Back to Journals » Patient Preference and Adherence » Volume 15
Evaluation of the Community Pharmacy Comorbidities Screening Service on Patients with Chronic Diseases
Authors Lewicki J, Religioni U ![]() , Merks P
, Merks P
Received 23 March 2021
Accepted for publication 24 June 2021
Published 17 July 2021 Volume 2021:15 Pages 1611—1619
DOI https://doi.org/10.2147/PPA.S312341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jędrzej Lewicki,1 Urszula Religioni,2 Piotr Merks3
1Department of Pharmaceutical Technology, Faculty of Pharmacy, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland; 2Collegium of Business Administration, Warsaw School of Economics, Warsaw, Poland; 3Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszyński University, Warsaw, Poland
Correspondence: Piotr Merks
Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszynski University in Warsaw, Wóycickiego 1, Warsaw, 01-938, Poland
Email [email protected]
Objective: Evaluation of the implementation of pharmaceutical services to detect comorbidities in at-risk patients.
Methods: This study was carried out in community pharmacies across Poland in 2019 inside the specially designed service “Refer the Patient”. The project was intended for patients with selected chronic diseases. The patients were identified on the basis of their medications (active substances). At-risk patients were referred for prophylactic examinations to detect comorbidities.
Results: A total of 78 pharmacies took part in this study and 209 at-risk patients were identified. Out of the patients referred for examinations, 30% had deviant results, and 0.95% were diagnosed with new diseases.
Conclusion: Pharmaceutical services supporting screening tests among at-risk patients are highly recommended. Pharmacist intervention allows for early detection of comorbidities and prompt treatment. The pharmaceutical service “Refer the Patient” makes it possible to detect a disease at an early stage. Rapid implementation of treatment can prevent serious health consequences, maintains patient quality of life, and reduce treatment costs.
Keywords: pharmaceutical care pilot study, pharmaceutical care, pharmaceutical service, implementation, screening tests, chronic diseases
Introduction
Pharmaceutical care is characterized by the comprehensive care of patients by a pharmacist. This includes improvements in safety parameters of medication, treatment effectiveness and adherence. These have resulted in a reduction in the number of hospitalizations. The lack of patient adherence is the most significant cause of treatment failure.1–5 Global trends of development in the pharmaceutical services offered in community pharmacies are already improving pharmaceutical care, aiming also at making sure pharmacists can reach their full potential.6 In countries with a high standard of pharmaceutical service (eg Great Britain, USA, Canada, Finland), a high level of access to healthcare and a high quality of healthcare services can be observed (as evaluated by a Health Assessment Questionnaire),7 which is significantly different from the current standards of pharmacies in Poland.8,9 The provision of pharmaceutical care assumes improvements in the quality of life of patients, and in support for local healthcare systems, such as reducing healthcare costs.10–12
The pharmacy, as a healthcare facility, is the most frequently visited place by patients. According to the Polish Pharmaceutical Chamber, in August 2019 a pharmacy in Poland was visited on average by 3650 patients monthly.13 The availability of pharmacies combined with limited access to other health professionals makes pharmacies a good place for providing various medical services. One service that can be provided in pharmacies is identifying patients with potential comorbidities, along with referrals for diagnostic tests and medical consultations.14,15 In line with global trends, implementing these kinds of pharmaceutical services in Poland should be considered. These activities would increase the detection of comorbidities in many chronic patients and reduce future costs related to possible hospitalisations that are borne by public funds (the National Health Fund).16,17
Chronic diseases are currently the greatest challenge for healthcare systems in highly developed countries. Such diseases are associated with a high risk of death, reduced physical capacity and quality of life, as well as high costs.18–20 In 2018, 9.9 million people in Poland aged 18 years and older were diagnosed with hypertension, (around 31.5% of the adult population), and 2.9 million adults suffered from diabetes (9.1% of the population), constituting a large portion of Polish society.21,22 A lot of chronic patients are not diagnosed – in the case of diabetes, up to 45%.23 Considering the trend of population aging, the problems related to chronic diseases are going to worsen.
A lack of (or delayed) diagnosis of chronic diseases results in a rapid decline in health status and premature deaths of patients (from complications), which translates into higher costs borne by the healthcare system and lower state budget income.24–26 To maximize the possible prevention and detection of chronic diseases, screening tests are in use.27,28 Diseases designated for screening tests should have a high rate of incidence, be a serious health problem for the patients and society, show a high incidence and death rate, and have a relatively long symptom-free or early-symptomatic (possible to detect) period.29,30 Chronic diseases have all of the previously mentioned features and therefore screening tests are of great significance in this respect, with the effects noticeable at both health and financial levels.31
The vast majority of patients over the world are interested in screening tests in community pharmacies. Patients are attracted to the convenience of this solution, disclosing trust in their pharmacists and are willing to pay for these tests.32,33 In accordance with international standards, pharmacists are remunerated for providing this kind of service.34 In countries with the highest standards of pharmaceutical care, the supportive role of pharmacists can be seen in helping to conduct screening tests and to raise the number of people using this service.35
The main objective of this study was to evaluate the possibility of implementing a service in community pharmacies to detect comorbidities in patients at risk of chronic diseases. This study was also intended to increase the knowledge and awareness of patients and society on the key elements of a healthy lifestyle.
