Back to Journals » Patient Preference and Adherence » Volume 20
Evaluation of Treatment Modalities for Radiation Therapy-Induced Trismus, Considering the Timing and Adherence to Progress in Mouth Opening and Oral Health–Related Quality of Life: A Systematic Review
Authors Meidarlina I ![]() , Rikmasari R, Wicaksono S
, Rikmasari R, Wicaksono S ![]() , Maskoen Snr AM, Kusumadjati A
, Maskoen Snr AM, Kusumadjati A
Received 30 November 2025
Accepted for publication 30 January 2026
Published 9 March 2026 Volume 2026:20 585596
DOI https://doi.org/10.2147/PPA.S585596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ista Meidarlina,1,2 Rasmi Rikmasari,2 Satrio Wicaksono,3 Ani Melani Maskoen Snr,4,5 Adji Kusumadjati6,7
1Doctoral Program in Biotechnology, Department of Biotechnology, Graduate School, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Prosthodontics, Faculty of Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Faculty of Mechanical and Aerospace Engineering, Institut Teknologi Bandung, Bandung, West Java, Indonesia; 4Department of Biotechnology, Graduate School, Universitas Padjadjaran, Bandung, West Java, Indonesia; 5Department of Oral Biology, Faculty of Dentistry, Universitas Jendral Achmad Yani, Bandung, West Java, Indonesia; 6Department of Radiation Oncology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 7Department of Radiation Oncology, Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
Correspondence: Ista Meidarlina, Email [email protected]
Purpose: To assess the effectiveness of treatment modalities for radiation-induced trismus in improving mouth opening (MO) and oral health–related quality of life (OHRQoL), with considering of treatment timing and patient adherence.
Methods: Electronic databases (PubMed, Google Scholar, Scopus, EBSCOhost, and ScienceDirect) were searched for studies published between 2015 and 2025 using relevant Medical Subject Headings (MeSH) combined with Boolean operators, including “Treatment OR therapy AND trismus OR limited mouth opening AND radiation therapy OR radiotherapy AND head and neck neoplasm OR head and neck cancer” and “Timing OR starting time AND treatment OR exercise AND trismus OR limited mouth opening OR restricted mouth opening.” After duplicate removal, titles, abstracts, and full texts were screened for eligibility.
Results: The initial search identified 472,480 articles, of which 18 met the inclusion criteria after screening titles, abstracts, and full texts. Kruskal–Wallis analysis demonstrated significantly greater improvement in mouth opening when trismus treatment was initiated during or after radiotherapy compared to before radiotherapy (p = 0.020). The greatest improvement was observed with combined laser therapy and Therabite exercises, initiated concurrently with radiotherapy for 3 months with high adherence, resulting in a mean increase of 26.95 mm in MO and an improvement in OHRQoL. The second most effective modality was threaded tapered screw appliance (TTSA) therapy combined with low-level laser therapy (LLLT) administered post-radiotherapy for 6 weeks, yielding a 15 mm improvement with high adherence.
Conclusion: The effectiveness of treatment for radiation-induced trismus is influenced by the therapeutic modality, timing of therapy initiation, and patient adherence, all of which contribute to improvements in MO and OHRQoL. Combination therapy modalities, particularly laser therapy combined with jaw movement devices, initiated during or after radiotherapy and supported by high patient adherence, optimize mouth opening and enhance OHR-QoL.
Keywords: adherence, mouth opening, oral health–related quality of life, radiation therapy, treatment modalities, trismus
Introduction
Trismus is characterized by a reduction in maximal interincisal opening (MIO). Individuals with trismus exhibit a mouth opening of less than 35 mm, measured measured as the interincisal distance between the maxillary and mandibular anterior incisors, or less than 40 mm, measured from the interalveolar ridge distance.1,2 Trismus is classified as mild (25 to 35 mm), moderate (16 to 25 mm), or severe (15mm or less interincisally).3 Limited mouth opening may result from various factors, including complications following wisdom tooth extraction, physical trauma or post-accident injuries, tetanus infections, malignancies, and temporomandibular-joint disorders that cause inflammation and structural damage.4 Additionally, trismus may develop in head and neck cancer (HNC) patients due to tumor proximity to the masticatory apparatus or as a consequence of radiation therapy (RT) with or without concurrent chemotherapy (ChT) or surgery in the head and neck region.5
Radiation-induced inflammation results from endothelial injury, hypoxia, and fibrosis. Radiation-induced cell damage in irradiated tissues results from double-strand DNA damage and the generation of reactive oxygen species. Enzymes released during tissue injury further increase oxidative stress, leading to tissue ischemia and vascular thrombosis. These processes intensify local tissue damage and stimulate the production of inflammatory cytokines and chemokines. The resulting inflammatory response typically leads to hypoxia and irreversible radiation-induced fibrosis of the masticatory apparatus, ultimately resulting in radiation-induced trismus (RIT).6
The incidence of post-radiation trismus in HNC patients averages 69%. Trismus typically occurs 3–4 months after radiation therapy and peaks at six months. Patients with trismus not only experience limited mouth opening but also reduced jaw movement, pain, and stiffness or tension in the masticatory muscles.6–8 These limitations adversely affect chewing, phonation, jaw function, and overall oral health-related quality of life (OHRQoL). Oral health-related quality of life has a substantial impact on daily functional activities as well as the psychosocial well-being of patients. The severity of functional limitations is subjectively perceived, and the associated psychosocial impact largely depends on individual patient perception.1,9,10
Many therapies have been carried out to overcome post-radiation trismus with or without chemotherapy or surgery in head and neck cancer patients, including mouth-opening exercises and jaw range-of-motion exercises.11–13 However, few syntheses provide a detailed overview of this topic.14,15 To address this gap, this review study aims to investigate and synthesize studies on whether mouth opening therapy is effective in terms of modality of treatment, the initial time of trismus therapy, adherence, and its effect on improving mouth opening related to the patient’s oral health-related quality of life.
Materials and Methods
Data Sources and Electronic Search
We used five electronic databases to identify studies (PubMed (United States National Library of Medicine), Google Scholar, Scopus, EbscoHost, and ScienceDirect) from January 2015 to December 2025. Several Medical Subject Headings combined into Boolean MeSH into search strategies are “Treatment or therapy and Trismus or limited mouth opening and Radiation therapy or Radiotherapy or Head and neck neoplasm or head and neck cancer” and “Timing or starting time and treatment or exercise and trismus or limited mouth opening or restricted mouth opening.” As a guide for the search strategy, the following Population, Intervention, Comparison/Control, and Outcomes (PICO) criteria were addressed. Population: individuals with head and neck cancer currently or already undergoing radiation with/without chemo and/or surgery therapy; Intervention: trismus treatment; Comparison/Control: No trismus treatment/usual care/no structured treatment; Outcomes: improving mouth opening related to the patient’s oral health-related quality of life.
