Back to Journals » Journal of Blood Medicine » Volume 12
Evaluation of Warfarin Anticoagulation at University of Gondar Comprehensive Specialized Hospital, North-West Ethiopia
Authors Masresha N, Muche EA ![]() , Atnafu A
, Atnafu A ![]() , Abdela O
, Abdela O ![]()
Received 23 September 2020
Accepted for publication 16 March 2021
Published 23 March 2021 Volume 2021:12 Pages 189—195
DOI https://doi.org/10.2147/JBM.S282948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Nahusenay Masresha,1 Esileman Abdela Muche,2 Asmamaw Atnafu,3 Ousman Abdela2
1Hospital Pharmacy, University of Gondar Comprehensive and Specialized Hospital, Gondar, Ethiopia; 2Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Ousman Abdela Tel +251-912-02-3692
Fax +251-58-114 1240
Email [email protected]
Purpose: To assess the quality of warfarin anticoagulation and its clinical outcomes on patients treated with warfarin at the University of Gondar comprehensive specialized hospital, North-west Ethiopia.
Methods: We reviewed medical records of patients treated with warfarin between June 1, 2016, and May 30, 2018, at the University of Gondar comprehensive specialized hospital. The quality of anticoagulation was evaluated using the percentage of time spent in the therapeutic range. Data were entered into Statistical Product and Service Solutions (SPSS), version 20. Descriptive statistics were used to describe the socio-demographic and clinical characteristics of study participants. Multivariable logistic regression analysis was performed to identify independent predictors of quality of anticoagulation. Statistical significance was declared when the p-value was less than 0.05 at 95% confidence interval (CI).
Results: From a total of 202 patients’ charts reviewed, women accounted for 134 (67.3%). The mean participants’ age was 44.33 years (± 17.05years SD). The median time spent in the therapeutic range was 37.91 with an IQR of (0.00– 65.86). More than two-third (143, (70.8%)) of participants had poor anticoagulation quality (time spent in the therapeutic range is less than 65%). Twenty-seven patients (13.4%) experienced adverse medication events of bleeding and thromboembolic events. Logistic regression analysis showed that potential medication interaction [p= 0.003 95% CI Adjusted odds ratio (AOR): 0.32 (0.152– 0.689)] and presence of co-morbidity [p= 0.037 95% CI AOR: 0.70 (1.046– 4.105)] were significantly associated with quality of anticoagulation.
Conclusion: The quality of warfarin anticoagulation at the University of Gondar comprehensive specialized hospital was poor. A strong effort is needed to improve the quality of anticoagulation. Patients who had other co-morbidity conditions and potentially interacting medication need special attention.
Keywords: warfarin, anticoagulation, University of Gondar, TTR, Ethiopia
Introduction
Cardiovascular disease (CVD) and stroke produce enormous health and economic burdens worldwide.1 CVD is becoming the second common cause of death in most African countries following infectious disease, estimated to account for 20% of total deaths in 2020.2
Anticoagulants are prescribed for the prevention and treatment of deep vein thrombosis, pulmonary embolism, atrial fibrillation, myocardial infarction, unstable angina, rheumatic heart disease, etc. They decrease the burden of CVD.3,4
Warfarin acts as an anticoagulant by reducing the synthesis of functional vitamin K-dependent clotting factors.5 It is thought to interfere with clotting factors by inhibiting the C1 subunit of the vitamin K epoxide reductase.6
Warfarin is underutilized in clinical care as it is related to adverse medication events.7,8 Some medications including clopidogrelor aspirin may increase the risk of bleeding complications if co-administered.9 Food supplements that are rich in vitamin k such as garlic, ginger, and ginkgo have interactions with warfarin.10,11 Inter-individual differences in medication response, and its narrow therapeutic range makes warfarin a problematic medication.10,12,13
Time in therapeutic range (TTR) is commonly used to evaluate the quality of warfarin therapy. It is defined as the percentage of time the patients INR was within the target range.6 There are three different methods for calculating TTR; Percent of INRs in the therapeutic range, the cross-section of the file’s method, and the Roosendaal linear interpolation method.14 Among these, the Roosendaallinear interpolated method has become a widely accepted measure of the quality of anticoagulation.7
Assessing TTR allows physicians to estimate the success of warfarin therapy.15 The quality of warfarin therapy is good if the average time of the INR in the therapeutic range is high and exceeds 65%.16
A time therapeutic range above 65% has been reported to be beneficial against stroke and vascular events among patients treated with warfarin. On the other hand, TTRs values of less than 40% are not associated with any significant mortality benefit.16–18 On contrary, patients with TTR <65% were found to have a 2.6-fold higher risk of stroke, 1.5-fold higher risk of major bleeding, and 2.4-fold higher risk of all-cause mortality.19
In general, assessing TTR is important to evaluate the current standard of anticoagulation.2 Studies addressing the quality of anticoagulation in Ethiopia are scarce. This study aimed to evaluate the quality of anticoagulation and associated factors among patients treated with warfarin at the chronic outpatient department of the University of Gondar comprehensive and specialized Hospital (UoGCSH), North-West Ethiopia.
