Back to Journals » International Journal of Women's Health » Volume 18
Evaluation of the Efficacy of Systemic Inflammatory Markers in Predicting Medical Treatment Failure in Patients with Tubo-Ovarian Abscess
Authors Akıncı GE, Karacan T, Baykus Y, Tigli A ![]() , Deniz R, Kilic SS
, Deniz R, Kilic SS ![]() , Aydin S
, Aydin S ![]()
Received 3 December 2025
Accepted for publication 4 February 2026
Published 13 February 2026 Volume 2026:18 577360
DOI https://doi.org/10.2147/IJWH.S577360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Güzide Ece Akıncı,1 Tolga Karacan,2 Yakup Baykus,3 Alihan Tigli,3 Rulin Deniz,3 Suleyman Sirri Kilic,4 Suleyman Aydin5
1Department of Obstetrics and Gynecology, Bandırma Training and Research Hospital, Balıkesir, Turkey; 2Department of Obstetrics and Gynecology, Canberra Hospital, Canberra, ACT, Australia; 3Department of Obstetrics and Gynecology, Faculty of Medicine, Bandırma Onyedi Eylül University, Balıkesir, Turkey; 4Samsun Health Practice and Research Center, Department of Infection Diseases, Samsun, Turkey; 5Department of Medical Biochemistry (Firat Hormone Research Group), Faculty of Medicine, Fırat University, Elazığ, Turkey
Correspondence: Suleyman Aydin, Department of Medical Biochemistry (Firat Hormone Research Group), Faculty of Medicine, Fırat University, Elazığ, Turkey, Email [email protected]
Background/Objectives: Tubo-ovarian abscess (TOA), a serious complication of pelvic inflammatory disease, poses a serious risk to sexually active women, characterized by high rates of morbidity and mortality. Despite antibiotic therapy being the primary treatment for non-ruptured, stable TOA cases, failure rates of medical management remain as high as 30%. This study investigates the potential of systemic inflammatory markers, particularly the systemic immune-inflammation index (SII), in predicting the necessity for surgical intervention following the failure of medical treatment in TOA patients.
Methods: A retrospective analysis was conducted on 101 patients diagnosed with TOA at the Bağcılar Training and Research Hospital’s Department of Obstetrics and Gynecology between January 2019 and June 2023. Data collected included demographic details, obstetric history, chronic conditions, clinical history (including intrauterine interventions), and preoperative admission laboratory parameters (CBC, CRP, Neutrophil-to-Lymphocyte Ratio (NLR), and Systemic Immune-Inflammation Index (SII)). Patients were categorized based on treatment outcomes: successful medical treatment versus surgical intervention. A multivariable logistic regression analysis was conducted to assess the predictive value of these markers and to identify independent predictors of medical treatment failure.
Results: The surgical group had significantly higher SII, NLR, and CRP levels compared to the medically managed group. An SII cut-off value of 1750 was a significant predictor of medical treatment failure, with an area under the curve (AUC) of 0.749 (95% CI: 0.649– 0.850), yielding a sensitivity of 73.2% and specificity of 76.7%. Similarly, NLR demonstrated predictive value with a cut-off value of 4.3, achieving an AUC of 0.694 (95% CI: 0.590– 0.798), with 80.5% sensitivity and 58.3% specificity. In the multivariable analysis, SII (OR: 1.002), NLR (OR: 0.706), length of hospital stay (OR: 1.181), and history of curettage (OR: 7.018) were identified as independent predictors of medical treatment failure. Although the mean abscess diameter was larger in the surgical group (64.0 mm vs 57.5 mm), this difference did not reach statistical significance (p=0.079).
Conclusion: Systemic inflammatory markers –particularly, the Systemic Immune-Inflammation Index (SII)– appear to be robust, cost-effective, and readily available tools for predicting medical treatment failure in patients with TOA. Predictive performance is enhanced when SII is interpreted in conjunction with NLR and relevant clinical history, especially prior curettage. Integrating these independent predictors into clinical decision-making may facilitate earlier identification of high-risk patients and expedite escalation to surgical intervention, thereby minimizing delays and improving patient outcomes.
