Back to Journals » Patient Preference and Adherence » Volume 20
Evidence-Based Contraceptive Guidance for Young Women Following Induced Abortion: A Systematic Summary
Authors Tu L ![]() , Wu H, Chen S, Wu Y, Yan H, Mei B, Xiao Y
, Wu H, Chen S, Wu Y, Yan H, Mei B, Xiao Y
Received 22 January 2026
Accepted for publication 3 April 2026
Published 15 April 2026 Volume 2026:20 598266
DOI https://doi.org/10.2147/PPA.S598266
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Lewei Tu,1,2,* Huijie Wu,1,* Shuwen Chen,2,* Yiqian Wu,2 Huiqi Yan,2,* Binbin Mei,2 Ying Xiao1
1Faculty of Medicine, Macau University of Science and Technology, Macau, 999078, People’s Republic of China; 2School of Nursing, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310035, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Binbin Mei, School of Nursing, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, Email [email protected] Ying Xiao, Faculty of Medicine, Macau University of Science and Technology, Macau, 999078, People’s Republic of China, Email [email protected]
Objective: To summarize the best available evidence on post-abortion contraceptive counseling for young women (aged 15– 24 years) and provide an evidence-based basis for clinical practice.
Methods: Following the “ 6S” model, we systematically searched international and Chinese guide websites, professional association websites, and databases in both Chinese and English, from inception to June 2025. The types of literature included clinical decisions, evidence summaries, guidelines, and expert consensus. Two researchers independently performed literature screening, data extraction, and quality assessment. Guidelines were assessed by AGREE II, systematic reviews by AMSTAR 2.0, and RCTs and expert consensus by JBI critical appraisal tools. Evidence was graded using the JBI Evidence Grading System (2014) and synthesized by topic.
Results: Fifteen articles were included the following: 3 clinical decision aids, 7 guidelines, 2 expert consensus statements, 2 systematic reviews, and 1 RCT. Thirty-three pieces of evidence were summarized across seven categories: provision of contraceptive services, timing of initiation, assessment and counseling, values clarification, complications and management, follow-up, and support.
Conclusion: This summary provides contraceptive guidance for young women after induced abortion. Healthcare providers should integrate local policies and personal preferences, follow patient-centered principles, and translate this evidence into practice to increase uptake of efficient contraceptive methods and reduce unintended pregnancies among young women.
Systematic Review Registration: Fudan University Center for Evidence-Based Nursing (Registration No. ES20257666).
Keywords: post-induced abortion, young women, contraception, evidence summary
Introduction
Unintended pregnancy remains a significant concern in global public health, particularly among young women, leading to a high rate of induced abortions.1 The World Health Organization (WHO) estimates that there are about 73 million induced abortions performed worldwide each year, nearly half of which are classified as unsafe.2 A significant number of these pregnancies and abortions are among young women, including 15% of abortions among teenagers aged 15–19 years and 26% among young women aged 20−24 years.3 These young women face unique reproductive health challenges. Without appropriate intervention, these individuals face increased risks of adverse reproductive outcomes, including infection, menstrual irregularities, impaired fertility, and psychological distress such as anxiety and depression.4–6 Moreover, the social and educational disruption caused by unintended pregnancy can have lasting effects on young women’s personal development and future opportunities.7
Unintended pregnancies and induced abortions in young women are caused by various factors. Limited knowledge of sexual and reproductive health is a primary issue,8 compounded by tolerant attitudes towards premarital sex and engagement in such activities.8–10 Inconsistent or non-use of contraception further exacerbates the problem.9 Societal stigma associated with premarital sex and out-of-wedlock pregnancies also plays a significant role.11 Many young women experience unintended pregnancies due to the failure to utilize contraceptives or reliance on less effective methods.12 In China, a nationwide cross-sectional study, 2,370 adolescents who had an abortion were enrolled and 39% of all these young women experienced repeat abortion. Overall, 67.9% of the unintended pregnancy was due to no contraception used at all.13 According to reports,14 approximately 33 million young women aged 15–24 worldwide still have unmet contraceptive needs. The 2030 Agenda for Sustainable Development includes Sustainable Development Goal (SDG) Indicator 3.7.1, aiming to meet the family planning needs of women of reproductive age using modern methods.15 However, in the 2019 study, among about 300 million adolescent women aged 15–19 years worldwide, 15 million unmet need for family planning were observed.16 The adolescent contraceptive needs were only met by modern methods in 59.2%, which is lower than the worldwide level of 75.7%.16 These findings indicate the importance to provide young women with effective contraceptive methods to help them prevent unintended pregnancies and avoid unnecessary abortions.
However, recent literature has emphasized that contraceptive counseling for young women in clinical practice faces multiple challenges, including knowledge gaps among providers and youth,17 healthcare provider biases,18 youth-specific counseling needs, and structural barriers to contraceptive access.19,20 Healthcare providers’ personal values and perceptions regarding contraception significantly influence their counseling practices; for example, clinicians’ views on side effects and their impact on contraceptive continuation can shape whether certain methods are recommended or discouraged.18 Such biases may affect youth’s access to and adherence with contraceptive methods. Additionally, many clinicians lack confidence in providing comprehensive contraceptive education,21 while youth require counseling that addresses developmental and psychosocial factors—including confidentiality concerns, discussions about sexual maturation, and the specific needs of vulnerable populations.22,23 Furthermore, young people continue to face social, cultural, and systemic barriers that hinder consistent contraceptive use, necessitating targeted strategies to overcome these obstacles.19,20
In recent years, several authoritative organizations have released relevant guidelines and recommendations. For instance, UpToDate published “Contraception: Postabortion” in 2017 and updated it in 2025,24 while ACOG issued “Counseling Adolescents About Contraception”25 in the same year. In 2018, UpToDate further issued “Contraception: Overview of issues specific to adolescents”, also updated in 2025.26 In 2022, the Royal College of Obstetricians and Gynecologists (RCOG) in the UK issued a document “Best practice in post-abortion contraception”.27 In 2022, WHO also released “Abortion care Guideline”.28 In 2020, the Chinese Journal of Obstetrics and Gynecology also issued “Guidelines for Contraceptive Services in Adolescents” in China.29 Although these documents provide updated frameworks for contraceptive counseling and emphasize individualized approaches tailored to youth-specific challenges, they have several limitations: inconsistent target populations, areas, scopes, and purpose across sources, alongside uneven methodological quality. More importantly, no existing single source offers a comprehensive synthesis of evidence specifically focused on contraceptive guidance for young women (aged 15–24) following induced abortion—a population with unique reproductive health needs. Furthermore, no coherent, structured framework currently exists to facilitate the translation of existing guidelines into routine clinical practice.
To address this gap, this study aims to systematically retrieve, evaluate, and synthesize the best available evidence on contraceptive guidance for young women after induced abortion. By adhering to the evidence-summary reporting standards of the Evidence-Based Nursing Center of Fudan University, we developed a rigorous, evidence-based framework to inform clinical practice. The findings are intended to support healthcare providers in delivering individualized, patient-centered contraceptive counseling that improves method uptake, reduces repeat unintended pregnancies, and ultimately enhances the reproductive health and autonomy of young women.
Methods
This evidence summary followed the evidence summary reporting standards of the Evidence-Based Nursing of Fudan University,30 which covers six components: problem identification, literature search, literature screening, literature appraisal, evidence synthesis and grading, and formulation of practice recommendations.
Study Registration
This evidence summary was registered with the Evidence-Based Nursing Center of Fudan University (Registration No.: ES20257666).
Problem Establishment
Fudan University Center for Evidence-based Nursing proposed the PIPOST31 model to address the first step in evidence summary reporting standards: problem formulation.