Methods
Study Area and Period
The study was conducted at the University of Gondar comprehensive specialized hospital (UoGCSH) from June 1st to July 30th, 2018. The hospital is located in Gondar city, North-West of Ethiopia. It is one of the tertiary care hospitals in the Amhara regional state, and it is offering outpatient, inpatient, and emergency services. The hospital provides services for about seven million populations in the catchment areas. The hospital has currently about 2000 medical and non-medical staff and has more than 598 beds.
Study Design
A retrospective cross-sectional study was conducted on adult patients treated with warfarin at UoGCSH North-West Ethiopia.
Population
Source population
All adult patients who were treated with warfarin and had follow-up at the chronic outpatient department of UoGCSH.
Study Population
All adult patients who were treated with warfarin and had attended their follow-up in the chronic outpatient department of UoGCSH from June 1st, 2016 to May 30th 2018.
Study Variables
Independent Variables
- Age, Sex, Residence, Duration of anticoagulation, Number of concomitant medications, presence of potentially interacting Medications, presence of co-morbidity, and presence of adverse drug event.
Dependent Variables
- Quality of anticoagulation.
Sampling Technique and Sample Size Determination
Sampling Technique
All adult patients who attended the chronic outpatient department of UoGCSH and received warfarin from June 1st, 2016 to May 30th, 2018, and fulfilled the inclusion criteria were included.
Inclusion and Exclusion Criteria
Inclusion Criteria
- All adult patients treated with warfarin for more than one month and on follow-up between June 1st, 2016 and May 30th, 2018 at the chronic outpatient department of UoGCSH.
Exclusion Criteria
- Patients with less than 2 INR measurements, INR value discrepancy between hematology laboratory record and chart data were excluded.
Data Collection Process
Patients’ charts were retrieved from the outpatient record office based on chart numbers on the chronic outpatient log book. Then, laboratory INR records of included charts were reviewed from the hematology laboratory office. A pre-designed structured data collection format was utilized to extract necessary data from patients’ medical files. Information on socio-demographics of participants, indications, and duration of warfarin therapy, comorbidities, concomitant medications, and international normalized ratio values, and the dates of the tests were extracted. Trained nurses who were working at the chronic outpatient department at the time of the data collection period filled the data abstraction form.
Data Quality Assurance
A pre-test was done on 5% of the sample size in another tertiary care hospital in Amhara regional state. Data were then collected, reviewed, and checked for completeness and relevance by the principal investigator each day.
Data Analysis and Interpretation
The extracted data were entered and analyzed by SPSS version 20. We used the Roosendaal linear interpolation method to calculate the TTR. The %TTR was calculated using excel. Those whose INR records out of range and in the range were given a %TTR value of 0% and 100% respectively. The predictor variables were checked by the chi-square test. Those variables that had full filled the assumption underwent bivariate analysis, and variables with P-value <0.20 were taken and analyzed using multivariable logistic regression. P-values less than 0.05 with 95% CI was taken to be statistically significant.
Ethical Consideration
The study was conducted after getting an ethical clearance letter from an ethical review committee of the school of pharmacy, University of Gondar. Letter of cooperation was obtained from the hospital clinical director and head of chronic outpatient department offices. Data were collected anonymously and kept confidential. This study was conducted in accordance with the Declaration of Helsinki.
