discussing genetic information may be familiar with underlying concepts, but could have gaps in knowledge about genetic processes/implications, so a provider needs to account for these gaps to ensure patients understand what is presented to them.3
Information needs refer to the set of specific information pertaining to genetic testing. This includes the testing procedure, results, and implications that are important to a patient (eg, what is communicated). Communication preferences refer to specific behaviors that are exhibited by the provider during counseling. For example, behaviors exhibited by the provider may include the allotment of sufficient time, respectful and sensitive communication, provision of emotional support through explanation, and the allowance of questions. Rather than focusing on what is communicated (informational needs), communication preferences focus on how information is communicated.4 Optimizing both informational needs and communication preferences and reaching the patient in a way that works best for them has been found to improve patient outcomes.2
The current study examines data from a larger study that analyzed communication preferences (A Baker, Clemson University, [email protected], June 2026). Due to the knowledge gap on what patients want from their doctors specifically, this study aims to examine whether there are differences in genetic information and communication preferences between sex and age. Bronfenbrenner’s Ecological Theory emphasizes one must consider age and sex when looking at the context of situations, specifically healthcare situations.5 For example, changes in technology within the last 50 years have been rapid and younger generations communicate and receive information in vastly different ways compared to older generations. These differences may transfer to healthcare communication preferences. Understanding demographic differences in preferences allows the healthcare system to provide patient centered care, specifically in regard to differences demonstrated by age and sex.6 We predict there will be differences in preferences based on identified sex as well as age, with women rating communication preferences as more important than men and older adults preferring more information and rating communication preferences as more important compared to younger populations.
Methods
Design and Recruitment
A cross-sectional design study was used to investigate information needs and communication preferences among US adults. Participants were recruited through convenience sampling from Prolific Academic LTD, London, United Kingdom. Inclusion was restricted to those 18 years of age or older, U.S. residents, are fluent in English, and have access to the survey. Participants were over the age of 18, US residents, and fluent in English, to prevent skewed data and limit bias due to survey language comprehension issues.
Participants
Participants were recruited using Prolific between March and April of 2024. Email invitations were sent out until the target number of 1000 participants was reached. To minimize the impacts of sampling bias, the participants were balanced to comprise a distribution of age, sex and ethnicity that is reflective of the larger U.S. population, resulting in a largely representative sample. Participants were limited to persons over the age of 18 years who reside in the United States and, further, to those fluent in English to limit bias due to survey language comprehension deficits. Among the 1023 participants who were recruited for the study, 22 responses were excluded due to duplicate Prolific ID numbers, 6 returned, 6 timed out responses, 2 incomplete responses, and 1 incomplete demographic information (age). This resulted in a final sample size of 986 participants.
Measures
Modified QUOTE-geneca Scale:6 The original QUOTE-geneca scale consisted of 19 informational needs questions and 25 communication preferences and was designed for use in cancer genetic counseling applications. This study modified the original QUOTE-geneca scale to contain 10 items regarding informational needs and 13 questions regarding communication preferences. The scale was modified to be applicable to non-cancer-specific patient-provider communication of genetic information settings. Further, redundant questions were removed to reduce participant burden. The modified QUOTE-geneca scale was rated on a 4-point Likert scale by participants based on the importance of genetic counseling-related topics (informational needs) and provider behaviors (communication preferences) as “Not Important at All,” “Somewhat Unimportant,” “Somewhat Important,” or “Very Important.” This Likert scale is consistent with the original QUOTE-geneca scale.
Procedure
The purpose of the study was shared on Prolific. Participants who met the eligibility requirements and provided informed consent were eligible to complete the survey. Demographic data was obtained by using the participant’s Prolific identification to keep the participants’ anonymity and to limit participants to only one questionnaire completion. Eligible individuals completed a series of self-report measures assessing information needs and communication preferences. The data used for this study was originally collected as part of a larger study that examined socio-cognitive factors, needs, and preferences for effective communication in healthcare genetics. The larger study included 65 Likert-type and/or multiple-choice questions developed from validated scales. However, this study only focused on the modified QUOTE-geneca scale for analyses. The survey forced participants to complete every question. Participants were forced to complete every question to limit incomplete data. The Qualtrics survey took 15 minutes to complete. Upon completion, participants who passed the attention checks were compensated for their time through the Prolific platform at a rate of USD 3. This compensation amount is consistent with Prolific’s recommended rate of USD 12 per hour. No personally identifiable information was obtained through Prolific or Qualtrics, and the study was reviewed by Clemson University IRB (IRB2023-0974).