The first P refers to the target population (young women aged 15–24 years who have undergone induced abortion); I refers to interventions (provision of contraceptive counseling, education, and guidance); the second P refers to professionals (healthcare providers including physicians, nurses, and contraceptive counselors); O refers to outcomes (uptake of highly effective contraceptive methods, reduction in unintended pregnancy and repeat abortion rates, improvement in contraceptive knowledge, and correct use of contraceptive methods); S refers to settings (hospitals, clinics, community health centers); and T refers to types of evidence (clinical guidelines, summary of evidence, expert consensus, systematic reviews/meta-analyses, high-quality randomized controlled trials (RCTs), quasi-experimental studies).
Evidence Retrieval
Following the “6S”25 evidence resource model, a top-down searches were conducted across databases and professional sites, including: Up To Date, BMJ Best Practice, World Health Organization (WHO), Guidelines International Network (GIN), the UK’s National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), the U.S. National Guideline Clearinghouse (NGC), Canadian Medical Association: Clinical Practice Guidelines (CMA Infobase), the U.S. Centers for Disease Control and Prevention (CDC), Registered Nurses’ Association of Ontario (RNAO), American College of Obstetricians and Gynecologists (ACOG), the UK’s Royal College of Obstetricians and Gynecologists (RCOG), the JBI Evidence Based Healthcare Center Database (JBI), Cochrane Library, PubMed, CINAHL, Embase, Web of Science, Medlive, China National Knowledge Infrastructure (CNKI), Chinese Wanfang Database, and Chinese Biomedical Literature Database (CBM). The search period covered the time from the establishment of the database to June 28, 2025. Taking Pub Med as an example, the retrieval strategy is illustrated in Figure 1.
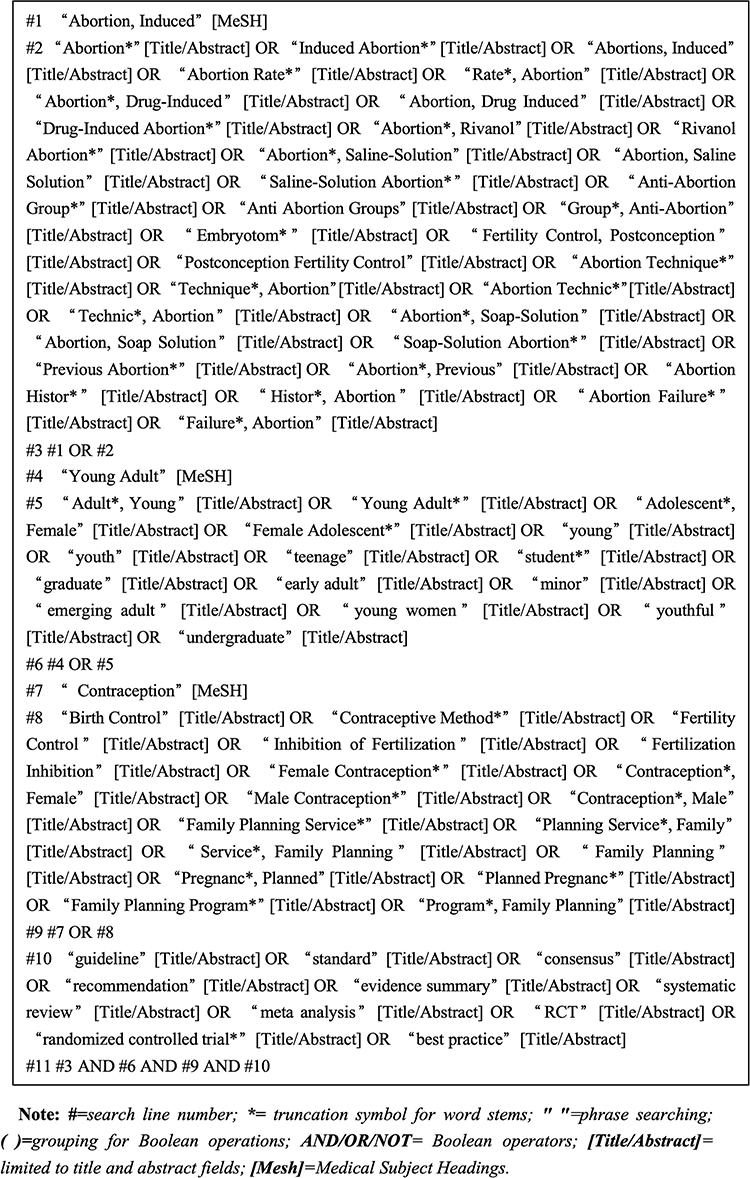 |
Figure 1 PubMed search strategy. |
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: studies covering young women aged 15–24 post-abortion; evaluating contraceptive methods (LARC, short-acting methods) or interventions (counseling, education); reporting contraceptive knowledge, unintended pregnancy rates, repeat abortion rates, uptake of effective methods, or correct use; including high-quality RCTs, systematic reviews, guidelines, evidence summaries, quasi-experimental studies; published in English or Chinese.
The exclusion criteria were as follows: abstract-only records, duplicate publications, studies with insufficient scientific quality or incomplete data, irrelevant studies.
Literature Screening and Data Extraction
All retrieved literature was imported into Endnote and duplicate literature was removed. All literature was independently screened by two researchers who received systematic evidence-based training. In the first round of screening, they reviewed titles, abstracts, and keywords. Subsequently, they read full text and re-screened the literature to evaluating the quality of the re-screened literature. When there was dispute, an authoritative expert specializing in evidence-based research was consulted to reach a consensus. Priority for conflicting evidence was determined by recent results, recognized principles, and high-quality studies.
Literature Quality Evaluation Criteria
The Appraisal of Guidelines for Research and Evaluation (AGREE II) tool33 was used to evaluate the quality of the guidelines. Expert opinions, consensuses, quasi-experimental studies, randomized controlled trials, and cohort studies were evaluated using the Australian JBI Evidence-Based Health Care Center tool.34 Meanwhile, due to the lack of recognized quality assessment tools for best practice evidence, evidence summaries, and recommended practices, we assessed the quality of these types of evidence by tracing back the original studies from which each source and selecting the appropriate assessment tools for quality evaluation. Use the AMSTAR 2.0 standard35 to evaluate the quality of the systematic reviews. All literature quality assessments were independently conducted by two researchers who had received training in evidence-based practice. Disagreements between the two reviewers were resolved through discussion by consulting a third researcher when necessary.
Evidence Extraction and Summary
Two researchers carefully and thoroughly read these 15 articles, extracting, analyzing, and comparing evidence that is consistent with the research topic and objectives. Then, they synthesized and classified similar and repetitive evidence into preliminary themes through discussion. Evidence was extracted and synthesized based on the following criteria: for independent evidence items, original texts were maintained without excessive embellishment; for similar recommendations, the version with more professional, brief, and strong readability was selected; for complementary recommendations, evidence was combined into complete statements following logical order; and for conflicting evidence, priority was given to high-quality evidence, evidence-based sources, and latest published authoritative literature. If there was any disagreement about evidence classification or interpretation, a third researcher with experience in evidence-based methods was consulted to reach a consensus. Through multiple rounds of discussion employing an iterative consensus-building approach, our research team carefully reviewed each piece of evidence, referencing similar frameworks developed in the field, to generate the final themes and entries.
This study used the evidence grading and evidence recommendation level system (2014 edition)36 of the JBI Evidence-Based Health Care Center (Australia) to uniformly grade the original literature included with evidence. According to the design type of literature, the level of evidence is ranked from Levels 1 to 5, with Level 1 representing the highest quality and Level 5 the lowest. Meanwhile, by analyzing the feasibility, validity, suitability, and clinical significance of adopted evidence, an expert meeting was convened to establish the strength of evidence recommendations. Finally, it was divided into strong recommendation (grade A) and weak recommendation (grade B).
Results
Literature Screening Results
The search yielded 3,634 records. After removing duplicates, screening titles/abstracts (n=3,115), and full-text review (n=52), 15 documents were included the following: 3 clinical decision aids, 7 guidelines, 2 expert consensus statements, 2 systematic reviews, and 1 RCT (Figure 2). Figure 2 shows the literature screening process. Table 1 lists the general characteristics of the included literature.