Methods
This study was carried out in willing community pharmacies across Poland between April and December 2019. The study was approved by the Bioethics Committee of the Nicolaus Copernicus University in Toruń (KB 33/2019; 29 January 2019). All participants were informed about the purpose of the study.
“Refer the Patient” is a modern pharmaceutical service provided by pharmacists to support public health. Community pharmacies refer patients at risk of chronic comorbidities for screening tests.6,36 This service has been adopted from similar services in Great Britain, the USA and Canada. Tests offered by pharmacists to at-risk patients are intended for early disease detection. Initially, a pharmacist qualifies a patient to the risk group for conducting diagnostic tests, before visiting a doctor, which assists in providing a prompt medical diagnosis and implementation of pharmacotherapy.
This project was designed for patients with the most problematic chronic conditions in Poland. To be enrolled in the study, a patient had to suffer from at least one of the selected diseases: diabetes (type 1 or 2), cardiovascular disorders (hypertension, abnormal heart rhythm), endometriosis, Crohn’s Disease, or rheumatoid arthritis (RA) of the hip or knee. Patient age was also an important criteria (>18 yrs).
The patients qualified for the screening tests received a referral sheet listing the different tests, to be given to the diagnostic facility. The tests evaluated kidney and liver function, lipid metabolism (cholesterol metabolism), and carbohydrate metabolism (glucose metabolism). Every package of tests covered a complete blood count, blood glucose levels, lipid profile, creatinine and albumin concentration, glycated haemoglobin (HbA1c), ALAT and ASPAT.
For a successful provision of the “Refer the Patient” service, the pharmacies received remuneration reimbursement proportional to the tasks performed by the pharmacists (in compliance with approved international standards for providing pharmaceutical care) – remuneration was paid on a monthly basis. Randomization of the pharmacies participating in this project was an important element based on demographic and geographic stratification, and categorization of the pharmacies (either independent or in a pharmacy chain).
Any community pharmacy in Poland could apply for participation in the “Refer the Patient” project. However, location criteria had to be met; a maximum distance of 30 km to the centre of the province main city where the Synexus diagnostic facility was situated to allow patients to freely reach the private diagnostic centre. The cities that took part in this study were: Gdynia, Gdańsk, Białystok, Warsaw, Lublin, Łódź, Krakow, Katowice, Częstochowa, Wrocław, Poznań and Szczecin. Information on the project was published on the website of the pilot project (www.skierujpacjenta.pl), on their Facebook page, on the websites of the Polish Pharmaceutical Chamber and Regional Pharmaceutical Councils, in the journal of the Polish Pharmaceutical Chamber, on trade web portals, in videos published on YouTube37–42, and in announcements during regional workshops (participants received leaflets about the pilot project). Pharmacies could apply for the project online or during workshops.
Designated pharmacists with a valid licence were responsible for providing this service in a given pharmacy. All the selected pharmacists had to complete a special training session. Thanks to pictogram pop-ups displayed on the screen of the software OPFARM Soft Nova, pharmacists were easily able to identify at-risk patients who could take part in the study. The “Refer the Patient” pop-up was displayed after scanning the EAN (European Article Number) code of the prescribed medication (including some OTC medications, eg for RA) used in the treatment of a disease qualifying patients for the screening tests. The pictogram suggested that the patient receiving the given medication was in a risk group and could be qualified for the pilot project (Figures 1 and 2).
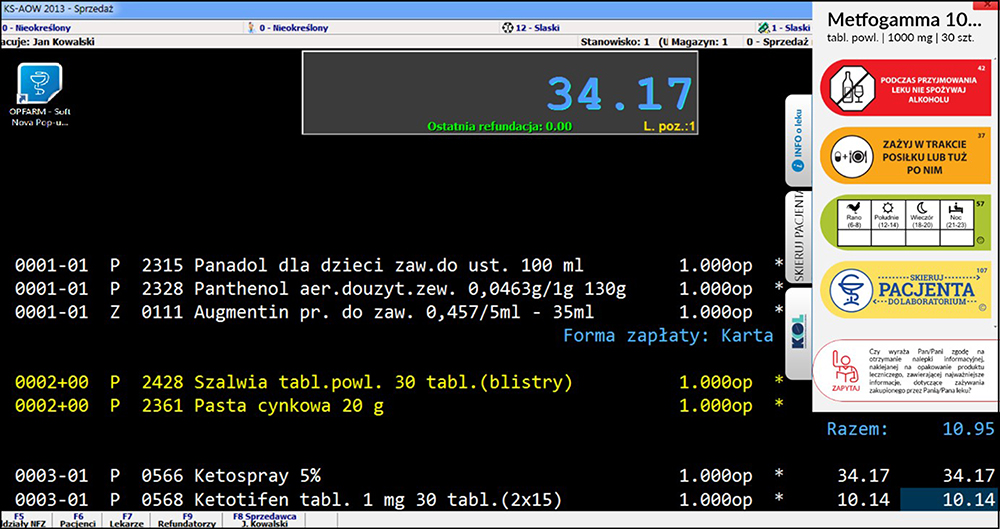 |
Figure 1 OPFARM Soft Nova pharmacy program (KAMSOFT program in the background) – displaying “pop-ups“ helping implement pharmaceutical care. The ”Refer the Patient” pop-up for a drug containing metformin. |
 |
Figure 2 “Refer the Patient” pop-up pattern – informing about the patient’s eligibility for screening tests. |
The software was developed in such a way that particular active substances in medications caused the pictogram pop-up to be displayed. There were 141 active substances assigned to the project, including those for the given diseases qualifying for tests, namely: 51 active substances used for diabetes type 1 and 2, 38 for cardiovascular disorders, 23 for endometriosis, 13 for Crohn’s Disease, and 16 for RA. This identification was used by the system to mark the patient as suitable for the study.