Data Processing
Data was cleaned and coded in Excel, and all statistical analyses were conducted using R (Version 4.5.2). Responses were paired with the participant’s demographic background obtained from Prolific. Participant responses were matched with demographic information obtained via Prolific. Prior to analyses, all variables were inspected for missing values, normality, and outliers. Participants were excluded if they did not complete the entire survey, failed attention checks, or had missing demographic information.
First, descriptive analyses were run to gain a full understanding of the sample characteristics and dependent variables. Age was recoded into categorical groups to facilitate group comparisons, rather than remaining as a continuous variable. Age groups were defined based on developmental and healthcare relevance: 18–25 (emerging adulthood), 36–34 (early adulthood), 35–54 (midlife), and 55+ (older adulthood).5 Third, a multivariate analysis of variance (MANOVA) was conducted to examine differences across sex (male versus female) and age groups on the modified QUOTE-GENECA scale. Pillai’s Trace was used as the test statistic due to its robustness against violations of normality. Scale items were not summed; rather, each item was analyzed independently. Each item was analyzed independently because the modified QUOTE-geneca scale measures multiple distinct concepts. Therefore, a single composite score is not applicable or reliable to examine across multiple concepts. Rather, assessing specific information needs and communication preferences at the individual scale item level is preferred. Next, individual analysis of variance tests (ANOVAs) were conducted for each item to identify specific effects. To control for Type I error across multiple comparisons, Bonferroni adjustments were applied to the significance thresholds. Finally, Tukey’s HSD analyses were run to examine which groups significantly differ while controlling for Type I error. An alpha level of.05 was used to determine statistical significance.
Results
Participants had a mean age of 47, SD = 17.6 and had about an equal identified sex—based on self-reported Prolific profile—split with 51.5% of the sample being female and 63% being White. Age ranged from 18–104 in the sample and was categorized into four groups to run analysis ranging from 18–25 (group 1; n = 133), 26–34 (group 2; n = 158), 35–54 (group 3; n = 331), and 55+ (group 4; n = 364). A full summary of sample demographics can be found in Table 1.
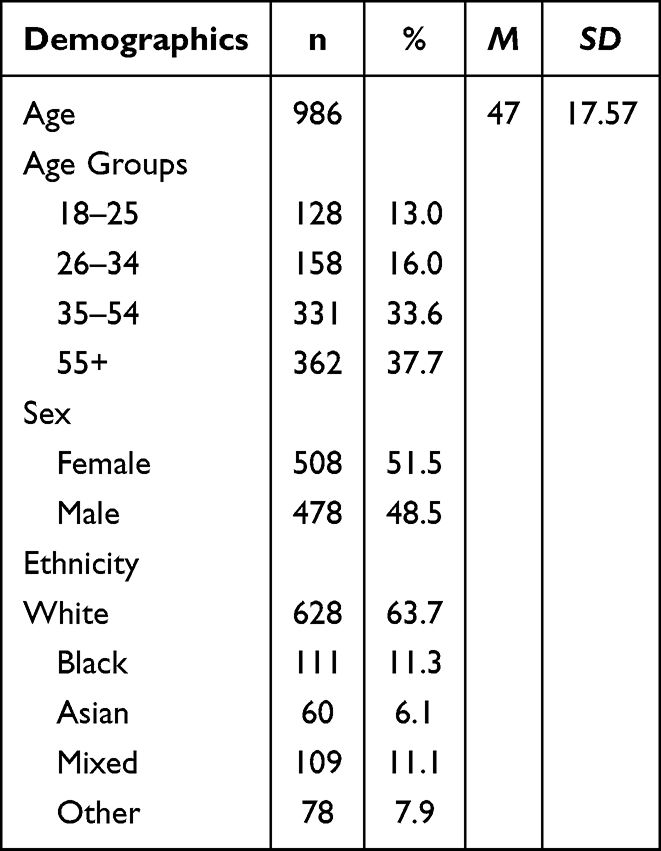 |
Table 1 Sample Demographic Summary |
Information Needs
Descriptive statistics were run on information needs items of the QUOTE-geneca scale to evaluate mean scores of the items. In general, the sample found it “Somewhat Important” or “Very Important” to receive adequate information from their provider. A full summary of information need item means can be found in Table 2.