Data Collection and Selection Techniques
Initially, all authors selected titles and abstracts that could potentially meet the inclusion criteria. The inclusion criteria included published academic articles; publications from 2015 to 2025; cross-sectional, randomized controlled, and prospective study designs; and studies involving radiation therapy in the head and neck region, with or without chemotherapy and/or surgical treatment. The exclusion criteria included non-open-access articles, non-English publications, studies focusing on single surgical or chemotherapy interventions, post-radiation therapy complications other than trismus, studies without instruments for measuring quality of life, and animals or plant studies.
Statistical Analysis
The statistical test used in this study was descriptive statistics, followed by the Shapiro–Wilk normality test. Then, the Kruskal–Wallis test was used to determine differences in mouth-opening progress between studies at the initial time point (before, during, and after radiation therapy).
A descriptive ranking was conducted to identify the most effective therapy modality for achieving optimal mouth opening across studies.
Results
Study Selection
After removing duplicate articles, excluding those that did not meet the inclusion criteria, selecting the abstracts, and reading the entire contents, the articles were filtered. A total of 472,480 titles were found by electronic searches of the databases (PubMed, Google Scholar, Scopus, Ebsco Host, and Science Direct). Following the removal of articles that did not meet the inclusion criteria and had the same title, 106 relevant articles were found through a rapid title-based search. A total of 64 publications were retrieved following a brief abstract-based search. Furthermore, continuing the search using the full-text articles, 18 articles met the criteria and were approved by all reviewers. The process of selecting studies is displayed in Figure 1.
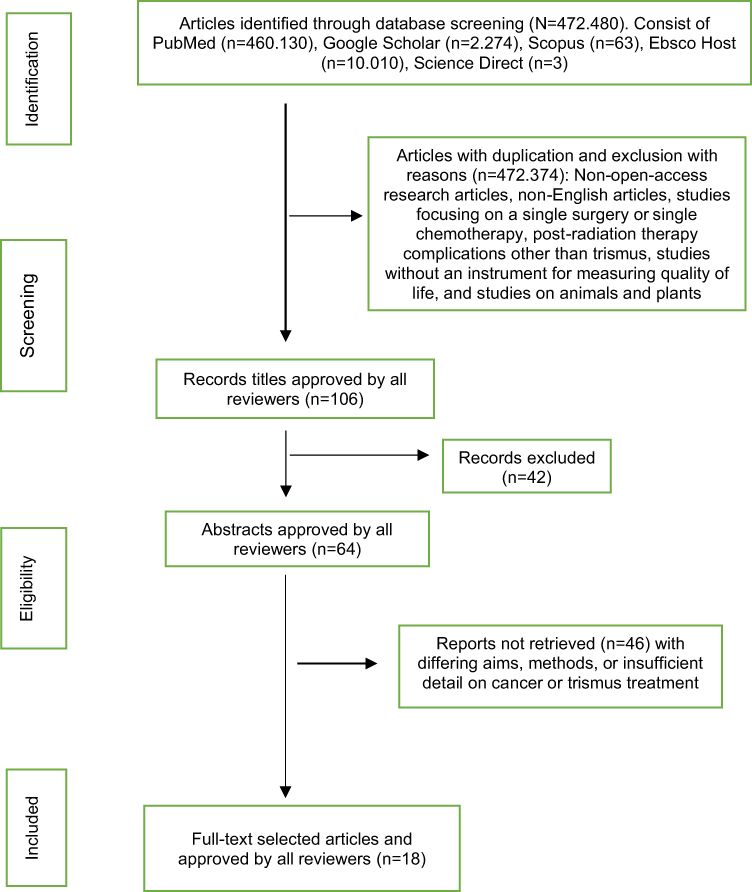 |
Figure 1 The process of selecting studies. |
Table 1 summarizes the extracted study characteristics, including study design, sample size, age, sex, and cancer treatment. The included studies comprised three randomized controlled trials (RCTs); one randomized, open-label, controlled, three-centre feasibility study; eight prospective studies; one pilot randomized controlled experimental study; one single-arm clinical trial; one prospective single-arm cohort feasibility study; one prospective RCT; one randomized, controlled, double-blind, three-arm, parallel-group prevention clinical trial; and one quasi-experimental study.
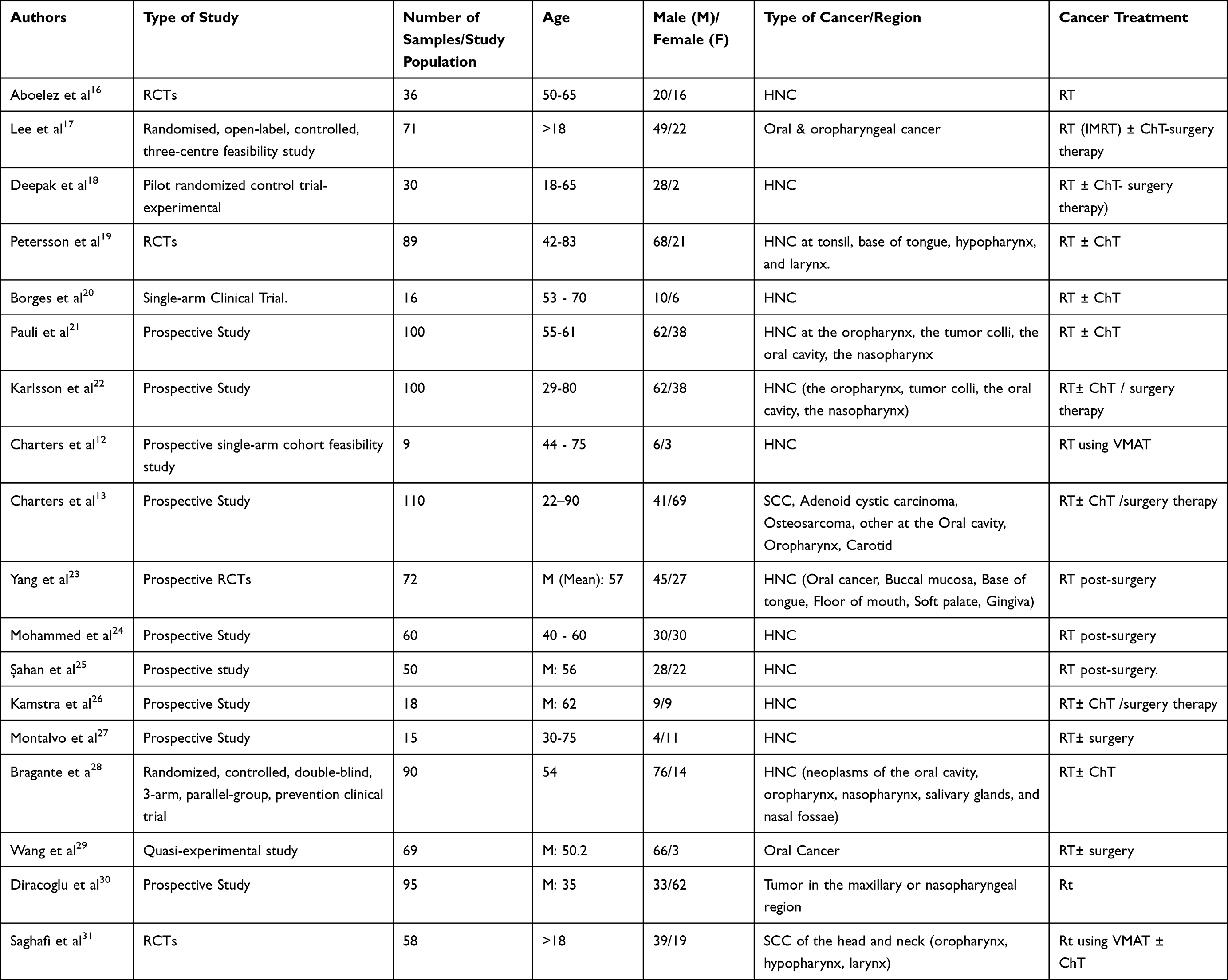 |
Table 1 Characteristics of the Included Studies (N= 18) |
The total sample size across the included studies was 1,088 participants aged 18 years or older, comprising 676 males and 412 females. Tumor sites included the oral cavity, pharynx, oropharynx, nasopharynx, floor of mouth, hypopharynx, tonsil, tongue, buccal mucosa, mandible, maxilla, and salivary glands. Cancer treatments included radiotherapy (RT), delivered using conventional techniques, intensity-modulated radiation therapy (IMRT), or volumetric modulated arc therapy (VMAT), with or without chemotherapy (ChT) and/or surgical intervention.