The Standard Operating Procedure (SOP) for the “Refer the Patient” service is as follows:
- A patient visits a pharmacy to have a prescription filled.
- A pharmacist fills the prescription. When scanning the EAN code of the medication, the information is transmitted to the OPFARM Soft Nova software. If the test algorithm detects a predisposing active substance or a combination of active substances, the software displays the “Refer the Patient” pop-up. This information informs the pharmacist that the patient administering a given medication suffers from one of the 5 analysed diseases (is in the risk group) (Figure 3).
- The patient is informed about the project and signs his/her consent to participate in the project.
- The pharmacist enters additional data of the patient and the pharmacy. All data entered in the registration tab is sent directly to the company managing the network of diagnostic centres.
- The follow-up patient interview and providing information by the coordinator about a healthy lifestyle.
 |
Figure 3 Patient workflow. |
The patient visits a particular diagnostic centre on the scheduled day and time. In the case of deviant results, the attending physician (patient’s own GP) can recommend more specialist examinations, or can diagnose a new disease and implement a new treatment, which means that the treatment can be implemented at an early stage of the disease. In the study, patients were also asked about their satisfaction with the service provided.
Results
Of the 145 pharmacies interested in the project (of which 66.2% were pharmacy chains and 33.8% independent pharmacies), 78 were enrolled (about 1% of all pharmacies in Poland). The remaining facilities did not undergo the entire procedure with the patient. Of all the pharmacies interested in the pilot project, 53.8% took part in the study, of which 75.7% were pharmacy chains and 24.4% independent pharmacies.
209 patients were enrolled in the study – 139 from independents pharmacies (66.5% of all the patients) and 70 from pharmacy chains (33.5% of all the patients). The mean age of the patients was 59.7 years (SD=11.5) (aged 24–83 years). The percentages of women and men for the entire study group were 64.1% and 35.9%, respectively. Of the 78 pharmacies that took part in the study, the average number of patients per pharmacy was 2.68.
In the vast majority of cases (87.0% of the patients), the active substances qualifying patients for the diagnostic tests were medications used for cardiovascular disorders. Type 1 or 2 diabetes was reported in 11 patients (6.83%). Finally, 6.21% of the active substances indicated RA.
The project coordinator managed contacted 174 out of the 209 patients taking part in the project (83.3% of all the participants) (follow-up). Of these contacted patients, 60.% were from independent pharmacies and 32.4% from pharmacy chains. The percentage of patients that did not have the time or were not interested in the project accounted for 9.4% from independent pharmacies and 22.1% from pharmacy chains. There were statistically significant differences in the distributions of particular answers between the groups of patients from independent pharmacies and pharmacy chains (p=0.0077).
Of the 71 patients who answered the coordinator’s question “Have the screening tests been carried out?”, 28 answered affirmatively to the question regarding taking the diagnostic tests (39.4%). Of the contacted patients who performed the tests, 48.1% were from independent pharmacies and 15.8% were from pharmacy chains. Of the contacted patients who did not perform the tests, 30.7% were from independent pharmacies and 47.4% were from pharmacy chains, and those who did not need diagnostic tests were 21.2% and 36.8%, respectively. From the entire study group, 39.4% took the diagnostic tests, 35.2% did not take the diagnostic tests and 25.4% did not need screening tests.
Of the 174 contacted patients, 50 (28.73% of contacted patients; 23.9% of all participants) answered the question regarding the test results. In the entire study group, 32% had normal results, 30% had deviant results, 30% had a lack of understanding of the results, 6% had a lack of knowledge of the results and needed to consult them with a doctor, and 2% were unwilling to discuss. In addition, some of the patients informed the coordinator about their deviant results, indicating mainly glucose and cholesterol levels, ALAT and ASPAT.