Operational Definitions
Good quality anticoagulation: The time spent in the therapeutic range (TTR) is greater than or equal to 65%.
Poor quality anticoagulation: The time spent in the therapeutic range is less than 65%.
Therapeutic: The time they spent in the therapeutic range (INR between 2 & 3 and including them).
Subtherapeutic: The time they spent in the sub-therapeutic range (INR<2)
Supra therapeutic: The time they spent in supratherapeutic range (INR>3)
Definition of Terms
Major bleeding: are non-surgical bleedings that result in death, are life-threatening, cause chronic sequelae or consume major health care resources. All non-major bleeds will be considered minor bleedings.
Thromboembolism: Formation in a blood vessel of a clot (thrombus) that breaks loose and is carried by the blood stream to plug another vessel.
Results
Socio-Demographic and Clinical Characteristics of Participants
A total of 202 patients’ charts fulfilled the inclusion criteria and hence studied. Slightly higher than two-third of the studied subjects (134, (67.3%)) were females. Most of the participants (140, (69.3%)) had taken warfarin for less than one-year duration. Hundred and twenty-six (62.67%) patients had co-morbid conditions; heart failure (45 (22.3%)), hyperthyroidism (23, (11.4%)), and hypertension (20 (9.9%)) being the three most frequent co-morbidities (see Table 1).
 |
Table 1 Socio-Demographic and Clinical Characteristics of Participants at UoGCSH from June 2016 to June 2018 (n=202) |
Clinical Outcomes of Participants
Participants’ mean time spent during their anticoagulation therapy was 41% in the therapeutic range, 42% of their time in the sub-therapeutic range, and 17% of their time in the supra-therapeutic range. Twenty-seven patients experienced adverse medication events; 9 patients (4.5%) had bleeding events, 15 patients (7.4%) had thromboembolic events, and 3 (1.5%) had emergency hospital visits (see Table 2).
 |
Table 2 Clinical Outcome of Patients on Warfarin in COPD at UoGCSH from June 2016 to June 30th 2018 (N= 202) |
Warfarin Indications
Warfarin was prescribed for treatment ofthe following diseases: Atrial fibrillation (131, (39.8%)), valvular heart diseases (127, (38.6%)), deep venous thrombosis (49 (14.9%)), and Pulmonary embolism (PE) (22, (6.7%))
Number of Concomitant Medications
Most study participants (178 (88.1%)) had at least one medication besides warfarin. The mean number of concomitant medications was 2.08 (SD ± 1.4), and 53.5% of participants had more than four medications (Table 3). A total of 703 INR measurements were analyzed. The mean INR measurement frequency per patient was 3.48 ±1.26 SD. The median time-frequency of INR measurement was 20.875 days IQR (25–16.27). The median time spent in the therapeutic range was 37.91 with an IQR of (0.00–65.86)
 |
Table 3 Frequency and Number of Concomitant Medications Among Patients on Warfarin COPD at UoGCSH from June 2016 to June 2018 (N=202) |
Associated Factor for Quality of Anticoagulation
Determinants of poor quality of anticoagulation on multivariable logistic regression analysis were potential medication interaction (p= 0.003; AOR with 95% CI = 0.32 (0.15–0.69)) and presence of co-morbidity condition (p= 0.037; AOR with 95% CI = 0.70 (1.05–4.11)) (see Table 4).