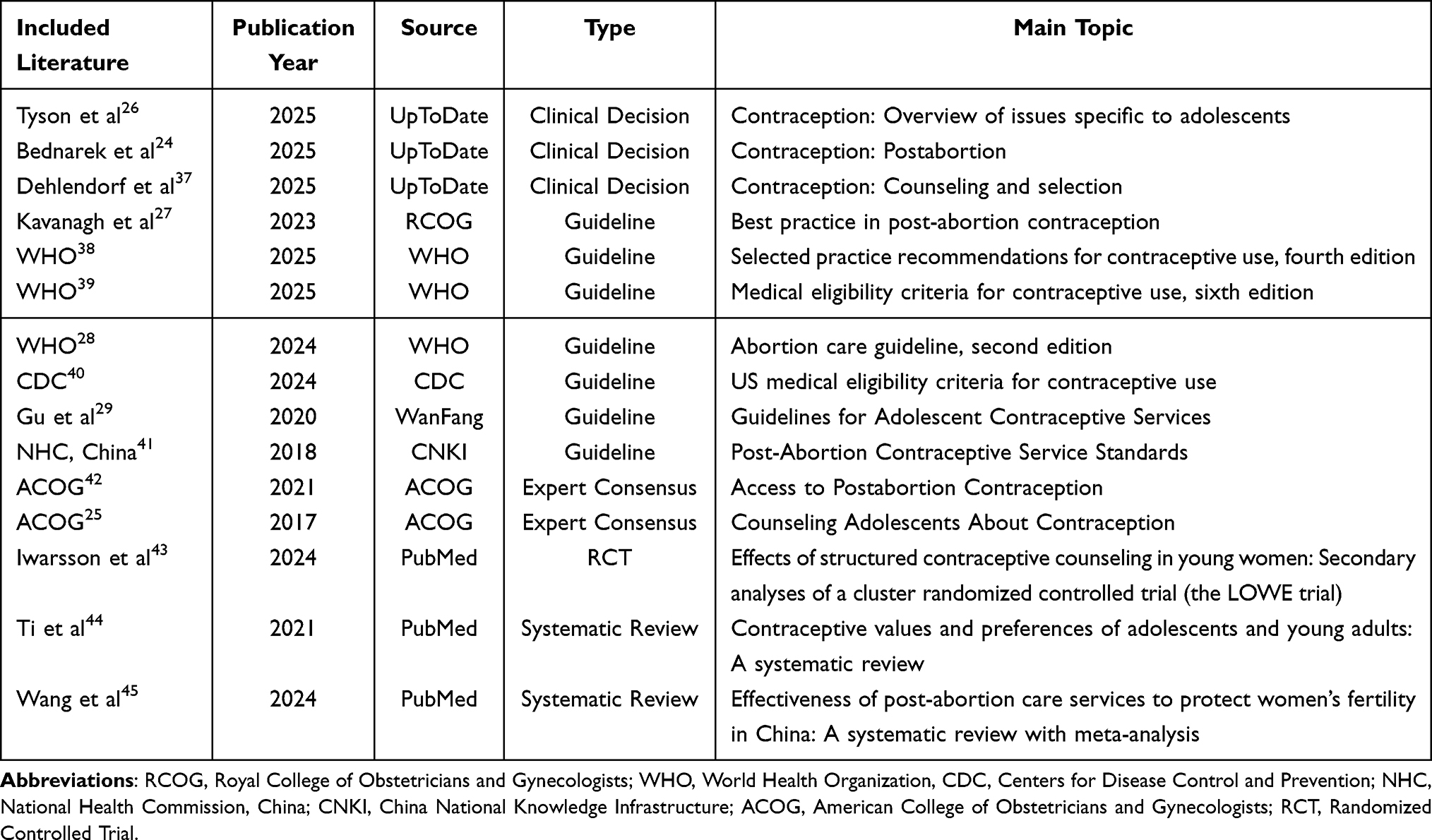 |
Table 1 General Characteristics of Included Literature (n=15) |
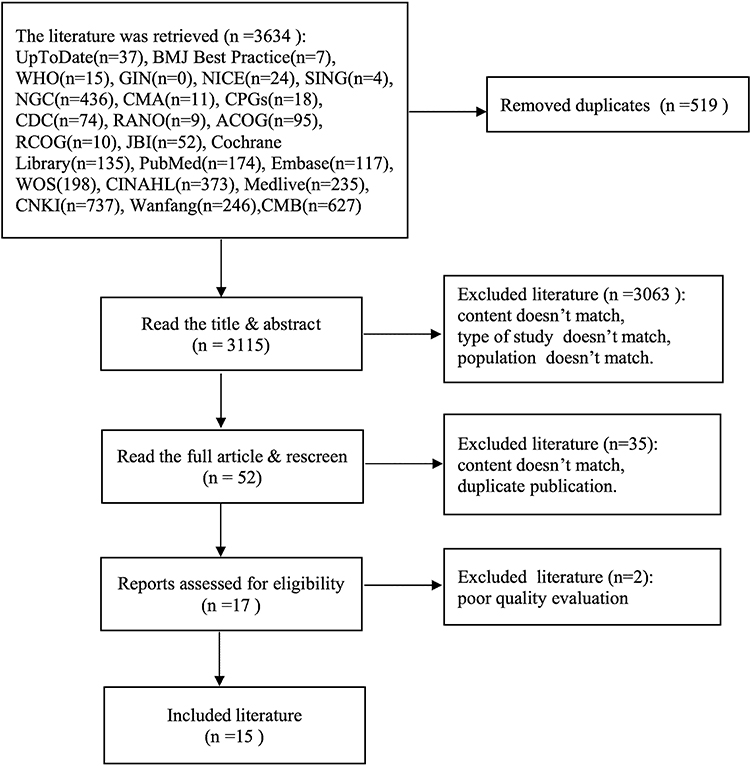 |
Figure 2 The flow chart of literature screening. |
Results of Literature Quality Evaluation
Quality Evaluation Results of Guidelines
This study used AGREE II to assess the quality of seven guidelines. Due to standardized scores of ≥ 60% in each field, four guidelines were rated as A-level, while two guidelines were rated as B-level, indicating overall high quality. For detailed content, refer to Table 2.
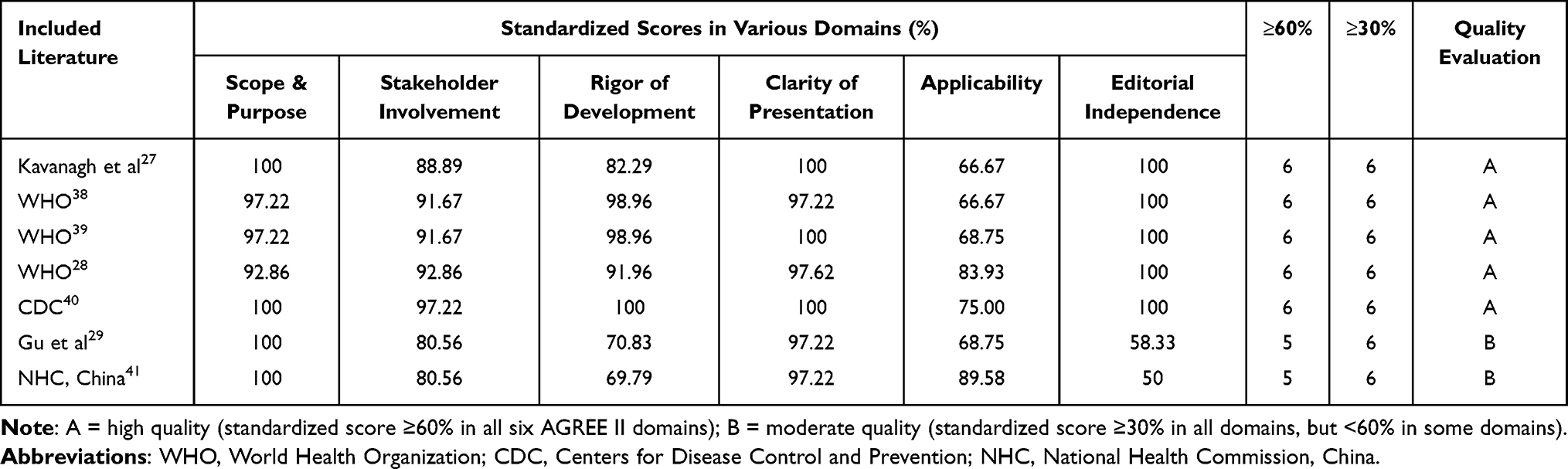 |
Table 2 AGREE II Quality Appraisal Results for Guidelines (n=7) |
Quality Evaluation Results of Expert Consensus
Two expert consensus25,42 studies from ACOG were included in this study. One42 of these received every item rated as “Yes.” In the other,25 all items were evaluated “Yes” except for Item 6, which was assessed as “unclear.” Both showed high quality and were retained.