Of the 174 patients that the project coordinator managed to contact, 37 patients (21.3% of the contacted patients; 17.7% of all participants) made use of the results of the diagnostic tests, presenting those results to their doctors (64.5% from independent pharmacies and 16.7% from pharmacy chains). The patients visiting independent pharmacies presented their results to their doctors significantly more often than the patients visiting pharmacy chains (p=0.0304). The percentage of patients in the entire group who presented their results to their doctors was 56.8%. 43.2% of patients did not present their results to their doctor.
Two women (0.95% of all participants) aged 64 and 72 years suffering from hypertension and taking a beta-blocker (64-year-old: bisoprolol, 72-year-old: nebivolol) were diagnosed with a new disease. Thanks to performing the diagnostic tests and presenting the results to their attending physicians, both participants were diagnosed with a new disease: the 64-year-old woman (qualifying substance: bisoprolol) informed that in her case this was type 2 diabetes, and the other (72 years) did not give any additional information regarding her new disease. Both women informed their attending physicians about the implementation of a new treatment.
Of the 174 patients that the project coordinator managed to contact, 43 patients (24.7% of the contacted patients; 20.6% of all participants) answered the question regarding the appropriateness of this form of pharmacist care for patients, and whether this service should be offered in all pharmacies in the future, with 75% of those patients from independent pharmacies and 63.6% from pharmacy chains answering affirmatively to the question: “In your opinion, is this form of pharmacist care over patients good?”
Discussion The increasing number of chronic patients and comorbidities that is noticeable all over the world has already been seen in Poland.18,21,22,43 Screening tests are essential to diagnose chronic diseases and community pharmacies are the perfect places to identify at-risk patients.15,30,34,44 On the basis of the outcomes, it can be stated that this service has been successfully implemented in community pharmacies in Poland and detecting deviant test results allows for the diagnosis of new diseases. Similar outcomes have been obtained in other studies conducted in community pharmacies across the world.45,46
Another objective of the project was to increase the knowledge and awareness of patients and society of the key elements of a healthy lifestyle. Only patients aware of their health condition and potential risk are properly motivated to undertake changes and if necessary, implement a new treatment.31,47,48 This element was fully accomplished – 72.1% of the patients gave an affirmative answer to the question regarding the appropriateness of the project.
Despite the continuous promotion, pharmacies were moderately interested in the pharmaceutical care pilot project, with only 145 pharmacies in Poland interested in carrying it out, of which 78 (by signing a research contract) declared achieving the principles of the pilot project (53.79% of the applying pharmacies). Pharmacists around the world have shown much more interest in this kind of project. During the project of screening tests for type 2 diabetes organised in Italy in the region of Piedmont, 93% of the pharmacies (1400 facilities) were interested in the project, of which 1298 implemented it (92.71% of all the interested pharmacies).49 The outcomes of the questionnaire survey conducted by pharmacists from community pharmacies in Poland in 2019 indicate that pharmacists feel as if they do not have the time/space to provide pharmaceutical care, this is not their duty, they are insufficiently trained/educated, and that this is not reimbursed.50
The vast majority of pharmacies that took part in the project were pharmacy chains (75.65% of the pharmacies). What is more, only 38.77% of the applying independent pharmacies signed a research contract, compared to 61.64% of the chain pharmacies. It is noticeable that even though pharmacy chains significantly outnumber independent pharmacies in the “Refer the Patient” project, the latter performed better, registering and referring more patients for tests. Similar outcomes were obtained in the study on pharmaceutical services in the United States.51
Global projects show that the ratio of the number of pharmacies actively taking part in the study to the number of participating patients is significantly higher than in the case of the “Refer the Patient” service. In a 2019 study organized in Great Britain, 9 pharmacies conducted screening tests for diabetes; 328 patients took part in the project within six months (36.5 patients per pharmacy).12 A higher result was obtained in an Australian study.15 The low interest in Poland may result from the low number of pharmacists (ca. 2) per pharmacy,52,53 which makes it difficult to provide effective additional pharmaceutical care. The World Health Organisation points out that the number of pharmacists per 10,000 inhabitants in Poland is lower than in the countries with a top level of pharmaceutical care.54
209 patients took part in the “Refer the Patient” project. A joint compilation of 50 projects related to screening tests conducted in pharmacies all over the world has reported between 18 and 93,258 patients participated in the study groups.31 Although the group of patients in the “Refer the Patient” service is at the low end of this participation, this is enough to evaluate the implementation.