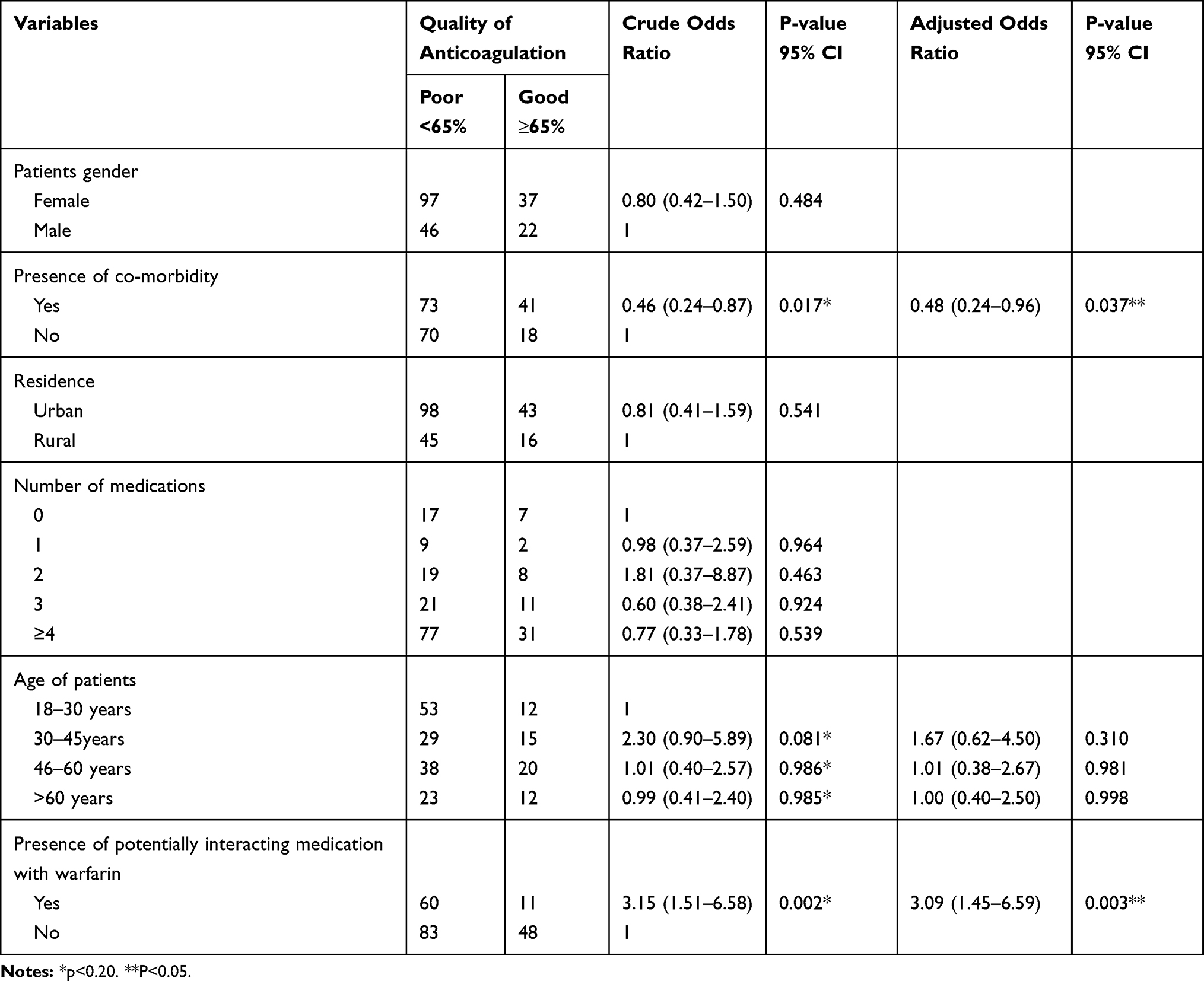 |
Table 4 Predictors of Quality of Anticoagulation Among Patients Treated with Warfarin at UoGCSH from June 2016 to June 2018 (N=202) |
Discussion
The current study revealed that warfarin prescription for more than two-thirds (70.8%) of participants was of poor quality. The mean time spent in the therapeutic range is 41%. This figure is lower compared to the report from South Africa (48.5%) 13, USA (56.7%) 27, Spain (63.8%) 26, Iran (54.9%) 18, Portugal (60.3%) 19, Sweden (77%) 21, Finland and Australia%28. The reason behind this difference may be their standard of care is much better than the current setting.20–22
In the current study, participants spent more than half of the time (59%) out of the therapeutic range. They spent the majority of their time (42%) in the sub-therapeutic range. Time spent in the therapeutics range of patients is related to mortality benefit. More than half of study participants had a TTR of less than 40%. Therefore; they may not get mortality benefits from warfarin treatment. This is evidenced by a meta-analysis done by Mearns ES et al which showed patients having %TTR less than 40% do not have mortality benefit.20
The current study showed that male participants had a better quality of anticoagulation compared to their female counterparts. This finding is supported by findings from Sweden and South Africa which reported males to have better coagulation outcomes than females. Their food habit of eating more green vegetables which have high Vit K was indicated as the reason behind the vulnerability of females for poor coagulation.12
The current study revealed the presence of co-morbidity to be a predictor of poor quality of anticoagulation (p= 0.037), AOR=0.70 (1.05–4.11) which means 29.8% less chance of getting a good quality of anti-coagulation than patients without the co-morbid condition. This is in line with the report from Israel,23 and Saudi Arabia.24 The study reported by Melamed et al and Khan et al also showed that poor quality of anticoagulation had been associated with populations affected by co morbidities.23,24
More than fifty percent of our patients had greater than four medications co-prescribed with warfarin. A study done in Iran by Farsad et al identified that the number of medications more than four has significant predictors of poor quality of anticoagulation this may be due to poor adherence.15
The current study also revealed that participants who have been prescribed warfarin with another medication(s) with the known potential of interaction with warfarin were found to have 67.6% less chance of good quality of anti-coagulation (p=0.003), AOR =0.32 (0.15–0.69). This finding is supported by reports from Canada which showed that patients who had taken warfarin with interacting medications had spent less time in the therapeutic range compared with those without concomitant medications.25 There are pieces of evidence that the medications commonly co-prescribed in the current study participants including digoxin, Aspirin, and NSAIDs have pharmacodynamic interaction with warfarin leading to poor quality of anticoagulation. A case report from Britania stated that loss of warfarin anticoagulation effect with prolonged INR > 10 was recorded on a patient who was on warfarin and digoxin.26