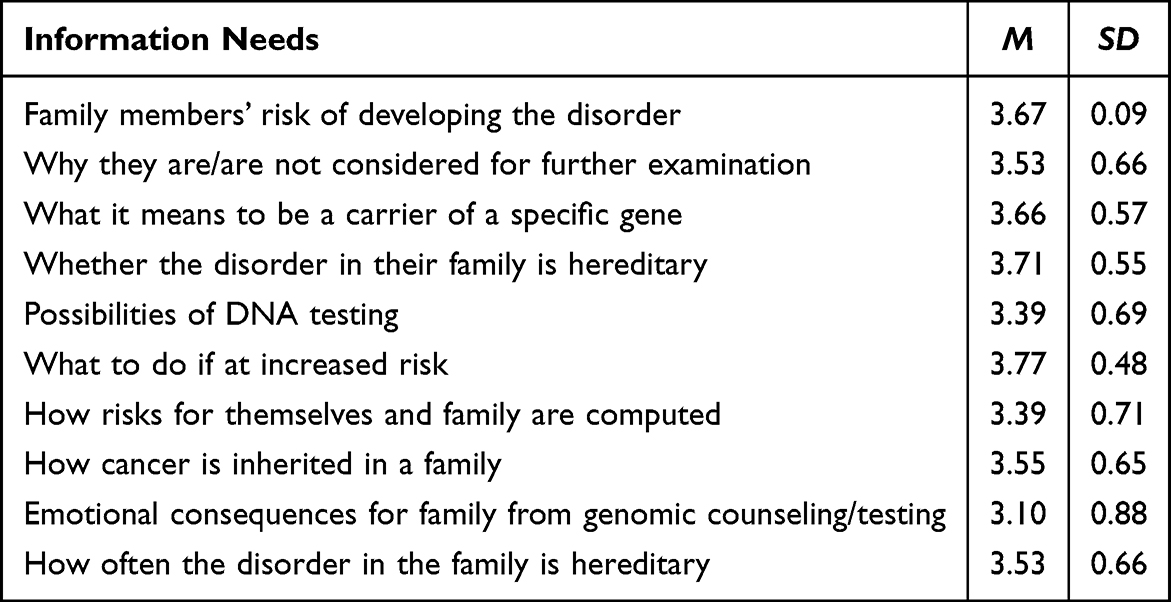 |
Table 2 Item Means and Standard Deviations for Information Needs |
Communication Preferences
Descriptive statistics were run on communication preference items of the QUOTE-geneca scale to evaluate mean scores of the items. In general, the sample found it “Very Important” to have clear and open communication with their provider. A full summary of communication preference item means can be found in Table 3.
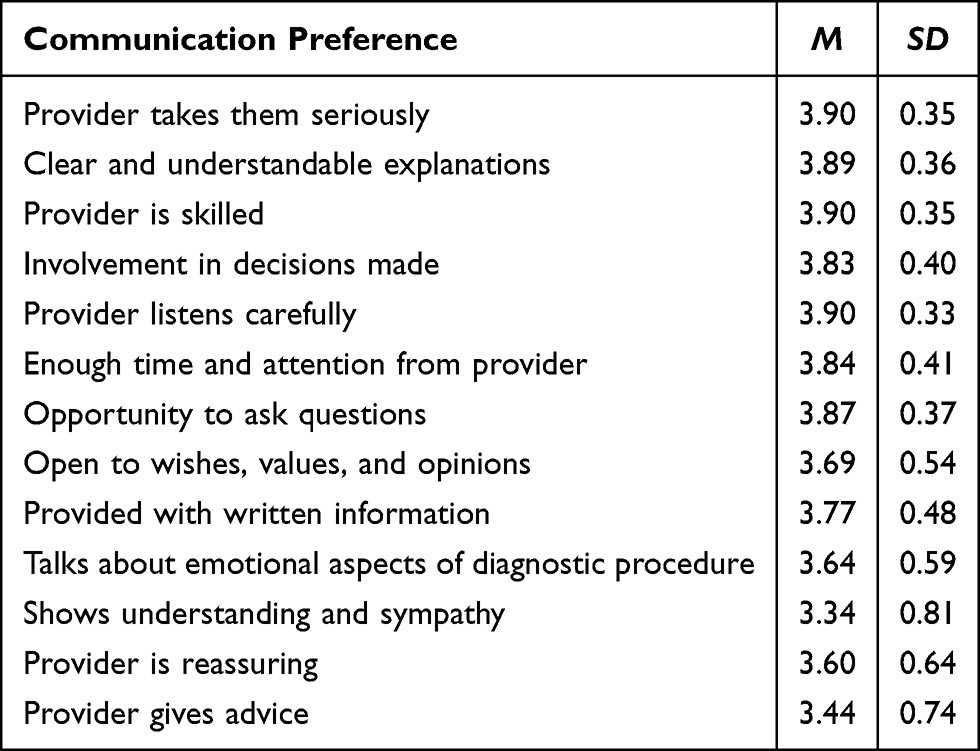 |
Table 3 Item Means and Standard Deviations for Communication Preferences |
Sex
Informational Needs
A multivariate analysis of variance was run to examine whether there were significant differences between males and females on the informational needs. Females viewed informational needs significantly more important than males on all questions including: when asked about their family members’ risk of developing the disorder (F = 6.06, p =0.01), why they are/are not considered for further examination (F = 40.92, p <0.001), what it means to be a carrier of a specific gene (F = 34.40, p <0.001), whether the disorder in their family is hereditary (F = 18.05, p <0.001), the possibilities of DNA testing (F = 31.67, p <0.001), what to do if their have an increased risk for the disorder (F = 21.26, p <0.001), how risks for themselves and their family are computed (F = 12.58, p <0.001), how cancer inherits in a family (F = 12.74, p <0.001), emotional consequences for their family as a result of genomic counseling/testing (F = 23.28, p <0.001), and how often the type of disorder occurring in their family is hereditary. (F = 10.96, p <0.001). A full summary of informational needs by sex can be found in Table 4.