Quality Evaluation Results of Systematic Reviews
Table 3 displays the quality evaluation findings for the two systematic reviews that were included.44,45 The systematic reviews were evaluated using the AMSTAR 2.0 standard.
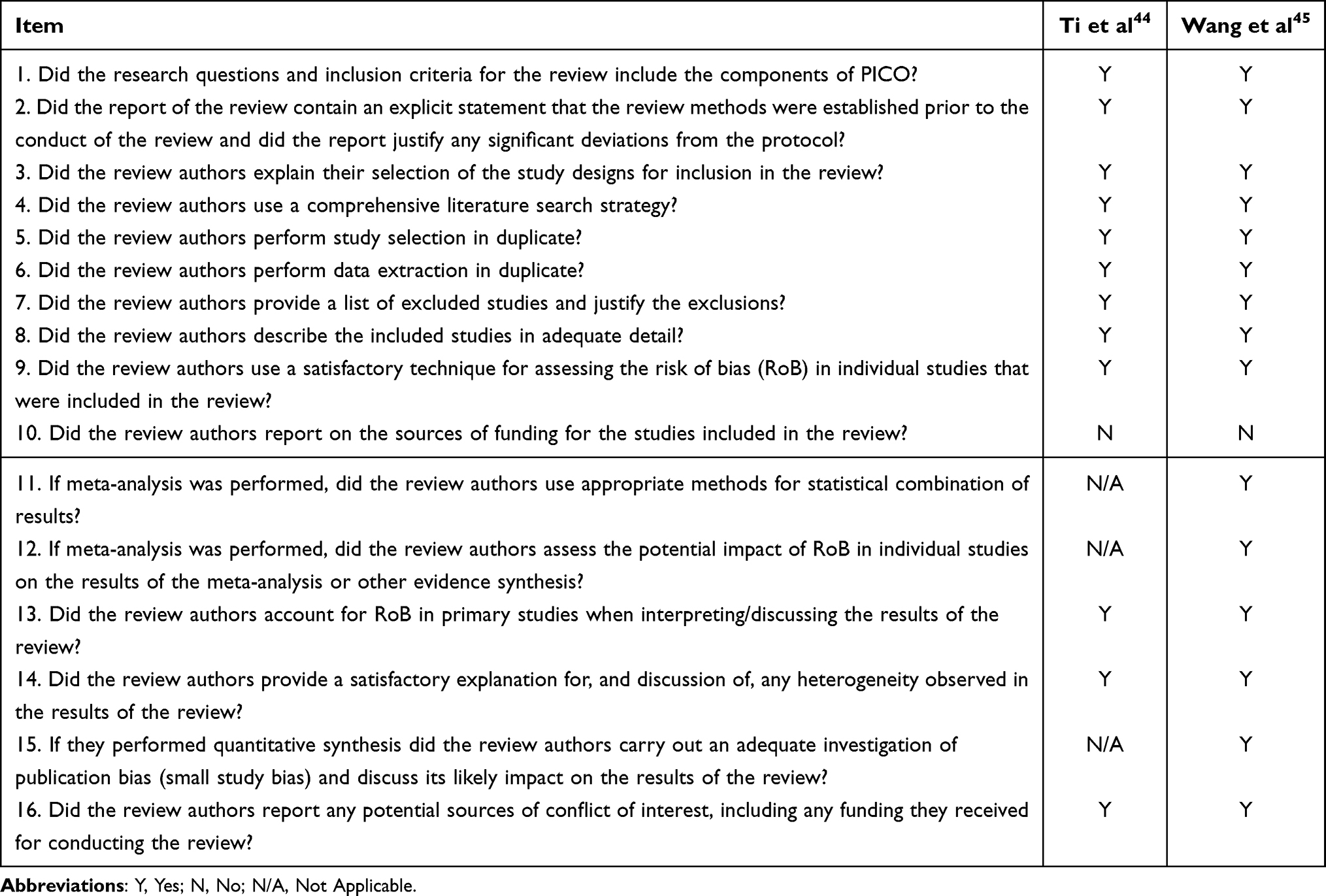 |
Table 3 Quality Evaluation Results of Included Systematic Reviews |
Quality Evaluation Results of RCT
One randomized controlled trial45 from PubMed was included in this study. All appraisal items were rated “Yes” except for Item 2 (allocation concealment) and Item 6 (blinding of outcome assessors), which were evaluated as “Unclear”, and Item 4 (blinding of participants) and Item 5 (blinding of interventionists), which were rated “No.” The overall quality was considered high, and the study was retained.
Best Evidence Synthesis
This study presents a comprehensive overview of the evidence on contraceptive guidance for young women following induced abortion. It encompasses provision of contraceptive services, timing of contraceptive initiation, assessment and counseling, values clarification, contraceptive methods introduction, complications and management, and follow-up and support. In total, 33 pieces of evidence are presented in Table 4.