In the “Refer the Patient” project, particular active substances prescribed to the patient qualified the patient to the risk group, and to take part in the study – the whole procedure took about 4 minutes. Studies conducted in pharmacies all over the world show that the most common form of qualifying patients to the risk group is a questionnaire survey and/or taking body measurements. Studies indicate that this process takes on average 10.5 minutes.31,55 The advantage of the system of detection of at-risk patients used in the “Refer the Patient” project is noticeable here. The method of qualifying pharmacy clients for screening tests was a standardized procedure. As other researchers point out, it is important to standardize all the procedures in this kind of project to allow for measurable outcomes.56
In the diagnostic service, 86.96% of the referred patients were being treated for cardiovascular disorders. None of the patients with endometriosis or Crohn’s Disease were qualified for diagnostic tests. For Crohn’s Disease, this was the result of a low frequency of the condition in relation to the diseases taken into consideration in this project.57
A month after registering a patient for diagnostic tests, the project coordinator contacted the patient on the phone. Over 83% of the patients answered the phone. Outcomes of the evaluation of this type of follow-up after screening tests for osteoporosis in pharmacies in the USA were much lower – only 57.33% of the study group answered the phone.58
In the “Refer the Patient” study, 30% of the patients reported deviant results from the diagnostic tests. Additional information given by the patients showed that these problems were largely connected with glucose and cholesterol levels, ALAT and ASPAT, which predisposed them to the group of patients with civilisation diseases. Outcomes obtained in similar projects carried out all over the world indicate an even higher percentage of deviant results. For example in Italy, 53% of the patients had deviant test results.40 In that study, 6% of the patients reported a lack of understanding of the results. A study carried out in a hospital in Baltimore in 2017 indicates that the vast majority of patients do not understand the test results and prefer that they are interpreted by a doctor.59
Also, in this study, 0.95% of the patients had a new disease detected and a new treatment implemented by their attending physician. It may be presumed that there were more patients diagnosed with a new disease – as it was not possible to contact some of the patients, some of those with deviant results may not have been relayed to the coordinator. In a study carried out in Italy, of the 5977 at-risk patients taking part in the project, 107 (1.79%) were diagnosed with diabetes.49 In Thailand, of 397 patients, 2 (0.5%) were diagnosed with type 2 diabetes.60 In a study conducted as an overview of similar projects, the percentage of confirmed diagnoses started with 0.35% of all the patients using the service.31
Patient opinions confirm a positive reception of the “Refer the Patient” service. In countries where the status of pharmacies and pharmacists is higher than in Poland, patients are willing to pay for receiving these tests in the pharmacy – 79% of respondents in the USA stated that they would pay up to $50 for such a test in a pharmacy.32
The implementation of pharmaceutical care is a gradual and long process. The cycle of changes should begin from the ground up and be realised in a coordinated manner. This may require radical legal, administrative and organizational solutions.61 Measuring the results of a given service to achieve accurate results (ie its evaluation) is only possible by harmonizing the procedures and criteria in this service. Standardization is responsible for maximum profitability and the effectiveness of the provided services.62
Conclusions
Our study indicates that a pharmacy service offering screening tests to patients at risk of chronic diseases is highly recommended. The outcomes of this project show a very big potential of this service, and pharmacists can be an important link in the course of a treatment prescribed by a doctor, complementing cooperation between medical professions. Pharmacist intervention can enable early diagnosis of new diseases and implementation of treatment. The “Refer the Patient” project indicates the high effectiveness of pharmaceutical care and at the same time the exhibits the unused potential of pharmacists in community pharmacies.
This project of screening tests was very well received by the patients. While the level of interest by the pharmacies in providing a new service is not satisfying, this may be a result of the pharmacists’ lack of awareness and willingness to get involved in pharmaceutical care services that are not obligatory in Poland.
A more detailed evaluation of the effectiveness of pharmaceutical services in detecting comorbidities requires further studies on a larger scale. Future projects should put more emphasis on educating pharmacists in the role of pharmaceutical care in public health.
Study Limitations
Only two criteria of patient inclusion were taken into account in the study: age and the presence of a specific disease entity. Patients’ past behavior and disease control have not been studied.
Ethics Statement
The study was approved by Ethics Committee at the Collegium Medicum in Bydgoszcz, Poland (KB 33/2019). All participants were informed about the purpose of the study. We confirm that consent was received from the study participants and that the guidelines outlined in the Declaration of Helsinki were followed.
Acknowledgments
Thank you to Dr Kevin Chung, Staff Pharmacist, Pharmacy Department at Children's Hospital of Eastern Ontario, Ottawa in Canada for proofreading the manuscript. We would like to thank Synexus for supporting the project.
Funding
The OPFARMSoftNova patient counselling software project has received financial support from LQT Fund S.A. in Gdańsk, and from The National Centre of Research and Development in Warsaw, on the basis of the Contract on Support within the Systemic Project “Bridge Alfa”, concluded on 3 December 2015.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hasan SS, Thiruchelvam K, Kairuz T, Abbas N,Babar ZUD. Pharmacy practice and its research: evolution and definitions. In: Babar ZUD, editor. Encyclopedia of Pharmacy Practice and Clinical Pharmacy. Elsevier - Academic Press: 2019:1–6.
2. Allemann S, Foppe van Mil JW, Botermann L, Berger K, Griese N, Hersberger K. Pharmaceutical care – the PCNE definition 2013. Int J Clin Pharm. 2014;36:544–555. doi:10.1007/s11096-014-9933-x
3. Aslani P, Ahmed R, Alves da Costa F. The Role of Adherence in Pharmaceutical Care. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer; 2019:41–57.