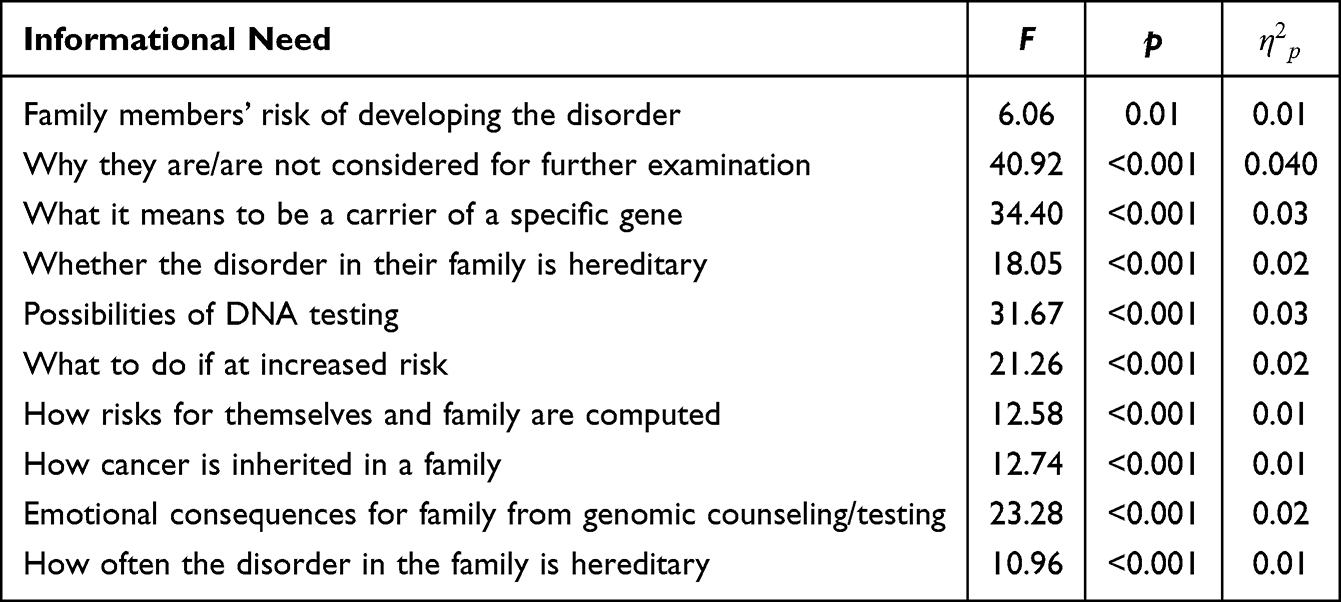 |
Table 4 Information Needs Differences by Sex |
Communication Preferences
A multivariate analysis of variance was run to examine whether there were significant differences between males and females on the communication preferences. Results revealed that females viewed communication preferences significantly more important than males when asked how important it was that their provider took them seriously (F = 26.82, p <0.001), provided clear and understandable explanations (F = 27.85, p <0.001), was skilled (F = 15.16, p <0.001), involved them in decisions that were made (F = 31.44, p <0.001), listened carefully (F = 18.41, p <0.001), gave them enough time and attention (F = 23.97, p <0.001), gave them the opportunity to ask questions (F = 29.75, p <0.001), give advice (F = 27.79, p <0.01), provided them with written information (F = 45.69, p <0.001), talked about the emotional aspects of the diagnostic procedure (F = 51.47, p <0.001), showed understanding and sympathy (F = 53.20, p <0.001), and was reassuring (F = 53.08, p <0.001). The only communication preferences that were not significantly more important to a particular sex was the importance of the provider to be open to wishes, values, and opinions (F = 2.45, p =0.10). A full summary of communication preferences by sex can be found in Table 5.