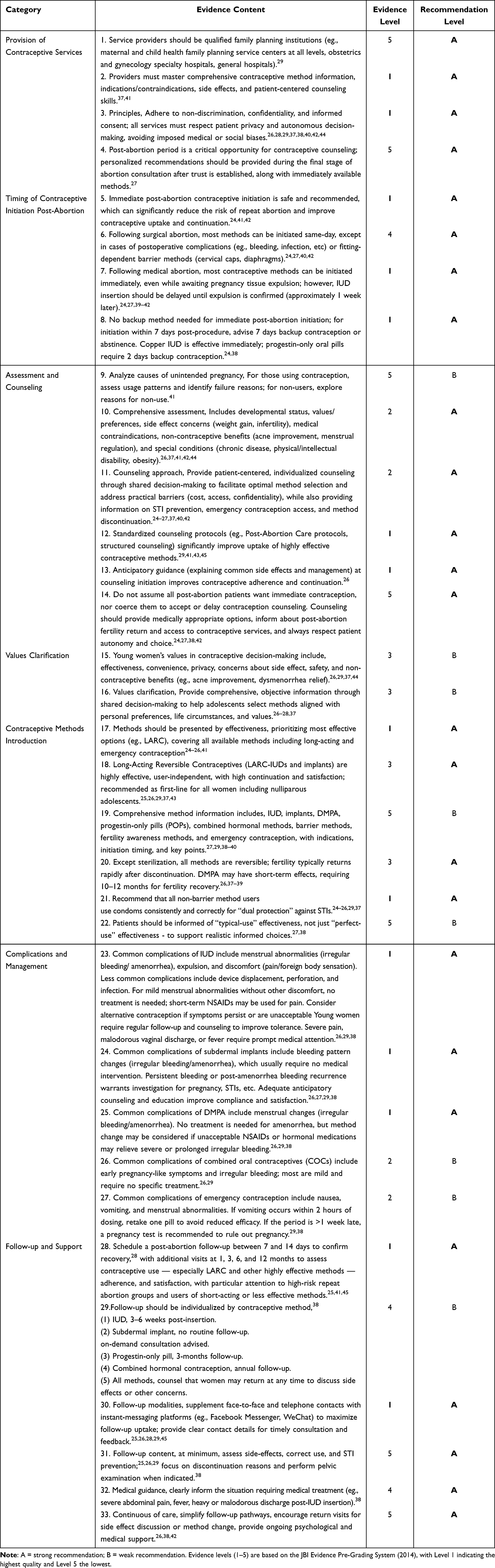 |
Table 4 Evidence Summary on Contraceptive Guidance for Young Women Post-Induced Abortion |
Discussion
Scientific Rigor and Evidence Profile
The evidence obtained from this summary is both reliable and instructive for contraceptive guidance in young women after induced abortion. This summary strictly followed the evidence summary reporting standards of the Evidence-Based Nursing of Fudan University. The AGREE II tool33 showed that five of the seven guidelines were Grade A and two were Grade B, indicating high methodological rigor and clinical applicability. The JBI critical-appraisal checklists for expert consensus and RCTs,34 together with the AMSTAR 2.0 standard for systematic reviews (2017 update),35 confirmed that all key items met high-quality thresholds. The evidence extraction was completed by two researchers independently to minimize individual bias, and all evidence was graded using JBI Evidence Pre Grading system, with recommendation strength determined through expert meetings based on the FAME structure.36
Critical Links in Post-Induced Abortion Contraceptive Care
The Critical Importance of Immediate Post-Abortion Contraceptive Initiation
Evidence 5–824,27,38–42 provide a comprehensive overview of post-abortion contraceptive timing-immediate initiation, same-day methods after surgical or medical abortion, and the need for back-up contraception. Several literatures26,27,29,42 underscore the importance of timely initiation of contraception following induced abortion to prevent unintended pregnancies. According to the American College of Obstetricians and Gynecologists (ACOG), access to postabortion contraception is crucial, although not all patients opt to initiate contraception immediately after the procedure.42 The recovery of ovulation after abortion occurs on average 21–29 days post-abortion but may occur as early as 8–10 days.24 Most women ovulate within 1 month, emphasizing the importance of prompt contraception initiation to prevent unexpected repeat pregnancies.28,46
Evidence from multiple sources24,27,41,42 suggests that contraception should be started immediately after the abortion procedure; same-day initiation increases both uptake and satisfaction while significantly reducing the risk of repeat abortion among young women.24,27,41,42,47 Cowett et al48 and Hohmann et al49 both demonstrated that same-day Etonogestrel-implant or Levonorgestrel-IUD insertion after D&E can ensure a 100% placement rate, and the 6-month continuation rate is significantly higher than delayed insertion. Hershman’s study also confirmed that immediate insertion of LARC after abortion can significantly reduce the 3-year repeat-abortion rate compared to women who did not receive LARC on the same day.50 These findings suggest that immediate initiation provides an advantage in reducing the vulnerability window of pregnancy, especially considering the rapid recovery of ovulation.28
The safety of various contraceptive methods after abortion has been established. All contraceptive methods are safe and effective when initiated immediately after abortion including hormonal contraception (depot medroxyprogesterone acetate (DMPA), intrauterine devices, and subdermal implants).40,42,51 Specifically, research has shown that beginning systemic hormonal contraception, such as DMPA, does not affect the success of subsequent abortions, suggesting that hormonal methods can be safely started at the time of or after an abortion procedure.46
Furthermore, clinical guidelines offer recommendations that account for individual variations. While early initiation is typically possible and effective, delayed initiation can be considered in certain cases, particularly when influenced by medical conditions or patient preferences.52,53 In conclusion, the current evidence supports the practice of early initiation of contraception after induced abortion, with a strong preference for same-day initiation to ensure optimal effectiveness and prevent subsequent unintended pregnancies. Individualizing the timing of initiation based on patient needs and preferences is an important aspect of post-abortion reproductive care.
Patient-Centered Assessment and Values Clarification
Evidence 9–16 states that, patient-centered assessment involves understanding not just medical eligibility for contraceptive methods, but also personal, social, and contextual influences on young woman’s contraceptive decision-making. In addition to completing standard medical eligibility screening, healthcare providers should understand the circumstances of the unintended pregnancy (contraceptive failure or non-use), developmental stage, health literacy, specific concerns about side effects (weight gain, changes in menstrual bleeding, etc), and desire for non-contraceptive benefits (acne treatment, menstrual regulation, etc.). For youth with chronic diseases, obesity, and/or disabilities, individualized risk–benefit assessment is critical to ensure safe and appropriate method selection. Overall, this individualized assessment enables providers to identify factors that may act as barriers or facilitators to contraceptive use and, ultimately, to person-centered recommendations.
The core of this individualized process is shared decision-making (SDM). Research has shown that person-centered contraception counseling for adolescents and young adults is directly associated with higher quality of care and increased uptake of preferred methods.54 For example, Durante et al55 emphasize that transitioning from a presumptive to an adolescent-centered, SDM approach can promote better communication, adherence, and reproductive autonomy, thereby clarifying values in real time. Ash et al56 further described contraceptive choice pathways and demonstrated how structured, dialogue-based on efficacy within the SDM framework supports informed and preference consistent decision-making.
Comprehensive evaluation is not limited to method selection, but also includes behavioral risk assessment and dual protection planning. Loh et al57 reported that the initiation of LARC may reduce the use of condom; through SDM, healthcare providers and patients can jointly develop a plan to protect against sexually transmitted infection (STI) when needed, ie., combining risk assessment with value negotiation. At the same time, assessment must address personal concerns, as demonstrated by Watson et al,58 who indicated that community college students are generally concerned about contraception affecting future fertility, which may pose barriers to the use of contraceptives.58 This finding is consistent with subsequent studies that emphasized the importance of incorporating discussions about fertility in patient-centered counseling to improve contraceptive uptake among youth.59 A systematic review44 in 2022 confirms that young people hold different contraceptive values, ranging from menstrual suppression to absolute discretion, and these values must be explicitly explored to meet their specific needs. The ACOG guideline60 emphasized that prioritizing the patient’s values in SDM can promote informed, autonomous choices and higher satisfaction. Similarly, for young women with IBD or other chronic conditions, personalized counseling will weigh the choice of estrogen-containing against the specific condition of the disease,61 emphasizing the importance of personalized counseling that considers individual health conditions.
Provision of Comprehensive Contraceptive Information with LARC Prioritization
Healthcare providers should present all contraceptive methods but prioritize those with the highest efficacy like long-acting reversible contraceptives (LARC), so young women have comprehensive and unbiased information upon which to base their decisions. Long-acting reversible contraceptives (LARC), such as intrauterine devices and subdermal implants, should be recommended as first-line methods due to their higher efficacy, continuation rates, and cost-effectiveness.27,29,38–40
In contrast to these benefits, a knowledge gap in LARC still exists in young women. According to a recent systematic review,62 the analysis found that AYAs (adolescents and young adults) have significant knowledge gaps entering their LARC counseling sessions, with misconceptions regarding eligibility, the reversibility of long-acting methods, and beliefs around infertility being prominent. Another study by Sharma et al63 supports the presence of a knowledge gap in young women, finding that these misbeliefs, specifically around eligibility, the reversibility, and the effectiveness of IUDs as emergency contraception, can lead to underutilization of LARC among AYAs. These findings further support and supplement the proposed study on the necessity to target the young women’s existing knowledge gap of LARC through education and counseling. Tailored educational approaches with a strong focus on were found to be significantly effective in increasing young women’s LARC acceptance and utilization.43
However, provider-based barriers, including implicit biases towards individuals of certain age, parity, or socioeconomic status, may preclude equitable LARC provision.64 This could lead to a hesitancy to offer or recommend LARC to young women, thereby continuing to fuel the disparity in contraceptive access and quality of contraceptive care. Policy statements65 and recent studies66,67 support eliminating implicit and explicit bias in contraceptive care with the ultimate goal of person-centered contraceptive care.