Keywords: tubo-ovarian abscess, systemic immune-inflammation index, surgical treatment, inflammatory markers, pelvic inflammatory disease
Introduction
Pelvic inflammatory disease (PID) encompasses a spectrum of inflammatory disorders of the female upper genital tract, including salpingitis, endometritis, tubo-ovarian abscesses (TOAs), and pelvic peritonitis, predominantly caused by sexually transmitted microorganisms such as N. gonorrhoeae and C. trachomatis. PID has also been linked to several vaginal microorganisms, including anaerobic bacteria, G. vaginalis, Haemophilus influenzae, enteric gram-negative bacteria and Streptococcus agalactiae.1
PID symptoms and indicators can vary significantly, making prompt diagnosis difficult due to the vague nature of the clinical presentation. A full physical examination is usually used to establish the diagnosis, which is further supported by laboratory testing and imaging modalities that confirm the positive results.2 Various inflammatory markers such as C-reactive protein (CRP), white blood cell count (WBC), procalcitonin (PCT), erythtrocyte sedimentation rate (ESR) and systemic immune-inflammation index (SII), frequently correlate with disease severity and are used to diagnose and monitor treatment.3 Although treatment protocols vary, typically Centers for Disease Control and Prevention’s (CDC) recommendations for oral or parenteral antibiotic therapy are followed. The efficiency of the treatment is directly related to the severity of the condition. Failure in treatment can lead to immediate complications such as pain, abscess rupture, and sepsis, and long-term complications might include infertility, chronic pelvic pain, and ectopic pregnancy.4
TOA is defined as an inflammatory mass affecting the adnexa and surrounding pelvic organs, representing a serious complication in approximately 10–15% of PID cases.5 Antibiotic therapy, which constitutes the first line of treatment, has a success rate of about 70%.6 In cases where medical treatment fails, which occurs in 25–30% of instances, abscess drainage is considered for suitable patients, while surgical removal of the abscess and/or surrounding tissue may be necessary.7 There is no consensus on deciding between surgical or medical treatment for patients diagnosed with TOA. Studies have associated the diameter of the abscess with the success of medical treatment, finding significant relationships between abscess sizes greater than 5 cm and medical treatment failure.8 Furthermore, cases of medical treatment failure have been linked with higher WBC counts.9 The use of intrauterine devices (IUDs) remains a contentious issue, with some publications indicating that long-term IUD use can lead to an increase in abscess size and necessitate surgical intervention due to complicated abscess formation related to increased incidence of actinomycosis, whereas other studies have not found a significant need for medical treatment due to IUD use.10,11
The SII, calculated from complete blood count parameters, has emerged as an accessible and cost-effective inflammatory marker. Initially developed by Hu et al in a retrospective study among hepatocellular carcinoma patients between 2005 and 2006, its utility was later validated in a prospective study between 2010 and 2011.12 While SII has primarily been utilized as a prognostic marker in oncological cases, it has also been found to be a significant prognostic marker in inflammatory diseases.13–15 The present study aims to investigate the demographic characteristics and risk factors of patients diagnosed with TOA at our clinic, evaluating the efficacy of the systemic inflammation index calculated from routine laboratory tests and ultrasonography findings in predicting the success of treatment and determining the feasibility of using SII as a decisive parameter in surgical treatment decisions.16–20
Materials and Methods
This investigation was conducted as a retrospective observational analysis, adhering to rigorous ethical standards as dictated by the Health Sciences University Bakırköy Dr. Sadi Konuk Training and Research Hospital Clinical Research Ethics Committee (Ethics Approval No: 2023/248). The study population comprised individuals assessed at Bağcılar Training and Research Hospital’s Gynecology and Obstetrics Clinic from April 2019 to May 2023. Although data collection was performed at Bağcılar Training and Research Hospital, ethical approval was granted by the regional ethics committee of Bakırköy Dr. Sadi Konuk Training and Research Hospital. The study’s commencement was contingent upon the acquisition of ethical clearance, and all procedures were executed in strict compliance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments, or comparable ethical standards.
Participant Recruitment
137 individuals with a diagnosis of TOA were found by a thorough search of the hospital’s database at the start of the recruiting procedure. Following a rigorous screening procedure that comprised predetermined inclusion and exclusion criteria, this initial cohort was lowered to 101 individuals.
The exclusion criteria included: incomplete data sets, pregnancy, abscess sizes exceeding predefined limits, favorable spontaneous pathology results, non-compliance with the treatment protocol, and loss to follow-up.
Several criteria, including the practitioner’s clinical assessment, the patient’s desire, and demographic variables (both patient and practitioner demographics), were used to allocate patients to research arms. The process of decision- making also took into consideration other realistic aspects, such the accessibility of particular treatment alternatives and financial concerns. Despite all efforts to minimize bias, the retrospective design of the study may have left certain confounding factors unaccounted for. Any unmeasured elements that could affect the outcomes and treatment assignment and alter the study’s conclusions are included in here.
To check if the group size of 101 (60 in the medical treatment group and 41 in the surgical treatment group) is sufficient to find statistically significant differences between groups, a power analysis was done. This analysis helps make sure the study has enough strength, so there are fewer chances of making Type II mistakes.
Data Extraction
Retrospective data were extracted from the hospital’s electronic medical records, covering the period from April 2019 to May 2023. Collected variables included demographic characteristics, obstetric history, previous surgical history, pathological findings, and complete blood count parameters obtained upon admission. The SII was calculated using the following formula: SII = (neutrophil count × platelet count) / lymphocyte count.
Statistical Approach
Data were analyzed using SPSS software (version 28.0). The normality of distribution for continuous variables was assessed using the Kolmogorov–Smirnov test. Continuous variables were presented as mean ± standard deviation (SD) or median (minimum-maximum), whereas categorical variables were expressed as frequencies and percentages. Between- group comparisons were performed using the Independent Samples t-test or Mann–Whitney U-test for continuous variables, and the Chi-square test or Fisher’s exact test for categorical variables, as appropriate. To determine the optimal cut-off values for SII and NLR for predicting medical treatment failure, Receiver Operating Characteristic (ROC) curve analysis was performed, and the Youden index (maximum sensitivity + specificity - 1) was calculated. Variables that were statistically significant in univariable analyses were subsequently entered into a multivariable binary logistic regression model to identify independent predictors of treatment failure. Adjusted odds ratios (OR) with 95% confidence intervals (CIs) were calculated. A two-sided p-value of <0.05 was considered statistically significant.