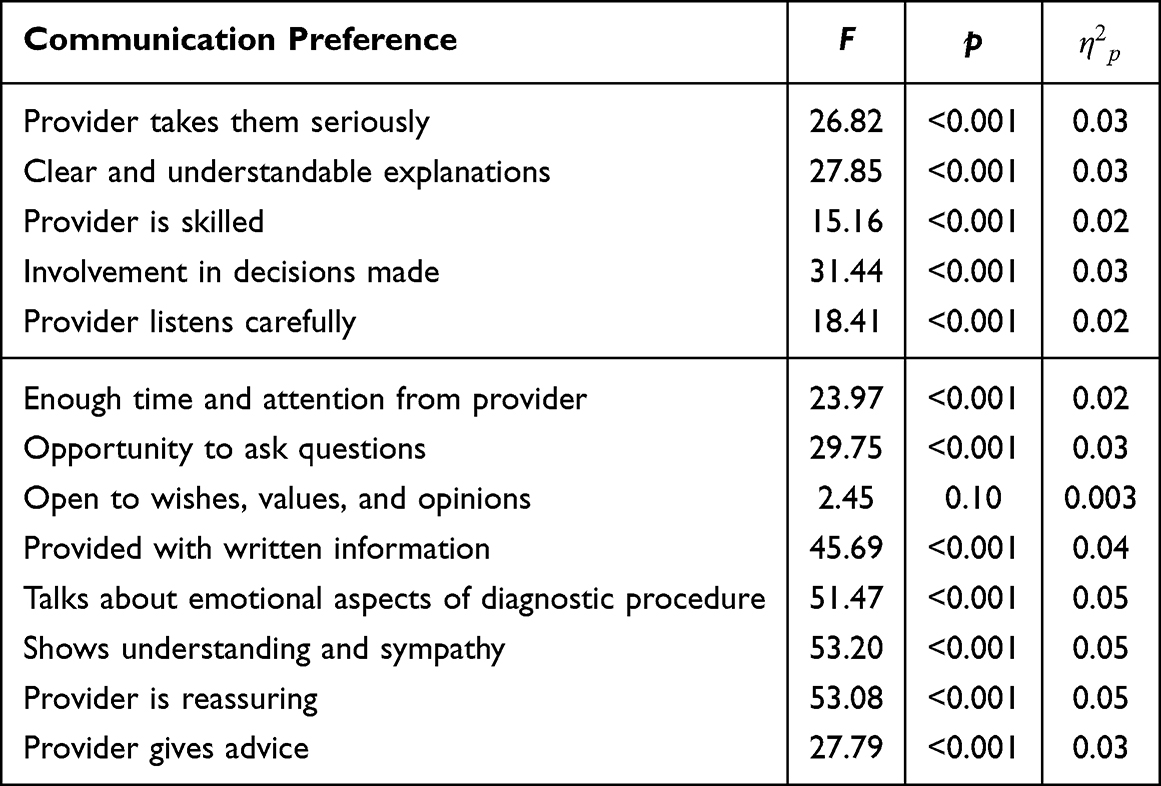 |
Table 5 Communication Preference Differences by Sex |
Age
Informational Needs
A multivariate analysis of variance was run to examine whether the importance of informational needs significantly differed by age. Results revealed that there were significant differences by age when asked how important it was to know why they are/are not considered for further examination (F = 4.33, p <0.01), what it means to be a carrier of a specific gene (F = 3.19, p <0.05), the possibilities of DNA testing (F = 10.31, p <0.001), how the risks for themselves and their family are computed (F = 12.50, p <0.001), how cancer inherits their family (F = 4.05, p <0.01), the emotional consequences of their family as a result of genomic counseling/testing (F = 9.48, p <0.001), and how often the type of disorder occurring in their family is hereditary (F = 3.51, p =0.01). Post hoc comparisons revealed that group 3 (p =0.007) and group 4 (p =0.007) had found it more important than group 1 to be considered in future examinations. Group 4 found it more important than group 3 (p =0.044) to know what it means to be a carrier of a specific gene. Group 2 (p =0.045), group 3 (p <0.001), and group 4 (p <0.001), all found it more important than group 1 to know the possibilities of DNA testing. Group 1 (p =0.039), group 2 (p <0.001) and group 3 (p <0.001) found it more important to know how the risks for themselves and their family are computed, and group 4 (p =0.012) also found it significantly more important than group 2. Group 4 (p =0.001) found it more important to know how cancer is inherited in a family than group 1. Group 4 found it more important to know the consequences for their family as the result of genetic counseling/testing than group 1 (p =0.004), group 2 (p <0.001), and group 3 (p =0.001). Lastly, group 4 found it more important than group 1 (p =0.008) to know how often the type of disorder occurring in their family is hereditary. A full summary of informational needs by age can be found in Table 6.