4. Roque Obreli-Neto P, Molino Guidoni C, Oliveira Baldoni A, et al. Effect of a 36-month pharmaceutical care program on pharmacotherapy adherence in elderly diabetic and hypertensive patients. Int J Clin Pharm. 2011;33:642–649. doi:10.1007/s11096-011-9518-x
5. Wei L, Yang X, Jie L, et al. Effect of pharmaceutical care on medication adherence and hospital admission in patients with chronic obstructive pulmonary disease (COPD): a randomized controlled study. J Thorac Dis. 2014;6:656. doi:10.3978/j.issn.2072-1439.2014.06.20
6. Merks P. Opieka Farmaceutyczna Od Zdefiniowania Pojęcia Do Mechanizmów Realizacji Na Przykładzie Wielkiej Brytanii. Związek Zawodowy Pracowników Farmacji (ZZPF); 2018:119.
7. GBD 2016 Healthcare Access and Quality Collaborators. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: a systematic analysis from the Global Burden of Disease Study 2016. Lancet. 2018;391:2236–2271.
8. Brown L, Seoane-Vazquez E. The Pharmacist Guide to Implementing Pharmaceutical Care. North America: Pharmaceutical Care; 2019:145–158.
9. Alves da Costa F. The Pharmacist Guide to Implementing Pharmaceutical Care. Europe: Pharmaceutical Care; 2019:159–171.
10. Barry HE, Hughes CM. Economical, Clinical, and Humanistic Outcomes and Pharmaceutical Care. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer; 2019:119–127.
11. Świeczkowski D, Bandurska E, Merks P, Krysiński J. Opieka farmaceutyczna w szpitalu szansą na poprawienie ekonomii szpitala, zdrowia pacjenta i budżetu państwa [Pharmaceutical care in a hospital as an opportunity to improve the hospital’s economy, patient health and the state budget]. Farm Pol. 2013;69:567–570.
12. Wrigh D, Little R, Turner D, Thornley T. Diabetes screening through community pharmacies in England: a cost-effectiveness study. Pharmacy. 2019;7:1–12.
13. Rynek apteczny w sierpniu 2019 wyżej niż rok wcześniej (+2.3%). Spadek względem lipca 2019 (−6.7%); 2019. Available from: http://www.aptekarzpolski.pl/2019/09/rynek-apteczny-w-sierpniu-2019-wyzej-niz-rok-wczesniej-2-3-spadek-wzgledem-lipca-2019-6-7/.
14. Corlett SA, Krska J. Evaluation of NHS health checks provided by community pharmacies. J Public Health (Oxf). 2016;38(4):e516–e523. doi:10.1093/pubmed/fdv153
15. Mc Namara KP, Krass I, Peterson GM, et al. Implementing screening interventions in community pharmacy to promote interprofessional coordination of primary care - a mixed methods evaluation. Res Social Adm Pharm. 2020;16(2):160–167. doi:10.1016/j.sapharm.2019.04.011
16. NHF on health. Registered Epidemiology. Warsaw, Warszawa: Cukrzyca, Headquarters of the National Health Fund; 2019:12–17.
17. NHF on health. Hypertension in the Data of the National Health Fund, Hypertension. Warsaw: National Health Fund Headquarters; 2019:13–32.
18. Scaratti C, Leonardi M, Silvaggi F, et al. Mapping European Welfare Models: state of the art of strategies for professional integration and reintegration of persons with chronic diseases. Int J Environ Res Public Health. 2018;15(4):781–801. doi:10.3390/ijerph15040781
19. Health at a glance: Europe 2016 State of health in the EU cycle; 2016. Available from: https://www.oecd-ilibrary.org/docserver/9789264265592en.pdf?expires=1590314324&id=id&accname=guest&checksum=648349C2A614F180B8422DA0D4BC7FF2.
20. Brennan P, Perola M, van Ommen GJ, Riboli E; European Cohort Consortium. Chronic disease research in Europe and the need for integrated population cohorts. Eur J Epidemiol. 2017;32(9):741–749. doi:10.1007/s10654-017-0315-2
21. NFZ o zdrowiu, nadciśnienie tętnicze [NHF on health, arterial hypertension]; 2019. Available from: https://zdrowedane.nfz.gov.pl/pluginfile.php/80/mod_resource/content/1/nadcisnienie-tetnicze-raport-nfz-2019-small.pdf.
22. NFZ o zdrowiu, cukrzyca [NHF on health, diabetes]; 2019. Available from: https://zdrowedane.nfz.gov.pl/pluginfile.php/205/mod_resource/content/4/nfz_o_zdrowiu_cukrzyca.pdf.
23. Krass I, Hoti K, Mc Namara K. Management of endocrine disorders and the Pharmacist’s role: diabetes. In: Zaheer-Ud-Din B, editor. Encyclopedia of Pharmacy Practice and Clinical Pharmacy. Elsevier Inc; 2019:447–460.