In this study, thromboembolic events were the most prevalent clinical outcome followed by bleeding events. This is in line with the report from the United States of America.20 The reason why the thromboembolic event was more prevalent in our study might be because the current study participants spent most of their time in the sub-therapeutic range.
Limitations of the Study
The study design was retrospective crossectional. Due to incompleteness of data, variables that may potentially affect the quality of anti-coagulation including, educational status, income, diet, use of over-the-counter medications, adherence, and others were not studied. In addition, patients might seek health service in other hospital or clinic and had other co-morbid conditions and medications that were not recorded. Otherwise, the study tried to show the quality of anticoagulation in resource limited settings.
Abbreviations
AOR, Adjusted Odds Ratio; CVD, Cardio Vascular Disease; DVT, Deep Venous Thrombosis; INR, International Normalization Ratio; ISI, International Sensitivity Index; MI, Myocardial Infarction; OR, Odds Ratio; PE, Pulmonary Embolism; SD, Standard Deviation; TTR, Time in Therapeutic Range; VKA, Vitamin K Antagonist; VTE, Venous Thrombo Embolism; UoGCSH, University of Gondar comprehensive Specialized Hospital.
Data Sharing Statement
The datasets during and/or analyzed during the current study are available from the author on reasonable request.
Acknowledgments
We would like to thank the University of Gondar for funding this research project. We are also very grateful to the nursing staffs of the chronic outpatient department of UoGCSH for their cooperation in the data collection process.
Funding
This research was done with the financial support of the University of Gondar.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38–e360. doi:10.1161/CIR.0000000000000350
2. Mbewu A. The burden of cardiovascular disease in sub-Saharan Africa: burden of cardiovascular disease. SA Heart J. 2009;6(1):4–10.
3. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3):338S–400S.
4. Wadelius M, Pirmohamed M. Pharmacogenetics of warfarin: current status and future challenges. Pharmacogenomics J. 2007;7(2):99. doi:10.1038/sj.tpj.6500417
5. Barnes G, Ageno W, Ansell J, Kaatz S. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC of the ISTH. J Thromb Haemost. 2015;13(6):1154–1156. doi:10.1111/jth.12969
6. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2008;133(6):160S–98S.
7. Ageno W, Gallus AS, Wittkowsky A, Crowther M, Hylek EM, Palareti G. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2):e44S–e88S.