Data Availability Statement
All data that does not identify individuals supporting the study’s results will be available to the public in a repository, with specific access codes given after review and prior to publication, to meet ethical standards of transparency and benefit the scientific community.
The methods used and the ethical standards maintained during the study are detailed in this report, providing a solid basis for reproducibility and verification by the scientific community.
Results
This part explains the important results from retrospective data, highlighting how systemic inflammation markers can help predict the success of medical treatment in patients with TOA.
Patient Demographics and Medical History
The study comprised 60 patients managed with medical therapy and 41 patients who required surgical intervention due to lack of clinical response to antibiotic treatment within 72 hours. The mean age was 39.2 ± 10.5 years in the medical group and 39.2 ± 8.7 years in the surgical group (p>0.05). Diabetes mellitus was observed in 25% of patients in the medical group and 19.5% in the surgical group (p>0.05). No statistically significant differences were identified between the groups with respect to menopausal status or smoking habits (Table 1).
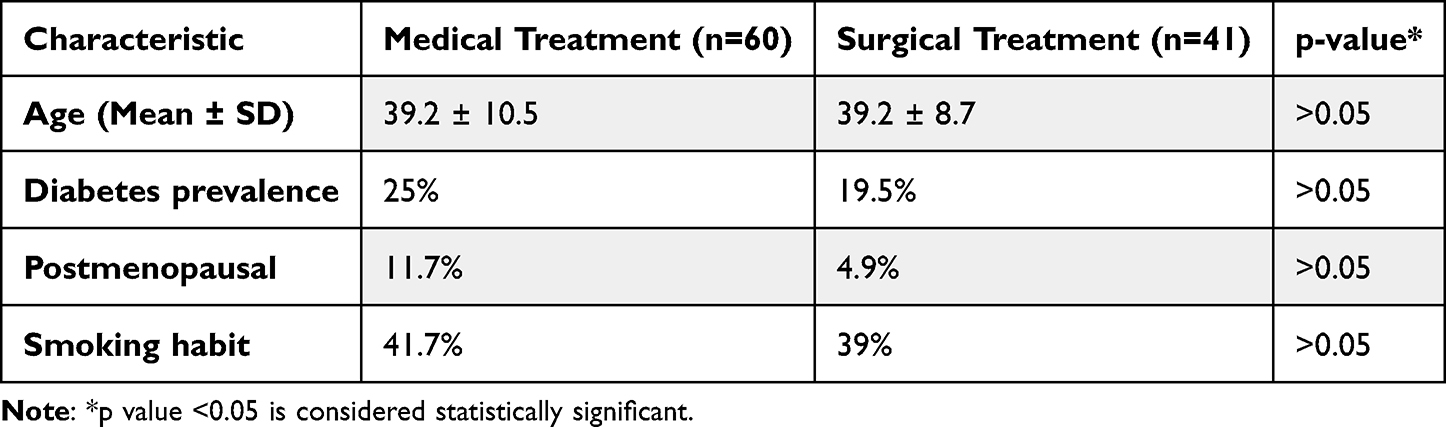 |
Table 1 Descriptive and Clinical Characteristics of Patients by Treatment Outcome |
Obstetric History
Regarding obstetric history, 10.0% of patients in the medical group and 9.8% in the surgical group were nulliparous. The mean number of births was 2.7 ± 2.0 in the medical group and 2.6 ± 1.2 in the surgical group (p>0.05). No significant differences were observed in the rates of vaginal or cesarean deliveries between the groups (Table 2). However, a history of curettage was significantly more frequent in the surgical group (22.0%) compared to the medical group (5.0%) (p=0.010).
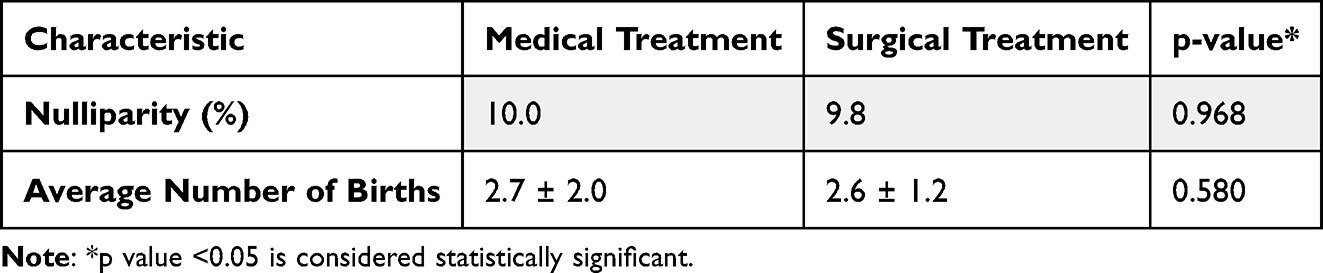 |
Table 2 Obstetric History Comparison |
Inflammatory Markers, Abscess Diameter, and Hospital Stay
Comparisons of clinical and laboratory parameters is summarized in Table 3. The surgical group demonstrated significantly higher inflammatory marker levels than the medical group. Specifically, the mean WBC count was 14,765 ± 5800 /mcL vs 11,300 ± 4600 /mcL (p=0.002), and the mean neutrophil count was 11,928 ± 5100 /mcL vs 8468 ± 4300 /mcL (p<0.001). The mean SII value in the surgical group (3267.1 ± 2501.6) was more than twofold of the medical group (1376.2 ± 903.8) (p<0.001).