The overall risk of bias assessment included seven randomized controlled trials (RCTs) evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool (Table 2) and eleven non-randomized studies assessed using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool (Table 3). The RoB 2 assessment indicated that five studies had some concerns, while two studies were judged to have a low risk of bias. In contrast, the ROBINS-I assessment showed that all eleven non-randomized studies were at serious risk of bias.
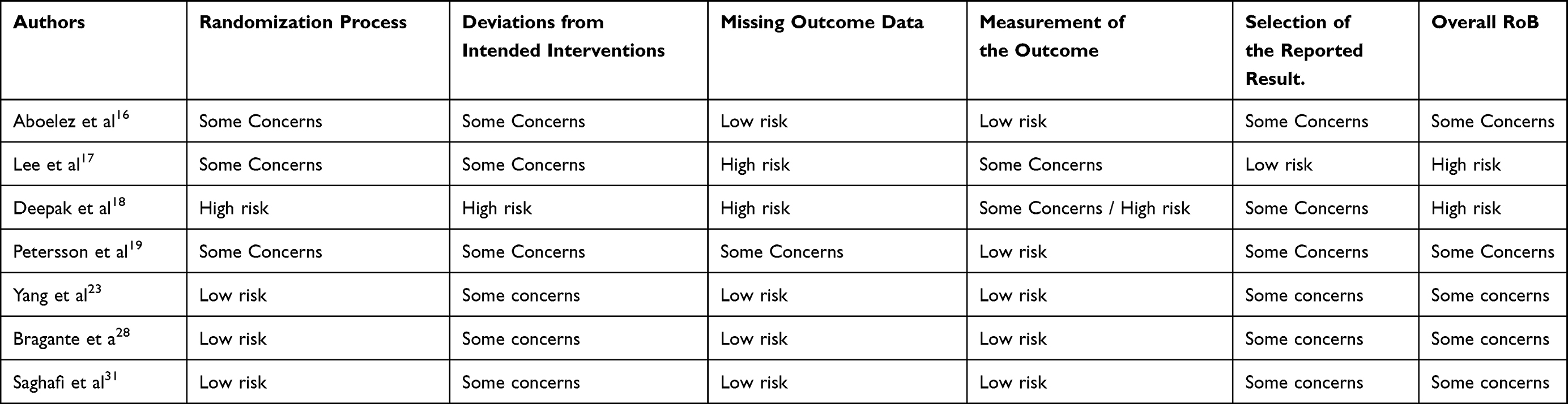 |
Table 2 Overall Risk of Bias Assessment for Randomized Controlled Trials (RoB 2; n = 7) |
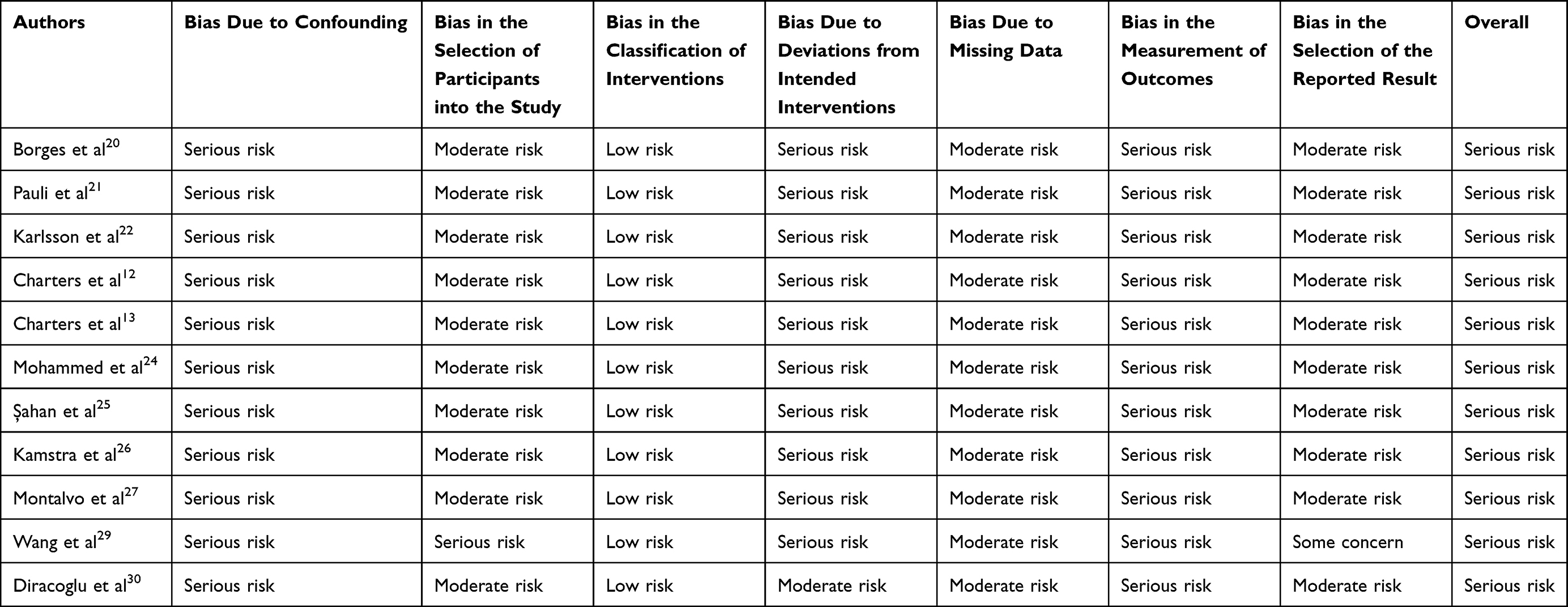 |
Table 3 Overall Risk of Bias Assessment for Non-Randomized Studies (ROBINS-I; n = 11) |
Table 4 displays the extracted data, including the initial time of treatment for trismus, duration, modalities, progress on MIO, level of adherence, and oral health-related quality of life. The treatment of trismus consists of active jaw movement, passive jaw movement (using a device), and a combination of active and passive jaw movement.