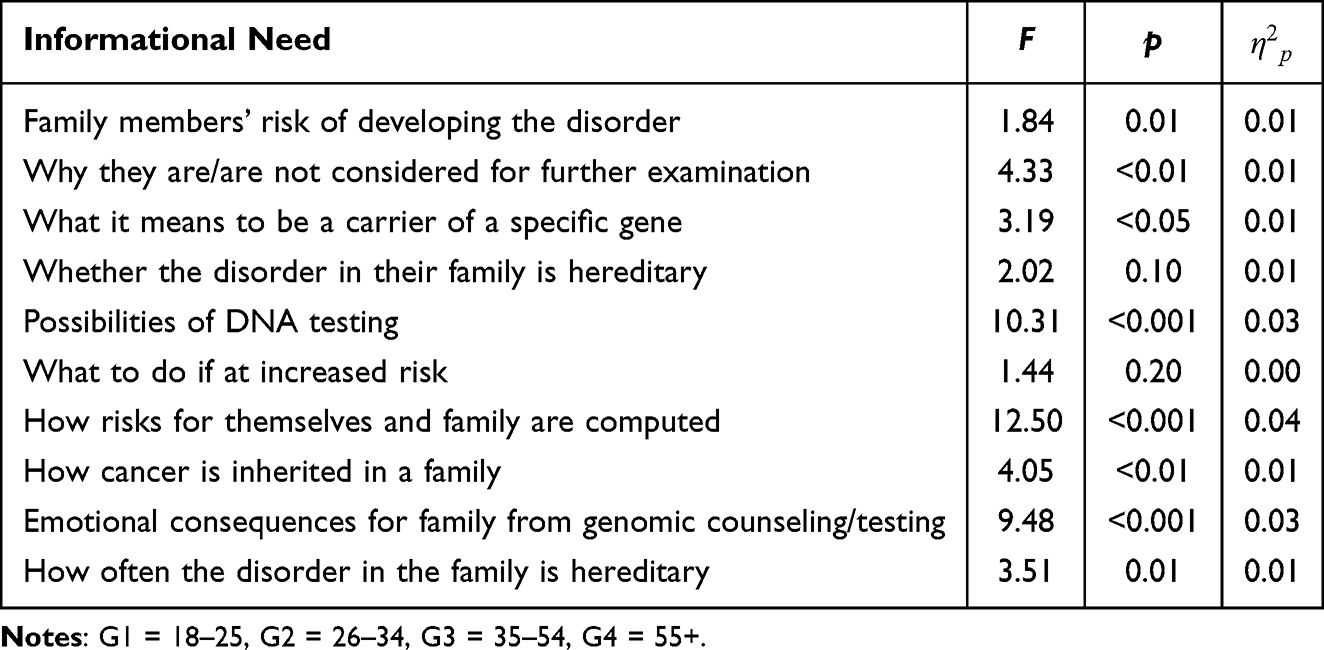 |
Table 6 Informational Need Differences by Age |
Communication Preferences
A multivariate analysis of variance was run to examine whether communication preferences significantly differed by age. Results demonstrated that there were significant differences by age when asked how important it is for their provider to involve them in decisions that are made (F = 7.09, p <0.001), listen carefully (F = 0.93, p <0.05), give them the opportunity to ask questions (F = 4.17, p <0.01), have enough time and attention from provided (F = 2.66, p <0.05) provide them with written information (F = 3.48, p <. 05), talk about the emotional aspects of the diagnostic procedure (F = 6.79, p <0.001), and show understanding and sympathy (F = 7.54, p <0.001). Post hoc comparisons revealed that group 3 (p =0.044) found it more important than group 1 to be involved in decisions that are made, and group 4 found it more important than group 1 (p <0.001) and group 2 (p =0.018). Group 4 (p =0.040) found it more important than group 1 for the provider to listen carefully. Group 3 (p =0.048) and group 4 (p =0.003) found it more important to be given the opportunity to ask questions compared to group 1. Group 4 (p =0.033) found it more important than group 2 that their provider be open to their wishes, values, and opinions. Group 4 found it more important than group 1(p =0.025), group 2 (p <0.001), and group 3 (p =0.037) to be provided with written information. Group 4 found it more important than group 2 (p <0.001) and group 3 (p =0.003) to talk about the emotional aspects of the diagnostic procedure. A full summary of communication preference differences by age can be found in Table 7.