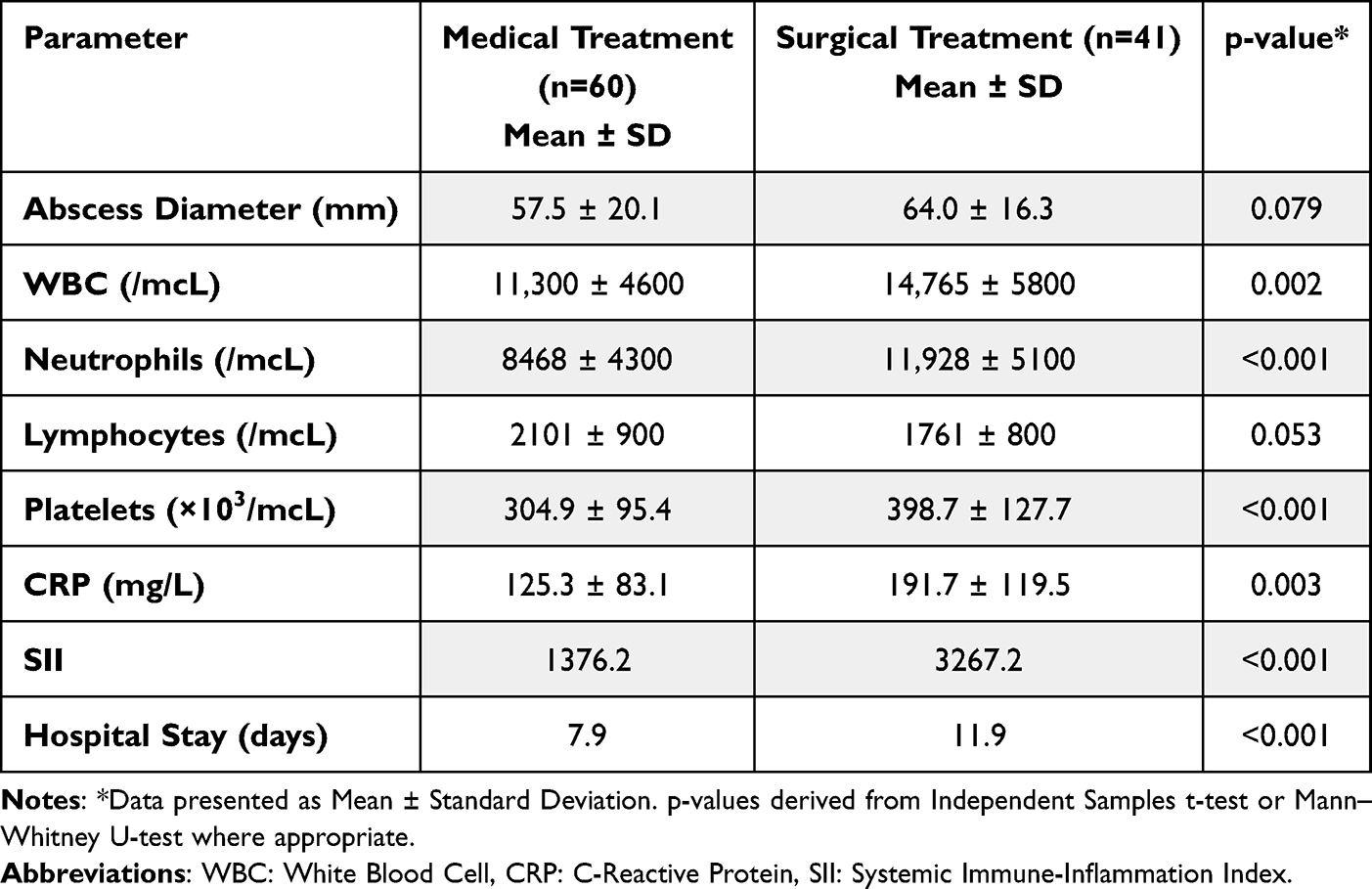 |
Table 3 Comparison of Clinical Characteristics and Inflammatory Markers Between Medical and Surgical Treatment Groups |
Regarding abscess size, the mean ultrasosnographic abscess diameter was larger in the surgical group (64.0 ± 16.3 mm) compared to the medical group (57.5 ± 20.1 mm); however, this difference did not reach statistical significance (p=0.079). The requirement for erythrocyte suspension transfusion was significantly higher in the surgical group (24.4%) compared to the medical group (3.3%) (p=0.001). The length of hospital stay was significantly longer in the surgical group (11.9 ± 5.4 days) compared to the medical treatment group (7.9 ± 3.4 days) (p<0.001).