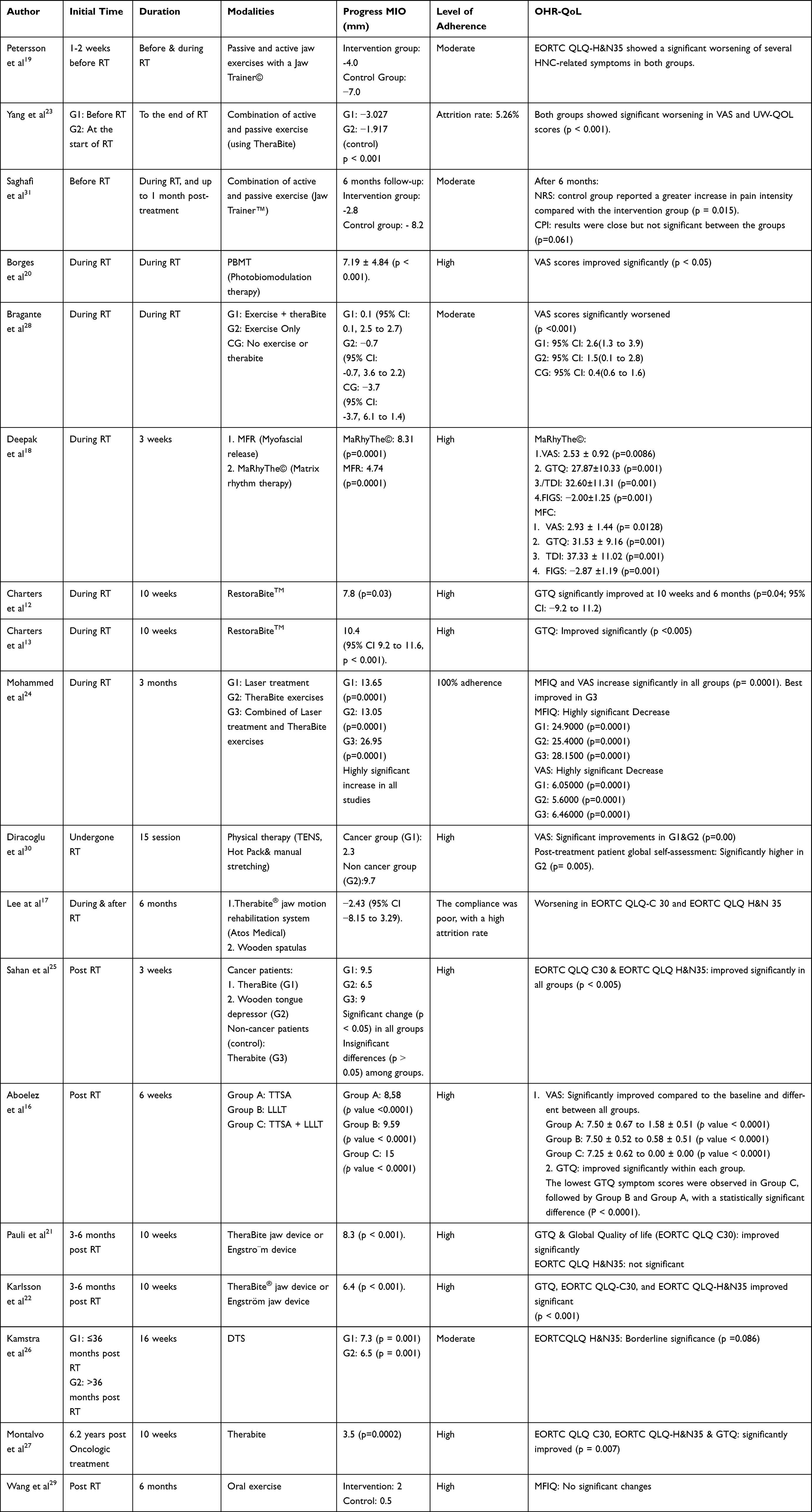 |
Table 4 Characteristics of the Trismus Treatments |
Active jaw movement interventions included myofascial release (MFR; n = 1), Matrix Rhythm Therapy (MaRhyThe®; n = 1), and oral exercises (n = 2). Passive jaw movement interventions included the TheraBite® jaw motion rehabilitation system or Engström device (n = 2), TheraBite® jaw motion rehabilitation system (n = 5), wooden spatulas or wooden tongue depressors (n = 2), threaded tapered screw appliance therapy (TTSA; n = 1), low-level laser therapy (LLLT; n = 1), photobiomodulation therapy (PBMT; n = 1), RestoraBite™ (n = 2), laser therapy (n = 1), and the Dynasplint Trismus System (DTS; n = 1).
The combination exercise included passive and active jaw exercises with a Jaw Trainer© (n=2); a combination of active and passive exercise using theraBite (n=1); combination of physical therapy using transcutaneous electrical nerve stimulation (TENS), hot pack dan manual stretching (n=1), combined of TTSA and LLLT (n=1), combination of laser therapy and theraBite exercises (n=1).
The timing of trismus therapy varied, with interventions initiated before radiotherapy (n = 3), during radiotherapy (n = 8), and after radiotherapy (n = 7). The duration of treatment ranged from 3 to 24 weeks. Compliance levels varied from high (n = 12) to moderate (n = 5) and low (n = 1). Regarding changes in mouth opening following treatment, an increase was reported in 21 studies, whereas a decrease was observed in 5 studies.
Several instruments used in the included studies assessed oral health–related quality of life (OHRQoL), either directly or indirectly. These instruments included the Visual Analogue Scale (VAS), Numerical Rating Scale (NRS) for pain, Composite Pain Index (CPI), Gothenburg Trismus Questionnaire (GTQ), European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), EORTC Quality of Life Questionnaire–Head and Neck 35 (EORTC QLQ-H&N35), Temporomandibular Joint Disability Index (TDI), Functional Intraoral Glasgow Scale (FIGS), Functional Assessment of Cancer Therapy–Head and Neck (FACT-H&N), Global Quality of Life (GQL), Mandibular Function Impairment Questionnaire (MFIQ), and University of Washington Quality of Life questionnaire (UW-QOL). The scores obtained from these instruments indicated improvement (n = 11), no significant change (n = 1), worsening (n = 5), and borderline outcomes (n = 1).