8. Kuruvilla M, Gurk-Turner C. A review of warfarin dosing and monitoring. Proc (Bayl Univ Med Cent). 2001;14(3):305. doi:10.1080/08998280.2001.11927781
9. Drugs.com. Warfarin drug interactions; February 2, 2021. https://www.drugs.com/drug-interactions/warfarin.html.
10. Nutescu EA, Shapiro NL, Ibrahim S, West P. Warfarin and its interactions with foods, herbs and other dietary supplements. Expert Opin Med Saf. 2006;5(3):433–451. doi:10.1517/14740338.5.3.433
11. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its medication and food interactions. Arch Intern Med. 2005;165(10):1095–1106. doi:10.1001/archinte.165.10.1095
12. Sonuga BO, Hellenberg DA, Cupido CS, Jaeger C. Profile and anticoagulation outcomes of patients on warfarin therapy in an urban hospital in Cape Town, South Africa. Afr J Prim Health Care Fam Med. 2016;8(1):1–8. doi:10.4102/phcfm.v8i1.1032
13. Teles JS, Fukuda EY, Feder D. Warfarin: pharmacological profile and medication interactions with antidepressants. Einstein (Sao Paulo). 2012;10(1):110–115. doi:10.1590/S1679-45082012000100024
14. Karuri SW Quality of oral anticoagulation management among patients on follow up at Kenyatta national hospital. University of Nairobi; 2016.
15. Farsad B-F, Abbasinazari M, Dabagh A, Bakshandeh H. Evaluation of Time in Therapeutic Range (TTR) in patients with non-valvular atrial fibrillation receiving treatment with Warfarin in Tehran, Iran: a cross-sectional study. J Clin Diagn Res. 2016;10(9):FC04. doi:10.7860/JCDR/2016/21955.8457
16. Caldeira D, Cruz I, Morgado G, et al. Evaluation of time in therapeutic range in anticoagulated patients: a single-center, retrospective, observational study. BMC Res Notes. 2014;7(1):891. doi:10.1186/1756-0500-7-891
17. Morgan CL, McEwan P, Tukiendorf A, Robinson PA, Clemens A, Plumb JM. Warfarin treatment in patients with atrial fibrillation: observing outcomes associated with varying levels of INR control. Thromb Res. 2009;124(1):37–41. doi:10.1016/j.thromres.2008.09.016
18. Connolly SJ, Pogue J, Eikelboom J, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation. 2008;118(20):2029–2037. doi:10.1161/CIRCULATIONAHA.107.750000
19. Haas S, Ten Cate H, Accetta G, et al. Quality of vitamin K antagonist control and 1-year outcomes in patients with atrial fibrillation: a global perspective from the GARFIELD-AF registry. PLoS One. 2016;11(10):e0164076. doi:10.1371/journal.pone.0164076
20. Mearns ES, White CM, Kohn CG, et al. Quality of vitamin K antagonist control and outcomes in atrial fibrillation patients: a meta-analysis and meta-regression. Thromb J. 2014;12(1):14. doi:10.1186/1477-9560-12-14
21. Steffel J, Verhamme P, Potpara TS, et al. The 2018 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1330–1393.
22. McDonald KM; UCSF-Stanford E. Making health care safer a critical analysis of patient safety practices. Am J Health Syst Pharm. 1995;52:2543–2549. doi:10.1093/ajhp/52.22.2543
23. Khan TI, Kamali F, Kesteven P, Avery P, Wynne H. The value of education and self‐monitoring in the management of warfarin therapy in older patients with unstable control of anticoagulation. Br J Haematol. 2004;126(4):557–564. doi:10.1111/j.1365-2141.2004.05074.x
24. Melamed OC, Horowitz G, Elhayany A, Vinker S. Quality of anticoagulation control among patients with atrial fibrillation. Am J Manag Care. 2011;17(3):232–237.
25. Verhovsek M, Motlagh B, Crowther MA, et al. Quality of anticoagulation and use of warfarin-interacting medications in long-term care: a chart review. BMC Geriatr. 2008;8(1):13. doi:10.1186/1471-2318-8-13
26. Bhattacharyya A, Bhavnani M, Tymms DJ. Serious interaction between digoxin and warfarin. Br J Cardiol. 2002;9(6):356–357.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.