Among the 41 patients who required surgical intervention, the majority underwent laparoscopic surgery (61.0%), followed by percutaneous drainage (22.0%) and laparotomy (17.1%). Subgroup analysis revealed no statistically significant differences in preoperative SII or NLR levels between patients treated with laparoscopy, laparotomy, or percutaneous drainage (p>0.05).
Predictive Value and Multivariable Analysis
ROC analysis was performed to determine the predictive value of inflammatory markers. For SII, the optimal cut-off value was determined to be 1750 × 109/L using the Youden index. The Area Under the Curve (AUC) for SII was 0.749 (95% CI: 0.649–0.850, p<0.001). At this cut-off, sensitivity was 73.2%, specificity was 76.7%, positive predictive value was 68.2%, and negative predictive value was 80.7%. For NLR, a cut-off value of 4.3 yielded an AUC of 0.694 (95% CI: 0.590–0.798, p=0.001), with 80.5% sensitivity and 58.3% specificity.
Univariate logistic regression analysis indicated that platelet count, neutrophil count, NLR, SII, WBC, CRP, length of hospital stay, history of curettage, and additional antibiotic requirement were significantly associated with medical treatment failure. To identify independent predictors, a multivariable binary logistic regression model was established (Table 4). The analysis identified SII (OR: 1.002, 95% CI: 1.001–1.003, p<0.001), NLR (OR: 0.706, 95% CI: 0.540–0.924, p=0.011), length of hospital stay (OR: 1.181, 95% CI: 1.035–1.348, p=0.014), and history of curettage (OR: 7.018, 95% CI: 1.221–40.345, p=0.029) as independent predictors of medical treatment failure.
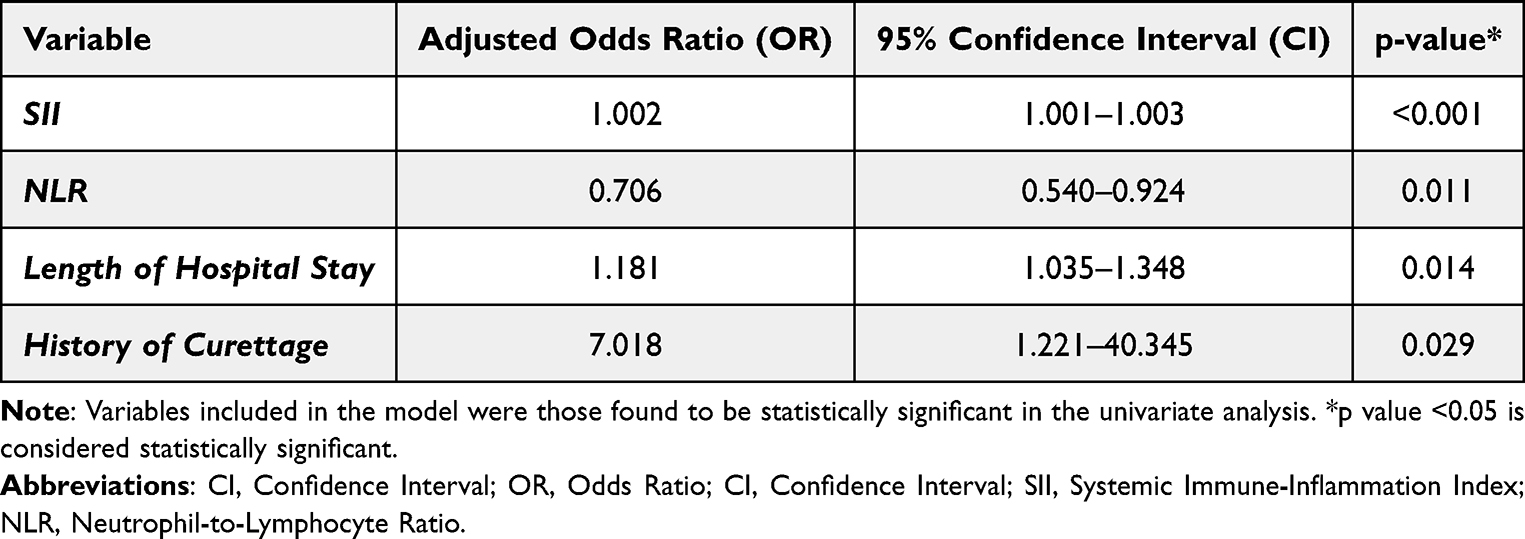 |
Table 4 Multivariable Binary Logistic Regression Analysis Identifying Independent Predictors of Medical Treatment Failure in Patients with TOA |
Discussion
This single-center, retrospective observational study evaluated patients with TOA treated medically or required surgical intervention. The primary objective was to determine whether the SII-a cost-effective and easily applicable inflammatory marker-could predict the need for surgical intervention. Our findings suggest that SII is a strong independent predictor of medical treatment failure in TOA cases.