To evaluate changes in mouth opening according to the timing of trismus therapy, descriptive statistical analyses were performed (Table 5), followed by the Shapiro–Wilk normality test. Descriptive statistics showed that the mean change in mouth opening during radiotherapy (M = 7.61 ± SD 8.04) and after radiotherapy–based trismus therapy (M = 7.71 ± SD 3.38) was greater than that observed in pre-radiotherapy trismus therapy (M = −3.28 ± SD 0.64). The Shapiro–Wilk test indicated that changes in mouth opening across the three treatment time points (before, during, and after radiotherapy) were normally distributed (p > 0.05).
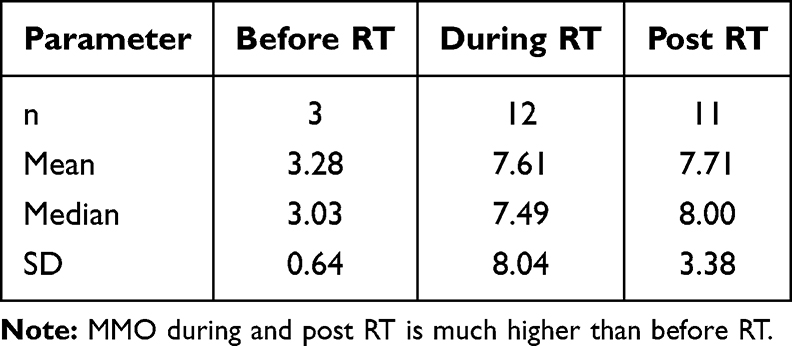 |
Table 5 Descriptive Statistics of Maximum Mouth Opening (MMO) (Mm) |
However, because the sample sizes across groups were unbalanced and the data were derived from different studies rather than longitudinal measurements within the same subjects, a nonparametric independent Kruskal–Wallis test was used to compare changes in mouth opening across time points. The results demonstrated a significant difference among the groups before radiotherapy, during radiotherapy, and after radiotherapy (H = 3.00, p = 0.020).
To identify the therapy modalities associated with the greatest improvements in mouth opening across studies, a descriptive ranking analysis was performed (Table 6). Based on the available data, the combination of laser therapy and TheraBite® exercises, initiated concurrently with radiotherapy for a duration of three months, was associated with the largest improvement in mouth opening (26.95 mm) and improvements in oral health–related quality of life (OHRQoL). The next highest-ranked modality was the combination of threaded tapered screw appliance therapy (TTSA) and low-level laser therapy (LLLT), administered after radiotherapy for six weeks, which resulted in a 15 mm improvement in mouth opening and improvements in OHRQoL.
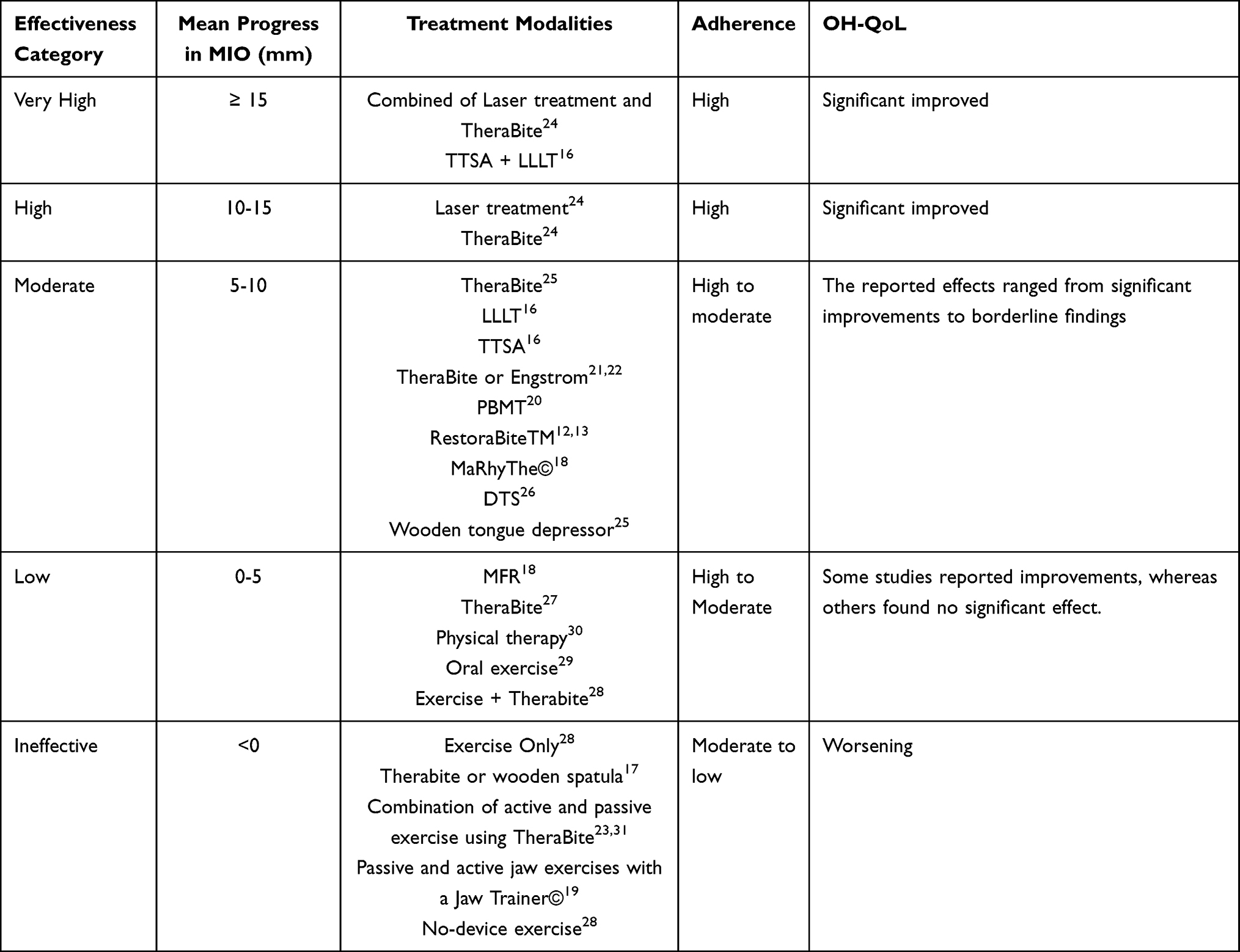 |
Table 6 Categories of Treatment Modalities Based on Clinical Effectiveness |
Discussion
Radiation-induced fibrosis results from the activation and dysregulation of fibroblastic activity, leading to tissue atrophy in the irradiated region. This is referred to as the fibroatrophic theory of radiation damage. This phenomenon involves transforming growth factor beta1 (TGF-β1), a key cytokine that regulates fibroblast proliferation and differentiation. Differentiated fibroblasts synthesize collagen and proteoglycans in the extracellular matrix. Radiation induces overexpression of TGF-β1, likely caused by oxidative stress and an inflammatory response. Elevated serum levels of TGF-β1 correlate with an increased risk of fibrosis in cancer patients. Progressive fibrosis leads to excessive collagen deposition and extracellular matrix accumulation, resulting in tissue stiffness and scar formation in the masticatory muscles and tissues surrounding the temporomandibular joint, thereby contributing to trismus.32
Radiation-induced trismus (RIT) significantly impairs daily activities and key oral functions. These include speech, eating, drinking, and oral hygiene. RIT is also linked to psychological distress, malnutrition, and dehydration, which reduce oral health-related quality of life (OHRQoL).9 Currently, there is no consensus on the best management for trismus related to head and neck cancer (HNC) patients.33 Studies in this paper used different treatment types, starting times, and durations for trismus. While all aimed to improve mouth-opening and oral health-related quality of life, they produced varied results.