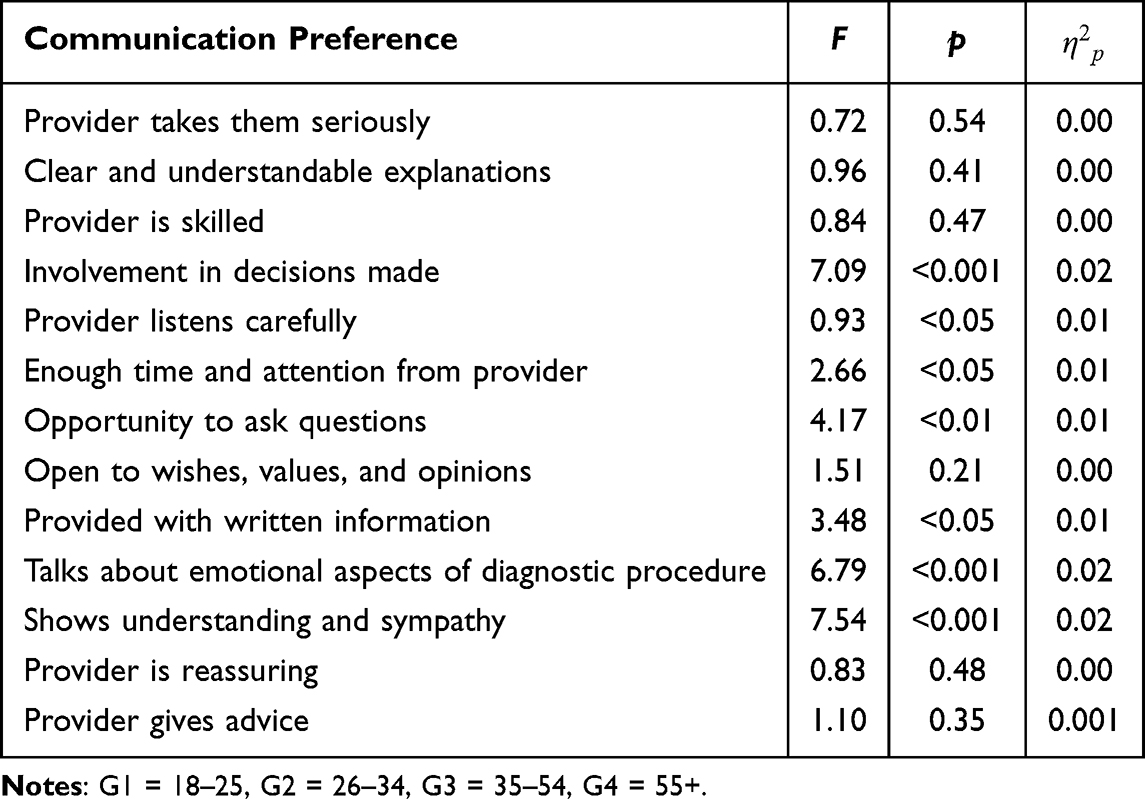 |
Table 7 Communication Preference Differences by Age |
Discussion
Our study aligns with findings that show differences in healthcare communication preferences based on demographic variables, specifically age and sex.6 Females found it more important to have more information provided to them, though males also on average found it important. This contrast in informational needs could be related to sociocultural factors along with societal norms. Females prioritize privacy and communication but historically do not get what they prioritize.7 Females also found it more important to have open and clear communication with their provider compared to males, though males still found it important. This could perhaps be due to disparities females have historically experienced in healthcare, especially around being offered treatments and being taken seriously about their pain.7,8
This study also highlights the importance of age differences in informational needs and communication preferences. When looking at age, no group found it more important than another to be given advice. All ages prioritize getting factual information in an efficient manner, not necessarily advice on how to handle results.8 Older adults found it more important to receive information from the provider. Health information may feel more salient and relevant to older adults with aging related increases in physical conditions and with the genetic result extending to their older children. Older adults also found it more important to have open and clear communication with their provider, preferably through face to face and/or written information. Ladin et al study supports these findings and found older adults preferred in-person visits with their provider for kidney disease.9
Implications
This study opens the door for future changes to be made by practitioners to better reach patients with important genetic health information. Providers should ensure that all questions are addressed by leaving adequate time to talk with patients and bring up typical questions the clinic tends to get that the patient may not have thought of in the moment. Also, physical handouts with information based on what a patient would typically ask (family implications, background information on genetics, etc.) could also be sent home. Clinic visits can be overwhelming, and patients may appreciate having the resources to go over later when they have had time to process the information or when questions may arise. Physical handouts would address our findings of older patients preferring written information and address the need to cover all patients’ questions.