TOA affects sexually active women and can lead to significant mortality and morbidity if diagnosis and treatment are delayed. Although clinical history, physical examination, laboratory testing, and imaging modalities support diagnosis, selecting between medical and surgical management remains clinically challenging. Delayed surgical intervention can exacerbate adnexal inflammation, increasing the risk of long-term complications such as infertility and chronic pelvic pain.21 Therefore, early identification of patients likely to require surgical treatment is critical.
In our study, the optimal SII cut-off value for predicting failure of medical management was 1750 × 109/L. fAt this threshold, the sensitivity was 73.2% and specificity was 76.7%, with a negative predictive value of 80.7%.22 Management strategies for such infections often relies on established guidelines, such as those from the CDC, which emphasize prompt initiation of appropriate antibiotic therapy.23 However, risk factors vary across populations; for instance, adolescents and young adults carry distinct risks due to behavioral factors.24,25 Although diabetes mellitus has been reported as a risk factor for surgical intervention in prior studies,26,27 we did not observe a significant difference in diabetes prevalence between the medical and surgical groups in our cohort (p>0.05).
Diagnosing and managing TOA entails several clinical challenges, including differentiation from other pelvic pathologies.28 Certain subgroups-particularly postmenopausal women- may present with atypical or nonspecific symptoms, requiring a high index of suspicion to prevent delays in diagnosis and treatment.29 Furthermore, the polymicrobial etiology of TOA, often involving pathogens like Chlamydia trachomatis and Neisseria gonorrhoeae, can contribute to heterogeneous inflammatory responses and complicate clinical assessment.30,31 Understanding the complex mechanisms of abscess formation in these infections is crucial for developing targeted treatment strategies.32
Unlike previous studies that relied solely on univariate comparisons, we performed a multivariable logistic regression analysis to confirm the independent predictive value of inflammatory markers. The analysis revealed that SII (OR: 1.002), NLR (OR: 0.706), length of hospital stay (OR: 1.181), and a history of curettage (OR: 7.018) were independent predictors of medical treatment failure. Notably, the association between prior curretage and a substantially increased risk of treatment failure provides clinically relevant insight and aligns with existing evidence suggesting that intrauterine interventions may predispose to ascending infection. Regarding clinical parameters, abscess size is often cited as a major determinant for surgery. In our cohort, the mean abscess diameter was larger in the surgical group (64.0 mm) than in the medically treated group (57.5 mm); however, this difference did not reach statistical significance (p=0.079). This finding suggests that inflammatory burden -reflected by SII and NLR-may, in some settings, serve as a more sensitive early indicator of resistance to medical therapy than abscess size alone.
Intrauterine interventions pose a known risk for TOA. In our cohort, IUD use was documented in 31.7% of patients successfully managed with medical therapy and in 43.9% of these requiring surgical intervention This finding might reflect the prevalence of IUD use in our patient population, likely due to its provision as a free contraceptive method and its ease of use, suggesting a higher utilization rate compared to other studies.33 IUD use is not only an independent risk factor for TOA but is also associated with actinomyces-associated PID in the literature.34,35 Notably in our sample, seven patients with IUD use exceeding 10 years exhibited a higher rate of medical treatment failure, consistent with prior evidence suggesting that prolonged IUD duration may adversely affect treatment outcomes.36
Compared with single inflammatory markers like WBC count or CRP, integrated indices like SII and NLR offer distinct advantages. SII incorporates three hematologic parameters -neutrophils, platelets, and lymphocytes-reflecting the balance between the systemic inflammatory response and immune regulation. While WBC and CRP are sensitive markers, they are susceptible to elevation in a wide range of non-specific conditions, which may limit their discriminatory value in certain clinical contexts. SII has demonstrated prognostic utility across diverse inflammatory and infectious conditions, as well as malignancies. In line with this evidence, our findings support the clinical relevance of SII in TOA, suggesting that it offers a more integrative and informative reflection of inflammatory status than isolated markers alone. Several limitations of our study should be acknowledged. First, the retrospective design and the non-randomized allocation of treatment based on clinical judgment and patient preference introduce an inherent selection bias. Second, the study was conducted at a single center with a relatively small sample size, which may limit generalizability. Nevertheless, the use of consistent management protocols and the exclusion of important confounders (eg, ruptured abscess at presentation) represent key methodological strengths.
Conclusion
The findings of this study highlight the SII as a robust, accessible, and cost-effective marker for predicting medical treatment failure in patients with TOA. Specifically, an SII cut-off value of 1750 × 109/L demonstrated significant efficacy in differentiating patients who can be managed conservatively from those requiring surgical intervention. Identifying patients above this threshold allows for earlier surgical planning, potentially reducing the risks associated with delayed intervention, such as increased adnexal inflammation and long-term sequelae like infertility or chronic pelvic pain.