Purkayastha et al,34 stated that before RIT appears, acute side effects as edema, inflammation, and muscular spasms may occur during or right after RT. Long-term effects, including fibrosis and scarring, may potentially arise, depending on the dose and fractionation schedule used. However, Somay et al,35 stated that there is no consensus on the appropriate timing for initiating trismus therapy before RT or CRT.
This study found that the increase in mouth opening was greater in the group that underwent trismus therapy during and after radiotherapy. Variation in mouth opening improvement was influenced by treatment modalities and patient compliance. Factors influencing patient compliance include motivation, treatment protocol, acute reaction to radiation, overlapping exercise schedules with radiation therapy, cancer stage affecting systemic health, and the combined effects of chemotherapy and radiation, which can exacerbate trismus.
Reduced mouth opening adversely affects patients’ quality of life, as reflected by poor scores on the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck Module (EORTC QLQ-H&N35). In this study, preventive exercises did not demonstrate significant effects on mouth opening between the intervention and control groups. These findings are consistent with those of Hogdal N et al,36 and Saghafi et al,31 who also reported no significant benefits of early exercise interventions for preventing trismus following radiotherapy for head and neck cancer (HNC) patients when adherence was moderate, and combination therapy was used. Preventive mouth-opening exercises performed before radiotherapy may not demonstrate a significant therapeutic effect on mouth opening because radiation-induced trismus primarily results from progressive fibrosis that develops during and after radiation exposure. Although pre-radiation exercises may improve baseline muscle flexibility, they do not prevent the subsequent fibrotic remodeling of the masticatory muscles, connective tissues, and periarticular structures of the temporomandibular joint induced by radiation. Consequently, the structural and biochemical changes caused by radiotherapy may override any initial functional gains achieved through pre-treatment exercises, resulting in no significant improvement in post-radiation mouth opening.
A recent study showed a significant increase in mouth opening at the initial time during and after radiation therapy, and using a combination of modalities for trismus treatment. This was observed in patients receiving laser therapy combined with TheraBite exercises, and in those treated with TTSA plus LLLT. Their training lasted 6–24 weeks, with a significant increase in the average maximum interincisal opening (MIO) of 26.95 mm and 15 mm. Treatment for trismus began during and after radiation therapy. All participants completed the practice session and showed improved quality of life, evidenced by higher VAS, MFIQ, and GTQ scores.16 Factors such as patient motivation and treatment adherence may have contributed to their results, and the patients were not in a state of acute pain.
Combination therapy using laser therapy and a jaw mobilization device was associated with greater improvements than either modality alone. Laser therapy offers several benefits, including biostimulation and analgesia without increasing temperature. It also promotes vasodilation, reduces edema, increases cellular metabolism, changes cell membrane structure to enhance pain threshold, and shortens wound-healing time. In this study, a diode laser with a peak output of 500 mW and a wavelength of 810 nm was used. The application lasted 2 minutes, twice weekly, targeting the pterygoid, masseter, and temporal muscles.37
Low-level laser therapy (LLLT) is generally well tolerated and acceptable to patients. It is cost-effective, noninvasive, painless, safe, and well-tolerated. The procedure is rapid and needs minimal dental chair time. Laser supports tissue healing by reducing pain, swelling, and inflammation without side effects. Its effect on soft-tissue trauma pain stems from its indirect reduction of edema, bleeding, neutrophil activity, pro-inflammatory cytokines, and enzyme activity. LLLT minimizes swelling and pain and supports tissue repair by speeding up lymphatic vessel regeneration and limiting vascular permeability.37
The patient’s strength and motivation influence the applied force.38 TTSA targets the depressor muscle group. The smaller end is inserted between the premolars. The handle is rotated clockwise two or three times daily. This approach increases maximum mouth opening and restores normal function, likely because both therapies promote vasodilation. The combination of TTSA and LLLT resulted in the most favorable health-related quality-of-life outcomes (P < 0.0001).16 These results match those of Zecha et al,39 and Geethu et al,40 who also found LLLT and TTSA highly beneficial after HNC chemotherapy and radiation therapy.
The TheraBite device was employed to facilitate jaw mobilization. It features a mandibular mouthpiece that lowers appropriately when the handle is pressed. Force is distributed to protect the teeth through large mouthpieces equipped with foam cushions. A precision-adjusting screw enables slow opening and accurate positioning. During the stretching procedure, a C-shaped hand aid assists the patient or caregiver in maintaining finger extension. The protocol consisted of 10 consecutive sets of stretches, each lasting 30 seconds, with brief rest intervals between sets. The TheraBite Jaw Motion Rehabilitation System is based on the principle of passive movement and is specifically designed for patients with mandibular hypomobility and restricted mouth opening. The primary objective is to enhance jaw strength and increase the range of motion by restoring mobility and flexibility to the jaw muscles, joints, and connective tissues through repeated passive motion and stretching. Combining low-level laser therapy (LLLT) with TheraBite exercises offers a promising approach for improving mandibular mobility and reducing pain in head and neck cancer patients experiencing trismus.24
This study found that the optimal increase in mouth opening was observed in the group with high therapy compliance.16,24 These findings are consistent with those of Charters et al,41 who reported that adherence to the exercise program was associated with greater improvement in maximum interincisal opening.
The quality-of-life assessments across these studies found that the group with optimal mouth-opening improvement also had optimal quality-of-life improvement. These results are in line with Montalvo et al,27 who reported that increased mouth opening is associated with improved quality of life. The greater the improvement in mouth opening, the greater the improvement in quality of life.