In conclusion, providing comprehensive contraceptive information, employing LARC as a first-line option, and addressing providers and clients’ knowledge gaps through structured education, can all be key elements to quality post-abortion contraceptive care among young women. These, and other approaches to address quality contraceptive care for women, work together to improve reproductive autonomy, as well as increase method uptake and continuation and avert future repeated unintended pregnancy.
Systematic Follow-Up and Continuity of Care
Based on the evidence included in the literature, systematic follow-up and continuity of care are considered key components in maintaining contraceptive use, preventing repeated unintended pregnancy, and supporting the overall health of young women after induced abortion. According to the WHO guidelines,28 comprehensive post-abortion care (PAC) should include not only include safe management of abortion procedure, but also counseling and follow-up to ensure physical and mental health. Several evidence suggest developing a structured follow-up schedule to confirm recovery from 7 to 14 days, followed by contact at 1, 3, 6, and 12 months after abortion to assess contraceptive use, particularly adherence and satisfaction with LARC and other highly effective methods. This schedule is particularly important for high-risk populations, such as women with a history of repeated abortions or who use short-acting or ineffective contraceptive methods.25,28,41,45
Follow-up after abortion can reduce mortality and morbidity due to unsafe abortion and can prevent future unintended pregnancies through provision of contraceptive services.68,69 In addition, follow-up after abortion should also include psychosocial support, which may help reduce negative emotional outcomes. One study found that mental health disorders occur more frequently after induced abortion compared to other pregnancy outcomes, and psychological support throughout follow-up may be important.70 A randomized controlled trial in Kenya found that person-centered telephone follow-up resulted in significantly better post-abortion mental health, suggesting that mobile-based support is feasible in resource-poor settings.71
Innovative strategies such as mobile-based support and electronic health tools are increasingly recognized for their potential to improve follow-up engagement. During the COVID-19 pandemic, telemedicine-based approaches received special attention. Dixon et al72 conducted a prospective cohort study evaluating the use of long-acting reversible contraception (LARC) NHS Lothian telemedicine abortion services, indicating that telemedicine can be an effective platform for post-abortion follow-up. Similarly, Reynolds-Wright et al73 described a post-abortion contraception text-and-call service aimed at supporting patients in accessing effective contraception after remote medical abortion. Educational interventions, such as demand-based education through platforms like WeChat, have been proven to support post-abortion recovery and provide valuable information to women, thereby improving overall outcomes.74 Electronic health tools have become an important way to follow-up after abortion. Shahrokhi et al systematically reviewed 33 studies and identified their effectiveness in enhancing follow-up, promoting contraceptive counseling, and reducing nursing barriers, which can improve post-abortion outcomes for young women.71,75
In addition, targeted support mechanisms such as youth-friendly education, counseling, and clinical services have been proven to promote young people’s acceptance of post-abortion contraception. A study reports that facilities supported for youth-friendly education and counseling significantly increase youth utilization of service, highlighting the importance of tailored support services in post-abortion contexts.76 Similarly, the development of youth-friendly post-abortion care services is considered a key factor in reducing barriers and increasing contraceptive prevalence, as demonstrated by the attributes identified in program supported by Pathfinder.77
Limitations
The findings of this evidence summary specifically focus on young women aged 15–24 after induced abortion and may not be directly applicable to women of other reproductive ages or in other reproductive health contexts. Despite an extensive search of major Chinese and English databases, we may have missed unindexed gray literature and local guidelines. Most of the included evidence was in English or reflected clinical contexts in China, and their generalizability to other ethnic, cultural, or health-system settings is uncertain. Furthermore, the legality of abortion varies significantly by region, which may influence the availability and provision of post-abortion contraceptive services. Healthcare providers should consider local values, resources, and policies to confirm and adapt the recommendations prior to implementation.
Conclusion
We systematically reviewed the available evidence on seven areas of contraception guidance for young women after induced abortion: the provision of contraceptive services, timing of initiation post-abortion, assessment and counseling, values clarification, introduction of contraceptive methods, complication management, and follow-up and support. The evidence supports the use of contraception soon after abortion with long-acting reversible contraceptive methods prioritized, and the delivery of a structured and personalized follow-up care for at least 12 months. This evidence-based framework provides healthcare providers with actionable strategies to overcome barriers such as stigma and lack of training while promoting young women’s reproductive autonomy. It serves as a practical reference to facilitate contraceptive uptake and continuation, ultimately helping to reduce the risk of repeat unintended pregnancies in young women.
In the future, when applying in clinical practice, healthcare providers should fully consider the local policies and personal preferences and adhere to the patient-centered principle. The focus of future research may be on the implementation of the above strategies, situational adaptation, and the evaluation of long-term effects. This will help to improve the evidence-based practices of the above-mentioned key area of reproductive health for young women.
Data Sharing Statement
The data supporting the results of this study are available from the first author (Lewei Tu) upon reasonable request.
Ethics Statement
This study does not require ethical approval because it is based only on a review of publicly available literature.
Disclosure
The authors declare no conflicts of interest.
References
1. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020;8(9):e1152–17. doi:10.1016/S2214-109X(20)30315-6
2. World Health Oganization. Abortion [EB/OL]. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/abortion.
3. Shah IH, Ahman E. Unsafe abortion differentials in 2008 by age and developing country region: high burden among young women. Reprod Health Matters. 2012;20(39):169–173. doi:10.1016/S0968-8080(12)39598-0
4. American College of Pediatricians. Induced abortion: risks that may impact adolescents, young adults, and their children [EB/OL]. 2016. Available from: https://acpeds.org/position-statements/induced-abortion-risks-that-may-impact-adolescents-young-adults-and-their-children.
5. Tang BWJ, Ibrahim BB, Shorey S. Complex journeys of adolescents after induced abortion: a qualitative systematic review. J Pediatric Nurs. 2024;77:e67–e80. doi:10.1016/j.pedn.2024.03.033
6. Arboleda NN. Mental health implications of abortion and abortion restriction: a brief narrative review of U.S. longitudinal studies. Ame J Psychiatry Residents’ J. 2024;20(1):11–15. doi:10.1176/appi.ajp-rj.2024.200106
7. Obare F, Kabiru CW, Chandra-Mouli V. Reducing early and unintended pregnancies among adolescents. Family Planning Evidence Briefs. 2018. https://knowledgecommons.popcouncil.org/departments_sbsr-rh/220/.
8. Zhao R, Zhang L, Fu X, Su C, Zhang Y. Sexual and reproductive health related knowledge, attitude and behavior among senior high school and col-lege students in 11 provinces and municipalities of China. Chin J Public Health. 2019;35(10):1330–1338. doi:10.11847/zgggws1124531
9. Ruan F, Fu G, Yan Y, et al. Inequities in consistent condom use among sexually experienced undergraduates in mainland China: implications for planning interventions. BMC Public Health. 2019;19(1):1195. doi:10.1186/s12889-019-7435-4
10. Huang M, Xiao Y, Wang S. Investigation on the status of sexual conception and behavior of college students in 6 universities in Guang-zhou under the background of internet. Chin J Hum Sex. 2020;29(10):157–160. doi:10.3969/j.issn.1672-1993.2020.10.044
11. Moges Y, Worku SA, Niguse A, Kelkay B. Factors associated with the unplanned pregnancy at Suhul General Hospital, Northern Ethiopia, 2018. J Pregnancy. 2020;2020:2926097. doi:10.1155/2020/2926097
12. Li X, Zhang H, Zhao S, Tang K. Predicting risky sexual behavior among college students through machine learning approaches: cross-sectional analysis of individual data from 1264 universities in 31 provinces in China. JMIR Public Health Surveillance. 2023;9:e41162. doi:10.2196/41162
13. Liu J, Wu S, Xu J, Temmerman M, Zhang W-H. Is repeat abortion a public health problem among chinese adolescents? A cross-sectional survey in 30 provinces. Int J Environ Res Public Health. 2019;16(5):794. doi:10.3390/ijerph16050794
14. Casey SE, Gallagher MC, Kakesa J, et al. Contraceptive use among adolescent and young women in North and South Kivu, Democratic Republic of the Congo: a cross-sectional population-based survey. PLoS Med. 2020;17(3):e1003086. doi:10.1371/journal.pmed.1003086
15. United Nations. SDG indicators: metadata repository [EB/OL]. 2025. Available from: https://unstats.un.org/sdgs/metadata/?Text=&Goal=3&Target=3.7.