24. Goto M, Goto A, Ikeda N, Noda H, Shibuya K, Noda M. Factors associated with untreated diabetes: analysis of data from 20,496 participants in the Japanese National Health and Nutrition Survey. PLoS One. 2015;10(3):1–8. doi:10.1371/journal.pone.0118749
25. Ismail H, Azahadi Omar M, Aqilah Noor Hisham A, et al. Undiagnosed type 2 diabetes mellitus and its risk factors among malaysians: findings of a nationwide study. Int J Public Health Res. 2016;6:677–684.
26. Clarke P, Gray A, Legood R, Briggs A, Holman R. The impact of diabetes-related complications on healthcare costs: results from the United Kingdom Prospective Diabetes Study (UKPDS Study No. 65). Diabet Med. 2003;20(6):442–450. doi:10.1046/j.1464-5491.2003.00972.x
27. Deyo D, Hemingway J, Hughes DR. Identifying patients with undiagnosed chronic conditions: an examination of patient costs before chronic disease diagnosis. J Am Coll Radiol. 2015;12(12):1388–1394. doi:10.1016/j.jacr.2015.09.012
28. Benefits and risks of screening tests; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279418/.
29. Fórmankiewicz B, Jawień A. The role of screening in early diagnosis of abdominal aortic aneurysm. Acta Angiol. 2012;18:1–8.
30. What makes a screening exam “good”?; 2006. Available from: https://journalofethics.ama-assn.org/article/what-makes-screening-exam-good/2006-01.
31. Ayorinde AA, Porteous T, Sharma P. Screening for major diseases in community pharmacies: a systematic review. Int J Pharm Pract. 2013;21(6):349–361. doi:10.1111/ijpp.12041
32. Hohmeier KC, Loomis B, Gatwood J. Consumer perceptions of and willingness-to-pay for point-of-care testing services in the community pharmacy. Res Social Adm Pharm. 2018;14(4):360–366. doi:10.1016/j.sapharm.2017.04.011
33. Brewer A, Hanna C, Eckmann L, Schadler A, Divine H. Patient awareness, willingness, and barriers to point-of-care hepatitis C screening in community pharmacy. J Am Pharm Assoc (2003). 2018;58(4):69–72. doi:10.1016/j.japh.2018.04.031
34. Service specification for NHS community pharmacy blood pressure and atrial fibrillation drop-in service; 2018. Available from: https://psnc.org.uk/nottinghamshire-lpc/wp-content/uploads/sites/21/2019/02/2018_01_DENO-Blood-Pressure-and-AF-ScreeningProject-Service-Specificati….pdf.
35. Hill H, Cardosi L, Henson L, et al. Evaluating advanced pharmacy technician roles in the provision of point-of-care testing. J Am Pharm Assoc (2003). 2020;60(4):1–6. doi:10.1016/j.japh.2020.02.024
36. Merks P. Informacje dla aptek i farmaceutów: usługa farmaceutyczna skieruj pacjenta - do laboratorium na badanie profilaktyczne [Information for pharmacies and pharmacists: pharmaceutical service refer the patient - to the laboratory for a preventive examination]; 2019. Available from: https://www.skierujpacjenta.pl/o-projekcie.
37. Programy pilotażowe opieki farmaceutycznej w Polsce [Pilot pharmaceutical care programs in Poland]; 2019. Available from: https://www.nia.org.pl/2019/03/14/programy-pilotazowe-opieki-farmaceutycznej-w-polsce/.
38. Skieruj pacjenta [refer the patient]; 2019. Available from: https://www.facebook.com/Skieruj-Pacjenta-489016134955707/.
39. NIA on Pharmaceutical Care Pilot Programs. NIA o programach pilotażowych opieki farmaceutycznej; 2019. Available from: https://www.aptekarzpolski.pl/aktualnosci/nia-o-programach-pilotazowych-opieki-farmaceutycznej/.
40. Skieruj pacjenta! [refer the patient!]; 2019. Available from: http://www.farmakoekonomika.com.pl/skieruj-pacjenta/.
41. Europejski program badania pilotażowego usług opieki farmaceutycznej w chorobach przewlekłych [European Chronic Disease Pharmaceutical Care Pilot Study Program]; 2019. Available from: https://www.loia.pl/news/2418/europejski-program-badania-pilotazowego-uslug-opieki.html.
42. Usługa farmaceutyczna: skieruj pacjenta [pharmaceutical service: refer the patient]; 2019. Available from: https://www.youtube.com/watch?v=74VdWns-1fM.
43. Busse R, Blümel M, Scheller-Kreinsen D, Zentner A. Tackling Chronic Disease in Europe - Strategies, Interventions and Challenges. European Observatory on Health Systems and Policies. WHO Regional Office Europe; 2010:111.