In general, the heterogeneity identified across studies includes patients’ compliance, oncologic treatment, trismus treatment, and unequal initial treatment time and treatment duration. Motivation, health conditions, cancer staging, treatment protocols, and exercise schedules influence patients’ compliance. Attrition rates during the study will affect the significance of the study results.42,43
Oncology treatment affects the risk of trismus. Patients treated with combined radiation, chemotherapy, and/or surgery face more limitations in mouth opening than those treated with radiation alone.44 Furthermore, radiotherapy delivered using intensity-modulated radiotherapy (IMRT) is associated with a lower incidence of trismus compared with conventional techniques.5,14,45 Differences in modalities, techniques, exercise duration, and intensity across studies lead to substantial heterogeneity in results. Unequal initial treatment time and treatment duration may also affect conclusions regarding the effectiveness or safety of the intervention.
A major limitation of the present study was the high heterogeneity among the included studies. Future research should aim to improve study homogeneity by applying more standardized study designs, intervention protocols, and outcome measures.
Conclusion
The effectiveness of treatment for radiation-induced trismus is influenced by therapeutic modality, timing of therapy initiation, and patient adherence, all of which contribute to improvements in mouth opening and oral health–related quality of life. Combination therapies, particularly laser therapy combined with jaw movement devices initiated during or after radiotherapy and supported by high patient adherence, optimize mouth opening and enhance oral health–related quality of life.
Acknowledgments
The authors would like to acknowledge Universitas Padjadjaran and the EQUITY Program for administrative and technical support during the conduct of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The publication costs of this article were funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (Lembaga Dana Abadi Pendidikan, LPDP), under the Ministry of Higher Education, Science, and Technology of the Republic of Indonesia, and managed through the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Disclosure
There are no competing interests to declare.
References
1. Aghajanzadeh S, Karlsson T, Tuomi L, Engström M, Finizia C. Trismus, health-related quality of life, and trismus-related symptoms up to 5 years post-radiotherapy for head and neck cancer treated between 2007 and 2012. Support Care Cancer. 2023;31(3):1–16. doi:10.1007/s00520-023-07605-w
2. Abd-zaid AT, Ali DKA, Al-fahham AA. Assessment of trismus among patients with head and neck cancer. Kufa J Nurs Sci. 2023;13(2):7–16.
3. McMillan H, Barbon CEA, Cardoso R, et al. Manual therapy for patients with radiation-associated trismus after head and neck cancer. JAMA Otolaryngol - Head Neck Surg. 2022;148(5):418–425. doi:10.1001/jamaoto.2022.0082
4. Somay E, Yilmaz B, Kucuk A, Topkan E. A comprehensive review of the pros and cons of definitions of radiation-induced trismus. J Adv Med Med Res. 2022;34(22):255–266. doi:10.9734/jammr/2022/v34i2231599
5. Meidarlina I, Kusumadjati A. Head and neck cancer patients’ radiation-induced oral and temporomandibular joint complications: a review. J Int Oral Heal. 2024;16(6):432–438. doi:10.4103/jioh.jioh_46_24
6. Somay E, Yilmaz B, Topkan E, Kucuk A, Pehlivan B, Selek U. Definitions of radiation-induced trismus in head and neck cancer: current concepts and controversies. Adv Cancer Res. 2023;(10):23–40.
7. Pauli N, Mejersjö C, Fagerberg-Mohlin B, Finizia C. Temporomandibular disorder in head and neck cancer patients undergoing radiotherapy: clinical findings and patient-reported symptoms. Head Neck. 2019;41(10):3570–3576. doi:10.1002/hed.25878
8. Kamstra JI, Dijkstra PU, Van Leeuwen M, Roodenburg JLN, Langendijk JA. Mouth opening in patients irradiated for head and neck cancer: a prospective repeated measures study. Oral Oncol. 2015;51(5):548–555. doi:10.1016/j.oraloncology.2015.01.016
9. Somay E, Yilmaz B, Kucuk A, Topkan E. Impact of radiation-induced trismus on patients’ life quality. Arch Curr Res Int. 2022;22(5):12–24. doi:10.9734/acri/2022/v22i530288
10. Aghajanzadeh S, Karlsson T, Tuomi L, Engström M, Finizia C. Facial pain, health-related quality of life and trismus-related symptoms up to 5 years post-radiotherapy for head and neck cancer. Support Care Cancer. 2023;31(12). doi:10.1007/s00520-023-08162-y
11. Lee R, Molassiotis A, Rogers SN, Edwards RT, Ryder D, Slevin N. Protocol for the trismus trial - Therabite versus wooden spatula in the amelioration of trismus in patients with head and neck cancer: randomised pilot study. BMJ Open. 2018;8(3):e021938. doi:10.1136/bmjopen-2018-021938
12. Charters E, Loy J, Wu R, et al. Pilot study of intensive trismus intervention using restorabiteTM during unilateral adjuvant radiation for head and neck cancer. Dysphagia. 2024;39(5):864–871. doi:10.1007/s00455-024-10668-4
13. Charters E, Cheng K, Dunn M, et al. RestorabiteTM: Phase II trial of jaw stretching exercises using a novel device for patients with trismus following head and neck cancer. Int, J, Cancer. 2024;155(4):731–741. doi:10.1002/ijc.34941
14. Bensadoun RJ, Riesenbeck D, Lockhart PB, Elting LS, Spijkervet FKL, Brennan MT. A systematic review of trismus induced by cancer therapies in head and neck cancer patients. Support Care Cancer. 2010;18(8):1033–1038. doi:10.1007/s00520-010-0847-4
15. Chee S, Byrnes YM, Chorath KT, Rajasekaran K, Deng J. Interventions for trismus in head and neck cancer patients: a systematic review of randomized controlled trials. Integr Cancer Ther. 2021;20:1–12. doi:10.1177/15347354211006474
16. Aboelez MA, Ibrahim AM, ElSawy MA, El-Khamisy NES. Efficiency of different treatment modalities on radiation induced trismus for maxillofacial cases: a parallel randomized clinical trial. BMC Oral Health. 2025;25(332):1–12. doi:10.1186/s12903-025-05600-7
17. Lee R, Yeo ST, Rogers SN, et al. Randomised feasibility study to compare the use of Therabite® with wooden spatulas to relieve and prevent trismus in patients with cancer of the head and neck. Br J Oral Maxillofac Surg. 2018;56(4):283–291. doi:10.1016/j.bjoms.2018.02.012
18. Deepak R, Tanna BR, Pattanshetty A. Efficacy of matrix rhythm therapy (MaRhyThe©) over conventional therapy on radiation-induced trismus‑A pilot randomised control trial. J Cancer Res Ther. 2023;20(1):118–125. doi:10.4103/jcrt.jcrt_1198_22
19. Petersson K, Finizia C, Pauli N, Tuomi L. Preventing radiation-induced dysphagia and trismus in head and neck cancer—A randomized controlled trial. Head Neck. 2025;47(1):159–174. doi:10.1002/hed.27886
20. Borges MMF, Malta CEN, Carlos ACAM, et al. Photobiomodulation therapy in the treatment of radiotherapy-related trismus of the head and neck. Lasers Med Sci. 2023;38(1):1–13. doi:10.1007/s10103-023-03920-0
21. Pauli N, Svensson U, Karlsson T, Finizia C. Exercise intervention for the treatment of trismus in head and neck cancer – a prospective two-year follow-up study. Acta Oncol. 2016;55(6):686–692. doi:10.3109/0284186X.2015.1133928
22. Karlsson O, Karlsson T, Pauli N, Andréll P, Finizia C. Jaw exercise therapy for the treatment of trismus in head and neck Cancer: a prospective three-year follow-up study. Support Care Cancer. 2021;29(7):3793–3800. doi:10.1007/s00520-020-05517-7
23. Yang L, Hao G, Yang W, Hou L. The impact of different timing of mouth opening exercises on trismus in postoperative radiotherapy patients with oral cancer. J Stomatol Oral Maxillofac Surg. 2025;126(3):1–8. doi:10.1016/j.jormas.2024.102104
24. Mohammed SH, Mowafy ZME, El Ghany SA, DA A. Pain and mandibular trismus response to laser therapy and therabite exercise after head and neck cancer surgeries. Ibero-American J Exerc Sport Psychol. 2025;20(5):547–551.