16. Kantorová V, Wheldon MC, Dasgupta ANZ, Ueffing P, Castanheira HC, Anglewicz P. Contraceptive use and needs among adolescent women aged 15–19: regional and global estimates and projections from 1990 to 2030 from a Bayesian hierarchical modelling study. PLoS One. 2021;16(3):e0247479. doi:10.1371/journal.pone.0247479
17. Decide Pt. Youth reproductive health access (your health) survey[EB/OL]. 2025. Available from: https://powertodecide.org/what-we-do/information/resource-library/youth-reproductive-health-access-survey-2025-data-report.
18. Soin KS, Yeh PT, Gaffield ME, Ge C, Kennedy CE. Health workers’ values and preferences regarding contraceptive methods globally: a systematic review. Contraception. 2022;111:61–70. doi:10.1016/j.contraception.2022.04.012
19. Streifel C. Best practices for sustaining youth contraceptive use[EB/OL]. 2020. Available from: https://www.prb.org/wp-content/uploads/2021/01/best-practices-for-sustaining-youth-contraceptive-policy-brief.pdf.
20. Reilly K, Schmuhl KK, Bonny AE. Removing barriers to contraceptive access for adolescents. J Pediatr Pharmacol Ther. 2024;29(3):331–335. doi:10.5863/1551-6776-29.3.331
21. Reade LM, Sheeder JL, Richards MJ. The role of pediatric subspecialists in adolescent contraceptive care: knowledge, attitudes, and barriers. J Pediatr Adolesc Gynecol. 2025;38(3):377–383. doi:10.1016/j.jpag.2024.12.018
22. Rusterholz C. Responsible Pleasure: The Brook Advisory Centres and Youth Sexuality in Postwar Britain. Oxford: Oxford University Press; 2024.
23. Corley AG, Sprockett A, Montagu D, Chakraborty NM. Exploring and monitoring privacy, confidentiality, and provider bias in sexual and reproductive health service provision to young people: a narrative review. Int J Environ Res Public Health. 2022;19(11):6576. doi:10.3390/ijerph19116576
24. Bednarek P. Contraception: postabortion [EB/OL]. 2025. Available from: http://www.uptodate.zdby.sjuku.top/contents/zh-Hans/contraception-postabortion?search=Contraception%3A%20Postabortion&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
25. American College of Obstetricians and Gynecologists. Committee opinion No. 710: counseling adolescents about contraception. Obstetrics Gynecol. 2017;130(2):e74–e80. doi:10.1097/AOG.0000000000002234
26. Tyson N. Contraception: overview of issues specific to adolescents [EB/OL]. 2025. Available from: http://www.uptodate.zdby.sjuku.top/contents/contraception-overview-of-issues-specific-to-adolescents.
27. The Royal College of Obstetricians and Gynaecologists. Best practice in post-abortion contraception [EB/OL]. 2022. Available from: https://www.rcog.org.uk/guidance/browse-all-guidance/best-practice-papers/best-practice-in-post-abortion-contraception-best-practice-paper/.
28. World Health Oganization. Abortion Care Guideline.
29. Gu X, Wu S. Guidelines for adolescent contraceptive services. Chin J Obstet Gynecol. 2020;55(2):83.
30. Xing W, Hu Y, Zhou Y, et al. Promoting the transformation of evidence into clinical practice: making and writing evidence summary. J Nurses Train. 2020;35(12):1129–1132. doi:10.16821/j.cnki.hsjx.2020.12.016
31. Zheng Zhu YH, Xing W, Zhou Y, Ying G. The composition of different types of evidence based problems. J Nurses Train. 2017;32(21):1991–1994. doi:10.16821/j.cnki.hsjx.2017.21.025
32. Dicenso A, Bayley L, Haynes RB. Accessing pre-appraised evidence: fine-tuning the 5S model into a 6S model. Evidence Based Nursing. 2009;12(4):99–101. doi:10.1136/ebn.12.4.99-b
33. Fen Zhou YH, Cong X, Yao X. Supplementary explanation of agree II and scores in various fields for guideline research and evaluation tool. J Nurs. 2018;25(18):3. doi:10.16460/j.issn1008-9969.2018.18.056
34. Joanna Briggs Institute. Critical Appraisal Tools[EB/OL]. 2025-03. Available from: https://jbi.global/critical-appraisal-tools.
35. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Br Med J. 2017:
36. Wang Q, Hu Y. JBI evidence pre-classification and evidence rank system (2014 edition). J Nurses Train. 2015;30(11):964–967. doi:10.16821/j.cnki.hsjx.2015.11.002
37. Dehlendorf C. Contraception: counseling and selection [EB/OL]. 2025. Available from: https://www.uptodate.cn/contents/contraception-counseling-and-selection.
38. World Health Organization. Selected Practice Recommendations for Contraceptive Use.
39. World Health Organization. Medical Eligibility Criteria for Contraceptive Usee.
40. Nguyen AT, Curtis KM, Tepper NK, et al. US medical eligibility criteria for contraceptive use, 2024. MMWR Recomm Rep. 2024;73(3):1–77. doi:10.15585/mmwr.rr7304a1
41. National Health Commission of the People’s Republic of China. Post-abortion contraceptive service standards (2018 edition) [EB/OL]. 2018. Available from: https://www.nhc.gov.cn/fys/c100078/201808/cbae0db1ed204d01ba73232da68b980a.shtml.
42. American College of Obstetricians and Gynecologists. Access to postabortion contraception: ACOG committee opinion summary, number 833. Obstet Gynecol. 2021;138(2):324–325. doi:10.1097/AOG.0000000000004476
43. Iwarsson KE, Podolskyi V, Bizjak I, Kallner HK, Gemzell‐Danielsson K, Envall N. Effects of structured contraceptive counseling in young women: secondary analyses of a cluster randomized controlled trial (the LOWE trial). Acta Obstet Gynecol Scand. 2024;103(11):2242–2251. doi:10.1111/aogs.14954
44. Ti A, Soin K, Rahman T, Dam A, Yeh PT. Contraceptive values and preferences of adolescents and young adults: a systematic review. Contraception. 2022;111:22–31. doi:10.1016/j.contraception.2021.05.018
45. Wang X, Deng M, Zhu Y, Wu S, Mao Q, Wang H. Effectiveness of post-abortion care services to protect women’s fertility in China: a systematic review with meta-analysis. PLoS One. 2024;19(6):e0304221. doi:10.1371/journal.pone.0304221
46. Kim C, Nguyen AT, Berry-Bibee E, Ermias Y, Gaffield ME, Kapp N. Systemic hormonal contraception initiation after abortion: a systematic review and meta-analysis. Contraception. 2021;103(5):291–304. doi:10.1016/j.contraception.2021.01.017
47. International Federation of Gynecology and Obstetrics. Post-abortion contraception including long-acting reversible contraceptives [EB/OL]. 2021. Available from: https://www.figo.org/resources/figo-statements/post-abortion-contraception-including-long-acting-reversible-contraceptives.