44. Saldarriaga EM, Vodicka E, La Rosa S, Valderrama M, Garcia PJ. Point-of-care testing for anemia, diabetes, and hypertension: a pharmacy-based model in Lima, Peru. Ann Glob Health. 2017;83(2):394–404. doi:10.1016/j.aogh.2017.03.514
45. Sushilkumar PL, Mahendrakumar BJ, Suman B, Gloria S, Chaitanya K. Implementation and evaluation of health screening services to diabetic and hypertensive patients in a selected community pharmacy at belgaum city. Asian J Pharm Clin Res. 2015;8:305–315.
46. Jahangard-Rafsanjani Z, Hakimzadeh N, Sarayani A, et al. A community pharmacy-based cardiovascular risk screening service implemented in Iran. Pharm Pract (Granada). 2017;15(2):1–6. doi:10.18549/PharmPract.2017.02.919
47. Waszyk-Nowaczyk M, Guzenda W, Plewka B, et al. Screening services in a community pharmacy in Poznan (Poland) to increase early detection of hypertension. J Clin Med. 2020;9(8):2572–2583. doi:10.3390/jcm9082572
48. Gruman J, Rovner MH, French ME, et al. From patient education to patient engagement: implications for the field of patient education. Patient Educ Couns. 2010;78(3):350–356. doi:10.1016/j.pec.2010.02.002
49. Gnavi R, Sciannameo V, Baratta F, et al. Opportunistic screening for type 2 diabetes in community pharmacies. Results from a region-wide experience in Italy. PLoS One. 2020;15(3):1–11. doi:10.1371/journal.pone.0229842
50. Aptekarz Polski, Opieka farmaceutyczna – w opinii aptekarzy [Polish pharmacist, pharmaceutical care - in the opinion of pharmacists]; 2010. Available from: https://www.aptekarzpolski.pl/opieka-farmaceutyczna/01-2010-opieka-farmaceutyczna-w-opinii-aptekarzy/.
51. Briesacher B, Corey R. Patient satisfaction with pharmaceutical services at independent and chain pharmacies. Am J Health Syst Pharm. 1997;54(5):531–536. doi:10.1093/ajhp/54.5.531
52. Główny Urząd Statystyczny, Apteki i punkty apteczne w 2018 roku [Central Statistical Office of Poland, pharmacies and pharmacy outlets in 2018]; 2018. Available from: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/apteki-i-punkty-apteczne-w-2018-roku,15,3.html.
53. Merks P, Bryła A, Harężlak T, et al. Ocena jakości pracy farmaceutów w aptekach ogólnodostępnych na terenie Polski [Assessment of the quality of pharmacists’ work in generally accessible pharmacies in Poland]. Farm Pol. 2019;75:233–237. doi:10.32383/farmpol/116222
54. World Health Organization. Density of pharmacists (total number per 10 000 population, latest available year); 2018. Available from: https://www.who.int/gho/health_workforce/pharmacists_density/en/.
55. Willis A, Rivers P, Gray LJ, Davies M, Khunti K. The effectiveness of screening for diabetes and cardiovascular disease risk factors in a community pharmacy setting. PLoS One. 2014;9(4):1–9. doi:10.1371/journal.pone.0091157
56. Fikri-Benbrahim N, Martínez-Martínez F, Saéz-Benito L, et al. Assessment of a screening protocol for type 2 diabetes in community pharmacy. The DiabNow study. Diabetes Res Clin Pract. 2015;108(3):49–52. doi:10.1016/j.diabres.2015.03.006
57. Wawryniuk A, Rybak M, Szwajkosz K, et al. Choroba Leśniowskiego Crohna będąca przewlekłym stanem zapalnym przewodu pokarmowego [Crohn’s disease, which is a chronic inflammation of the gastrointestinal tract]. J Educ. 2017;7:80–98.
58. Goode JV, Swiger K, Bluml BM. Regional osteoporosis screening, referral, and monitoring program in community pharmacies: findings from project ImPACT: osteoporosis. J Am Pharm Assoc (2003). 2004;44(2):152–160. doi:10.1331/154434504773062609
59. Athar MW, Mativo C, Landis R, Wright SM. Communication of laboratory data and diagnostic test results to hospitalized patients: a study of preferences and recall. Patient Prefer Adherence. 2016;10:1409–1413. doi:10.2147/PPA.S111190
60. Dhippayom T, Fuangchan A, Tunpichart S, Chaiyakunapruk N. Opportunistic screening and health promotion for type 2 diabetes: an expanding public health role for the community pharmacist. J Public Health (Oxf). 2013;35(2):262–269. doi:10.1093/pubmed/fds078
61. Merks P, Świeczkowski D, Blicharska E, et al. Perspektywy wdrożenia opieki farmaceutycznej do praktyki aptecznej w warunkach polskiego systemu opieki zdrowotnej [Prospects for the implementation of pharmaceutical care into pharmacy practice in the conditions of the Polish healthcare system]. Czasopismo Aptekarskie. 2015;8–9:28–38.
62. Lavelle J, Schast A, Keren R. Standardizing care processes and improving quality using pathways and continuous quality improvement. Curr Treat Options Peds. 2015;1:347–358. doi:10.1007/s40746-015-0026-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.