Crucially, our study extended beyond the evaluation of single markers; the multivariable analysis demonstrated that alongside SII, the NLR and a history of curettage are independent predictors of medical treatment failure. These findings suggest that TOA management should not rely on a single parameter; rather, it should incorporate a multidimensional assessment that reflects both the inflammatory burden and relevant patient history.
Integrating SII and NLR into baseline risk stratification and preoperative evaluation may enhance the precision of management algorithms and support earlier escalation to surgical intervention in high-risk patients. Although our results underscore the clinical utility of SII and NLR, multicenter studies with larger cohorts are needed to validate these associations and to develop and externally validate integrated predictive models suitable for routine clinical practice.
Institutional Review Board Statement
The study was conducted according to the Declaration of Helsinki and approved by the Institutional Review Board of Health Sciences University Bakırköy Dr. Sadi Konuk Training and Research Hospital (protocol code 2023/248 and date of approval March 5, 2023).
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Workowski KA, Bolan GA. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021. 70:1–9.
2. Peipert JF, Boardman LA, Badger GJ, Allsworth JE, Xu X, Lundsberg LS. Clinical predictors of endometritis in women with symptoms and signs of pelvic inflammatory disease. Am J Obstet Gynecol. 2001;184:856–864. doi:10.1067/mob.2001.113847
3. Vural T, Toğrul C, Işık H, Yıldız Y, Yücesoy I, Vural F. Can the risk factors predicting surgical treatment be determined in patients with tubo-ovarian abscess? Gynecol Obstet Reprod Med. 2022;1–9. doi:10.21613/gorm.2022.1325
4. Kim HY, Lee SJ, Choi JH, et al. Comparison of severe pelvic inflammatory disease, pyosalpinx and tubo-ovarian abscess. J Obstet Gynaecol Res. 2015;41:742–746. doi:10.1111/jog.12617
5. Granberg S, Gjelland K, Ekerhovd E. The management of pelvic abscess. Best Pract Res Clin Obstet Gynaecol. 2009;23:667–678. doi:10.1016/j.bpobgyn.2009.01.010
6. Krivak TC, Cooksey C, Propst AM. Tubo-ovarian abscess: diagnosis, medical and surgical management. Compr Ther. 2004;30:93–100. doi:10.1007/s12019-004-0003-5
7. Gözüküçük M, Yıldız EG. Is it possible to estimate the need for surgical management in patients with a tubo-ovarian abscess at admission? A retrospective long-term analysis. Gynecol Surg. 2021;18:14.
8. Çoşkun B, Şimşir C. Evaluation of risk factors predicting surgical treatment in tuboovarian abscess cases. Med Sci Discov. 2019;6:235–240. doi:10.36472/msd.v6i10.309
9. Hsu C-T, Lai C-H, Ou Y-C, Ho H-C, Su H-Y. Actinomycosis affecting the fallopian tube and ovary: report of 3 cases, with special reference to 2 cases following IUD application. Obstet Gynaecol. 1988;14:275–284.
10. Ersak T, Ersak B, Kokanalı MK. The effect of intrauterine device presence and other factors in medical treatment success of tuboovarian abscess. J Gynecol Obstet Hum Reprod. 2021;50:101983. doi:10.1016/j.jogoh.2020.101983
11. Kapustian V, Namazov A, Yaakov O, Volodarsky, M, Anteby EY, Gemer O. Is intrauterine device a risk factor for failure of conservative management in patients with tubo-ovarian abscess? An observational retrospective study. Arch Gynecol Obstet. 2018;297:1201–1204. doi:10.1007/s00404-018-4690-z
12. Charonis G, Larsson PG. Prolonged use of intrauterine contraceptive device as a risk factor for tubo-ovarian abscess. Acta Obstet Gynecol Scand. 2009;88:680–684. doi:10.1080/00016340902893678
13. Akselim B, Karaşin SS, Demirci A, Üstünyurt E. Can antibiotic treatment failure in tubo-ovarian abscess be predictable? Eur J Obstetrics Gynecol Reprod Biol. 2021;258:253–257. doi:10.1016/j.ejogrb.2021.01.011
14. Greenstein Y, Shah AJ, Vragovic O, et al. Tuboovarian abscess. Factors associated with operative intervention after failed antibiotic therapy. J Reprod Med. 2013;58:101–106.