Limitations and Future Directions
While this study demonstrated strengths regarding patient-provider informational needs and communication preferences, questionnaires may not have captured all informational and communication preferences of the sample. In addition, a large percentage of the sample were White, which may limit generalizability to other racial and ethnic groups. Further, convenience sampling was used, which may also limit generalizability. Finally, self-report measures were used which introduces social desirability bias. Future research should consider using a mixed-methods approach (instead of the cross sectional design) to explore if there are other information needs and communication preferences not included in the measure. Finally, future research would benefit from recruiting a more diverse sample to identify whether there are more significant information needs and communication preference differences between different racial and ethnic groups. Further, examining a wider variety of demographic variables is an area of future investigation to gain a better understanding of patient-provider information needs and communication preferences.
Conclusions
These findings support previous literature regarding effective patient-provider communication.2 Providers should provide information and communication to accommodate different needs to improve patient-centered care and shared decision-making for genomic counseling populations. When discussing genetic information, providers should pay close attention to a patient’s informational needs. Practically, this could include physical handouts for older patients or having prepared visual information. Providers could also add buffer time between patients to ensure they have ample time to address any concerns/questions specifically for female patients. Further, considering sociocultural differences within healthcare may inform providers on how to enhance the delivery of necessary genetic testing results to patients, thus enhancing their overall quality of care. Future research could include analyzing a more diverse sample as well as doing a mixed methods approach to ensure all patient’s informational needs and communication preferences are considered.
Data Sharing Statement
Data is available from the corresponding author.
Ethical Approval
Ethical approval for this study was granted by the Institutional Review Board at Clemson University.
Consent
The online survey was anonymous and no personally identifiable information was collected. Informed consent was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Clemson University.
Disclosure
No potential conflicts of interest reported by the authors.
References
1. Cotter JD, Jones K, Davis S, Baker A, Koci A, Boccuto L. Effective patient-provider communication in healthcare genetics: a concept analysis. Front Commun. 2024;9:1373505. doi:10.3389/fcomm.2024.1373505
2. Sharkiya SH. Quality communication can improve patient-centred health outcomes among older patients: a rapid review. BMC Health Serv Res. 2023;23(1):886. doi:10.1186/s12913-023-09869-8
3. Lea DH, Kaphingst KA, Bowen D, Lipkus I, Hadley DW. Communicating genetic and genomic information: health literacy and numeracy considerations. Public Health Genomics. 2011;14(4–5):279–9. doi:10.1159/000294191
4. Timmins F. Exploring the concept of ‘information need’. Int J Nurs Pract. 2006;12(6):375–381. doi:10.1111/j.1440-172X.2006.00597.x
5. Arnett JJ, Žukauskienė R, Sugimura K. The new life stage of emerging adulthood at ages 18–29 years: implications for mental health. Lancet Psychiatry. 2014;1(7):569–579. doi:10.1016/S2215-0366(14)00080-7
6. Pieterse AH, van Dulmen S, Ausems MG, Schoemaker A, Beemer FA, Bensing JM. QUOTE-geneca: development of a counselee-centered instrument to measure needs and preferences in genetic counseling for hereditary cancer. Psychooncology. 2005;14(5):361–375. doi:10.1002/pon.853
7. Moore JE, Mompe A, Moy E. Disparities by sex tracked in the 2015 National Healthcare Quality and Disparities Report: trends across national quality strategy priorities, health conditions, and access measures. Womens Health Issues. 2018;28(1):97–103. doi:10.1016/j.whi.2017.08.006
8. Kalaja R. Determinants of patient satisfaction with health care: a literature review. Eur J Nat Sci Med. 2023;6(1):43–54.
9. Ladin K, Porteny T, Perugini JM, et al. Perceptions of telehealth vs in-person visits among older adults with advanced kidney disease, care partners, and clinicians. JAMA Network Open. 2021;4(12):e2137193. doi:10.1001/jamanetworkopen.2021.37193
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.