48. Cowett AA, Ali R, Cooper MA, Evans M, Conzuelo G, Cremer M. Timing of etonogestrel implant insertion after dilation and evacuation: a randomized controlled trial. Obstet Gynecol. 2018;131(5):856–862. doi:10.1097/aog.0000000000002590
49. Hohmann HL, Reeves MF, Chen BA, Perriera LK, Hayes JL, Creinin MD. Immediate versus delayed insertion of the levonorgestrel-releasing intrauterine device following dilation and evacuation: a randomized controlled trial. Contraception. 2012;85(3):240–245. doi:10.1016/j.contraception.2011.08.002
50. Hershman SR, Reider MW. Does immediate post-abortion long-acting reversible contraception reduce rates of repeat abortion? [14I]. Obstet Gynecol. 2020;135(1):955. doi:10.1097/01.AOG.0000664152.59679.23
51. Rocca ML, Palumbo AR, Visconti F, Carlo CD. Safety and benefits of contraceptives implants: a systematic review. Pharmaceuticals. 2021;14(6):548. doi:10.3390/ph14060548
52. Bansal A, Kullu A, Dixit P. Understanding the healthcare provider role on post abortion contraception adoption in India using national family health survey-5. Reprod Health. 2023;20(1):123. doi:10.1186/s12978-023-01667-z
53. Pearlman Shapiro M, Stowers P, Raidoo S. Contraception after abortion. Clin Obstet Gynecol. 2023;66(4):749–758. doi:10.1097/GRF.0000000000000809
54. Whitfield B, Wilkinson TA, Lindberg LD. Adolescents’ and young adults’ receipt of person-centered contraceptive counseling. JAMA Network Open. 2025;8(12):e2551287. doi:10.1001/jamanetworkopen.2025.51287
55. Durante JC, Sims J, Jarin J, Gold MA, Messiah SE, Francis JKR. Long-acting reversible contraception for adolescents: a review of practices to support better communication, counseling, and adherence. Adolesc Health Med Therapeutics. 2023;14(14):97–114. doi:10.2147/ahmt.S374268
56. Ash MD, Watson IS, Matera LE, et al. An exploration of contraceptive choice pathways in adolescents and young adults. J Pediatr Adolesc Gynecol. 2024;37(5):505–509. doi:10.1016/j.jpag.2024.06.009
57. Loh M, Niu L, Arden M, Burk RD, Diaz A, Schlecht NF. Long-acting reversible contraception and condom use: a cohort study of female adolescents and young adults in New York City. Contraception. 2023;125:110081. doi:10.1016/j.contraception.2023.110081
58. Watson A, Yarger J, Sedlander E, et al. Concern that contraception affects future fertility: how common is this concern among young people and does it stop them from using contraception? Contraception. 2023;5:100103. doi:10.1016/j.conx.2023.100103
59. Zimmerman LA, Karp C, Shiferaw S, Seme A, Bell SO. Assessing the effect of concerns about contraceptive-induced fertility impairment on hormonal contraceptive use by parity and residence: evidence from PMA Ethiopia 2020 cross-sectional survey. BMJ Open. 2024;14(8):e077192. doi:10.1136/bmjopen-2023-077192
60. American College of Obstetricians and Gynecologists. Patient-centered contraceptive counseling: ACOG committee statement number 1. Obstet Gynecol. 2022;139(2):350–353. doi:10.1097/AOG.0000000000004659
61. Brenner EJ, Grewe ME, Tobi CB, et al. Perspectives on contraception, pregnancy, and reproductive health counseling from young women with inflammatory bowel disease. Crohns Colitis 360. 2024;7(1):otae078. doi:10.1093/crocol/otae078
62. Kirubarajan A, Li X, Yau M, et al. Awareness, knowledge, and misconceptions of adolescents and young people regarding long-acting reversible contraceptives: a systematic review and meta-analysis. Fertil Steril. 2022;118(1):168–179. doi:10.1016/j.fertnstert.2022.03.013
63. Sharma A, McCabe E, Jani S, Gonzalez A, Demissie S, Lee A. Knowledge and attitudes towards contraceptives among adolescents and young adults. Contracept Reproduct Med. 2021;6(1):2. doi:10.1186/s40834-020-00144-3
64. Allison BA, Bullington BW, Makhijani SA, Arora KS. Exploring primary care physician biases in adolescent contraceptive counseling. Contraception. 2025;141:110706. doi:10.1016/j.contraception.2024.110706
65. Ott MA, Hoopes AJ, Sucato GS, Leroy-Melamed M, Alderman EM. Contraception for adolescents: policy statement. Pediatrics. 2025;156(1):e2025072217. doi:10.1542/peds.2025-072217
66. Bryson A, Koyama A, Hassan A. Addressing long-acting reversible contraception access, bias, and coercion: supporting adolescent and young adult reproductive autonomy. Curr Opin Pediatr. 2021;33(4):345–353. doi:10.1097/MOP.0000000000001008
67. Hartheimer JS, Allison BA, Perry MF. Increasing access to LARC removal in pediatrics to support adolescent reproductive justice in the United States. Perspectives Sexual Reproduct Health. 2024;56(2):85–89. doi:10.1111/psrh.12270
68. Mbehero F, Momanyi R, Hesel K. Facilitating uptake of post-abortion contraception for young people in Kenya. Front Glob Womens Health. 2022;2:733957. doi:10.3389/fgwh.2021.733957
69. Arshad A, Aziz H, Shabbir G, Shakya S, Munir Z. Improving safe post-abortion care practices: a study on interventions implemented by Ipas Pakistan. Original Research. Front Public Health. 2023;11:01–07. doi:10.3389/fpubh.2023.1004381
70. Auger N, Healy-Profitos´ J, Ayoub A, Lewin A, Low N. Induced abortion and implications for long-term mental health: a cohort study of 1.2 million pregnancies. J Psychiatr Res. 2025;187:304–310. doi:10.1016/j.jpsychires.2025.05.031
71. Sudhinaraset M, Landrian A, Cotter SY, et al. Improving stigma and psychosocial outcomes among post-abortion Kenyan women attending private clinics: a randomized controlled trial of a person-centered mobile phone-based intervention. PLoS One. 2022;17(6):e0270637. doi:10.1371/journal.pone.0270637
72. Dixon A, Reynolds-Wright JJ, Cameron ST. Uptake of long-acting reversible contraception after telemedicine delivered abortion during Covid-19. Eur J Contracept Reprod Health Care. 2022;27(4):284–288. doi:10.1080/13625187.2022.2085680
73. Reynolds-Wright JJ, Cameron ST. A post-abortion contraception text-and-call service to support patients to access effective contraception after telemedicine abortion. BMJ Sexual Reproduct Health. 2025;51(1):51–53. doi:10.1136/bmjsrh-2024-202391
74. Shi D, Liu C, Huang L, Chen X-Q. Correction: post-abortion needs-based education via the WeChat platform to lessen fear and encourage effective contraception: a post-abortion care service intervention-controlled trial. BMC Womens Health. 2024;24(1):194. doi:10.1186/s12905-024-03033-y
75. Shahrokhi SN, Salmani H, Ahmadi M. The role of electronic health tools in unwanted pregnancy prevention, abortion and post-abortion follow-up: a systematic review. Iranian J Nurs Midwifery Res. 2023;28(5):487–503. doi:10.4103/ijnmr.ijnmr_312_20
76. Kigongo E, Ekungu E, Edmonton A, et al. Bridging participation gaps: a community-led inception for integrating comprehensive adolescent-friendly family planning and post-abortion care (CAFFP–PAC) into primary healthcare facilities in Northern Uganda. Open Access J Contracept. 2025;Volume 16(16):81–96. doi:10.2147/OAJC.S550132
77. Stephens B, Mwandalima IJ, Samma A, Lyatuu J, Mimno K, Komwihangiro J. Reducing barriers to postabortion contraception: the role of expanding coverage of postabortion care in Dares Salaam, Tanzania. Glob Health Sci Pract. 2019;7(Suppl Supplement 2):S258–s270. doi:10.9745/ghsp-d-19-00146
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.