15. Yongue G, Mollier J, Anin S, et al. Tubo-ovarian abscess: a proposed new scoring system to guide clinical management. Int J Gynecol Obstet. 2022;157:588–597. doi:10.1002/ijgo.13932
16. Göksever Çelik H, Çelik E, Yüksel S, Baştu E, Ark HC. Different surgical techniques in tubo-ovarian abscess management. Gynecol Obstet Reprod Med. 2017;23:32–36. doi:10.21613/GORM.2016.639
17. Alay I, Kaya C, Karaca I, et al. The effectiveness of neutrophil to lymphocyte ratio in prediction of medical treatment failure for tubo-ovarian abscess. J Obstetrics Gynaecol Res. 2019;45:1183–1189. doi:10.1111/jog.13946
18. Protopapas AG, Diakomanolis ES, Milingos SD, et al. Tubo-ovarian abscesses in postmenopausal women: gynecological malignancy until proven otherwise? Eur J Obstetrics Gynecol Reprod Biol. 2004;114:203–209. doi:10.1016/j.ejogrb.2003.10.032
19. Huang H, Liu Q, Zhu L, Zhang Y, Lu X, Wu Y. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci Rep. 2019;9:3284. doi:10.1016/j.ejogrb.2003.10.032
20. Demirtas O, Akman L, Demirtas GS, Hursitoglu BS, Yilmaz H. The role of the serum inflammatory markers for predicting the tubo-ovarian abscess in acute pelvic inflammatory disease: a single-center 5-year experience. Arch Gynecol Obstetrics. 2013;287:519–523. doi:10.1007/s00404-012-2600-3
21. de Carvalho NS, Botelho AB, Mauro D. Sexually transmitted infections, pelvic inflammatory disease, and the role from intrauterine devices: myth or fact? J Biomed Sci. 2017;06:1 doi:10.21767/2254-609X.100047
22. Ribak R, Grisaru D, Bejar R, Cohen A, Raviv O, Klein Z. Can the need for invasive intervention in tubo-ovarian abscess be predicted? The implication of C-reactive protein measurements. J Minimally Invasive Gynecol. 2020;27:541–547. doi:10.1016/j.jmig.2019.04.027
23. Sharma R. To evaluate role of transvaginal sonography over transabdominal sonography in delineating adnexal masses. JK Sci. 2019;21:26–34.
24. Munro K, Gharaibeh A, Nagabushanam S, Martin C. Diagnosis and management of tubo-ovarian abscesses. Obstet Gynaecol. 2018;20:11–19. doi:10.1111/tog.12447
25. Avendaño ALEM, Totomoch Arroyo JA, Villarreal Portillo DA, Moreno MM. Diagnosis and treatment of fitz-hugh-curtis syndrome: review of current literature. Int J Med Sci Clin Res Stud. 2023;03:871–873.
26. Fouks Y, Ziv A, Nativ O, Gidron A, Baniel J, Levin I. Surgical intervention in patients with tubo-ovarian abscess: clinical predictors and a simple risk score. J Minimally Invasive Gynecol. 2019;26:535–543. doi:10.1016/j.jmig.2018.06.013
27. Erenel H, Yilmaz N, Oncul M, et al. Usefulness of serum procalcitonin levels in predicting tubo-ovarian abscess in patients with acute pelvic inflammatory disease. Gynecol Obstetric Investig. 2017;82:262–266. doi:10.1159/000449161
28. Lee SW, Rhim CC, Kim JH, et al. Predictive markers of tubo-ovarian abscess in pelvic inflammatory disease. Gynecol Obstetric Investig. 2016;81:97–104. doi:10.1159/000381772
29. Ertürk Aksakal S, Güvenç Saçıntı H, Kiykac Altınbaş Ş, Tapısız ÖL, Engin-üstün Y. Tubo-ovaryan apseli hastalarda sistemik inflamatuvar belirteçlerin medikal tedavi başarısızlığını öngörmedeki yeri. Ege Tip Dergisi. 2022;61:184–191. doi:10.19161/etd.1128214
30. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infectious Dis Clin North Am. 2013;27:793–809. doi:10.1016/j.idc.2013.08.004
31. Romosan G, Valentin L. The sensitivity and specificity of transvaginal ultrasound with regard to acute pelvic inflammatory disease: a review of the literature. Arch Gynecol Obstetrics. 2014;289:705–714. doi:10.1007/s00404-013-3091-6
32. Delgado-Morell A, Nieto-Tous M, Andrada-Ripolles C, et al. Transvaginal ultrasound accuracy in the hydrosalpinx diagnosis: a systematic review and meta-analysis. Diagnostics. 2023;13(5):948. doi:10.3390/diagnostics13050948
33. Psilopatis I, Beckmann MW, Emons J, Schulmeyer CE. Ureterocele as differential diagnosis of hydrosalpinx—an interesting case from the clinical practice. J Surg Case Rep. 2024;2:rjad730. doi:10.1093/jscr/rjad730
34. Frock-Welnak DN, Tam J. Identification and treatment of acute pelvic inflammatory disease and associated sequelae. Obstet Gynecol Clin. 2022;49(3):551–579. doi:10.1016/j.ogc.2022.02.019
35. Che D, Yang Z, Wei H, Wang X, Gao J. The Adler grade by Doppler ultrasound is associated with clinical pathology of cervical cancer: implication for clinical management. PLoS One. 2020;15(8):e0236725. doi:10.1371/journal.pone.0236725
36. Floyd R, Anglim B. Tubo-ovarian abscess after vaginal delivery: a case report and review of current literature. Case Rep Women’s Health. 2023;39:e00526. doi:10.1016/j.crwh.2023.e00526
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of the CALLY Index in Hospitalized Patients with Pelvic Inflammatory Disease and Tubo-Ovarian Abscess
Ozbilgec S, Akkuş F, Donmez EE, Sahin M, Bahceci P, Acar A
International Journal of Women's Health 2026, 18:595902
Published Date: 7 April 2026