25. Şahan MH, Gökçe B. The evaluation of therabite and wooden tongue depressor in the treatment of trismus and health-related quality of life. Eur Rev Med Pharmacol Sci. 2023;27(4):66–75. doi:10.26355/eurrev_202306_32746
26. Kamstra JI, Reintsema H, Roodenburg JLN, Dijkstra PU. Dynasplint trismus system exercises for trismus secondary to head and neck cancer: a prospective explorative study. Support Care Cancer. 2016;24(8):3315–3323. doi:10.1007/s00520-016-3131-4
27. Montalvo C, Finizia C, Pauli N, Fagerberg-Mohlin B, Andréll P. Impact of exercise with therabite device on trismus and health-related quality of life: a prospective study. Ear Nose Throat J. 2020;96(1):1–6.
28. Bragante KC, Groisman S, Carboni C, et al. Efficacy of exercise therapy during radiotherapy to prevent reduction in mouth opening in patients with head and neck cancer: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;129(1):27–38. doi:10.1016/j.oooo.2019.09.011
29. Wang TJ, Wu KF, Wang HM, Liang SY, Lin TR, Chen YW. Effect of oral exercise on trismus after oral cancer radiotherapy: a quasi-experimental study. Biomedicines. 2022;10(11):1–11. doi:10.3390/biomedicines10112951
30. Dıraçoğlu D, Şen Eİ, Vatansever S, Çapan N, Karan A. Physical therapy in cancer-related vs non-cancer trismus. Stomatologija. 2016;18(4):107–111.
31. Saghafi E, Kadhim K, Andås CA, et al. Jaw exercise in head and neck cancer patients for prevention of temporomandibular disorders: a randomized controlled trial. J Cancer Surviv. 2024. doi:10.1007/s11764-024-01717-w
32. Lyons AJ, Crichton S, Pezier T. Trismus following radiotherapy to the head and neck is likely to have distinct genotype dependent cause. Oral Oncol. 2013;49(9):932–936. doi:10.1016/j.oraloncology.2013.05.009
33. Pauli N, Fagerberg-Mohlin B, Andréll P, Finizia C. Exercise intervention for the treatment of trismus in head and neck cancer. Acta Oncol. 2014;53(4):502–509. doi:10.3109/0284186X.2013.837583
34. Purkayastha A, Sharma N, Sarin A, Bhatnagar S, Chakravarty N. Radiation fibrosis syndrome: the evergreen menace of radiation therapy. Asia-Pacific J Oncol Nurs. 2019;6(3):238–245. doi:10.4103/apjon.apjon_71_18
35. Somay E, Topkan E, Bascil S. Global immune-nutrition-inflammation index as a novel comprehensive biomarker in predicting the radiation-induced trismus rates in locally advanced nasopharyngeal carcinoma patients. Biomol Biomed. 2024;24(6):1703–1710. doi:10.17305/bb.2024.10616
36. Hogdal N, Juhl C, Aadahl M, Gluud C. Early preventive exercises versus usual care does not seem to reduce trismus in patients treated with radiotherapy for cancer in the oral cavity or oropharynx: a randomised clinical trial. Acta Oncol. 2015;54(1):80–87. doi:10.3109/0284186X.2014.954677
37. De Oliveira Chami V, Maracci LM, Tomazoni F, et al. Rapid LLLT protocol for myofascial pain and mouth opening limitation treatment in the clinical practice: an RCT. Cranio - J Craniomandib Pract. 2022;40(4):334–340.
38. Poornima G, Poornima C. Trimus. J Heal Sci Res. 2014;5(December):15–20.
39. Zecha JAEM, Raber-durlacher JE, Nair RG, et al. Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 2: proposed applications and treatment protocols. Support Care Cancer. 2016;24(6):1–22.
40. G RM, Rodrigues SV, V KR. Threaded tapered screw appliance, a cost effective gear for the management of trismus. J Prosthet Implant Dent. 2023;6(3):168–172.
41. Charters E, Loy J, Sharman AR, Cheng K, Dunn M, Clark J. Exercise adherence for patients with trismus after head and neck cancer treatment. Head Neck. 2024;46(11):2717–2724. doi:10.1002/hed.27799
42. Wang YH, Huang YA, Chen IH, Hou WH, Kang YN. Exercise for trismus prevention in patients with head and neck cancer: a network meta-analysis of randomized controlled trials. Healthc. 2022;10(3):1–14.
43. Wang T, Su J, Leung K, Liang S, Wu S, Wang H. European journal of oncology nursing effects of a mouth-opening intervention with remote support on adherence, the maximum interincisal opening, and mandibular function of postoperative oral cancer patients: a randomized clinical trial. Eur J Oncol Nurs. 2019;40:111–119. doi:10.1016/j.ejon.2019.04.001
44. Borges M, Ribeiro R, De MJ, Rebouças L, Costa F. Chemotherapy increases the prevalence of radiotherapy-related trismus in head and neck cancer patients: a systematic review and meta-analysis. J Clin Exp Dent. 2024;16(4):503–515. doi:10.4317/jced.61385
45. Kamal M, Rock C, Grant S, et al. KAH on behalf of the MAH and NCSWG. Dose-volume correlates of the prevalence of patient-reported trismus in long-term survivorship after oropharyngeal IMRT: a cross-sectional dosimetric analysis. Radiother Oncol. 2020;149:142–149. doi:10.1016/j.radonc.2020.04.053
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.